search and rescue technician pre-hospital protocols and
TRANSCRIPT

1 Canadian Air Division
Search and RescueTechnician Pre-Hospital Protocols and Procedures5th Edition
Effective Date 01-01-15
l B-GA-005-000/FP-D01
WPO 30889
SAR TECH PLEDGE
Without regard for my personal comfortor self-advancement
to the best of my abilityand to the limits of my physical and psychological endurance, I
solemnly pledge to make every effort to return to safety,those victims of disaster entrusted to my care
by the assignment of the mission to which I have consented. These things I shall do: “That others may live”.

1 Canadian air division
Search and reScue Technician Pre-hoSPiTal ProTocolS and ProcedureS5th Edition
(EnGLisH)
(Supersedes B-Ga-005-000/FP-d01 dated 01 September 2011)
issued on authority of the chief of the defence StaffPubliée avec l'autorisation du chef d'état-major de la défense
oPi: Fleet rdns, So Sar 2015-01-01
B-Ga-005-000/FP-d01l
NOTICEThis documentation has been reviewed by the technical authority and does not contain controlled goods.
AVISCette documentation a été révisée par l’autorité technique et ne contient pas de marchandises contrôlées.

liST oF eFFecTive ProTocolSinsert latest changed protocols; dispose of superseded protocols in accordance with applicable orders.
noTeon a changed protocol, the portion of the text affected by the latest change is indicated by a vertical line in the margin of the protocol. Changes to illustrations are indicated by miniature pointing hands, or black vertical lines.dates of issue for original and changed protocols are:
Total number of pages in this manual is 98.
original . . . . . 0 . . . . 2015-01-01 Ch . . . . . . . . 3 . . . . .Ch . . . . . . . . . 1 . . . . Ch . . . . . . . . 4 . . . . .Ch . . . . . . . . . 2 . . . . Ch . . . . . . . . 5 . . . . .
A
a ...............................................0i to vi .........................................01 to 1.6 ......................................02 to 2.3 ......................................03 to 3.5 ......................................0
4 to 4.7.......................................05 to 5.5.......................................06 to 6.32 ....................................07 to 7.11 ....................................08 to 8.10 ....................................0

ForewordB-Ga-005-000/FP-d01, Pre-Hospital Protocols and Procedures, searchand rescue Technician, is issued on authority of the Chief of the defenceStaff. This document is a field manual of medical procedures and proto-cols to be used by operational sar Techs to provide pre-hospital care inthe performance of search and rescue operations. The manual has been developed by the 1 Canadian air division surgeon and approved by thesurgeon General.
This publication B-Ga-005-000/FP-d01, dated 2015-01-01, is effective upon receipt.
inquiries and suggestions for change shall be forwarded through normal channels to the 1 Canadian air division Fleet rdns, so sar Tech for ap-proval by the division surgeon.
i

PreFaceThis set of medical protocols and procedures is evidence-based and forms the bonafide occupational medical requirement for CF SAR Technicians. It is the result of an extensive review of SAR medical field rescue requirements and suggestions from the field and is based on a review of over 1100 medical pa-tient rescues over the past 10-year period. a formal board including members who are sar Techs, paramedic instructors, physician specialists in aerospace medicine, anaesthesiology, trauma surgery, intensive care, emergency medicine and medical and paramedical education met together and in subcommittee to produce this manual. The protocols have been colour coded for ease in identifying QL specific tasks. all of the components of the protocols that are not in yellow highlight are trained at the QL5a (Primary Care Paramedic) level. The steps in protocols that are in yellow highlight require more skill and/or experience and they are instructed at the Ql6a part 1 level. The portions in blue refer to pediatric patients.The protocols emphasize the use of clinical judgement. This is reflected in both the protocols themselves and especially in the associated curriculum. This is not cookbook medicine and the sar Flight surgeons endorse the need for SAR Techs to act and be supported as fellow clinicians making difficult choices based on the specifics (environmental and medical) of each case. A specific example is the fact that these protocols are designed to function with two sar Techs on scene. in emergencies, where patient numbers and/or condition and/or multiple locations make it necessary for a sar Tech to act alone, it is understood that slight alterations to these protocols, which do not deviate from the key therapeutic principles (i.e. aBCs, early transport, etc.), may be required due to the environment (e.g. too cold to start an iv) or safety of the patient or sar team. These protocols have been reviewed by representative(s) of the standing Com-mittee on operational Medicine in ottawa before being sent to the surgeon General for approval. The Clinical Council and surgeon General have reviewed the final product and have sanctioned these protocols for field use. H Wright Md, MPH, aBPM(aM), CCFP, Cd Lieutenant-Colonel 1 Canadian air division surgeon P (Ben) Wahl, Md, dip avMEd, CCFP, Cd Lieutenant-Commander aerospace Medical Programs Flight surgeon r Hannah BPE, Md, MPH, aBPM(aM), CCFP, Cd Major aerospace standards and Clinical services Flight surgeon and sar Medical director
ii

TaBle oF conTenTSPage
List of Effective Pages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . aForeword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iPreface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iiTable of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iiisar Tech Contact # . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vi
SecTion 1 – cardiovaScular (cv) ProTocolS . . . . . . . .
1.1 Cardiac Chest Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.2 Cardiac arrest – aEd . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.3 Post-arrest stabilization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.4 discontinue resuscitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.5 do not resuscitate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.6 stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SecTion 2 – reSPiraTorY ProTocolS . . . . . . . . . . . . . . . .
2.1 soB with History Suggestive of asthma/CoPd . . . . . . . . . . . . . . . .2.2 Tension/symptomatic Pneumothorax . . . . . . . . . . . . . . . . . . . . . . 2.3 anaphylaxis/anaphylactic shock – adult and Child . . . . . . . . . . .
SecTion 3 – TrauMa ProTocolS . . . . . . . . . . . . . . . . . . . . .
3.1 Hemorrhagic shock . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.2 Tranexamic acid (TXa) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.3 Burns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.4 Fluid replacement requirements for Burn victims . . . . . . . . . . . .3.5 Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SecTion 4 – Medical ProTocolS
4.1 altered LoC – nYd . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.2 Hypoglycemic Emergency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.3 narcotic overdose – adult (suspected) . . . . . . . . . . . . . . . . . . . . 4.4 seizure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.5 antibiotic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.6 agitated Patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . .
4.7 Hiv Post Exposure Prophylaxis (PEP) . . . . . . . . . . . . . . . . . . . . .
iii
iv
conTenTS (continued)SecTion 5 – environMenTal ProTocolS . . . . . . . . . . . . . .
5.1 Hypothermia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.2 Hyperthermia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.3 High altitude illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.4 decompression illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.5 Motion sickness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SecTion 6 – druG MonoGraPhS . . . . . . . . . . . . . . . . . . . . . .
6.1 acetaminophen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.2 acetazolamide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.3 acetylsalicylic acid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.4 Bacitracin & Polymyxin B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.5 Cefoxitin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.6 Clindamycin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.7 dexamethasone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.8 dextrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.9 dimenhydrinate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.10 diphenhydramine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.11 Epinephrine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.12 Glucagon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.13 Glucose Gel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.14 Haloperidol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.15 ibuprofen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.16 ipratropium Bromide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.17 Ketorolac . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.18 Lidocaine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.19 Lorazepam . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.20 Midazolam . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.21 Morphine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.22 Moxifloxacin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.23 naloxone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.24 nifedipine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.25 nitroglycerin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.26 normal saline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.27 oxygen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.28 PEP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.29 ringers Lactate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

v
conTenTS (continued)
6.30 salbutamol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.31 Thiamine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.32 Tranexamic acid (TXa) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SecTion 7 – STandard Medical ProcedureS . . . . . . . . .
7.1 Patient assessment Model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7.3 assessment of suspected spinal injuries . . . . . . . . . . . . . . . . . . . 7.4 Urinary Catheterization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.5 EZ-io (intra-osseous) Power driver . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7.8 Tourniquet removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.9 Chest decompression (needle Thoracostomy) . . . . . . . . . . . . . .
7.11 Notification and Hospital Report . . . . . . . . . . . . . . . . . . . . . . . . . .
Sec
EZ-IO Needle Sets Size7.6 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Tion 8 – aBBreviaTionS/reFerenceS . . . . . . . . . . . . . .
8.1 Common Medical abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . .8.2 Glasgow Coma scale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.3 neurologic red Flags . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.4 rapid neurologic assessment . . . . . . . . . . . . . . . . . . . . . . . . . . .8.5 Pediatric Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.6 apgar score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.7 Example Calculation of Fluid replacement for Burn victims . . . .8.8 iv drip rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.9 Formulae . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8.10 Minutes of o2 supply by Pressure and Flow rate . . . . . . . . . . . .
7.10 orogastric (oG) Tube insertion . . . . . . . . . . . . . . . . . . . . . . . . . . .
7.2 airway insertionadvanced . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
EZ-io
7.7 EZ-io Insertion Sites
vi
Sar Tech contact numbersJrCC Halifax 1 800 565-1582 or 902 427-8200
JrCC Trenton 1 800 267-7270 or 613 965-3870
JrCC victoria 1 800 567-5111 or 250 413-8933
1 Can div surg daytime Pager for call back 204 931-1622
silent Hours BB 204 801-8983
Local Flight surgeon
Local Wing ops
other
“sar Techs won’t say it for themselves, so i’ll say it for them. These guys have repeatedly risked their lives by making do with this and other equipment so they can keep going out there saving people. They have the courage to put their lives on the line again and again. They care. They have had the courage to take these extra risks to make things work and they deserve the best we can give them.”
doc Ben Wahl in forum on SAR Tech equipment deficiencies,
sarEX 2013.

1
SecTion 1 – cardiovaScular (cv) ProTocolS1.1 Cardiac Chest Pain1.2 Cardiac arrest – aEd1.3 Post-arrest stabilization1.4 discontinue resuscitation1.5 do not resuscitate1.6 stroke
cardiac

cardiac
notes:

1.1 cardiac chest Painindication◊ Patients with a history suggestive of cardiac chest pain.
Primary interventions
Chewable asa 160 mg Po (single dose only)
o2 to sao2 ≥ 92%nitroglycerin spray 1 0.4 mg sL q5 min (max 3 doses) 2
if systolic BP ≥ 100 mmHg cycle can be repeated q30min prn (contraindicated if pulse <50 or >100 bpm or patients BP is 30% below normal)
start iv rL @ 100 mL/hr or iv lock
assess pain relief following up to 3 doses of nitroglycerin
Pain relief no pain relief
Monitor &Contact EP BP ≥ 90 mmHg BP < 90 mmHg
- Morphine 2.5 mg iv/io q5 min until pain relief: max 15 mg
iv rL 250 mL fluid bolus
- if no iv access, 10 mg sC/iM q2 hr- dosing cycle may be repeated q2 hr re-assess- With first dose of Morphine give
dimenhydrinate 25-50 mg iv/io or 50-100 mg iM 3
repeat iv rL 250 mLfluid bolus
Contact EP
1.1
1. Do not give if patient has recently taken medication for erectile dysfunction. If HR> than 100 BPM consult EP.
2. if no or very limited pain relief with nTG then morphine should be given early.
3. if patient is 60 years of age or older use ½ dose (25 mg) dimenhydrinate.

1.2 cardiac arrest – aedindication◊ absent carotid pulse and continued loss of consciousness and
not breathing.contraindication◊ Patients under 1 (one) Yoacautions◊ Children 1- 8 Yoa use child pads and child key/settings on aEd
if available.◊ severe hypothermia. 1◊ asphyxiation. 2◊ Traumatic arrest.
suspected or sar Tech witnessed arrest
Yes
attach leads/analyzeFollow aEd prompts
Consider advanced airway
if no signs of life after 3 cycles through aEd, contact physician for further direction while repositioning pads and continuing treatment
Pulse present
verify airway 1.3 Post-arrest stabilization Protocol
rule out treatable causesConsider:- iv/io rL x 1 L minimum bolus 3- Bilateral chest decompressions 4- Hypothermia 1
if unable to contact physician: go to discontinue resuscitation Protocol 1.4
1.2
1. Defibrillation is less likely to be effective below 30ºC PR/core temp. If first shock ineffective reposition aEd pads and analyze. Focus efforts on good chest compressions. re-warm patient per 5.1 Hypothermia Protocol.
2. if hypoxic arrest, e.g. drowning, emphasis should be on oxygenation. 3. or 20 mL/kg rapid infusion for children. 4. needle decompression effectively rules out pneumothorax from injury caused by CPr
as a cause of failure of resuscitation. see 7.9 Chest decompression Procedure.

1.3
1.3 Post-arrest Stabilizationindication◊ Patient post-cardiac arrest with a pulse +/- spontaneous respira-
tions.obtain baseline vital signs and monitor minimum q5 min 1
Maintain BLs as required
ventilate and oxygenate patient
Consider advanced airway insertion
if spontaneous resps > 12/min, titrate o2 to maintain sao2 ≥ 92% 2
iv rL @ 100 mL/hr(Titrate to Uo of 0.5 - 1 mL/kg/hr)
Contact EP
Consider:- IV RL 250 mL fluid bolus if BP < 90 mmHg
repeat prn to a maximum of 1L- if abdomen distended, 7.10 orogastric Tube
insertion Procedure- 7.4 Urinary Catheterization Procedure- allow for active cooling if patient verbally
unresponsive and BP > 100 mmHg. Target core temp 34°C. 3
1. Constant monitoring of the patient’s pulse is critical in the first 10 minutes post-arrest.
2. avoid over-oxygenation – maintain sao2 92% - 95%. 3. only if able to monitor core temp continuously, if pt is stable and is
unconscious (not to be attempted in fully conscious pt). if no continuous core temp monitoring then target is 35°C. Cooling methods may include:
a. Minimal attempts to warm patient;b. Non warmed IV fluids (1 L drops temp 1°C);c. ice packs in groin and axillae (only if transport time 2 hr or less).

1.4
1.4 discontinue resuscitationindication◊ Patients with absent vital signs who have not responded to treat-
ment.CPr/BLs initiated 1
Transport ≥ 1 hr Transport < 1 hr
BLs x 30 min Continue BLs until one of the following occurs:- return of circulation &
respiration- Care transferred to higher
medical authority- rescuers too exhausted to
continue BLs 4
aBC’s and reassess for 1 min
Continue BLs until all of the following criteria are met: 2 - advanced airway in place- symmetrical air entry to lungs
on 100% O2- Consider bilateral chest
decompressions in the event of (suspected) traumatic cardiac arrest
- 1.2 Cardiac arrest – aEdProtocol completed
- IV access with RL 500 mL fluidbolus
- rule out hypothermia- reliable criteria for determina-
tion of death are recognized 3,4
Update notice of CrashLocation (noCL)
Update notice of Crash Location (noCL)
1. special considerations: Continue resuscitation for children, for near drowning, and for hypothermic victims.
2. Where possible, EP should be contacted to authorize the discontinuation of resuscitation.
3. no pulse or respirations detected over 1 min, and no response to painful stimuli, AND pupils fixed and dilated.
4. all interventions (e.g. tubes, ivs, etc.) must be left in place (medico-legal requirement).

