review of invasive prenatal testing at rahima moosa …
TRANSCRIPT

REVIEW OF INVASIVE PRENATAL
TESTING AT RAHIMA MOOSA
MOTHER AND CHILD HOSPITAL
Chrysanthi Georgiou
A Dissertation submitted to the Faculty of Health Sciences, University f the
Witwatersrand, in partial fulfilment of the requirements for the degree of Master of
Medicine in the branch of Obstetrics and Gynaecology
Johannesburg, 2016

ii
DECLARATION
I, Chrysanthi Georgiou, declare that this M.Med is my own, unaided work. It is being
submitted for the Degree of Master of Medicine in Obstetrics and Gynaecology at the
University of the Witwatersrand, Johannesburg. It has not been submitted before for
any degree or examination at any other University.
.................................
..............day of ...................2017 in...............................

iii
To my parents,
who taught me the art of medicine and the importance of women's healthcare.
Thank you for your support, guidance and teaching, always.

iv
PUBLICATIONS AND PRESENTATIONS
Presentation at Academic Meeting, Rahima Moosa Mother and Child Hospital,
December 2016
Poster presentation at the Royal College of Obstetricians and Gynaecologists World
Congress, Cape Town 2017
Publication of abstract in the British Journal of Obstetrics and Gynaecology, Vol 124
(DOI: 10.1111/1471-0528.3_14572)
Presentation will be presented at the BIT 5th International Congress of Gynaecology
and Obstetrics, China, Nov 2017

v
ABSTRACT
Introduction
Invasive prenatal testing is the gold standard of prenatal diagnosis of chromosomal
abnormalities. Outcomes of invasive prenatal procedures have been studied
previously, however it has not been looked at in a resource poor, tertiary setting in
South Africa.
Aim and objectives
The aim of this study is to review the outcome of invasive prenatal testing at Rahima
Moosa Mother and Child Hospital (RMMCH) from January 2014 to May 2016. The
main objectives of the study were to evaluate invasive prenatal testing in terms of
indications, ultrasound markers, cytogenetic diagnosis, complications and pregnancy
outcome.
Methods
The study took place at RMMCH, a regional academic hospital in Johannesburg
which performs approximately 12 000 deliveries annually. Charts were reviewed
retrospectively for patients who underwent invasive prenatal testing.
Results
Ninety-seven patients were identified and 96 results obtained. The main indication
for invasive prenatal testing was abnormal ultrasound findings followed by advanced
maternal age. In total, 12,5% of test results were abnormal, including two patients
with Trisomy 13, two with Trisomy 18, two with Trisomy 21, two with Klinefelter
syndrome, one with a balanced translocation, one with cystic fibrosis, one with spinal
muscular atrophy and one with Wolf-Hirschorn syndrome. The miscarriage rate was
1,5%. There were four terminations of pregnancy directly related to an abnormal
invasive test result.
Conclusion
It is expected that in a resource restricted area where biochemical screening is not
available that advanced maternal age and ultrasound findings are the main reasons
to lead to invasive prenatal testing. The rate of abnormalities found is higher than
internationally quoted and the miscarriage rate higher than the internationally

vi
accepted 0,5-1%, this is likely due to selection bias and sample size. The study
shows that an invasive testing service can be successfully run in a resource
restricted setting but ongoing education of the availability of the service in the public
sector is needed.

vii
ACKNOWLEDGEMENTS
Thank you to Professor H Lombaard and Dr A Wise, my supervisors, for your
guidance, advice and support throughout the research process.
Thank you to Dr R Adams, Dr E Bera and my supervisors for providing an excellent
invasive prenatal testing service at Rahima Moosa Mother and Child Hospital.
Thank you to the staff at the records department, ultrasound department and
National Health Laboratory at Rahima Moosa Mother and Child Hospital for all their
assistance.
The staff of the ultrasound team must be commended on their excellent skills in
detecting both soft markers and structural abnormalities.

viii
TABLE OF CONTENTS
DECLARATION......................................................................................................... ii
DEDICATION............................................................................................................ iii
PUBLICATIONS AND PRESENTATIONS............................................................... iv
ABSTRACT............................................................................................................... v
ACKNOWLEDGEMENTS........................................................................................ vii
TABLE OF CONTENTS.......................................................................................... viii
LIST OF ABBREVIATIONS..................................................................................... xii
LIST OF TABLES.................................................................................................... xiii
LIST OF DIAGRAMS...................................................................................... ....... xiv
LIST OF GRAPHS................................................................................................... xv
1. INTRODUCTION .................................................................................................... 1
1.1 Background ........................................................................................... 1
1.1.1 Serum Markers and Ultrasound screening tests........................................ 1
1.1.2 Non Invasive Prenatal Testing (NIPT)............. ......................................... 6
1.1.3 Invasive Prenatal Testing......................... ................................................ 8
1.1.3.1 Introduction.......................................................................................... 8
1.1.3.2 Amniocentesis...................................................................................... 9
1.1.3.3 Chorionic Villous Sampling.................................................................10
1.1.3.4 Cordocentesis.....................................................................................10
1.1.4 Indications for Invasive Prenatal Testing..................................................11
1.1.4.1 Advanced Maternal Age..................................................................... 12
1.1.4.2 Chromosomal Abnormalities.............................................................. 14
1.1.4.3 Other Indications for Invasive Prenatal Testing................................. 16
1.1.5 Laboratory Technique in Invasive Prenatal Testing................................. 17
1.1.6 Complications of Invasive Prenatal testing............................................... 18
1.1.6.1 Risk of Fetal Loss.............................................................................. 18
1.1.6.2 Other complications of amniocentesis............................................... 20

ix
1.1.6.3 Other Complications of Chorionic Villous Sampling.......................... 21
1.1.6.4 Other Complications of Cordocentesis.............................................. 22
1.1.6.5 Infective complications including HIV transmission........................... 22
1.1.7 Counselling for Prenatal Testing............................................................... 24
1.2 Purpose of Study............................................................................................ 25
1.3 Setting............................................................................................................. 26
1.4 Objectives of study......................................................................................... 27
2. MATERIALS AND METHODS ............................................................................. 28
2.1 Study sample....................................................................................... 28
2.1.1 Study population............................................................................ 28
2.1.2 Timing ............................................................................................ 28
2.2 Methods..................................... .......................................................... 28
3. RESULTS... ..........................................................................................................30
3.1 Study Population Demographics.................................................................... 30
3.1.1 Age........................................................................................................... 30
3.1.2 Ethnicity.................................................................................................... 30
3.1.3 Parity......................................................................................................... 31
3.1.4 Gravidity.................................................................................................... 31
3.1.5 Chronic Illnesses and Medication use...................................................... 31
3.1.6 Smoking, Alcohol use and Illicit Drug use................................................. 32
3.1.7 Booking Status of Patients........................................................................ 33
3.1.7.1 Rhesus Blood Group......................................................................... 33
3.1.7.2 HIV Status.......................................................................................... 33
3.1.7.3 RPR Status........................................................................................ 34
3.1.7.4 Haemoglobin..................................................................................... 34

x
3.1.8 Gestational age at first booking................................................................ 34
3.2 Patient results................................................................................................. 34
3.2.1 Chromosomal and Genetic Abnormalities found in the sample................ 36
3.2.1.1 Trisomy 21......................................................................................... 37
3.2.1.2 Trisomy 18......................................................................................... 38
3.2.1.3 Trisomy 13......................................................................................... 38
3.2.1.4 Sex Chromosome Abnormalities....................................................... 39
3.2.1.5 Other Chromosomal Abnormalities.................................................... 40
3.2.1.6 Genetic Abnormalities........................................................................ 40
3.2.2 Structural Abnormalities found in the sample........................................... 44
3.3 Indications for Invasive Prenatal Testing....................................................... 47
3.3.1 Abnormal Ultrasound Findings................................................................. 48
3.3.2 Advanced Maternal Age........................................................................... 51
3.3.3 Family History of Chromosomal and Genetic Abnormalities................... 52
3.3.4 Positive Biochemical Screening Tests...................................................... 52
3.3.5 Other Indications for Invasive Prenatal Testing........................................ 53
3.4 Invasive Prenatal Tests Performed................................................................. 53
3.5 Cytogenetic Diagnosis Made.......................................................................... 55
3.5.1 Laboratory Analysis of Results................................................................. 55
3.5.2 Sexing Errors and Culture Errors.............................................................. 55
3.6 Complications of Invasive Prenatal Testing.................................................... 56
3.7 Pregnancy Outcomes..................................................................................... 56
4. DISCUSSION....................................................................................................... 58
4.1 Introduction..................................................................................................... 58

xi
4.2 Patient Population Demographics.................................................................. 58
4.2.1 Antenatal Care - Booking and Referrals................................................... 58
4.2.2 Ethnicity.................................................................................................... 59
4.2.3 HIV and Invasive Prenatal Testing........................................................... 59
4.3 Indications for Prenatal Testing...................................................................... 61
4.3.1 Abnormal Ultrasound Findings................................................................. 62
4.3.2 Advanced Maternal Age........................................................................... 63
4.3.3 Chromosomal Abnormalities..................................................................... 63
4.4 Invasive Prenatal Tests Performed................................................................. 64
4.5 Cytogenetic Tests Performed......................................................................... 65
4.6 Complications of Invasive Prenatal Testing.................................................... 66
4.7 Pregnancy Outcomes..................................................................................... 66
4.8 Record Keeping and Loss to Follow up.......................................................... 67
4.9 Invasive Prenatal Testing Service.................................................................. 67
4.10 Limitations..................................................................................................... 68
4.11 Recommendations........................................................................................ 69
4.12 Conclusion.................................................................................................... 70
APPENDIX A............................................................................................................ 72
APPENDIX B............................................................................................................ 77
APPENDIX C............................................................................................................ 78
REFERENCES......................................................................................................... 79

xii
LIST OF ABBREVIATIONS
ACOG American College of Obstetricians and Gynaecologists
AMA Advanced Maternal Age
ART Antiretroviral Therapy
BHCG Human Chorionic Gonadotropin
CD4 Cluster of Differentian 4
CVS Chorionic Villous Sampling
DNA Deoxyribonucleic Acid
FISH Fluorescent In Situ Hybridisation
FMF Fetal Medicine Foundation
Hb Haemoglobin
HIV Human Immunodeficiency Virus
IUFD Intrauterine Fetal Death
LR Likelihood Ratio
MA Maternal Age
NB Nasal Bone
NIPT Non Invasive Prenatal Testing
NT Nuchal Translucency
PAPP-A Pregnancy Associated Plasma Protein A
PCR Polymerase Chain Reaction
PIPP Perinatal Problem Identification Program
QF-PCR Quantitative Fluorescent Polymerase Chain Reaction
REDCAP Research Electronic Data Capture
RCOG Royal College of Obstetricians and Gynaecologists
RMMCH Rahima Moosa Mother and Child Hospital
RPR Rapid Plasma Reagin
SOGC Society of Obstetricians and Gynaecologists of Canada
TOP Termination of Pregnancy
VL Viral Load

xiii
LIST OF TABLES
Table 1.1: Likelihood ratios for Trisomy 21 for each soft marker .................... 3
Table 1.2: Detection rate of Trisomy 21 and false positive rate of
screening tests .................................................................................. 6
Table 1.3: Rates of chromosomal abnormalities in several studies............... 15
Table 3.1: Chromosomal abnormalities found in the sample......................... 42
Table 3.2: Outcome of pregnancies with fetuses affected by
chromosomal abnormalities......................................................... 44
Table 3.3: Indications for invasive prenatal testing........................................ 47

xiv
LIST OF DIAGRAMS
Diagram 3.1: Flow diagram of results............................................................ 35
Diagram 3.2: Relationship between chromosomal and structural abnormalities
....................................................................................................................... 36

xv
LIST OF GRAPHS
Graph 3.1: Sample distribution by ethnicity............ ...................................... 30
Graph 3.2: Chromosomal abnormalities in the sample.................................. 37
Graph 3.3: Indications for invasive prenatal testing....................................... 48
Graph 3.4: Frequency for types of ultrasounds performed initially................ 49
Graph 3.5: Frequency of soft markers........................................................... 50
Graph 3.6: Invasive prenatal tests performed................................................ 54
Graph 3.7: Laboratory analysis of results...................................................... 55

1
1 INTRODUCTION
1.1 BACKGROUND
In the modern era of medicine combined first trimester screening is the gold standard
for screening women for chromosomal anomalies. If a patient is screened high risk –
non invasive prenatal testing (NIPT) is the recommended second line screening that
should be offered to these patients. Anatomical problems in a fetus can be identified
by ultrasound, this combined with maternal serum markers can be used as screening
to identify fetuses at risk of chromosomal abnormalities (1). Cell free
deoxyribonucleic acid (DNA) can be obtained from maternal serum for genetic
screening and one can perform genetic testing on preimplantation embryos but this
is often not feasible or cost effective in a resource restricted setting. It must also be
remembered that cell free DNA analysis is a screening test and not a diagnostic tool
(2).
Prenatal screening has been defined as the identification, among apparently normal
pregnancies, of those at sufficient risk for a specific fetal disorder to justify
subsequent invasive and/or costly prenatal diagnostic tests or procedures (3). The
prevalence of Trisomy 21 in live births is relatively high in the absence of prenatal
screening and is said to be about 1 in 600 live births and Trisomy 18 is 1 in 4000 live
births (4). The widespread implementation of prenatal screening combined with
prenatal diagnosis and termination of pregnancy services has substantially reduced
the expected number of infants born with Down Syndrome (5).
1.1.1 Serum Markers and Ultrasound screening tests
Multiple screening tests are available. The first trimester combined test includes
sonographic nuchal translucency and biochemical markers. The biochemical
markers used are free human chorionic gonadotropin (BHCG) and pregnancy
associated plasma protein-A (PAPP-A). This test is done between 11-14 weeks.
Based on these results, as well as the patient’s age and other variables (for
example body mass index and singleton or multiple pregnancy), the patient can be
given an adjusted risk of whether she is possibly carrying a fetus with a

2
chromosomal abnormality (6). In pregnancies with Trisomy 21 the fetal nuchal
translucency measurement is increased and free BHCG is higher and PAPP-A is
lower than a chromosomally normal fetus (7,8).
During the first trimester ultrasound the measurement of nuchal translucency has
been shown to identify 75% of fetuses affected by Trisomy 21 with a 5% false
positive rate. Another marker of Trisomy 21 in the first trimester ultrasound is the
absence of the nasal bone. When maternal age, nuchal translucency and nasal bone
are combined, the detection rate is 90% with a false positive rate of 2%.
Abnormalities of the ductus venosus flow are observed in up to 80% of fetuses
affected by Trisomy 21. Studies have reported an association between fetal
tachycardia with Trisomy 13 and Turner Syndrome and between fetal bradycardia
with Trisomy 18 and Triploidy. (7,9,10).
In the second trimester, with the patient's age, the triple test measures the level of
the biochemical markers alpha feto-protein, unconjugated estriol and human
chorionic gonadotropin in maternal serum. The quadruple test has the added serum
marker of Inhibin A. These tests are performed between 15-20 weeks (6). The
quadruple test was the most commonly performed test for Down Syndrome
screening in the United States of America in 2012 (8,11).
Ultrasound is a method of screening that can be used in association with other
screening tests to give an associated risk for chromosomal abnormalities as
previously discussed. Both first trimester and second trimester markers can be
associated with chromosomal abnormalities (12).
Soft markers are ultrasound findings that could be a variant of normal but may
indicate an increased risk of fetal aneuploidy (13). These markers in isolation do not
refute or confirm a chromosomal abnormality and most fetuses (> 99%) with an
isolated marker will not be affected (12).
Soft markers associated with chromosomal abnormalities are choroid plexus cysts, a
thickened nuchal fold, an echogenic cardiac focus, echogenic bowel, renal
pyelectasis, shortened humerus, shortened femur, single umbilical artery, mild
ventriculomegaly, enlarged cisterna magna, nasal bone hypoplasia, brachycephaly,
increased iliac angle, shortened ear length, shortened middle phalanx and an absent
subclavian artery (12,13).

3
According to the Van der Hof et al. only five of the above mentioned soft markers
should be used in a screening ultrasound namely an increased nuchal fold,
echogenic bowel, mild ventriculomegaly, echogenic foci in the heart and choroid
plexus cysts. Choroid plexus cysts are mainly associated with Trisomy 18. A single
umbilical artery, an enlarged cisterna magna and pyelectasis do not have a well-
established association with aneuploidy but might be important in the diagnosis of
non chromosomal problems (13).
Each of these markers have an associated likelihood ratio associated with the
occurrence of a certain aneuploidy. Multiple abnormalities seen on ultrasound thus
increase the overall likelihood of an aneuploidy as each associated likelihood ratio is
multiplied by a patient’s background risk and risks found on other screening tests.
Thus multiple markers have a cumulative effect and will increase a patient’s
individual risk (14).
Table 1.1 below shows the likelihood ratio for Trisomy 21 for each isolated soft
marker (7,13)
Table 1.1 Likelihood ratios for Trisomy 21 for each soft marker
Soft Marker LR for isolated marker
Nuchal fold 9 – 17
Nasal bone hypoplasia or absence
51
Short humerus 4 - 7.5
Short femur 1 - 2.7
Ventriculomeglay 9
Hydronephrosis 1.0
Echogenic cardiac focus
1 – 2
Echogenic bowel 3 – 6
4
So called hard markers are structural abnormalities found on ultrasound that
represent major abnormalities and even if found in isolation should warrant invasive
prenatal testing (9).
During the second trimester ultrasound a single abnormality found should prompt the
search for other markers as certain clusters of markers are associated with certain
aneuploidies. As discussed above each soft marker has a certain likelihood ratio of
associated risk to the fetus. If only second trimester markers are used as a screening
test it will have a detection rate of 75% with a false positive rate of up to 15% (9). In
the absence of ultrasound soft markers, the background risk of chromosomal
abnormalities is reduced. (14).
The risk of an aneuploidy increases with structural abnormalities found at ultrasound
and is strongly associated with the number of structural abnormalities found. The
more abnormalities found, the more likely the diagnosis of an aneuploidy at invasive
testing (13).
It must be remembered that ultrasound like any screening test does not give a
definitive diagnosis of a chromosomal abnormality and it must be weighed against a
false positive result causing unnecessary anxiety and clinical intervention, in the
same breath a false negative result might give reassurance to a women carrying a
child with an abnormality (12).
If maternal age only is used as a screening test for chromosomal abnormality there
is a 50% detection rate and a 15% false positive rate. The detection rate increases to
75% if maternal age and nuchal translucency are combined for the same false
positive rate of 5%. A combination of the above with nasal bone further increases the
detection rate to 90% while the false positive rate remains unchanged. In conclusion,
in a resource-limited setting where serum markers might not be available, materal
age specific risk should be combined with early ultrasound markers of aneuploidy for
screening purposes (7).
In the South African setting the maternal age and background risk factors combined
with ultrasound are often the only methods of screening available due to the cost of
serum markers. In a local study conducted by Naidoo et al. at Chris Hani
Baragwanath Academic Hospital nuchal translucency, maternal age and a first
trimester anatomical survey at ultrasound were used as a screening test. They

5
found that the sensitivity was 92,9% and specificity was 88,6% in detecting structural
and chromosomal abnormalities with their screening protocol without biochemical
screening. They concluded that their protocols were equivalent to international
standards (15).
In order to calculate an individual’s risk, their background risk is taken into account
which includes factors like maternal age and gestational age. Sequential screening is
used and can be done by multiplying the background factors by several independent
factors depending on serum and ultrasound findings. Every time a new test is
performed it is multiplied by the background risk to calculate a new risk, which then
becomes the background risk for the next test. (9).
The table below published by Nicolaides et al. illustrates the detection rate of
Trisomy 21 and false positive rate of screening tests (7).

