statewide strategic plan - myflorida.com€¦ · partnership for child health ... rene anderson...
TRANSCRIPT

2012Florida Department of Children and FamiliesSubstance Abuse/Mental Health Program&Department of Child and Family StudiesCollege of Behavioral and Community Sciences University of South Florida
Be One Florida
Statewide Strategic Plan for System of Care Expansion of Services for Children with Mental Health Needs and their Families
2012-2016

Prepared for the Department of Children and Families’ Substance Abuse and Mental Health Program Office by staff and faculty at the Louis de la Parte Florida
Mental Health Institute, College of Behavioral and Community Sciences, University of South Florida, 2012
FMHI Project Team:
Mary Armstrong, PhD
Don Policella, MA
Norín Dollard, PhD
Kathy Lazear, MA
Stephen Roggenbaum, MA
Cathy Sowell, MA
Dawn Khalil

1
Table of Contents
Acknowledgement of Stakeholders .................................................................... 2
Systems of Care .................................................................................................. 4
Florida’s Systems of Care History ...................................................................... 6
Vision, Mission and Values ................................................................................. 9
Logic Model ...................................................................................................... 10
Goals & Strategies at a Glance .......................................................................... 11
Strategic Plan ..................................................................................................... 12
Glossary of Acronyms ....................................................................................... 36
References ......................................................................................................... 37

2
Stakeholders
Representatives from the agencies listed here have participated in the strategic planning processes.
Agency for Health Care Administration
Agency for Persons with Disabilities Central Florida Behavioral Health Network
Community Based Care of Central Florida - Families and Communities Together Daniel Kids Foundation
Department of Children & Families – Office of Child Welfare Department of Children & Families – Substance Abuse & Mental Health Program Office
Department of Education Department of Health
Department of Juvenile Justice Division of Vocational Rehabilitation
Family Café Federation of Families of Florida
Federation of Families of Hillsborough Federation of Families of Northeast Florida
Florida Diagnostic & Learning Resources Center Florida Youth Council
Made By Us Mental Health America of Northeast Florida
NAMI Florida Partnership for Child Health – Jacksonville SOC Initiative
Sarasota Partnership for Children's Mental Health SEDNET
South Florida Behavioral Health Network - FACES Success 4 Kids & Families
The Florida Center for Early Childhood Top Shelf Consulting
University Area Community Development Corporation University of South Florida
Wraparound Orange Youth Advocate Programs
Youth Shine

3
Special thanks to the following individuals for their contributions to the Strategic Plan.
Aida Santana Alex Brown
Alex Demola Alex DeMolina
Amy Silva Andrea Bourget Angel Rosado
Angela McCann Anne Marie Sheffield
Annette Tavera Annie Palmer
Ansley Steward Becky Pengelly Beth Piecora
Bethany Allaer Beverly Wilkinson
Blair Parker Bob Streater, III Brian Williams
Bruce Strahl Carly Fahey
Carmen Dupoint Carol Barr Platt
Carol Eloian Carol Pittman Casey Minor
Cassandra Bouchard Cathy Claud
Celeste Putnam Celocia Dobbey Charletta Clegg Charlotte Curtis Chris Duggan
Cindy Johnston Clint Rayner
Colleen Lenfestey D.D. Pickle
Dalacy Boudreaw Dalacy Joseph Daniel O’Neill David Gonzalez David Wheeler
Dee O'Neill Dell Brown
Derek Carraway Desiree Durham-
DeLeon Don Policella
Dondrell Hudson Donna Wyche Eboney Brown
Ellen Fitzgibbon Felecia Peguero
Frank Platt Frederick Andrews Gwendolyn Hinson
Jackie Beck Jaheim Hall Jane Streit
Janice Arthur Jarren McDonald
Jasmine Harris Jay Ballon
Jeannie Becker-Powell Jeannie Forthuby
Jelisa Hudson Jennifer Evans
Jennifer Marshall Jennifer Tulloch
Jeremy Countryman Jim McCready
Joe Anson John Fair
John Rodger Judith Evans Julie Etienne
Julie Radlauer-Doerfler Kate Prendiville Kathryn Shea
Katrina Bushner Kayla Crawford
Kelvin Lewis Keyonia Graham
Khush Jagus
Kimberley Brown Kimi Ramey
Kirk Hall Kristin Murray Kyle Baldwin Larry English Laurie Eckely Laurie Herring
Lee Storey Lakeesha Hines
Ligon Carrie Linda Outlaw Linda Radigan Linda Rayner Lisa Hetrick Lisa Houston Liza Leonard Lori Fahey
Lynn Laredo Marie Mosley
Martarshia Burke Mary Armstrong Mary Jane Henry Matthew Hudson Maura Bourget
Melissa Witmeier Michael Williams
Michael Lowry Michelle Lawrence
Mike Ballon Mona Kelly
Moniece Jackson Muriel Jones
Natacha Adolphe Nicki Young
Nicole Attong Norín Dollard
Otti Young Pam Jeffre Pat Kramer Pat Tuthill
Patricia Adams
Patrick Deleme Paula Thomas
Ramona Burrows Reilly O’Neill
Rene Anderson Rita Robinson
Rodger Flanders Roma Burrow
Roosevelt Badger Rosaly Guzman
Rosemarie McDonald Ruth Colon Sam Ross
Samuel Kelly Savi Marie
Sebrina Barron Senta Goudy
Seyney Dressler Shirley Outlaw Silvia Quintana Stacey Hermer
Stephanie Colston Susan Kurtin
Susan McLean Tabetha Smith Tammy Turner
Tammy Workman Tawney Harden
Tim Turner Tracy Pellegrino
Ute Gazioch Veree Jenkins
Vicki Draughon Vicki Waytowich
Ward Cox Whitney Gilbert Whitney Harris
Willie Hines Xavier Williams
Yamile Diaz

4
Systems of Care
Originally articulated in 1986 in A System of Care for Children and Youth with Severe Emotional Disturbances (Stroul & Friedman, 1986), the
definition of system of care has been refined and was most recently updated
to read ‘A spectrum of effective, community-based services for children and
youth with or at risk for mental health or other challenges and their
families, that is organized into a coordinated network, builds meaningful
partnerships with families and youth, and addresses their cultural and
linguistic needs, in order to help them to function better at home, in school,
in the community and throughout life’ (p.2, Stroul & Friedman, 2011).
Systems of Care are guided by these three core values and twelve principles:
CORE VALUES
1.) Family-Driven and Youth-Guided, with the strengths and needs of the child and family
determining the types and mix of services and supports provided;
2.) Community-Based, with the locus of services as well as system management resting within a
supportive, adaptive infrastructure of structures, processes, and relationships at the
community level; and
3.) Culturally and Linguistically Competent, with agencies, programs, and services that reflect the
cultural, racial, ethnic, and linguistic differences of the populations they serve to facilitate
access to and utilization of appropriate services and supports.
GUIDING PRINCIPLES
1.) Ensure availability of and access to a broad, flexible array of effective, evidence-informed, community-based services and supports for children and their families that addresses their physical, emotional, social, and educational needs, including traditional and nontraditional services as well as informal and natural supports
2.) Provide individualized services in accordance with the unique potential and needs of each child and family, guided by a strengths-based, wraparound service planning process and an individualized service plan developed in true partnership with the child and family
3.) Deliver services and supports within the least restrictive, most normative environments that are clinically appropriate
4.) Ensure that families, other caregivers, and youth are full partners in all aspects of the planning and delivery of their own services and in the policies and procedures that govern care for all children and youth in their communities, states, territories, tribes, and Nation
5.) Ensure cross-system collaboration, with linkages between child-serving agencies and programs across administrative and funding boundaries and mechanisms for system-level management, coordination, and integrated care management

5
6.) Provide care management or similar mechanisms to ensure that multiple services are delivered in a coordinated and therapeutic manner and that children and their families can move through the system of services in accordance with their changing needs
7.) Provide developmentally appropriate mental health services and supports that promote optimal social and emotional outcomes for young children and their families in their homes and community settings
8.) Provide developmentally appropriate services and supports to facilitate the transition of youth to adulthood and to the adult-service system as needed
9.) Incorporate or link with mental health promotion, prevention, and early identification and intervention to improve long-term outcomes, including mechanisms to identify problems at an earlier stage and mental health promotion and prevention activities directed at all children and adolescents
10.) Incorporate continuous accountability mechanisms to track, monitor, and manage the achievement of system of care goals; fidelity to the system of care philosophy; and quality, effectiveness, and outcomes at the system level, practice level, and child and family level
11.) Protect the rights of children, youth, and families and promote effective advocacy efforts 12.) Provide services and supports without regard to race, religion, national origin, gender,
gender expression, sexual orientation, physical disability, socioeconomic status, geography, language, immigration status, or other characteristics; services should be sensitive and responsive to these differences
Since 1993, the Substance Abuse and Mental Health Service Administration’s has funded
grants to more than 170 communities to promote the implementation of system of care values and
principles, including 8 in Florida. The outcomes of these grants have been positive for youth and
their caregivers, as well as in terms of costs and improvements in service system infrastructure. In
a recent review of data collected for communities funded in 2002 and 2003 (ICF Macro, 2010)
children and youth served under this grant program evidenced increased strengths and fewer
problem behaviors and symptoms, fewer justice system encounters and delinquent behaviors,
spent fewer days in psychiatric hospitals, and were doing better in school. Positive outcomes were
also seen among caregivers, who missed fewer days of work due to their child’s emotional and
behavioral issues and experienced less strain due to their care-giving responsibilities. Funded
communities were also assessed to determine the degree to which they were building or revamping
infrastructure in ways that were consistent with system of care values and principles. Positive
results have been observed in this as well, with funded communities improving in the areas of
providing care that is family-focused, culturally competent and individualized, that the service
system maximized the use of integrated, collaborative approaches, and that services were
community-based and provided in the least restrictive environments. Cost savings to the
communities due to reduced use of inpatient services was estimated at $2,377 per child and savings
from reduced justice encounters at $622 per child.

