single rooms in hospital estimate of the medical need
TRANSCRIPT
1063
Special Articles
SINGLE ROOMS IN HOSPITALESTIMATE OF THE MEDICAL NEED
J. W. D. GOODALLM.D. Edin., F.R.C.P.E.
MEMBER OF TEAM INVESTIGATING FUNCTIONS AND DESIGN OF
HOSPITALS (NUFFIELD PROVINCIAL HOSPITALS TRUST AND THEUNIVERSITY OF BRISTOL)
THE proportion of beds to be provided in single roomswithin the ward unit has an important bearing on warddesign. Single rooms may be needed as an amenity, forprivileged or paying patients, or on medical grounds.This paper is concerned solely with the medical reasonsfor giving patients special accommodation.
Studies of the present practice in hospitals do notgive a clear indication of what proportion of beds shouldbe in single rooms, or which patients should have them.It is, I think, fair to say that at present the provision ofsingle rooms is inadequate. The large open ward, whichis still the commonest type in this country, has usuallyone or two single rooms (or in some cases double rooms)attached to it. These rooms are often used for conva-lescent patients of a different social class who would beill at ease in a large ward, and it is quite common to findthe single rooms occupied by sick members of the’medicalor nursing staff or their near relatives. But this, ofcourse, is by no means always the case, and many of thepatients in single rooms are there on purely medicalgrounds. For example, the hyperthyroid patient who isvery nervous and sometimes irritable, the infectiouspatient or the patient suspected of infection, and inmaternity hospitals the pre-eclamptic.Single rooms are also occupied by " nuisance " cases
- e.g:, patients suffering from lung abscess or gangreneof the lung, patients who shout or use foul language,and unsociable or quarrelsome patients, though theselatter categories are rather rare. In some instances the
dying or seriously ill are removed from large wards tosingle rooms ; but more often they are " screened off
"
in the open ward at a place convenient to the nursingstaff for observation.
If the above description of present practice in hospitalwards is accepted, it will be evident that the claims ofthe doctor, the nurse, and the patient are all beingconsidered in rather a haphazard way.
Since most hospitals were built great advances havebeen made in medical knowledge. We now know moreof the causes of infections, and how to control or curethem. Consequently, many more tuberculous patientsand more infectious patients who would formerly havebeen sent to isolation hospitals are being treated ingeneral hospitals ; and they usually require single roomsor segregation in small wards. In addition we have learntthat there are certain groups of patients who are parti-cularly susceptible to infection-especially infants,patients suffering from burns, and those undergoingplastic operations-and they must be isolated.Thus there are overriding medical reasons for providing
single rooms. Naturally, in so far as segregation ofpatients increases the work of the nurses and makesobservation of patients more difficult, the medicaldemands may have to be modified. But it is essential toknow what they are.
CLASSIFYING THE REASONS
I began my investigation by asking a number ofclinicians, drawn from all specialties, on what medicalgrounds they would place their patients in singlerooms. The reasons given by 24 specialists can besummarised under five headings : .
--
(a) Infective cases (patients liable to infect others).(b) Infectable cases (patients particularly susceptible to
infection).(c) Dying and seriously ill cases.(d) Nuisance cases (patients likely to disturb others or be
disturbed by others).(e) Cases requiring special attention.Each specialist was also asked to indicate the propor-
tion of beds which he thought should be provided in theform of single rooms, and to state approximately howlong a patient would be required to stay in a single roomfor each reason. Only a minority attempted suchestimates ; but a few were very definite. Two super-intendents of fever hospitals said that all infectious
patients must have single rooms. The specialist in thetreatment of burns also required 100% single rooms forhis patients, and the paediatrician asked for single roomsfor all babies from birth to two years of age. Some
surgeons wanted their patients to stay in single rooms for24-48 hours after operation. Other specialists estimatedthe proportion of single rooms required as between 2and 20%.In order to obtain more precise information on this
point I drew up a schedule of conditions warrantingsingle-room accommodation, based on the replies fromthe 24 specialists. Each qualification for a single roomwas given a number, so that when records came tobe made a number could be entered for each patientwho qualified. The 31 conditions fall into the five
categories shown above; but it became apparentthat patients requiring separate accommodation can
also be divided into two main groups : (1) those whohave to be kept under close observation, and (2) thosewho require to be separated but who do not necessarilyneed constant supervision by the nursing staff. Examplesof the former, which I shall call type A, are dying orseriously ill patients, and cardiac patients needing peaceand quiet ; examples of the latter (type B) are patientssuspected of infection and patients who are smelly orsocially unpleasant. The division is important from theward planning point of view, since type-A single roomsmust be situated for easy observation, and thereforenear the centre of the ward, whereas type-B single roomscan if necessary be placed at the periphery of the ward.The schedule was as follows :All dying cases
A Dying cases.
