sash : cerebrovascular disease - stroke by dr georgina child
TRANSCRIPT
NY Desk calendar 2015
Cerebrovascular disease - Stroke
Georgina Child BVSc DACVIM (Neurology)
SASH North Ryde NSW


www.sashvets.com
Cerebrovascular disease (CVA)
• May be due to haemorrhage or infarction (most common)
• Clinical signs usually acute and non progressive
• Neurologic deficits may indicate forebrain, brainstem or cerebellar abnormality
Courtesy Dr Chris Holland
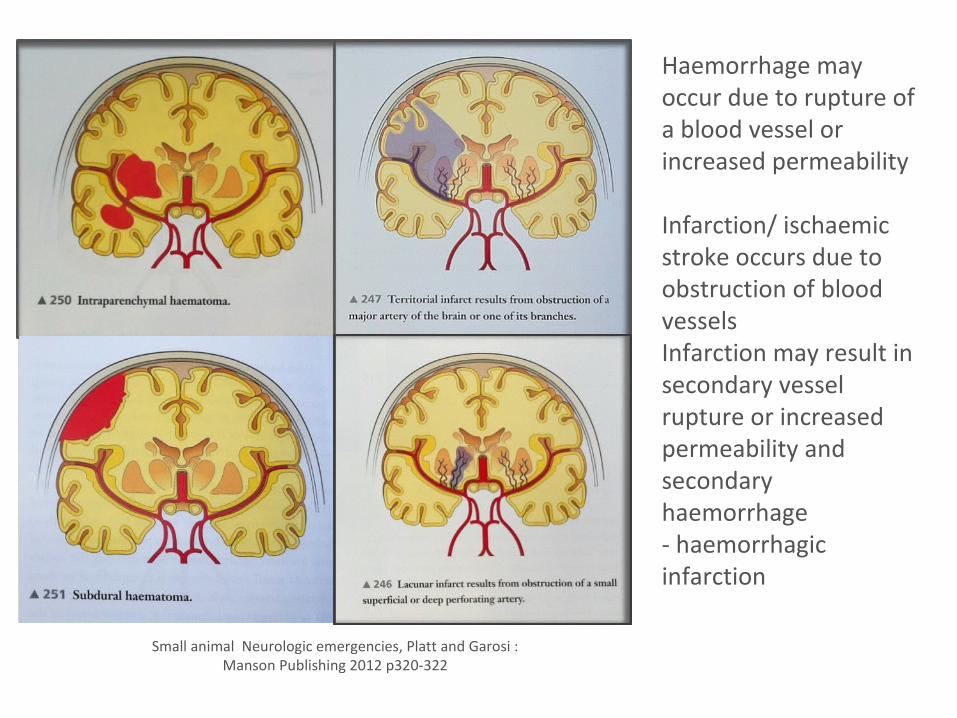
Small animal Neurologic emergencies, Platt and Garosi : Manson Publishing 2012 p320-322
Haemorrhage may occur due to rupture of a blood vessel or increased permeability
Infarction/ ischaemic stroke occurs due to obstruction of blood vesselsInfarction may result in secondary vessel rupture or increased permeability and secondary haemorrhage- haemorrhagic infarction
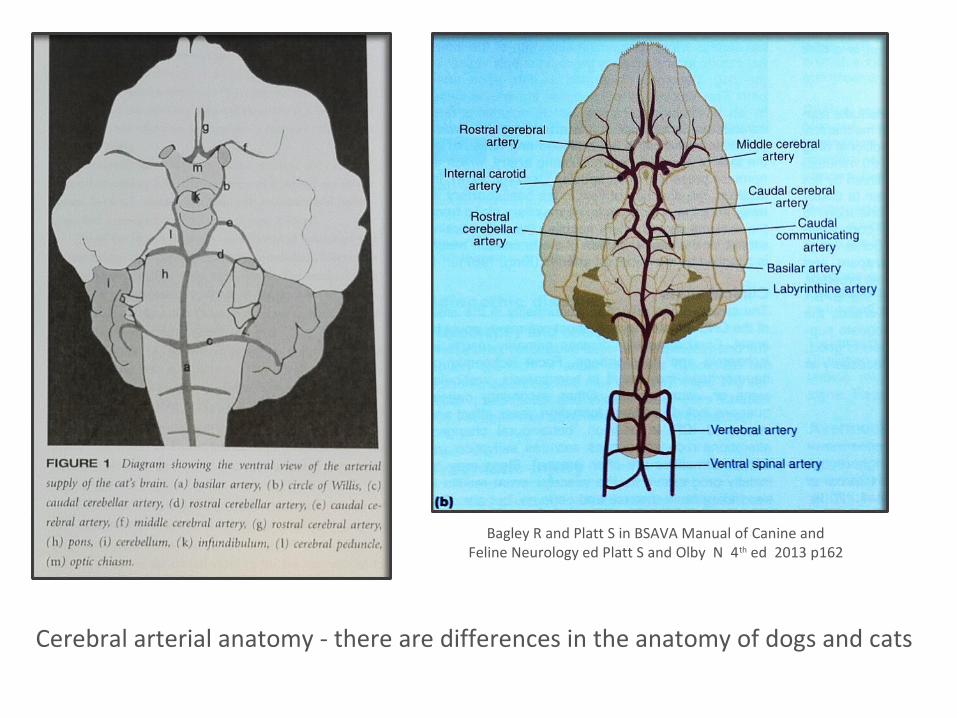
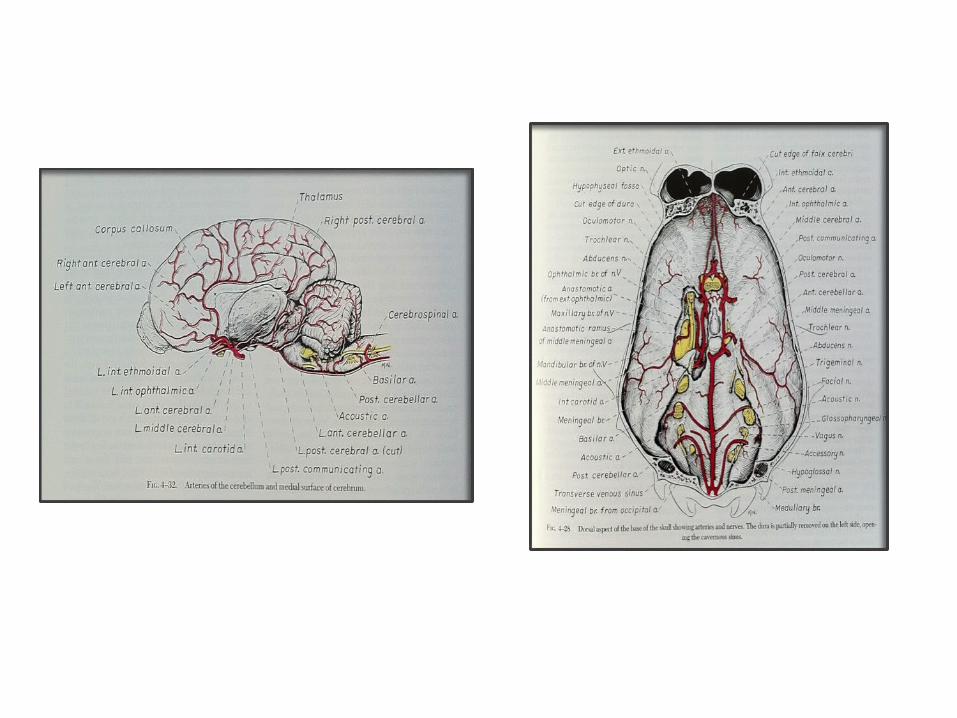
Cerebral arterial anatomy - there are differences in the anatomy of dogs and cats
