sustainability and transformation partnership area: bath ... · virtual word (woc)(v) pn community...
TRANSCRIPT
#NHSAgeingWell
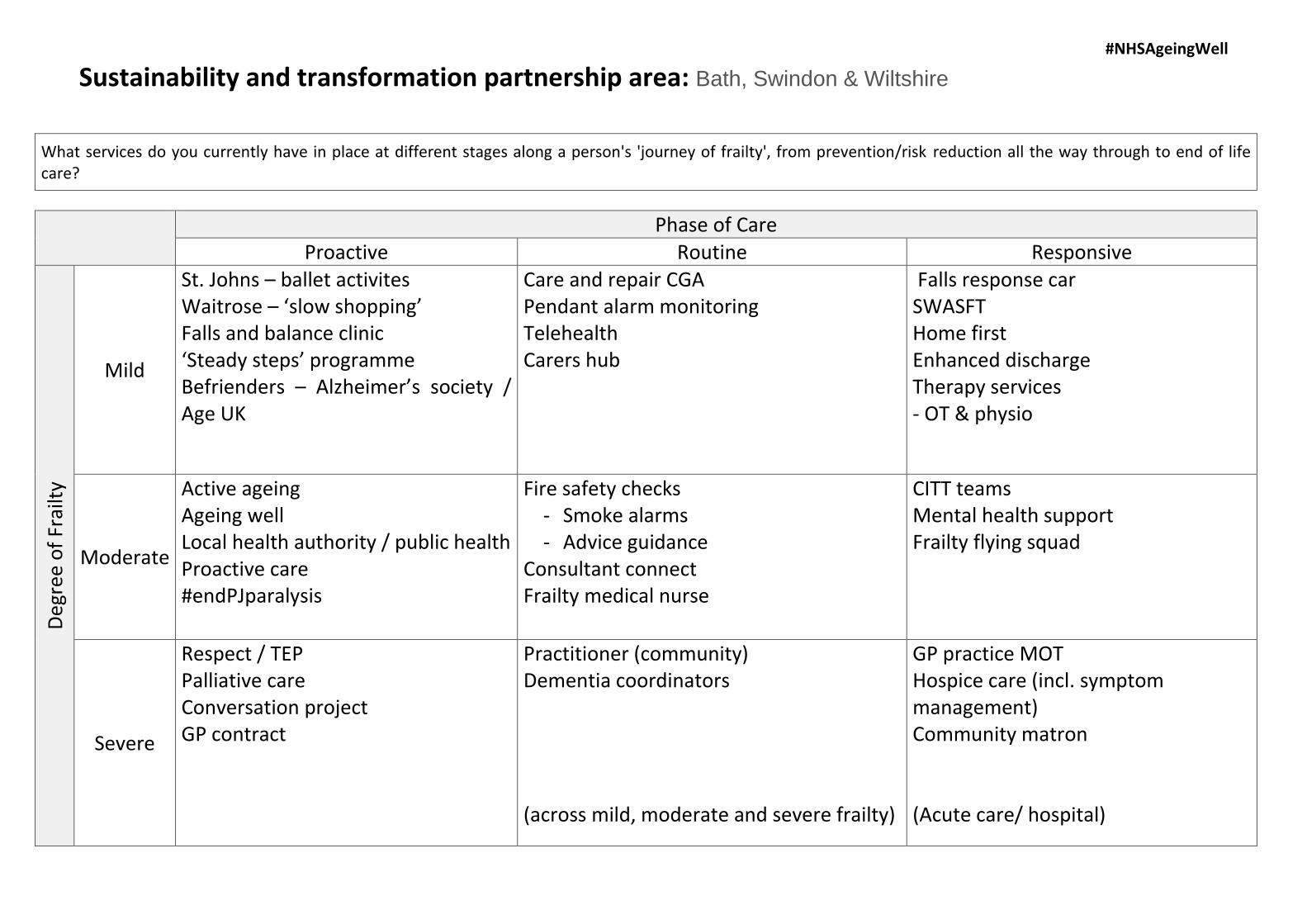
Sustainability and transformation partnership area: Bath, Swindon & Wiltshire
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
St. Johns – ballet activites Waitrose – ‘slow shopping’ Falls and balance clinic ‘Steady steps’ programme Befrienders – Alzheimer’s society / Age UK
Care and repair CGA Pendant alarm monitoring Telehealth Carers hub
Falls response car SWASFT Home first Enhanced discharge Therapy services - OT & physio
Moderate
Active ageing Ageing well Local health authority / public health Proactive care #endPJparalysis
Fire safety checks - Smoke alarms- Advice guidance
Consultant connect Frailty medical nurse
CITT teams Mental health support Frailty flying squad
Severe
Respect / TEP Palliative care Conversation project GP contract
Practitioner (community) Dementia coordinators
(across mild, moderate and severe frailty)
GP practice MOT Hospice care (incl. symptom management) Community matron
(Acute care/ hospital)
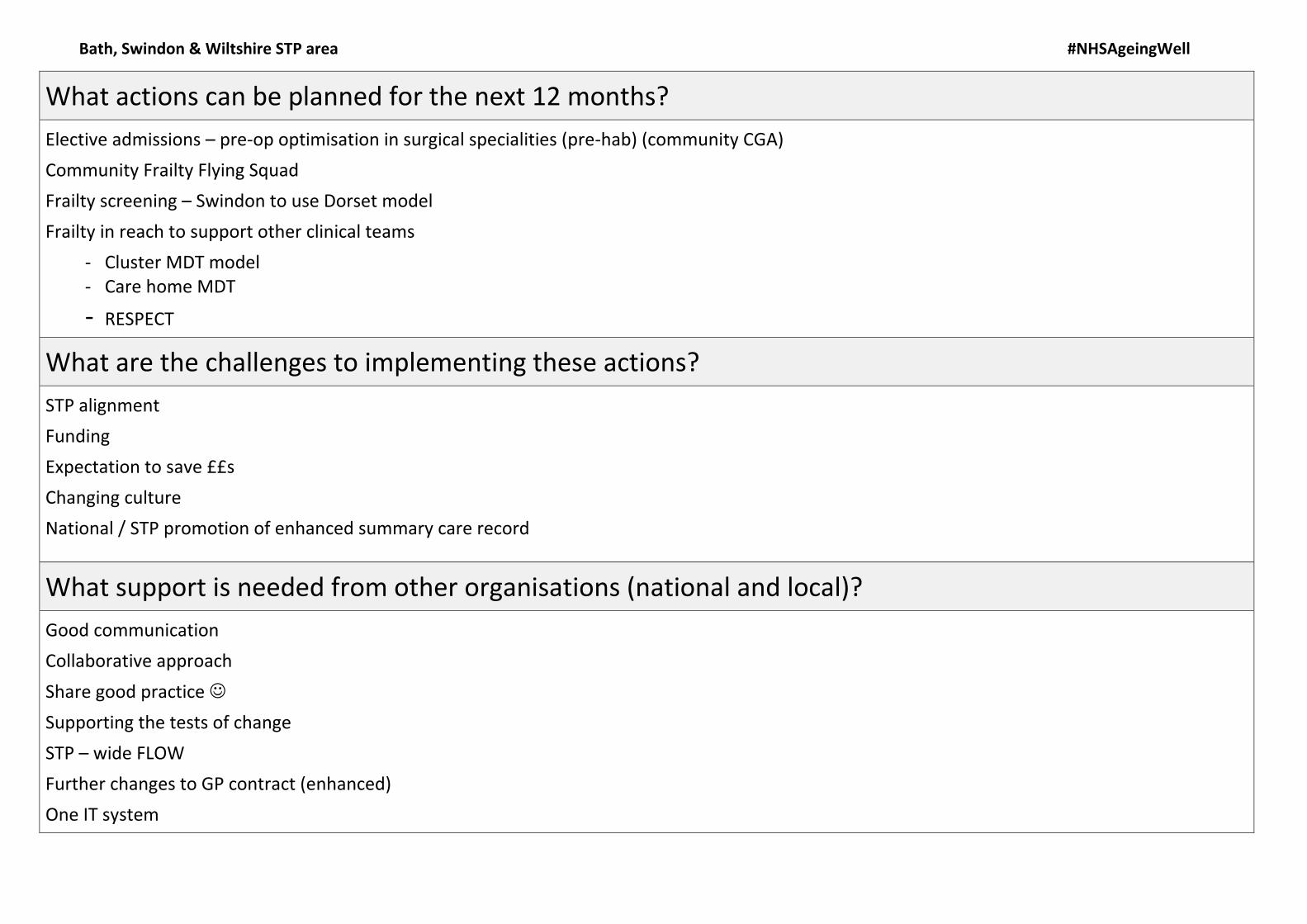
Bath, Swindon & Wiltshire STP area #NHSAgeingWell
What actions can be planned for the next 12 months?