Infective casesB Exanthemata: chickenpox, &c.B Tuberculosis : all " open " cases ; all meningitis cases ; all
cases receiving special treatment.B Venereal disease in infectious stage.B Ringworm of scalp.B Mastoid cases.B Sinus infections.B All hare-lips, cleft palates, and major skin losses.B Suspected cases of infection (likely to infect others).B Other infections.
Seriously ill casesA Pre-eclamptic and eclamptic cases.A Bacterial endocarditis.A Other seriously ill cases.
Infectable casesB All burns : for whole period in hospital.A All infants from birth to age of two years : for whole period
.
in hospital.B Other infectable cases (particularly susceptible to infection).
" ivuisance " casesA Nervous, restless, irritable patients-e.g., cerebral irritation
and severe hyperthyroid.B Smelly or otherwise unpleasant cases-e.g., lung abscess,
fistula in perineum, offensive discharge.A Cardiac cases needing peace and quiet.A Severe vomiting.3 Post-traumatic psychosis-e.g., foul language, indecent
behaviour (mainly in association with head injuries andoperations).
B Other nuisance cases.
Cases requiring special attention ’
A Eye cases with complications-e.g., pneumonia.A Cases receiving special treatment-e.g., oxygen tent.A Postoperative cases (other than very minor operations),
and all fenestration cases, for 48 hours unless longer periodthought necessary.
1064
A Epilepsy ant all cases of " fits."A Shock cases ’having drip treatment.A Cases in labour a long time with ruptured membranes.A Failed forceps.A Cases requiring constant supervision.A Other cases requiring special attention.
THE SURVEY
In the main survey (undertaken after a preliminarypilot survey) residents in 8 hospitals cooperated byrecording on their daily rounds those of their patients whoqualified for a single room according to the scheduleI had prepared. Returns were made by residents in 29wards over a period of at least a month. There were 10surgical wards, 10 medical, 4 gynsecological, 3 maternity,and 1 each of children, and of ear, nose, and throatpatients. The total number of beds covered was 1010.The records showed that, of the 31 possible reasons for
wishing to place patients in single rooms, some were givenmuch more often than others. For example, patientsoften qualified for single rooms because their conditionwas smelly, infectious, or otherwise unpleasant. Com-paratively few needed separate accommodation becausethey had sinus infections, eclampsia, or eye complications.This was to be expected, because most of the recordswere made in general hospitals and not in hospitals orwards for special diseases.
It was found that the demand for separate accommoda-tion fluctuated widely from day to day in all the wards ;but except for two surgical wards, both in the samehospital, the types of demand for single rooms appearedto be roughly comparable within a given specialty.Because of these considerable fluctuations in dailydemand, a simple estimate of the average requirementfails to give a correct estimate of the number of roomsthat should be provided. The data therefore neededstatistical analysis, and this was undertaken by Mr.N. T. J. Bailey, statistician to the Department of Medi-cine, University of Cambridge, with the results set outbelow.
