sesa - ultrassonografia em obstetrícia€¦ · ultrassonografia em obstetrÍcia aspectos prÁticos...
TRANSCRIPT

ULTRASSONOGRAFIA EM OBSTETRÍCIA
ASPECTOS PRÁTICOSDR. RAFAEL FREDERICO BRUNS
Professor Adjunto Departamento de Tocoginecologia - UFPR

É necessário fazer ultrassonografia de
rotina?

Background Many clinicians advocate routine ultrasound screening during pregnancy to detect congenital anomalies, multiple-gestation pregnancies, fetal growth disorders, placental abnormalities, and errors in the estimation of gestational age. However, it is not known whether the detection of these conditions through screening leads to interventions that improve perinatal outcome.
Methods We conducted a randomized trial involving 15,151 pregnant women at low risk for perinatal problems to determine whether ultrasound screening decreased the frequency of adverse perinatal outcomes. The women randomly assigned to the ultrasound-screening group underwent one sonographic examination at 15 to 22 weeks of gestation and another at 31 to 35 weeks. The women in the control group underwent ultrasonography only for medical indications, as identified by their physicians. Adverse perinatal outcome was defined as fetal death, neonatal death, or neonatal morbidity such as intraventricular hemorrhage.
Results The mean numbers of sonograms obtained per woman in the ultrasound-screening and control groups were 2.2 and 0.6, respectively. The rate of adverse perinatal outcome was 5.0 percent among the infants of the women in the ultrasound-screening group and 4.9 percent among the infants of the women in the control group (relative risk, 1.0; 95 percent confidence interval, 0.9 to 1.2; P = 0.85). The rates of preterm delivery and the distribution of birth weights were nearly identical in the two groups. The ultrasonographic detection of congenital anomalies had no effect on perinatal outcome. There were no significant differences between the groups in perinatal outcome in the subgroups of women with post-date pregnancies, multiple-gestation pregnancies, or infants who were small for gestational age.
Conclusions Screening ultrasonography did not improve perinatal outcome as compared with the selective use of ultrasonography on the basis of clinician judgment.

ULTRASSONOGRAFIA EM OBSTETRÍCIA
POR QUÊ A MAIORIA DOS PROTOCOLOS RECOMENDA 3 EXAMES?

ULTRASSONOGRAFIA EM OBSTETRÍCIA
1o. Trimestre - TN2o. Trimestre - Anatomia
3o. Trimestre - Crescimento

MARCOS ULTRASSONOGRÁFICOS
S. Gestacional
Vesícula
Embrião
BCE
2 3 4 5 6 7 8 9 10 11 12

VALORES DISCRIMINATÓRIOS
Estrutura Quando tem que ser visto
Saco Gestacional Ữ-hCG > 3.500
Vesícula DMSG > 8 mm
Embrião DMSG > 18 mm
BCE Embrião > 5 mm

GRAVIDEZ ECTÓPICA
GESTAÇÃO DE 4s E 3 d
SACO GESTACIONAL DE 2 mm

GRAVIDEZ ECTÓPICA
CLASSIFICAÇÃO ULTRASSONOGRÁFICA
PROVÁVEL GRAVIDEZ TÓPICA Estrutura intrauterina semelhante ao saco gestacional
GRAVIDEZ TÓPICA DEFINIDA Saco gestacional intrauterino com vesícula vitelina ou embrião
!PROVÁVEL GRAVIDEZ ECTÓPICA
Útero vazio e massa anexial !
GRAVIDEZ ECTÓPICA DEFINIDA Saco gestacional extra-uterino com embrião ou vesícula
!GRAVIDEZ EM LOCAL INDETERMINADO
ß-hCG acima do nível discriminatório, sem evidência de saco gestacional Barnhart et al, Fertility and sterility 2011

GRAVIDEZ ECTÓPICA
CLASSIFICAÇÃO ULTRASSONOGRÁFICA
Barnhart et al, Fertility and sterility 2011