6
Florida’sSystemofCareHistoryNo stranger to the philosophy and practice entailed by adherence to
System of Care principles and values, Florida has had 8 Children’s
Mental Health Initiative grants and received its first award in 1998. A
synopsis of these communities follows:
Years of Funding
Community Project Name Fiscal Agent Description
1998 -2004
Hillsborough
County
THINK - Tampa
Hillsborough Integrated
Network for Kids
Children’s Board of
Hillsborough County
“THINK” - a community-based program
providing mental health services to children under the age of 21 who have been diagnosed with
Severe Emotional Disturbances (SED) in Hillsborough County, either by the school system
according to their behavioral criteria, or by a psychologist, according to a DSM-III diagnosis. In addition, children served by this program received services by more than one agency or professional
organization (i.e., multi-system treatment).
1999 - 2005
Palm Beach
County
Family HOPE -
Helping Organize
Partnerships for Empowerment
Florida
Department of Children and Families
& Palm Beach County
Family HOPE - a community collaborative
designed to develop and implement a seamless system of care to prevent children with serious emotional disturbance, birth through 21, from moving into overly restrictive treatment services and prevent duplication of services. Building on
system of care values and principles, Family HOPE proposed to establish and grow family
empowerment services and to implement Assertive Community Treatment teams.
2002 - 2008
Broward County
One Community
Partnership - Working
Together For Our Children
Broward County Human Services
Department
One Community Partnership (OCP) - a county-
wide initiative to evaluate and redesign the existing array of children’s mental health services in
Broward County, Florida. OCP focused on building an infrastructure that supports on-going
collaboration among local stakeholders by addressing long-standing systemic issues, service
gaps, and barriers that have historically prevented this community from keeping children with SED
in the community.

7
Years of Funding
Community Project Name Fiscal Agent Description
2005 - 2011
Sarasota County
Sarasota County Early Childhood Mental Health
Partnership
Sarasota County
Department of Health
The Sarasota Early Childhood Mental Health Partnership - convened to improve and increase
mental health and non-mental health services and supports provided for infants and very young
children consistent with System of Care principles and best practices. The project linked the existing elements of the children's mental health system with those of the early childhood system to: 1]
create an early childhood mental health system of care; 2] expand key services needed to improve the behavioral health of these children; and 3] deliver comprehensive training and technical
assistance to ensure cross-training of system-of-care staff from the two systems.
2009 - 2015
Orange County
Wraparound
Orange
Orange County
Wraparound Orange - implements integrated community based services and supports for
children with SED and their families through development of effective and enduring systems of
care. All partners are committed to working together; to optimize outcomes; serve as a catalyst
for broad-based sustainable systematic change; facilitate policy reform; develop infrastructure;
and utilize evidenced-based practices in a culturally and linguistically competent manner.
The primary program goal is to expand community capacity by offering mental health and
support services through focused outreach, treatment, education, and prevention activities in a variety of settings and times to facilitate a family's ability to access services and to ensure there is "no
wrong door" for accessing services. 2009 - 2015
Miami-Dade
County
FACES –
Families and Communities
Empowered for Success
Department of Children and Families
FACES - a collaborative effort to enhance, expand
and strengthen the existing community-based family and youth mental health services in Miami-
Dade County, in order to better serve children who have serious emotional disturbances and
their families or caretakers. FACES is a component of the broader Miami Dade County Children's Mental Health system of care and is
intended to enable youth with multiple and changing needs to remain in the least restrictive settings in their community, in school, out of the
juvenile justice/legal system and attain and maintain a physical-mental-emotional-spiritual
recovery. The population of focus for the project is adolescents with co-occurring mental health and
substance abuse disorders.

8
Years of Funding
Community Project Name Fiscal Agent Description
2010 - 2016
Seminole County
FACT – Families and Children
Together
County of Seminole
The FACT initiative - being implemented in order to refine the existing system of coordinated
juvenile justice, school, child welfare and children’s mental health services. Supports,
consisting of local public and private organizations working in teams, plan, enhance & implement an enhanced set of services tailored to each child's
physical, emotional, social, educational and family needs. FACT is intended to integrate services for children and youth involved with multiple service systems and their families at home, in school and
in the community. 2010 - 2016
Jacksonville
Jacksonville
System of Care Initiative
City of
Jacksonville
Jacksonville’s System of Care Initiative (SOCI) seeks to establish a sustainable and replicable
model system of care to provide a continuum of individualized, culturally and linguistically
competent prevention, diagnostic and treatment services to children with or at-risk for SED, from
birth through transition into adulthood, who are in or at-risk for involvement in the child welfare and juvenile justice systems, as well as homeless youth. The model establishes a public-private-academic
sector partnership to integrate systems of care principles with those of the Medical Home Model of care for children with special health care needs
and the Core and Essential Functions of public health.
In the fall of 2011, the Florida Department of Children and Families’ Substance Abuse and
Mental Health Program Office was awarded a System of Care Expansion Planning grant. This
grant was awarded to enhance the state’s ability to take the lessons learned from its graduated and
active grant sites and take the system of care philosophy and principles to scale statewide. Under
the leadership of the DCF Substance Abuse and Mental Health Program Office, families, youth,
providers, and state agency representatives joined together to develop a logic model, strategic plan
and social marketing plan.
This strategic plan was developed through a progressive, sustained collaborative process led by
the Core Planning Team and included five sub-committees that developed strategies, indicators
and responsible parties in order to move the state forward towards full realization of system of care
values and principles. These sub-committees were organized by each goal and an additional group
was convened for social marketing. The sub-committees held both in-person meetings and
conference calls to complete their tasks. Additionally, focus groups, key informant interviews, and
a two-day meeting of Florida’s family leadership were convened to provide further input from
youth and family members. The final strategic plan was approved by the statewide Stakeholder

9
Planning Team at their final meeting on September 14, 2012 in Tampa. The Core Planning
Team and the Stakeholder Planning Team developed a vision, mission and value statement:
Vision
Florida's children with behavioral health challenges and their families are engaged as primary decision makers in a culturally relevant, coordinated healthcare setting that provides the highest quality services and supports and promotes their individual growth to reach their maximum potential.
Mission
Our mission, as a dedicated Florida group of youth and families, child-serving agencies, and other stakeholders is to develop a comprehensive strategic plan to guide the expansion of family driven and youth guided systems of care to improve outcomes for children and families within their cultural context. We will accomplish this through effective utilization of resources, having youth and families in all discussions, intervening early with prevention and intervention, and promoting mental health as a recognized health issue.
Values
Family-Driven; Youth-Guided; Culturally & Linguistically Competent; Community Based; Data Driven; Evidence-Based; Outcome-Oriented

10
Florida’s Logic Model
A logic model (Hodges & Hernandez, 2006) was developed to provide a road map outlining how the expansion of system of care values and principles will occur and includes the population, mission and vision, the strategies to achieve the goals, and the expected outcomes (Hernandez & Hodges & 2005).

11
Goals & Core Strategies at a Glance
The CMHSOC Stakeholders and Core Planning Team identified the following goals:
Goal #1: Consistent Family and Youth Voice at All Levels Goal #2: Collaboration / Integration among Community
Partners Goal #3: Link with Early Childhood Initiatives to Promote
Screening, Prevention and Early Intervention for Behavioral Issues
Goal #4: Implement Local System of Care Sites Goal #5: Implementation of Evidence-Based Practices
These goals serve as the foundation to the strategic plan. To ensure that the goals address all
aspects of system of care implementation (e.g., policy change, service implementation), five core
strategies were identified to organize the activities that will contribute to the attainment of the goals.
These core strategies, identified by Stroul and Friedman, 2011, are outlined below.
Core Strategy #1: Implementing Policy, Administrative, and Regulatory Changes Core Strategy #2: Developing Services and Supports Based on the System of Care
Philosophy and Approach Core Strategy #3: Creating Financing Mechanisms Core Strategy #4: Providing Training, Technical Assistance, and Coaching Core Strategy #5: Generating Support
In sum, the values and principles
identified herein drive all aspects of SOC
Expansion. Through the devoted effort of
stakeholders, consensus has been obtained on the
strategies necessary to achieve these goals and
provide a concrete set of tasks to move forward
with implementation. The following strategic plan
details these activities, which are organized by goal
and core strategy.

