review on current technology hiv/aids care and control will mobile technology "do it"?...
TRANSCRIPT

HIV/AIDS care and control
Will Mobile Technology "Do It"?Review on current technology
Richard Lester, MD, FRCPCBCCDC / University of British Columbia
University of Nairobi, WelTelJuly 25, 2012

CREDIT: http://www.armybase.us/2009/04/air-force-yields-in-f-22-fighter-dispute/

Can mobile (communication) technologies “Do it”?

mHealth-Hype?Problem: People living with HIV Response: People on ART People with mobile phones
mPhones =A Gift

HIV Cascade of care
Prevention TestingAccess/
Linkage to care
Access to treatments
(supply chain)
Adherence Retention
HIV Care & Prevention
• = preventionAccess (Uptake)
• = preventionAdherence
• = preventionRetention
Access + Adherence +Retention =Engagement

Two Randomized Controlled Trials (Kenya)
March 27, 2011 Nov 27, 2010
WelTel weekly SMS check-ins (two way):*24% improvement in achieving 95% adherence over 1y*19% improvement in achieving viral suppression at 1y
(NNT = 9 & 11)
SMS reminders/motivation (one way):*Weekly (short) messages 32% improvement in 90% adherence (MEMS) over 1y*9% decrease in treatment interruptions*No adherence improvement with daily, longer reminders*No viral load/clinical outcomes
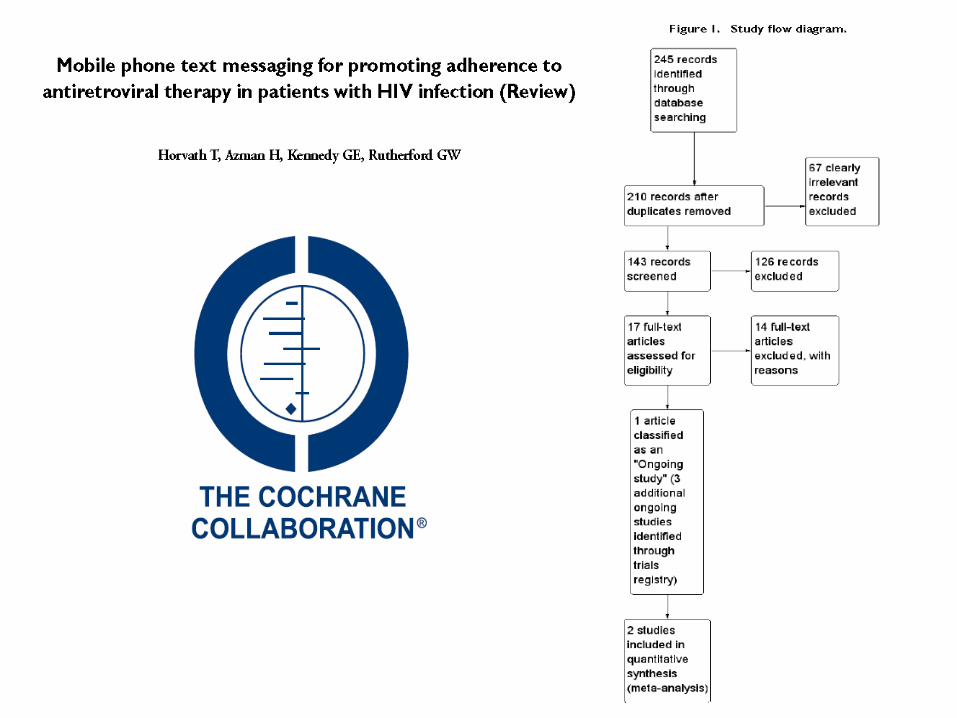

243 references ID’d to Nov 2011:

Bella Hwang – mHealth Summit 2011
WelTel: PEPFAR (2.485M people)
Cost of SMS Intervention
Total Cost Savings Net Savings
Breakdown: Costs Saved of 2nd Line therapy
Breakdown: Costs Saved of Opportunistic Infections
Breakdown: Costs Saved for Clinic Time Needed
Year 1 2,920,259$ 6,147,108$ 3,226,850$ 1,107,088$ 1,338,673$ 3,701,347$ Year 2 14,601,293$ 49,263,454$ 34,662,161$ 5,535,441$ 6,693,365$ 37,034,648$ Year 3 29,202,586$ 172,638,554$ 143,435,968$ 11,070,882$ 13,386,730$ 148,180,942$
Figure . Costs of SMS Intervention vs. Costs Savings over 3 years for PEPFAR Global Cohort on ART (2.485M patients)
+230,000 suppressed