6
Table 1.2: Detection rate of Trisomy 21 and false positive rate of
screening tests
Screening Test Percentage
detection rate
Percentage false
positive rate
MA 50 15
MA + serum BhCG + PAPP-A at
11-14 weeks
60 5
MA + fetal NT at 11-14 weeks 70 2
MA + fetal NT + NB at 11-14
weeks
90 2
MA + fetal NT + serum BhCG +
PAPP-A at 11-14 weeks
80 2
MA + fetal NT + fetal NB + serum
BhCG + PAPP-A at 11-14 weeks
95 5
MA + serum biochemistry at 15-18
weeks
60-70 5
Ultrasound for fetal defects and
markers at 16-23 weeks
75 10-15
1.1.2 Non invasive prenatal testing (NIPT)
The testing of cell free DNA, in maternal blood is another method of screening
known as non invasive prenatal testing (NIPT) . The method screens mainly for the
most common Trisomies and Sex Chromosome abnormalities (2). Other uses
include fetal sexing and fetal Rh typing (16). It is used as a primary or secondary
screening tool. These tests have a 99% sensitivity and a 99% specificity when
screening for both Trisomy 18 and 21. Trisomy 13 and Sex Chromosome
abnormalities have a sensitivity of between 80-90% and a specificity of 99% (2).

7
The American Colleges of Medical Genetics and Obstetricians and Gynaecologists
guidelines state that NIPT should be done in the following patients as an effective
screen for Down Syndrome: (17)
Patients 35 years and older
A mother with a fetus affected previously with Trisomy 13, 18 or 21
A parental translocation involving chromosome 13 or 21
Fetal ultrasound or other screening test that specifically increases the
risk for Down Syndrome
Norton et al. provided support for offering this test to all woman as a form of
screening. Over 15 000 woman presenting at 10 -14 weeks of gestation at 35
international centres underwent both standard screening (with measurement of
nuchal translucency and biochemical markers) and cell free DNA testing regardless
of their baseline risk of aneuploidy. For Trisomy 21, NIPT had a 100% sensitivity
and had a positive predictive value of 80,9% while standard first trimester screening
had sensitivity of 78,9% and a positive predictive value of 3,4%.Cell free DNA
screening had a higher sensitivity for detection of Down Syndrome, a lower false
positive rate and a higher positive predictive value (18). However the ACOG
recommends given the performance of conventional screening methods, the
limitations of cell free DNA screening performance, and the limited data on cost
effectiveness in the low-risk population, conventional screening methods remain the
most appropriate choice for first line screening for most women in the general
population (2).
NIPT testing is available in South Africa but the genomic and bioinformatics
information of samples needs to be done in other countries. This option is not
available in the public sector in South Africa mainly due to the large cost associated
with it, and is only available in the private sector for those who can afford the out of
pocket payment or are members of certain medical aids (19).
If the patient has a screen positive test she can either undergo secondary screening
or might want a definitive diagnostic test. It can be seen that an individualised risk
assessment must be done for every patient including background risk and screening
results before an invasive test is offered (14). A population can be divided into high
risk (1:100 or lower), intermediate risk (1:101-1:2500) and low risk (<1:2500), NIPT

8
should be offered to patients in the intermediate risk category. Some studies suggest
that NIPT should be offered in a patient with a risk of 1:101-1:2500 (20,21)
The Society of Obstetricians and Gynaecologists of Canada (SOGC) recommends
that no definitive obstetric decision should be made in pregnancies with a positive
non-invasive prenatal testing result without an invasive diagnostic test to confirm the
diagnosis (22). It is estimated that around 5% of the pregnancy population in the
United Kingdom are offered a choice of invasive prenatal diagnostic tests (23).
1.1.3 Invasive Prenatal Testing
1.1.3.1 Introduction
Invasive prenatal testing is a definitive form of diagnosis used during pregnancy to
detect among other things chromosomal abnormalities. There are three forms of
invasive prenatal testing namely amniocentesis, CVS and cordocentesis.
Prenatal detection of chromosome abnormalities has been offered for more than 40
years, first by amniocentesis in the early 1970s and additionally by CVS in the 1980s
(6). Prenatal testing decreases the burden of disease to the affected individual and
their family and gives new parents time to prepare for the birth of their infant. The
American College of Obstetricians and Gynaecologists recommend that all women
should be offered aneuploidy screening before 20 weeks of gestation and all women
should have the option of invasive testing, regardless of maternal age (24).
Diagnostic testing requires the harvesting of fetal cells derived from skin, mucous
membranes, amnion, placenta or umbilical cord during pregnancy for subsequent
karyotype and genetic analysis (25). The diagnostic accuracy of karyotyping cultured
cells obtained by invasive testing has been found to be 97,5 to 99,8% (6).
Invasive prenatal testing remains the gold standard for conclusive prenatal genetic
diagnosis.

9
1.1.3.2 Amniocentesis
Amniocentesis was first used for fetal karyotyping in 1966 (26).Today it is widely
accepted as the method most easily performed among the prenatal invasive
diagnostic methods, especially when carried out in the second trimester (27).
Amniocentesis is used as prenatal diagnostic procedure to obtain amniotic fluid for
prenatal diagnosis. It is usually performed after 15 weeks gestation but can be
performed in the first trimester (16,23,25).
Amniocentesis should be done under ultrasound guidance in order for the position of
the placenta to be visualised and a suitable entry point to the mother’s abdomen is
found (23). Continuous visualisation of the needle with ultrasound guidance reduces
bloodstaining from 2.4% to 0.8% (28), it also reduces serious fetal trauma or
maternal bowel injury that can be caused by the needle (23).
Transplacental passage of the needle should be avoided unless this is the only way
to access an adequate pool of liquor. If this approach is used the insertion of the
cord must be avoided and the thinnest part of the placenta must be traversed (23).
A prospective case control study done by Mungen et al. of 2068 women undergoing
second trimester amniocentesis and their 2068 controls showed that there was no
significant difference between the transplacental and non-transplacental approach
(29).
Amniocentesis should be performed using a sterile technique, an amniocentesis
needle and ultrasound guidance. A sterile technique is achieved by the use of
abdominal antiseptic cleaning, sterile gloves, sterile drapes, sterile ultrasound gel
and a sterile ultrasound cover (16). Generally a sample of 20-30 mls of amniotic fluid
is obtained from a liquor pocket that is free of fetal parts and umbilical cord (24). The
fluid obtained for testing is usually from fetal skin and bladder cells and is processed
for chromosome, protein, biochemical and enzymatic analysis of the amniotic fluid
supernatant (16). Amniocentesis has been shown to have a cytogenetic accuracy of
more than 99% (24).
SOGC recommends decreased physical activity for 12-24 hours after the procedure
but bed rest is not required. The use of prophylactic antibiotics is not required (16).

10
1.1.3.3 Chorionic villous sampling
The Royal College of Obstetricians and Gynaecologists (RCOG) recommend that
CVS is performed between 11 weeks and 13 weeks and six days. It is a
transabdominal or transcervical technique where placental villae are aspirated or
biopsied (23).
It is recommended that both transabdominal and transcervical CVS be performed
under continuous ultrasound guidance. The tip of a needle or specialised catheter is
placed in the placenta without entering the amniotic sac. Negative pressure with a
syringe is used to aspirate a small amount of placental villi (24). RCOG recommends
that the technique used, whether aspiration by negative pressure syringe, negative
pressure by vacuum aspirator or biopsy forceps, should be under the guidance of an
experienced obstetrician (23).
The advantage that CVS has over amniocentesis is that the diagnosis can be given
earlier in pregnancy and the expecting couple can make definitive treatment
decisions earlier in pregnancy.
The success rate of cytogenetic diagnosis on CVS samples is reported to be 99.7%
with 1.1% of patients requiring a further diagnostic test to interpret results (30).
1.1.3.4 Cordocentesis
Cordocentesis is a procedure done at later gestations and is generally done between
16 and 24 weeks and is used for both fetal diagnosis and therapy (31).
A 20-22 gauge needle is directed under continuous ultrasound guidance into the
umbilical vein. Puncture of the umbilical artery might cause constriction and can lead
to fetal cardiac abnormalities. The needle can be directed to various sites like the
umbilical cord insertion site, fetal intrahepatic vein or a free loop of cord (16).
Cordocentesis is rarely performed with the availability of other invasive procedures
like amniocentesis and CVS but can be very useful in a case of chromosomal
mosaiscm found at amniocentesis or CVS (24).

11
1.1.4 Indications for invasive prenatal testing
Invasive prenatal testing is usually offered to a population in which a there is a
predetermined risk of chromosomal abnormality as previously mentioned. The most
frequent indication for invasive prenatal testing is:
advanced maternal age
diagnosis of diseases associated with DNA analysis
enzyme analysis of metabolic disease
determination of congenital infection
abnormalities detected on ultrasound
increased first and second trimester screening risk
family history of chromosomal abnormalities
patient request (32)
The ACOG recommend that diagnostic prenatal testing be offered to all pregnant
women but especially patients with a previous pregnancy complicated by fetal
Trisomy, at least one major or two minor fetal structural abnormalities on ultrasound
in the current pregnancy, a chromosomal inversion, aneuploidy or translocation in
the pregnant woman or her partner (24).
Chang et al. did a retrospective review of 30 years at the Tapei General Hospital,
Taiwan looking at the indications and outcomes of amniocentesis. 16749 women
were included between 1981 and 2010 who had undergone midtrimester
amniocentesis. The main indications for amniocentesis were advanced maternal
age, increasing risk maternal triple marker Trisomy 21 screening, history of previous
birth of a baby with an abnormality, abnormal ultrasound findings, family history of
chromosomal abnormality, abnormal parental karyotype, drug and radiation
exposure, abnormal CVS and intrauterine fetal death. The most common indication
was advanced maternal age that accounted for 65.5% (33).

12
Daniilides et al. found in a retrospective study in Greece over a four year period that
the main indications for amniocentesis were an increased risk for Down Syndrome,
maternal request, abnormal ultrasound findings and family history of chromosomal
abnormality (25).
A study conducted in Korea by Cho et al. which included 2000 women, showed that
the indications for amniocentesis were advanced maternal age, abnormal serum
markers and abnormal ultrasound findings. The most common indication was
advanced maternal age (34).
Kim et al. conducted a similar study in Korea which included 2942 patients and
concluded that in this setting the most common indication for invasive testing was
abnormal maternal serum markers (35). Pala et al. in a study conducted in Turkey in
2012 looked at 83 cases of amniocentesis performed also found the most common
indication for was increased in serum markers. This study also found a 10% rate of
maternal request for amniocentesis, maternal request is either a very small
percentage in other studies or not mentioned at all (36).
1.1.4.1 Advanced maternal age
Advanced maternal age is commonly defined as an age of 35 years or older (37).
Delayed child bearing is an increasing trend in developing countries and this has led
to an increased burden of prenatal testing (38). This trend has been attributed to
contraception being available, advances in infertility medicine, delaying marriage,
high rates of divorce and remarriage and women finding education and careers
important (39).
Women of advanced maternal age are at increased risk of delivering an infant with a
chromosomal or congenital abnormalities (39,40). Most chromosomal abnormalities
originate from abnormalities in female meiosis (aberrations in meiotic spindle
assembly in oocytes) (41,42). Sex chromosome abnormalities don’t have an
association with advanced maternal age (7). In a study done by Hook et al. which
looked at chromosomal abnormality rates in women with only advanced maternal
age as a risk factor it was found that the rate was 5/1000 at age 35 years, 15/1000 at
age 40 years and 50/1000 at age 45 years (43).

13
From 1970 to 2000, live births among women aged 35 and older in the United States
increased from 5% to 13% of live births (44). In South Africa 13, 4% of pregnant
women fall into the advanced maternal age category which accounts for the high
prevalence of Down Syndrome, documented to be 1,8 and 2,09 per 100 live births in
urban and rural populations respectively (45,46).
Most of the studies mentioned above showed that advanced maternal age was the
most common indication for invasive prenatal testing. Advanced maternal age was
the main screening tool for invasive testing before the advent of serum and
ultrasound screening tests. In a resource restricted setting maternal serum screening
is often not possible and ultrasound screening might be limited thus advanced
maternal age is still a mainstay of screening in a resource restricted setting like the
South African public health service.
Antenatal care aims to provide the identification of avoidable factors to provide a
normal pregnancy and delivery of a healthy infant with the least possible morbidity.
Advanced maternal age is an easily recognisable risk factor that can be used in
antenatal care to provide prenatal genetic counselling for invasive prenatal testing. In
Johannesburg invasive prenatal testing has been free since 1994 and there is an
open referral system to academic hospitals who provide the service (40).
In a local study by Kromberg et al. 55% of mothers of infants affected with Trisomy
21 were over the age of 35 but none of these women were offered prenatal testing.
Kromberg et al. also found in their study that 73% of these women would have
accepted prenatal diagnosis if it had been offered to them and 52% said that they
would have considered termination of pregnancy (47). In other local studies Delport
et al. found 52% of mothers of Trisomy 21 infants were over the age of 35 (48), while
Venter et al. found 56% in theirs (49). Another showed that in the local population
the overall acceptance rate of amniocentesis was 75.9% and of termination of
pregnancy was 76,3% (50). These studies show that offering invasive prenatal
testing will increase the rate of Trisomy 21 detection and give the patient options for
further management. They further show that prenatal testing is acceptable to most
patients.

14
1.1.4.2 Chromosomal abnormalities
Chromosomal abnormalities are major causes of perinatal death and childhood
morbidity thus the detection of chromosomal abnormalities is a common indication of
invasive prenatal testing (7).
The prevalence of chromosomal abnormalities if recognised in early pregnancy loss
is greater than 50%. Fetuses with aneuploidy account for 6-11% of stillbirths and
early neonatal deaths (24). Major fetal abnormalities occur in approximately 5% of all
live births , 3% are identifiable prenatally and 2% at birth or during the first year of life
(16).
In a developing country like South Africa issues of infectious disease and
malnutrition are being brought under control and it can be expected that congenital
abnormalities will assume a greater relative proportion of childhood causes of
morbidity and mortality (48). According to under five mortality statistics in South
Africa 3% of infant deaths between 0-11 months are because of congenital
abnormalities (51). Data from the Perinatal Problem Identification Program (PIPP) in
2014 showed that congenital abnormalities is the third leading cause of early
neonatal death after hypoxia and immaturity. With immaturity accounting for 40,6%
of deaths, hypoxia 10% of deaths and congenital abnormalities 9,6% of deaths
(52,53).
In a local study done by Delport et al. 17351 black infants were examined at birth in
an urban hospital and the total congenital anomalies incidence were found to be
11,87/1000. This study also showed that Down Syndrome was the most common
chromosomal abnormality diagnosed with an incidence of 1,33 per 1 000 Iive births
or 1 in 752 babies delivered . The study concluded that the incidence of congenital
anomalies in black South African neonates were comparable to that of First and
Third world countries (48). Similarly, another local study by Venter et al. which took
place in a rural community and included 7617 infants reported an incidence of
congenital abnormalities of 14,97/1000 (49).
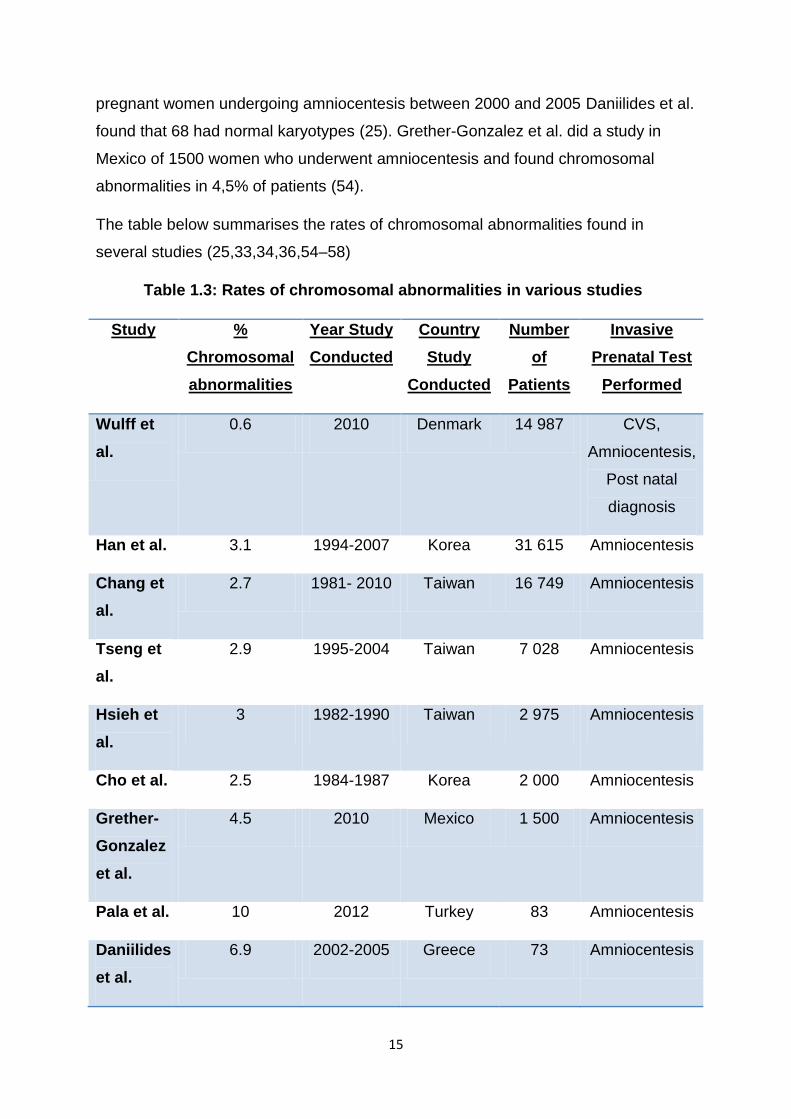
Several international studies found the following rate of chromosomal abnormalities.
Chang et al. found the overall rate of abnormalities to be 2,72% (455/16 749
patients) and among these abnormalities 274 were chromosomal abnormalities and
181 were structural abnormalities (33). In the 73 cases in a study in Greece of
15
pregnant women undergoing amniocentesis between 2000 and 2005 Daniilides et al.
found that 68 had normal karyotypes (25). Grether-Gonzalez et al. did a study in
Mexico of 1500 women who underwent amniocentesis and found chromosomal
abnormalities in 4,5% of patients (54).
The table below summarises the rates of chromosomal abnormalities found in
several studies (25,33,34,36,54–58)
Table 1.3: Rates of chromosomal abnormalities in various studies
Study %
Chromosomal
abnormalities
Year Study
Conducted
Country
Study
Conducted
Number
of
Patients
Invasive
Prenatal Test
Performed
Wulff et
al.
0.6 2010 Denmark 14 987 CVS,
Amniocentesis,
Post natal
diagnosis
Han et al. 3.1 1994-2007 Korea 31 615 Amniocentesis
Chang et
al.
2.7 1981- 2010 Taiwan 16 749 Amniocentesis
Tseng et
al.
2.9 1995-2004 Taiwan 7 028 Amniocentesis
Hsieh et
al.
3 1982-1990 Taiwan 2 975 Amniocentesis
Cho et al. 2.5 1984-1987 Korea 2 000 Amniocentesis
Grether-
Gonzalez
et al.
4.5 2010 Mexico 1 500 Amniocentesis
Pala et al. 10 2012 Turkey 83 Amniocentesis
Daniilides
et al.
6.9 2002-2005 Greece 73 Amniocentesis