12
Florida’s Statewide Children’s Mental Health System of Care Expansion Strategic Plan 2012 – 2016

13
Goal #1: Consistent Family and Youth Voice at All Levels Core Strategy: Implementing Policy, Administrative, and Regulatory Changes
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 1.a.1 (Policy) Family organizations to meet consistently statewide PRIORITY
A statewide consortium of family leaders with aligned goals and advocacy strategies
1. Compile comprehensive list of family run organizations throughout the state serving the population of focus
‐Family Run Organization
‐Statewide SOC Core Team
10/31/12
2. Identify lead family run organization to initiate communication process
Statewide SOC Core Team
10/31/12
3. Identify family coordinator to work with Project Director to implement Goal 1.
‐Family & Youth Run Organizations
‐Statewide SOC Core Team
12/31/12
4. Convene meetings of family leadership group ‐Lead Family Run Org.
‐DCF SAMH Program Office
12/31/12
5. Develop forum for sharing strategic goals and resources including development of MOUs to support all SOC core values, including family‐driven and youth‐guided care
‐Lead Family Run Org.
7/31/2013
6. Outreach to diverse/underserved populations ‐Lead Family Run Org.
9/30/13
7. Provide advocacy to the legislature during the next session
‐Lead Family Run Org.
‐State MH Planning Council
9/30/13
Objective 1.a.2 (Policy) Youth organizations to meet consistently statewide PRIORITY
A statewide consortium of Youth leaders with aligned goals and advocacy strategies
1. Link with youth organizations and existing youth forums such as Youth Summit, Youth M.O.V.E and youth & family websites to compile list of youth organizations throughout the state serving the population of focus.
‐Statewide SOC Core Team
‐Family Run Organizations
10/31/12
2. Identify lead youth run organization to initiate communication process, convene group meeting of leadership groups, and develop forum for sharing strategic goals and resources.
‐Statewide SOC Core Team
‐Statewide family network/ consortium
10/31/12
3. Develop SOC website with interactive forum such as discussion boards to solicit youth input regarding needed resources and system improvements.
‐DCF SAMH Program Office
‐SOC Core Team 12/31/12
4. Outreach to diverse/underserved populations. ‐Lead Youth Org. ‐Local SOC Planning Teams
7/31/12
5. Convene focus groups to identify opportunities and needs of youths
‐Lead Youth Run Organization
9/30/13
6. Provide advocacy to the legislature during the next session
‐Lead Youth Run Organization
‐Youth Summit 9/30/13

14
Objectives Key Indicators of
Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 1.a.2 Continued
7. Identify youth coordinators to work with Project Director to implement Goal 1.
‐Family & Youth Run Organizations
‐Statewide SOC Core Team
12/31/12
Objective 1.a.3.(Policy) Standards for youth and family voice/ involvement in contracts with publicly funded providers
Family & youth representation on state & local advisory boards and board of directors
1. Review Managing Entities contracts for inclusion of family and youth representatives on board of directors and provide feedback
‐DCF SAMH Program Office
‐Consortium of youth and family organizations
12/31/12
2. Maintain a calendar of statewide workgroup meetings on the SOC webpage
‐Statewide SOC Project Director
‐Other child serving agencies (DJJ, Health, Education, AHCA, Child Welfare, APD, etc.)
12/31/12
Objective 1.a.4.(Policy) Youth and Families are active participants in system and service evaluation processes
Family and youth voice is represented is all quality assurance, quality improvement, monitoring, evaluation and research activities
1. Identify or develop satisfaction and service effectiveness evaluations to family and youth service recipients informed by surveys, focus groups, and other methods, through in‐person and on‐line formats.
‐Providers ‐Independent evaluators
‐Consortium of youth and family organizations
3/31/14
2. Include peer recovery specialists and/or family members in all monitoring, evaluation and research activities regarding system of care implementation as well as specific interventions.
‐Providers ‐Independent evaluators ‐MEs ‐State partner agencies
‐Consortium of youth and family organizations
9/30/14
Objective 1.a.5.(Policy) Accessible and user‐friendly dissemination of evaluation outcomes
Youth and family members have access to service/ program outcomes
1. Link report cards for behavioral health providers to the SOC webpage
‐Statewide SOC Project Director
9/30/14
2. Write evaluation outcomes and processes in plain language and have them reviewed and edited by youth and family members prior to dissemination
‐Providers ‐Evaluators
‐Family run organization ‐Youth run organization ‐Office of Consumer Affairs
9/30/14
3. Identify and utilize mechanisms to bring information to families and underserved populations with limited access to technology (e.g. public health centers, guidance counselors, Exceptional Student Education Specialists, etc.)
‐DCF Regional SAMH Offices
‐Family run organization ‐SEDNET
9/30/15

15
Core Strategy: Developing Services and Supports Based on the System of Care Philosophy and Approach Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 1.b.1 (Service)
Consistent statewide team planning approach driven by the family and guided by youth
PRIORITY
Availability of Wraparound/ team planning based services for youth and families with complex behavioral health needs and /or multi‐system involvement
1. Add wraparound team meetings as a mandatory Medicaid service code with ability to be billed by all qualified team members for the same time period.
‐AHCA ‐Current Wraparound Providers ‐DCF SAMH
9/30/14
2. Adopt the wraparound guidelines and principles as the foundation for person‐to‐person training for targeted case child case managers
‐AHCA ‐FMHI ‐DCF SAMH ‐Family Orgs. ‐Youth Run Orgs.
9/30/14
3. Develop or identify Wraparound guides in plain language for families and youth delineating what to expect from the provider and how to drive the team process.
‐DCF SAMH Program Office
‐Family Run Orgs. ‐Youth Run Orgs.
9/30/13
4. Explore train‐the‐trainer mechanisms and develop a statewide training plan.
‐Statewide SOC Core Team
‐Certified Wrap. Trainers ‐FMHI
9/30/13
5. Crosswalk steps of Wraparound approach with available, billable services (e.g. Arizona model)
‐Statewide SOC Core Team
‐DCF SAMH ‐AHCA
3/31/14
Objective 1.b.2 (Service)
Family Care Plans instead of “treatment plan” (interpreted as a single plan of care or a master care plan)
Integrated care plan that provides consistent goals and is inclusive of or references all treatment and service plans that affect a family
1. Identify lead facilitator / agency(s) to manage process ‐Statewide SOC Core Team
9/30/16
2. Convene group meeting of stakeholders ‐Identified Lead Facilitator
Stakeholders 9/30/16
3. Review plans across systems to identify common/distinct elements
‐Identified Lead Facilitator
Stakeholders 9/30/16
4. Identify ‘required’ plan elements for each system ‐Identified Lead Facilitator
Stakeholders 9/30/16
5. Negotiate elements of a common plan ‐Identified Lead Facilitator
Stakeholders 9/30/16
6. Secure consensus and implement ‐Identified Lead Facilitator
Stakeholders 9/30/16
7. Reconvene or identify group to review and evaluate implementation
‐Identified Lead Facilitator
Stakeholders 9/30/16

16
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 1.b.3 (Service)
Availability of youth and family peer support services
Annual increase in employed recovery peer specialists ‐family
1. Add Peer Support as a stand‐alone, billable service to the Medicaid Handbook
‐ Statewide SOC Core team
‐ AHCA ‐ Consortium of youth & family orgs
9/30/16
2. Increase availability and access to youth and caregiver run support group specific to the cultural and linguistic needs of the community
‐ Consortium of youth and family organizations
‐Local SOC Planning Teams
9/30/14
3. Consider youth peer certification
‐State SOC Project Coordinator
‐Florida Certification Board ‐Statewide SOC Core Team ‐ Consortium of youth & family orgs
9/30/16
Core Strategy: Creating Financing Mechanisms
Objective 1.c.1 (Financing) Funding opportunities for family and youth organizations, including funding parent and youth support services
PRIORITY
A business plan to secure and sustain family and youth support services Sustained youth and family organizations to ensure family and youth voice
1. Identify Medicaid and non‐Medicaid sources to support family and youth involvement at all levels of the system of care including independent fundraising and fund stream development including but not limited to :
a. Private sector donors, b. Grant opportunities, c. Children Services Councils, d. County Governments
‐ Consortium of youth and family organizations
9/30/13
2. Legislative advocacy for dedicated block grant funding for family run organizations to provide parent and youth support partners and support groups.
‐ Consortium of youth and family organizations
‐DCF SAMH (Chief level or higher) ‐State MH Planning Council
9/30/13
3. Develop local partnerships with providers and child serving agencies (e.g. YMCA, Boys & Girls Clubs, Faith‐based organizations, HMO’s, rotaries, schools & universities) to share resources such as space, volunteers, trainings, food, etc.
‐ Consortium of youth and family organizations
9/30/13
4. Engage university business schools to identify opportunities for help in growing non‐profit family and youth organizations
‐ Consortium of youth and family organizations
9/30/13
5. Add Family Support as a mandatory Medicaid service code.
‐AHCA ‐SOC Core Team ‐State MH Planning Council
9/30/14