What doesn’t work?
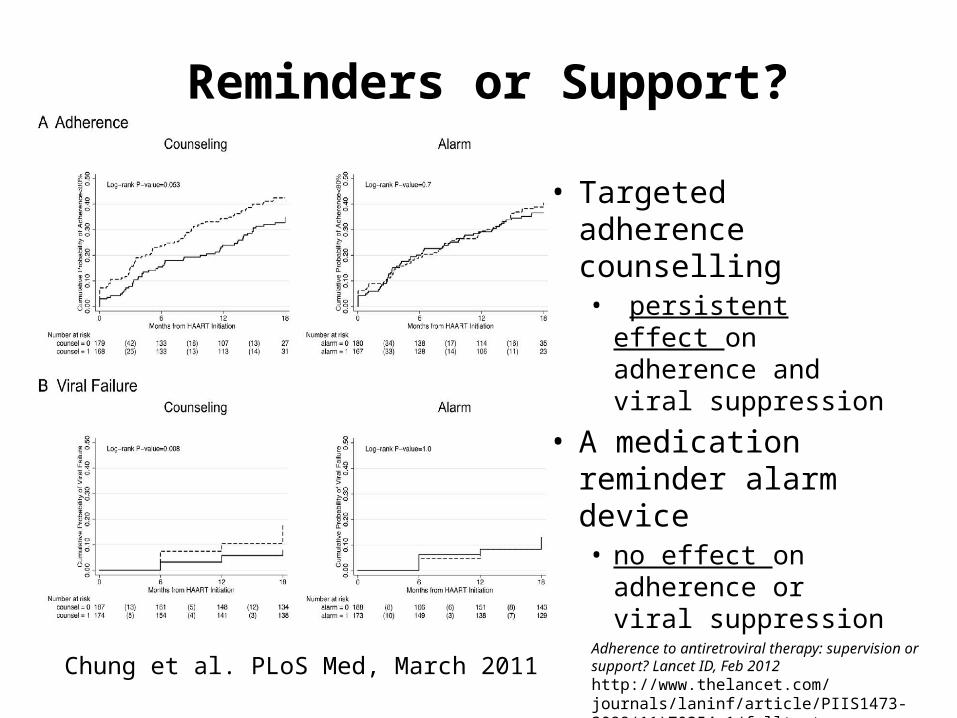
Reminders or Support?
• Targeted adherence counselling • persistent effect on
adherence and viral suppression
• A medication reminder alarm device • no effect on
adherence or viral suppression
Chung et al. PLoS Med, March 2011Adherence to antiretroviral therapy: supervision or support? Lancet ID, Feb 2012http://www.thelancet.com/journals/laninf/article/PIIS1473-3099(11)70354-1/fulltext

Monitoring Adherence & Results
Challenges in Using Mobile Phones for Collection of Antiretroviral Therapy Adherence Data in a Resource-Limited Setting
SMS and IVR Adherence Real Time Monitoring in Uganda
Jessica E. Haberer1, 2, 3 , Julius Kiwanuka4, Denis Nansera4, Ira B. Wilson5 and David R. Bangsberg2, 3, 6
• (1) Department of General Internal Medicine, Massachusetts General Hospital, Boston, MA, USA(2) Harvard Initiative for Global Health, Mbarara University of Science and Technology, Kampala, Uganda, online: 8 June 2010
High acceptability for cell phone text messages to improve communication of laboratory results with HIV-infected patients in rural Uganda: a crosssectional survey study.
• BMC Med Inform Decis Mak. 2012 Jun 21;12(1):56. [Epub ahead of print]• Siedner MJ, Haberer JE, Bwana MB, Ware NC, Bangsberg DR.


Other cell phone studiesAIDS Patient Care STDS. 2011 Mar;25(3):153-61. Epub 2011 Feb 16.Randomized controlled trial of a personalized cellular phone reminder system to enhance adherence
to antiretroviral therapy. N=19 adultsHardy H, Kumar V, Doros G, Farmer E, Drainoni ML, Rybin D, Myung D, Jackson J, Backman E, Stanic A, Skolnik
PR
Trials. 2011 Jun 9;12:145.The challenges and opportunities of conducting a clinical trial in a low resource setting: the case of the
Cameroon mobile phone SMS (CAMPS) trial, an investigator initiated trial. N=198 adultsMbuagbaw L, Thabane L, Ongolo-Zogo P, Lang T.
AIDS Patient Care STDS. 2011 May;25(5):303-10. Epub 2011 Apr 2.Brief behavioral self-regulation counseling for HIV treatment adherence delivered by cell phone: an initial
test of concept trial. N=40 adultsKalichman SC, Kalichman MO, Cherry C, Swetzes C, Amaral CM, White D, Jones M, Grebler T, Eaton L.
Lancet. 2011 Aug 27;378(9793):795-803. Epub 2011 Aug 3.The effect of mobile phone text-message reminders on Kenyan health workers' adherence to
malaria treatment guidelines: a cluster randomised trial. N=2269 childrenZurovac D, Sudoi RK, Akhwale WS, Ndiritu M, Hamer DH, Rowe AK, Snow RW.