Elective admissions – pre-op optimisation in surgical specialities (pre-hab) (community CGA)
Community Frailty Flying Squad
Frailty screening – Swindon to use Dorset model
Frailty in reach to support other clinical teams
- Cluster MDT model- Care home MDT
- RESPECT
What are the challenges to implementing these actions?
STP alignment
Funding
Expectation to save ££s
Changing culture
National / STP promotion of enhanced summary care record
What support is needed from other organisations (national and local)?
Good communication
Collaborative approach
Share good practice
Supporting the tests of change
STP – wide FLOW
Further changes to GP contract (enhanced)
One IT system
Bath, Swindon & Wiltshire STP area #NHSAgeingWell
Name
Victoria Nelson
Nic Aplin
Gemma Quick
Catherine Phillips
Patricia Gordon
#NHSAgeingWell
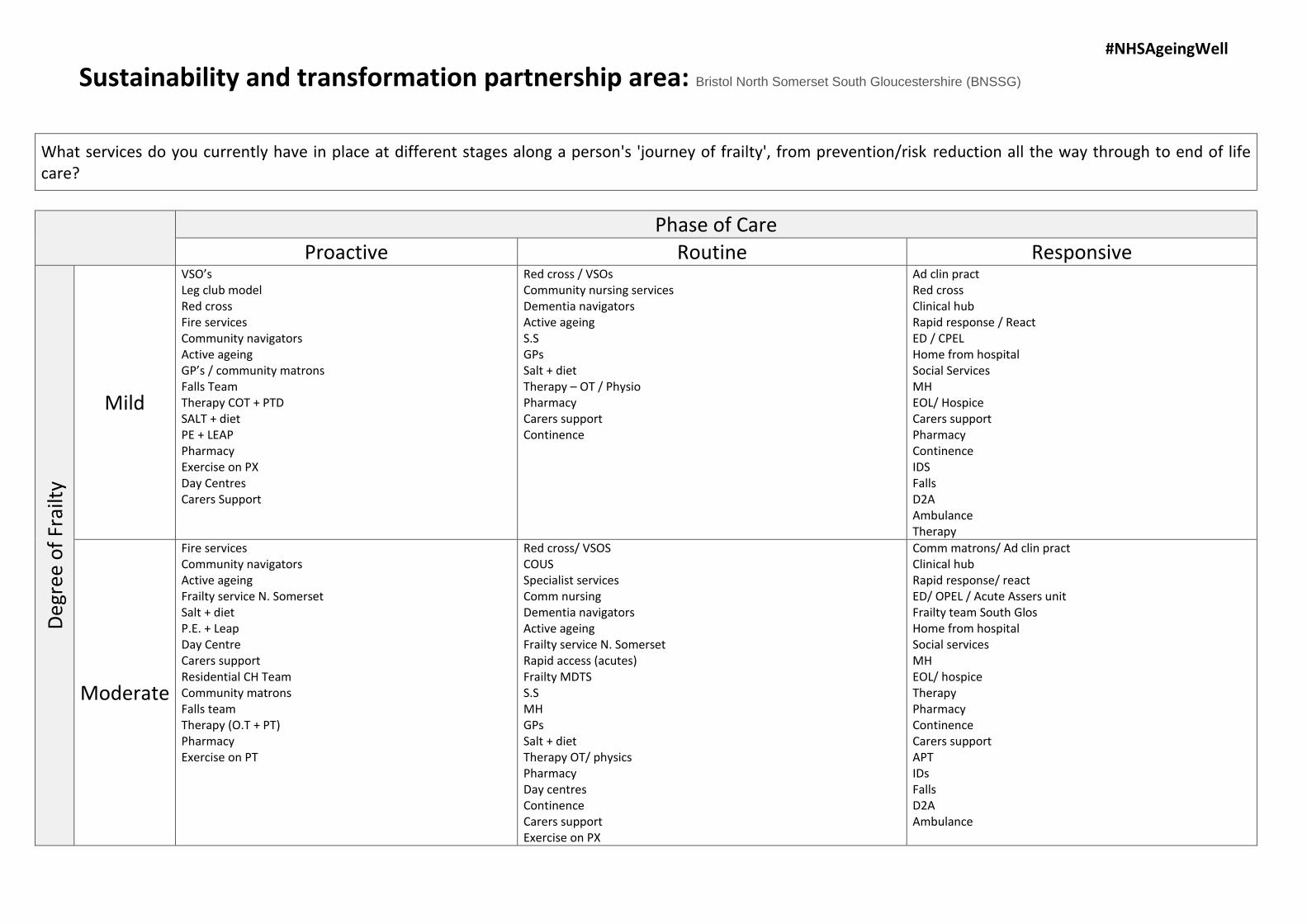
Sustainability and transformation partnership area: Bristol North Somerset South Gloucestershire (BNSSG)
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
VSO’s Leg club model Red cross Fire services Community navigators Active ageing GP’s / community matrons Falls Team Therapy COT + PTD SALT + diet PE + LEAP Pharmacy Exercise on PX Day Centres Carers Support
Red cross / VSOs Community nursing services Dementia navigators Active ageing S.SGPsSalt + dietTherapy – OT / PhysioPharmacyCarers supportContinence
Ad clin pract Red cross Clinical hub Rapid response / React ED / CPEL Home from hospital Social Services MH EOL/ Hospice Carers support Pharmacy Continence IDS Falls D2A Ambulance Therapy
Moderate
Fire services Community navigators Active ageing Frailty service N. Somerset Salt + diet P.E. + Leap Day Centre Carers support Residential CH Team Community matrons Falls team Therapy (O.T + PT) Pharmacy Exercise on PT
Red cross/ VSOS COUS Specialist services Comm nursing Dementia navigators Active ageing Frailty service N. Somerset Rapid access (acutes) Frailty MDTS S.SMHGPsSalt + dietTherapy OT/ physicsPharmacyDay centresContinenceCarers supportExercise on PX