16
It can be seen from the above table and discussion that the rate of chromosomal
abnormalities found in various studies range between two and ten percent.
Daniilides et al. found the majority of chromosomal abnormalities identified to be
Trisomy for chromosomes 13, 18, 21 and Sex Chromosome aneuploidies (25).
These abnormalities were also found to be the most common in an analysis by
Grether-Conzalez et al. of 1500 women who underwent amniocentesis (54). In all the
studies above, Trisomy 21 was the most common chromosomal abnormality found
by invasive testing.
1.1.4.3 Other indications for invasive prenatal testing
Advanced paternal age has been associated with an increased risk of single gene
disorders and this pertains mainly due to mutations that occur during
spermatogenesis (59). Although there is no consensus advanced paternal age is
considered to be from 40-50 years of age and older (24).
Other risk factors for a positive invasive prenatal test result include: A couple
carrying a chromosomal rearrangement. Carriers of balanced chromosome
rearrangements can produce gametes with unbalanced chromosomes that result in a
genetic abnormality in their children (60). Parental aneuploidy or aneuploidy
mosaicism (61). In parents who are carriers of genetic disorders their offspring might
be affected. In an autosomal dominant disorder the offspring has a 50% risk of
having the disorder.
A couple who has had child with a structural birth defect has a 2-3% risk of the next
child being affected but this varies in terms of the abnormality and sex of the affected
child (24).
A previous child with an autosomal Trisomy or sex chromosome aneuploidy gives a
higher risk of occurrence in the current pregnancy. This depends on the type of
Trisomy, age of the patient in the current pregnancy and the age of the mother in the
previous pregnancy and whether the previous abnormal pregnancy ended in
spontaneous miscarriage (62,63). In a study of 2054 women who had a previous
pregnancy with Down Syndrome it was found that the risk of recurrence in the
subsequent pregnancy was 0.75% higher than the maternal and gestational age-

17
related risk. The risk of Trisomy 18 was also found to be 0.75% but it was found that
the risk in these women were not increased for Down Syndrome and it was
concluded that the risk of recurrence is specific to the chromosomal abnormality (7).
Knowledge of the indications of prenatal invasive testing is of paramount importance
in prenatal counselling of the pregnant patient. Cho et al. found that maternal age,
maternal serum markers and information on ultrasound should be included in
prenatal counselling (34).
1.1.5 Laboratory technique in invasive prenatal testing
The type of test that the laboratory performs on a invasive test specimen is guided
by the gestational age at which the test is performed and the indication for the test.
Karyotyping is done for chromosomal disorders and DNA analysis for genetic
disorders where a specific mutation is suspected. (24).
Karyotyping is the traditional test performed for the identification of aneupoloidies
which include Trisomies and Sex Chromosome abnormalities. Karyotyping can also
detect large rearrangements. Mosaicism in the fetus may not be detected by
karyotype analysis if the specific fetal line of cells tested does not contain the
mosaicism (24). Karyotyping has a diagnostic accuracy of more than 99% for
aneuploidy and chromosomal aberrations of larger than 5-10 megabases(64).
Quantitative fluorescent polymerase chain reaction (QF-PCR) is a method that can
be beneficial in a resource restricted setting as it takes away the need for fetal cell
culture thus making it very cost effective. It is also characterised by a rapid turnover
time and is fully automated. Specific DNA sequences are amplified by fluorescent
primers. These DNA segments are then quantified as peak areas on DNA scanners.
It has a very high detection rate of up to 98,6% for certain chromosomal
abnormalities like Trisomy 21, 18, 13 and Sex Chromosome abnormalities X & Y.
This method has the disadvantage that some abnormalities might be missed as the
primers only test for the five chromosomal aberrations mentioned above (65).
If the aim of the test is to find smaller microdeletions and duplications fluorescent in
situ hybridisation (FISH) can be considered as this method uses detection via
chromosomal microarray. Fluorescent -labelled probes for a specific region of the

18
chromosome are used and find the number of those chromosome regions that are in
the specimen. Many panels are available on special request but the one most
commonly used is a panel including chromosome 13, 18, 21, X and Y. This method
remains a screening test and a positive result must only be acted upon in the
following cases: when there is a confirmatory karyotype or chromosomal microarray,
clinical findings that support the FISH result or another positive screening test (66).
Chromosomal microarray analysis is a method that can detect both major aneuploidy
and submicroscopic changes that cannot be detected by karyotyping (24). It is
recommended that a patient who has structural abnormalities on ultrasound should
be offered this test. In fetuses with a normal karyotype it has been shown to detect
chromosomal abnormalities in 6% and 1,7% in patients with normal karyotypes and
normal ultrasound examinations (67,68). ACOG recommends that this method be
offered to any women undergoing prenatal invasive testing (24).
1.1.6 Complications of invasive prenatal testing
An invasive diagnostic test will give a definitive diagnosis regarding the presence of
certain fetal abnormalities; however the risk of the test must be weighed against the
need for a diagnosis.
1.1.6.1 Risk of fetal loss
Miscarriage is the most widely quoted complication of invasive prenatal testing. In a
landmark randomised control trial by Tabor et al. 4606 women at low risk of
miscarriage aged 24-35 were randomised to have (or not to have) an amniocentesis.
Most procedures were performed between 16 and 18 weeks of gestation. The
amniocentesis group had a loss rate which exceeded the control group by 1%. This
study also concluded that raised levels of alpha feto protein, tranplacental passage
and retrieving discoloured amniotic fluid were associated with increased risk of
spontaneous miscarriage (27). In a review done by Tabor et al. it was found that
procedure related miscarriage rate for midtrimester amniocentesis was 0,5-1% (14).
The Danish Fetal Medicine Study Group did a large study, with a cohort of 147 987
women, aiming to assess the risk of fetal loss with invasive testing following

19
combined first trimester screening for Trisomy 21. Risk was assessed by propensity
score stratification. Risk of fetal loss following CVS over time points between three
and 21 days after combined first trimester screening showed a range of 0.08-0.41%
for miscarriage and for stillbirth a risk of 0.18-0.58%. Risk of fetal loss following
amniocentesis was taken over time points of 28-42 days after combined first
trimester screening. This showed a risk of fetal loss by miscarriage of between 0.42-
0.56% and risk of stillbirth of 0.09-0.26%. The study thus found that the risk of fetal
loss by miscarriage or stillbirth was not increased significantly in women undergoing
CVS or amniocentesis compared to women not undergoing a invasive prenatal test.
They thus concluded that the procedure related risk of invasive prenatal testing was
very low.(58)
It has been shown that operators who perform procedures frequently have lower
miscarriage rates (69), consequently single centre studies might have lower
miscarriage rates because of very skilled operators but it must be emphasized that
these rates cannot be used for counselling in general (14).
Early amniocentesis has higher rates of complications than that of late
amniocentesis. It has been found that the pregnancy loss rate is significantly higher
than that of midtrimeter amniocentesis. In a multicentre randomized trial, the
spontaneous loss rate after early amniocentesis was 2.5% compared with 0.7% for
midtrimester amniocentesis, significantly higher rates of amniotic fluid culture failures
and talipes equinovarus were also found (70).
Meta analyses of all randomised control trials comparing CVS and second-trimester
amniocentesis showed excess pregnancy loss following CVS (23). However a
randomised control trial by Smidt-Jensen et al. showed similar pregnancy loss
between transabdominal CVS and amniocentesis (71). A Cochrane review of
amniocentesis and CVS concluded that the total pregnancy loss of transabdominal
CVS is comparable to that of midtrimester amniocentesis, while transcervical CVS
has a much higher rate of miscarriage than midtrimester amniocentesis (1). Some
studies find the overall loss rate after CVS is greater than the rate after midtrimester
amniocentesis. This can be explained by the increased background rate of
spontaneous pregnancy loss between nine and sixteen weeks of gestation. Thus it

20
can be concluded that the procedure related loss rate is similar to that of
midtrimester amniocentesis (24).
In a Cochrane review Alfirevic et al. concluded that second trimester amniocentesis
is safer than early amniocentesis or trancervical CVS, and this is the procedure of
choice for second trimester testing. If a diagnosis is needed earlier, transabdominal
CVS is regarded as the procedure of choice over transcervical CVS and early
amniocentesis (1).
Cordocentesis is associated with a pregnancy loss rate of 1,3% in fetuses with no
fetal abnormalities and 1.3% to 25% in fetuses with single or multiple abnormalities
or intrauterine growth restriction (16).Total miscarriage rate in fetuses with IUGR is
up to 14% and in fetuses with hydrops fetalis up to 25% (72). Wilson et al. in a four
year retrospective review showed that the procedural loss rate of cordocentesis was
higher in fetuses where an abnormality was diagnosed (73).
1.1.6.2 Other complications of amniocentesis
Amniocentesis is also associated with talipes equinovares, which is increased if early
amniocentesis is done, and is mainly secondary to temporary or intermittent
oligohydramnios (74). A Swedish national study which included 21748 women who
had an amniocentesis and 47854 controls, showed an increased risk of
musculoskeletal deformities when amniocentesis was done before 14 weeks of
gestation (75).
Other minor complications caused by amniocentesis might include transient vaginal
spotting and amniotic fluid leakage. Amniotic fluid leakage occurs in 1-2% of cases
(70). The rate of amniotic fluid leakage increases the earlier the amniocentesis is
performed (14). Bombard et al. suggests that there was less amniotic fluid flow from
the puncture site with smaller gauge needles (76).The perinatal survival rate in cases
of amniotic fluid leakage after midtrimester amniocentesis is greater than 90% (77).
Culture failure occurs in 0.1% of samples (24). There may be an association with
amniotic band syndrome and amniocentesis (78).
Midtrimester amniocentesis has been associated with neonatal respiratory distress
syndrome and neonatal pneumonia. An animal study where primates underwent

21
midtrimester amniocentesis had structural changes in their lungs which were not
found in controls (79).
1.1.6.3 Other complications of chorionic villous sampling
CVS associated vaginal spotting can occur in up to 32% of patients and this is less in
transabominal versus transvaginal CVS (80). ACOG postulates that the incidence of
infection, culture failure or amniotic fluid leakage after CVS is less than 0,5% (24).
Chorionic villous sampling before ten weeks gestation has previously been shown to
have an association with oromandibular limb hypoplasia and isolated limb disruption
defects. This association was first reported in 1991 when a cluster of five babies with
limb reduction defects was reported among a series of 289 women undergoing
transabdominal CVS between eight and nine weeks (81). In an analysis by the World
Health Organisation, an incidence of limb reduction defects after CVS was found to
be 6/10000 which is not significantly greater than the incidence in the general
population. After ten weeks there was no increased risk of limb reduction defects,
while there might be an association with a CVS being performed before ten weeks of
gestation (76,82). The RCOG recommend that CVS is not performed before ten
weeks of gestation (23).
Although more studies are needed there has been an association between CVS and
the development of preeclampsia which might be explained by the procedure
causing placental disruption and consequently placental dysfunction (83).
Chromosomal mosaicsm is the presence of more than one cell line during
cytogenetic analysis, it occurs in 0.25% of amniocentesis samples and 1% of
chorionic villous samples. Confined placental mosaism is a condition where
mosaicism is only present in the placenta, it is found in 1-2% of placentas. This
condition can be found in fetuses which have a normal amount of chromosomes but
may have a genetic abnormality such as uniparental disomy, this might impact the
CVS result (16). Another case of mosaicism is maternal cell contamination of the
fetal specimen. This can be minimised by discarding the first 1-2ml of fluid obtained
at amniocentesis and by careful dissection of chorionic villi from maternal decidua
(24). It must be mentioned at this point that there is an association with confined

22
placenta mosacism and a false positive results in non invasive prenatal testing
(NIPT). This is due to the fact that cell free DNA is mainly derived from the placental
trophoblast. As there is a known risk of false positive results with NIPT, each positive
NIPT result should be confirmed with an invasive prenatal test before definitive
management is instituted (84,85).
1.1.6.4 Other complications of cordocentesis
Cordocentesis might be associated with continual bleeding from the cord with
significant anaemia and hypotension in the fetus. Fetal bradycardia is another
complication that might occur in 5-10% of fetuses. (16)
1.1.6.5 Infective complications including HIV transmission
Severe sepsis including maternal death has been reported following invasive
prenatal techniques. The risk is likely to be less than 1/1000. RCOG recommends
the use of strict sterile techniques, as discussed previously, in all invasive prenatal
tests (23).
Blood borne virus transmission from mother to fetus poses a potential risk during
invasive testing. Davies et al. concluded that the risk of transmission of Hepatitis B is
very low (86). Vertical transmission rate is not increased in women who have low
viral load, whereas women with high viral loads might have a 21 fold increased rate
of transmission and newborn infection (87).
There is no evidence that Hepatitis C is transmitted (88). In a study of 22 pregnant
women who were hepatitis C positive and who underwent second trimester
amniocentesis, only one woman had hepatitis C virus detected in the amniotic fluid
and none of the infants born had the virus (88).
It is thought that transmission of HIV is not a risk provided that the viral load of the
mother is low and that antiretroviral therapy has been instituted (23). Somigliana et
al. demonstrated no difference in transmission rates between HIV positive women
undergoing amniocentesis and those who did not and this was also shown by
Mandelbort et al. (89,90). One study did show that transmission rate is high if there

23
was no treatment in place or mono or double therapy was being used (91). Data
from the French Perinatal Cohort study included 81 HIV infected patients who had
amniocentesis and were on combination antiretroviral therapy. There was no
difference in the rate of vertical transmission in this group compared with controls
who did not have an amniocentesis (90). A study done by Floridia et al. also
concluded that HIV transmission is not increased if a patient is virally suppressed
and undergoes invasive prenatal testing (92). The RCOG recommends that the viral
load be undetectable before an invasive test is done (93).
South Africa has a large burden of HIV and more than 50% of the people living with
HIV in South Africa are women and many of these are of child bearing age. The
South African Department of Health showed in 2013 that 29,7% of pregnant women
were infected with HIV (94,95). Clinical practice guidelines published in the South
African Medical Journal in 2014 state that if a HIV positive woman requires an
amniocentesis antiretroviral therapy should be initiated and that the procedure
should be delayed until the viral load is suppressed (94). In 2012 Mnyani et al
recommended a patient should be on antiretroviral therapy for four to six weeks to
become adequately virally suppressed (96). The decision should be guided by the
nature of the chromosomal abnormality suspected. If the abnormality is thought to be
severe and might cause great morbidity, exposing the fetus to a small risk of HIV
transmission will be outweighed by the benefit of a prenatal diagnosis (94).
It is further stated that third trimester amniocentesis, CVS and cordocentesis are not
recommended in HIV positive woman. Mnyani et al. states that due to the increased
technical difficulty CVS and cordocentesis procedures might have a significantly
increased risk of transmission to the fetus even if the patient is on antiretroviral
therapy (96). It is also advised that transplacental amiocentesis is avoided (97).
There must be a clear indication for the use of an invasive prenatal test in a HIV
positive woman and the use of screening tests are recommended (94,96). This is
supported by Naidoo et al. in a local study that concluded that in a country with a
very high rate of HIV that a first trimester screening programme was needed as it
would lead to less invasive tests being needed (15).
It is advisable that a viral load is obtained in the woman before an invasive test is
done and that this should form part of the counselling procedure. It is also good

24
practise to repeat an HIV test before an invasive prenatal procedure if the patient
initially tested HIV- negative (96).
It is of upmost importance that a patient should be counselled on the risk of mother
to child transmission of HIV as part of the informed consent process for the invasive
prenatal testing (96).
1.1.7 Counselling for prenatal testing
Counselling of a patient and her family, whether she is undergoing a screening test
or an invasive prenatal test, is probably the most important aspect of the procedure.
A thorough knowledge of the procedure is needed by the clinician in order to do this
and the approach of a multidisciplinary team including the use of genetic counsellors,
clinical geneticists and support groups must be remembered.
Firstly the patient must understand that all screening and invasive testing is
completely voluntary (98). ACOG recommends that prenatal genetic testing be
discussed as early as the first antenatal visit and that a risk of aneuploidy be made
as early as possible (24).
The RCOG recommend that the following should be included when written consent
for an invasive prenatal test is obtained: (23)
The indication for the procedure
The type of cytogenetic result that might be obtained
Risks nationally and locally pertaining to pregnancy loss
Limitations of the laboratory tests that are available
How the results will be communicated to the patient
Possible outcomes of a test and available treatments and follow up for
a positive result
Genetic prenatal counselling can often be difficult to the patient and the clinician. It
must be remembered that non directive counselling should be given to the patient
and her partner. Autonomy, one of the principles of medical ethics, dictates that the
physician respects the patient’s preferences towards her care (10).