“mobile phone HIV” publications
0tan28a5
66528
0tan29a5
66529
0tan30a5
66530
0tan1a5
66510tan28a566028
0tan4a56604
0tan9a56609
0tan14a566014
0tan19a566019
0tan24a566024
0tan29a566029
number (Pubmed)
number (Pubmed)
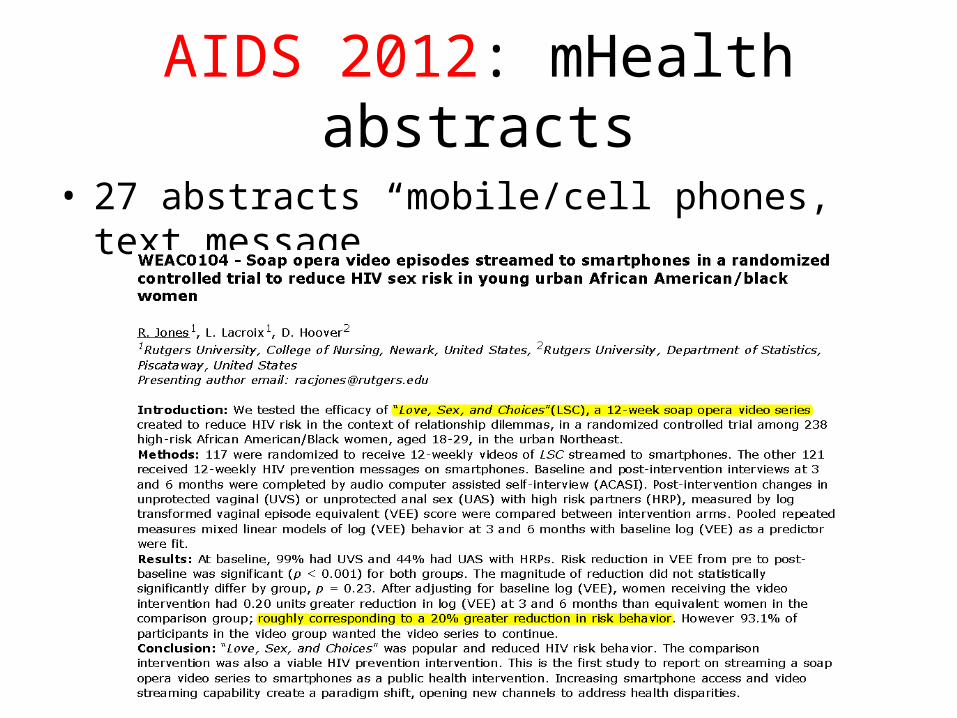
AIDS 2012: mHealth abstracts
• 27 abstracts “mobile/cell phones, text message”
AIDS 2012: RCT2
• TUPE673 - Poster Exhibition
SMS messaging improves treatment outcome among the HIV-positive Mayan population in rural Guatemala
» J.M. Ikeda1, R. Barrios2, J.B. Lopez Lopez3, N. Hearst4
– 226 HIV positive clients from the Integrated Care Clinic in Quetzaltenango
– The mean time to viral load suppression: 7 months intervention group and 10 months control group.

Summary of RCT Evidence on mHealth Interventions to improve ART outcomes
• Adherence monitoring by SMS? - ?– not yet known if effective for adherence promotion– Challenging to implement, cost, compliance, stigma?
• Targeted adherence counselling? - Y– improves adherence and viral suppression (1yr)
• Digital alarm reminders? - N– No improvement on adherence or VL (1yr)
• One way cell phone SMS reminders? – N/Y– no improvement in adherence (by MEMS), for daily reminders– effective with short weekly messages. (1yr)
• Two-way cell phone SMS çheck-ins’/access to HCW? -Y– Improves adherence and viral suppression (1yr)
• Level of Evidence: Grade A (weekly SMS)• Support (access to care) > Reminders?
My take home messages
• Keep it simple– Every extra step (complexity) loses someone
• Keep it low cost– Resource limited settings, vulnerable groups
• Conduct controlled studies– What really works, and what doesn’t?
• Seize the opportunity– mHealth is a gift

Can mobile (communication) technologies “Do it”?
Future Direction
Grand Challenges Canada• Formed a non-profit organization to
assist implementing the WelTel model
globally (WelTel International mHealth Society).
• PMTCT in Kenya– Supported by IDRC/GHRI
Current Research Projects:
• WelTel HAARTBC1– Oak Tree Clinic, Vancouver– Supported by BCCDC foundation
and Bristol-Myers-Squibb• WelTel LTBI
– BCCDC TB clinics, latent TB infection support (RCT)
– Supported by BCLA, CIHR• WelTel Retain
– Pre-ART retention in care with AMREF in Kenya
– Supported by NIMH
• EPIC– PrEP in San Francisco– Supported by NIMH

Thank you
Your health, in your handswww.weltel.org The future is now.