1.5
1.5 do not resuscitateat Time of assessment◊ Monitor vitals with vsM, aEd, and Pulse oximetry.◊ Contact EP.
initiate BLs if possible unless criteria for not resuscitating are met 1,2
document patient assessment and situation
Update notice of Crash Location (noCL)
Follow Coroner/rCMP instructions
1. all patients require resuscitation unless: a. more than 15 min have conclusively elapsed in cardiac and respiratory
arrest without any BLs; b. there is clear evidence that death has occurred (i.e. decapitation, tran-
section, rigor mortis, or decomposition); c. victim submersed in water (warm or cold) for more than 60 min (where
doubt exists as to duration of submersion, follow resuscitation procedures); or
d. sar Techs are in possession of an advanced directive not to resuscitate (e.g. “no CPr” bracelet).
2. if CPr is sustained for longer than 30 min and three consecutive “no shock advised” messages then go to 1.4 discontinue resuscitation Protocol.

1. F.a.s.T. stroke assessment = Face, arm, speech TestPt with 1/3 findings = 72% probability of an acute stroke if symptoms are newPt with 3/3 findings = 85% probability of an acute stroke if symptoms are new
a. Facial droop: Have the person smile or show his or her teeth. if oneside doesn’t move as well as the other so it seems to droop, that could be sign of a stroke.• normal: Both sides of face move equally• abnormal: one side of face does not move as well as the other
(or at all)b. Arm drift: Have the person close his or her eyes and hold his or her
arms straight out palm up for about 10 seconds. if one arm does notmove, or one arm drifts down more than the other, that could be asign of a stroke.• normal: Both arms move equally or not at all• abnormal: one arm does not move, or one arm drifts down
compared with the other side and/or hand will pronate.c. Speech: Have the person say, “You can’t teach an old dog new tricks,”
or some other simple, familiar saying. if the person slurs the words,gets some words wrong, or is unable to speak, that could be sign ofstroke. • normal: Patient uses correct words with no slurring• abnormal: slurred or inappropriate words or mute
d. Time: Time patient was last known to be normal and emphasizes need to urgently transport to stroke centre.
1.6
1.6 Strokeindication◊ rapid onset of unilateral facial droop, unilateral arm weakness,
speech difficulties, or gait abnormality.Primary interventions including blood glucose
stroke assessment using FasT approach 1
o2 to sao2 ≥ 92%
iv lock (must not delay transport)
initiate urgent transport to stroke centre if available andensure stroke team is alerted.
document neurological exam (protocol 8.4)

Stroke centresname Phone location1.
2.
3.
4.
5.
6.
7.
8.
notes:
1.6

notes:

2
SecTion 2 – reSPiraTorY ProTocolS2.1 soB with History of asthma/CoPd2.2 Tension/symptomatic Pneumothorax2.3 anaphylaxis/anaphylactic shock – adult and Child
reSP

Primary interventions & O2 to keep O2 sat ≥ 92% 1,2
If not improving
If obtunded
Salbutamol 5 mg nebs continuous withalternate Ipratropium bromide 0.5 mg via neb OR
8 puffs q10 min up to 3 doses 3
Salbutamol 5 mg nebs PRN up to 3 doses ORSalbutamol MDI 4-8 puffs PRN q10 min up to 3 doses
100% O2 via BVM to keep O2 sat ≥ 92%
Salbutamol continuous MDI 2 puffs per min through BVM
Epinephrine 0.3 mg IM X 1 dose 4
Decreased LOC, inability to speak,↓ SPO2 or signs of cyanosis
Initiate transport
If transport delayed > 1 hr then give
Improving
Dexamethasone 10 mg IM / IV X 1 dose
Contact EP 4Pediatric Dosage: ≤ 12 YOASalbutamol 2.5 mg nebulized/MDI 2-4 PuffsIpratropium 0.25 mg nebulized/MDI 4-8 PuffsEpinephrine 0.01 mg/kg (Max 0.3 mg) SC/IM q2 hr prnDexamethasone PO, IM, IV 0.6 mg/kg once (maximum dose 10 mg)
◊ Patients who are SOB with a history suggestive of asthma or COPD.
2.1 SOB with a History Suggestive of Asthma/COPDIndications
2.1
1. Consider other causes of SOB such as CHF, MI, pulmonary embolism,pneumothorax, pneumonia, foreign body (especially in children) and HAPE.2. Watch for loss of hypoxic drive in COPD patients receiving supplementaloxygen – SaO2 of 92 to 95% is generally safe in these patients.3. Give Ipratropium in a ratio of one dose for every 2 doses of Salbutamol.4. Consider Glucagon if pt is on beta blocker and is not responding to treatment. Contact EP for order.

2.2 Tension/Symptomatic Pneumothorax indications 1 ◊ Penetrating torso trauma above the level of the umbilicus
or◊ Unilateral absent breath sounds or tracheal deviation especially
with blunt injury (bruising, crepitus, obvious flail, asymmetry oninspection), blast injury (by history, particularly blast in confinedspace) or possible hyperbaric injury (diving/high pressure gas) 2 or
◊ rapid decompression. 2
WiTH anY onE oF THE FoLLoWinG:◊ BP systolic < 90 mmHg, or loss of radial pulse
or◊ Significant respiratory distress
or◊ Oxygen saturation less than 90%
or◊ Unexplained vsa or profound instability from unknown source.
Primary interventions
100% O2 3
assess respiratory status
Landmark and perform 7.9 Chest decompression Procedure
- assess respiratory status- Monitor patient for improvement
Consider repeat Chest decompression 4
Contact EP 5
2.2
1. Contact EP if these requirements are only partially met. Watch for patient deterioration during air evacuation.
2. With any possible decompression injury, go to 5.4 decompression illness Protocol once pneumothorax decompressed.
3. Oxygen flow may be reduced after chest decompression to maintain SaO2 ≥ 92%. 4. if pt fails to respond or shows transient improvement only, multiple
decompressions may be required. remember – if in doubt insert needlemore laterally on chest.
5. recommend maintaining lowest safe altitude for evacuation by air.

2.3
2.3 anaphylaxis/anaphylactic Shock – adult and childindication / diagnostic criteriaanaphylaxis is highly likely when any onE of the following 3 criteria (i, ii, iii) are fulfilled:
i. acute onset of an illness (minutes to several hours) withinvolvement of the skin, mucosal tissue, or both (eg, generalized hives, pruritus or flushing, swollen lips-tongue-uvula) and aT LEasT onE oF THE FoLLoWinG a. respiratory compromise (e.g., dyspnea, wheeze-
bronchospasm, stridor, sPo2 ≤ 92%) B. reduced BP or absent radial pulse or decreased level of
consciousnessor
ii. TWo or MorE oF THE FoLLoWinG that occur rapidly afterexposure to a likely allergen for that patient (minutes to severalhours):
a. involvement of the skin-mucosal tissue (e.g., generalizedhives, itch-flush, swollen lips-tongue-uvula)
B. respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, sPo2 ≤ 92%)
C. reduced BP or absent radial pulse or decreased level ofconsciousness
d. Persistent gastrointestinal symptoms (e.g., crampyabdominal pain, vomiting)
oriii. reduced BP after exposure to a known allergen for that patient
(minutes to several hours):
A. Infants and children: low systolic BP (age specific)* orgreater than 30 % decrease in systolic BP
B. adults: systolic BP of less than 90 mmHg or greater than30 % decrease from that person’s baseline

2.3
2.3 anaphylaxis/anaphylactic Shock – adult and child For mild allergic rash without other symptoms of anaphylaxis, consider diphenhydramine 50 mg iM.
cautions◊ Elderly patients are at an increased risk of side effects.◊ Patient on beta blocker medication may not respond adequately
to Epinephrine or salbutamol treatment.Primary intervention 1, 2
Epinephrine 0.3 mg iM q5 min prn x 3 doses
Provide supplemental oxygen
initiate iv rL 1L bolus Repeat boluses to titrate to BP ≥ 90 mmHg
diphenhydramine 25-50 mg iv/iM 3
if soB or wheeze persists following repeated doses of Epinephrine give salbutamol 5 mg and ipratropium 0.5 mg
nebulized 4 q5 min X 3 PrnContact EP
Consider dexamethasone 5
Pediatric dosage ≤ 30kg - Epi 0.15 mg iM q5 min prn x 3 doses (if < 10 kg/1 Yoa, give 0.01 mg/kg)- salbutamol 2.5 mg nebulized q5 min X 3 Prn- rL Bolus 20 ml/kg- diphenhydramine 1 mg/kg (30 mg max) iv/iM- ipratropium 0.25 mg nebulized q5 min X 3 Prn
1. remove precipitant (e.g. bee sting – remove stinger). 2. if anaphylaxis is anticipated in an asymptomatic patient because of prior
history, nature of exposure or patient’s condition, consider contacting EP for Epinephrine/diphenhydramine/Glucagon orders.
3. decrease diphenhydramine dose by ½ in the elderly, as this population is more susceptible to side effects.
4. salbutamol (4-8 puffs) / ipratropium (4-8 puffs) may be given by Mdi with spacer.5. Consider dexamethasone if patient response is poor or symptoms reoccur; to
be given by physician order only.

notes:

3
SecTion 3 – TrauMa ProTocolS This section covers the protocols and procedures for: 3.1 Hemorrhagic shock3.2 Tranexamic acid (TXa)3.3 Burns 3.4 Fluid replacement requirements for Burn victims 3.5 Pain
TrauMa

TrauMa
3.1
3.1 hemorrhagic Shockindications ◊ systolic BP < 90 mmHg (or hypotensive for age) or other signs
of shock in the setting of trauma (altered mental status in the absence of head trauma and/or absent radial pulse).
Precautions ◊ Hypothermia severely diminishes clotting 1◊ Head injury 2, blunt/crush injury to the chest.
Primary interventions 3
BP ≥ 90 mmHg BP < 90 mmHg
iv lock iv/io rL 500 mL rapid infusion. Then titrate with rL to maintain BP at approximately 90 systolic, palpable radial pulse or improved mental status.
Give TXa if indicated (see Protocol 3.2)
Contact EP and reassess patient after 2 L infused
Perform 7.4 Urinary Catheterization Procedure 4-Monitor blood glucose and urine output.Target Uo: > 0.5 mL/kg/hr for adults
> 1 mL/kg/hr for children
Contact EPPediatric dosage:initial bolus: iv rL 20 mL/kg rapid infusion. May repeat x 1 dose.subsequent bolus: iv rL 20 mL/kg rapid/pressure infusion (max 60 mL/kg total).once hemodynamically stable, consult EP for d10W order to prevent hypoglycaemia.1. Early focus must be on keeping trauma patients warm. 2. in a casualty with an altered mental status due to a head injury, a higher BP is
often needed to maintain cerebral perfusion. Therefore, systolic pressure must be titrated to ≥ 100 mm/Hg
3. Consider sites of potential blood loss: chest, abdomen, pelvic fracture, femur fracture.4. only use if prolonged evacuation expected (greater than 2 hrs). do not insert
a urinary catheter if there are signs and symptoms of urethral injury such as peroneal or scrotal bruising, blood at the urethral meatus, pelvic fracture, or vaginal or rectal bleeding.

3.2
3.2 Tranexamic acid (TXa) indications ◊ Adult trauma with clinical evidence of significant hemor-
rhage (systolic BP < 90 mmHg or Hr >110 or both).Precautions ◊ To be administered as soon after injury as feasible.◊ delivery of TXa should not delay evacuation of patient.◊ Maximum cumulative dose 2 grams.contraindications◊ documented allergy to TXa.◊ if > 3 hr after initial injury.◊ not for use in Pediatrics
if directed from Protocol 3.1Hemorrhagic shock
draw up 1 gram of TXa (1 g per 10 mL) in a 10 mL syringe and give by slow iv injection over 10 min (1 mL per min) 1
continue fluid resuscitation
after 1 hourdraw up 1 gram of TXa (1 g per 10 mL) in a 10 mL syringe
and give by slow iv injection at 1 mL every hour.
reassess and consult EP
1. do not give TXa iv push as it may cause hypotension.

3.3
3.3 Burns indications ◊ Patients with 2nd and 3rd degree burns covering greater than
20% BSA or lesser area with hand, face or genital involvement.
Primary interventionsKeep patient warm and dry
IV/IO RL with warm IV fluid and high flow O2if hypotensive rL 500 mL rapid infusion.Repeat prn to achieve ≥ 90 mmHg.
Consider Protocol 3.1
irrigate burn and apply sterile occlusive dressing.3.5 Pain Protocol
adult: iv/io rL 500 mL rapid infusion prn.Repeat prn to achieve ≥ 90 mmHg.
Calculate BsaGive fluid replacement (Protocol 3.4)
7.4 Urinary Catheterization ProcedureMonitor urine output target 1
> 0.5 mL/kg/hr for adult > 1 mL/kg/hr for children
Contact EPConsider antibiotics (Protocol 4.5)
Pediatric dosage:Child: iv/io rL 20 mL/kg rapid infusion. May repeat x 1 dose then refer to 8.5 Pediatric tableonce hemodynamically stable, consult EP for d10W order to prevent hypoglycemia.
1. Titration of fluid administration to urinary output is the only reliable way toinsure adequate fluid resuscitation in the field.