Comm matrons/ Ad clin pract Clinical hub Rapid response/ react ED/ OPEL / Acute Assers unit Frailty team South Glos Home from hospital Social services MH EOL/ hospice Therapy Pharmacy Continence Carers support APT IDs Falls D2A Ambulance

#NHSAgeingWell
Severe
Fire services Salt + diet Community matrons Frailty service N. Somerset/ MDTS Residential CH Team GP/ Community matrons Therapy (OT +PT) Pharmacy Carers support
Red cross / VSOs Specialist services Comm nursing Dementia navigators Community matrons/ AD clin pract Frailty service N. Somerset Rapid access (acutes) Frailty MDTs GP’s S.SMHTherapy OT/ physicsPharmacyCarers supportSalt + diet
EOL/ hospice Clinical hub / SPA Rapid response/ react Comm matrons/ Ad clin pract ED/ OPEL / Acute Assers unit Frailty team South Glos Home from hospital Social services Social services MH Therapy Carers support APT IDs Falls D2A Ambulance
Bristol North Somerset South Gloucestershire (BNSSG)
#NHSAgeingWell
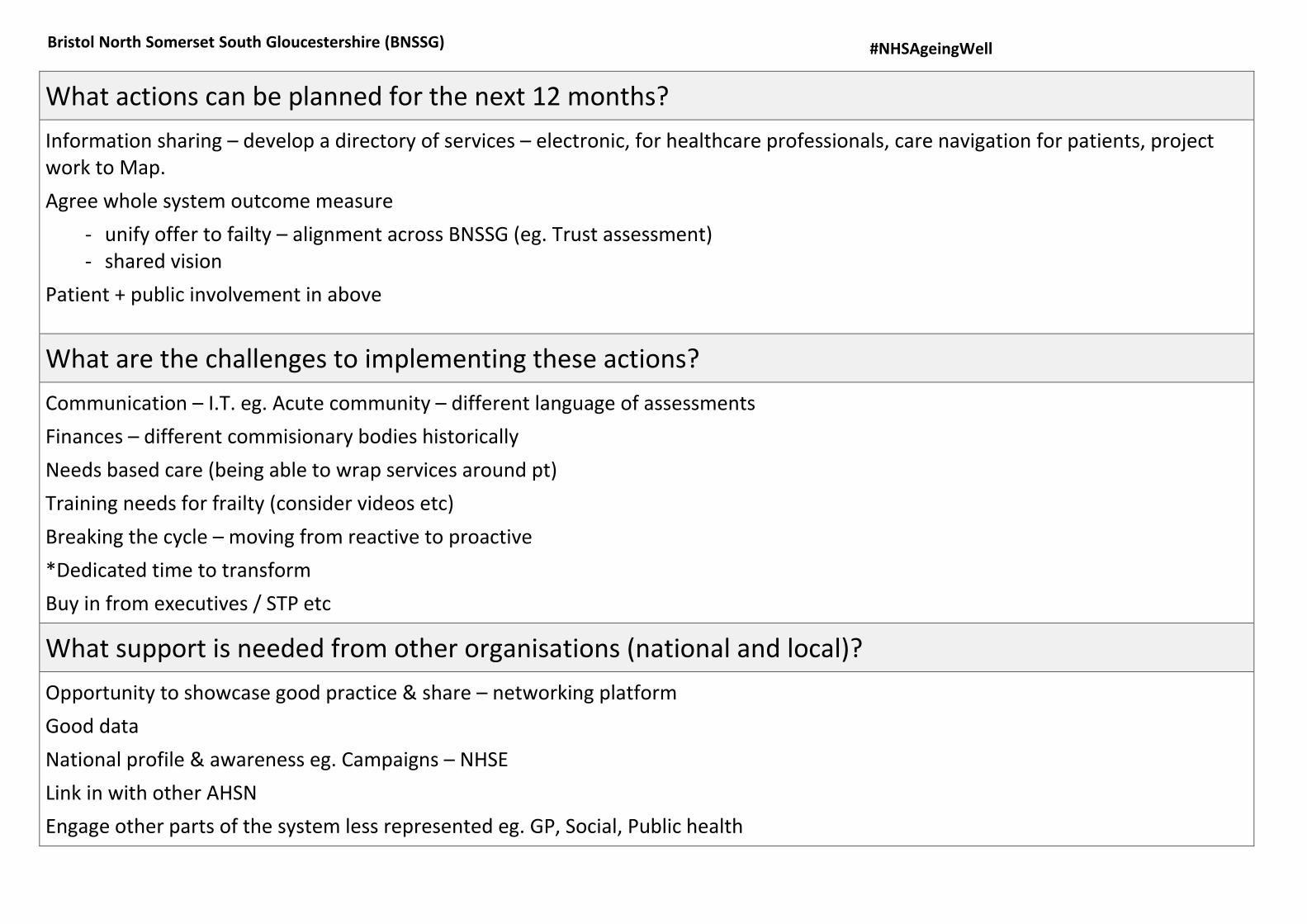
What actions can be planned for the next 12 months?
Information sharing – develop a directory of services – electronic, for healthcare professionals, care navigation for patients, project work to Map.
Agree whole system outcome measure
- unify offer to failty – alignment across BNSSG (eg. Trust assessment)- shared vision
Patient + public involvement in above
What are the challenges to implementing these actions?
Communication – I.T. eg. Acute community – different language of assessments
Finances – different commisionary bodies historically
Needs based care (being able to wrap services around pt)
Training needs for frailty (consider videos etc)
Breaking the cycle – moving from reactive to proactive
*Dedicated time to transform
Buy in from executives / STP etc
What support is needed from other organisations (national and local)?