Bagley R and Platt S in BSAVA Manual of Canine and Feline Neurology ed Platt S and Olby N 4th ed 2013 p162
www.sashvets.com
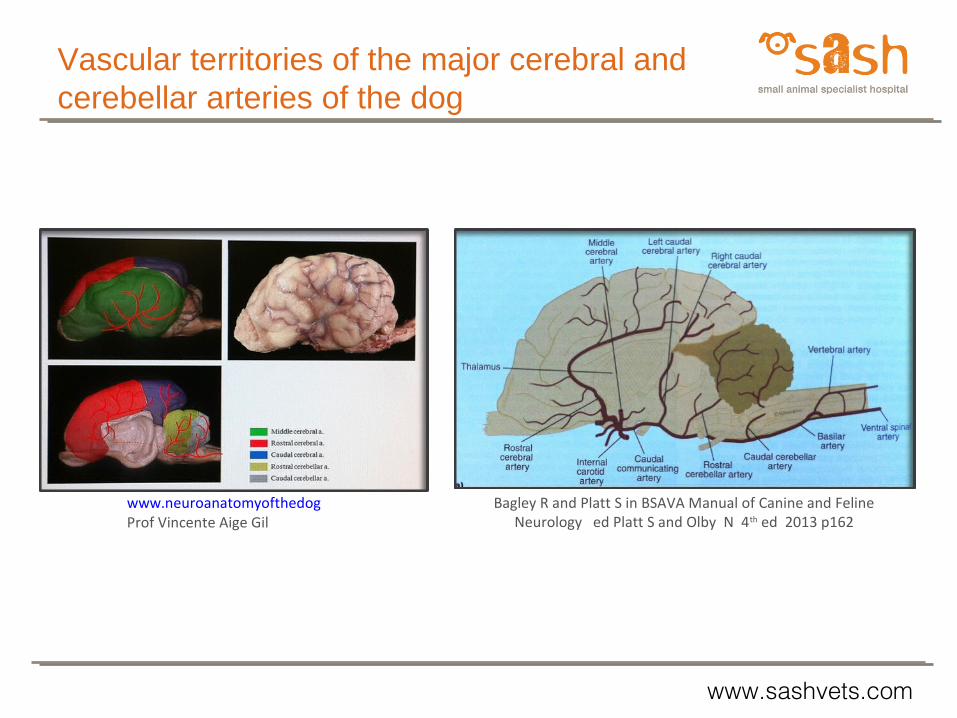
Bagley R and Platt S in BSAVA Manual of Canine and Feline Neurology ed Platt S and Olby N 4th ed 2013 p162
www.neuroanatomyofthedogProf Vincente Aige Gil
Vascular territories of the major cerebral and cerebellar arteries of the dog
www.sashvets.com
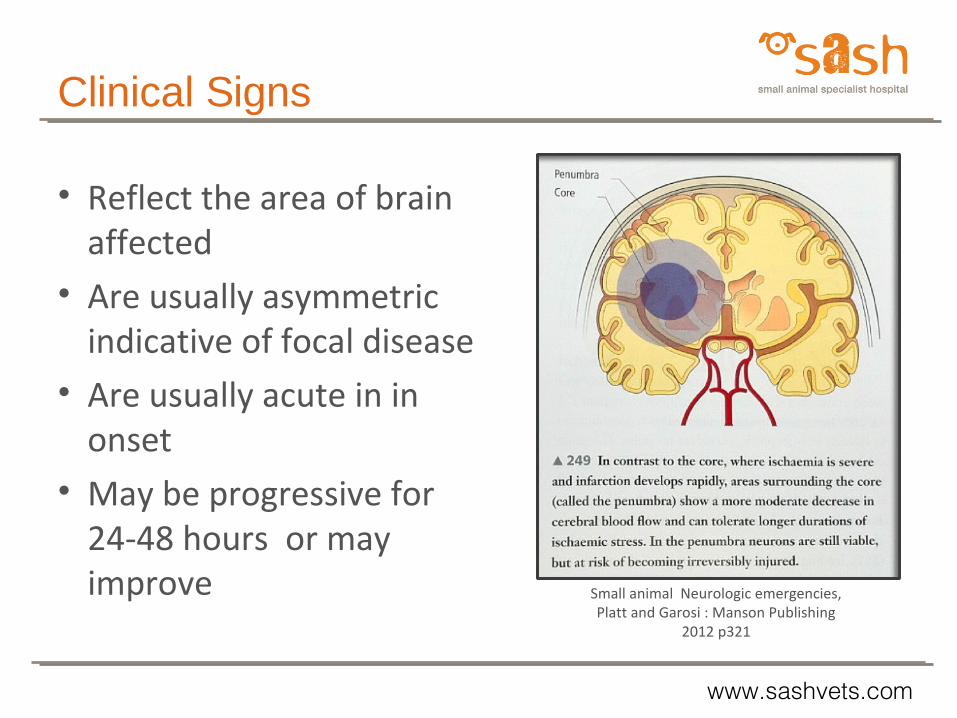
Small animal Neurologic emergencies, Platt and Garosi : Manson Publishing
2012 p321
Clinical Signs
• Reflect the area of brain affected
• Are usually asymmetric indicative of focal disease
• Are usually acute in in onset
• May be progressive for 24-48 hours or may improve

www.sashvets.com
Clinical Signs of Forebrain (Prosencephalic) Disease
• Altered mentation +/or consciousness• Abnormal behaviour, pacing• Circling towards the side of the lesion• Head turn/ adversive syndrome with thalamic lesions• Postural reaction deficits (contralateral)• Little gait abnormality• Menace deficit (contralateral) with or without visual deficit• Hemi-inattention or neglect (if unilateral lesion) • Seizures

www.sashvets.com
Clinical signs of midbrain dysfunction
• Altered level of consciousness (dull - coma)
• Compulsive circling (to the side of the lesion), head turn
• Postural reaction deficits ( I or C)• Hemiparesis / tetraparesis• Lack of normal eye movements (lack of
vestibulo-ocular reflexes)• Cranial nerve III deficits/pupillary
abnormalities• Respiratory pattern abnormalities• Decerebrate posturing if severe
Small Animal Neurology Fitzmaurice 2010 p7
www.sashvets.com
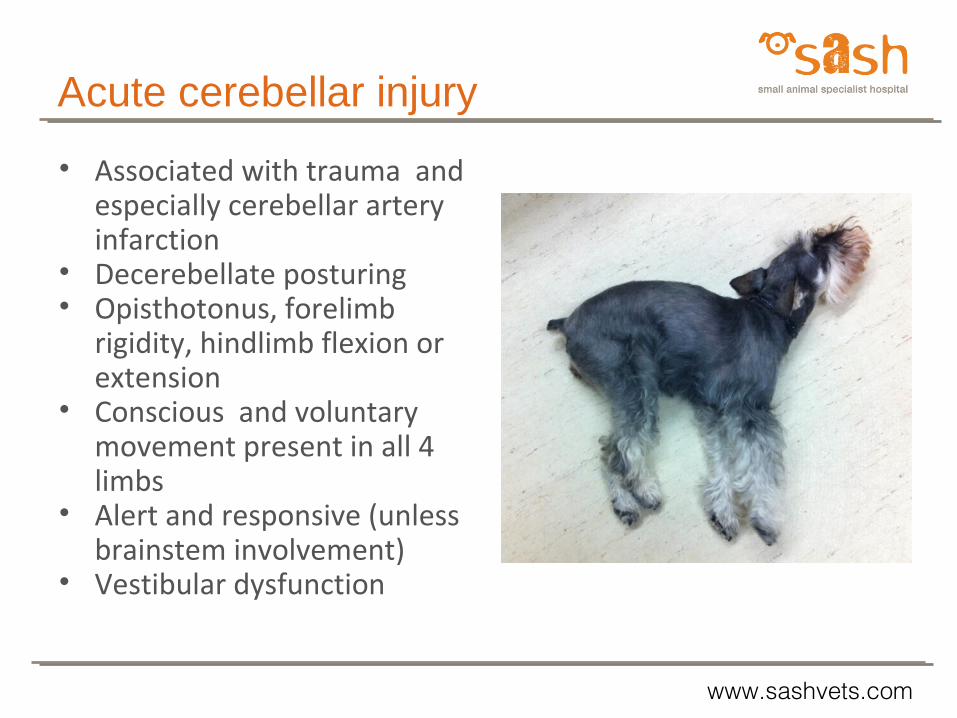
Acute cerebellar injury
• Associated with trauma and especially cerebellar artery infarction
• Decerebellate posturing• Opisthotonus, forelimb
rigidity, hindlimb flexion or extension
• Conscious and voluntary movement present in all 4 limbs
• Alert and responsive (unless brainstem involvement)
• Vestibular dysfunction
www.sashvets.com