25
Genetic counselling starts with a good patient history which must include a family
pedigree and previous obstetric and genetic history. In certain circumstances
parental karyotyping might be needed especially if a family history of genetic
translocation risks is elicited. The patient should be counselled in a language she
understands and at her level of literacy (16).
If a chromosomal abnormality is diagnosed the patient should be provided with
information of the natural history of the disease and the decision of termination of
pregnancy should also discussed. It must be remembered that invasive prenatal
testing is not only done in order to aid a patient with the decision to terminate her
pregnancy but may provide details to the patient and her medical team to plan the
rest of her pregnancy, delivery and care in the neonatal period (24). According to the
SOGC it is a common misconception that invasive testing is only offered to patient’s
who will undergo termination of pregnancy (98). It is pivotal that patient’s understand
although a decision of termination of pregnancy will be supported, if a decision is
made to continue with the pregnancy the best possible care will be given. This care
must include a discussion of intrapartum care, fetal monitoring, mode of delivery and
care of the fetus at birth. It is often of value to include a neonatologist in this
discussion (99).
Another important aspect to discuss in a positive test is the small possibility of a false
positive result and the converse is also true in that a negative test might not mean
that all abnormalities have been ruled out (98).
It is important to give a couple time to discuss the findings with their family and
schedule follow up appointments with ample time for question asking.
1.2 PURPOSE OF STUDY
Invasive prenatal diagnosis is the gold standard of prenatal diagnosis of
chromosomal abnormalities in the modern era of medicine. Although non-invasive
screening tests should always be considered it is often not available in a resource
restricted setting such as the public sector in South Africa. In the South African
public sector biochemical screening and NIPT is not available, methods of screening
mainly rely on advanced maternal age and antenatal ultrasound. Although outcome

26
of invasive prenatal procedures have been studied previously, it has not been looked
at in a resource poor, tertiary setting in South Africa.
The aim of this study is to review the outcome of invasive prenatal testing at Rahima
Moosa Mother and Child Hospital over a two year period and will include a review of
patient selection, complications and diagnosis. It is important to conduct a review of
a service provided by a centre and compare this to international standards as these
findings can be used in counselling patients on the possible complications and
outcomes of such a procedure.
1.3 SETTING
The study took place at Rahima Moosa Mother and Child Hospital, a tertiary hospital
in Johannesburg which performs approximately 12 000 deliveries per annum. The
hospital has a dedicated ultrasound department, genetics clinic and antenatal clinic.
Invasive prenatal diagnostic testing is available. The patients are referred from
consultants, registrars and sonographers to the specialists providing the service for
consideration of further testing. Outside referrals from private doctors are also seen.
The dedicated ultrasound department does approximately 13 000 ultrasounds per
annum. It should be noted that this includes ultrasounds for paediatric and
gynaecological pathology. The team consists of one fetal medicine specialist, one
fellow in fetal medicine, two consultants in obstetrics and gynaecology with a special
interest in fetal medicine and three full time sonographers. There are four ultrasound
machines available in rooms that are equipped for invasive procedures.
Three types of ultrasounds are done in the department. The first being a dating scan
that is mainly opportunistic and can also be done by registrars in the obstetrics and
gynaecology department at the time of a patient presenting for antenatal care. This
scan may then be done at any gestation. The second is a nuchal translucency scan
that is done between 11 and 13 weeks six days gestation. The third is a fetal
anomaly scan that is done between 18 and 23 weeks gestation.
If a patient is booked or referred early enough she may be referred for a nuchal
translucency scan and afterwards will be booked for a fetal anomaly scan. If any
abnormalities are detected in any ultrasound the patient is referred to one of the

27
clinicians in the department and further follow up is organised as needed after the
patient is seen by the clinicians. All invasive prenatal testing is performed by the
aforementioned specialists.
The department is also supported by dedicated genetic counselling clinic which is
available by appointment.
1.4 OBJECTIVES OF THE STUDY
The main aim of the study is to evaluate prenatal invasive testing, including
amniocentesis, CVS and cordocentesis over the period from January 2014 to May
2016 in terms of
1. Describing ultrasound markers that lead to a prenatal test being
offered to a patient
2. Cytogenetic diagnosis made
3. Complications and complication rates related to the procedure
4. Pregnancy outcome and final diagnosis where possible

28
2 MATERIALS AND METHODS
2.1 STUDY SAMPLE
2.1.1 Study population
The study included all patients who had had an invasive prenatal diagnostic tests,
including amniocentesis, CVS and cordocentesis at Rahima Moosa Mother and
Child Hospital .
2.1.2 Timing
The testing was carried out over the period January 2014 to May 2016. The patients
had to have completed their pregnancy by the end of July 2016. There were 97
patients who had a test in this time period. One of these 97 patients was excluded as
her invasive test result was not found on the laboratory data base.
A retrospective chart review was done on all the patients’ files who underwent the
above mentioned testing. The list of patients on whom an invasive prenatal test was
performed was obtained from a data base kept within the ultrasound department. It
was expected that some files would not be available in the hospital's record
department as a certain number of patients would have continued their antenatal
care in other facilities, provinces or countries and would have taken their maternal
chart with them.
2.2 METHODS
Patients who underwent invasive prenatal testing including amniocentesis, CVS and
cordocentesis, were identified using the data base that exists in the ultrasound
department of Rahima Moosa Mother and Child Hospital. The patient name, hospital
number, indication for invasive test, type of invasive test and gestation at which the
test was performed of all patients undergoing prenatal invasive testing are recorded
and kept in book form in the ultrasound department.
Charts of the patients identified from the above mentioned data base were obtained
from the Rahima Moosa Mother and Child records department and information was

29
collated on a data sheet and entered into the Redcap (research electronic data
capture) program. In the Redcap program each patient had a unique code and all
patient identifiers were removed to keep anonymity. Patient identifying data was only
known to the researcher. (Appendix 1)
The result of the invasive prenatal testing was obtained from the National Health
Laboratory Service system and reports of ultrasound examination during the
patients’ pregnancy were obtained from patients' files.
As outlined in the objectives complications related to the procedure were identified
and a fetal loss that occurred within two weeks of the procedure was recorded as a
complication associated with the procedure. Most miscarriages related to invasive
prenatal testing occur within 72 hours of the procedure and previous studies in this
field have defined the cut off for procedure related miscarriage to be two weeks
(36,100). Pregnancy outcome, where available, was also identified and this included
all known pregnancy losses including termination of pregnancy, spontaneous
miscarriage, stillbirths and perinatal mortality. According to the South African
Maternal Care guidelines of 2015 a miscarriage can be defined as a fetus of 28
weeks or less with no evidence of life at delivery (101). According to the South
African PIPP guideline perinatal mortality can be defined as all babies who have
demised after 22 weeks of gestation (500g or more) (52) thus in this study a
miscarriage was defined as a fetus weighing less than 500g. Where a normal
karyotype or PCR result was obtained the phenotypic appearance of the baby at
birth as described in the patient delivery chart was recorded.

30
3 RESULTS
A total of 97 invasive prenatal tests were performed between January 2014 to May
2016, of these results 96 results were obtained. During this time Rahima Moosa
Mother and Child Hospital had performed 29380 deliveries.
3.1 STUDY POPULATION DEMOGRAPHICS
3.1.1 Age
The mean age of women in the sample was 35 years. The oldest patient in the
sample was 47 years old and the youngest patient was 19 years old.
3.1.2 Ethnicity
Among the patients evaluated 71, 9% were Black, 9,4% were Caucasian, 12,5%
were from the Coloured community and 6,3% were from the Indian community.
Graph 3.1: Sample distribution by Ethnicity
Black 72%
Caucasion 9%
Indian 6%
Coloured 13%
Sample Distribution by Ethnicity
Black Caucasion Indian Coloured
31
There were three Black patients in the sample with infants with chromosomal
abnormalities, three with fetuses with chromosomal and structural abnormalities and
four patients with infants with normal karyotypes but structural abnormalities at birth.
In the Caucasian population there was one patient with a fetus affected by a
chromosomal abnormality.
In the Coloured community there were two patients with fetuses affected by
chromosomal abnormalities, two with fetuses with chromosomal and structural
abnormalities and two patients with infants with normal karyotypes but structural
abnormalities at birth.
In the Indian Community there was one patient with a fetus affected with a
chromosomal and structural abnormality.
3.1.3 Parity
Parity of 69 (72%) patients was known. The mean parity was two live births, with a
range from nought to seven live births.
3.1.4 Gravidity
Gravidity of 69 (72%) patients in the sample was known. The mean gravidity was
three pregnancies, with a range from one to eight pregnancies.
3.1.5 Chronic illnesses and medication use
Of the 66 patients in which this information was known, 14 patients had hypertension
with one not being on treatment. No chromosomal abnormalities were found in these
patients. One patient had a fetus with structural abnormalities and is discussed later
as patient 6.
Three patients had gestational diabetes. There were no patients with Type 1 or Type
2 diabetes. All the patients were managed with a diabetic diet and were not on
medication. One of these patients had a infant with a balanced translocation and is
discussed later as patient I.

32
There was one patient who is epileptic not on medication. She had an infant with a
normal karyotype who was healthy at birth.
There was one patient with Tuberculosis on treatment. She had an infant with a
normal karyotype who was healthy at birth.
There were three patients with asthma in the cohort who were all on treatment. Their
infants had normal karyotypes. Two patients had normal infants at birth, one birth
outcome is unknown.
There was one patient with hyperthyroidism on treatment who had a fetus with
Trisomy 21, this patient is discussed later as patient B. One patient was known with
thyroid cancer of the papillary type and was scheduled for surgery after the delivery
of her infant. She had an infant with a normal karyotype who was healthy at birth.
There was one patient with major depressive disorder on treatment. She had an
infant with a normal karyotype who was healthy at birth.
One patient had a previous deep vein thrombosis and was on anticoagulation in the
studied pregnancy. She had an infant with a normal karyotype who was healthy at
birth.
There was a patient in the sample with idiopathic intracranial hypertension on
treatment. She had an infant with a normal karyotype who was healthy at birth.
There were no known cardiac patients in the sample.
There was one patient with a known genetic condition, namely neurofibromatosis.
She had an infant with a normal karyotype who was healthy at birth.
3.1.6 Smoking, alcohol use and illicit drug use
There was one patient in the sample who smoked three cigarettes a day, the
duration is not known. This patient also drank four to five glasses of alcohol a day,
the type of alcohol and duration is not known. She had an infant with a normal
karyotype who was healthy at birth.
There were no patients that used illicit drugs.

33
3.1.7 Booking status of patients
Booking status of 66 (69%) patients was known.
3.1.7.1 Rhesus blood group
In the sample six patients (9%) were recorded as Rhesus blood group negative.
There was no record in the patient's files of whether these patients received anti-D
immunoglobulin after their invasive prenatal procedures. It is a standing
departmental policy that Anti-D should be administered to all Rhesus negative
women after an invasive procedure.
3.1.7.2 HIV status
Seventeen patients were found to be HIV positive, sixteen of these patients were on
antiretroviral therapy at the time of invasive prenatal diagnosis and one patient had
defaulted her treatment. CD4 counts of fourteen of the patients were available; the
range being 29cells/uL to 987cells/uL. Viral loads of five of the patients were known,
with three being lower than detectable and the other two having viral loads of 1910
IU/ml and 862IU/ml respectively. In the patient who had a viral load (VL) of
1910IU/ml antiretroviral therapy was initiated before booking for her pregnancy, in
the other patient the duration of antiretroviral treatment was not known. It is not
known what the viral loads were at the time of the invasive procedure being done as
the patient with a VL of 1910IU/ml had her VL done after the invasive procedure was
done, there is no record of a VL before the procedure. In the patient with a VL of
862IU/ml it is not known when in relation to the invasive procedure the VL was done.
Of the sixteen patients on antiretroviral therapy, it is known that six started their
antiretroviral treatment at the time of booking, this means that the minimum duration
that the patients were on antiretroviral therapy before their invasive prenatal test
ranged between one week and five weeks. Five patients started their antiretroviral
therapy before booking but the exact duration is unknown. The duration of
antiretroviral therapy taken is unknown in five patients.

34
3.1.7.3 RPR status
One patient was found to be RPR positive at time of invasive prenatal diagnosis and
was adequately treated.
3.1.7.4 Haemoglobin
The haemoglobin (Hb) of 57 patients were known, the mean Hb was 12,1g/dL at the
time of booking, with a range from 7,8g/dL to 14.8g/dL. There were eight patients
with haemoglobin values below 11g/dL.
3.1.8 Gestational age at first booking
The gestational age of first booking was known in 62 patients. The average
gestational age at booking was 16 weeks. The gestational age at first booking
ranges from five weeks to 27 weeks.
3.2 PATIENT RESULTS
Between the study period of January 2014 to May 2016, a total of 97 invasive tests
were performed. Results of 96 of these tests were obtained as one test result could
not be retrieved from the National Health Laboratory Services system.
There were 94 (98%) singleton pregnancies and two (2%) multiple pregnancies, both
being twin pregnancies. One twin pregnancy had one fetus affected by a
chromosomal abnormality (Patient F below), the other twin pregnancy had no
abnormalities found.

35
Diagram 3.1: Flow diagram of results
Total number of patients undergoing invasive
prenatal testing
97
1 result not retrieved
Total number of known invasive test results
96
All abnormalities
18
Total number of pregnancy outcomes
known
65

36
All abnormalities
found
Diagram 3.2: Relationship between chromosomal and structural
abnormalities
3.2.1 Chromosomal and genetic abnormalities found in the sample
A total of 12 (12, 5%) chromosomal abnormalities were found in the sample of
96 patients. Six of these patients had fetuses with Trisomies, two with Trisomy 21,
two with Trisomy 13 and two fetuses with Trisomy 18. Two fetuses were affected by
sex chromosome abnormalities in the form of Klinefelter Syndrome. One fetus had a
balanced translocation [4;13 (q35;q14)], one a diagnosis of cystic fibrosis,
one had spinal muscular atrophy and one had Wolf-Hirschorn syndrome.
6 6 5
Chromo-
somal and
structural
abnormalities
6
Structural
abnormalities
only
6
Chromosomal
abnormalities
only
6

37
Graph 3.2: Chromosomal abnormalities in the sample
3.2.1.1 Trisomy 21
Patient A
The first patient with a fetus with Trisomy 21 was a 38 year old P1G2 with no
previous history of chromosomal abnormalities. She booked at 21 weeks where a
fetal anomaly scan was done which found several markers namely thickened nuchal
oedema and an echogenic focus in the left ventricle. A second trimester
amniocentesis was offered to her and once the results of Trisomy 21 were
communicated and counselling done, the patient opted for a termination of
pregnancy at 24 weeks gestation. She delivered a 595g female fetus.
Patient B
The second patient with a fetus with Trisomy 21 was a 45 year old P3G7 known with
hyperthyroidism and on treatment who booked in the first trimester and underwent a
nuchal translucency scan at 13 weeks gestation that showed an increased nuchal
translucency and an absent nasal bone. The patient underwent a CVS that
Aneuploidies 50%
Sex Chromosome abnormalities
17%
Other 33%
Chromosomal Abnormalities

38
confirmed Trisomy 21. The patient opted for a termination of pregnancy in the first
trimester.
3.2.1.2 Trisomy 18
Patient C
The first patient with Trisomy 18 was a 42 year old P1G2 with a family history of a
child affected with ectrodactyly and missing right hand metacarpals. She had an
increased Trisomy 18 risk on her first trimester biochemical screening of 1 in 14.
Second trimester amniocentesis confirmed Trisomy 18. A fetal anomaly scan
showed choroid plexus cysts and a fetus with clenched fists and rocker bottom feet.
The outcome of her pregnancy is unknown
Patient D
The second patient found to have an infant affected with Trisomy 18 was a 27 year
old P3G4 with no previous history of chromosomal abnormalities. Her fetal anomaly
scan showed multiple abnormalities namely a mono-ventricle with thalami fused, the
cerebellum splayed with an absent vermis, a flattened forehead, cardiomegaly with a
pericardial effusion, an echogenic focus in the left ventricle and polyhydramnios. A
provisional diagnosis of holoprosencephaly was made. The patient underwent a
second trimester amniocentesis. The patient opted not to have a termination of
pregnancy or fetocide and delivered at 41 weeks by normal vaginal delivery. The
neonatal team made a clinical diagnosis of Trisomy 13 rather than the prenatal
diagnosis of Trisomy 18 but there was no karyotyping available after birth to confirm
the diagnosis. Unfortunately the infant was lost to follow up.
3.2.1.3 Trisomy 13
Patient E
The first patient with a fetus with Trisomy 13 was a 41 year old P7G8 who booked at
20 weeks gestation. She had no previous family or obstetric history of chromosomal

39
anomalies. She underwent an ultrasound at 25 weeks which found several
ultrasound abnormalities namely brachycephaly, micrognathia, alobar
holoprosencephaly, bilateral echogenic foci in the heart and an abnormal nose. A
second trimester amniocentesis showed Trisomy 13. The patient declined
termination of pregnancy and fetocide and delivered a fetus with features of Trisomy
13 at 32 weeks gestation by caesarean section. The patient's records state the
indication for the caesarean section was grand multiparity. The baby passed away
shortly after birth.
Patient F
The second patient to have fetus with Trisomy 13 was a 26 year old P1G2
who booked at 12 weeks gestation where a twin pregnancy was found.
The patient underwent a fetal anomaly scan at 21 weeks where features of
Trisomy 13 were found in the second twin namely a bulky thalamus, a
distorted cerebellum, a brachycephalic head, a soft tissue mass protruding
from the nasal area and a hypoplastic left ventricle. The first twin was
sonographically normal. A second trimester amniocentesis confirmed a
normal karyotype in the first twin and Trisomy 13 in the second twin. The
patient underwent a caesarean section at 33 weeks gestation. The patient's
records state that the indication for her caesarean section was a
compound presentation with a cord presentation. The first infant was healthy
at birth and the second twin had clinical features of Trisomy 13 and passed away
shortly after birth.
3.2.1.4 Sex Chromosome Abnormalities
Patient G
The first patient found to have a fetus with Klinefelter Syndrome was a 25 year old
female who underwent an anomaly scan at 23 weeks where an echogenic focus in
the left ventricle was found and the fetal growth was on the 5th centile. The patient

40
was offered a second trimester amniocentesis that showed Klinefelter Syndrome.
The outcome of her pregnancy is unknown.
Patient H
The second patient with a fetus with Klinefelter Syndrome was a 42 year old P1G2
with no history of previous chromosomal abnormalities in her family or other child.
She had a normal fetal anomaly scan and underwent a second trimester
amniocentesis. She delivered an infant at term by normal vaginal delivery with no
abnormal features noted at delivery and is being followed up by paediatrics.
3.2.1.5 Other Chromosomal Abnormalities
Patient I
A 23 year old P1G2 underwent an amniocentesis at 21 weeks as her partner was
known with a 4;13 and 8;10 translocation. She had also previously had an early
neonatal death following her previous pregnancy. Facial and brain abnormalities
were found in that infant. Her amniocentesis results showed that this fetus carried a
translocation 4;13 (q35;q14) but not a translocation 8;10. A healthy looking infant
was delivered at 40 weeks gestation by caesarean section.
3.2.1.6 Genetic abnormalities
Patient J
One case of cystic fibrosis was found in a 21 year old patient known with gestational
diabetes who had previously had a daughter with cystic fibrosis. She underwent an
amniocentesis at 18 weeks gestation which confirmed that her fetus was
homozygous for the F508 mutation. The outcome of her pregnancy is unknown.
41
Patient K
A 38 year old patient underwent a second trimester amniocentesis at 19 weeks
gestation as she had a son with spinal muscular atrophy who had a homozygous
deletion SMN1 exon 7 (CGC1301363). The patient was tested and was found to be
a carrier for spinal muscular atrophy. The second trimester amniocentesis revealed a
fetus who was also a carrier of the disease. The outcome of her pregnancy is
unknown.
Patient L
A 23 year old primigravida who had a fetal anomaly scan at 23 weeks gestation was
found to have a fetus with Wolf-Hirshcorn disease. She had no previous family
history of chromosomal abnormalities. The fetal anomaly scan showed multiple
abnormalities namely an absent nasal bone, increased prenasal oedema, an
hourglass posterior fossa, a thickened nuchal translucency, short femur and
humerus, clinodactyly, a probable membranous venrticuloseptal defect, a clubfoot,
rocker bottom feet and a single umbilical artery. The patient opted for a fetocide at
30 weeks gestation and delivered a 1000g infant by normal vaginal delivery. The
postnatal diagnosis was compatible with the antenatal diagnosis.

42
Table 3.1: Chromosomal abnormalities found in sample
Patient Chromosomal
abnormality
Aneuploidy
Patient A Trisomy 21
Patient B Trisomy 21
Patient C Trisomy 18
Patient D Trisomy 18
Patient E Trisomy 13
Patient F Trisomy 13
Sex Chromosome
Abnormalities
Patient G Klinefelter Syndrome
Patient H Klinefelter Syndrome
Translocation
Patient I Balanced Translocation
4;13 (q35;q14)
Genetic
Abnormalities
Patient J Cystic Fibrosis
Patient K Spinal Muscular Atrophy
Patient L Wolf-Hirshcorn Disease
In summary there were six patients (50%) who were of advanced maternal age in the
sample of patients who had chromosomal abnormalities. Two patients (17%)

43
underwent invasive prenatal testing due to a previous history of chromosomal
abnormalities. In the sample eight patients (67%) had abnormal ultrasound findings.
There were three patients (25%) with both risk factors of advanced maternal age and
abnormal ultrasound findings. Of the twelve patients, eleven had singleton
pregnancies and one patient had a twin pregnancy. The invasive tests included ten
second trimester amniocenteses, one third trimester amniocentesis and one CVS.
Outcome of eight pregnancies (67%) are known and of these two patients (17%)
underwent termination of pregnancy and one patient (8%) underwent fetocide. There
was one instance (Patient D) where neonatal findings did not agree with invasive
test results but this finding was not confirmed.