17
Core Strategy: Providing Training, Technical Assistance, and Coaching
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 1.d.1 (Training & TA) Training for youth & families in leadership, self‐advocacy & policy development
PRIORITY
A statewide training plan for youth and families
1. Conduct needs assessment and develop training initiative from evaluations conducted that have relevance to families and youth, e.g., youth in transition study
‐‐‐Consortium of family & youth orgs
‐DCF SAMH Program Office
9/30/13
2. Identify and review existing training curriculums and update/modify as necessary.
‐‐Consortium of family & youth orgs
‐DCF SAMH Program Office; past and currently funded SOC grantees
9/30/13
3. Identify leaders, such as Jack Levine, who can train on advocacy
‐Consortium of family & youth orgs
‐DCF SAMH Program Office
9/30/13
4. Identify and/or create one website in the state where all trainings are listed (See also 1.b.6)
‐Consortium of family & youth orgs
‐DCF SAMH Program Office
9/30/13
Objective 1.d.2 (Training & TA) Families are aware of what to expect from the behavioral health system
Availability of web‐based and written materials in plain language for families accessing services on what to expect
1. Identify or develop tip sheets / guides for various service systems written by youth and family members with TA from content experts for: a. Mental Health b. Juvenile Justice c. Schools – Individualized Education Plans
‐Youth Council ‐Consortium of family and youth organizations
‐Statewide SOC Core Team Providers ‐Child Serving Agencies
9/30/14
2. Make tip sheets available on SOC website
‐Statewide SOC Project Director
9/30/14
3. Ensure tools are appropriate and relevant to diverse cultural groups
‐CLC Coordinator ‐Consortium of family & youth orgs
9/30/14
4. Link with providers to distribute guides at point of first contact
‐Managing Entities ‐Statewide SOC Core Team
9/30/14

18
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 1.d.3 (Training & TA) Parents and youth in a variety of training roles
Family & /or youth as sole or co‐trainer for SOC and Team Planning trainings as a minimum standard
1. Build community training collaborative to maximize resources
‐Local SOC Coordinator
‐Local SOC Planning Teams
9/30/14
2. Train, utilize and pay parents, family members and young adults to be trainers
‐DCF SAMH Program Office
‐Managing Entities ‐Consortium of family & youth orgs
9/30/15
3. Utilize young adults with system experience to share stories in college programs to train upcoming workforce (e.g. medical schools, psychology & social work programs, etc.)
‐Consortium of family and youth organizations
‐Youth Council ‐DCF SAMH Program Office ‐Board of Regents
9/30/15
4. Provide Wraparound training to stakeholders in addition to service providers
‐Training Collaborative
‐Local SOC Planning Teams ‐Managing Entities
9/30/15
Objective 1.d.4 (Training & TA) Service providers proficient in the areas of engagement and active listening skills
Qualitative evaluations indicate that youth and families were successfully engaged in services and felt heard
1. Develop or identify video based trainings with youth and caregivers depicting effective engagement and client/provider interactions vs. what does not work.
‐Consortium of family and youth organizations
‐DCF SAMH Program Office ‐Statewide SOC Core Team
9/30/14
2. Teach active listening skills as well as strength‐based assessment skills (e.g. ask families what they need)
‐Training Collaborative
‐Certified Wraparound Trainers
9/30/14
3. Engage family and youth peer specialists in trainings
‐Training Collaborative
‐Certification Board 9/30/15
Core Strategy: Generating Support
Objective 1.e.1 (Support) Decrease stigma of MH/SA
PRIORITY
Implementation of Social Marketing Plan
1. Support and endorse strategies outlined in the SOC Social Marketing Plan
‐Family and Youth Organizations
‐DCF SAMH Program Office
9/30/13
2. Identify venues to share youth and family stories ‐Family and Youth Organizations
‐DCF SAMH Program Office
9/30/13
3. Promote public and professional awareness of mental health as general health issue through social media tools and websites
‐Family and Youth Organizations
‐DCF SAMH Program Office
9/30/13
4. Identify opportunities for prevention of mental health / substance abuse disorders
‐Family and Youth Organizations
‐DCF SAMH Program Office
9/30/13

19
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 1.e.2 (Support) Reach “invisible” (underserved and unconnected) populations
Increase service utilization by underserved populations
1. Analyze data at the local or regional level to determine unmet needs and determine who these underserved populations are (needs assessment on who is served, who serves them, & with what services)
‐DCF Regional SAMH Office
‐Family run organization ‐Managing Entity
9/30/14
2. Select one group to focus on (for current year) and engage them in helping to identify what the strategies are to best engage this group; identify the places to engage them (schools, faith based organizations; community leaders)
‐DCF Regional SAMH Office
‐Family run organization ‐Managing Entity
9/30/15
3. Utilize mobile unit to access underserved areas and provide information on available resources
a. Staff with volunteers b. Utilize donated computers c. Spread SOC message d. Track # of individuals reached e. Charge community for use
‐Family run organization
9/30/15
Objective 1.e.3 (Support) Enhancing support and engagement of families and youth at all levels of the system
Business plan to support involvement at state and local levels
1. Provide outreach to where families are (e.g. libraries, faith‐based organizations, Boys & Girls Clubs, YMCA, schools (ESE), after‐school programs, etc.) a. Educate and train community on tools, resources
and SOC principles b. Utilize Great American Teach In model c. Link with existing resources such as 211 d. Link with foster and adoptive families and youth
‐Family run organization
‐Local SOC Planning Teams ‐Local Foster Parent Association
9/30/15
2. Identify family and youth leaders in schools & neighborhoods
‐Family run organization
‐Local SOC Planning Teams
9/30/15
3. Include input from leaders from various community
organizations – all inclusive‐for profit,‐non‐profit,
business leaders, clergy, neighborhood associations,
etc.

20
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 1.e.4 (Service) Develop multiple methods of connecting families and youth to resources, information and other families and youth
Youth and families are connected via website, resource guides, web chat capacity, and hotlines
1. Utilize social media tools a. Blogging/ Facebook / Apps b. Discussion board for both parents and for youth
‐Consortium of family and youth organizations
‐DCF SAMH Program Office
9/30/13
2. Mobile unit to reach populations without transportation a. Community‐supported with donations b. Identify infrastructure supports financially for
bus/vehicle liabilities
‐Consortium of family and youth organizations
9/30/15
3. Develop hotline staffed by certified recovery peer specialists for families and youth statewide to gain access to information, resources and support. Costs to be shared by family and youth organizations statewide.
‐Consortium of family and youth organizations
9/15/16

21
Goal #2: Collaboration / Integration among Community Partners Core Strategy: Implementing Policy, Administrative, and Regulatory Changes
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 2.a.1 (Policy) Establish common practices and policies across agencies that reflect SOC and Trauma Informed Care (TIC) values and principles PRIORITY
MOU’s between governmental entities that incorporate SOC and TIC language, values and principles and required data elements SOC and TIC language spelled out in provider contracts and included in monitoring protocols Multiagency workgroup created to work on standardized assessment framework and produce plan for Years 2‐4
1. Link with workgroups where this is being addressed, operationalize SOC and TI Care, as needed, and review MOUs currently being edited to include TI Care language, SOC language and physical health care.
‐DCF SAMH Program Office
‐TI Care Interagency workgroup
9/30/13
2. Coordinate and engage agency representatives to identify minimum common assessment elements, processes for each agency to review and approve assessment changes, and generate recommended steps to achieve in Years 2‐4. a. Workgroup will consider linking with Georgetown
Crossover Youth Practice Model Initiative for communication guidelines related to child welfare – justice involved youth
b. Identify resources outside of child welfare that would fund CBHA assessments and expand Medicaid eligibility / definition that would allow for billing under this code outside of child welfare
c. Revise or develop assessment procedures for use outside of the child welfare context
d. Identify training and support for sharing comprehensive behavioral health assessments (CBHA) across systems, train agency staff in using CBHAs in family support / care planning.
‐Statewide SOC Project Director
‐Georgetown Crossover Youth Practice Model Initiative workgroup ‐AHCA ‐DCF SAMH Program Office ‐DJJ ‐Child Welfare ‐Managing Entities
9/30/13
3. Utilize common language understandable to all a. Develop a cross‐agency glossary b. Publish the glossary on the SOC webpage
‐Statewide SOC Project Director
‐Statewide SOC Core Team ‐Consortium of family & youth orgs
9/30/15
4. Review age requirements across systems and revise to make them consistent
‐Statewide SOC Project Director
‐Statewide SOC Core Team
9/30/16
5. Standardize release/request for information forms within regions
‐Local SOC Coordinator
‐Local SOC Planning Teams ‐Managing Entities – Providers
9/30/16