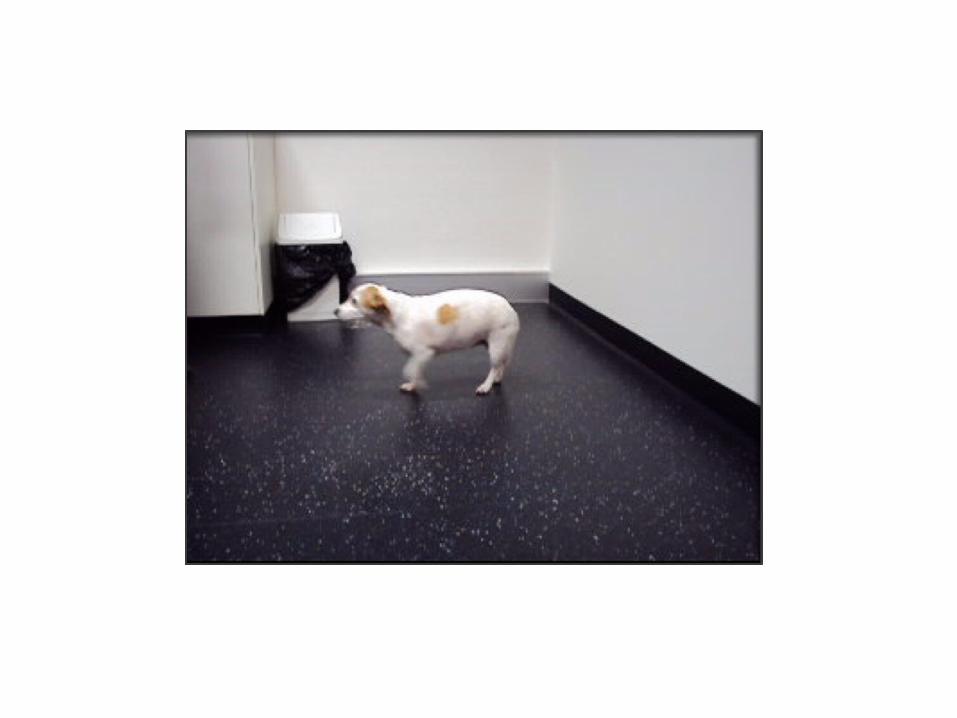
Clinical Signs of Caudal Brainstem Disease -pons and medulla oblongata
• Hemiparesis (ipsilateral) or tetraparesis(UMN)• Postural reaction deficits• Ataxia (vestibular)• Alteration in level of consciousness• Cranial nerve V-XII abnormalities especially
vestibular • Respiratory pattern abnormalities
if severe

www.sashvets.com
Courtesy University of Melbourne Veterinary Hospital
Cushi - 6yo FS JRT with acute onset of repetitive seizure activity and R postural deficits
www.sashvets.com
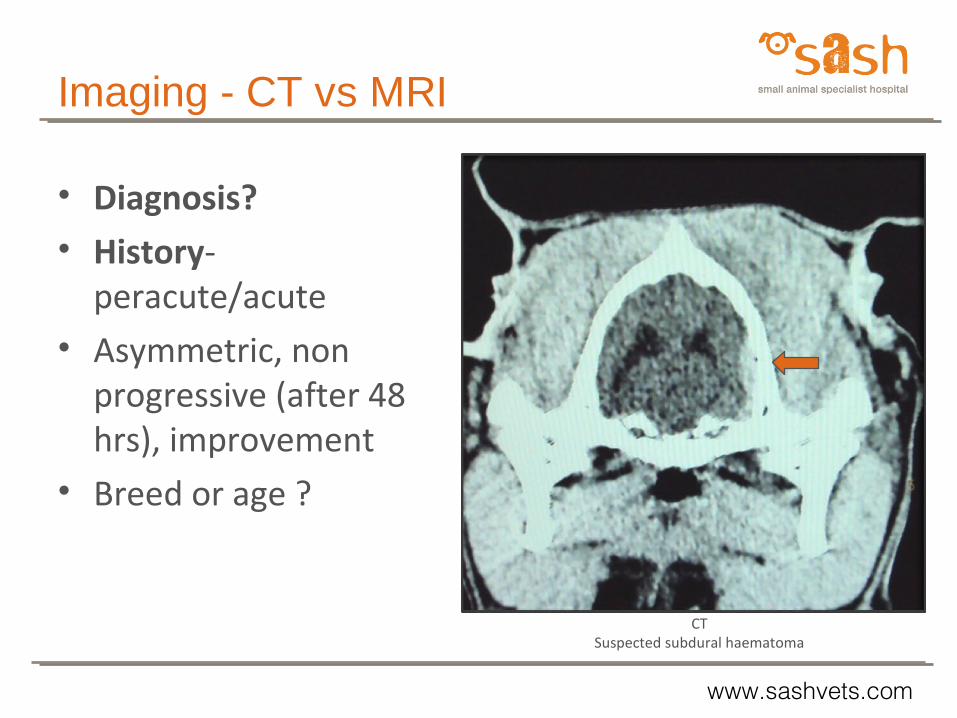
CT Suspected subdural haematoma
Imaging - CT vs MRI
• Diagnosis?• History-
peracute/acute • Asymmetric, non
progressive (after 48 hrs), improvement
• Breed or age ?
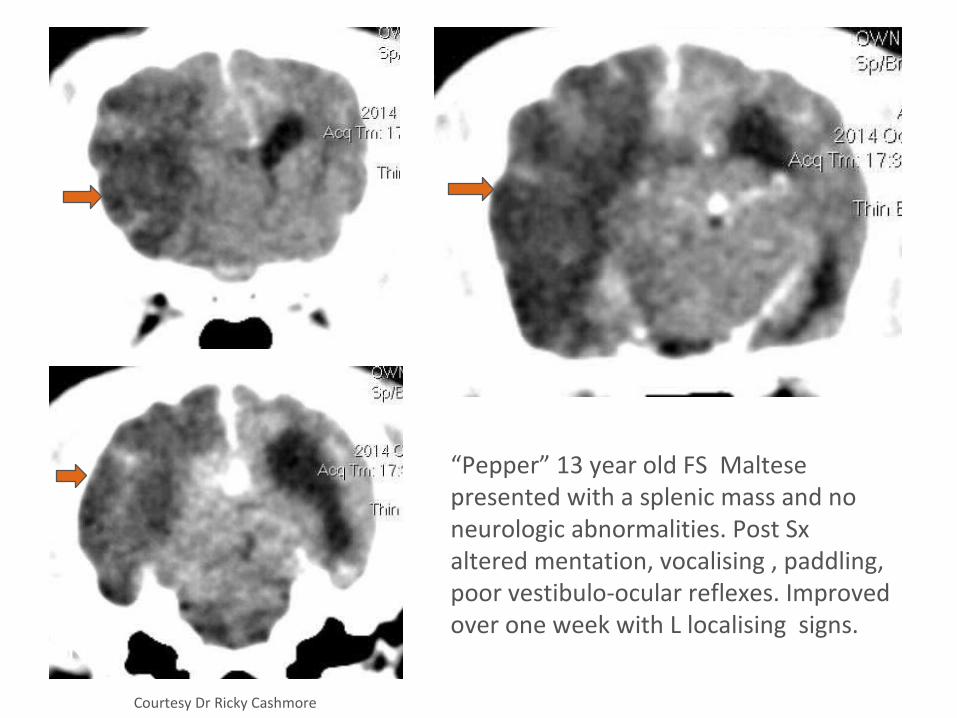
“Pepper” 13 year old FS Maltese presented with a splenic mass and no neurologic abnormalities. Post Sx altered mentation, vocalising , paddling, poor vestibulo-ocular reflexes. Improved over one week with L localising signs.