Opportunity to showcase good practice & share – networking platform
Good data
National profile & awareness eg. Campaigns – NHSE
Link in with other AHSN
Engage other parts of the system less represented eg. GP, Social, Public health
Bristol North Somerset South Gloucestershire (BNSSG)
#NHSAgeingWell
Name
Nigel Jowles
Arvind Kumar
Sandra Akintola
Emma-Kate Reed
Jarrod Richards
Charlotte Kane Sabrina McAndrew
Denise Chambers
Allanagh Hart
Karen Field
Ben Piper
Vee Spandoni
Rachael Morris-Smith
Bristol North Somerset South Gloucestershire (BNSSG)

#NHSAgeingWell
Sustainability and transformation partnership area: Cornwall Green = RCHT | Blue = CPFT (community) | Led voluntary | Group work (v) = variable across the county
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Centipede clubs (v) PN Community makers Comm. Rehab Voluntary organisations (v) Memory cafés Health promo service (v) Merlin (ms charity) Living Well (v)
Health promo service (v) Falls service Specialist nurses PN Focus on frailty falls Facebook page Telecalls
GP Home first D2A SWASFT STEPS Community nurses Acute GPs Acute GPs ACAH
Moderate
Virtual word (woc)(v) PN Centipede clubs (v) Community makers vol. sector Comm. Rehab team Voluntary organisations (v) Memory cafes Health promo (v) Merlin (ms charity) Living Well
Falls practitioner Frailty nurses / CGA Therapies / frailty MDT Community matrons – case mgt Specialist nurses End of life spec nurses Falls clinic ® Community nurses Falls service PN comm. Rehab PCP
Silver phone – geriatricians Falls practitioner OPAL unit Frailty nurses/ CGA Therapies / Frailty MDT Liasion (Onward care) Acute GPS Falls/ eldercare clinic STEPS Red Cross 24 hr rehab end PJ paralysis ACAH CMS Home First D2A SWASFT
#NHSAgeingWell
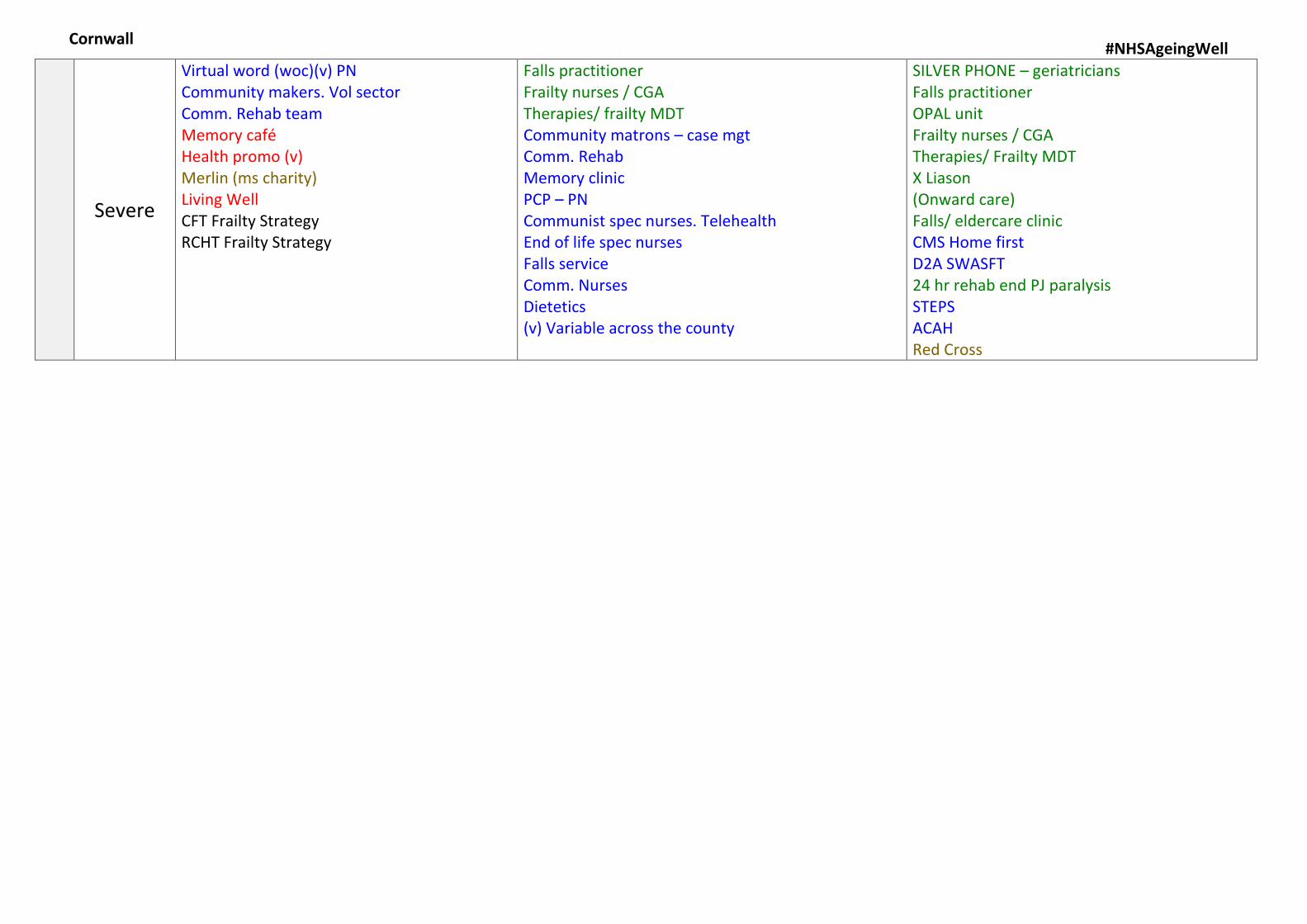
Severe
Virtual word (woc)(v) PN Community makers. Vol sector Comm. Rehab team Memory café Health promo (v) Merlin (ms charity) Living Well CFT Frailty Strategy RCHT Frailty Strategy
Falls practitioner Frailty nurses / CGA Therapies/ frailty MDT Community matrons – case mgt Comm. Rehab Memory clinic PCP – PN Communist spec nurses. Telehealth End of life spec nurses Falls service Comm. Nurses Dietetics (v) Variable across the county
SILVER PHONE – geriatricians Falls practitioner OPAL unit Frailty nurses / CGA Therapies/ Frailty MDT X Liason (Onward care) Falls/ eldercare clinic CMS Home first D2A SWASFT 24 hr rehab end PJ paralysis STEPS ACAH Red Cross
Cornwall
#NHSAgeingWell
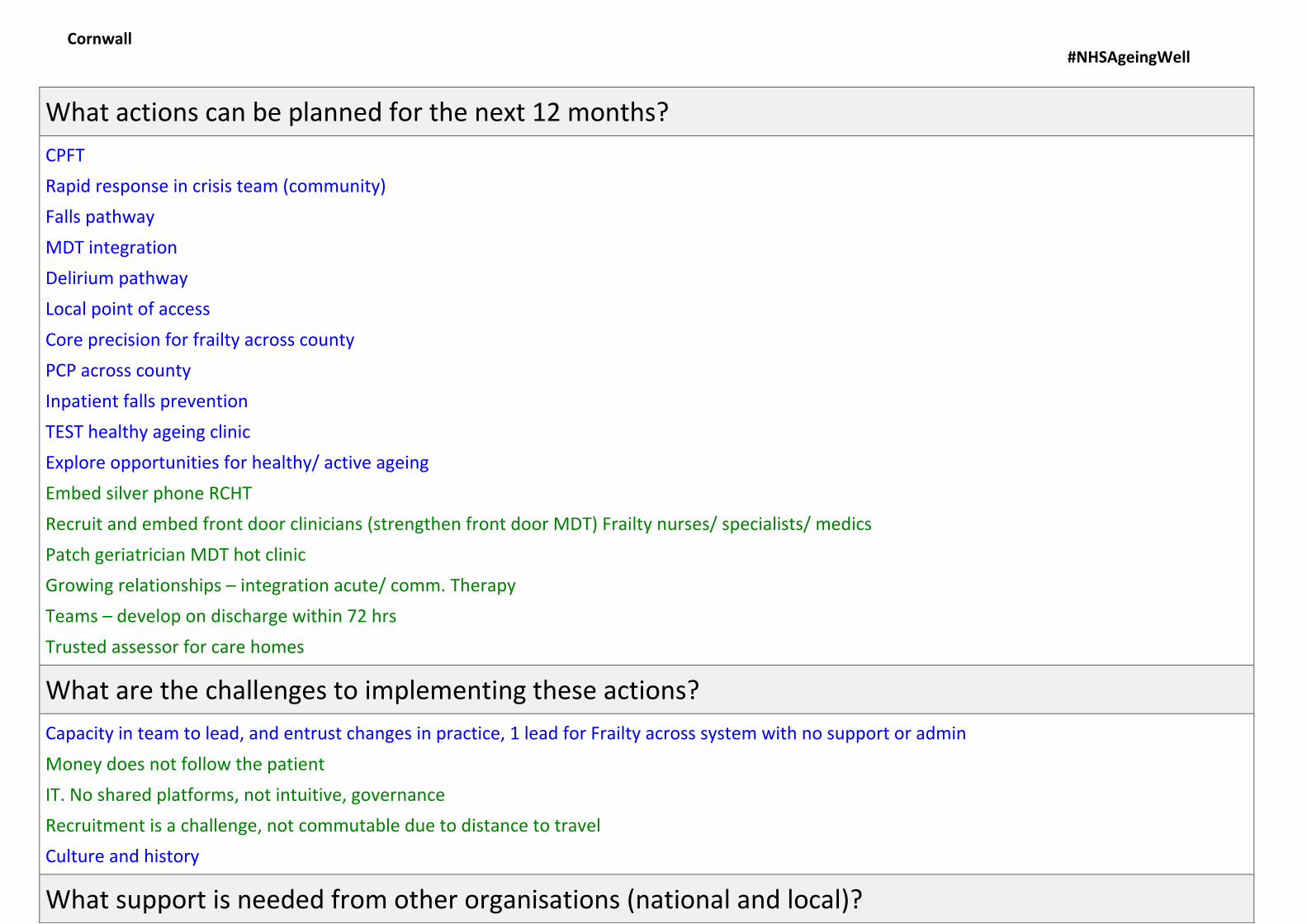
What actions can be planned for the next 12 months?