22
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 2.a.2 (Policy) Common
outcomes across
child serving
systems
including:
Child/family
functioning,
school drop‐
outs, out‐of‐
home
placements,
caregiver stress,
suspensions /
expulsions,
employment,
school
attendance &
arrests
PRIORITY
Cross‐system report card, common monitoring and evaluation tools (Years 2‐4)
1. Identify lead facilitator / agency
‐Statewide SOC Core Team
9/30/13
2. Convene stakeholders (possibly an existing group like the state Children’s Cabinet) to review outcomes for each system identify common domains.
‐Lead Facilitator ‐Agency CQI and IT staff ‐Consortium of family & youth orgs ‐Child Serving Agencies
3/31/14
3. Identify evaluation tools for core data set across systems
‐Stakeholder Workgroup
‐Agency CQI and IT staff ‐Consortium of family & youth orgs
3/31/15
4. Review measures for each domain, identify strengths of measures.
‐Stakeholder Workgroup
‐Agency CQI and IT staff ‐Consortium of family & youth orgs
3/31/15
5. Propose core data set for child and family service agencies
‐Stakeholder Workgroup
‐Agency CQI and IT staff ‐Consortium of family & youth orgs
9/30/15
6. Review evaluation, QA/QI and data monitoring resources in each agency and develop funding for impartial evaluation of systems & services.
‐Stakeholder Workgroup
‐Agency CQI and IT staff ‐Consortium of family & youth orgs
9/30/15
7. Develop a common data base to be to be shared across systems, accessible to stakeholders including youth and families
‐Stakeholder Workgroup
‐Agency CQI and IT staff ‐Consortium of family & youth orgs ‐Child Serving Agencies
9/30/16

23
Core Strategy: Developing Services and Supports Based on the System of Care Philosophy and Approach Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 2.b.1 (Service) Single point of care coordination
PRIORITY
An identified individual or entity responsible for cross‐system communication, practice, and QA/QI
1. Identify EBPs that support team‐based single point of care approach (e.g., wraparound, medical home)
‐DCF CW‐CBC pilot on single point of care
‐Statewide SOC Core Team
3/31/13
2. Implement individualized family‐specific team planning process for children, youth and family with complex needs
‐Managing Entities ‐DCF CW‐CBC pilot on single point of care
‐Providers ‐AHCA ‐Regional SAMH Office
9/30/14
3. Implement team based discharge/ transition planning process for youth in residential care and youth transitioning to adult services
‐Managing Entities ‐DCF CW‐CBC pilot on single point of care
‐Providers ‐AHCA ‐Regional SAMH Office
9/30/14
4. Use Managing Entity (ME) contracts to reinforce single point of care
‐DCF SAMH Program Office
9/30/14
5. Monitoring tools will be developed and used to identify that single points of contacts are being used appropriately in each region
‐DCF SAMH Program Office
‐Consortium of Youth & Family Orgs
9/30/14
6. ME and Regional SAMH Directors provide TA to circuits / local service areas on team planning and single point of care
‐DCF Regional SAMH Office
‐DCF SAMH Program Office
9/30/14
7. Review current guidelines for the use of 100800 funds (CBCs use children’s MH general revenue funds to provide non‐Medicaid compensable community MH services and natural supports to children in out of home care and those at risk of removal. The purpose of the funds is to build resiliency through a wraparound approach to service provision and amend as needed to support team planning).
‐DCF Regional SAMH Office
‐DCF CW‐CBC pilot on single point of care
9/30/14
8. Utilize curricula from team planning approaches, such as Wraparound, to develop consistent and comprehensive targeted case management training as required by AHCA.
‐AHCA ‐FMHI ‐Statewide SOC Core Team
9/30/14

24
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 2.b.2 Early intervention, screening and assessment based on SOC values and principles
‐Reduced time from problem identification to screening ‐Increased number of BH screenings
1. Identify mechanisms and supports to help parents obtain screenings, assessments and early intervention as soon as a problem is identified and remain engaged through the process.
‐ DCF SAMH Program Office
‐Local community ECC & SOC Teams ‐ Providers ‐ Family Orgs. ‐ DOE
9/30/15
2. Provide screenings and services in the community that are easily accessible to families (e.g., pediatrician offices, childcare centers, schools, home‐based, etc.).
‐ Providers ‐ Local community ECC & SOC Teams ‐ Providers
9/30/16
3. Conduct school‐based screenings earlier and include parents in each step of screening, assessment and referral process.
‐ SEDNET ‐ Local SOC Planning Team ‐ DOE
9/30/16
4. Provide outreach, education and supports to underserved populations regarding the importance of early screening and assessment (e.g., single parents, relative caregivers, foster/adoptive families, etc.).
‐ Family Orgs ‐ Local SOC Planning Team
9/30/16
Core Strategy: Creating Financing Mechanisms
Objective 2.c.1 (Financing)
Maximize service accessibility and usage of funding streams
PRIORITY
All children will be served through the age of 21 for more than just basic clinical services; case management and intensive levels of care will be provided to all children through age 21.
1. Ensure that the SOC Expansion Toolkit includes strategies and incentives to leverage resources for outreach, prevention and intervention.
‐Statewide SOC Project Director
Statewide SOC Core Team
12/31/12
2. Create forums to discuss leveraging resources at the community level (e.g. providing training on SOC opens up conversation on “how can you help us?”)
‐Local SOC Coordinators
‐Local SOC Teams ‐Providers ‐State and local business comm.
9/30/13
3. Dedicated DCF managed care person ‐Chief of SAMH Program Office
‐AHCA 12/31/12
4. Increase awareness of existing funding sources so that staff and families have comprehensive list of available resources
‐Local SOC Coordinators
‐Local SOC Planning Teams ‐Providers
9/30/14
5. Expand Medicaid coverage through age 21 for children with eligible mental health diagnoses
‐AHCA Statewide SOC Core Team
9/30/15
6. Train ACCESS staff on Medicaid eligibility for youth in foster care through age 21
‐Child Welfare ‐AHCA 9/30/15
7. Maximize use of private insurance for eligible youth and families by assisting providers in entering private insurance networks so they are eligible to bill
‐Managing entities ‐AHCA ‐Local SOC Planning Teams
9/30/15

25
Core Strategy: Providing Training, Technical Assistance, and Coaching Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 2.d.1 (Training & TA) Universities and community colleges as partners in SOC implementation
YEARS 2‐4
Florida universities and community colleges incorporate SOC in their curricula
1. Identify programs that produce workforce (i.e. social work, psychology, mental health counseling, early childhood, child care, etc.)
‐Statewide SOC Project Director
‐Statewide SOC Core Team
9/30/14
2. Identify any curricula already available inclusive of SOC philosophy and practices
‐Statewide SOC Project Director
‐Statewide SOC Core Team
9/30/14
3. Identify SOC champion within the university system ‐FMHI ‐Statewide SOC Core Team
9/30/14
4. Undergraduate and graduate programs – provide guest speakers / experts in the field to speak with classes about SOC and reality of current practices
‐ Statewide SOC Project Director
‐Statewide SOC Core Team ‐FMHI
10/1/13‐9/30/16
5. Link with community college child care programs and leadership groups to introduce EBP’s such as mental health consultation and SOC principles
‐Statewide SOC Project Director
‐Statewide SOC Core Team ‐FMHI
10/1/13‐9/30/16