3.4
3.4 Fluid replacement requirements for Burn victimsPediatric: 4 mL RL x Weight in (kg) x Body Surface Area (BSA) affected in (%) = mL/24 hrs amount.
1/2 in 1st 8 hrs 1/4 in 2nd 8 hrs 1/4 in 3rd 8 hrs = Total in 24 hrs
This is expected minimum fluid requirement, however you must titrate to clinical condition (adequate = good urinary output, oversupply = fluid overload including pulmonary edema). adequate urinary output rate is > 0.5 mL/kg/hr for adults and > 1 mL/kg/hr for children < 25 kg.
adult: Estimate total BSA burned to the nearest 10% using Rule of NinesFluid resuscitation using the Usaisr rule of Ten: - If burns are greater than 20% of total BSA, fluid resuscitation
should be initiated as soon as iv/io access is established. resuscitation is to be initiated with ringer’s lactate.
- Initial IV/IO fluid rate is % total BSA burned x 10 mL/hr for adults weighing 40-80 kg.
- For every 10kg above 80kg, increase initial rate by 100 mL/hr. if hemorrhagic shock is also present, resuscitation for hemorrhagic shock takes precedence over resuscitation for burns. remember the need for maintenance fluids.
14% 14% 18% 18%
18%
18% anterior18% posterior
9%9%
9%
18% anterior18% posterior
9%9%
1%
child adult

3.5 Pain indication◊ Patients exhibiting signs of pain.contraindications◊ Morphine: altered LoC and/or hypotension (hypotensive for age)
and/or respiratory distress or at significant risk of developing hypotension or respiratory distress.
◊ allergy to medication used in protocol.◊ Ketorolac: Uncontrolled bleedingcautions◊ severe chest injuries or blunt or penetrating head trauma.◊ Unknown cause of pain.
Primary interventions
assess patient’s pain 1
if mild – moderate pain ....... then nsaid + acetaminophen
ibuprofen 400-800 mg q4-6 hr Po prn 2,3
orKetorolac 4 - adult: 30 mg iv/io/iM q6 hr (max 120 mg/24 hr)- Elderly/Adult ≤ 50 kg: 15 mg IV/IO/IM q6 hr (max 60 mg/24 hr)
and / oracetaminophen 650 -1000 mg Po q4-6 hr prn 5
reassess pain.if severe pain add morphine ....... (assuming not hypotensive or in respiratory distress or at imminent risk for either condition).
dimenhydrinate 25-50 mg iv/io or 50-100 mg iM/PoMorphine 2.5-5 mg iv/ io 6,7 q5 min
(max 15 mg in 30 min), may repeat X 1 8
reassess pain. if pain still not controlled
if >1 hour from last Morphine dose may giveMorphine 2.5-5 mg iv/ io 6,7 q5 min
(max 15 mg in 30 min), may repeat X 1 8
Contact EPreassess pain q5 min
3.5Pediatric dosage: See notes

3.5
3.5 notesPediatric dosage:2-16 Yoa (< 2 Yoa = contact EP)- ibuprofen 10 mg/kg Po q8 hr prn 2,3
- Ketorolac 0.5 mg/kg iv/io (max dose 15 mg) or - 1 mg/kg iM 4 (max 30 mg single dose only) Contact EP for
further dose.- acetaminophen 10-15 mg/kg Po q4-6 hr prn 5
- dimenhydrinate 1 mg/kg iM or age appropriate Po dose 9
- Morphine (patient < 50 kg) 0.1 mg/kg/dose iv / io 7 q5 min (max 3 doses in 30 min). repeat every 2-4 hours. if Patient > 50 kg use adult dosing.
1. avoid Po medication in patients with severe pain.2. if allergic to ibuprofen or acetylsalicylic acid (asa) then give acetami-
nophen only. 3. do not administer two nsaids together. Ketorolac and ibuprofen are not
to be given within 8 hrs of each other. For all other nsaids taken by the patient, contact EP.
4. anti-emetic is recommended with Ketorolac administration. 5. acetaminophen may be given concurrently with ibuprofen or Ketorolac for
synergistic effect. 6. Where iv or io access is unavailable, Morphine 10 to 15 mg (patient < 50 kg
0.1 mg/kg/dose) sC/iM may be given. Goal is patient able to tolerate pain.7. Use Morphine 2.5 mg for elderly or unstable patients and Morphine 5 mg for
younger or stable patients. 8. Ensure narcan is available in case of overdose. 9. dimenydrinate may be administered orally to children over 2 years of age.
see 6.9 dimenhydrinate Monograph for pediatric dosages.

notes:

4
SecTion 4 – Medical ProTocolS 4.1 altered LoC – nYd 4.2 Hypoglycemic Emergency 4.3 4.4 4.5 4.6
narcotic overdose – adult (suspected) seizure antibiotic
agitated Patient 4.7 Hiv Post Exposure Prophylaxis (PEP)
Med

4.1
4.1 altered loc – nYdindication ◊ For patients presenting with a decreased LoC from unknown
origin.1
Primary interventions including blood glucose
BP ≥ 90 mmHg BP < 90 mmHg (or hypotensive for age)
iv/io rL 500mL rapid infusion. 2Repeat prn to achieve ≥ 90
mmHg.
Blood glucose ≥ 4.0 mmol/L 2
Yes no 3
naloxone 1 mg sC/iM q15 min or
0.5 mg iv/io over 1 min q2-3 min prn iv rL @ 100 mL/hr
Go to 4.2 Hypoglycemic Emergency Protocol and if no improvement in LoC
return to 4.1 altered LoC – nYd
Contact EP
Pediatric dosage: iv/io rL 20mL/kg rapid infusion.May repeat x 1 dose then refer to 8.5 Pediatric Table.
1. Causes of altered LoC may include alcohol, Epilepsy, insulin, overdose, Ure-mia, Trauma, infection, Psychological, and stroke (aeiouTiPS). aMs, hypoxia,and hypothermia should also be considered.
2. if glucose > 20 mmol/L UsE norMaL saLinE and contact EP – high risk ofdKa (diabetic Ketoacidosis) or HHs (Hyperosmolar Hyperglycaemic state).Urinary output will remain high even if patient is hypovolemic.
3. if chronic alcoholism is a potential cause factor, give patient 100 mg thiamine.
Med

4.2
4.2 hypoglycemic emergencyindications◊ For patients with known or suspected hypoglycemia.
Primary interventions including check blood glucose
Blood glucose ≥ 4.0 mmol/L Blood glucose < 4.0 mmol/L
Go to 4.1 Protocol Liquid glucose gel 1 (if conscious)
iv d10W 100 mL fluid bolus if no iv access give Glucagon 2 1 mg iM
Then get vascular access (iv/io)recheck blood glucose
Blood glucose ≥ 4.0 mmol/L Blood glucose < 4.0 mmol/L
iv d10W 100 mL fluid bolus then recheck blood glucose
oral glucose/food once patient alertContact EP and recheck blood glucose q1 hr
Pediatric dosage:iv d10W 5 mL/kg (max 100 mL)Glucagon for child ≤ 20 kg: 0.5 mg IM (or 0.02-0.03 mg/kg/dose) q20 min prn iv rL @ maintenance rate (Table 8.5)
1. Post oral glucose administration, if patient’s LoC improves, iv not required.2. Glucagon often causes nausea and vomiting which may be treated with dimen-
hydrinate 20-50 mg iv or 50-100 mg iM q4-6 hr prn.
4.3
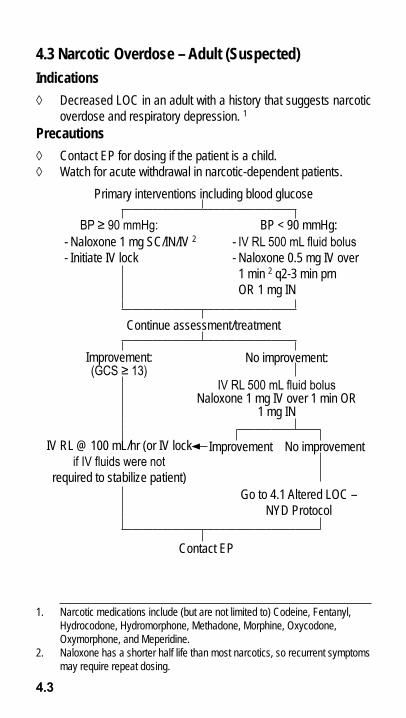
4.3 narcotic overdose – adult (Suspected)indications◊ decreased LoC in an adult with a history that suggests narcotic
overdose and respiratory depression. 1Precautions◊ Contact EP for dosing if the patient is a child.◊ Watch for acute withdrawal in narcotic-dependent patients.
Primary interventions including blood glucose
BP ≥ 90 mmHg: BP < 90 mmHg:- naloxone 1 mg sC/in/iv 2- initiate iv lock
- IV RL 500 mL fluid bolus- naloxone 0.5 mg iv over 1 min 2 q2-3 min prn or 1 mg in
Continue assessment/treatment
improvement: (GCS ≥ 13)
no improvement:
IV RL 500 mL fluid bolusnaloxone 1 mg iv over 1 min or
1 mg in
iv rL @ 100 mL/hr (or iv lock if IV fluids were not
required to stabilize patient)
improvement no improvement
Go to 4.1 altered LoC – nYd Protocol
Contact EP
1. narcotic medications include (but are not limited to) Codeine, Fentanyl, Hydrocodone, Hydromorphone, Methadone, Morphine, oxycodone, oxymorphone, and Meperidine.
2. naloxone has a shorter half life than most narcotics, so recurrent symptoms may require repeat dosing.

4.4
4.4 Seizureindication◊ seizure activity for longer than 5 min. 1
Primary interventions including blood glucose
Midazolam 5 mg in/ iv 2 q5 min up to max 15 mg.or Midazolam 5 mg iM q15 min up to max 15 mg.
May repeat Midazolam q1 hr prn x 2 maximum.
iv rL @ 100 mL/hr
recheck Glucose 3
if BG < 4 mmol/L, go to Hypoglycemia Protocol 4.2
Consider Lorazepam for delayed or long transport 4,5
Contact EP
Pediatric dosage:Child > 2 MOA and ≤ 20 kg: Midazolam 0.1 mg/kg iv over 2 min (titrate to effect) or 0.2 mg/kg iM/in. 5 repeat in 5 min x 1 dose if necessary. Contact EP if seizures persist.iv d10W 5 mL/kg (max 100 mL)Glucagon for child ≤ 20 kg: 0.5 mg IM (or 0.02-0.03 mg/kg/dose) q20 min prn
1. as most seizures are self-limiting, only those that are prolonged or cause respiratory distress need to be treated. Status epilepticus is defined as three successive seizures without fully regaining consciousness in between and/or continuous seizure activity for longer than 5 minutes.
2. if iv already in place, iv should be used as primary route.3. Even if glucose is not initially low, it can become low by this point due to the
energy expenditure caused by the seizure. 4. Continuing seizure may be due to a number of causes including hypoglycemia,
drug withdrawal, or head injury.5. May repeat Midazolam x 1 dose if seizure recurs during transport.

4.5
4.5 antibiotic urgent indication:◊ Penetrating eye injury. 1
indications ◊ open wounds with obvious surface contamination and delayed
transit times (>2hrs). This includes open fractures, open wounds, penetrating injuries to the thoracic cavity.
◊ abdominal injury with suspected/known hollow viscus injury.
contraindications ◊ drug allergies to Moxifloxacin, Penicillin (Cefoxitin), or Clindamy-
cin.Primary interventions
iv lock if able to tolerate Po medication 2 give:
Moxifloxacin 400 mg Po q24 h or
if not able to tolerate Po meds or fluoroquinolone 3 antibiotics and no penicillin allergy give:
Cefoxitin 2 g iv (over 5 min) or iM 4 q8 h orif allergic to penicillin antibiotics5 give:
Clindamycin 600 mg iv (over 30 min) or iM q8 h 6
Monitor patient
Pediatric dosage (over 1 Moa):- Cefoxitin 30 mg/kg iv (over 5 min) or iM 5 q8 h or- Clindamycin 5 mg/kg iv (over 30 min) or iM 7 q8 h
1. antibiotics should be given asaP and preferably within 60 minutes of penetrating eye trauma.
2. avoid Po medication if surgery is anticipated. 3. All end in “floxacin” s: ciprofloxacin, levofloxacin, norfloxacin, ofloxacin,
gatifloxacin and besfloxacin – at time of printing.4. iv administration is preferred. iM administration, when required, should be
into large muscle masses. 5. Penicillins all end in “cillin” such as amoxicillin (amoxil, Clavulin). all Cepha-
losporins start with “Ceph” or “Cef” such as Cephalexin (Keflex), Cefazolin (Ancef) or cefixime (Suprax).
6. Clindamycin is the alternative to Cefoxitin where a patient is allergic to Peni-cillin and cannot take moxifloxacin.

4.6
4.6 agitated Patient indications ◊ anxious or uncontrollable adult, threatening to harm himself, oth-
ers, or otherwise jeopardizing flight safety. cautions ◊ Haloperidol: risk of severe side effects 3. ◊ Use half doses of Haloperidol, Midazolam and Lorazepam in el-
derly patients (above 60 Yoa). Primary interventions 1
Patient uncooperative Patient cooperative
offer Lorazepam 1-2 mg sL
Midazolam 2 mg iM 2 andHaloperidol 5 mg iM 3
if Lorazepam ineffectivemay give Haloperidol 5 mg Po 3
repeat Midazolam or Haloperidol in 30 min if required (may repeat
Midazolam in 10 min if first dose IV) 4
reassure/monitor patient
reassure/monitor patient
1. rule out underlying causes that may include tension pneumothorax, head injury, hypoglycemia, hypotension, drug/alcohol problems, postictal confu-sion, and hypoxia.
2. if iv in place then give Midazolam 1 mg iv q5 min to max 3 doses (unless further ordered by physician).
3. always be prepared to administer diphenhydramine 25-50 mg iv/iM in case of the emergence of extra-pyramidal symptoms or an oculogyric crisis. Haloperidol lowers seizure threshold.
4. For repeat doses of medication, Midazolam should be given first, however if patient is intoxicated because of alcohol or other drugs (remember this could be prescribed medication) Haloperidol is often the best choice. Con-sult with EP if possible to ensure best choice if there is any concern.

4.7
4.7 hiv Post exposure Prophylaxis (PeP)indications◊ Management of significant exposure to fluids capable of transmit-
ting Hiv 1,2,3 on the order of a physician (preferably a CF Flightsurgeon, but consult most available physician to avoid unneces-sary delays).
◊ The PEP starter kit is for sar Tech use only (i.e. do not give topatients except on order of physician).
immediate assessment/actions to be taken: Upon exposure, contaminated clothing should be removed to allow bleeding of the wound. The affected area should then be washed with soap and water. if the eyes, nose or mouth are involved, they should be flushed with copious amounts of water. Prophylactic medications should be initiated quickly (preferably within 2 hours) after significant exposure.
Primary interventionsProphylactic treatment should generally be initiated
within 2 hours post-exposure. Ensure source patient’s identifying information and location is recorded.Specific treatment will be as per physician order which will likely include: 4
raltegravir (isentress) 400mg Po bid 5 andTenofovir and emtricitabine (Truvada) Po once daily 5
(tenofovir 300 mg and emtricitabine 200mg)report to nearest physician on completion of mission
whether or not PEP drugs taken 6.Complete CF 98
1. Significant exposure to blood-borne viruses include infectious fluid expo-sure through a penetrating injury (e.g. needle-stick, bite with broken skin), non-intact skin (e.g. abrasion) or mucous membrane (eyes, nose, mouth).
2. Infectious fluids include any blood, semen, CSF, amniotic fluid, peritoneal fluid, synovial fluid, inflammatory fluid or exudate, breast milk, vaginal secretions, or tissues and organs.
3. Non-infectious fluids (unless visibly contaminated with blood) include stool, urine, tears, nasal secretions and vomitus. no PEP or Mo follow-up required for exposure to these fluids. Must see MO if have significant exposure to saliva as it can transmit Hepatitis B.
4. The medications will be carried for immediate administration. The medications will be adjusted periodically in order to achieve best possible treatment results.
5. With food if possible. 6. Physician will assess risk of Hiv, Hepatitis B, and C and need for prophylaxis.