Courtesy Dr Ricky Cashmore
R
R
R
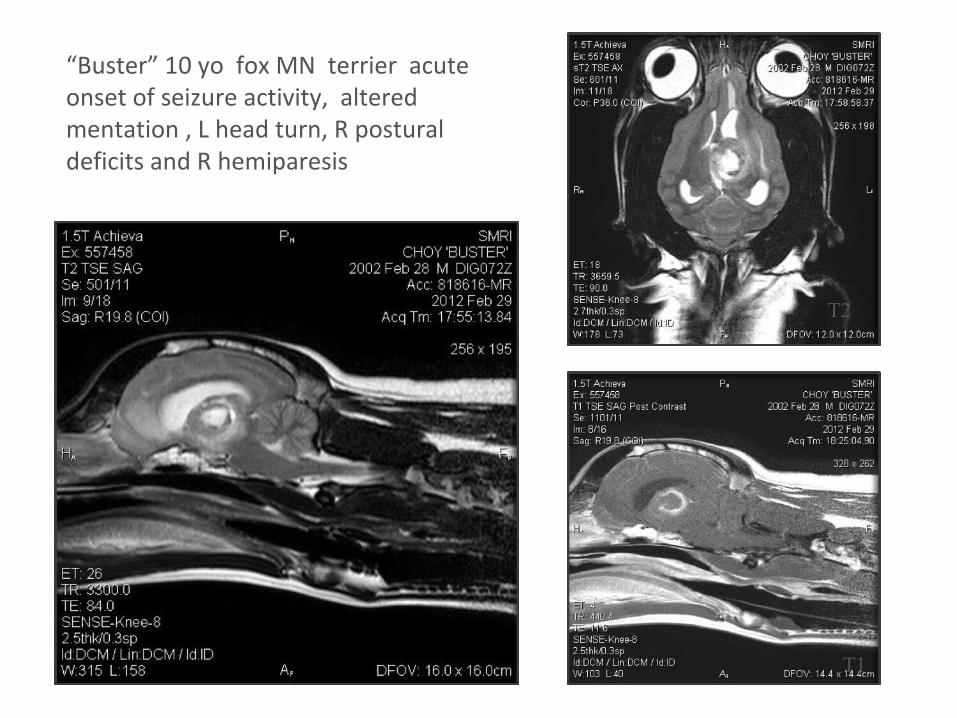
“Buster” 10 yo fox MN terrier acute onset of seizure activity, altered mentation , L head turn, R postural deficits and R hemiparesis
T2
T2
T1
www.sashvets.com
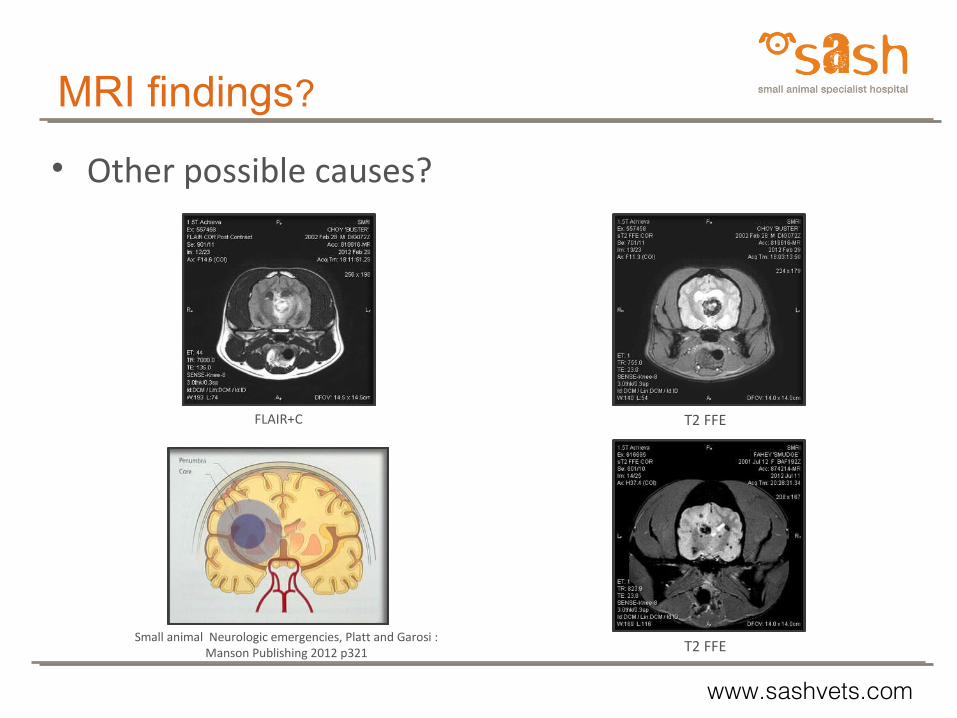
FLAIR+C T2 FFE
T2 FFESmall animal Neurologic emergencies, Platt and Garosi :
Manson Publishing 2012 p321
MRI findings?