Because of the daily fluctuations in demand it is
important to distinguish between how much of thedemand can be met (efficiency of provision), and to whatextent the single rooms available are occupied for theirproper purpose (efficiency of utilisation). The former
efficiency can be made very high only at the expense ofthe latter, and vice versa ; for if enough single rooms areprovided to cope with all requirements on
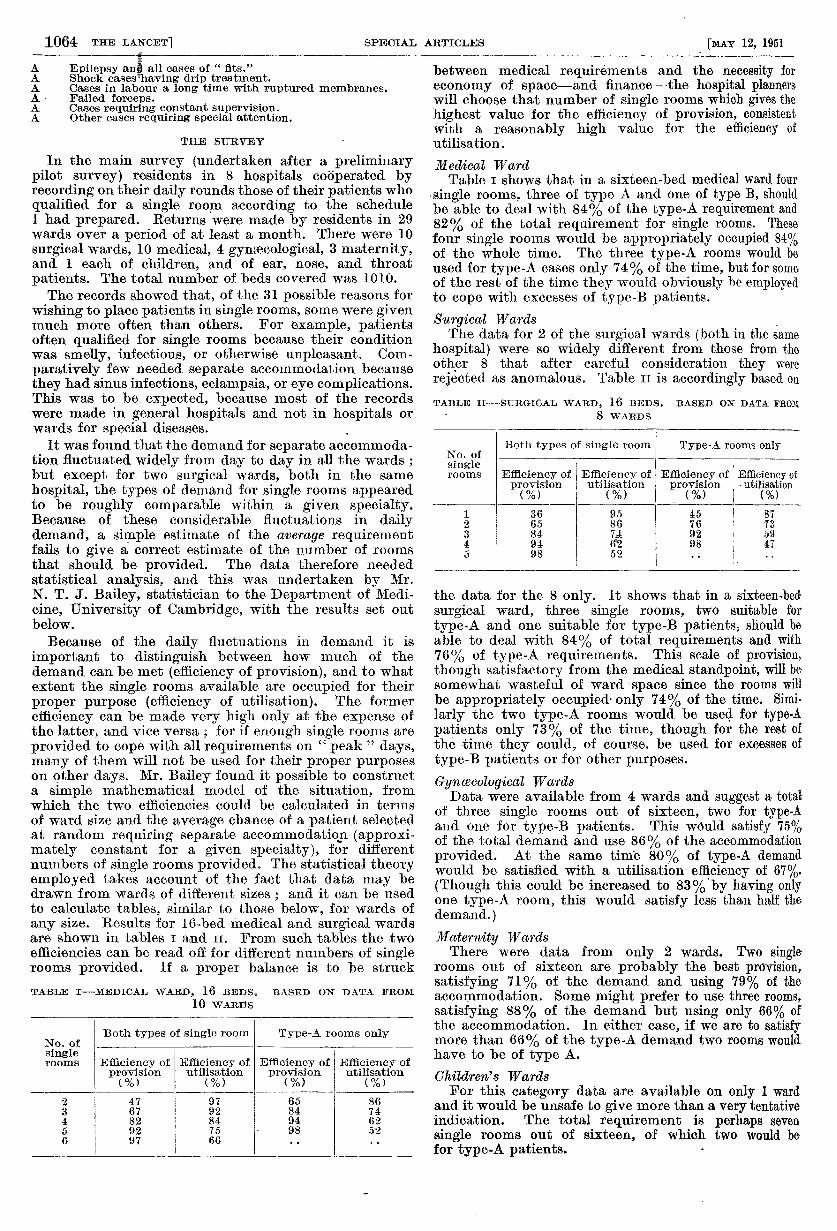
" peak " days,many of them will not be used for their proper purposeson other days. Mr. Bailey found it possible to constructa simple mathematical model of the situation, fromwhich the two efficiencies could be calculated in termsof ward size and the average chance of a patient selectedat random requiring separate accommodation (approxi-mately constant for a given specialty), for differentnumbers of single rooms provided. The statistical theoryemployed takes account of the fact that data may bedrawn from wards of different sizes ; and it can be usedto calculate tables, similar to those below, for wards ofany size. Results for 16-bed medical and surgical wardsare shown in tables i and 11. From such tables the twoefficiencies can be read off for different numbers of singlerooms provided. If a proper balance is to be struck
TABLE I-MEDICAL WARD, 16 BEDS. BASED ON DATA FROM
10 WARDS
between medical requirements and the necessity for
economy of space-and finance-the hospital plannerswill choose that number of single rooms which gives thehighest value for the efficiency of provision, consistentwith a reasonably high value for the efficiency ofutilisation.
Medical WardTable i shows that in a sixteen-bed medical ward four
single rooms, three of type A and one of type B, shouldbe able to deal with 84% of the type-A requirement and82% of the total requirement for single rooms. Thesefour single rooms would be appropriately occupied 84%of the whole time. The three type-A rooms would beused for type-A cases only 74% of the time, but for someof the rest of the time they would obviously be employedto cope with excesses of type-B patients.Surgical Wards .
The data for 2 of the surgical wards (both in the samehospital) were so widely different from those from theother 8 that after careful consideration they were
rejected as anomalous. Table 11 is accordingly based onTABLE II-SURGICAL WARD, 16 BEDS. BASED ON DATA FROM
- 8 WARDS
the data for the 8 only. It shows that in a sixteen-bed
surgical ward, three single rooms, two suitable for
type-A and one suitable for type-B patients, should beable to deal with 84% of total requirements and with76% of type-A requirements. This scale of provision,though satisfactory from the medical standpoint, will besomewhat wasteful of ward space since the rooms willbe appropriately occupied’ only 74% of the time. Simi-
larly the two type-A rooms would be used for type-Apatients only 73% of the time, though for the rest ofthe time they could, of course, be used for excesses oftype-B patients or for other purposes.