5
SecTion 5 – environMenTal ProTocolS 5.1 Hypothermia 5.2 Hyperthermia 5.3 High altitude illness 5.4 decompression illness 5.5 Motion sickness
enviro

5.1
5.1 hypothermia indication ◊ Physical collapse or altered mental status as the result of exposure
to cold 1 ◊ Trauma
Primary interventions 2 Handle gently 3
Keep patient horizontal 4
Core temperature
< 30ºC (No Shivering) < 35ºC (Shivering Present)
active rewarming initiate whole bodytruncal areas only 5 rewarming
iv lock 6
Consider 7.4 Urinary Catheterization Procedure 7
Contact EP
see 8.5 Pediatric Table for pediatric maintenance rates and other pediatric indices.
1. also consider hypothermia following trauma, iv administration, uncon-sciousness for an extended period, near drowning, and in the clinical set-tings of Cva, aMs, drug overdose, alcohol intoxication, and dehydration.
2. ventilate the non-breathing, severely hypothermic patient at a rate of 8 -10 resps/min. Take 45 seconds to determine pulselessness at carotid in the severely hypothermic patient prior to starting chest compressions.
3. Patients with severe hypothermia must be handled gently as even minimal movement can induce ventricular fibrillation. Minimize patient movement.
4. If core temperature ≥ 35ºC then horizontal position is not required. 5. active external rewarming consists of applying hypothermia wrap and heat
source. Focus on truncal areas. 6. If IV fluid resuscitation is used IV fluid should be warmed to 40-42ºC7. Catheterization of hypothermic patients to remove cold fluids from body
core is extremely important.
enviro

5.2
5.2 hyperthermia indication ◊ Physical collapse including sudden and severe fatigue, weakness,
nausea, dizziness, light-headedness) or altered mental status (including confusion, unable to say name, date, location), loss of consciousness, seizures/convulsions, irrational behavior, irritability, emotional instability) as the result of exposure to heat. 1
◊ aLTErEd MEnTaL sTaTUs associated with hyperthermia is amedical emergency.
Primary interventionsventilate the non-breathing, severely hyperthermic
patient at a rate of 8-10 resps/min
For elevated core temperature ≥ 40ºC initiate active cooling as follows:• rest in shade• remove clothing (to undergarments)• Wet patient skin and fan• Cool packs on neck, axillae and groin 2
Check blood glucose. if blood glucose < 4.0 mmol/L then go to 4.2 Hypoglycemic Emergency Protocol.
reassess for other causes of persistent decreased LoC
Contact EP 3
• If tolerated, give oral fluids with electrolyte• start iv, give 250 mL rL bolus repeatedly until vs corrected
(max 2 L) 4
• Monitor urinary output. 5
Consider 7.4 Urinary Catheterization Procedure.• observe for seizure. if seizure develops, then treat as per 4.4
seizure Protocol.
1. May occur at moderate temperatures with exertion and/or high humidity. 2. rapid cooling reduces morbidity and mortality. initiate asaP before
transport. 3. if patient is shivering, may request Midazolam order. 4. no more than 2 litres of rL should be administered without lab surveillance
except on the order of a physician. 5. Perform 7.4 Urinary Catheterization Procedure if patient is not fully conscious.

5.3
5.3 high altitude illnessindications ◊ Exposure to altitudes in excess of 8000 ft (2500 m) and signs
or symptoms of acute Mountain sickness (aMs), High altitudePulmonary Edema (HaPE), or High altitude Cerebral Edema(HaCE). 1
Precautions ◊ Patients in hypovolemic and/or cardiogenic shock.◊ Consult with physician prior to giving acetazolamide in patients
with sulfa or penicillin allergies.Primary interventions
High-flow O2 and descend 2
aMs 3 HaPE 4 HaCE 5
acetazolamide 500 mg Po
nifedipine 10 mg Po/sL
dexamethasone 8 mg iv/iM/Po
Contact EP salbutamol 5 mg by nebulizer or
equivalent by Mdi 6if symptoms worsen despite treatment start
dexamethasone 4 mg Po/iM/iv q6 hr
Contact EP Contact EP
repeat acetazolamide
250 mg Po q12 hr prn
repeat nifedipine10 mg Po q4 hr prn
repeat dexamethasone4 mg Po/iv/iM/
q6 hr prn
iv rL @ 100 mL/hrConsider 7.4 Urinary Catheterization Procedure if not voiding.
Monitor vitals and urinary output

5.3
1. Unacclimatized rescuers may take prophylactic acetazolamide 500 mg Po x 1 dose then 250 mg Bid. Where heavy exertion is expected, dexametha-sone 4 mg Po q6 hr may be used prophylactically by sar Techs. Fluid intake must increase when taking acetazolamide to avoid dehydration.
2. descend to < 6500 ft (2000 m) above sea level asaP. if not able to descend this much a descent of as little as 1500 – 3000 ft (500-1000 m) may be sufficient. If immediate descent is not possible, treat on scene. Pul-monary edema or neurologic signs (decreased LoC or ataxia) are reasons for emergency descent.
3. signs and symptoms of aMs include the presence of headache and at least one of the following: anorexia, nausea, vomiting, fatigue, weakness, dizziness, lightheadedness, or difficulty sleeping in the setting of a recent gain in altitude.
4. signs and symptoms of HaPE include at least two of the following: soB at rest, cough, weakness/decreased exercise performance, or chest tightness/congestion, plus at least two of the following: crackles/wheezing in at least one lung field, central cyanosis, tachypnea, tachycardia or bradycardia < 66 bpm).
5. signs and symptoms of HaCE include mental status changes and/or ataxia in a person with signs and symptoms of aMs or the presence of both mental status changes and ataxia in a person without signs and symp-toms of aMs. Patients may exhibit signs of urinary retention and require catheterization.
6. if available and patient load permits administer by Mdi/spacer (BvM with Mdi adapter): 4-8 puffs (100 mcg Mdi) q20 min prn for symptoms otherwise use nebulized meds. Frequency of dosing may be adjusted in accordance with symptoms and onset of adverse effects, however, at least q6 hr is usually required to control symptoms. all nebulizer doses must be in no less than 5 mL total fluid volume.
5.3 notes

5.4
5.4 decompression illness indications ◊ For patients with a history of : sCUBa diving, rapid decompres-
sion 1 or exposure to extreme altitude within 48 hours of the onset of symptoms that cannot be fully explained by incurred trauma ora previously known medical problem.
Primary interventions
100% O2 via BvM with tight seal 2
Treat all life-threatening medical conditions 3
initiate warm iv rL 500 mL bolus then run @ 100 mL/hr 4
Keep patient warm/comfortable in supine position
initiate transport to nearest hyperbaric chamber 5, 6
Complete rapid-neuro assessment
Contact advanced diving Mo/Hyperbaric Physician or Flight surgeon
1. decompression illness (dCi) includes both decompression sickness (dCs) and arterial Gas Embolism (aGE). Both conditions are treated in the same fashion and symptoms may include joint pain, skin mottling, headache, visual disturbance, numbness, weakness, paralysis, confusion, vertigo, soB, cough, chest pain, and/or loss of consciousness.
2. Focus on oxygenation to achieve highest possible o2. 3. in addition to dCi, life threatening medical conditions associated with
sCUBa diving include myocardial infarction, bronchospasm & asthma exacerbation, pneumothorax, trauma, hypoglycemia and hypothermia.
4. see 8.5 Pediatric Table for pediatric maintenance rates and other pediatric indices.
5. Maintain cabin pressure at sea level if possible or at lowest possible altitude. 6. divers alert network (dan) Emergency Hotline (919) 684-8111 has a list of
chambers.

5.5
5.5 Motion Sickness indications ◊ For patients or passengers exhibiting signs/symptoms of motion
sickness 1
Motion sickness in a patient or aircraft passenger 2
dimenhydrinate 50 -100 mg Po q4-6 hr prn 3
if unable to tolerate oral medication give dimenhydrinate 50 mg iM q4 hr prn 3
iv rL 100 mL/hr prn
Pediatric dosage (over 2 Yoa):- 2-6 Yoa dimenhydrinate 25 mg Po q6-8 hr prn- 6-12 Yoa dimenhydrinate 50 mg Po q6-8 hr prn- 12+ Yoa dimenhydrinate 50 mg Po q4-6 hr prn- if unable to tolerate oral medication give dimenhydrinate 1 mg/kg iM 4 - iv rL as per 8.5 Pediatric Table
1. Motion sickness medications are not approved for use in CF aircrew. 2. Signs and symptoms of motion sickness include malaise, warmth, flushing,
salivation, swallowing, headache, abdominal awareness or discomfort, lethargy, apathy, nausea, pallor, sweating, retching, and/or vomiting.
3. If patient ≥ 60 yrs old then consider giving half dose.4. not to be repeated except on the advice of a physician.

notes:

Index
SecTion 6 – druG MonoGraPhS This section contains the drug monographs for: 6.1 acetaminophen 6.2 acetazolamide 6.3 acetylsalicylic acid 6.4 Bacitracin & Polymyxin B 6.5 Cefoxitin 6.6 Clindamycin 6.7 dexamethasone 6.8 dextrose 6.9 dimenhydrinate 6.10 diphenhydramine 6.11 Epinephrine 6.12 Glucagon 6.13 Glucose Gel 6.14 Haloperidol 6.15 ibuprofen 6.16 ipratropium Bromide 6.17 Ketorolac 6.18 Lidocaine6.19 Lorazepam6.20 Midazolam 6.21 Morphine 6.22 Moxifloxacin 6.23 naloxone 6.24 nifedipine 6.25 nitroglycerin 6.26 normal saline6.27 oxygen 6.28 PEP 6.29 ringers Lactate6.30 salbutamol6.31 Thiamine 6.32 Tranexamic acid
druG

Ace -
6.1 acetaminophen (Tylenol, atasol, Tempra) indications: 3.5 Pain. contraindications: Hypersensitivity to acetaminophen, known G6Pd deficiency, or liver failure. Precautions: May cause severe liver toxicity in overdose. Use cautiously in patients with alcoholic liver disease. Excessive alcohol intake can increase risk of acetaminophen-induced liver toxicity. adverse effects: Uncommon, as < 1% patients experience any adverse effects. Pharmacology: onset of action < 1 hour; time to peak effect (oral dosing) = 10-60 minutes; t½ (half-life) = 1-3 hours; duration of action = 4-6 hours. dosage and administration: ◊ adults/Children over 12 Yoa: 650-1000 mg Po q4-6 hr prn, max
4000 mg q24 hr.◊ Children 12 Yoa and under: 10-15 mg/kg Po q4-6 hr prn
druG

Ace - ASA
6.2 acetazolamide (diamox) indications: 5.3 High altitude illness (aMs). Contraindications: Hypersensitivity to acetazolamide, sulfonamides, or penicillin. History of liver disease (see Precautions), or severe kidney dysfunction. Precautions: Use in impaired liver function may result in coma. May cause hyperglycemia. Consult EP if history of allergy to: sulfonylureas, penicillin, thiazide diuretics (hydrochlorothiazide, indapamide, metolazone, chlorthalidone), and loop diuretics (furosemide, ethacrynic acid). avoid the use of acetazolamide if previous reaction was severe. adverse effects: More than 10% of individuals will experience malaise, unusual drowsiness or weakness, nausea, vomiting, diarrhea, metallic taste, polyuria, numbness, tingling, or burning in hands, feet, fingers, toes, mouth, lips, tongue, or anus. Convulsions and/or hyperglycemia have been noted in less than 1% of individuals. Pharmacology: Time to peak effect = 1-4 hours; t½ (half-life) = 2.4-5.8 hours; duration of action = 8-12 hours. dosage and administration: ◊ aMs: 500 mg Po initially followed by 250 mg Po q12 hr◊ Prophylaxis: 125-500 mg Po q12 hr for un-acclimatized rescu-
ers working at high altitudes. Generally should start taking 48 hrsprior to ascent and continue as needed. For rapid ascent, 500 mg Po q12 hr is recommended.
6.3 acetylsalicylic acid (aSa, aspirin) indications: 1.1 Cardiac Chest Pain. contraindications: Hypersensitivity to asa or other anti-inflammatories, bleeding disorder or active gastrointestinal bleeding. not for use in children (under 12 Yoa).Precautions: Patients with a history of asthma and/or nasal polyps. adverse effects: Mainly gastrointestinal complaints, nausea and heartburn. dosage and administration: ◊ Chewable asa 160 mg Po (single dose only)

Bac - Cef
6.4 Bacitracin & Polymyxin B (Polysporin, Polytopic) indications: 3.3 1st degree burns or burns to face. contraindications: Hypersensitivity to either component. Precautions: application to extensive open areas of skin may increase systemic absorption. adverse effects: rash and pruritis. dosage and administration: ◊ apply topically to affected areas 3-4 times daily.
6.5 cefoxitin indications: 4.5 antibiotic. contraindications: Hypersensitivity to cephalosporins and/or penicillins. Precautions: review with EP before using in patients with history of penicillin allergy, especially anaphylaxis or urticaria.adverse effects: diarrhea and mild headache. rash, urticaria and/or pruritis are manifestations of allergic reactions which can be severe or precede anaphylaxis. dosage and administration: ◊ adults: 2 gm iM into two large muscle masses (2 gm Cefoxitin
powder mixed with 4 mL sterile water; 1g max/muscle). For ivinjection, dilute with 10-20 mL sterile water (or d10W or rL) andgive over 3-5 min.
◊ Children (>1 Moa): 30 mg/kg iM into a large muscle mass (1 gmCefoxitin powder mixed with 2 mL sterile water). For iv adminis-tration, mix 1 gm dose in 10 mL sterile water ( d10W or rL), butgive only 30 mg/kg over 3-5 min.

Cli - Dex
6.6 clindamycin (dalacin-c) indications: 4.5 antibiotic. contraindications: Hypersensitivity to clindamycin, liver impairment. do not use in infants < 1 month old (neonates). Precautions: Use with caution in patients with history of Ulcerative Colitis or Crohn’s. adverse effects: Hypotension, nausea, vomiting, diarrhea and abdominal pain, urticaria and rashes, thrombophlebitis, irritation at injection site. Pharmacology: Time to peak effect (iM) = 1-3 hr; t½ = 1.6-5.3 hr (average 2-3 hr). dosage and administration: ◊ adults: 600 mg iv (over 30 min) or iM◊ Children (> 1 Moa): 5mg/kg iv (over 30 min) or iM
6.7 dexamethasone (decadron, dexasone) indications: 2.1 soB with History of asthma/CoPd, 2.3 anaphylaxis/anaphylactic shock – adult and Child, 5.3 High altitude illness (aMs & HaCE).contraindications: Hypersensitivity to dexamethasone. Precautions: Use cautiously in patients with diabetes or history of peptic ulcer. adverse effects: nausea, vomiting, insomnia, nervousness, euphoria, hyperglycemia, arthralgia, epistaxis. Pharmacology: Time to peak effect (oral) = 1-2 hr, (iM) ≈ 8 hr; t½ (half-life) = 1.8-3.5 hr; biological t½ = 36-54 hr; duration of metabolic action = 72 hr. dosage and administration: Parenteral administration usually reserved for patients unable to swallow the oral tablets. ◊ HaCE: 8 mg Po/iv/iM initially followed by 4 mg Po/iv/iM q6 hr◊ aMs: 4 mg Po/iv/iM q6 hr◊ asthma and anaphylaxis by physician order. Usual adult dose: 8
mg Po/iv/iM initially followed by 4 mg Po/iv/iM q6 hr.