GESTAÇÃO GEMELARDIZIGÓTICA MONOZIGÓTICA

GESTAÇÃO GEMELAR
DICORIÔNICA
DIZIGÓTICA

GESTAÇÃO GEMELAR<4 dias 4-8 dias 8-13 dias >13 dias
Mórula Blástula
Blastocisto
DICORIÔNICA
DIAMNIÓTICA
MONOCORIÔNICA
DIAMNIÓTICA
MONOCORIÔNICA
MONOAMNIÓTICA
GEMELARIDADE
IMPERFEITA
MONOZIGÓTICA

GESTAÇÃO GEMELAR MORTALIDADE
Sebire et al: Br J Obstet Gynaecol 104:1203, 1997
Perd
as G
esta
cion
ais
Acu
mul
adas
(%
)
0,0
3,5
7,0
10,5
14,0
Idade Gestacional (semanas)12 16 20 24 28 32 36 40
MONOCORIÔNICA
DICORIÔNICA

GESTAÇÃO GEMELAR

SINAIS DE MAL PROGNÓSTICO
HIDRÓPICA > 6 mm
ECOGÊNICA < 2 mm

SINAIS DE MAL PROGNÓSTICO
Mal Progóstico FCE < 100 bpm

SINAIS DE MAL PROGNÓSTICO
DMSG - CCN < 5 mm

TRANSLUCÊNCIA NUCAL
Adaptado de: Nicolaides KH, Sebire NJ, Snijders RJ. O Exame Ultra-Sonográfico entre 11-14 semanas. Diagnóstico de Anomalias Fetais.

TRANSLUCÊNCIA NUCAL
Método de Rastreamento Fetos T21 Rastreados
Sensibilidade
Teste Positivo 5% N=5.000
Down N=200
100.000 gestações
Idade Materna 6030%
Bioquímica com 16 semanas 13065%
TN com 12 semanas 75% 150
TN + ß-hCG + PAPP- A com 12s 18090%
Nicolaides KH. Fetal nuchal translucency. Am J Obstet Gynecol 2004

TRANSLUCÊNCIA NUCAL
45 50 55 60 65 70 75 80 85
1,0
2,0
3,0
4,0
Comprimento Cabeça-Nádegas
Tran
sluc
ênci
a N
ucal
P95
O QUE É TRANSLUCÊNCIA NUCAL AUMENTADA?

TRANSLUCÊNCIA NUCAL
0 1 2 3 4 0 1 2 3 4
0
5
10
15
0100200
600
1000
1400
TN (mm) TN (mm)
Ris
co (
1 em
)
Like
lihoo
d R
atio
O QUE É TRANSLUCÊNCIA NUCAL AUMENTADA?

TRANSLUCÊNCIA NUCAL
!
• CCN entre 45 e 84 mm • Plano sagital • Polo cefálico ocupando ¾ da tela • Mede-se o espaço anecóico (calipers on-to-on) • Posição neutra da cabeça em relação ao corpo
TÉCNICA DO EXAME

TRANSLUCÊNCIA NUCAL
PLANO SAGITAL

TRANSLUCÊNCIA NUCALMAGNIFICAÇÃO DA IMAGEM

TRANSLUCÊNCIA NUCAL
POSICIONAMENTO DO CALIPER

TRANSLUCÊNCIA NUCAL
POSIÇÃO DE REPOUSO DA CABEÇA EM RELAÇÃO AO CORPO
Hiperextensão
A hiperextensão pode aumentar a medida da TN

TRANSLUCÊNCIA NUCAL
Souka et al. Ultrasound Obstet Gynecol 2001;18:9-17; n=1,320
TRANSLUCÊNCIA NUCAL AUMENTADA COM CARIÓTIPO NORMAL

SEGUNDO TRIMESTRE

MALFORMAÇÕES CONGÊNITAS
4.000.000 DE CRIANÇAS NASCEM POR ANO NOS EUA CERCA DE 120.000 COM MALFORMAÇÕES
6%8%
7%
15%
22%
42%
CoraçãoFenda labialT21Tubo neuralParede abdominalMembros