• Other possible causes?
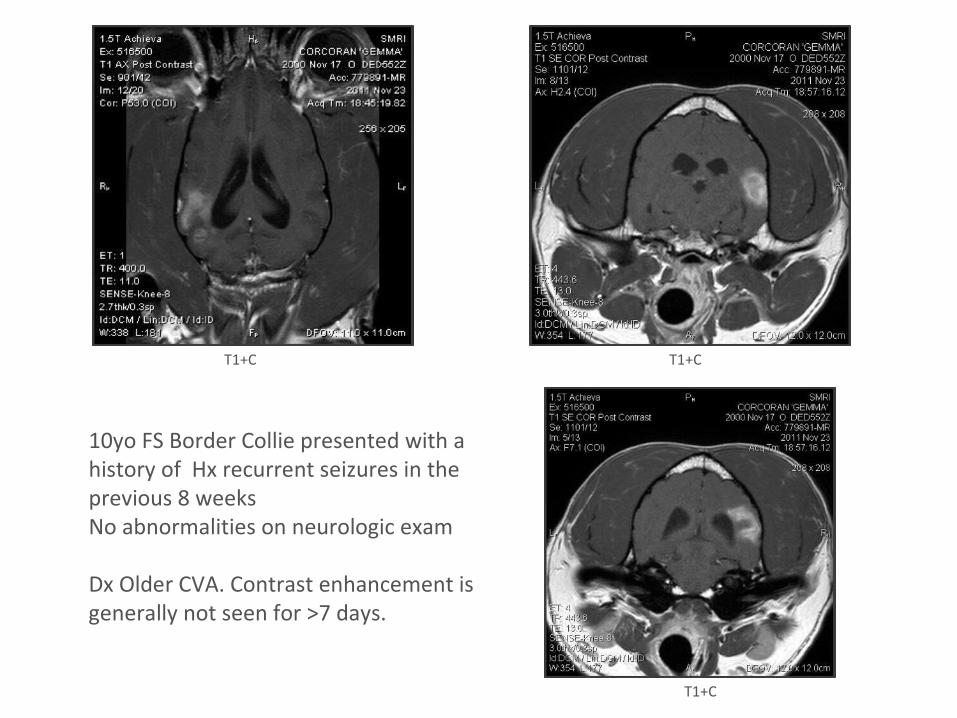
10yo FS Border Collie presented with a history of Hx recurrent seizures in the previous 8 weeksNo abnormalities on neurologic exam
Dx Older CVA. Contrast enhancement is generally not seen for >7 days.
T1+C T1+C
T1+C
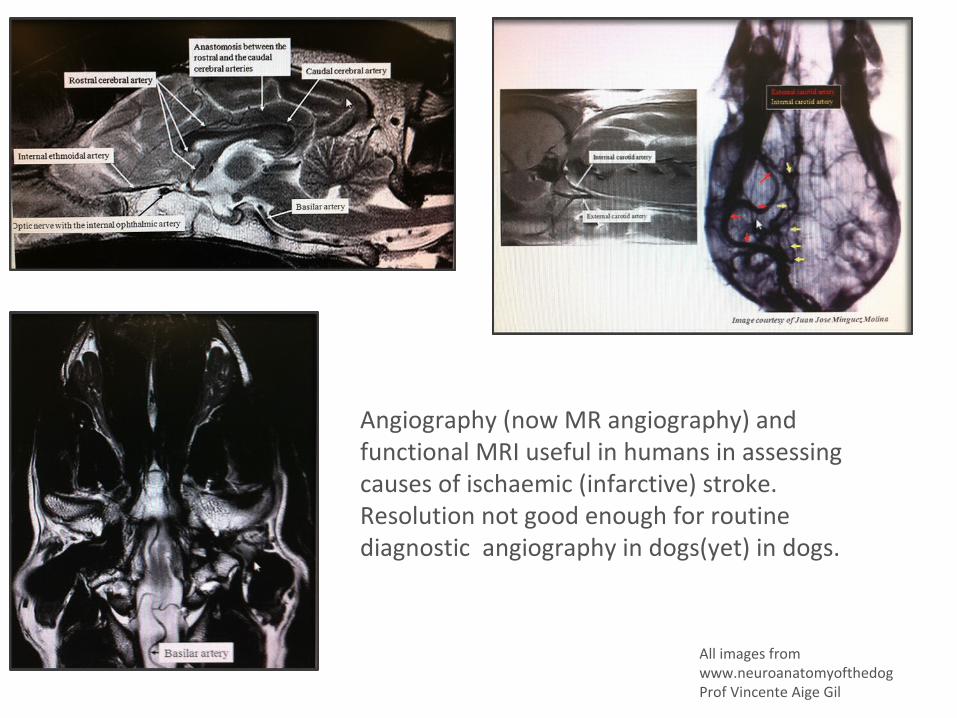
All images fromwww.neuroanatomyofthedogProf Vincente Aige Gil
Angiography (now MR angiography) and functional MRI useful in humans in assessing causes of ischaemic (infarctive) stroke. Resolution not good enough for routine diagnostic angiography in dogs(yet) in dogs.