D10W - Dim
6.8 dextrose (d10w)indications: 3.1 Hemorrhagic shock, 4.2 Hypoglycemic Emergency, 4.4 seizure, and in children.contraindications: Hyperglycemia. Precautions: Contact EP before administering to a patient with suspected head injury. dosage and administration: ◊ adult: 100 mL iv bolus x 2 prn blood glucose < 4.0 mmol/L, then
100 mL/hr (Max 250 mL)◊ Child: 5 mL/kg iv bolus x 2 prn blood glucose < 4.0 mmol/L (Max
100 mL)
6.9 dimenhydrinate (Gravol) indications: 1.1 Cardiac Chest Pain, 3.5 Pain, 4.2 Hypoglycemic Emergency, 5.5 Motion sickness. contraindications: Hypersensitivity to dimenhydrinate, do not administer to children under 2 Yoa. Precautions: overdose can cause seizure or respiratory depression. Be prepared to assist ventilations or initiate 4.4 seizure Protocol. adverse effects: drowsiness, dizziness, lassitude, excitement (children), dry mouth, nausea. dosage and administration: Cardiac Chest Pain: ◊ adults: 25-50 mg (diluted in rL to a total of 10 mL) iv over 2 min
or 50-100 mg iM q4 hr prn◊ Elderly: decrease dose by ½ for patients 60 Yoa or older. May be
safely combined with the first dose of Morphine but not with sub-sequent doses (its longer half-life would cause it to accumulateinto a possible overdose).
Pain and Motion sickness:◊ adults: 25-50 mg iv over 2 min (diluted in rL to a total of 10 mL)
or50-100 mg iM or 50-100 mg Po q4-6 hr prn. Maximum dose 400mg in 24 hrs.
◊ Child: 1 mg/kg iM or◊ Child over 12 Yoa: 50 mg Po q4-6 hr prn◊ Child 6-12 Yoa: 25-50 mg Po q6 hr prn (Max 150 mg in 24 hr)◊ Child 2-6 Yoa: 12.5-25 mg Po q6 hr prn (Max 75 mg in 24 hr)◊ Elderly (> 60Yoa): decrease dose by ½ as this population can
be more susceptible to side effects.

Dip -
6.10 diphenhydramine (Benadryl, allerdryl, allernix) indications: 2.3 anaphylaxis/anaphylactic shock – adult and Child, 4.6 agitated Patient. contraindications: Hypersensitivity to diphenhydramine or acute asthma. do not use in neonates. Precautions: Use with caution in patients with angle-closure glaucoma, patients with urinary obstructions, elderly, and may cause paradoxical excitation in children. adverse effects: Hypotension, tachycardia, palpitations, drowsiness, dizziness, coordination difficulties, headache, nervousness, paradoxical excitement, insomnia, euphoria, confusion, nausea, vomiting, diarrhea, dry mouth and mucous membranes, urinary retention, urinary frequency, difficulty urinating, tremor, parasthesia, blurry vision. dosage and administration: anaphylaxis/anaphylactic shock: ◊ adults: 25-50 mg iM/iv q2-4 hr prn (Max dose 400 mg/day)◊ Children: 1 mg/kg iM/iv q6-8 hr prn (Max dose 5 mg/kg/day)Hostile/violent patient (and other indications): ◊ adult dose: 25-50 mg iM/iv q6-8 hr prn (Max dose 400 mg/day)◊ Elderly (> 60 Yoa): decrease dose by ½, as this population can
be more susceptible to side effects.
Epi -
6.11 epinephrine (adrenaline, epipen, epipen Jr) indications: 2.1 soB with a History of asthma/CoPd, 2.3 anaphylaxis/anaphylactic shock – adult and Child. contraindications: There are no contraindications to giving epinephrine for a life threatening allergic response such as anaphylaxis. adverse effects: Tachycardia, arrhythmias, angina, flushing, anxiety, tremor, headache, dizziness, nausea and vomiting (in children), dry mouth, acute urinary retention in patients with bladder outflow obstruction, weakness and trembling, wheezing and dyspnea, and increased diaphoresis. Precautions: Use with caution in elderly, diabetes mellitus, cardiac arrhythmias, cardiovascular disease or thyroid disease. Watch for tachycardia and hypertension, which may compromise a patient with poor cardio-pulmonary reserve. Be prepared to go to 1.1 Cardiac Chest Pain Protocol. dosage and administration: ◊ adults: Epinephrine 0.3 mg sC/iM q5 min to a max of 3 doses.◊ Children: Epinephrine 0.01 mg/kg (Max 0.3 mg) sC/iM q5 min to
a max of 3 doses.nB: The preferred site for administration of Epinephrine sC or iM is in the thigh (use the shoulder as an alternative). Massage the site after administration to promote localized circulation of blood. storage note: Protect medication from light. MuST noT Be Given iv – MaY cauSe cardiac arreST

Glu - Glu
6.12 Glucagon (GlucaGen) indications: 4.2 Hypoglycemic Emergency (no timely iv/io access), 4.4 seizure and may be required in 2.3 anaphylaxis/anaphylactic shock – adult and Child. contraindications: Hypersensitivity to Glucagon or its components, insulinoma, pheochromocytoma. Precautions: supplemental carbohydrates should be given to patients who respond to Glucagon for severe hypoglycemia to prevent secondary hypoglycemia. Monitor blood glucose levels closely. adverse effects: Hypotension, hypertension, and tachycardia. nausea and vomiting (may be treated with dimenhydrinate 25-50 mg iv or 50 mg iM or 50-100 mg Po). Pharmacology: onset of action (iM) = 30 min; duration of action (glucose elevation) = 60-90 min; t½ (half-life) = 8-18 min. dosage and administration: Glucagon solutions should not be used unless they are clear and of a water-like consistency. ◊ adults and children > 20 kg: 1 mg iM q20 min prn◊ Children ≤ 20 kg: 0.5 mg IM (or 0.02-0.03 mg/kg/dose) q20 min
prn
6.13 Glucose Gel (insta-Glucose)indications: 4.2 Hypoglycemic Emergency.contraindications: nil. Precautions: not to be administered to an unconscious patient. dosage and administration: ◊ apply up to 1 tube to inside lip and cheeks. rub on and do not
apply as a “clump” if any airway compromise.

Hal -
6.14 haloperidol (haldol) indications: 4.6 agitated Patient. contraindications: Hypersensitivity to haloperidol, severe cardiac or liver disease. Patients with severe Cns depression, a history of spastic disorders, or Parkinson’s. Precautions: Caution with patients with hemodynamic instability, risk of orthostatic hypotension, history of seizure disorder, and severe hepatic or renal impairment. May alter temperature regulation. Use with caution in the elderly; observe for lethargy. due to the fact that the elderly may lose thirst sensation, monitor for signs of dehydration. Contact EP in the event of hypotension. adverse effects: Hypotension, hypertension, tachycardia, arrhythmias, seizure, hypoglycemia, tremors, anxiety, spasms (oculogyric crisis), altered central temperature regulation and heat stroke, drowsiness, vertigo, headache, confusion, nausea, vomiting, dry mouth, urinary retention, bronchospasm. Pharmacology: onset of action (sedation) < 1 hr; duration of action = 2-4 hr; t½ (half-life) = 20 hr; time to peak = 20 min. dosage and administration: adults: ◊ 5 mg iM. May repeat x 1 dose after 10 min if required (best to
wait for approx 45 min until peak biologic effect before repeatingdose if possible), or
◊ 5 mg Po. May repeat x 1 dose in 1 hr then q12 hr prn. May beadministered concurrently with Midazolam iM as per 4.6 agitatedPatient Protocol.
Elderly (>60 Yoa): ◊ 2 mg iM. May repeat x 1 dose after 30 min if required (best to
wait for approx 45 min until peak biologic effect before repeatingdose if possible), or
◊ 2.5 mg Po. May repeat x 1 dose in 1 hr if required.nB: storage note: Protect from light.

Ibu -
6.15 ibuprofen (advil, Motrin) indications: 3.5 Pain. (drug of choice for frostbite) contraindications: Hypersensitivity to asa, ibuprofen, or other NSAIDs, peptic ulcer, or active inflammatory bowel disease. Precautions: Use with caution in patients with impaired renal function, heart failure, liver dysfunction, those taking diuretics and anticoagulants, the elderly, those with systemic lupus erythematosus. do not combine with other nsaids. do not give within 8 hrs of ketorolac. adverse effects: nausea, diarrhea, epigastric pain, abdominal cramps or pain, heartburn, bloating or flatulence, dizziness, headache, nervousness, rash, pruritis, tinnitus, anemia, decreased appetite, edema, or fluid retention. Pharmacology: onset of action < 1 hr; time to peak effect (oral) = 1-1.5 hr; t½ (half-life) = 1.8-2.0 hr; duration of action = 4-6 hr. dosage and administration: ◊ adults: ibuprofen 600 mg Po q4-6 hr prn (Max 2400 mg/day)

Ipr -
6.16 ipratropium Bromide (atrovent)indications: 2.1 soB with History of asthma/CoPd, 2.3 anaphylaxis/anaphylactic shock – adult and Child. contraindications: Hypersensitivity to ipratropium Bromide, atropine or other anticholinergics, or any other aerosol components. Precautions: should not be used for acute episodes of bronchospasm where rapid response is required since the drug has a slower onset of action than adrenergic agonist aerosols (e.g. salbutamol). adverse effects: Chest pain/palpitations (3%), hypotension (< 1%), mydriasis (< 1%). Constipation, diarrhea, vomiting, headache, dizziness, dry mouth and throat. Pharmacology: onset of action = 5-15 min; time to peak effect = 1-2 hr; t½ (half-life) = 2 hr; duration of action ≈ 8 hr. dosage and administration: nebulized inhalation solution: ◊ adults: 0.5 mg (diluted in sterile water or ns to a total of 5 mL)
q20 min x 3 doses then prn for urgent patients. For emergent/critical patients doses may be given back to back.
◊ Children (< 12 Yoa): 0.125-0.250 mg q20 min x 3 doses then prn for urgent patients. For emergent/critical patients doses may be given back to back.
Metered dose inhaler (Mdi): adults and children: ◊ Emergency – Mdi 4-8 metered doses for each dose with doses
given back to back until patient improves (alternating with primary treatment: back to back salbutamol)
◊ Urgency – Mdi 4-8 metered doses q20 min ◊ standard – 2-4 metered doses by Mdi q4-6 hr

Ket -
6.17 Ketorolac (Toradol) indications: 3.5 Pain. contraindications: Hypersensitivity to Ketorolac or other nsaids, active or recent history of peptic ulcer disease or Gi bleeding. Uncorrected hypovolemic shock, renal impairment or insufficiency, patient taking pentoxifylline (Trental), and impending or actual labour and delivery. Precautions: Use with caution in patients with active bleeding (inhibits platelet function), asthma, hypertension, hepatic impairment (for repeat doses), and in those taking concurrent nsaids. adverse effects: serious gastrointestinal (Gi) effects including bleeding, ulceration and/or perforation of the stomach, small intestine, or large bowel. Headache (17%), GI pain/nausea (13%), hypertension, increased bleeding time, tinnitus, dizziness, drowsiness, pruritis, rash, local injection site pain. Pharmacology: onset of action = 10 min; time to peak effect = 2-3 hr; t½: = 2-6 hr (increased 30-50% in elderly, 300% in renal impairment); duration of action = 6-8 hr. dosage and administration: adults > 50 kg: ◊ 30 mg iM q6 hr (Max 120 mg/day)◊ 30 mg iv q6 hr (Max 120 mg/day)◊ Elderly and adults ≤ 50 kg:◊ 30 mg iM x 1 dose followed by 15 mg iM q6 hr prn (Max 60 mg/
day)◊ 15 mg iv x 1 dose followed by 15 mg iv q6 hr prn (Max 60 mg/
day)Children (2-16 Yoa): do not exceed adult doses. ◊ 0.5 mg/kg iv x 1 dose followed by 0.25-0.50 mg/kg iv q6 hr prn
(Max 90 mg/day x 2 days)NB: Dosage adjustments in elderly (≥ 60 YOA), renal insufficiency, or low body weight (≤ 50 kg). All these groups have an increased incidence of Gi bleeding, ulceration and perforation. Maximum combined duration of treatment (for parenteral and oral) is 5 days. Limited pediatric studies.

Lid -
6.18 lidocaine 2% Preservative Free (Xylocaine)indications: 7.5 EZ-io (intra-osseous iv) – For conscious or semi-conscious patients (GCs > 6) where clinical situation allows.contraindications: Patient with confirmed hypersensitivity to local anesthetics of the amide type, patients with myasthenia gravis, impaired cardiac conduction, and uncorrected hypovolemia or untreated severe hemorrhage/severe shock.Precautions: intravascular injection or over dosage may result in heart block, myocardial depression, bradycardia, anxiety, apprehension, restlessness, confusion, tremors, convulsions, respiratory arrest, or cardiovascular collapse.adverse (or Side) effects: Usually a result of improper technique, inadvertent iv, excessive dosage or rate of administration, or injection into highly vascular tissue.cardiovascular: Bradycardia, heart block, decreased myocardial contractility (uncommon); arrhythmias, cardiac arrest, death (rare).cnS: restlessness, irritability, tremor, sedation, paresthesia or dizziness, occasionally. seizure, coma, respiratory arrest, and death are rare. wiTh iv/io adMiniSTraTion Slurred SPeech and decreaSed loc iS coMMon and TRANSIENT.hypersensitivity: dermatologic reactions, edema, asthma, anaphy-laxis and death. True allergy is rare.Pharmacology: onset of action (iv) = 45-90 secs; duration of action = 10-20 mins.dosage and administration:Adults and Children ≥ 12 YOA:◊ 40 mg IO over 2 min prior to flush. May be followed by 20 mg IO
over 1 min if pain relief is inadequate and patient condition allowstemporary cessation of iv therapy.
Children > 3 Yoa:◊ 0.5 mg/kg slow push prior to flushor use following table
(Continued on next page)

Lid - Lor
lidocaine dosing using Preservative Free 2% Solution (20 mg/ml)◊ newborn = 0.1 mL (2 mg)◊ 1 Yoa = 0.2 mL (4 mg)◊ 2 Yoa = 0.3 mL (6 mg)◊ 4 Yoa = 0.4 mL◊ 6 Yoa = 0.5 mL◊ 10 Yoa = 0.8 mL◊ >10 Yoa = 1 mL◊ Adult ≥ 12 YOA = 2 mL (1 mL in elderly, frail or cardiac patients)
6.19 lorazepam (ativan)indications: 4.4 seizure, 4.6 agitated Patient. contraindications: Hypersensitivity to Lorazepam or its components. Use of benzodiazepines solely for sedation is contraindicated during pregnancy. Precautions: May cause severe respiratory depression. Use caution with the elderly and patients taking Cns depressants (e.g. Morphine or other narcotics – hypotension risk). should not use in shock, coma, or acute alcohol intoxication. adverse effects: decreased respiratory rate and tidal volume, hypotension, drowsiness, over-sedation. Pharmacology: onset of action (sL) = 20-60 min, (Po) = 1-3 hr; t½ (half-life) = 12-15 hr; duration of action = 10-16 hr. dosage and administration: Adults and Children ≥ 12 YOA: ◊ 1-2 mg sL (preferred) or Po q2 hr (Max 6 mg/day). note that 1
mg is the standard initial dose and 2 mg should be used for larger patients (> 70 kg) and for repeat doses where a higher dose hasbeen shown to be needed.
nB: Lorazepam may be used in 4.4 seizure Protocol because of its long duration of action compared to Midazolam. ideally, it is used only after seizures have been controlled with Midazolam when transport is delayed. if used for a seizure patient, airway must be secure (i.e. conscious patient able to protect own airway or patient with advanced airway in place). not for use in children under 12 Yoa.