MALFORMAÇÕES CONGÊNITAS
CERCA DE 12.000 MORRERÁ NO PRIMEIRO DIA DE VIDA
Hyett et al., Ultrasound Obstet Gynecol. 1997;10(4)
Óbitos por Malformação
Óbito Perinatal Óbito Pós-neonatal
40%60%
60%
40%
Coração Outras

PERFIL FETAL
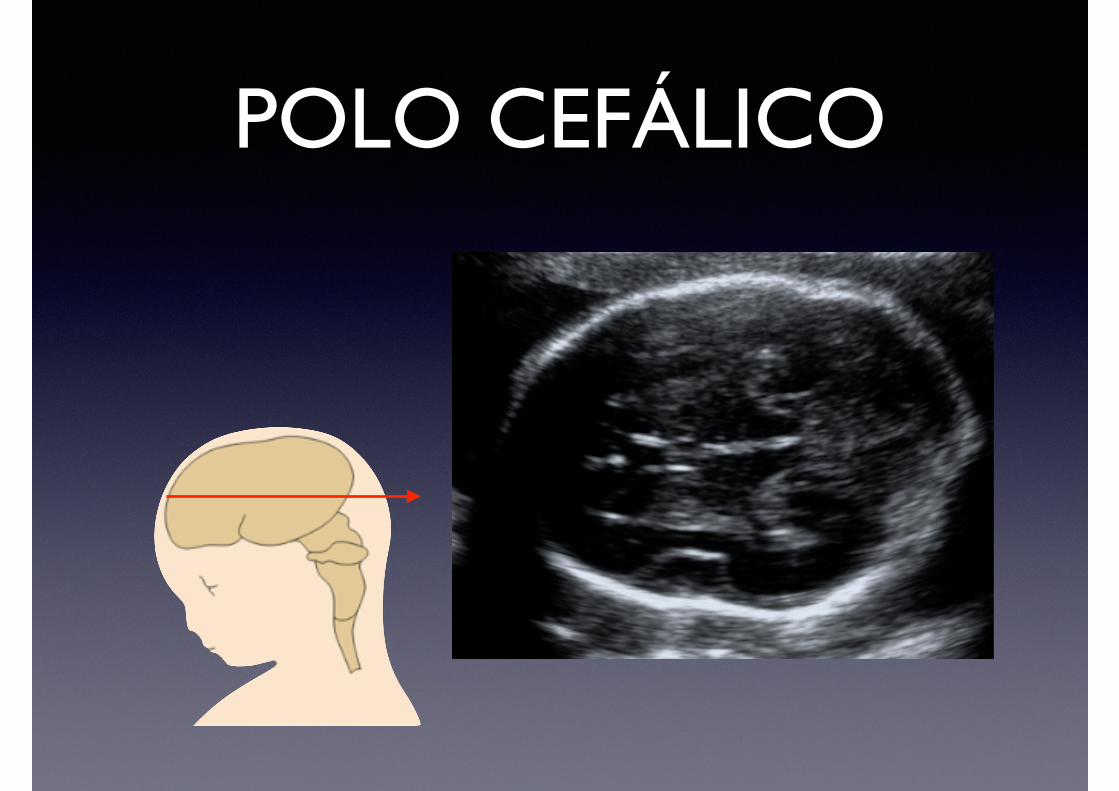
POLO CEFÁLICO

POLO CEFÁLICO

POLO CEFÁLICO

CORAÇÃO FETAL

CORAÇÃO FETAL
• Melhor prognóstico: !
1. Síndrome hipoplásica do coração esquerdo1
2. Transposição de grandes artérias2
3. Coarctação de aorta3
1 Tworetzky W et al., Circulation. 2001 3 Franklin O et al., Heart. 2002 2 Bonnet D et al., Circulation. 1999
EXISTE BENEFÍCIO NA DETECÇÃO PRÉ-NATAL?