44
Table 3.2: Outcome of pregnancies with fetuses affected by
chromosomal abnormalities
Abnormality Continued
pregnancy
TOP Fetocide Unknown
Trisomy 21 2
Trisomy 18 1 1
Trisomy 13 2
Klinefelter
Syndrome
1 1
Cystic
fibrosis
1
Spinal
muscular
atrophy
1
Wolf-
Hirschorn
Syndrome
1
Translocation 1
Total 6 2 1 3
3.2.2 Structural abnormalities in the sample
In the sample of 97 patients, there were thirteen patients with major structural
anomalies at ultrasound alluding to possible outcome of structural abnormality at
birth. Two of these patients had normal infants at birth. Six patients had fetuses with
chromosomal abnormalities confirmed at karyotyping and are discussed above
(Patients A, B, D, E, F and L) .

45
Below the remaining five patients with major structural anomalies on ultrasound and
structural abnormalities in their infants confirmed at birth are discussed. One patient
is also discussed where only soft markers were found in her infant at ultrasound but
structural abnormalities at birth.
Patient 1
The first patient who had a fetus with structural abnormality diagnosed on ultrasound
was 34 year of P2G4. A large exomphalos with liver involvement was found at a 21
week fetal anomaly scan. The patient had no previous history of chromosomal
abnormalities and her second trimester amniocentesis had a normal karyotype. The
patient delivered at 32 weeks gestation by caesarean section due to cord prolapse.
The antenatal findings were confirmed by the neonatal team and the infant was
admitted into their care.
Patient 2
The second patient was a 23 year old P0G1 who underwent an ultrasound at 31
weeks gestation that found the fetus had an increased biparietal diameter,
hypomineralisation of the fetal skull bones, strawberry sign head, frontal bossing, a
small mandible and mouth, a short humerus, an enlarged cardiothoracic ratio,
polyhydramnios, an absent stomach bubble alluding to a trachea-eosophageal
fistula, an omphalocoele involving small bowel, a bowed femur, bowed tibia and
fibula and rocker bottom feet. It must be assumed that this late scan was done
opportunistically at time of referral. The patient underwent a third trimester
amniocentesis which showed a normal karyotype. Although the patient had booked
at eight weeks gestation she was referred to Rahima Moosa Mother and Child
Hospital in her third trimester. She underwent a caesarean section at 37 weeks
gestation and the antenatal findings were confirmed by the neonatal team. Her infant
demised shortly after birth.

46
Patient 3
The third patient was a 37 year old P3G4 who had a previous early neonatal death.
The only record made of this death is that the infant was found to have a short
umbilical cord at birth. The patient underwent a fetal anomaly scan at 20 weeks
gestation that showed holoprosencephaly, this finding was confirmed on an
antenatal MRI. The patient had a cordocentesis at 30 weeks gestation with a normal
karyotype. The patient opted for fetocide at 30 weeks gestation and underwent a
caesarean section as induction of labour had failed.
Patient 4
The fourth patient was a 23 year old P1G2 with an unremarkable antenatal history.
The patient underwent an opportunistic ultrasound at 28 weeks gestation which
showed polyhydramnios, cerebellar vermis agenesis, an abnormal four chamber
heart view, cardiomegaly and axis deviation, a small stomach bubble, a single
kidney, bilateral cleft lip and palate, a single umbilical artery and flat facial profile.
The patient underwent a second trimester amniocentesis which found a normal
karyotype. She presented with an IUFD at 37 weeks gestation and delivered by
normal vaginal delivery. No notes were made of the postnatal findings of the infant at
birth. Placental histology showed features of uteroplacental underperfusion.
Patient 5
The fifth patient was a 24 year old who underwent an anomaly scan which showed
holoprosencephaly, a second trimester amniocentesis showed a normal karyotype in
her fetus. Due to this patient's record being lost no further information about the
outcome of her pregnancy is known.
Patient 6
The sixth patient was a 23 year old primigravida who had a fetus with several soft
markers on ultrasound namely a ventriculomegaly, echogenic bowel and a lemon
shaped head. The patient had a second trimester amniocentesis with the fetus

47
having a normal karyotype. At birth this infant was found to have a cleft lip and
palate, low set ears, elongated anterior fontanelles, flat nasal bridge and upfolding
epicanthic folds. The infant is being followed up by paediatrics and has
multiple cardiac abnormalities including a patent ductus arteriosus, a
ventriculoseptal defect and neonatal dilated cardiomyopathy. The infant also
developed epilepsy and is neurodevelopmentally delayed, a specific genetic
diagnosis has not been made but follow up is ongoing.
3.3 INDICATIONS FOR INVASIVE PRENATAL TESTING
Table 3.3: Indications for invasive prenatal testing
Indication Number Percentage (%)
Abnormal Ultrasound
Findings
60 63
Advanced Maternal Age 58 60
Family History 9 9
Maternal Request 2 2
Abnormal Screening
Test
2 2
Recurrent first and
second trimester
miscarriages
1 1

48
Graph 3.3: Indications for invasive prenatal testing
As can be seen from the above mentioned table and chart there were some patients
who had more than one indication for invasive prenatal testing. The most common
being abnormal ultrasound findings and advanced maternal age. There were three
patients (25%) with both risk factors of advanced maternal age and abnormal
ultrasound findings in the group with chromosomal abnormalities and one patient
with both risks in the group with structural abnormalities.
3.3.1 Abnormal Ultrasound Findings (Objective 1)
As per objective one, in 90 women it is known when their first ultrasound was done,
the mean gestational age of first ultrasound was 19 weeks, the range was from six to
34 weeks.
A dating scan was performed in 43 patients (47.8%) with one of these patients going
on to have a nuchal translucency scan as her dating scan was done at six weeks
gestation. Fifteen of these patients went on to have an anomaly scans. Nuchal
translucency scans were done in four patients (4,4%), one having a dating scan
0
10
20
30
40
50
60
70 63 60
9 2 2 1
Indications for Invasive Prenatal Testing

49
initially as aforementioned. These three patients went on to have a fetal anomaly
scan.
Fetal anomaly scans were done in 43 (47,8%) patients as their initial scan. Thus 61
patients underwent anomaly scans either initially or after other types of ultrasounds.
Of the four patients who underwent nuchal translucency scans, three went on to
have anomaly scans. One of the patients with an increased nuchal translucency had
a CVS that showed Trisomy 21 (Patient B). Of the remaining three patients, one had
a normal nuchal translucency and anomaly scan and the indication for invasive
prenatal testing was based on advanced maternal age. The second patient had an
abnormal nuchal translucency scan with an increased nuchal thickness and
subsequently had an amniocentesis at 16 weeks gestation due to this finding. The
amniocentesis showed a normal karyotype in the fetus. She had a previous infant
affected with pyelectasis. An anomaly scan later in the studied pregnancy did show
pyelectasis but she had a healthy infant at birth. The third patient had an abnormal
nuchal translucency scan at 13 weeks and two days and underwent a amniocentesis
because of this finding at 16 weeks gestation. The result of the amniocentesis was
normal.
Graph 3.4: Frequency for types of ultrasounds performed initially
48%
4%
48%
Frequency for types of ultrasounds which are performed initially
Dating scan Nuchal Translucency scan Fetal Anomaly scan

50
In 60 patients (63%) the abnormal ultrasound findings led to an invasive prenatal test
being performed.
The most common soft marker found of all the ultrasounds performed was an
echogenic cardiac focus which was found in 33 patients (34,7%). The following
distribution of frequency of soft markers were found; intracardiac echogenic focus in
33 patients, increased nuchal fold thickness in thirteen patients, echogenic bowel in
eleven patients, ventriculomegaly in four patients, choroid plexus cysts in three
patients, pyelectasis in three patients and a short femur in two patients. Thirteen
patients had more than one soft marker. In the patients where soft markers were
found seven patients had an abnormal karyotype (Patients A, B, C, D, E, G and L)
thus 11,6% had abnormal karyotypes. All these patients had multiple soft markers
accept patient G who had only one soft marker.
Graph 3.5: Frequency of Soft Markers
13
3
33
3 2 4
11
3 1
4
0 1 0 0
Frequency of Soft Markers
Frequency of soft marker Frequency of abnormal karyotype with soft marker

51
There were thirteen patients in which structural abnormalities were found in the fetus
at ultrasound. A range of major structural anomalies were found on ultrasound
namely exomphalos, holoprosencephaly, duodenal atresia, omphalocoele,
tracheoesphageal fistula, absent nasal bone, cerebellar vermis agenesis, cleft lip
and palate. The most common major structural anomaly found in fetuses was
holoprosencephaly followed by duodenal atresia. In five patients both hard and soft
markers were found in the fetuses. Nine patients had antenatal major structural
anomaly findings in the fetuses confirmed at the birth. Of these eight patients, six
patients were also found to have fetuses with abnormal karyotypes with
chromosomal abnormalities (Patients A,B,D,E,F and L), one patient with an infant
with exomphalos was admitted into neonatal care (Patient 1), one patient with a baby
with an omphalocoele and a tracheoesphageal fistula underwent a caesarean
section and the infant passed away shortly after birth (Patient 2). One patient with a
fetus affected with holoprocencepaly opted for fetocide (Patient 3), one patient with a
fetus affected by cerebellar vermis agenesis presented with an IUFD (Patient 4).
One of the twelve patients with a fetus affected by the major structural anomaly of
holoprosencephaly was lost to follow up. Two of the patients who were thought to
have fetuses affected with duodenal atresia antenatally had structurally normal
infants at birth. One patient had multiple soft markers on ultrasound but structural
abnormalities were found at birth (Patient 6).
3.3.2 Advanced Maternal Age
In the sample of 96 women, 58 were of advanced maternal age. The mean age of
women in the sample was 35 years. The oldest patient in the sample was 47 years
old and the youngest patient was 19 years old. Advanced maternal age was found in
six (50%) of the women with chromosomal abnormalities. One patient with structural
abnormalities and a normal karyotype was of advanced maternal age. Of the total of
58 advanced maternal women, seven abnormalities were found (chromosomal and
structural), thus 12%. The chromosomal abnormalities found were Trisomies most
commonly Trisomy 21. Abnormal ultrasound markers were found in 24 (25%) women
of advanced maternal age. Six patients of advanced maternal age had a previous
history of a chromosomal or structural abnormality, two having a previous infant born
52
with Trisomy 21 and one with a previous infant born with Trisomy 13. These three
patients had normal karyotypes in the pregnancy studied.
There were 2334 patients of advanced maternal age who attended Rahima Moosa
Mother and Child Hospital antenatal clinic over the period studied which means 7,9%
of the patients who delivered over the study period was of advanced maternal age.
Therefore 58 out of 2334 patients underwent invasive testing meaning 2.5% of
advanced maternal age mothers were offered invasive prenatal testing. (E Bera
2016, Principal Specialist at RMMCH, oral communication, 30 September 2016)
3.3.3 Family History of Chromosomal and Genetic Abnormalities
Twelve patients underwent invasive prenatal testing due to a family or personal
history of chromosomal, genetic or structural abnormality. Of these abnormalities
three were previous infants with Trisomy 21, one with a previous infant with Trisomy
13, one with a previous infant with pyelectasis, one patient with a previous child with
cystic fibrosis (Patient J), one patient with neurofibromatosis, one patient with a
previous infant with brain and facial abnormalities as well as a known balanced
translocation in her partner (Patient I), one patient with an infant death due to
congenital heart disease, one with a previous infant with spinal muscular atrophy
(Patient K), one patient with an unexplained stillbirth at term but also known with
gestational diabetes and one with a sister with an infant with ectrodactyly and
missing right hand metacarpals (Patient C).
Seven of the twelve patients were of advanced maternal age and five of the twelve
patients had abnormal ultrasound findings.
Four of patients had fetuses with abnormal karyotypes namely patients C, I, J and
K. Of these patients only patient C had abnormal ultrasound findings.
3.3.4 Positive Biochemical Screening Tests
Two patients were transferred from the private sector for invasive prenatal testing
due to an abnormal first trimester screening test. This was a 36 year old P4G5 with
an increased first trimester Trisomy 21 risk. She had no previous history of

53
abnormalities and a normal ultrasound. The patient underwent a second trimester
amniocentesis that was found to be normal. She delivered a healthy infant at 31
weeks gestation via normal vaginal delivery. The reason for her premature labour is
unknown.
The second patient was Patient C as discussed above (pg. 45)
3.3.5 Other Indications for Invasive Prenatal Testing
A 26 year old patient underwent second trimester amniocentesis as she had suffered
several first trimester and second trimester miscarriages as well as an IUFD. On
ultrasound severe intrauterine growth restriction was found. Her amniocentesis result
was normal but unfortunately the outcome of her pregnancy is unknown as she was
lost to follow up.
There were two patients who requested invasive prenatal testing. These patients
were Patient I and J as discussed above.
3.4 INVASIVE PRENATAL TESTS PERFORMED
There were 97 invasive prenatal tests performed with 96 results being obtained. One
second trimester amniocentesis result was lost and cannot be found on the National
Health Laboratory Service system. CVS was done in one patient in the first trimester,
second trimester amniocenteses was done in 90 patients, four patients underwent
third trimester amniocentesis and one patient underwent cordocentesis at 30 weeks
gestation. No first trimester amniocentesis were done.
The gestation at which second trimester amniocentesis was done is known in 86
patients with a mean gestation of second trimester amniocentesis is 21 weeks, and a
range from 16 weeks to 27 weeks.

54
Graph 3.6: Invasive Prenatal Tests Performed
The CVS was done in a 45 year old P3G7 who booked in the first trimester and
underwent a nuchal translucency scan at 13 weeks gestation that showed an
increased nuchal translucency and an absent nasal bone. The patient underwent a
CVS that confirmed Trisomy 21. The patient opted for a termination of pregnancy in
the first trimester (Patient B).
Third trimester amniocentesis was done in four patients. The first patient had a
dating scan at 32 weeks gestation that showed several soft and major structural
anomalies, she had a normal karyotype subsequently. The second patient was a 24
year old P1G2 who had multiple abnormalities found on fetal anomaly scan and
underwent an amniocentesis at 27 weeks gestation, the fetus consequently had a
normal karyotype. The third patient who underwent a third trimester amniocentesis
was a 21 year of P0G1 who underwent an amniocentesis at 34 weeks gestation due
to suspected duodenal atresia found on ultrasound. Her fetus had a normal
karyotype and she delivered a normal infant at birth. The fourth patient with a third
trimester amniocentesis was a 23 year old P0G1 who had the procedure at 31
weeks gestation due to multiple structural abnormalities seen on ultrasound. Her
fetus had a normal karyotype, her infant was born confirming the antenatal structural
abnormalities passing away shortly after birth (Patient 2).
Chorion villous
sampling 1%
Second trimester amniocentesis
94%
Thrid trimester amniocentesis
4%
Cordocentesis 1%
Invasive Prenatal Tests Performed
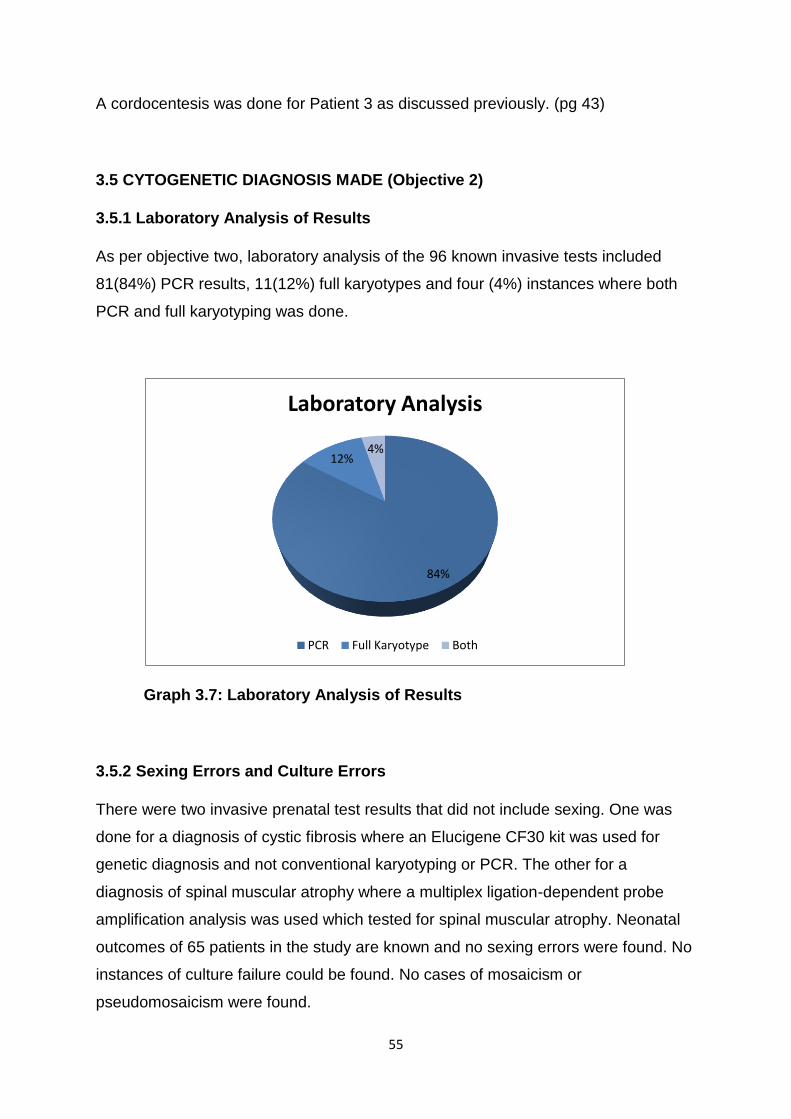
55
A cordocentesis was done for Patient 3 as discussed previously. (pg 43)
3.5 CYTOGENETIC DIAGNOSIS MADE (Objective 2)
3.5.1 Laboratory Analysis of Results
As per objective two, laboratory analysis of the 96 known invasive tests included
81(84%) PCR results, 11(12%) full karyotypes and four (4%) instances where both
PCR and full karyotyping was done.
Graph 3.7: Laboratory Analysis of Results
3.5.2 Sexing Errors and Culture Errors
There were two invasive prenatal test results that did not include sexing. One was
done for a diagnosis of cystic fibrosis where an Elucigene CF30 kit was used for
genetic diagnosis and not conventional karyotyping or PCR. The other for a
diagnosis of spinal muscular atrophy where a multiplex ligation-dependent probe
amplification analysis was used which tested for spinal muscular atrophy. Neonatal
outcomes of 65 patients in the study are known and no sexing errors were found. No
instances of culture failure could be found. No cases of mosaicism or
pseudomosaicism were found.
84%
12% 4%
Laboratory Analysis
PCR Full Karyotype Both

56
3.6 COMPLICATIONS OF INVASIVE PRENATAL TESTING (Objective 3)
As per objective three, only one case of miscarriage after a second trimester
amniocentesis was found. This patient was a 36 year old patient who had had two
previous second trimester miscarriages that were thought to be due to cervical
incompetence. She underwent a amniocentesis at 22 weeks due to her advanced
maternal age and an echogenic intracardiac focus found at ultrasound. She had a
spontaneous complete miscarriage of a 550g infant two days after the amniocentesis
was done. The amniocentesis procedure was uneventful and showed a normal
karyotype.
The outcome of the pregnancy in 65 patients (68%) was known, thus the
miscarriage rate is 1,5%.
No other complications due to the procedure were found in the study.
3.7 PREGNANCY OUTCOMES (Objective 4)
As per objective four, in the sample of 97, the outcomes of 65 (68%) of the
pregnancies are known.
Included are two cases of termination of pregnancy that were directly related to the
result of the invasive prenatal test. Both terminations of pregnancy were done for
confirmed Trisomy 21 fetuses, one in the first trimester and one in the second
trimester (Patients A and B)
There was one case of elective fetocide directly related to prenatal testing. A case of
a fetus affected with Wolf-Hirschorn syndrome where a fetocide was done at 30
weeks gestation (Patient L). There was another case of fetocide of a infant affected
by holoprosencephaly where a fetocide was done at 30 weeks gestation, this was
done as a direct result of antenatal ultrasound diagnosis and not prenatal testing.
(Patient 3).
There was one case of intrauterine fetal death. This was a case of a woman where
multiple ultrasound abnormalities were found including agenesis of the cerebellar
vermis and cleft lip and palate. She presented with an IUFD at 37 weeks gestation
and underwent an induction of labour (Patient 4).