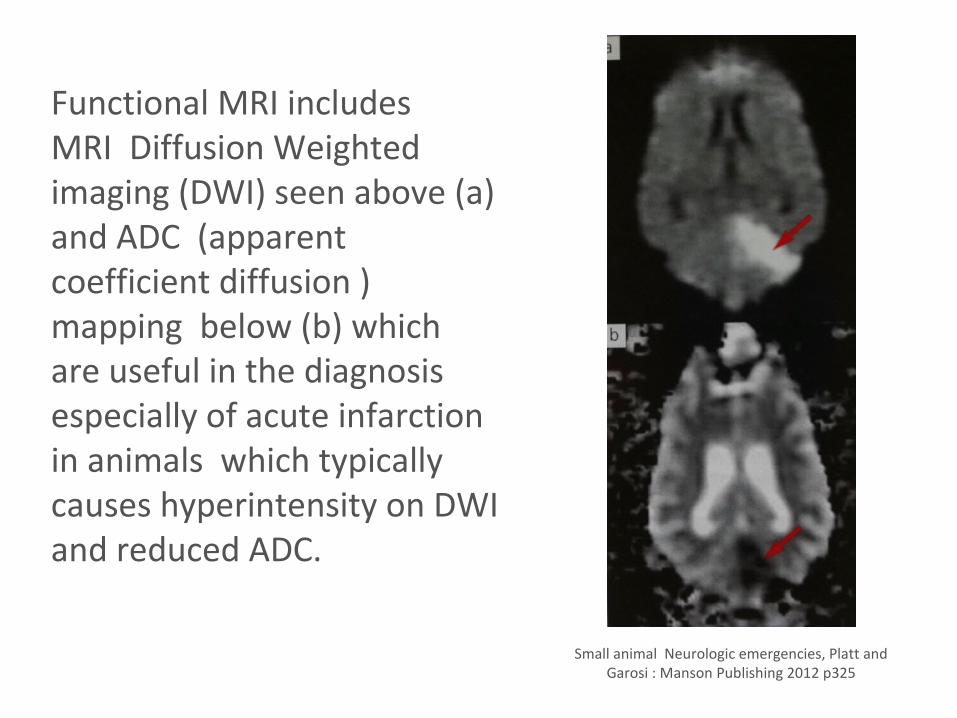
Functional MRI includesMRI Diffusion Weighted imaging (DWI) seen above (a) and ADC (apparent coefficient diffusion ) mapping below (b) which are useful in the diagnosis especially of acute infarction in animals which typically causes hyperintensity on DWI and reduced ADC.
Small animal Neurologic emergencies, Platt and Garosi : Manson Publishing 2012 p325
www.sashvets.com
CausesHaemorrhagic •Any cause of coagulopathy •Hypertension•Vasculitis•Intracranial neoplasia•(trauma)
Ischaemic (infarctive) •Thrombus formation or embolic disease •Which may be due to vascular disease eg atherosclerosis, hyaline •Degeneration of blood vessel walls •Hypertension•Cardiac disease •Any disease that may increase coaguability•Parasite migration •Intracranial neoplasia
Spontaneous •Cause unknown 50% or more of cases where concurrent •Disease is not found
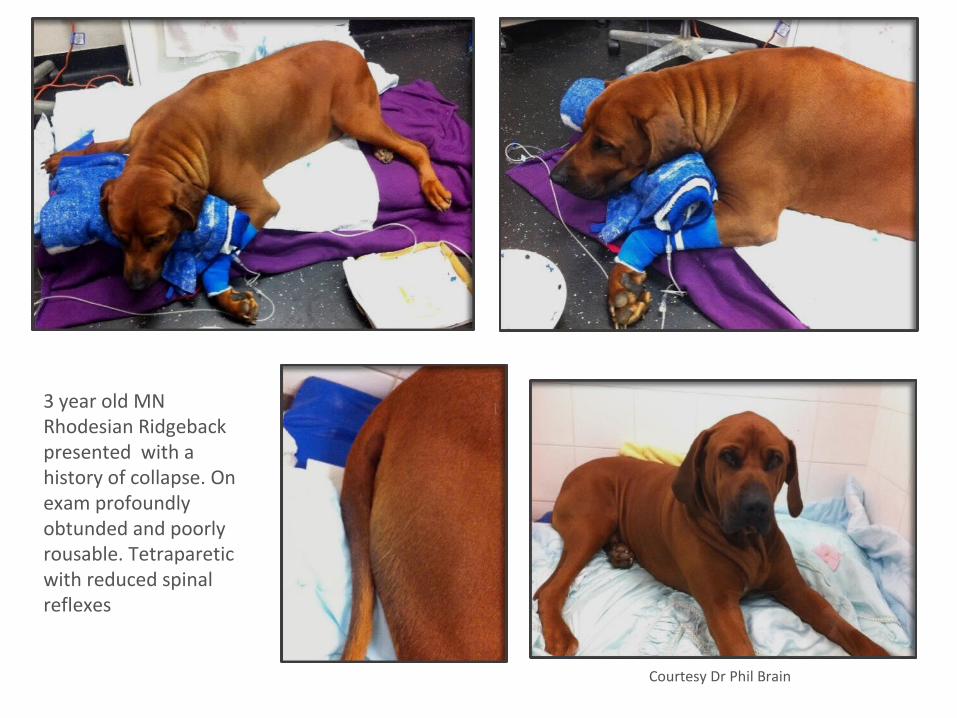
3 year old MN Rhodesian Ridgeback presented with a history of collapse. On exam profoundly obtunded and poorly rousable. Tetraparetic with reduced spinal reflexes
Courtesy Dr Phil Brain

• “Albert” 13 yo MN Himalayan cat presented with Hx of sudden onset of abnormal behaviour . Unresponsive to owner, pacing and circling to the R. On examination proprioceptive deficits evident LF and LH.
• BP 200 mmHg
• No abnormalities on CBC and Biochemistry profile
• USG 1.015
• MRI performed 1 week after onset of clinical signs.