CPFT
Rapid response in crisis team (community)
Falls pathway
MDT integration
Delirium pathway
Local point of access
Core precision for frailty across county
PCP across county
Inpatient falls prevention
TEST healthy ageing clinic
Explore opportunities for healthy/ active ageing
Embed silver phone RCHT
Recruit and embed front door clinicians (strengthen front door MDT) Frailty nurses/ specialists/ medics
Patch geriatrician MDT hot clinic
Growing relationships – integration acute/ comm. Therapy
Teams – develop on discharge within 72 hrs
Trusted assessor for care homes
What are the challenges to implementing these actions?
Capacity in team to lead, and entrust changes in practice, 1 lead for Frailty across system with no support or admin
Money does not follow the patient
IT. No shared platforms, not intuitive, governance
Recruitment is a challenge, not commutable due to distance to travel
Culture and history
What support is needed from other organisations (national and local)?
Cornwall
#NHSAgeingWell
Name
Clare Rotman
Narissa Kelland
Fern Elkin
Laura Wesson
Naomi Wakely
Magda Morgan
Kerry Crowther
Marie Prior
Project management / admin supoort
Networks
Investment in the right places
Time
Learning proven models – not reinventing the wheels
“Pinching with pride”
Localise learning – a lot of very good conferences but difficult to attend London or North of country due to cost, releasing staff to attend
South West Frailty network resources| platform to share
Time to meet networks / colleagues locally / permission to practice and attend
Cornwall Fire service
Nationally accepted definition for frailty
Challenge national policies
Cornwall

#NHSAgeingWell
Sustainability and transformation partnership area: Devon
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Medication reviews Falls assessment Fire services AGE UK Befrienders Exercise groups League of friends GP
GP Practice nurse Community nurses AGE UK Falls nurse Parkinson’s nurse MND Nurse Specialist nurses Stroke nurse Ambulatory nursing clinics Community hospitals
Community nurses MAAT SWAST D2A RADS – rapid assessment discharge service GP Rapid response
Moderate
Voluntary services Community connectors Police Befrienders Community matrons Continence nurse GP
Community nurses Police GP Community pharmacists Voluntary services Care agencies Memory clinic Specialist nurses SALT Ambulatory nursing clinics
Social care reablement MAAT – medical admission avoidance team Police SWAST D2A RADS Intermediate care beds GP Rapid response
Severe
Community matrons Complex health and social care teams (Core group) Continence SALT GP
Core group Intermediate care Marie Curie CCT GP
Electronic Frailty Index Core Group
Urgent care response Intermediate care GP MAAT Marie Curie SWAST Crisis team Hospice D2A RADS
#NHSAgeingWell
Torbay RADS
Dawn Thomas
Louise Williams
Exeter Community
Karen Tetley – Team manager
Bonita Elworthy
Karen Riggs Matron
NEW Devon
Linda Haynes RGN
Marie Curie
Rapid response
Devon
#NHSAgeingWell
Name
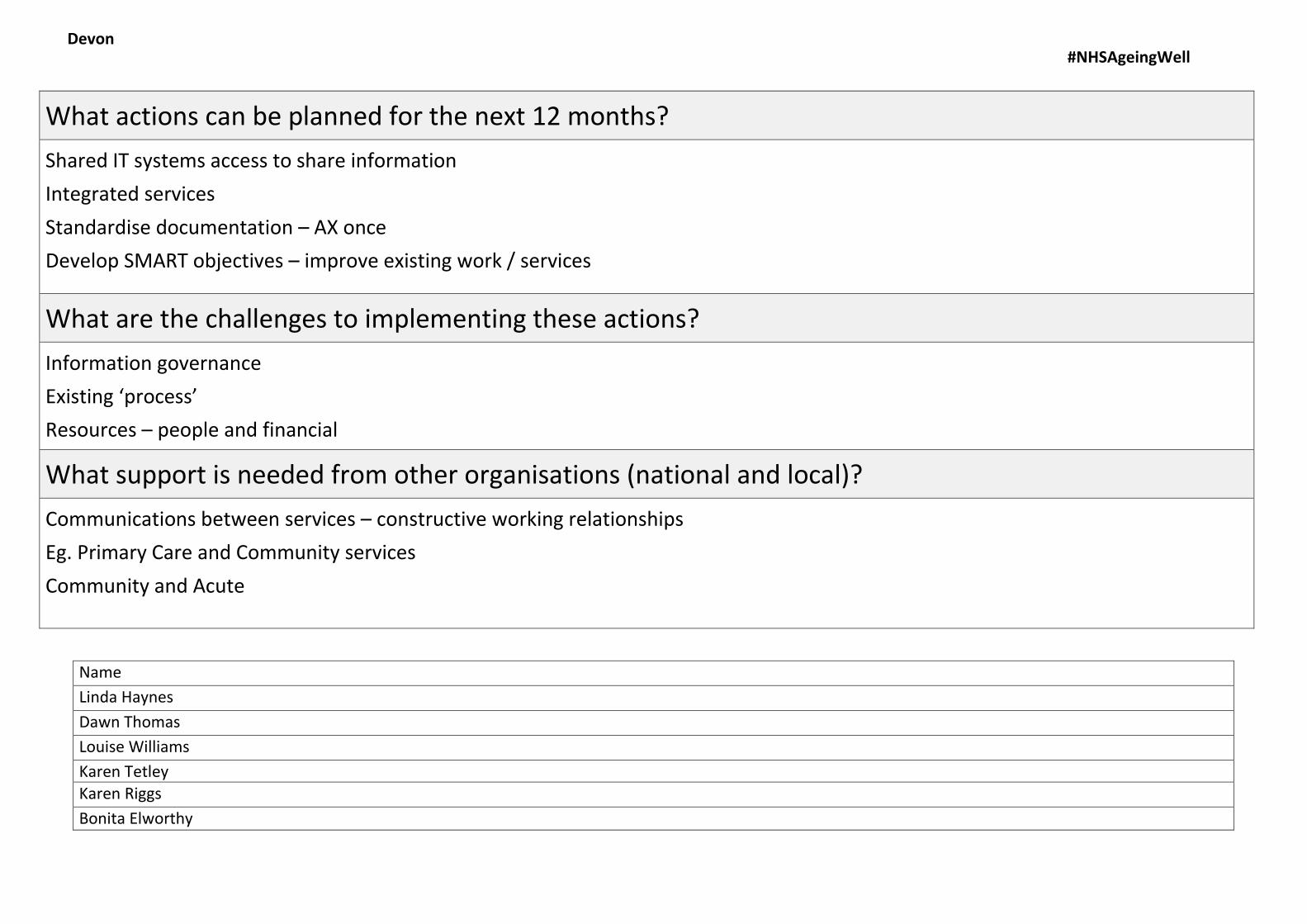
Linda Haynes
Dawn Thomas
Louise Williams
Karen Tetley
Karen Riggs
Bonita Elworthy
What actions can be planned for the next 12 months?