57
After excluding chromosomal and structural abnormalities, 84 pregnancies with
normal karyotypes were traced. Pregnancy outcome of 65 of the cohort of 96
patients are known, 52 of these pregnancies had infants with normal phenotypic
appearances at birth, eight patients had features of chromosomal abnormalities as
diagnosed prenatally and five patients had features of structural abnormalities that
were diagnosed prenatally.

58
4. DISCUSSION
4.1 INTRODUCTION
Invasive prenatal testing has been available in the public sector in South Africa since
1994 (40). The review of this service at Rahima Moosa Mother and Child hospital
has highlighted several successes and shortcomings of such a service being run in a
resource restricted setting.
4.2 PATIENT POPULATON DEMOGRAPHICS
4.2.1 Antenatal care - Booking and referrals
Antenatal care aims to provide the identification of avoidable factors to provide a
normal pregnancy and delivery of a healthy infant with the least possible morbidity
(40). Patients tend to book late in their pregnancies, the average gestational age of
booking in the study was 16 weeks, with 61 of the 62 patients in which this
information is known booking before 24 weeks gestation. Myer et al. showed in a
study done in rural South Africa that women generally do not perceive antenatal care
as important as pregnancy is not perceived to carry risk but showed that there is a
perception that labour and delivery carries the risk. They found that women mainly
went for one antenatal clinic visit to receive an antenatal card to present at delivery
(102). Peripheral clinics are also referring patients late, this was also found by
Watcham et al (40). This creates a situation where the opportunity for invasive
prenatal screening and testing especially in the first trimester is missed.
In the government sector ultrasound is one of the methods available for screening
due to the cost related to other screening options. The literature has shown that this
is a method of screening that can be used in association with other screening tests
to give an associated risk and both first trimester and second trimester markers can
be associated with chromosomal abnormalities (12). During the first trimester
ultrasound the measurement of nuchal translucency has been shown to identify 75%
of fetuses affected by Trisomy 21 with a 5% false positive rate. Another marker of
Trisomy 21 in the first trimester ultrasound is the absence of the nasal bone. When

59
maternal age, nuchal translucency and nasal bone measurement are combined it
has a detection rate of 95% with a false positive rate of 5% (7,9,10). By booking late
or being referred late the patient also misses the opportunity of a screening
ultrasound.
All of this highlights the lack of understanding and education in the community of the
importance of antenatal care and the lack of knowledge by referring healthcare
professionals of the importance of prenatal diagnosis in a high risk population. As the
average age of booking was found to be 16 weeks and all the patients except one
booked before 24 weeks there is potentially a missed opportunity as all patients
could not have a fetal anomaly scan. The gestation at booking for all the patients
who delivered in this time period has not been examined.
4.2.2 Ethnicity
There were chromosomal abnormalities found in all ethnic groups in the sample with
the most being found in the Black community. Most structural abnormalities with
normal karyotypes were found in the Black community. This may be explained by the
fact the Black community comprised the largest component of the sample at 71,9%
Venter et al. concluded in their study that the incidence of congenital anomalies in
black South African neonates were comparable to the incidence in that of other First
and Third world countries (49).
Inferences of incidence of congenital anomalies in different ethnic groups cannot be
drawn in this study cohort due to the small study sample, bigger population based
studies are needed.
4.2.3 HIV and invasive prenatal testing
South Africa has a large burden of HIV and 29,7% of pregnant women were infected
with HIV in 2013 (94,95). In the study cohort seventeen patients were found to be
HIV positive at the time of an invasive prenatal test being performed.
HIV transmission during invasive prenatal testing is thought not to be a risk provided
that the mother is on antiretroviral therapy and has a low viral load (86–89,91)

60
One patient was not on antiretroviral therapy as she had defaulted her treatment. It is
advisable that a patient be on antiretroviral therapy for 4-6weeks before an invasive
procedure is performed as this will allow for adequate viral suppression (96). Of the
sixteen patients on antiretroviral therapy it is known that six started their antiretroviral
treatment at the time of booking, this means that the minimum duration that the
patients were on antiretroviral therapy before their invasive prenatal test ranged
between one week to five week. Five patients started their antiretroviral therapy
before booking. This indicates that patients might not have had a adequate duration
of antiretroviral treatment before their invasive prenatal tests were done.
Of the patients with known viral loads three had lower than detectable viral loads and
two had viral loads of 1910IU/ml and 862IU/ml. The RCOG recommends that the
viral load of a patient be undetectable before and invasive procedure is done (93). In
the last two patients mentioned it is not known what the viral loads were at the time
of invasive testing as the VL test was performed after the invasive procedure in one
patient and it is not known when the viral load was done in relation to the
amniocentesis in the second patient. Guidelines state that viral load of a patient
should be done before the invasive test is done and that this is a part of counselling
for the invasive test (96).
The implementation of first trimester screening can limit the amount of invasive tests
needed in a country like South Africa where the burden of HIV is high and resources
for VL testing might not be available. This is also supported by Naidoo et al. in their
local study as well as Constantatos et al. (15,94).
In summary HIV transmission must be taken into consideration when an invasive
prenatal test is performed. The patient must be on antiretroviral therapy and have a
known suppressed viral load. Most importantly the patient must be counselled on
the risk of transmission as part of informed consent for the procedure (96). We live in
an era where HIV testing and antiretroviral therapy is freely available and every
patient has the opportunity to be virally suppressed and undergo an invasive
prenatal test safely. Serious ethical and medico-legal issues can be the
consequence if there is no attention paid to a patient's HIV status.

61
4.3 INDICATIONS FOR PRENATAL TESTING
Different settings in the world have different indications for invasive prenatal testing,
notably in resource restricted settings and third world countries advanced maternal
age remains the mainstay of screening where in the first world abnormal serum
markers and abnormal ultrasound findings are much more common indications for
invasive testing (25,33,35,36). In the setting of this study abnormal ultrasound
findings (63%) was the most common indication for invasive testing with advanced
maternal age (60%) being a close second.
As mentioned above the greatest indications for invasive prenatal testing are
abnormal ultrasound findings and advanced maternal age. In the modern era of fetal
medicine there are many advances in non invasive prenatal testing and biochemical
markers to detect chromosomal abnormalities. It has been shown that a combination
of maternal age, nuchal translucency, nasal bone an biochemical markers in the first
trimester have a detection rate of 95% and a 5% false positive rate for Trisomy 21
(7).
In the study population only two patients underwent biochemical screening that led to
invasive prenatal testing. Both these patients were referred from the private sector
and had had positive first trimester screening tests. This highlights the outdated
system of risk assessment and screening of patients needing invasive prenatal
testing, which is mainly based on advanced maternal age and ultrasound findings. It
would greatly benefit the pregnant population in the public sector in South Africa if
either combined first trimester screening service by accredited personnel or second
trimester screening was made available to them. As resources are limited the cost to
benefit ratio must be taken into consideration before such a service is implemented.
Naidoo et al. did however show that the use of nuchal translucency and maternal
age as a screening protocol were equivalent to international standards (15). This
protocol of course has the caveat that patients need to book early enough to have a
nuchal translucency scan.
A very encouraging finding in the study is the that there were eleven patients who
underwent invasive prenatal testing due to a family history of chromosomal or
genetic abnormalities and that there were two patients who requested invasive
prenatal testing (both having a previous history of a chromosomal abnormality). In

62
the literature Pala et al. found a 10% rate of maternal request in their study but in
most studies maternal request is either a very small component of the indications for
invasive testing or not mentioned at all (36).
Although these numbers are small it is encouraging that the community and the
referring healthcare workers show understanding and knowledge for other
indications for invasive prenatal testing.
Non invasive prenatal testing (NIPT) was not done in any patients in the cohort as
this service is not available in the public sector in South Africa (19). The ACOG do
currently recommend that conventional screening methods remain the most
appropriate choice for most women in the general population but does recommend it
being done in certain high risk populations (2,17). A population can be divided into
high risk (1:100 or lower), intermediate risk (1:101-1:2500) and low risk (<1:2500),
NIPT should be offered to patients in the intermediate risk category. Some studies
suggest that NIPT should be offered in a patient with a risk of 1:101-1:2500 (20,21).
4.3.1 Abnormal Ultrasound Findings
As previously discussed the most common indication for invasive prenatal testing
was abnormalities found on ultrasound. The most common ultrasound that was
performed initially was a dating scan, dating scans are generally opportunistic
ultrasounds done when patients present to RMMCH antenatal clinic and may be
performed by registrars in the department or by the ultrasound department. If the
dating scan is early enough an anomaly scan will be booked. Anomaly scans were
done in 59 patients and this can be explained by the mean gestational age at first
ultrasound being late, at nineteen weeks gestation. This advance gestation at
ultrasound is most probably a combination of late booking by patients and late
referral by surrounding clinics. But due to the average age of booking being 16
weeks gestation it may be that late referral plays a bigger role as well as availability
of trained staff to do anomaly scans. In seven of the patients where soft markers
were found there was also a chromosomal abnormality found. Six of these patients
had multiple soft makers, the literature supports this in that multiple soft markers
have a cumulative effect and will increase a patient's risk of having an aneuploidy
(14).

63
Thirteen of the patients in the cohort had so called major structural anomalies that
alluded to possible structural abnormalities at birth, ten of these patients had
structural abnormalities confirmed at birth (six having a concomitant chromosomal
abnormality). This is supported by the literature where the risk of aneuploidy
increases with structural abnormalities found (13).
4.3.2 Advanced Maternal Age
Women with advanced maternal age are at increased risk of delivering an infant with
a chromosomal or congenital abnormalities (40,103). In South Africa 13,4% of
pregnant women fall into the advanced maternal age category (46). The study
showed 60% of women were of advanced maternal age. Of the patients with fetuses
with either chromosomal and/or structural abnormalities 7 were found to be of
advanced maternal age. It is well known from the literature that this is a important
risk factor that needs to be taken into account when screening is done (39,40,43).
But it is inadequate to use it as an independent risk factor with the advances in fetal
medicine and other screening methods. It is still an important component of prenatal
testing but independently advanced maternal age has a 50% detection rate for
Trisomy 21 with a 15% false positive rate which shows it needs to be used in
combination with other screening tests (7). The high number of AMA patients is one
of the reasons the results are biased towards an increased rate of abnormalities.
.
4.3.3 Chromosomal abnormalities
In the study cohort twelve patients (12,5%) were identified with chromosomal
abnormalities in comparison to international studies which range from 2-10%
(25,33,36,54). The high rate is most probably due to the fact that the study
population was small and biased towards more high risk individuals.
The Perinatal Problem Identification Program (PIPP) in 2014 showed that congenital
abnormalities is the third leading cause of early neonatal death in South Africa (52),
thus highlighting the importance detecting chromosomal abnormalities prenatally. In
most studies the most common chromosomal abnormality detected was Trisomy 21
(25,48,54). In this study Trisomies were the most common chromosomal abnormality
64
found with Trisomy 21, Trisomy 18 and Trisomy 13 found in equal measures (six
patients were found to have fetuses affected by Trisomies, two with fetuses affected
by Trisomy 21, two with Trisomy 18 and two with Trisomy 13). In the patients who
were of advanced maternal age with fetuses affected by chromosomal abnormalites
two had fetuses affected with Trisomy 21, one fetus was affected with Trisomy 18
and one fetus with Trisomy 13.
Klinefelter syndrome was found in two fetuses of mothers who underwent invasive
prenatal testing. One test was done due to advanced maternal age with no
abnormalities on ultrasound and one test was done due to an echogenic focus in the
left ventricle and fetal growth being on the 5th centile on ultrasound . Both infants
were healthy looking at birth. This diagnosis is usually incidental and not due to
ultrasound abnormalities or abnormalities found at delivery of the infant. Gruchy et
al. showed that making the diagnosis is important and can provide information to the
expecting couple in terms of treatment options for the infant. These patients usually
present with infertility thus infertility treatments can be offered earlier to the affected
individual. Delayed language development can also be seen and can be corrected
by early speech therapy. Their study also showed that providing adequate
counselling to the couple at the time of diagnosis and treatment options decreased
the rate of termination of pregnancy and that although it is mostly an incidental
diagnosis it is an important one to make (104).
It has been shown that the widespread implementation of prenatal screening
combined with prenatal diagnosis and termination of pregnancy services
substantially reduced the expected number of infants born with Trisomy 21 (5).
Delport, Kromberg and Christianson et al. showed that Trisomy 21 is a important
condition in South Africa. (47,48,50).
4.4 INVASIVE PRENATAL TESTS PERFORMED
Second trimester amniocentesis was the most common invasive prenatal test
performed in the study population and it can be concluded that the trend of late
booking and the high number of second trimester fetal anomaly scans led to this.
The average gestation at which ultrasound was performed was 19 weeks. Second
trimester amniocentesis is accepted in the literature as the method most easily

65
performed among the invasive diagnostic methods (27). Third trimester
amniocentesis was done in four patients where structural abnormalities were found
at late gestations. It can be concluded that in view of the severity of the ultrasound
findings an invasive test was a reasonable offer despite the advanced gestation .
This might have aided patients to assist in counselling on prognosis and to help in
the future when determining risk of recurrence.
Only one patient in the cohort underwent a CVS and this was due to abnormalities
found on a nuchal translucency scan. There were two instances that abnormalities
were found on a nuchal translucency scan but a second trimester amniocentesis was
opted for later on during the patients' pregnancies. There may be several reasons for
this, both these patients underwent their nuchal translucency scan at thirteen weeks
gestation which may have necessitated a second trimester amniocentesis due
appointment for invasive testing only being available in their second trimester. It may
also have been due to the patients choice of waiting for a second trimester
ultrasound and the spontaneous miscarriage risk of CVS being higher than that of
second trimester amniocentesis (1), or that there were no personnel skilled in CVS
available at the time of their abnormal nuchal translucency scan.
There was one case where a cordocentesis was performed in a patient who had a
late diagnosis of an fetus affected by holoprosencephaly on ultrasound. Literature
dictates that cordocentesis is rarely performed with the availability of other invasive
prenatal testing techniques that are easier to perform and safer (16,24). This patient
also underwent a fetocide at the same time as her cordocentesis and this might be
the reason this type of test was opted for.
4.5 CYTOGENETIC TESTS PERFORMED
The most common test performed for cytogenetic diagnosis was a PCR, this might
be explained by this test overcoming the need for culture of fetal cells, making it
more cost effective with a rapid turn over time. It is also fully automated (65). In a
resource limited setting a cost effective automated test is of great value.

66
4.6 COMPLICATIONS OF INVASIVE PRENATAL TESTING
Spontaneous abortion as a complication of invasive prenatal procedure was found in
one patient who underwent a second trimester amniocentesis. Thus a spontaneous
abortion rate of 1.5% was found in the cohort, the patient however did have cervical
incompetence which might have been a confounding factor. The rate of 1,5% is
higher than the 0.5-1% quoted by Tabor et al (14). While the Danish Fetal Medicine
Study Group found that CVS and amniocentesis do not significantly increase
miscarriage rates and the fetal loss rate due to invasive procedure should be very
low.(58) This information is helpful in terms of counselling as one can provide an
institutionally specific rate for invasive prenatal procedures at RMMCH, however the
sample size is small and there is missing data.
4.7 PREGNANCY OUTCOMES
It can be seen from the results that management options were conservative in terms
of an abnormal invasive test result and that respect for patient choices exists as
there are several instances of termination of pregnancy and fetocide but also several
instances where termination of pregnancy was declined or where fetocide was
declined. In these instances the Rahima Moosa Mother and Child team continued
the care of the mother and fetus and provided paediatric support where indicated at
birth. This is of upmost importance in a setting where many different cultures and
beliefs come into play.
The SOGC showed that it is a common misconception that termination of pregnancy
is only offered if a patient will undergo termination of pregnancy (98). Clark et al.
showed in their study that the decision of declining termination of pregnancy must be
supported once the patient has been adequately counselled and a multidisciplinary
team approach must be followed (99). Counselling for the patient to make an
informed decision about their pregnancy once a result of an abnormal invasive test is
given remains one of the most important aspects of antenatal care in the setting of
prenatal testing (24) .

67
4.8 RECORD KEEPING AND LOSS TO FOLLOW UP
Record keeping was probably the greatest flaw uncovered by this review. The
ultrasound department kept a very good record of the invasive prenatal tests
performed and the National Health Laboratory Service had only one patient where
the result of the invasive prenatal test was lost. The problem arises from the records
department where of the 97 patients who underwent invasive prenatal testing only 65
(67%) patient charts could be located. This led to only 67% of pregnancy outcomes
being known and several outcomes of babies where abnormalities were identified
were lost to follow up. Many pieces of vital information including gestational age at
booking and booking bloods could thus not be included in the study. It must be noted
that some of the patients might have been from other provinces and countries and
might have travelled home for further antenatal care and delivery, thus their data
would not have been available. Furthermore the ultrasound department does not
keep a duplicate record of all the ultrasounds performed for a patient as these
records are kept within the patient's chart. It can thus be seen if the patient's chart is
missing that this vital information pertaining to their ultrasound findings will also be
missing. It must be commended that most indications leading to invasive prenatal
testing as well as the most important findings at ultrasound were indicated in the
invasive prenatal procedure book.
4.9 INVASIVE PRENATAL TESTING SERVICE
It is difficult to ascertain whether this service is adequately provided to the patient
population that Rahima Moosa Mother and Child Hospital serves as not all patients
who deliver at the hospital attend the hospital's antenatal clinic. There were 29380
deliveries during the study period but only 97 invasive procedures were done.
Because not all of these patient underwent antenatal care at the institution it is
difficult to deduce whether the number of invasive prenatal tests is reasonable for the
number of deliveries done.
Of the 2334 advanced maternal age women who attended Rahima Moosa Mother
and Child hospital's antenatal clinic only 58 (2,5%) underwent invasive prenatal
testing. This finding is very concerning and may be due to patients not being
counselled and referred appropriately to have invasive prenatal testing. This may be

68
due to lack of primary healthcare clinics referring patients of advanced maternal age,
late booking of patients thus missing the opportunity of genetic counselling and
prenatal testing and lack of knowledge and education by healthcare professionals in
the primary and academic settings for the need of prenatal testing. This finding is
similar to the that of Watchman et al. where it was shown that patients were not
being offered invasive prenatal testing although the service is available. They mainly
found that it was a lack of referral by primary healthcare clinics to academic
institutions and lack of academic institutions acting on referrals in a timely manner
that lead to advanced maternal age women not being offered genetic counselling
and invasive prenatal testing (40).
Another factor that has to be taken into consideration is the increasing amount of
medico-legal issues that surround pregnancy and prenatal screening. It is thus of
great importance to have such a service in the public sector and to increase its
capacity. Although the ACOG recommend that all women should have the option of
invasive testing, regardless of maternal age (24), this is not feasible in a resource
restricted setting as RMMCH.
4.10 LIMITATIONS
The small sample size of 97 patients is limiting in that it is a small number from which
important rates such as spontaneous miscarriage rate need to be worked out. This
number is further compounded by the loss to follow up of patients due to poor record
keeping. There were 32 patients (33%) lost to follow up due to files being lost or
patients delivering elsewhere and vital data thus being lost. This may lead to an
under or overestimation of various results including the complication rate.
An example of the above discussion is the abortion rate of 1,5%, this is possibly an
overestimation looking at the 33% loss to follow up rate.
The results in terms of rates of abnormalities are not generlisable to the entire
antenatal population, due to the afore-mentioned selection bias of higher risk
individuals.

