supraspinatus tendinitis
DESCRIPTION
Supraspinatus TendinitisTRANSCRIPT

Supraspinatus Tendinitis

Supraspinatus tendinitis is associated with Subacromial Impingement Syndrome, Shoulder Impingement Syndrome or Rotator Cuff Tendinitis
Inflammation of the tendon of the supraspinatus muscle leads to supraspinatus tendinitis. This is the most common cause of shoulder pain.
or

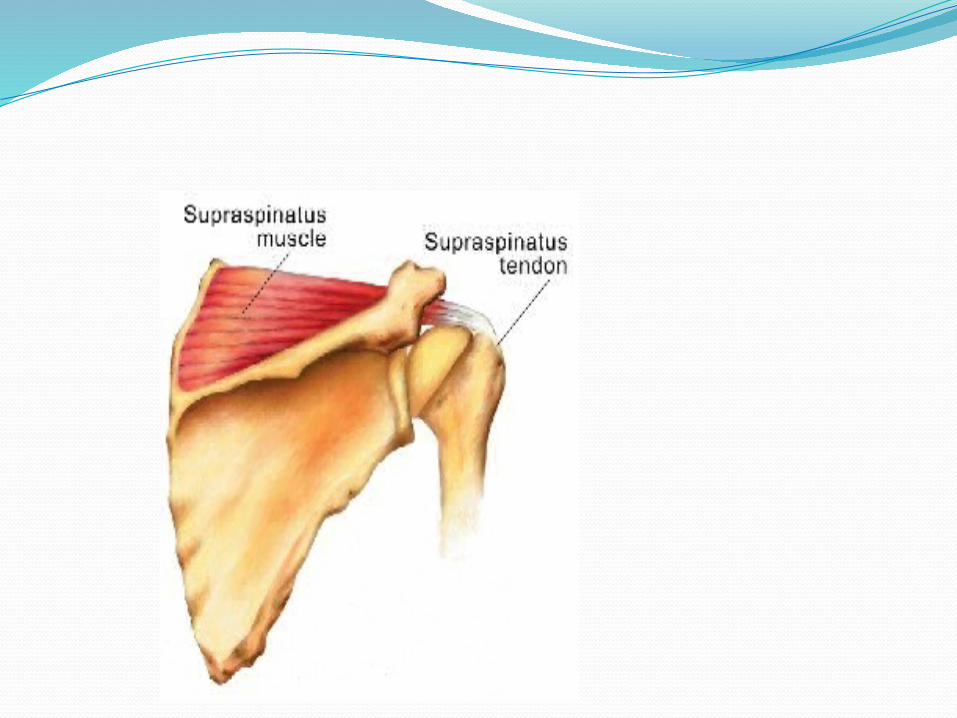
supraspinatus muscle which one of the four rotator cuff muscles in the shoulder and it passes over the top of the joint to attach to the top of the humerus .
Tendonitis generally affects more than one of these muscles and is known as rotator cuff tendonitis.


The Cause and Risk Factors of Supraspinatus TendonitisThe main cause of supraspinatus tendonitis is repetitive over-use of the muscle, which causes small tears to occur in the tendon fibers. The supraspinatus tendon is at risk of being pinched in the joint during repetitive movement
The risk factors include sports which involve repetitive over-arm actions as in swimming, pitching and weight lifting. Age is another risk factor as the tendons become more brittle and less elastic as we age.

Other causes include genetic abnormality, shoulder instability, unaccustomed intense exercise and lack of adequate raised arm raised are required. core strength. Workplace and household activities can also cause tendonitis,

Supraspinatus tendonitis can also be caused by extrinsic and intrinsic factors.
Extrinsic factors are divided into primary and secondary impingement. Increased subacromial loading, overhead activities, or trauma can cause primary impingement. Rotator cuff overload and muscle imbalance can cause secondary impingement. Supraspinatus tendonitis can also occur because of the decrease in the supraspinatus outlet space due to underlying instability of the glenohumeral joint

The supraspinatus outlet is a space formed by the acromion, acromioclavicular joint, and coracoacromial arch. The supraspinatus tendon runs through this outlet. Any abnormalities of this outlet can cause impingement of the supraspinatus tendon.