Shared IT systems access to share information
Integrated services
Standardise documentation – AX once
Develop SMART objectives – improve existing work / services
What are the challenges to implementing these actions?
Information governance
Existing ‘process’
Resources – people and financial
What support is needed from other organisations (national and local)?
Communications between services – constructive working relationships
Eg. Primary Care and Community services
Community and Acute
Devon

#NHSAgeingWell
Sustainability and transformation partnership area: Devon 2
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Medicine R/V’s within care homes Flu clinics Carers/ providers Frailty scores to map services AGE UK | Vol. services | housing Wellbeing services Library Public health / media/ churches day services Community transport
Annual R/V’s of long term conditions – specialist clinics Integrated MDT DN & CTT Dementia services O/P geriatric AX Caring for carers Dementia day service Singing for the brain Memory café and lunch clubs
Falls clinic/ service DTA / reablement Rapid response – A&E CCRT CCOMM. Crisis response team AC@H (Acute care at home) AAU (Acute care assessment) SWAST ESD Continence clinics Equipment provision Rehab / comm. Hospital Red Cross Memory service
Moderate
Flu clinics Care home promotion of H&WB Befriending services Comm. Transport Churches Day services Dementia action alliance Carers Fire services
Integrated MDT DN & CTT Long term conditions Dementia services O/P geriatric AX Care providers Respite Dementia day services
DTA/ reablement Rapid response CCRT AC@H AAO SWAST Memory service ESD (early supported discharge) Red Cross Continence clinics Equipment provision Rehab Placement in a care home
Severe
GP screening Flu clinics Care home promotion of H&WB Comm transport Carers
Integrated MOT DN & CTT Long term conditions Continence AX Care providers
DTA Rapid response CCRT EOL TEAMS AC@H

#NHSAgeingWell
Name
Anna Fort
Maria Kneller
Kylie Stonehouse
Amiel Celocia
Jon Green
Julian Elston
Fire service Respite AAU SWAST Red Cross Equipment Provision Placement in a care home
Devon 2
DEVON 2 STP #NHSAgeingWell
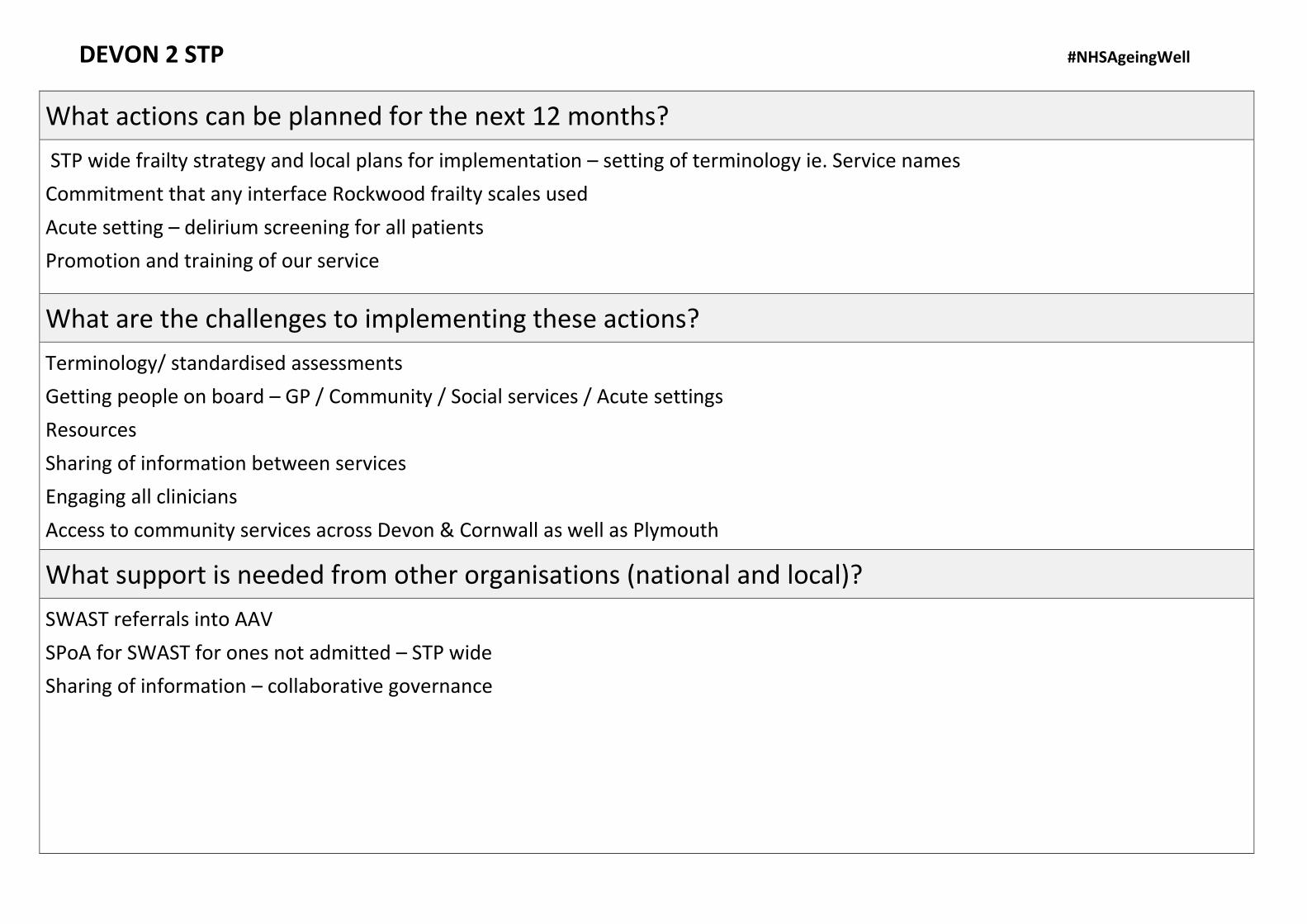
What actions can be planned for the next 12 months?
STP wide frailty strategy and local plans for implementation – setting of terminology ie. Service names
Commitment that any interface Rockwood frailty scales used
Acute setting – delirium screening for all patients
Promotion and training of our service
What are the challenges to implementing these actions?
Terminology/ standardised assessments
Getting people on board – GP / Community / Social services / Acute settings
Resources
Sharing of information between services
Engaging all clinicians
Access to community services across Devon & Cornwall as well as Plymouth
What support is needed from other organisations (national and local)?