69
4.11 RECOMMENDATIONS
Late booking of patients decreases the rate of early detection of abnormalities on
sonar and referral for other indications for invasive prenatal testing thus decreasing
the use of CVS which is the first choice for first trimester invasive prenatal testing. It
also limits the adequate use of genetic counselling services to prepare patients for
invasive prenatal testing and the possible diagnosis of an aneuploidy in the fetus.
Education on referral of high risk patients and referral protocols must be put in place.
Emphasis must also be placed on early referral of patients at risk of chromosomal
abnormalities as this will allow time for first trimester ultrasound, planning of invasive
prenatal testing and adequate genetic counselling. Better orientation of staff at all
levels to services like antenatal ultrasound, genetic counselling clinic and invasive
prenatal testing being available is needed.
As previously discussed patients of advanced maternal age are not adequately
referred for risk assessment and counselling regarding the option of invasive testing
at Rahima Moosa Mother and Child Hospital. Further education is needed on the
indications for invasive testing and that invasive prenatal testing does not only test
for common Trisomies. Indications like families affected by previous chromosomal
abnormalities must be highlighted.
Records should be kept of the patients undergoing invasive prenatal testing where
there is a copy of their patient chart with the outcome of their pregnancy within the
ultrasound department as this will ease the audit of the invasive prenatal testing
services in the future. It is also recommended that the ultrasound department keep a
separate record of all ultrasounds performed in the event that a patient's chart is lost.
Some of the outcomes of pregnancy were possibly not known in this cohort due to
patients delivering in other facilities, provinces and countries. The hand held
antenatal card goes with the patient wherever she undergoes antenatal care and
delivery. A digital system recording the patient's antenatal care and pregnancy
outcome which can be accessed nationally would greatly help the continuity of care
of patients.
It must be brought up at a provincial and national level that there are many
advances in fetal medicine. It would greatly benefit the pregnant population in the
public sector in South Africa if either combined first trimester screening by accredited

70
personnel or second trimester screening was made available to them. Currently
screening is opportunistic and not universal due to the inequitable distribution of
resources. Better referral systems and increasing capacitance at health facilities is
required as well as investment in skills training and equipment.
It is of great importance that HIV positive women undergoing invasive prenatal
testing be well informed about the risk of transmission, the woman should be on
antiretroviral therapy for an adequate duration and should be virally suppressed.
Viral load results must be known before the procedure is done.
Rhesus negative women must be given anti-D after their invasive prenatal
procedure, although there were six patients who were Rhesus negative and
underwent invasive prenatal testing there were no notes in their records of anti-D
being given.
4.12 CONCLUSION
The review of invasive prenatal testing at Rahima Moosa Mother and Child Hospital
is of value as it has highlighted several recommendations that will better the service
in the future.
There was a 12,5% rate of chromosomal abnormalities diagnosed with a
spontaneous miscarriage rate of 1,5%. This shows that the procedure is beneficial in
assisting the healthcare workers to better manage the patient and her pregnancy.
Both for those with an abnormal finding and reassuring those with normal results.
Although the miscarriage rate is higher than internationally quoted due to the small
sample size; it translates to only one spontaneous miscarriage occurring in the
cohort. The service appears safe in the hands of the Rahima Moosa Mother and
Child team. The most common indication for invasive prenatal testing was
abnormalities found at ultrasound followed by advanced maternal age. This
highlights that a good ultrasound service is available at the hospital. Also that
although advanced maternal age is a known risk factor for chromosomal
abnormalities it is seen as an independent risk factor and this needs further
education of healthcare professionals. Unfortunately there was a 33% loss to follow

71
up in the sample. This loss to follow up challenges the strength of any conclusions
that might be made by the study.
It can be argued that in a resource limited setting where malnutrition and infectious
disease play such a big role and take precedence, an invasive prenatal testing
service should not be at the forefront of the services. However it must be
remembered that the birth of a child with abnormalities can place tremendous burden
on an already impoverished family. Thus giving such a family a choice of knowing
prenatally of a child with abnormalities is vital..
Invasive prenatal testing remains the gold standard for conclusive prenatal diagnosis
and it decreases the burden of disease to the affected individual and their family. As
well as giving new parents time to prepare for the birth of their infant. The study
shows that an invasive testing service can be successfully run in a resource
restricted setting but ongoing education of the availability of the service in the public
sector is needed. It is important to better the services provided in the government
sector to match the international progression in fetal medicine and invasive prenatal
diagnosis as all our patients deserve optimal care during their pregnancies for their
unborn infants.

72
APPENDIX A
Data collection sheet
Study number:___________
Baseline information
Age:___________Ethnicity:____________
Parity:_________Gravidity:____________
Chronic illnesses:
Diabetes Hypertension Epilepsy Cardiac
disease
TB Thyroid
Disease
Other
Medication use:
Yes No Unknown If yes, type of medication:
Smoking :
Yes No Unknown
Alcohol use:
Yes No Unknown
Illicit drug use:
Yes No If yes, type of drug:
Current pregnancy: (pregnancy in which amniocentesis was done)
Rh:______(antibodies if negative:_______RPR:__________Hb:__________
RVD:________CD4:_______VL:_______Treatment:______________Duration:____
_________
Gestational age at booking:____________

73
Previous pregnancies:
Previous pregnancy outcomes:
YEAR MODE GA AT
DELIVERY
SEX LIVE BIRTH,
STILLBIRTH,
MISCARRIAGE
OR TOP
COMPLICATIONS
Previous diagnosis of chromosomal or structural abnormalities:
YEAR DIAGOSIS
Family History of chromosomal, genetic or structural abnormalities:
Yes No Unknown/not
recorded
If yes, type of abnormality:
Ultrasound findings:
Gestation at first ultrasound :__________
Singleton/Multiple gestation

74
Type of ultrasound:
DATING NT FETAL
ANOMALY
REVIEW
SCAN
Detail of scans:
Gestation at ultrasound:_________________________
Details of
findings:____________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
________
Gestation at ultrasound:_________________________
Details of
findings:____________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
________
Gestation at ultrasound:_________________________
Details of
findings:____________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
________
Did ultrasound finding prompt prenatal invasive test:
Yes No If yes, details of findings:

75
Invasive prenatal test:
Chorionic villous sampling Amniocentesis Cordocentesis
Gestation:________
Indication:
Advanced
maternal age
Abnormal
ultrasound
finding
Family History Maternal
request
Karyotype result:
Complications related to procedure:
Misciarriage Amniotic
fluid
leak
Preterm
labour
infection Other
Pregnancy outcome:
Misciarriage:
Yes No If yes, gestation

76
TOP:
Yes No If yes, gestation and reason
At Birth
Date Mode Weight Sex Gestational
age
Apgars Complications
If abnormalities detected at birth, genetic follow
up:_______________________________________

77
APPENDIX B
Approval letter from the University of the Witwatersrand Human Resources
Ethics Committee

78
APPENDIX C
Turnitin Report

79
REFERENCES
1. Alfirevic Z, Sundberg K, Brigham S. Amniocentesis and chorionic villus
sampling for prenatal diagnosis. Cochrane Database Syst Rev. 2003
(1):CD003252. Available: http://www.thecochranelibrary.com [Accessed
21.08. 2016]
2. American College of Obstetricians and Gynaecologists. Committee Opinion
No. 640: Cell-Free DNA Screening For Fetal Aneuploidy. Obstet Gynecol.
2015;126(3):e31-7. doi: 10.1097/AOG.0000000000001051 [Accessed
22.10.2016]
3. Chordirker BN, Cadrin C, Davies G, Summer AM, Wilson RD., Winsor EJ , et
al. The Society of Obstetricians & Gynaecologists of Canada. Clinical Practise
Guideline no. 168 : Techniques for prenatal diagnosis. J Obstet Gynecol Can.
2005; 27(11):1048–54. Available: http://www.jogc.com/article/S1701-
2163(16)30506-0/pdf [Accessed 22.10.2016]
4. Morris JK, Mutton DE, Alberman E. Revised estimates of the maternal age
specific live birth prevalence of Down’s syndrome. J Med Screen.,
2002;9(1):2–6.
5. Palomaki GE, Haddow JE, Beauregard LJ. Prenatal screening for Down’s
syndrome in Maine, 1980 to 1993. N Engl J Med. 1996;334(21):1409–10.
Available: http://www.nejm.org/doi/abs/10.1056/NEJM199605233342117
[Accessed 21.08.2016]
6. Norwits ER, Levy B. Noninvasive prenatal testing: the future is now. Rev
Obstet Gynecol,. 2013;6(2):48–62.
7. Nicolaides KH. Screening for chromosomal defects. Ultrasound Obstet
Gynecol. 2003;21(4):313–21. Available: http://doi.wiley.com/10.1002/uog.128
[Accessed 20.08.2016]
8. Wald NJ, Watt HC, Hackshaw AK. Integrated screening for Down’s syndrome
on the basis of tests performed during the first and second trimesters. N Engl
J Med. 1999;341(7):461–7. Available:
http://www.ncbi.nlm.nih.gov/pubmed/10441601 [Accessed 20.08.2016]
9. Nicolaides KH, Snijders RJM, (editors). Assessment of risks. In: Ultrasound
Markers for Fetal Chromosomal Defects. Carnforth: Parthenon Publishing,
1996, pp. 63–120.
80
10. Nicolaides KH. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat
Diagn. 2011;31:7–15. Available: http://doi.wiley.com/10.1002/pd.2637
[Accessed 18.09.2016]
11. Palomaki GE, Knight GJ, Ashwood ER, Best RG, Haddow JE. Screening for
Down Syndrome in the United States: Results of Surveys in 2011 and 2012.
Arch Pathol Lab Med. 2013;137(7):921–6. Available:
http://www.archivesofpathology.org/doi/abs/10.5858/arpa.2012-0319-CP
[Accessed 21.08.2016]
12. Smith-Bindman R, Hosmer W, Feldstein VA, Deeks JJ, Goldberg JD. Second-
trimester ultrasound to detect fetuses with Down syndrome: a meta-analysis.
J Am Med Ass. 2001;285(8):1044–55. Available:
http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.285.8.1044
[Accessed 18.09.2016]
13. Van den Hof MC, Wilson RD. Fetal soft markers in obstetric ultrasound. J
Obstet Gynecol Can. 2005;27(6):592–636. Available:
http://www.ncbi.nlm.nih.gov/pubmed/16100637 [Accessed 18.09.2016]
14. Tabor A, Alfirevic Z. Update on procedure-related risks for prenatal diagnosis
techniques. Fetal Diag and Ther 2010;27(1):1–7. Available:
http://www.karger.com/doi/10.1159/000271995 [Accessed 21.08.2016]
15. Naidoo P, Erasmus I, Jeebodh J, Nicolau E, Van Gelderen EJ. Nuchal
translucency as a method of first-semester screening for aneuploidy. S Afr J
Obstet Gynecol. 2008;14(1):38–42. Available:
https://www.scopus.com/inward/record.url?eid=2-s2.0-
44649151042&partnerID=40&md5=724937c1387e53bbc55bc192478197f2
[Accessed 18.09.2016]
16. Wilson RD, Gagnon A, Audibert F, Campagnolo C, Carrol J. Prenatal
Diagnosis Procedures and Techniques to Obtain a Diagnostic Fetal Specimen
or Tissue: Maternal and Fetal Risks and Benefits. J Obstet Gynecol Can.
2015;37(7):656–68. Available:
http://linkinghub.elsevier.com/retrieve/pii/S170121631530205X [Accessed
21.08.2016]

81
17. American College of Obstetricians and Gynecologists. Committee Opinion No.
545: Noninvasive prenatal testing for fetal aneuploidy. Obstet Gynecol.
2012;120(6):1532–4. doi: 10.1097/01.AOG.0000423819.85283.f4. [Accessed
22.10.2016]
18. Norton ME, Jacobsson B, Swamy GK, Laurent LC, Ranzini AC, Brar H, et al.
Cell-free DNA analysis for noninvasive examination of trisomy. N Engl J Med.
2015;372(17):1589–97. Available:
http://www.ncbi.nlm.nih.gov/pubmed/25830321 [Accessed 22.10.2016]
19. Urban M, Morris S, Schoeman M, Norman K. Appropriate clinical use of non-
invasive prenatal testing in South Africa. Obstet Gynecol Forum
2014;24(1):35–40. Available:
http://academic.sun.ac.za/Health/Media_Review/2014/17Mar14/files/Appropri
ate.pdf [Accessed 21.08.2016]
20. Gratacós E, Nicolaides K. Clinical perspective of cell-free DNA testing for fetal
aneuploidies. Fetal Diag and Ther. 2014;35(3):151-5.
21. Gil MM, Giunta G, Macalli EA, Poon LC, Nicolaides KH. UK NHS pilot study
on cell‐free DNA testing in screening for fetal trisomies: factors affecting
uptake. Ultrasound Obstet Gynecol. 2015;45(1):67-73.
22. Langlois S, Brock JA, Wilson RD, Audibert F, Carroll J, Cartier L, et al.
Current Status in Non-Invasive Prenatal Detection of Down Syndrome,
Trisomy 18, and Trisomy 13 Using Cell-Free DNA in Maternal Plasma. J
Obstet Gynecol Can. 2013;35(2):177–81. Available from:
http://linkinghub.elsevier.com/retrieve/pii/S1701216315310252 [Accessed
21.08.2016]
23. Royal College of Obstetricians and Gynaecologists. Amniocentesis and
Chorionic Villus Sampling. R Coll Obstet Gynecol. RCOG Green 2010; (8):1–
13. Available:
https://www.rcog.org.uk/globalassets/documents/guidelines/gt8amniocentesis
0111.pdf [Accessed 21.08.2016]
24. American College of Obstetricians and Gynaecologists. Practice Bulletin No.
88: Invasive prenatal testing for aneuploidy. Obstet Gynecol.
2007;110(6):1459–67. Available:
http://www.ncbi.nlm.nih.gov/pubmed/18055749 [21.08.2016]
25. Daniilidis A, Karydas H, Zournatzi V, Tantanasis T, Giannoulis C, Tzafettas J.

82
A four-year retrospective study of amniocentesis: One centre experience.
Hippokratia 2008;12(2):113–5. Available:
http://www.hippokratia.gr/index.php/hippo/article/view/601/304 [Accessed
20.08.2016]
26. Steele M, Breg W. Chromosome analysis of human amniotic-fluid cells.
Lancet. 1966;1(4):383–5. Available from:
http://www.jpedsurg.org/article/0022-3468(66)90346-0/abstract [Accessed
21.08.2016]
27. Tabor A, Madsen M, Obel EB, Philip J, Bang J, Gaard-Pedersen B.
Randomised controlled trial of genetic amniocentesis in 4606 low- risk
women. Lancet 1986;327(8493):1287–92. Available from:
http://www.sciencedirect.com/science/article/pii/S0140673686912183
[Accessed 21.08.2016]
28. Crandon AJ, Peel KR. Amniocentesis with and without ultrasound guidance.
An Int J Obstet. 1979;86(1):1,6-9. Available:
http://onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.1979.tb10673.x/ful
[Accessed 21.08.2016]
29. Müngen E, Tütüncü L, Muhcu M, Yergok YZ. Pregnancy outcome following
second-trimester amniocentesis: A case-control study. Am J Perinatol.
2006;23(1):25–30. Available: https://www.thieme-
connect.com/products/ejournals/html/10.1055/s-2005-923432 [Accessed
21.08.2016]
30. Ledbetter DH, Martin AO, Verlinsky Y, Pergament E, Jackson L, Yang-Feng,
et al. Cytogenetic results of chorionic villus sampling - High success rate and
diagnostic accuracy in the United States collaborative study. Am J Obstet
Gynecol. 1990;162(2):495–501. Available:
http://www.sciencedirect.com/science/article/pii/0002937890904198
[Accessed 21.08.2016]
31. Tongsong T, Wanapirak C, Kunavikatikul C, Sirirchotiquakul S, Piyamongkol
W, Chanprapaph P. Cordocentesis at 16-24 weeks of gestation: Experience
of 1320 cases. Prenat Diagn. 2000;20(3):224–8. Available from:
http://onlinelibrary.wiley.com/doi/10.1002/(SICI)1097-
0223(200003)20:3%3C224::AID-PD788%3E3.0.CO;2-M/full [Accessed
21.08.2016]

83
32. Pala HG. Cordocentesis outcomes of tertiary care services in Manisa city: a
retrospective analysis of four years. Perinat J., 2014;22(2):79–82. Available:
http://www.perinataldergi.com/Archive/Article/20140222004 [Accessed
21.08.2016]
33. Chang YW, Chang CM, Sung PL, Yang MJ, Li WH, Li HY, et al. An overview
of a 30-year experience with amniocentesis in a single tertiary medical center
in Taiwan. Taiwan J Obstet Gynecol. 2012;51(2):206–11. Available:
http://www.sciencedirect.com/science/article/pii/S1028455912000630
[Accessed 19.08.2016
34. Cho JS, Park YW, Kim SK, Kim IK, Yang YH, Kwon HK, et al. Prenatal
Genetic Diagnosis in 2000 Amniocenteses. Korean J Obstet Gynecol.,
1999;42(1):65–71
35. Kim HJ, Lee SM, Kim EJ Cho EN, Park SY, Kang KH, et al. A review of
prenatal cytogenetic analysis in 2942 midtrimester amniocentesis. Korean J
Obstet and Gynecol., 2001;44(6):1109-14.
36. Pala H, Ulkumen B, Eskicioglu F, Ulucay S, Cam S, Bayture YB, et al.
Amniocentesis results of Manisa tertiary care in 2012. Perinat J.,
2014;22(1):23–7.
37. Johnson JA, Tough S. Delayed Child-Bearing. J Obstet Gynecol Can.
2012;34(271):80–93. Available: http://dx.doi.org/10.1016/S1701-
2163(16)35138-6 [Accessed 20.08.2016]
38. Mills TA, Lavender T. Advanced maternal age. Obstet Gynecol Reprod Med.
2011;21(4):107–11. Available:
http://www.sciencedirect.com/science/article/pii/S1751721410002204
[Accessed 20.08.2016]
39. Cleary-Goldman J, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock
CH, et al. Impact of maternal age on obstetric outcome. Obstet Gynecol.,
2005;105(5):983–90.
40. Watcham SJ, Schön S, Christianson AL. Neglect in the care of pregnant
South African women of advanced maternal age. S Afr Med J.
2007;97(11):1067–9. Available: http://www.samj.org.za [Accessed
21.08.2016]
41. Kuliev A, Cieslak J, Ilkevitch Y, Verlinsky Y. Chromosomal abnormalities in a
series of 6733 human oocytes in preimplantation diagnosis for age-related