Gynœcological WardsData were available from 4 wards and suggest a total
of three single rooms out of sixteen, two for type-Aand one for type-B patients. This would satisfy 75%of the total demand and use 86% of the accommodationprovided. At the same time 80% of type-A demandwould be satisfied with a utilisation efficiency of 67%.(Though this could be increased to 83%’by having onlyone type-A room, this would satisfy less than half thedemand.)
Maternity WardsThere were data from only 2 wards. Two single
rooms out of sixteen are probably the best provision,satisfying 71% of the demand and using 79% of theaccommodation. Some might prefer to use three rooms,satisfying 88% of the demand but using only 66% ofthe accommodation. In either case, if we are to satisfymore than 66% of the type-A demand two rooms wouldhave to be of type A.
Children’s WardsFor this category data are available on only 1 ward
and it would be unsafe to give more than a very tentativeindication. The total requirement is perhaps sevensingle rooms out of sixteen, of which two would befor type-A patients.
1065
SUMMARY
A survey was undertaken to determine what proportionof beds in a ward should reasonably be provided in singlerooms in order to satisfy the medical needs of the patient.
After reference to a number of consultants, a list of31 conditions qualifying patients for accommodation insingle rooms was compiled..
This schedule of conditions was used by housemen, in29 wards of 8 general hospitals, to record each day over aperiod of a month whether the patients in the wardqualified for single rooms.An analysis of these records enabled conclusions to
be drawn about the most desirable provision of singlerooms. For wards of sixteen beds these are :
General medical wards .... 4 single roomsGeneral surgical wards .... 3 " "
Gynaecological wards...... 3 " "
.
Maternity wards ...... 2 or 3 single rooms
-For larger wards the proportion of single-room beds tototal beds would be somewhat less and for smaller wardsit would be somewhat greater.
I should like to thank the staff of the 8 hospitals who keptsuch painstaking records on their daily rounds, and Mr. Baileyfor his invaluable statistical work on analysing the records.
WINTER ADMISSIONS TO LONDONHOSPITALS
Work of the Emergency Bed Service, 1950-51
As is generally known, in the past winter greatdifficulty was experienced in London in the admission ofacutely ill patients to hospital. These difficulties causedgreat hardship to patients as well as extra work for theirdoctors. But it is not easy to turn these generalisationsinto facts and figures. There are no figures to show thetotal number of urgent cases requiring admission to theLondon hospitals, though many of the hospitals keep anote of their own figures. Thus the figures of the
Emergency Bed Service (E.B.S.) seem to be the onlyones covering greater London as a whole.The E.B.S. is an auxiliary service intended to help
doctors who have made an unsuccessful direct applicationfor the -admission of a patient to the hospital of theirchoice. What proportion of the acute cases in Londonare admitted through such direct applications by theirdoctors could only be discovered by putting a lot ofextra work on hospital officials. Random checks haveshown that some hospitals admit three or four acutecases direct from doctors to every one admitted throughthe E.B.S. ; in others the proportion is about equal;and on the average the ratio of direct to E.B.S. seemsto be about 2 : 1. But these proportions apply to totaladmissions, and it must be remembered that the doctorwho cannot get his patient admitted direct can apply tothe E.B.S., who may be more fortunate ; whereas if theE.B.S. fails to find a bed for a patient the failure is usuallyfinal. Thus, though only about a third of all theadmissions are arranged through the E.B.S., the service’sfailures represent a much larger proportion of the total-indeed, if all London doctors make a rule of trying theE.B.S. before resigning themselves to keeping the patientat home, then the E.B.S. failures will be the total failuresin London. Broadly speaking, then, the E.B.S. experiencewill give a reasonably representative picture of theposition in London.