Mid -
6.20 Midazolam (versed) indications: 4.4 seizure, 4.6 agitated Patient, 5.2 Hyperthermia. contraindications: Hypersensitivity to Midazolam or its components including benzyl alcohol. Use of benzodiazepines solely for sedation is contraindicated during pregnancy.Precautions: May cause severe respiratory depression, respiratory arrest or apnea. Use caution with the elderly, patients with hepatic or renal impairment, and patients taking Cns depressants (e.g. Morphine or other narcotics – hypotension risk). May cause hypotension especially in pediatric patients or patients who already have some hemodynamic instability. should not use in shock, coma, or acute alcohol intoxication. adverse effects: decreased respiratory rate and tidal volume (> 10%), hypotension (1-10%), drowsiness, over-sedation, nausea, vomiting, hiccups, pain at injection site. Pharmacology: onset of action (iM) = 15 min, (iv/io) = 1-5 min, in (intranasal) = 5-10 min, t½ (half-life) = 1-4 hr (prolonged with cirrhosis, CHF, obesity and elderly); duration of action = 2-6 hr. dosage and administration: Adults and Children ≥ 20 kg: ◊ status Epilepticus: 5 mg iv/in x 1 dose then 5 mg q5 min until
seizure stops (Usually 5-15 mg).◊ agitation: 2 mg iM. May repeat x 1 dose after 10 min. note that
dose should be reduced by 30% if narcotics or other CNS depres-sants have been used.
Children < 20 kg and > 2 Moa: ◊ status Epilepticus: 0.1 mg/kg iv q5 min until seizure stops (Max
0.6 mg/ kg) or 0.2 mg/kg in, q5 min until seizure stops. Max 2doses for iv or in.
intranasal administration (in): ½ dose in each nostril.

Mor -
6.21 Morphineindications: 1.1 Cardiac Chest Pain, 3.5 Pain. contraindications: Hypersensitivity to Morphine, severe respiratory distress, severe hypotension, head injuries and decreased LoC. Precautions: Use with caution in pregnancy, elderly patients, those with pre-existing respiratory conditions (CoPd) and those patients that are intoxicated. nB: if severe respiratory depression or decreased LoC refer to 4.3 narcotic overdose – adult (suspected). if the patient becomes hypotensive, ensure supine, head down position, legs elevated and consider fluid bolus. adverse effects: Hypotension, dizziness, sedation and euphoria, nausea and vomiting, respiratory depression. Pharmacology: onset of action (iM/sC) = 20 min, (iv) = 1-5 min, (Po) < 1 hr; duration of action = 2-3 hr; t½ (half-life) = 2-4 hr; time to peak = 0.5-1 hr. dosage and administration: adults:◊ Cardiac Chest Pain: 2.5 mg iv/io over 1 min. repeat q5 min until
pain relief. Max dose 15 mg. Cycle may be repeated q2 hr. if noiv access, 10 mg sC/iM q2 hr.
◊ Pain: 2.5-5 mg iv/io over 1 min. repeat q5 min prn. Max dose15 mg. May repeat cycle q ½ hr prn. diluting 1 mL of 10 mg/ mLMorphine with 9 mL rL for a total volume of 10 mL makes dosingeasier. if no iv access, 10/15 mg sC/iM q1½ hr.
Children: ◊ Patient < 50 kg: 0.1 mg/kg/dose iv/io over 1 min q5 min (max 3
doses in 30 min) prn may repeat X 1 cycle.◊ Patient > 50 kg same dosing as adult.

Mox - Nal
6.22 Moxifloxacin (Avelox) indications: 4.5 antibiotic. contraindications: Hypersensitivity to Moxifloxacin hydrochloride or other quinolones and for patient under 18 Yoa. Precautions: serious hypersensitivity and/or anaphylactic reactions have been reported in patients receiving Moxifloxacin. Use caution in patients with known or suspected Cns disorders which may predispose to seizures or lower seizure threshold. Concurrent administration of nsaids may increase the risk of Cns stimulation and convulsions. adverse effects: abdominal pain, headache, nausea, diarrhea, vomiting, photoxicity and hypoglycemia. seizures may occur with quinolone therapy. dosage and administration: ◊ adults: 400 mg Po once daily
6.23 naloxone (narcan)indications: 4.1 altered LoC – nYd, 4.3 narcotic overdose – adult (suspected). contraindications: Hypersensitivity to naloxone. Precautions: naloxone may have a half-life as short as 30 min. in the case of narcotic overdose, the patient should be closely observed for a change in mental state. The patient may require further naloxone if the underlying problem is narcotic overdose. Pharmacology: onset of action (iv) = 2-3 min, (in) = 5-15 min, (sC/IM) ≤ 15 min; duration of action ≤ 1 hr (variable); t½ (half-life) = 1 hr. dosage and administration: adults: iv (preferred), iM, in, io or sC may be used if no iv access. ◊ 0.5-1 mg iv. May repeat q2-3 min prn.◊ 1-2 mg sC/iM q2-3 min prn◊ 2 mg in (1 mg per nostril); may repeat in 5 minutes if respiratory
depression persists.Children: iv (preferred), iM, in, io or sC may be used if no iv access.◊ < 5 years or ≤ 20 kg: 0.1 mg/kg/dose (maximum dose: 2 mg);
repeat every 2-3 minutes if needed◊ ≥ 5 years or > 20 kg: 2 mg; if no response, repeat every 2-3 minutesnB:◊ Massage site after sC injection.◊ if no response is observed after 10 mg total, consider other
causes of respiratory depression.

Nif - NTG
6.24 nifedipine (adalat)indications: 5.3 High altitude illness (HaPE).contraindications: Hypersensitivity to nifedipine. Precautions: Use with caution in patients with heart disease. Contact EP if possible. adverse effects: Facial flushing, hypotension, palpitations and lower extremity edema, headache, nausea and vomiting. Pharmacology: onset of action [ir (immediate release) capsule] = 20 min; duration of action = 4-8 hr; t½ (half-life) = 2-5 hr. dosage and administration: ◊ adults: nifedipine ir (immediate release) capsule 10 mg Po q4
hr prn.
6.25 nitroglycerin (nTG, nitroglycerin Spray) indications: 1.1 Cardiac Chest Pain. contraindications: Hypersensitivity and severe hypotension. due to hemodynamic concerns, nitrates of any kind should not be used within 24 hr of Viagra (sildenafil), within 48 hr of Cialis (tadalafil), or within 24 hr of Levitra (vardenafil). Precautions: if considering nTG and Hr <50 or >100 bpm sT’s must contact physician. Watch for hypotension. Monitor BP frequently.Pharmacology: onset of action (sL spray) = 1-2 min; peak effect = 4-10 min; duration of action = 30-60 min; t½ (half-life) = 1-4 min. adverse effects: Hypotension, headache, fainting, dizziness, weakness, face flushing, burning sensation of the tongue. dosage and administration: ◊ nitroglycerin spray 0.4 mg sL q5 min (max 3 doses every 30
min). if administering the patient’s own nitroglycerin tablets, place them under the tongue.
NS - O2
6.26 normal Saline (nS, 0.9% Sodium chloride) indications: dKa – any patient with blood glucose > 20 mmol/L. alternate for: 1.1 Cardiac Chest Pain, 1.2 Cardiac arrest – aEd, 1.3 Post-arrest stabilization, 1.4 discontinue resuscitation, 3.1 Hemorrhagic shock, 3.2 Tranexamic acid (TXa), 3.5 Pain, 4.1 altered LoC – nYd, 4.2 Hypoglycemic Emergency, 4.3 narcotic overdose – adult (suspected), 4.4 seizure, 4.5 antibiotic, 5.1 Hypothermia, 5.3 High altitude illness, 5.4 decompression illness. contraindications: Pulmonary edema. Maintenance Rates (unless otherwise specified): ◊ adults: 100 mL/hr◊ Children: see 8.5 Pediatric Table for maintenance rates and other
pediatric indices.
6.27 oxygen (o2) indications: all Protocols. contraindications: nil. Precautions: Caution in those patients with CoPd (target o2 sat at 92%), as it may depress respiratory drive. These patients require frequent monitoring. Be prepared to assist ventilation if required. dosage and administration: ◊ “100% O2” – Use Bag-valve-Mask (BvM) sealed to face.◊ “High Concentration o2” – Use face mask with reservoir bag.
Oxygen flow enough to keep reservoir bag inflated.◊ “High Flow o2” – 6-10 L/min by simple face mask.◊ “Low Flow o2” – 2-4 L/min by nasal prongs.
PEP -
6.28 PeP (Post exposure Prophylaxis for hiv)indications: 4.7 Hiv Post Exposure Prophylaxis (PEP). contraindications: Hypersensitivity to the medication(s).adverse effects: ◊ TDF: Renal insufficiency, Fanconi Syndrome, osteomalacia,
osteoporosis, asthenia, headache, diarrhea, nausea, vomiting,flatulence.
◊ raL: nausea, headache, diarrhea, pyrexia, muscle weakness,rhabdomyolysis and CPK elevation.
◊ FTC: Hyperpigmentation/skin discoloration, severe acute exac-erbation of hepatitis in patients co-infected with HBv when thismedication is discontinued.
dosage and administration: anti-retroviral tablets (arT) should be started within 2 hours of exposure and taken for 28 days total. The PEP starter kit contains 5 days of medication. Medications are taken with meals. Mo will prescribe the remaining 23 days of therapy if required. Therapy consists of: ◊ raltegir (isentress; raL) 400 mg Po bid and◊ Tenofovir dF (viread; TdF) 300 mg Po once daily and◊ Emtricitabine (Emvtriva; FTC) 200 mg Po once dailynB: These medications are to be used by sar Techs on themselves if required, and are not to be administered to patients. dosage forms may vary as some of these medications are available as combined products. These medications can cause significant symptoms in some people. This is the recommended drug regimen approved by the CF Pharmacy and Therapeutics Committee and the directorate of Force Health Protection. if sar Tech chooses to take the medication while on flight then they are immediately grounded and must be removed from aircrew specific duties. They can however continue to provide patient care to complete the mission. if the risk of infection is such that PEP is considered necessary, delay in taking the medication is to be avoided.
6.29 ringers lactate (rl)indications: 1.1 Cardiac Chest Pain, 1.2 Cardiac arrest – aEd, 1.3 Post-arrest stabilization, 1.4 discontinue resuscitation, 3.1 Hemorrhagic shock, 3.2 Tranexamic acid (TXa), 3.3 Burns, 3.5 Pain, 4.1 altered LoC – nYd, 4.2 Hypoglycemic Emergency, 4.3 narcotic overdose – adult (suspected), 4.4 seizure, 4.5 antibiotic, 5.3 High altitude illness, 5.4 decompression illness. contraindications: Pulmonary edema. adverse effects: risk of causing pulmonary edema especially in pediatric, frail and elderly patients.Use with caution and consult EP if large volume recusisitation is required in severe hypothermia (cold liver may not be able to metabolize the lactate). Maintenance Rates (unless otherwise specified): ◊ adults: 100 mL/hr◊ Children: see 8.5 Pediatric Table for maintenance rates and other
pediatric indices.
RL -

6.30 Salbutamol (ventolin) indications: 2.1 soB with a History of asthma/CoPd, 2.3 anaphylaxis/anaphylactic shock – adult and Child, 5.3 High altitude illness. contraindications: Hypersensitivity to salbutamol. adverse effects: Palpitations and tachycardia, nervousness, headache and tremor. Pharmacology: onset of action = 5-15 min; duration of action = 3-6 hr; peak effect = 30-60 min. dosage and administration: nebulizer:◊ adults/Children > 12 Yoa: 5 mg nebulized in 5 mL (dilute with
ns if required).◊ Child ≤ 12 YOA: 2.5 mg nebulized in 5 mL (dilute with NS if re-
quired). adjust o2 flow rate to make a mist (approx 6 L/min).Metered dose inhaler (Mdi): adults and Children: ◊ Emergency – Mdi 4-8 (100 mcg/ dose inhaler) metered doses for
each dose with doses given back to back until patient improves◊ Urgency – Mdi 4-8 (100 mcg/ dose inhaler) metered doses q20
min◊ standard – 2-4 (100 mcg/ dose inhaler) metered doses by Mdi
q4-6 hr.
6.31 Thiamine (vitamin B1, Betaxin)indications: 4.2 Hypoglycemic Emergency. contraindications: nil. Precautions: Thiamine is not to be given to children less than 12 years of age. Beware of hypotension risk with iv administration – hence slow administration. dosage and administration: adult: Thiamine 100 mg iv (diluted in 10 mL ns) over 1-2 min or iM.
Sal - Thi

6.32 Tranexamic acid (TXa)indications: 3.1 Hemorrhagic shock, 3.2 Tranexamic acid (TXa)contraindications: Hypersensitivity to tranexamic acid; subarachnoid hemorrhage. Treatment delayed more than three hours after injury. incompatible with solutions containing penicillin.adverse effects: Hypotension (with rapid iv injection), giddiness, allergic dermatitis, diarrhea, nausea, vomiting, blurred vision.Precautions: severe hypotension if infused too quickly.dosage and administration: ◊ 1 gm TXa slow iv injection over 10 min (draw up 1 gm of TXa
(1 gm/10 ml) in a 10 ml syringe then give 1 ml/min over 10 min).◊ Wait one hour and then give 1 ml (1 gm/10 ml) every 60 min for
10 doses.
TXA -

7
SecTion 7 – STandard Medical ProcedureS
7.1 Patient aadvanced airway insertionassessment of suspected spinal injuries
ssessment Model7.2 7.3 7.4 Urinary Catheterization7.5 7.6 7.7 7.8
EZ-io (intra-osseous) Power driver EZ-io needle sets sizeEZ-io insertion sitesTourniquet removal
7.9 Chest decompression (7.10 orogastric (oG) Tube insertion 7.11 Notification and Hospital Report
needle Thoracostomy)
Proced