T1+C
T2 dorsal
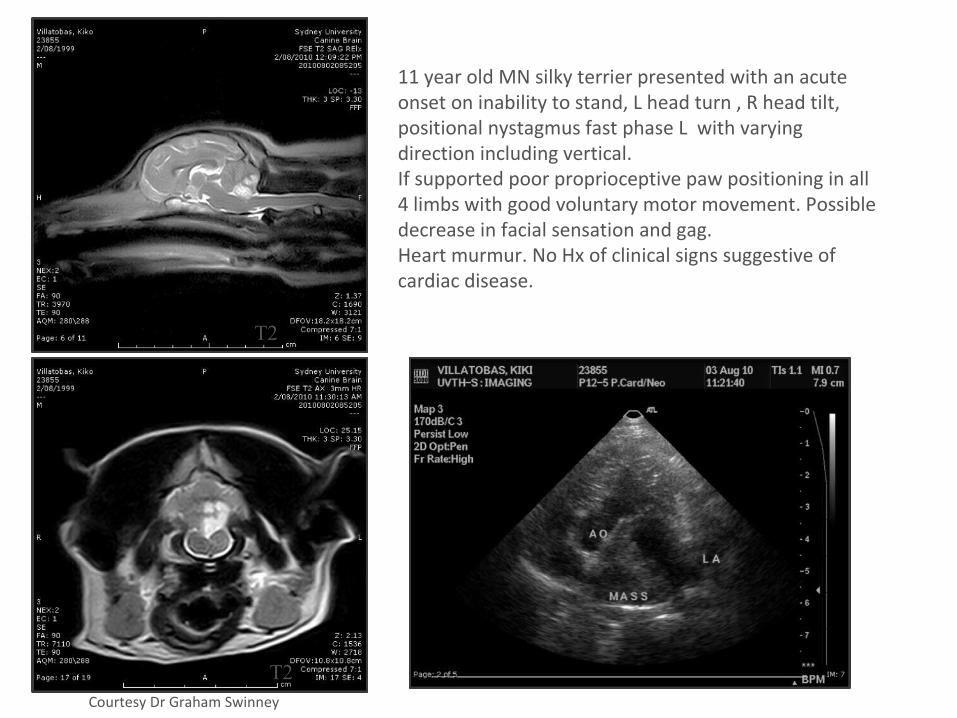
Courtesy Dr Graham Swinney
11 year old MN silky terrier presented with an acute onset on inability to stand, L head turn , R head tilt, positional nystagmus fast phase L with varying direction including vertical.If supported poor proprioceptive paw positioning in all 4 limbs with good voluntary motor movement. Possible decrease in facial sensation and gag.Heart murmur. No Hx of clinical signs suggestive of cardiac disease.
T2
T2
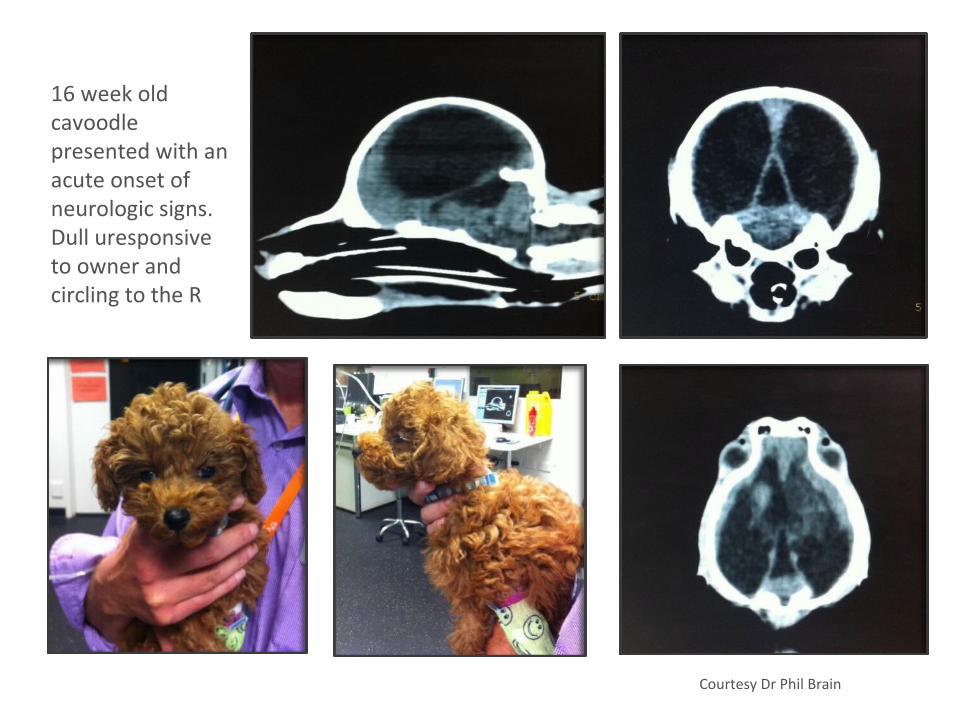
16 week old cavoodle presented with an acute onset of neurologic signs. Dull uresponsive to owner and circling to the R
Courtesy Dr Phil Brain
www.sashvets.com
Treatment
As for brain trauma•Maintain cerebral perfusion•Do not be overzealous in treating systemic hypertension•If deteriorating neurologic status suggests increasing ICP - treat as for brain trauma•Mannitol has not been shown to increase haemorrhage and may decrease blood viscosity•No evidence corticosteroids improve outcome - not effective in reducing the vasogenic or cytoxic oedema associated with CVA•Thrombolytic therapy?•Time and supportive care - improvement may continue for monthsUltimately recovery depends on the severity/extent of initial brain injury/ ischaemia•Treat any underlying cause•Risk of recurrence ? More likely if concurrent disease


www.sashvets.com.au twitter: @SASHvets Phone - (02) 9889 0289 Fax - (02) 9889 0431
Level 1, 1 Richardson Place, North Ryde 2113, Sydney, NSW