PAREDE ABDOMINAL

PELVE RENAL DILATADA
Isoladamente não aumenta risco de cromossomopatias
!85% tem resolução espontânea ao
nascimento !
Dilatações menores que 10 mm geralmente não estão associadas com
o comprometimento da função !
Informar ao pediatra (dilatação ureteral » ATB)

PELVE RENAL DILATADA
Thilaganathan B, Sairam S, Papageorghiou AT, Bhide A. Problem-Based Obstetrics Ultrasound. 1st ed. London: Informa Healthcare, 2007

RINS CÍSTICOS
RINS POLICÍSTICOS RINS MULTICÍSTICOS

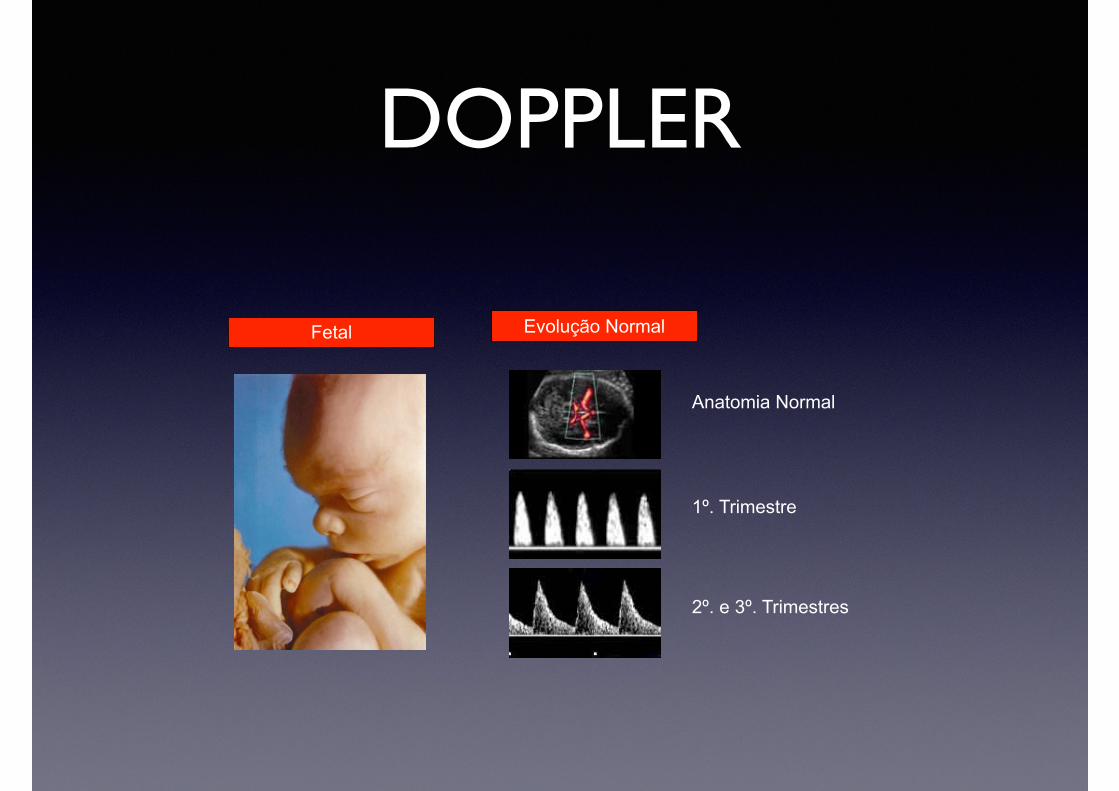
DOPPLER
Materno Fetal Placentário
Territórios de Interesse

DOPPLERMaterno Evolução Normal
1º. Trimestre
Início do 2º. Trimestre
Fim do 2º. Trimestre e 3º. Trimestre

DOPPLER
Placentário
ARTÉRIA UMBILICAL
DOPPLER
Fetal Evolução Normal
Anatomia Normal
1º. Trimestre
2º. e 3º. Trimestres

PONTOS IMPORTANTES
• 3 EXAMES POR GESTAÇÃO
• UM EM CADA TRIMESTRE
• 11 A 14 SEMANAS
• 20 A 24 SEMANAS
• 32 A 34 SEMANAS
• DOPPLER RESERVADO PARA CASOS AONDE O CRESCIMENTO FETAL ESTÁ ABAIXO DO ESPERADO