7.1
7.1 Patient assessment Model
reScue Scene evaluaTion (rSe)- Hazards- Environmental concerns- Mechanism of injury (Moi)- number of patients (Triage)
PriMarY SurveY 1
- MarCH 2- rapid Body survey (rBs)- s.o.a.P. 3- Skin- oxygen- airway- Position
deciSion PoinT- Patient “stable” or “Unstable”- “initiate Transport” or “Treat on scene”
SecondarY SurveY- History (Hx)- Chief Complaint- Hx of Chief Complaint(L.o.T.a.r.P.) 4- Past Medical Hx
- Present Medical Hx- Medications- allergies- identifying data- Functional inquiry
- vital signs: LoC (Glasgow Coma scale), Pulse, respirations, B/P, skin
ProTocolS
PHYsiCaL EXaMinaTion (Head to Toe)
TrEaTMEnT
iniTiaTE TransPorT (if not already started)
EMErGEnCY noTiFiCaTion
rECUrrEnT EvaLUaTion
HosPiTaL rEPorT (Patient Care report)
Proced

7.1
1. intervention, including entry into protocol-driven treatment, may be required at any stage of the assessment. often early assessment of vital signs will occur. once the emergency has been dealt with, return and complete the assessment starting at the point you left it. 2. March: Massive hemorrhage – immediate treatment of life threatening bleeding; airway with C-spine control – ensure airway patent, if not attempt to insert oPa, advanced airway or suction while protecting C-spine (LoC, d – rule out delicate spine and provide temporary stabilization); respiration – check rate/quality, if poor provide o2 +/- ventilatory support; circulation – carotid, radial (rate/rhythm). shock, risk of shock or lack of radial pulse requires immediate iv/io access; hypothermia – cover and keep casualty warm and dry. 3. SoaP: Skin: color, temperature, condition; o2: as early as possible in the mission; airway: recheck to ensure patency; Position: appropriate to medical problem (i.e., supine/ semi-prone/semi-sitting). 4. loTarP: location of pain, onset of pain (rapid/slow), Type of pain (i.e. crushing, stabbing, also determine severity on 1-10 scale), associated/aggravat-ing factors, radiating/relieving factors, Precipitating factors.
7.1 notes

7.2
7.2 advanced airway insertion indications◊ Cardio-respiratory arrest.◊ Casualty unable to protect own airway and tolerates oPa.◊ Casualty with decreased level consciousness who is difficult to
ventilate and tolerates an oPa.◊ directed by Physician.
contraindications◊ Responsive patients with an intact gag reflex.◊ Patients with known esophageal disease. 1
◊ Patients who have ingested caustic substances. 1
Preparation◊ Pre-oxygenate patient and monitor o2 saturation.◊ Choose correct size based on patient’s height. (see advanced
airway sizing Chart) (weight can also be used for size 2 and 2.5):◊ Test cuff inflation system for air leak.◊ apply water-soluble lubricant to the distal tip.
insertion◊ Hold the KLT-d/KLTs-d with the dominant hand at the proximal
end (connector) such that insertion will be accomplished in asingle, continuous motion.
◊ Use the lateral approach with chin lift.◊ insert the KLT-d/KLTs-d until the base of the connector is aligned
with teeth or gums.
Inflation◊ Using a syringe inflate cuff just enough to seal.◊ if altitude change of 4000 ft or greater is anticipated, water must
be used to inflate the cuff. Some air will remain in the cuff sothere must be continuous monitoring to avoid overpressure orair leakage.
◊ Check that the blue (pharyngeal) cuff is not visible in theoropharynx.

7.2
Final Positioning:◊ Withdraw the KLT-d/KLTs-d until ventilation is optimized.◊ Readjust cuff inflation.
Securing:◊ secure midline to the maxilla avoiding blocking the opening to the
gastric access lumen.note 1: in these patients advanced airway insertion can be attempted if it is likely that they will not survive without this procedure.
advanced airway Sizing chart
cuff colour Size weight height Inflation Volume
Green Cuff 2 12-25 Kg 90-115 cm (35-45 in) 25-35 ml
orange Cuff 2.5 25-35 Kg 105-130 cm (41-51 in) 30-40 ml
Yellow Cuff 3 n/a 122-155 cm (4-5 ft) 40-55 ml
red Cuff 4 n/a 155-180 cm (5-6 ft) 50-70 ml
Purple Cuff 5 n/a >180 cm (>6 ft) 60-80 ml
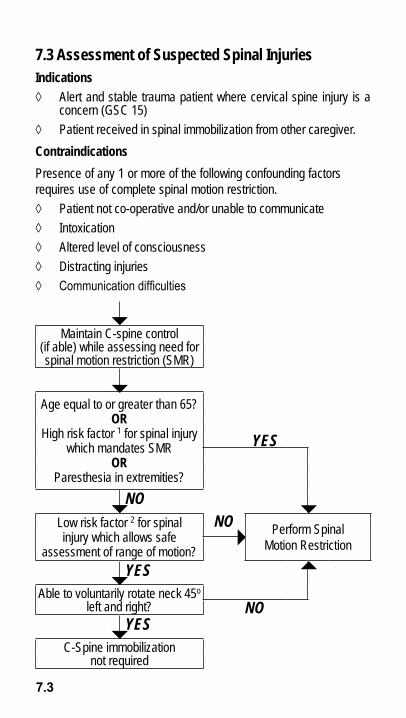
7.3
7.3 assessment of Suspected Spinal injuriesindications ◊ alert and stable trauma patient where cervical spine injury is a
concern (GsC 15)◊ Patient received in spinal immobilization from other caregiver.contraindicationsPresence of any 1 or more of the following confounding factors requires use of complete spinal motion restriction. ◊ Patient not co-operative and/or unable to communicate◊ intoxication◊ altered level of consciousness◊ distracting injuries◊ Communication difficulties
Maintain C-spine control (if able) while assessing need for spinal motion restriction (sMr)
age equal to or greater than 65?or
High risk factor 1 for spinal injury which mandates sMr
or Paresthesia in extremities?
YES
NOLow risk factor 2 for spinal injury which allows safe
assessment of range of motion?
NO Perform spinal Motion restriction
YESable to voluntarily rotate neck 45o
left and right? NOYES
C-spine immobilizationnot required

7.3
1. High risk factors for spinal injury include but are not limited to: ◊ Fall greater than or equal to 1 m / 5 stairs◊ axial load to head (e.g. diving accidents)◊ MvC (e.g. speed greater that 100 km/hr, rollover or ejection)◊ Bicycle, aTv, or snowmobile collision
2. Low risk factors for spinal injuries include:◊ simple rear-end MvC (excludes patient being pushed into on-
coming traffic, hit by bus/large truck, rollover, hit by high speed vehicle)
◊ ambulatory at any time◊ delayed (not immediate) onset of neck pain◊ absence of midline C-spine tenderness
7.3 notes

7.4
7.4 urinary catheterization indications ◊ Patients who will be under sar Tech care for an extended time
period and who are unable to void themselves.
contraindications ◊ Blood at meatus, perineal bruising, blood in scrotum, or suspect-
ed pelvic fracture.
Precautions ◊ resistance on insertion.
Procedure◊ Explain procedure to patient.◊ Position patient on back with legs apart (knees bent for females).◊ Ensure aseptic technique to prevent contamination of catheter.◊ Prepare equipment and attach drainage bag to catheter.◊ Test catheter balloon with 5 mL rL/sterile water while still in ster-
ile package.◊ Expose genitalia and clean with Betadine swabs (dispose after
each wipe).-Females: retract labia to expose urethral meatus and maintain thisposition throughout the procedure. Wipe from front to back.-Males: retract foreskin (if not circumcised) and wipe in circularmotion around urethra and glans.Hold catheter (using sterile gloves) about 3 cm from tip. dip exposed tip in lubricant and insert into urethra. in males, hold penis at 60o to patient’s body and apply light traction. advance catheter until urine flows and then a further 5 cm. Inflate balloon with 5 mL RL/sterile water and gently retract catheter until resistance is felt. secure catheter and bag to patient’s thigh. allow some slack in catheter (use catheter extension hose if required). record time, catheter size, amount and colour of urine.

7.5
7.5 eZ-io insertion Power driver eZ-io indications◊ Adults (≥ 40 kg) : For intra-osseous access anytime in which
vascular access cannot be obtained within two attempts or 90seconds in emergent, urgent or medically necessary cases.
◊ Pediatrics (3-39 kg): For intra-osseous access where vascularaccess is difficult in emergent, urgent or medically necessarycases.
contraindications◊ recent fracture or absent pulse to limbs considered for access.◊ Excessive tissue and/or absence of adequate anatomical land-
marks.◊ infection or cellulitis at the site of insertion.◊ Previous, significant orthopaedic procedure at the site (prosthetic
joint or any foreign body – plates, screws, stabilizing rods, etc…)◊ io placement at insertion site in the past 24hrs.insertion steps for Manual and Power driver◊ Locate insertion site using appropriate land-marking techniques:
◊ adult: Proximal humerus, Proximal tibia, distal tibia, sternum(Manual only)
◊ Child: Proximal tibia, distal tibia◊ Prepare insertion site: swab site with iodine solution, ensuring
aseptic technique and inform patient if conscious. allow area todry completely while preparing infusion kit.
◊ Prep infusion kit: draw up 10mL rL/ns. if using Lidocaine draw upappropriate dose. open clamp and purge air from line (extensionset) with either rL or Lidocaine. Leave syringe attached to line.
Main insertion Sites (noT Sternal site)◊ Ensure area is dry and have stabilization patch ready.◊ stabilize the site and position driver at insertion site 90° angle to
the bone. insert needle set until needle set tip touches the bone.◊ verify that the 5 mm “no Go” line is visible on the needle/stylet.◊ rotate Manual driver clockwise/counter-clockwise or squeeze
the Power driver trigger and apply gentle steady downward pres-sure. do not rock or bend during insertion.
◊ stop insertion when a sudden “give” or “pop” is felt or the desireddepth is obtained.

7.5
◊ Remove stylet and driver and confirm needle stability.◊ apply stabilizer patch.◊ attach primed line (extension set) to hub’s luer lock.◊ Use Lidocaine for patients responsive to pain and GCs > 6 prior
to flush.• if using Lidocaine, infuse slow at 1 mL per minute, and slow push
remaining 1 mL Lidocaine from catheter with 1st mL of IO flush.• Adults and Children ≥ 12 YOA: 40 mg Lidocaine IO over
2 min prior to flush. May be followed by 20 mg IO over1 min if pain relief is inadequate and patient condition allows tem-porary cessation of iv therapy.
• Children > 3 YOA: 0.5 mg/kg slow push prior to flush (See Lido-caine monograph for pediatric dosing).
◊ Flush io with 9 -10 mL of rL or ns. (4 - 5mL in Children)◊ remember: no FluSh = no Flow◊ Attach IV tubing and infuse IV fluids. Stabilize IV line. Place EZ-
io wristband◊ assess site for extravasion, bleeding, occlusion, or dislodgement.◊ same procedure is to be done for sternal application ensuring
sternal intra-osseous set is used.For Sternum• Ensure area is dry before applying the sternal Locator.• remove cap from sternal Locator and remove upper backing by
pulling on Tab #1.• align upper curve on locator with the sternal notch.• seat the Locator depth probes on the sternum by pressing down
firmly with both hands.• Press down adhesive upper portion then holding sternal Locator
pull down on Tab #2 to expose adhesive. Press down on adhesive.• remove needle cap from stylet/io needle.• Holding needle at 90° to the sternum, insert needle tip into the
centre cone of the sternal Locator and gently press down until itseats on the bone.
• apply gentle pressure while rotating clockwise until stylet clicksinto sternal Locator.
• remove stylet and attach line.

7.5 - 7.6
• if using Lidocaine, infuse slow at 1 mL per minute, and slow push remaining 1 mL Lidocaine from catheter with 1st mL of IO flush.
• Flush io with 9 -10 mL of rL or ns. (4 - 5mL in Children) • remember no FluSh = no Flow• attach iv line and stabilize iv line. Place EZ-io wristband• assess site for extravasion, bleeding, occlusion, or dislodgement.removalif removal is required, attach Luer lock syringe, continuously rotate clockwise while slowly and gently applying traction to catheter. do not rock or bend the catheter during removal.
7.6 eZ-io needle Sets Size
eZ-io needle Size / colour
Patient Size
insertion Site insertion Method
7.5 mm Green Hub
adult only sternum Manual insertion only
15 mm Pink Hub
3-39 kg Proximal and distal Tibia
Manual and Power drill
25 mm Blue Hub
≥40kg Proximal and distal TibiaProximal Humerus
Manual and Power drill
45 mm Yellow Hub
Patient with excessive tissue
Proximal and distal TibiaProximal Humerus
Manual and Power drillideal for Humerus in Patient ≥40kg

Z-io insertion Sites
7.7
7.7 Proximal tibia site
◊ adult: 1 cm medially to the tibial tuberosity.◊ Pediatric - Cannot palpate tibial tuberosity: Two finger widths
below the patella and one finger width medially along theflat aspect of the tibia.
◊ Pediatric – Can palpate tibial tuberosity: One finger widthdistal to the tibial tuberosity and one finger width mediallyalong the flat aspect of the tibia.
Distal tibia site◊ Adult Two finger widths proximal to the medial malleolus and
positioned midline on the medial shaft. ◊ Pediatric -one finger width proximal to the medial malleolus
–along the flat aspect of the medial distal tibia.Proximal humerus
◊ Expose shoulder and adduct humerus.◊ Place patient’s hand over umbilicus for correct humeral po-
sitioning.◊ Palpate and identify the mid-shaft humerus and continue
palpating toward the proximal aspect or humeral head.◊ identify two landmarks on the lateral shoulder consisting of
the acromion and the coracoid process.◊ identify the greater tubercle insertion site approximately
two-finger widths inferior to the midpoint of the coracoid pro-cess and the acromion.
Sternum◊ adult only procedure – insertion site is located midline be-
low the sternal notch at the point indicated by the sternalLocator Patch.
◊ Maintain an angle of 90◦ angle to the bone during insertion.
e

7.8
7.8 Tourniquet removalsar Techs should consider removing a tourniquet under the following circumstances: 1. To replace the initial tourniquet with a more effective/comfortable tourniquet such as a pneumatic version (e.g. the EMT) as soon as feasible. it should be applied just proximal to the initial tourniquet provided it is within 2.5-5 cm of the injury; or 2. Evacuation time to a surgical facility is expected to take more than 2 hours from time of application of tourniquet.
removal is contraindicated if: 1. The injury is a complete amputation (whereby a tourniquet is
likely required and continued use does not threaten the viability of the limb); or
2. The casualty is in hemorrhagic shock or has a decreased level of consciousness presumed secondary to hemorrhagic shock; or
3. The casualty is expected to be assessed in a surgical facility within 2 hours: or
4. The tourniquet has been in place for longer than 6 hours: or 5. Tourniquet has been applied to a crushed limb.
caution: Gradually reduce pressure on the tourniquet, leaving tourniquet in position. The wound should be inspected for bleeding to see if further management is required. if feasible, other methods of controlling hemorrhage should be instituted such as direct pressure, pressure dressings, or application of hemostatic agents. if these are unsuccessful in stopping the bleeding and/or the casualty develops symptoms or signs of shock, a tourniquet should be reapplied (preferably the EMT) and should remain in place until the casualty is assessed at a surgical facility. Before releasing a tourniquet on a casualty that has been resuscitated for hemorrhagic shock, ensure a positive response to resuscitation efforts (i.e. a peripheral pulse normal in character and normal mentation if there is no traumatic brain injury).