THE WINTER’S WORK
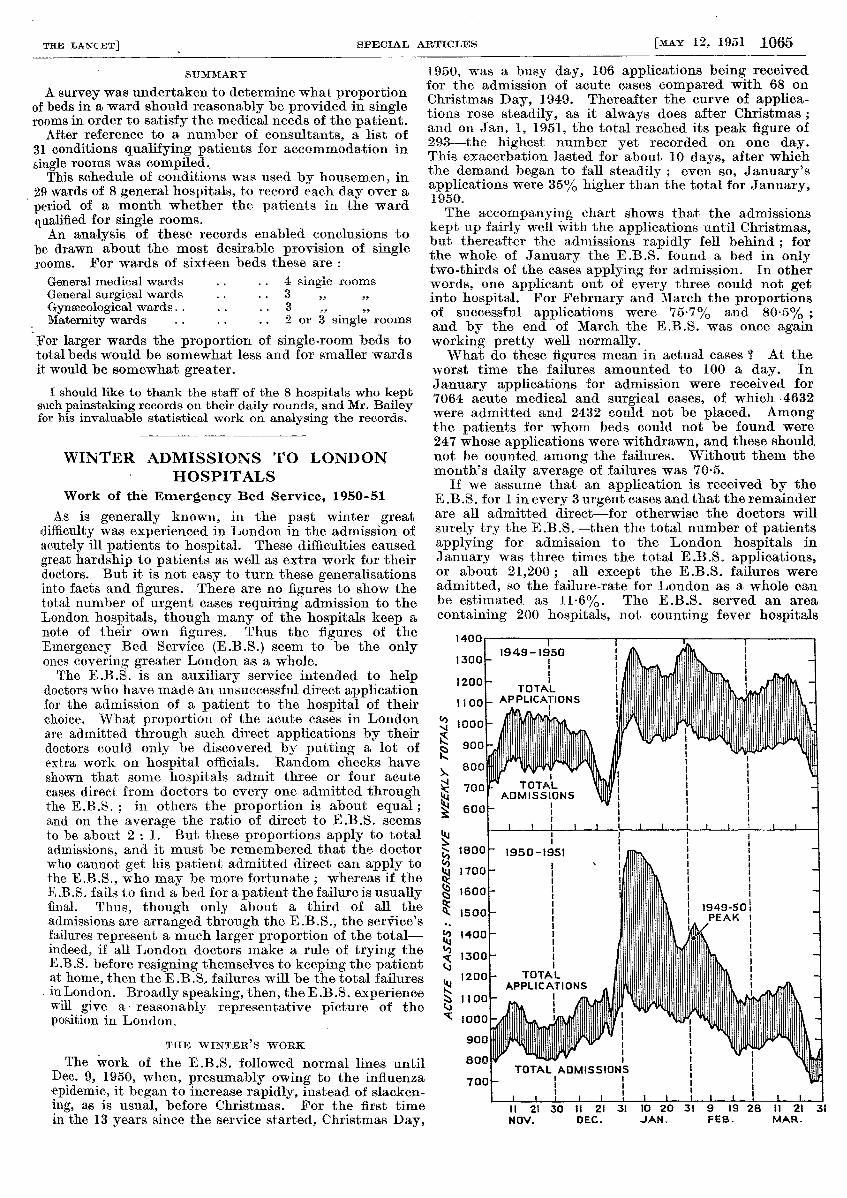
The work of the E.B.S. followed normal lines untilDec. 9, 1950, when, presumably owing to the influenzaepidemic, it began to increase rapidly, instead of slacken-ing, as is usual, before Christmas. For the first timein the 13 years since the service started, Christmas Day,
1950, was a busy day, 106 applications being receivedfor the admission of acute cases compared with 68 onChristmas Day, 1949. Thereafter the curve ofapplica-tions rose steadily, as it always does after Christmas ;and on Jan. 1, 1951, the total reached its peak figure of293-the highest number yet recorded on one day.This exacerbation lasted for about 10 days, after whichthe demand began to fall steadily ; even so, January’sapplications were 35% higher than the total for January,1950.The accompanying chart shows that the admissions
kept up fairly well with the applications until Christmas,but thereafter the admissions rapidly fell behind ; forthe whole of January the E.B.S. found a bed in onlytwo-thirds of the cases applying for admission. In otherwords, one applicant out of every three could not getinto hospital. For February and March the proportionsof successful applications were 75-7% and 80.5% ;and by the end of March the E.B.S. was once againworking pretty well normally.What do these figures mean in actual cases ? 2 At the
worst time the failures amounted to 100 a day. In
January applications for admission were received for7064 acute medical and surgical cases, of which 4632were admitted and 2432 could not be placed. Amongthe patients for whom beds could not be found were247 whose applications were withdrawn, and these shouldnot be counted among the failures. Without them themonth’s daily average of failures was 70-5.
If we assume that an application is received by theE.B .S: for 1 in every 3 urgent cases and that the remainderare all admitted, direct—for otlierwise tne doctors win
surely try the E.B.S.-then the total number of patientsapplying for admission to the London hospitals in
January was three times the total E.B.S. applications,or about 21,200; all except the E.B.S. failures wereadmitted, so the failure-rate for London as a whole canbe estimated as 11-6%. The E.B.S. served an area
containing 200 hospitals, not counting fever hospitals