26
Goal #3: Link with Early Childhood Initiatives to Promote Screening, Prevention and Early Intervention for Behavioral Issues Core Strategy: Developing Services and Supports Based on the System of Care Philosophy and Approach
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/ Due Date
Objective 3.b.1 (Service) Strengthening family involvement in EC SOC
PRIORITY
Work plan developed, meeting agendas and sign in sheets to document family involvement
1. Connect and coordinate existing early childhood groups (e.g., Infant Mental Health) and families to serve as workgroup to develop a plan to fully implement this objective
‐Project Director ‐Statewide Infant Mental Health Council
9/30/13
2. Explore the possibility of providing thebump.com website with Florida specific resources on parenting
‐Project Director ‐Local community ECC and parenting providers
3/31/13
Objective 3.b.2 (Service)
EBPs are utilized in early childhood settings
PRIORITY
Work plan developed Select EBP’s are implemented
1. Identify lead facilitator / agency to convene and staff process
‐DCF SAMH Program Office
9/30/13
2. Engage local early childhood coalitions (ECC) & groups to inventory system capacity & gaps
‐Local Project Directors
‐Local Early Childhood community
9/30/13
3. Identify Early Childhood EBPs and administer EBP survey to early childhood community
‐DCF SAMH Program Office
‐Florida Center 9/30/13
4. Provide TA in response to the survey including training the child care workforce to notice signs and symptoms early and how to deal with specific challenges prior to diagnosis.
‐DCF SAMH Program Office
‐Local community Local community ECC and parenting providers & FSU
9/30/13
5. Ensure child care contracts and licensure includes EBPs in their Continuing Education credits and training plans
‐DCF SAMH Program Office
‐FSU, Local ECC & parenting providers
9/30/13
Objective 3.b.3 (Service)
Trauma Services are available, especially for child welfare youth
Joint workgroup for TIC and SOC
1. Focus on Trauma Informed Care Trainings for Child Welfare staff, foster parents related to children 0‐5 as this is the largest percentage of children removed from homes.
‐Statewide TIC Workgroup
‐Child serving agencies ‐Providers ‐CBC’s
9/30/14
2. Ensure that members of the SOC planning workgroup are also on the Trauma Informed Care workgroup.
‐Statewide SOC Project Director
‐Statewide SOC Core Team
10/31/12
3. Coordinate the goals and objectives in the SOC Strategic Plan and the goals and objectives in the trauma informed care workgroup strategic plan.
‐Statewide SOC Project Director
‐Statewide SOC Core Team ‐TI Care Workgroup
9/30/16
4. Coordinate regional trauma informed workgroups in the local system of care.
‐Local SOC Coordinator
‐TI Care Workgroup 9/30/14

27
Core Strategy: Creating Financing Mechanisms Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 3.c.1 (Financing) Funding opportunities for prevention services & universal promotion
Educational materials developed for dissemination
1. Creating training and education for HMO’s about cost effectiveness of prevention and outreach.
‐‐Statewide SOC Core Team
‐AHCA 9/30/15
2. Link with AHCA to have these services covered under Medicaid.
‐Statewide SOC Core Team
‐AHCA 9/30/16
Core Strategy: Providing Training, Technical Assistance, and Coaching
Objective 3.d.1 (Training & TA) Educating primary care providers regarding availability of behavioral health screenings and how and where to refer young children
PRIORITY
Training Plans and materials for developed for dissemination Trainings and outreach to medical professionals
1. Bright Futures Initiative‐American Pediatric Society provides on their website holistic screenings to be used by pediatricians during well visits. Possible linkage with this already provided resources to include referrals for local SOC. Educating pediatrician offices regarding this free resource and benefit to patients and their families.
‐DCF SAMH Program Office Circuit 2
‐Florida Chapter of APA Association ‐CMS ‐Florida Center for Early Childhood ‐Florida Association for Infant Mental Health
9/30/13
2. Reach out to local pediatric society to provide awareness material and presentations to local pediatric doctors and nurses concerning early childhood mental health issues and training on use of the medical home model in providing holistic care to infants and young children and their families.
‐DCF SAMH Program Office Circuit 2
‐Florida Chapter of American Pediatric Association ‐CMS
9/30/13
3. Work with higher education on developing strategies to reach out to medical and nursing schools to provide exposure to early childhood mental health issues and providing holistic care to infants and young children and their families.
‐DCF SAMH Program Office Circuit 2
‐USF, FSU, UM and other Florida institutions of higher education
9/30/13
4. Utilize existing early childhood mental health collaboratives (e.g., Miami/Dade Children’s Trust, Hillsborough Early Childhood Council) as demonstration sites.
‐DCF SAMH Program Office Circuit 2
‐Local SOC Planning Teams
9/30/13

28
Goal #4: Implement Local System of Care Sites
Core Strategy: Implementing Policy, Administrative, and Regulatory Changes Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 4.a.1 (Policy) Assess each Florida region for readiness, opportunities and needs to implement local SOC’s
PRIORITY
All regions complete a readiness/needs assessment in the areas of family involvement, partner collaboration, quality of communication, cultural and linguistic competence, and EBP utilization
1. Reevaluate current SOC readiness assessment and inventory other readiness and needs assessments, modify as necessary for dissemination throughout the state.
‐DCF SAMH Program Office
‐Managing Entities ‐DCF SAMH Regional Offices
3/31/13
2. Ensure the readiness assessment is in plain language and family and youth friendly.
‐DCF SAMH Program Office
‐Consortium of family & youth orgs ‐CLC Coordinator
3/31/13
3. Ensure the assessment is available in other languages, including Spanish and Creole.
‐CLC Coordinator
‐DCF SAMH Program Office
3/31/13
4. Find multiple ways to engage families and youth in completion of the readiness/needs assessment.
‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office
9/30/13
5. Disseminate assessment to community stakeholders. ‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office
9/30/13
6. Develop mechanisms that allow information gathered through the readiness/needs assessment process to be disseminated broadly and quickly through multiple media
‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office
9/30/13
Objective 4.a.2.(Policy) Infrastructure for local SOC planning and implementation
PRIORITY
Completion of local strategic plans
1. Identify community leader / champion for SOC implementation
‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office ‐Consortium of family & youth orgs
3/31/13
2. Identify and engage community partners in the planning and implementation process – create local planning team. Ensure that families and youth are included in all implementation councils and groups.
‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office ‐Consortium of family & youth orgs
6/30/13
3. Develop strategic plan including a financing and service array plan.
‐Local SOC Planning Teams
9/30/13
4. Set clear expectations, protocols and standards of core performance for SOC implementation
‐Local SOC Planning Teams
‐SOC Core Team ‐CLC Coordinator
9/30/13
5. Provide training and technical assistance to local implementation sites, including a web‐based toolkit
‐DCF SAMH Program Office
‐Mentors from past & current SOC sites
9/30/13 ‐ongoing

29
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Coordinated with Timeframe/Due Date
Objective 4.a.3.(Policy) Continuous Quality Improvement processes for SOC service and infrastructure implementation
Expansion regions have evaluation plan with specific data requirements inclusive of process and clinical measures
1. Develop indicators based on SOC values and principles using the grant required outcome measures
‐Local SOC Coordinator
‐Evaluation Team ‐Local SOC Planning Teams
6/30/13
2. Ongoing surveys of participants in the SOC on quality of process. Surveys should have room for comments either in writing, or audio/video feedback if on‐line.
‐Local SOC Coordinator
‐Evaluation Team
10/1/12‐9/30/16
3. Any performance measures, surveys and reports (quantitative and qualitative) are to be written in common language to be reviewed by youth and parents with an ongoing feedback loop.
‐Local SOC Coordinator
‐Evaluation Team ‐Consortium of youth & family orgs ‐CLC Coordinator
10/1/12‐9/30/16
4. Make all assessments and data available on SOC webpage.
‐State SOC Project Director
‐Local SOC Coordinator
10/1/12‐9/30/16
5. Identify ways for families to access computers to access (i.e. link with local libraries, ACCESS kiosks).
‐Local SOC Planning Teams
‐Evaluation Team ‐Consortium of youth & family orgs
9/30/13
Core Strategy: Developing Services and Supports Based on the System of Care Philosophy and Approach
Objective 4.b.1. (Service) An array of needed services and supports are available
PRIORITY
All regions complete a readiness/needs assessment
1. Use multiple sources of information to conduct local needs assessments to determine:
a. What services are provided / available b. Who receives these services c. What the ideal array of services and supports
are (e.g., mobile crisis, team planning, respite)
‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office
9/30/13
2. Educate communities on array of services that have been successful for the population of focus in areas similar to their community (i.e. rural vs. urban, ethnic make‐up, poverty prevalence, etc.)
‐Managing Entities ‐DCF SAMH Regional Offices ‐Family & Youth Run Orgs
‐DCF SAMH Program Office ‐CLC Coordinator
9/30/13
3. Advocate with funders and providers to change / expand array based on need.
‐Managing Entities ‐DCF SAMH Regional Offices ‐Family & Youth Run Orgs
‐DCF SAMH Program Office
9/30/13
4. Create a mechanism for ongoing gap analysis ‐Managing Entities ‐DCF SAMH Regional Offices
‐DCF SAMH Program Office ‐Family & Youth Orgs
9/30/13