Incidence/Prevalence
In patients younger than 40 years of age, Supraspinatus Tendinitis occurs usually due to glenohumeral instability, acromioclavicular joint disease, or trauma.
Patients older than 40 years of Supraspinatus Tendinitis mostly due to degenerative joint disease, glenohumeral impingement syndrome, or rotator cuff disease. Most people who are at risk for Supraspinatus Tendinitis are people whose job requires repetitive overhead motions and athletes who compete in sports such as swimming, throwing sports, volleyball etc.age, experience

The Symptoms of Supraspinatus Tendonitis
The major symptoms of supraspinatus tendonitis are pain and inflammation.
The tiny tears that occur in the tendon cause inflammation which in turn, causes pain. The pain will start as mild, felt mainly after activity that uses the arm raised to the side, above shoulder-height. Moderate pressure on the tip of the shoulder will be painful. If not treated, the pain increases in duration and strength; it will be felt at other times, especially at night.

Other symptoms include stiffness and weakness of the shoulder joint, pain when the arm is raised, restricted movement and difficulty getting comfortable in bed.
There is also possibility of tenderness and swelling in the upper front part of the shoulder and in some severe cases, difficulty to raise the arm to shoulder level. Positive Neer’s, Hawkins and Empty Can Test indicate Supraspinatus Tendinitis.Patients also present with painful arc between 60o and 120o of shoulder abduction.

TREATMENTTime and rest are the most effective treatment of
supraspinatus tendonitis. Tendons can heal themselves, given rest and sufficient time. Continuing to exercise with tendonitis can cause it to progress to a serious condition that may need surgery to repair.
Exercise must be stopped, especially the actions that caused the tendonitis, and the shoulder rested. Application of ice for the first few days is essential to reduce swelling and inflammation. Hold an ice pack to the shoulder for 15 to 20 minutes every 1 to 2 hours for the first 48 hours.

Inflammation is treated with anti-inflammatory medications and topical gels. By treating the inflammation, PPAIN CAN NE RELEAVED. Supporting and immobilizing the arm will help to prevent inadvertent movements and assist in the healing.
As the pain starts to ease, small movements of the arm can be started, followed by light strengthening exercise. It is important to avoid any painful movements.

The Prevention of Supraspinatus Tendonitis
Once tendonitis, has occured there is a risk of a recurrence. Thus sufficient time is needed time for the tendons to heal fully before returning to sport or exercise. Focus is given on increasing the strength and flexibility of the shoulder muscles; this will help in the prevention of supraspinatus tendonitis.
IT IS ADVISED TO Always warm up and cool down with any exercise session,

SPECIAL TESTNeer’s, Hawkins-Kennedy, and Empty Can
Test are used to determine if patient has Supraspinatus Tendinitis2.
Neer’s Test is performed with patient seated. Physical therapist passively elevates patients arm and then medially rotates the arm. Pain indicates a positive sign.

Hawkins-Kennedy Test is also performed with patient in seated position. Therapist passively moves patients arm to 90o of shoulder flexion and 90oof elbow flexion. Arm is the medially rotated and moved in different angles of flexion or horizontal abduction. Pain indicates a positive sign.
Empty Can Test is performed with patient seated. Arms are abducted to 90o, internally rotated, thumbs are pointed down, and arms are moved about 30o forward. Therapist then applies resistance to abduction. Weakness or pain is positive sign.



DIAGNOSISAn orthopedist can recognize above
mentioned disorders of the supraspinatus tendon from the upward slipping of the head of the arm bone, and the pain that typically occurs during the middle range of lifting the arm.
X-ray helps in the diagnosis of a narrow coraco-acromial arch and acromial spurs.

An ultrasoundcan reveal tendon tears and tendinosis.
MRI is the only investigation that can detect tendinitis.