SWAST referrals into AAV
SPoA for SWAST for ones not admitted – STP wide
Sharing of information – collaborative governance

DEVON 2 STP #NHSAgeingWell
Anna Fort
Maria Kneller
Kylie Stonehouse
Amiel Celocia
Jon Green
Julian Elston

#NHSAgeingWell
Sustainability and transformation partnership area: Devon 3
Name
Michelle Langrishe
Hannah Squires
Liz Bombieri
Debbie Stoodley
Helen Ruse
Caroline Barrett
Stephen Spratling
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Social prescribing Dementia nurse MDT clinic
Rockwood scale EFI
Community matrons + dementia admiral
Moderate
Community matron / nurses Falls Social prescribing Dam pharmacist MDT clinic falls
Rockwood scale Acute – comm. EFI Virtual ward/ core group Community therapy Falls team
CCRT AAU Dementia nurse Pharmacist Frailty AX @ A+E
Severe
Falls team Hospice MDT clinic Hospital @ Home TEP / contingency plans
EFI Community therapy Community matron Hospice
CCRT AAU Hospice Hospital@Home / AC@H Frailty AX @ A+E

DEVON 3 STP #NHSAgeingWell
What actions can be planned for the next 12 months?
Identification of frailty
1. Same tool2. Information sharing
Training | Commitment | Changing culture
Contingency planning – single care planning – across boundaries of care
Develop social prescribing system
What are the challenges to implementing these actions?
How information can be shared across IT systems – information data warehouse
Changing culture
Forward planning
Managing expectations / language
- Staff- Family
- Patients
What support is needed from other organisations (national and local)?
Standardisation nationally/ regionally/ local directions for frailty
Self management – national drive
Building resilient 3rd sector market
Rotations across organisations
DEVON 3 STP #NHSAgeingWell
Name
Debbie Stoodley Helen Ruse Caroline Barrett Hannah Squires
Liz Baobien Michelle Langrishe Stephen Sprattling
#NHSAgeingWell
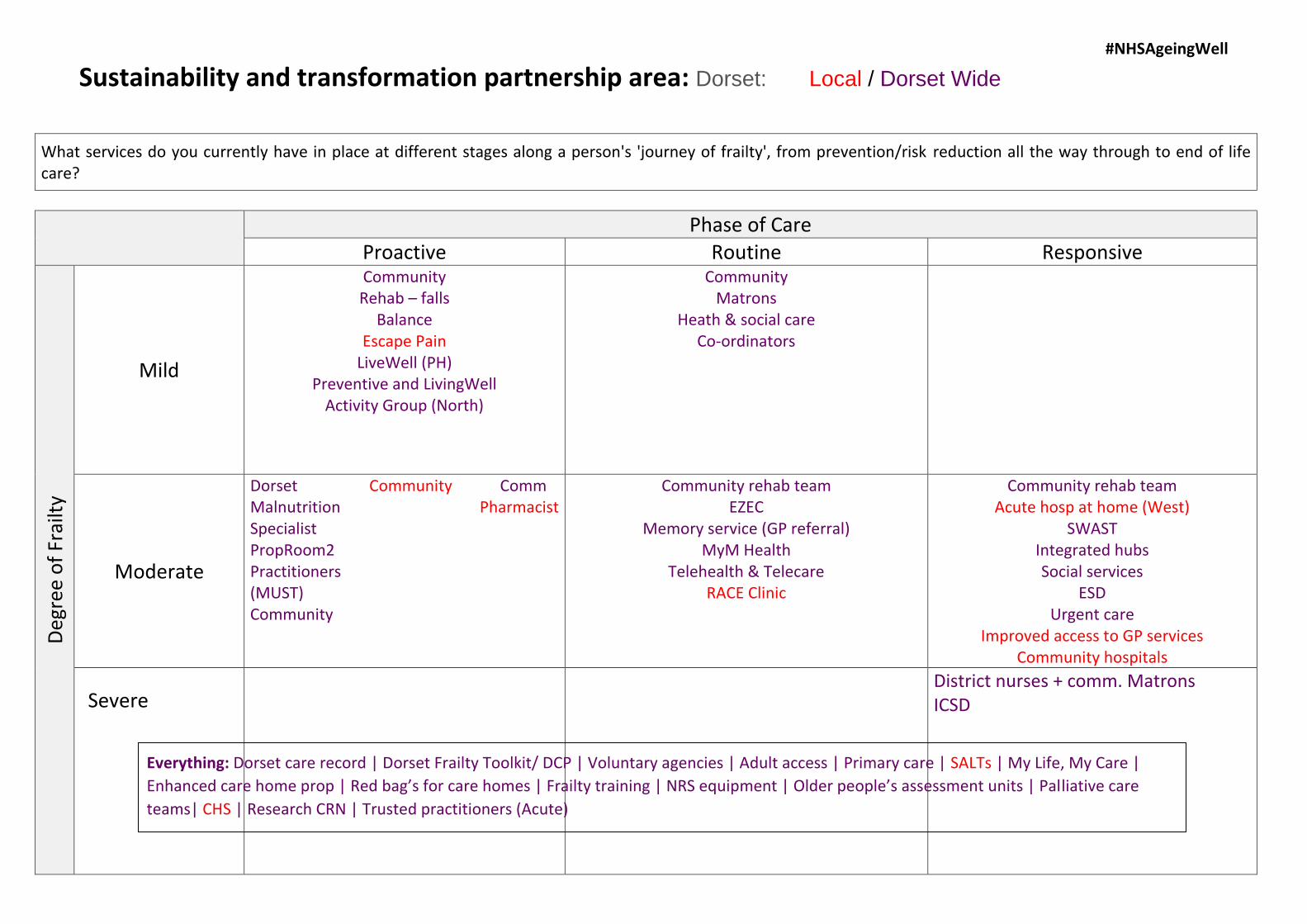
Sustainability and transformation partnership area: Dorset: Local / Dorset Wide
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Community Rehab – falls
Balance Escape Pain
LiveWell (PH) Preventive and LivingWell
Activity Group (North)
Community Matrons
Heath & social care Co-ordinators
Moderate
Dorset Community Comm Malnutrition Pharmacist Specialist PropRoom2 Practitioners (MUST) Community
Community rehab team EZEC
Memory service (GP referral) MyM Health
Telehealth & Telecare RACE Clinic
Community rehab team Acute hosp at home (West)
SWAST Integrated hubs Social services
ESD Urgent care
Improved access to GP services Community hospitals
District nurses + comm. Matrons ICSD Severe
Everything: Dorset care record | Dorset Frailty Toolkit/ DCP | Voluntary agencies | Adult access | Primary care | SALTs | My Life, My Care |
Enhanced care home prop | Red bag’s for care homes | Frailty training | NRS equipment | Older people’s assessment units | Palliative care
teams| CHS | Research CRN | Trusted practitioners (Acute)

Dorset #NHSAgeingWell Consistent approach to the recognition, assessment and care planning to recognise where patients are on the frailty continuum
What actions can be planned for the next 12 months?
Rollout and embed the Dorset Frailty Toolkit and care plan – consistent approach
Access to clinician by paramedics to provide devise ie. Conveyancing the pt.
How to care needs provide for short term need (e.g. care in hospital)
Fire service and paramedics able to refer patients to hubs (using health and social care coordinators)
Improve links with discharge teams
United CGA across primary / community / acute
Research
Consistent pathways & outcomes across Dorset – common expectations
Advanced care planning
Discharge planning
What are the challenges to implementing these actions?