30
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Coordinated with Timeframe/Due Date
Objective 4.b.2 (Service) Youth & families have equal access to services across systems & locations that are: 1.) Community‐based, 2.) Strengths‐based, 3.) Culturally & linguistically responsive, 4.) Holistic and 5.) Individualized
Increase in utilization of community based services
1. Educate communities on the array of services provided in a comprehensive SOC
‐Local SOC Coordinator
‐Local SOC Planning Teams ‐Family Org
3/31/14
2. Implement team planning approaches such as Wraparound for case management
‐Managing Entity ‐Local Providers ‐Local SOC Planning Teams
9/30/14
3. Identify a champion for Wraparound at the state level ‐Statewide SOC Core Team
9/30/13
4. Hire staff who are representative of the cultures prevalent in the community that they serve
‐Providers ‐CLC Coordinator 9/30/16
5. Include being multi‐lingual as a preferred qualification for service providers
‐Providers ‐CLC Coordinator 9/30/16
Core Strategy: Creating Financing Mechanisms
Objective 4.c.1 (Financing) Financing mechanisms sustain services consistent with SOC values & principles
PRIORITY
Financing grids that identify funding sources on the state level and local levels.
1. Convene Financing Workgroups on state & local levels to identify all potential sources & opportunities such as county government, independent tax districts, etc.
‐SOC Core Team ‐DCF SAMH Regional Offices
‐State Mental Health Planning Council
9/30/13
2. Develop financing plans in conjunction with the Strategic Implementation Plan
a. Statewide plan b. Local plans
‐SOC Core Team ‐DCF SAMH Regional Offices
‐State Mental Health Planning Council
9/30/13

31
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Coordinated with Timeframe/Due Date
Objective 4.c.2 (Financing) Financial structures promote flexibility, reduce duplication, and support SOC values
Funding follows the child as opposed to the service
1. Review and revise policies that promote multiple assessments and discourage assessment updates
‐Statewide SOC Project Director
‐Local SOC Planning Teams ‐Providers
10/1/12‐9/30/16
2. Assessments follow the child and family across providers and agencies
‐Local SOC Coordinator
‐Local SOC Planning Teams ‐Providers
10/1/12‐9/30/16
3. Identify and develop a crosswalk for flex funding opportunities in local communities
‐Local SOC Coordinator
‐Local SOC Planning Teams ‐Providers
10/1/12‐9/30/16
4. Identify / create / clarify mechanisms that allow maximal flexibility and support SOC values and principles, e.g., Care Management Entities, Administrative Service Organizations.
‐Statewide SOC Project Director
‐Local SOC Planning Teams ‐AHCA ‐Managing Entities ‐MCO’s
10/1/12‐9/30/16
5. Clarify similarities and differences between managed care organizations and managing entities
‐Statewide SOC Project Director
‐AHCA ‐DCF SAMH Program Office
10/1/12‐9/30/16
6. Standardize structures of MCO ‐AHCA 10/1/12‐9/30/16
Core Strategy: Providing Training, Technical Assistance, and Coaching
Objective 4.d.1 (Training & TA)
Provide a SOC blueprint to local communities outlining strategies for successful implementation.
PRIORITY
Web‐based, Florida specific SOC Implementation Toolkit
1. Develop a SOC orientation training that can be easily tailored for multiple audiences, including families and youth.
‐DCF SAMH Program Office
‐Core Planning Team
12/31/12
2. Develop a Florida SOC Implementation toolkit utilizing existing resources such as the Oklahoma Model.
3. Identify and update a system navigation guide written in plain language (no acronyms) by parents for other parents such as the Florida Parent Navigator
‐DCF SAMH Program Office
‐Core Planning Team ‐Consortium of Youth & Family Orgs
3/31/13
4. Market test all written materials prior to distribution
‐DCF SAMH Program Office
‐Core Planning Team ‐Consortium of Youth & Family Orgs
3/31/13
5. Make toolkit available in multiple media, including web‐based
‐DCF SAMH Program Office
3/31/13
32
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Coordinated with Timeframe/Due Date
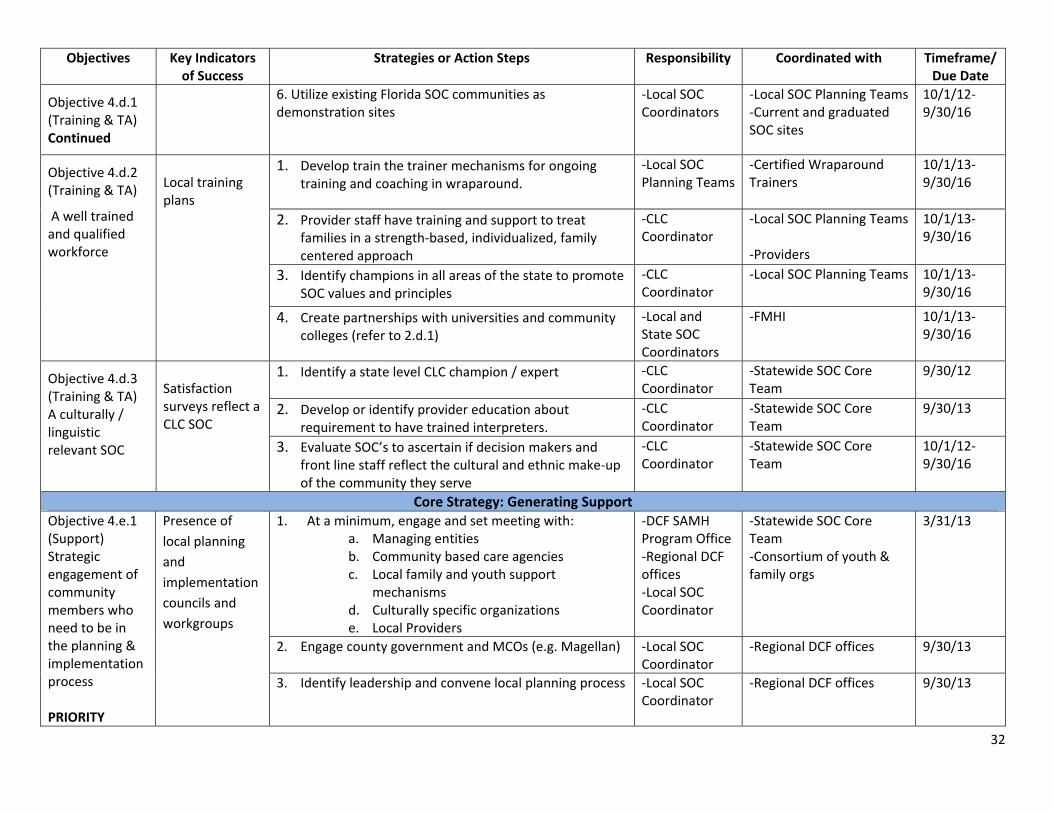
Objective 4.d.1 (Training & TA) Continued
6. Utilize existing Florida SOC communities as demonstration sites
‐Local SOC Coordinators
‐Local SOC Planning Teams‐Current and graduated SOC sites
10/1/12‐9/30/16
Objective 4.d.2 (Training & TA)
A well trained and qualified workforce
Local training plans
1. Develop train the trainer mechanisms for ongoing training and coaching in wraparound.
‐Local SOC Planning Teams
‐Certified Wraparound Trainers
10/1/13‐9/30/16
2. Provider staff have training and support to treat families in a strength‐based, individualized, family centered approach
‐CLC Coordinator
‐Local SOC Planning Teams ‐Providers
10/1/13‐9/30/16
3. Identify champions in all areas of the state to promote SOC values and principles
‐CLC Coordinator
‐Local SOC Planning Teams
10/1/13‐9/30/16
4. Create partnerships with universities and community colleges (refer to 2.d.1)
‐Local and State SOC Coordinators
‐FMHI 10/1/13‐9/30/16
Objective 4.d.3 (Training & TA) A culturally / linguistic relevant SOC
Satisfaction surveys reflect a CLC SOC
1. Identify a state level CLC champion / expert ‐CLC Coordinator
‐Statewide SOC Core Team
9/30/12
2. Develop or identify provider education about requirement to have trained interpreters.
‐CLC Coordinator
‐Statewide SOC Core Team
9/30/13
3. Evaluate SOC’s to ascertain if decision makers and front line staff reflect the cultural and ethnic make‐up of the community they serve
‐CLC Coordinator
‐Statewide SOC Core Team
10/1/12‐9/30/16
Core Strategy: Generating Support Objective 4.e.1 (Support) Strategic engagement of community members who need to be in the planning & implementation process PRIORITY
Presence of
local planning
and
implementation
councils and
workgroups
1. At a minimum, engage and set meeting with: a. Managing entities b. Community based care agencies c. Local family and youth support
mechanisms d. Culturally specific organizations e. Local Providers
‐DCF SAMH Program Office ‐Regional DCF offices ‐Local SOC Coordinator
‐Statewide SOC Core Team ‐Consortium of youth & family orgs
3/31/13
2. Engage county government and MCOs (e.g. Magellan) ‐Local SOC Coordinator
‐Regional DCF offices 9/30/13
3. Identify leadership and convene local planning process ‐Local SOC Coordinator
‐Regional DCF offices 9/30/13