7.9
7.9 chest decompression (needle Thoracostomy)indications ◊ Tension / symptomatic Pneumothorax 1,2
Procedure a. assess the patient’s chest and respiratory status; b. apply o2 at 100% with a non-rebreather mask; c. Landmark is 2nd intercostal space in the mid-clavicular line; 3 d. Prepare site by wiping with an alcohol or betadine swab; e. Put tension on skin over puncture site using two fingers and
holding until puncture has been completed; f. insert 14 gauge Cathelon (needle-catheter unit), along the up-
per border of the 3rd rib (mid-clavicular). You should feel a “pop” as the Cathelon enters the pleural space; 4
g. Advance Catheter 3 to 4 cm. If using water-filled syringe and pulling back on plunger, then you will see bubbles as air is drawn into syringe;
h. Withdraw needle from catheter before transport; i. Check catheter regularly to insure it has not become blocked.
Attach syringe with sterile water or RL, flush 1-2 mL and then draw back on plunger. Seeing bubbles confirms you are ex-hausting air from the chest. 5
j. Multiple needle thoracostomies may be required per patient as the catheters tend to plug off! For any repeat thoracostomies, use syringe with sterile water/ns. 4

7.9
1. a tension pneumothorax is a life-threatening condition; rapid action is critical. observe patient for improvement; another catheter may be required. if the patient does not have a tension pneumothorax, there is a 10-20% risk of producing a pneumothorax and/or causing damage to the lung.
2. during air transport, maintain cabin pressure at sea level if possible or at the lowest altitude possible to prevent complications from air expansion.
3. if in doubt, go more lateral. alternate is the 5th intercostal space in the mid-axillary line.
4. Confirming Cathelon function with water-filled syringe attached to Cathelon is optional for first needle insertion, recommended for repeat insertions (mandatory if performed inflight because can’t hear air escape through Cathelon).
5. if you obtain bright red blood while advancing the Cathelon, withdraw cathelon completely and attempt insertion in another site. if you obtain dark red blood, advance the Cathelon another 3 cm. if you continue to obtain blood, and there is no rush of air, remove the needle from catheter and apply chest seal and reassess patient condition and possibly your diagnosis.
2nd rib
2nd iCs – insert needle here!
3rd rib
7.9 notes

7.10
7.10 orogastric (oG) Tube insertion indications ◊ To accomplish gastric decompression. note that any patient who is ventilated by BvM for more than 15 minutes (or pediatric patient for more than 5 minutes) requires an oG tube to prevent regurgitation and subsequent airway compromise. if in doubt, insert an oG tube early.
contraindications- Esophageal / retro-pharyngeal Trauma - Caustic ingestion
advantages - safe to use with facial fractures - decreases risk of aspiration
Procedure Without advance airway in place: ◊ select appropriate tube size and apply lubricating gel (e.g. adult
= 36 French; Child = 22 French) ◊ Explain procedure to patient if conscious. ◊ If no C-spine concerns, gently flex patient’s head forward ◊ introduce oG tube into mouth and direct it toward the back of
the tongue and then downward through the oropharynx (if con-scious, ask patient to swallow and advance tube immediately after each gagging episode)
◊ Confirm intragastric placement (auscultate while injecting 30-50 mL of air)
◊ retention of the oG tube is a clinical decision based on circum-stances 1
◊ record time of insertion and removal, catheter size, etc.
1. in general, if a patient is being ventilated by BvM then the tube should remain in place to prevent gastric distention and regurgitation. if a patient is well enough to complain about discomfort from the oG tube, they are much less likely to require it.

7.11
7.11 Notification and Hospital Report This format is to be adopted in order to standardize the method of providing receiving hospitals with patient information. Be concise.
noTiFicaTion 1. Ensure notification is given ASAP (once en route and in contact
with receiving hospital).
2. Provide the Emergency Physician with the following information: ◊ sar Tech name ◊ Brief summary (including age, gender, and patient classification)
“ i have ____ casualt(y/ies) , ____year old _______(gender and any appropriate info) +/- and_____year old _____(gender)...”
◊ Patient’s CC ◊ Brief history of the CC (including mechanism of injury if relevant) ◊ Current vital signs ◊ Treatment and Protocols used ◊ ETa to hospital
hoSPiTal rePorT 3. Ensure a hospital report is given upon arrival at the hospital. 4. Provide the receiving medical authority with the following infor-
mation: ◊ age, gender and patient’s CC ◊ History of the CC – list injuries/illnesses including mechanism of
injury and treatment/interventions (i.e. Protocols used)◊ initial vital signs ◊ arrival vital signs ◊ Medical history ◊ Medications ◊ allergies ◊ Relevant physical exam findings ◊ Treatment and Protocol

notes:

8
SecTion 8 – aBBreviaTionS/reFerenceS 8.1 Common Medical abbreviations 8.2 Glasgow Coma scale 8.3 neurologic red Flags8.4 rapid neurologic assessment 8.5 Pediatric Table 8.6 apgar score 8.7 Example Calculation of Fluid replacement for Burn victims8.8 iv drip rate 8.9 Formulae 8.10 Minutes of o2 supply by Pressure and Flow rate
reF

8.1
8.1 common Medical abbreviations1° Primary, First degree n&v nausea & vomiting2° secondary, second degree nad no acute/apparent distress≈ approximately equal to nPo nothing By Mouth (per os)a Before (ante) nKa no Known allergiesabd abdomen nKda no Known drug allergiesaPE acute Pulmonary Edema nTG nitroglycerinBid Twice daily nYd not Yet diagnosedBP Blood Pressure P after (post)Bsa Body surface area PE Pulmonary EmbolismC With Pr Per rectumCa Cancer prn as neededCC Chief Complaint Q EveryC/o Complaining of q hr Every HourCHF Congestive Heart Failure q2 hr Every 2 Hours
Cva Cerebrovascular accident; Costo-vertebral angle Qid 4 Times a day
Cx Chest rx Prescribed ford10W Dextrose 10% Water s Withoutdx diagnosis sC subcutaneousd/C discontinue s/p status PostEd Erectile dysfunction s/s signs and symptomsEP Emergency Physician sL sublingualET Endotracheal sx seizureEToH alcohol soB shortness of BreathFasT Face, arm, speech test Tid Three Times a dayFx Fracture T TemperatureGtt drop Tx Transport; TreatmentGU Genitourinary Uo Urinary outputH/a Headache U/s Ultra soundH&PE History and Physical Exam vs vital signsHTn Hypertension WoB Work of BreathingHx History Yoa Years of agein intra-nasal decreasedio intra-osseus increasedJvd Jugular venous distension Ø no; none; nullLoC Level of Consciousness ψ PsychMdi Metered dose inhaler ♀ FemaleMi Myocardial infarction ♂ MaleMoa Months of age
reF

8.2 - 8.3
8.2 Glasgow coma ScaleinFanT child/adulT
eye opening4 spontaneous 4 spontaneous3 To speech 3 To speech2 To pain 2 To pain1 no response 1 no response
Best verbal response5 Coos, babbles 5 oriented4 irritable cries 4 Confused3 Cries to pain 3 inappropriate words2 Moans, grunts 2 incomprehensible sounds1 no response 1 no response
Best Motor response6 spontaneous 6 obeys commands5 Localizes pain 5 Localizes pain4 Withdraws from pain 4 Withdraws from pain3 Flexion (decorticate) 3 Flexion (decorticate)2 Extension (decerebate) 2 Extension (decerebate)1 no response 1 no response
8.3 neurologic red FlagsBeware of red Flags: Progressively declining level of consciousness Progressive declining neurologic examination Pupillary asymmetry seizures repeated vomiting Persistent Glasgow Coma scale < 15 LoC greater than 5 minutes double vision Worsening headache Motor or sensory deficit Unable to recognize people or disoriented to place ataxia other important signs (especially after concussion): Confusion Weaknessslurred speech vertigo or dizzinessUnusual behaviour Persistent headacheUnsteady on feet

8.4
8.4 rapid neurologic assessmenthead and neck normal abnormal
orientation (time, person, place/situation)visual acuity (count fingers, ask about double vision)Visual fields (bring fingers from behind patient’s head)Pupils equal and reactive to lightEye movement (“H” pattern – look for nystagmus) sensation of forehead, cheeks, lower jawClench teeth (check jaw muscles)Furrow browsmile or grimace (show teeth)Check hearing/noisesswallowshrug shoulders (check resistance)Protrude tongue (check for deviation to one side)
Sensation
any unusual sensations?Check sensation (arms, back, trunk, legs)is sensation the same on both sides?
Motor Function
Finger squeeze bilaterallyThumbs down, resist pushing arms apartFlexion and extension of hip, knee, anklePlantar reflex

8.5 - 8.6
8.5 Pediatric TablePreterm Term 6 Moa 1 Yoa 3 Yoa 6 Yoa
weight (lbs) 3 7.5 15 22 33 44
weight (kg) 1.5 3.5 7 10 15 20
heart rate (bpm) 140 125 120 120 110 100
respirations 40-60 40-60 24-26 22-30 20-26 20-24
Systolic BP (mmhg) 50-60 70 90±30 95±30 100±25 100±15
Fluid challenge (ml) 30 70 140 200 300 400
Fluid Maint (ml/hr) 6 14 28 40 60 80
8 Yoa 10 Yoa 11 Yoa 12 Yoa 14 Yoaweight (lbs) 55 66 77 88 99
weight (kg) 25 30 35 40 45
heart rate (bpm) 90 90 85 85 80
respirations 18-22 18-22 16-22 16-22 14-20
Systolic BP (mmhg) 105±15 110±20 110±20 115±20 115±20
Fluid challenge (ml) 500 500 500 500 500
Fluid Maint (ml/hr) 100 100 100 100 100
8.6 apgar Score (newborn assessment)
0 Points 1 Point 2 Points 0 Min 1 Min 5 Minheart rate absent < 100 > 100
resp effort absent slow, irreg. strong cry
Muscle Tone Flaccid Some flex active motion
irritability no response some vigorous
colourBlue
extremities, pale body
Blue extremities, pink body
Fully pink
Total

8.7 - 8.8
8.7 example calculation of Fluid replacement for Burn victims◊ Person Weight 35 kg x 36% BSA affected ◊ 4 mL x 35 kg x 36 = 5040 mL/24 hrs 1/2 in 1st 8 hrs = 5040 mL = 2520 mL 21/4 in 2nd 8 hrs = 2520 mL = 1260 mL 2520 mL = 1st 8 hrs 2 + 1260 mL = 2nd 8 hrs 1/4 in 3rd 8 hrs = 2520 mL = 1260 mL + 1260 mL = 3rd 8 hrs 2 = 5040 mL = Total in 24 hrs
8.8 iv drip rateMacro infusion Set – 10 Gtt Per Millilitre (Gtt/ml)
volume Per hour drop per minutes drop rate interval (Seconds)
50 mL 8 7.2 (1 drop every 7.2 secs)
100 mL 17 3.6
150 mL 25 2.4
200 mL 33 1.8
250 mL 43 1.4
300 mL 50 1.2
360 mL 60 1.0

8.9
8.9 Formulaeiv Flow raTeSvol to be infused in (mL) x drops of admin set in (Gtt/mL) = Gtts/min
Total time of infusion in (min)example◊ volume to be infused 5040 mL in 8 hrs5040 mL x 10 Gtt/mL = 105 Gtt/min or @ 2 Gtt/sec 480 min
druG adMiniSTraTion desired dose in (mg) _ = volume to be administered Concentration on hand in (mg/mL)example◊ desired dose is 20 mg, Concentration on hand is 10 mg/mL 20 mg_ = 2 mL volume to be administered 10 mg/mLchild’S weiGhT (1-6 Yoa)2 x age in (years) + 8 = approx Weight in (kg)example◊ 2 year old boy2 x 2 years + 8 = approx 12 kgcaTheriZaTion urinarY ouTPuTadult > 0.5 mL/kg/hr Child > 1 mL/kg/hrexample◊ Weight of adult = 70 kg; Weight of child = 12 kgadult: 0.5 mL x 70 kg = 35 mL/hr urinary output
hrChild: 1 mL x 12 kg = 12 mL/hr urinary output
hr

8.10
8.10 Minutes of o2 Supply by Pressure and Flow rateJumbo ‘d’ Format o2 (Full Tank ≈ 640 L)
Pressure litres Per Minute (lPM)(PSi) 2 4 6 8 10 152200 321 161 107 80 64 432000 292 146 97 73 58 391800 262 131 87 66 52 351600 232 116 77 58 46 311400 203 101 68 51 41 271200 173 87 58 43 35 231000 144 72 48 36 29 19900 129 65 43 32 26 17800 115 57 38 29 23 15700 100 50 33 25 20 13600 86 43 29 21 17 11500 72 36 24 18 14 10400 57 29 19 14 11 8300 43 22 14 11 9 5200 29 15 10 7 6 4100 16 8 5 4 PrePare To
rePlace o2 TanK
‘ee lite’ Format o2 (Full Tank ≈ 1360 L)Pressure litres Per Minute (lPM)
(PSi) 2 4 6 8 10 152200 680 340 226 170 136 912000 617 308 207 154 123 821800 554 277 185 139 111 741600 492 246 164 123 98 661400 429 214 143 107 86 571200 366 183 122 92 73 491000 304 152 101 76 61 41900 273 137 91 68 55 36800 242 121 81 61 48 32700 212 106 71 53 42 28600 182 91 61 45 36 24500 152 76 50 38 30 20400 122 61 41 30 24 16300 92 46 31 23 18 12200 62 31 21 16 12 8100 33 17 11 8 PrePare To
rePlace o2 TanK

‘MERCY FLIGHT’
Wilfrid “Wop” May and Vic Horner deliver much needed vaccines to the village of Fort Vermillion, Alberta , January 3rd 1929, completing a historic 1240 mile round trip in minus twenty degree temperatures in their open cockpit Avro Avian Bi-plane, to avert a diphtheria epidemic.
Wop May was awarded the Distinguished Flying Cross in WW I, credited with shooting down 13 enemy aircraft and “4 probables”. He is considered by many to be the father of Search and Rescue in Canada, recognising the need for and initiating a government sanctioned service to search for, and rescue downed aircrews.