84
aneuploidies. Reprod Biomed Online 2003;6(1):54–9. Available:
http://linkinghub.elsevier.com/retrieve/pii/S147264831062055X [Accessed
20.08.2016]
42. Battaglia DE, Goodwin P, Klein NA, Soules MR. Influence of maternal age on
meiotic spindle assembly in oocytes from naturally cycling women. Hum
Reprod. 1996;11(10):2217–22. Available:
http://www.ncbi.nlm.nih.gov/pubmed/8943533 [Accessed 22.10.2016]
43. Hook EB, Cross PK, Schreinemachers DM. Chromosomal Abnormality Rates
at Amniocentesis and in Live-Born Infants. J Am Med Ass 1983;249(15):2034.
Available:
http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.1983.033303900
38028 [Accessed 20.08.2016]
44. Marthin JA, Hamiltion BE, Ventura SJ, Menacker F, Park MM, Sutton PD.
Births: final data for 2001. Natl Vital Stat. 2002;51(2):1–102. Available:
http://www.ncbi.nlm.nih.gov/pubmed/12596439 [Accessed 19.08.2016]
45. Hunter AG, Thompson D, Speevak M. Midtrimester genetic amniocentesis in
eastern Ontario: a review from 1970 to 1985. J Med Genet. 1987;24(6):335–
43. Available: http://jmg.bmj.com/cgi/doi/10.1136/jmg.24.6.335 [Accessed
20.08.2016]
46. Statistics South Africa. 2013. Recorded live births 2013. Available:
http://www.statssa.gov.za/publications/P0305/P03052013.pdf [Accessed
21.08.2016]
47. Kromberg JG, Christianson AL, Duthie-Nurse G, Zwane E, Jenkins T. Down
syndrome in the black population. S Afr Med J. 1992;81(6):337. Available:
http://www.ncbi.nlm.nih.gov/pubmed/1533293 [Accessed 20.08.2016]
48. Delport SD, Christianson AL, Van den Berg HV, Wolmarans L, Gericke GS.
Congenital anomalies in black South African liveborn neonates at an urban
academic hospital. S Afr Med J., 1995;85(1):11–5.
49. Venter PA, Christianson AL, Hutamo CM, Makhura MP, Gericke GS.
Congenital anomalies in rural black South African neonates--a silent
epidemic? S Afr Med J. 1995;85(1):15–20. Available :
http://www.ncbi.nlm.nih.gov/pubmed/7784908 [Accessed 20.08.2016]
50. Christianson AL. Down syndrome in sub-Saharan Africa. J Med Genet.
1996;33(2):89–92. Available:

85
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1051830/ [Accessed
20.08.2016]
51. South African Medical Research Council. 2012. Under-5 Mortality Statistics in
South-Africa: Shedding some light on the trend and causes. Available:
http://www.mrc.co.za/bod/MortalityStatisticsSA.pdf [Accessed 21.08.2016]
52. South Africa. Dept. of Health. 2014. Ninth Report on perinatal care in South
Africa. Available: http://www.ppip.co.za/wp-content/uploads/Saving-Babies-
2012-2013.pdf [Accessed 15.07.2016]
53. Reid AE, Hendricks MK, Groenewald P, Bradshaw D. Where do children die
and what are the causes? Under-5 deaths in the Metro West geographical
service area of the Western Cape, South Africa, 2011. S Afr Med J.
2016;106(4):359. Available:
http://www.samj.org.za/index.php/samj/article/view/10521[Accessed
22.10.2016]
54. Grether-González P, Cámara-Polanco V, Ulloa-Avilés V, Salas-Labadia C,
Amanza-Marquez R, Kogan-Frenk S, et al. Prenatal diagnosis by
amniocentesis: Clinical and cytogenetic experience in 1500 cases. Ginecol
Obstet Mex., 2010;78(9):493–503.
55. Hsieh FJ, Ko TM, Tseng LH, Chang LS, Pan MF, Chuang SM, et al. Prenatal
cytogenetic diagnosis in amniocentesis. J Formos Med Assoc.,
1992;91(3):276–82.
56. Han SH, An JW, Jeong GY, Yoon HR, Lee A, Yang YH, et al. Clinical and
cytogenetic findings on 31,615 mid-trimester amniocenteses. Korean J Lab
Med., 2008;28(5):378-85. Available:
http://synapse.koreamed.org/DOIx.php?id=10.3343%2Fkjlm.2008.28.5.378
[Accessed 21.08.2016]
57. Tseng JJ, Chou MM, Lo FC, Lai Hy, Chen MH, Ho ES. Detection of
chromosome aberrations in the second trimester using genetic amniocentesis:
experience during 1995-2004. Taiwan J of Obstet Gynecol., 2006;45(1):39-
41.
58. Wulff CB, Gerds TA, Rode L, Ekelund CK, Peterson OB, Tabor A. Risk of fetal
loss associated with invasive testing following combined first-trimester
screening for Down syndrome: A national cohort of 147 987 singleton
pregnancies. Ultrasound Obstet Gynecol. 2016;47(1):38–44.

86
59. Toriello HV, Meck JM. Statement on guidance for genetic counseling in
advanced paternal age. Genet Med. 2008;10(6):457–60. Available:
http://www.ncbi.nlm.nih.gov/pubmed/18496227 [Accessed 21.08.2016]
60. Nussbaum R, McInnes R, Willard H. Principles of clinical cytogenetics and
genome analysis. In: Thompson & Thompson genetics in medicine. Elsevier
Health sciences, 2016, pp. 57–74. Available:
https://books.google.co.za/books?hl=en&lr=&id=4yV1CQAAQBAJ&oi=fnd&pg
=PP1&dq=Principles+of+clinical+cytogenetics+and+genome+analysis+nussb
aum&ots=3LODnFytDB&sig=GI0TkgQZ7ucQtDw483WVPHYKlAk [Accessed
21.08.2016]
61. Bovicelli L, Orsini LF, Rizzo N, Montacuti V, Bachetta M. Reproduction in
Down syndrome. Obstet Gynecol. 1982;59(6):13S–7S. Available:
http://journals.lww.com/greenjournal/Abstract/1982/06001/Reproduction_in_D
own_Syndrome.4.aspx [Accessed 21.08.2016]
62. Warburton D, Dallaire L, Thangavelu M , Ross L, Levin B, Kline J. Trisomy
recurrence: a reconsideration based on North American data. Am J Hum
Genet. 2004;75(3):376–85. Available:
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1182017&tool=pmc
entrez&rendertype=abstract [Accessed 21.08.2016]
63. Uehara S, Yaegashi N, Maeda T, Hoshi N, Fujimoto S, Fujimori K, et al. Risk
of recurrence of fetal chromosomal aberrations: analysis of trisomy 21,
trisomy 18, trisomy 13, and 45,X in 1,076 Japanese mothers. J Obstet
Gynecol Res. 1999;25(6):373–9. Available from:
http://doi.wiley.com/10.1111/j.1447-0756.1999.tb01180.x [Accessed
21.08.2016]
64. Jackson LG, Zachary JM, Fowler SE, Desnick RJ, Golcus MS, Ledbeter DH,
et al. The U.S. National Institute of Child Health and Human Development
Chorionic-Villus Sampling and Amniocentesis Study Group. A randomized
comparison of transcervical and transabdominal chorionic-villus sampling. N
Engl J Med. 1992;327(9):594–8. Available:
http://www.nejm.org/doi/abs/10.1056/NEJM199208273270903 [Accessed
21.08.2016]

87
65. Nicolini U, Lalatta F, Natacci F, Crucio C. The introduction of QF-PCR in
prenatal diagnosis of fetal aneuploidies: Time for reconsideration. Hum
Reprod Update., 2004;10(6):541–8.
66. Test and Technology Transfer Committee. Technical and clinical assessment
of fluorescence in situ hybridization: An ACMG/ASHG position statement:
Technical considerations. Genet Med. 2000;2(6):356–61. Available:
http://www.ncbi.nlm.nih.gov/pubmed/11339659 [Accessed 21.08.2016]
67. Wapner RJ, Martin CL, Levy B, Ballif BC, Eng CM, Zachary JM, et al.
Chromosomal microarray versus karyotyping for prenatal diagnosis. N Engl J
Med. 2012;367(23):2175–84. Available:
http://www.nejm.org/doi/abs/10.1056/NEJMoa1203382 [Accessed
21.08.2016]
68. De Wit MC, Srebniak MI, Govaerts LCP, Van Opstal D, Galjaard R, Go A.
Additional value of prenatal genomic array testing in fetuses with isolated
structural ultrasound abnormalities and a normal karyotype: A systematic
review of the literature. Ultrasound Obstet Gynecol. 2014;43(2):139–46.
Available from: http://onlinelibrary.wiley.com/doi/10.1002/uog.12575/full
[Accessed 21.08.2016]
69. Tabor A, Vestergaard CHF, Lidegaard O. Fetal loss rate after chorionic villus
sampling and amniocentesis: an 11-year national registry study. Ultrasound
Obstet Gynecol. 2009;34(1):19–24. Available from:
http://doi.wiley.com/10.1002/uog.6377. [Accessed 21.08.2016]
70. Wilson RD, Johnson JM, Dansereau J, Singer J, Drinnen SL, Winsor EJT, et
al. Randomised trial to assess safety and fetal outcome of early and
midtrimester amniocentesis. Lancet, 1998;351(9098):242–7.
71. Smidt-Jensen S, Philip J, Lundsteen C, Permin M, Zachary JM, Fowler SE.
Randomised comparison of amniocentesis and transabdominal and
transcervical chorionic villus sampling. Lancet 1992;340(8830):1237–44.
Available: http://linkinghub.elsevier.com/retrieve/pii/014067369292946D
[Accessed 21.08.2016]
72. Eller AG, Branch DW, Byrne JLB. Stillbirth at Term. Obstet Gynecol.,
2006;108:442–7.
73. Wilson D, Farquharson DF, Wittmann BK, Shaw D. Cordocentesis: Overall
Pregnancy Loss Rate as Important as Procedure Loss Rate. Fetal Diagn

88
Ther. 1994;9(3):142–8. Available from:
http://www.karger.com/doi/10.1159/000263922 [Accessed 22.10.2016]
74. Simpson JL. 2012. Invasive procedures for prenatal diagnosis: Any future
left? Best Practice and Research: Clin Obstet Gynecol., 2012. p. 26(5):625–
38.
75. Cederholm M, Haglund B, Axelsson O. Infant morbidity following
amniocentesis and chorionic villus sampling for prenatal karyotyping. BJOG:
An Int J Obstet Gynecol. 2005;112(4):394–402. Available:
http://doi.wiley.com/10.1111/j.1471-0528.2005.00413.x [Accessed
21.08.2016]
76. Bombard AT, Powers JF, Carter S, Schwartz A, Nitowsky HM. Procedure-
related fetal losses in transplacental versus nontransplacental genetic
amniocentesis. Am J Obstet Gynecol. 1995;172(3):868–72. Available:
http://linkinghub.elsevier.com/retrieve/pii/0002937895900136 [Accessed
21.08.2016]
77. Borgida AF, Mills AA, Feldman DM, Rodis JF, Egan JF. Outcome of
pregnancies complicated by ruptured membranes after genetic
amniocentesis. Am J Obstet Gynecol. 2000;183(4):937–9. Available:
http://linkinghub.elsevier.com/retrieve/pii/S0002937800962161 [Accessed
21.08.2016]
78. Strauss A, Hasbargen U, Paek B, Baerfeind I, Hepp H. Fetal demise caused
by amniotic band syndrome after standard amniocentesis. Fetal Diag Ther.,
2000;15(1):4-7.
79. Hislop AFD. Amniocentesis and lung growth: an animal experiment with
clinical implications. Lancet, 1982;320(8310):1271–2.
80. Benn PA, Hsu LYF. Prenatal diagnosis of chromosomal abnormalities through
chorion villus sampling and amniocentesis. In: Genetic disorders and the
fetus: diagnosis, prevention, and treatment. Baltimore: Johns Hopkins
University Press, 2004, pp. 214-296.
81. Firth H V., Boyd PA, Lindenbaum RH, Huson SM, Chamberlain P, Mackenzi
IZ. Severe limb abnormalities after chorion villus sampling at 56-66 days’
gestation. Lancet 1991;337(8744):762–3. Available:
http://linkinghub.elsevier.com/retrieve/pii/0140673691913744 [Accessed
21.08.2016]

89
82. Froster U. Jackson L. Limb defects and chorionic villus sampling: results from
an international registry, 1992-94. Lancet 1996;347(9000):489–94. Available f:
http://linkinghub.elsevier.com/retrieve/pii/S0140673696911368
83. Grobman WA, Auger M, Shulman LP, Elias S. The association between
chorionic villus sampling and preeclampsia. Prenat Diagn. 2009;29(8):800-3.
Available: http://onlinelibrary.wiley.com/doi/10.1002/pd.2296/full [Accessed
23.08.2016]
84. Grati FR, Malvestiti F, Ferreira JC, Bajaj K, Gaetani E, Agrati C, et al.
Fetoplacental mosaicism: potential implications for false-positive and false-
negative noninvasive prenatal screening results. Genet Med Off J Am Coll
Med Genet. 2014;16(8):1–5. Available:
http://www.ncbi.nlm.nih.gov/pubmed/24525917 [Accessed 22.10.2016]
85. Mardy A, Wapner RJ. Confined placental mosaicism and its impact on
confirmation of NIPT results. Am J Med Gen., 2016;172:118–22.
86. Hill J, Sheffield J, Kim JE. Risk of hepatitis B transmission in breast-fed
infants of chronic hepatitis B carriers. Obtet Gynecol. 2002;99:1049–52.
Available: http://www.hindawi.com/journals/idog/1999/159262/abs/ [Accessed
23.08.2016]
87. Yi W, Pan CQ, Hao J, Hu Y, Liu M, Li L, et al. Risk of vertical transmission of
hepatitis B after amniocentesis in HBs antigen-positive mothers. J Hepatol.,
2014;60(3):523–9.
88. Delamare C, Carbonne B, Heim N, Berkane N, Petit JC, Uzan S, et al.
Detection of hepatitis C virus RNA (HCV RNA) in amniotic fluid: a prospective
study. J Hepatol., 1999;31(3):416–20.
89. Somigliana E, Bucceri AM, Tibaldi C, Alberico S, Ravizza M, Savasi V, et al.
Early invasive diagnostic techniques in pregnant women who are infected with
the HIV: A multicenter case series. Am J Obstet Gynecol., 2005;193(2):437–
42.
90. Mandelbrot L, Jasseron C, Ekoukou D, Batallan A, Bongain A, Pannier E, et
al. ANRS French Perinatal Cohort. Amniocentesis and mother-to-child human
immunodeficiency virus transmission in the Agence Nationale de Recherches
sur le SIDA et les Hépatites Virales French Perinatal Cohort. Am J Obstet and
Gynecol. 2009;200(2):160-e1-160e9 Available:
http://www.ajog.org/article/S0002-9378(08)00985-X/abstract [Accessed

90
19.08.2016]
91. Ekoukou D, Khuong-Josses MA, Ghibaudo N, Mechali D, Rotten D.
Amniocentesis in pregnant HIV-infected patients. Absence of mother-to-child
viral transmission in a series of selected patients. Eur J Obstet Gynecol
Reprod Biol., 2008;140(2):212–7.
92. Floridia M, Masuelli G, Meloni A, Cetin I, Tamburrini E, Cavaliere AF, et al.
Amniocentesis and chorionic villus sampling in HIV‐infected pregnant women:
a multicentre case series. BJOG: An Int J Obstet Gynecol. 2016.
93. Royal College of Obstetricians and Gynaecologists. Management of HIV in
Pregnancy. Green-top Guideline No. 39. London, 2010. Available:
http://www.rcog.org.uk/womens-health/clinical-guidance/management-hiv-
pregnancy-green-top-39 [Accessed 21.11.16]
94. Constantatos SN, Boutall AH, Stewart CJ. Recommendations for
amniocentesis in HIV-positive women. S Afr Med J. 2014;104(12):844–5.
Available: http://www.samj.org.za/index.php/samj/article/view/8660 [Accessed
18.09.2016]
95. South Africa. Dept. of Health. 2010.The 2013 National Antenatal Sentinel
Prevalence Survey South Africa. Available: https://www.health-e.org.za/wp-
content/uploads/2016/03/Dept-Health-HIV-High-Res-7102015.pdf [Accessed
20.11.2016]
96. Mnyani CN, Nicolaou E, Bera E, Black V, Hull JC, McIntyre JA. Guideline on
invasive obstetric procedures in the HIV-infected pregnant woman. S Afr Med
J., 2012;18(1):3-5. Available:
http://www.sajog.org.za/index.php/SAJOG/article/download/419/252%5Cnhttp
://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed10&NEWS=
N&AN=2012099981 [Accessed 23.11.2016]
97. López M, Coll O. Chronic viral infections and invasive procedures: risk of
vertical transmission and current recommendations. Fetal Diag Ther.
2010;28(1):1-8.
98. Cartier L, Murphy-Kaulbeck L. The Society of Obstetricians & Gynaecologists
of Canada.Counselling Considerations for Prenatal Genetic Screening
Committee Opinion. J Obstet Gynecol Can. 2012;277(5):489–93 Available:
http://www.sciencedirect.com/science/article/pii/S1701216316352483
[Accessed 21.11.2016]

91
99. Clark SL, DeVore GR. Prenatal diagnosis for couples who would not consider
abortion. Am J Obstet Gynecol., 1989 Jun;73(6):1035–7.
100. Eddleman KA, Malone FD, Sullivan L, Dukes K, Berkowitz RL,
Kharbutli Y, et al. Pregnancy loss rates after midtrimester amniocentesis.
Obstet Gynecol. 2006;108(5):1067–72.
101. Malherbe HL, Woods DL, Aldous C, Christianson AL. Review of the
2015 Guidelines for Maternity Care with relevance to congenital disorders. S
Afr Med J. 2016;106(7):669. Available:
http://www.samj.org.za/index.php/samj/article/view/10813 [Accessed
18.09.2016]
102. Myer L, Harrison A. Why do women seek antenatal care late?
Perspectives from rural South Africa. J Midwifery Women’s Heal.
2003;48(4):268–72.
103. American College of Obstetrics and Gynaecology. Impact of Maternal
Age on Obstetric Outcome. Obstet Gynecol. 2006;105(5):983–90.
104. Gruchy N, Vialard F, Decamp M, Choiset A, Rossi A, Le Meur N, et al.
Pregnancy outcomes in 188 French cases of prenatally diagnosed Klinefelter
syndrome. Hum Reprod. 2011;26(9):2570–5.