33
Goal #5: Implementation of Evidence Based Practices Core Strategy: Implementing Policy, Administrative, and Regulatory Changes
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 5.a.1 (Policy) Accountability standards for providers to implement EBP’s that highlight individualized, family‐centered care PRIORITY
Contracts and monitoring protocols outlining expectations for EBP implementation
1. Managing Entities contracts require 80% of DCF publicly funded services must be EBP’s
‐DCF SAMH Program Office
‐Managing Entity ‐Family and Youth Organizations
9/30/13
2. Monitoring entities check for evidence that SOC values and EBP’s are implemented to fidelity.
‐DCF SAMH Program Office ‐AHCA ‐DJJ
‐Managing Entity ‐Family and Youth Organizations
9/30/13
3. Monitor the participation of youth and families in the identification of EBP’s for their community.
‐DCF SAMH Program Office ‐AHCA ‐DJJ
‐Managing Entity ‐Family and Youth Organizations
9/30/13
4. Implement a mechanism to collect ongoing feedback from the community on the effectiveness of implemented EBP’s (i.e. Angie’s list for EBP)
‐DCF SAMH Program Office ‐AHCA ‐DJJ
‐Managing Entity ‐Family and Youth Organizations
9/30/13
5. Convene workgroup with AHCA to explore how Medicaid can increase use of EBP’s
‐DCF SAMH Program Office ‐AHCA ‐DJJ
‐Managing Entity ‐Family and Youth Organizations
9/30/13
Objective 5.a.2 (Policy) Incentives for providers to implement EBP’s
EBP workgroup that includes all parties Statewide toolkit for implementing and sustaining and EBP
1. Identify and convene workgroup with multiple levels of expertise. Local workgroups could be established to leverage resources
‐Statewide and local SOC Coordinators
‐State and local SOC planning teams
10/1/13‐9/30/14
2. Educate providers on EBPs and how to sustain fidelity ‐EBP workgroup ‐State and local SOC planning teams
10/1/13‐9/30/16
3. Require % of workers within providers have certain certification.
‐Managing Entities ‐DCF SAMH Program Office ‐AHCA ‐Florida Council on Comm. Behavioral Health
10/1/15‐9/30/16

34
Objectives Key Indicators of Success
Strategies or Action Steps Responsibility Champion
Coordinated with Timeframe/Due Date
Objective 5.a.2 (Policy) Incentives for providers to implement EBP’s
CONTINUED
4. Obtain buy‐in from funders through education on improved outcomes and cost‐effectiveness
‐EBP workgroup ‐State and local SOC planning teams ‐Florida Council on Comm. Behavioral Health
10/1/13‐9/30/16
5. Quarterly calls with EBP workgroup that gives providers and opportunity to talk about successes and barriers
‐EBP workgroup 10/1/13‐9/30/16
6. Information from workgroup informs training and TA content
‐EBP workgroup ‐State and local SOC planning teams
10/1/13‐9/30/16
Core Strategy: Developing Services and Supports Based on the System of Care Philosophy and Approach
Objective 5.b.1. (Service) Broad statewide implementation of EBPs
PRIORITY
Increase to baseline on use of EBPs to fidelity
1. Annual provider self‐assessment
‐DCF SAMH Program Office ‐AHCA ‐DJJ
‐Providers, families & youth
9/30/13
2. Use NIATX models (quick change process improvement strategy) for implementing and assessing fidelity to an EBP
DCF SAMH Program Office
‐Providers 9/30/13
3. Provide incentives for providers for EBP implementation to fidelity (e.g. free training)
‐Managing Entities, ‐AHCA ‐DJJ
9/30/13
4. Develop review and monitoring process to assess implementation and fidelity checks, including cost to providers
‐DCF SAMH Program Office
‐Providers 9/30/13
5. Develop and sustain a competent workforce able to implement EBP’s to fidelity
‐Providers 9/30/13
6. Educate families and youth what EBPs are
‐Statewide SOC Core Team
‐Consortium of youth & family orgs
9/30/13
7. Ensure that EBPs identified include trauma‐informed and trauma‐specific interventions
DCF SAMH Program Office ‐AHCA
‐Maureen Honan, DJJ, Chair Statewide Trauma‐informed Care Interagency Workgroup
3/31/13

35
Core Strategy: Creating Financing Mechanisms Objectives Key Indicators
of Success Strategies or Action Steps Responsibility
Champion Coordinated with Timeframe/
Due Date
Objective 5.c.1 (Financing) Maximize funding for EBPs
PRIORITY
Develop matrix of funding sources and how they can be used to fund EBPs
1. Crosswalk all funding sources with EBPs to identify funding gaps (e.g., funding for supervision to ensure fidelity)
‐EBP Workgroup ‐Providers ‐AHCA ‐Managed Care Organizations ‐DJJ, DCF, DOH, DOE, ‐family and youth advocates ‐CSCs and county government
9/30/13
2. Create local / regional training collaborative to coordinate and share resources for trainings (e.g. Broward County)
‐Local SOC Coordinators
‐Local SOC Planning Teams
10/1/13‐9/30/15
3. MOU’s to address leveraging resources for shared ‘train the trainer’ trainings.
‐Local SOC Coordinator
‐Local SOC Planning Teams
10/1/13‐9/30/15
Core Strategy: Providing Training, Technical Assistance, and Coaching
Objective 5.d.2. (Training & TA) Trauma Informed Care
YEARS 2‐4
TI and trauma‐specific curricula are developed or identified for varied audiences including families, youth, and for populations and in settings for children, youth and youth adults 0‐25
1. Develop or identify curricula on TI Care, e.g., through National Child Traumatic Stress Network (NCTSN), for use with families and youth
‐DCF SAMH Program Office ‐AHCA
‐Statewide and Circuit Trauma‐informed Care Interagency Workgroups ‐Seminole Families and Communities Together (FACT) ‐Florida’s NCTSN sites
3/31/13
2. Develop statewide Trauma Informed Care training plan that includes EBPs and leverages state and local expertise and experience
‐DCF SAMH Program Office ‐AHCA
‐Statewide and Circuit Trauma‐informed Care Interagency Workgroups ‐Seminole (FACT) ‐Florida’s NCTSN sites
9/30/13

36
Glossary of Acronyms
211 - Telephone and web-based information and referral ACCESS - Automated Community Connection to Economic Self Sufficiency (food/temporary cash/medical assistance program) AHCA – Agency for Health Care Administration APA – American Pediatric Association APD - Agency for Persons with Disabilities CBHA - Comprehensive Behavioral Health Assessment CLC - Cultural and Linguistic Competence CMS - Children’s Medical Services CQI - Continuous Quality Improvement CW-CBC Child Welfare – Community-Based Care DCF SAMH - Department of Children and Families Substance Abuse and Mental Health Program Office DJJ - Department of Juvenile Justice DOE – Department of Education DOH – Department of Health EBP - Evidence-Based Practice(s) ECC - Early Childhood Coalition(s) ESE – Exceptional Student Education FMHI - Louis de la Parte Florida Mental Health Institute FSU - Florida State University HMO – Health Maintenance Organization IT – Information Technology MCO - Managed Care Organization ME - Managing Entity MH – Mental Health MOUs – Memoranda of Understanding NCTSN - National Child Traumatic Stress Network QA/QI – Quality Assurance / Quality Improvement SED – Serious Emotional Disturbance SEDNET - Network for Students with Emotional/Behavioral Disabilities SOC – System of Care TA – Technical Assistance TI – Trauma-Informed TIC Trauma - Informed Care UM - University of Miami USF – University of South Florida

37
References
Stroul, B., & Friedman, R. (1986). A system of care for children and youth with severe emotional
disturbances (rev. ed.). Washington, DC: Georgetown University Child Development
Center, National Technical Assistance Center for Children’s Mental Health.
Hernandez, M. & Hodges, S. (2006). Applying a theory of change approach to interagency
planning in child mental health. American Journal of Community Psychology, 38(3/4),
165-73.
Hernandez, M. & Hodges, S. (2005) Crafting logic models for systems of care: Ideas into action. [Making children’s mental health services successful series; no. 216-1-rev]. Tampa, FL: University of South Florida, The Louis de la Parte Florida Mental Health Institute, Department of Child & Family Studies. Available at http://rtckids.fmhi.usf.edu/rtcpubs/CMHseries/IdeasintoAction.html
Stroul, B., & Friedman, R.M. (2011). Effective strategies for expanding the system of care
approach. A report on the study of strategies for expanding systems of care. Atlanta, GA: ICF Macro.
Stroul, B., Blau, G., & Friedman, R. (2010). Updating the system of care concept and philosophy.
Washington, DC: Georgetown University Center for Child and Human Development, National Technical Assistance Center for Children’s Mental Health.