Resources / staffing levels / variative across county – equality of service
Rural vs. urban
Out of country boundaries – accessing services
Lif live on a border – patients house a worse deal
Varying apendas in the different localities – issues with consistent county-wide roll-outs – improve partnerships
What support is needed from other organisations (national and local)?
“Real” “live” training on system 1 modules
Balance of contractual obligations vs. implement of change (block contracts)
True pooled budgets – locality not service based
NHS funding vs. “ability to pay” social services – how to resolve (national issue)
Dorset #NHSAgeingWell
Name
Andrew Dean
Laura Godfrey
Sue Bridge
Vikki Tweedy
Jane Thomas
Chris Connell
Sarah Morston
Sara Froud
Brad Rootes
Kathy Wallis

#NHSAgeingWell
Sustainability and transformation partnership area: Gloucestershire
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
EFI Rockwood Clinical assessment Healthy ageing/ exercise Community wellbeing service Fire service MDT – primary care Care coordinators Active Gloucestershire – HPA Risk strategy Memory café Health loading + PAM Dementia cafes
Wellbeing coordinators Care navigators Housing support office Telehealth / telecare Bone health + MSK Specialist services MDT care home support team
Enhanced discharge service
Moderate
Fire service PN-ANP MDT Personal health budgets
Community dementia nurses – pilot CGA Falls service GP + PN Leads – HCA PN ANP Frailty matrons + Community geriatriciansMDT
EDS/ OPAL /RR
Severe
MDT CGA ‘my goals’ ‘me at my best’ PLANS GP + PN heads Frailty matrons Community geriatricians MTD
Gloucestershire #NHSAgeingWell
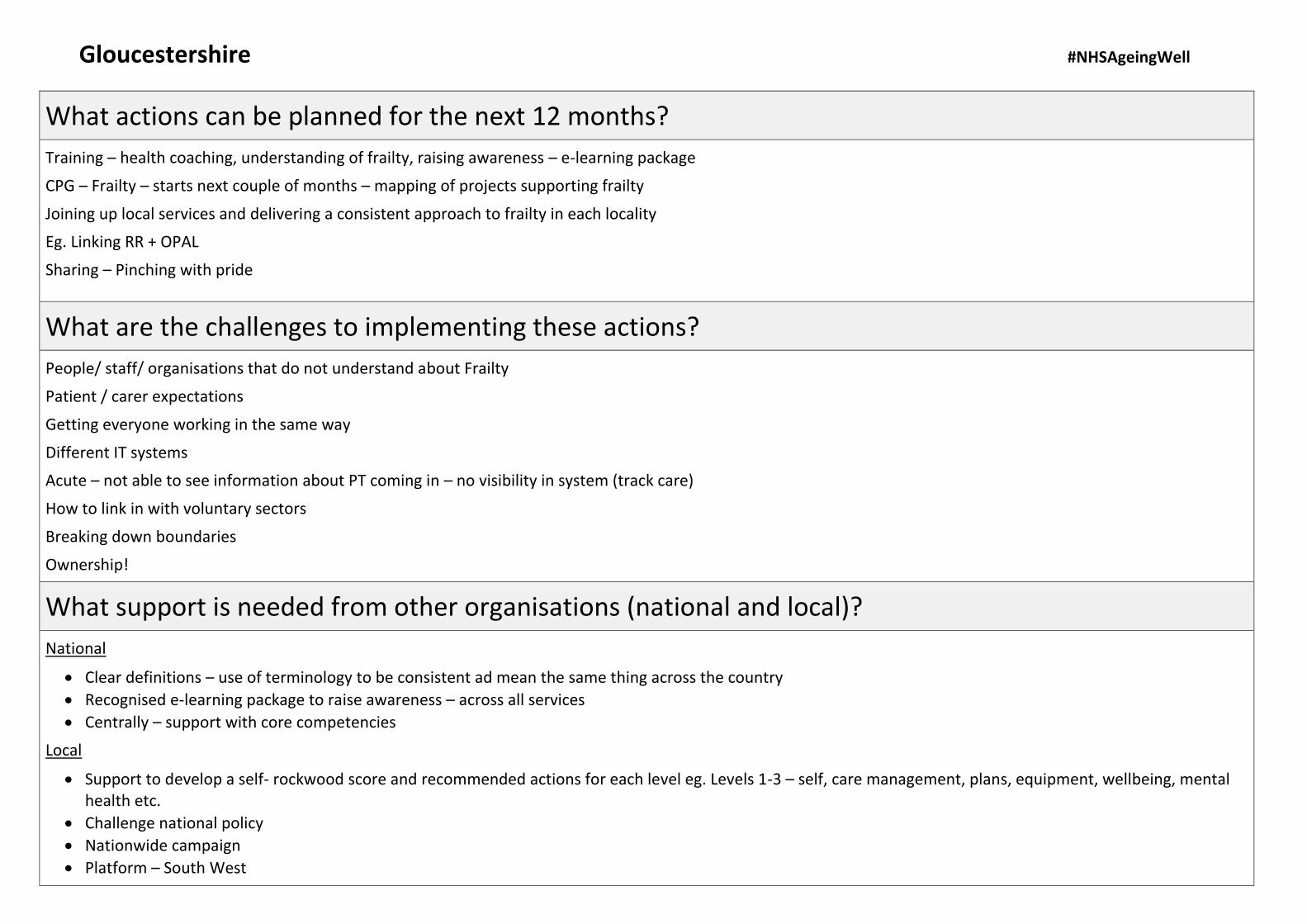
What actions can be planned for the next 12 months?
Training – health coaching, understanding of frailty, raising awareness – e-learning package
CPG – Frailty – starts next couple of months – mapping of projects supporting frailty
Joining up local services and delivering a consistent approach to frailty in each locality
Eg. Linking RR + OPAL
Sharing – Pinching with pride
What are the challenges to implementing these actions?
People/ staff/ organisations that do not understand about Frailty
Patient / carer expectations
Getting everyone working in the same way
Different IT systems
Acute – not able to see information about PT coming in – no visibility in system (track care)
How to link in with voluntary sectors
Breaking down boundaries
Ownership!
What support is needed from other organisations (national and local)?
National
Clear definitions – use of terminology to be consistent ad mean the same thing across the country
Recognised e-learning package to raise awareness – across all services
Centrally – support with core competencies
Local
Support to develop a self- rockwood score and recommended actions for each level eg. Levels 1-3 – self, care management, plans, equipment, wellbeing, mentalhealth etc.
Challenge national policy
Nationwide campaign
Platform – South West

Gloucestershire #NHSAgeingWell
Name
Jane Haros
Ian Donald
Helen Ballinger
Jackie Hagley
Terri Selby
Sandra Yates
Trudi Walker
(Hein Le Roux)

#NHSAgeingWell
Sustainability and transformation partnership area: Somerset
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Identification Cross county working Advance care planning FoPAS RHSS IRT Memory clinic IDS GP
Reassessing – medication R/V falls risk Health coach Community pharmacist
TEP county wide DNAR + TEP Interagency working
Moderate
CCG care home team Complex discharge ANP
CNS Paramedics
Symphony Social services Discharge to assess District nurses
A+E Trauma nurse Stroke nurse Mental health EOL discharge nurse Marie Curie
Severe
Somerset #NHSAgeingWell
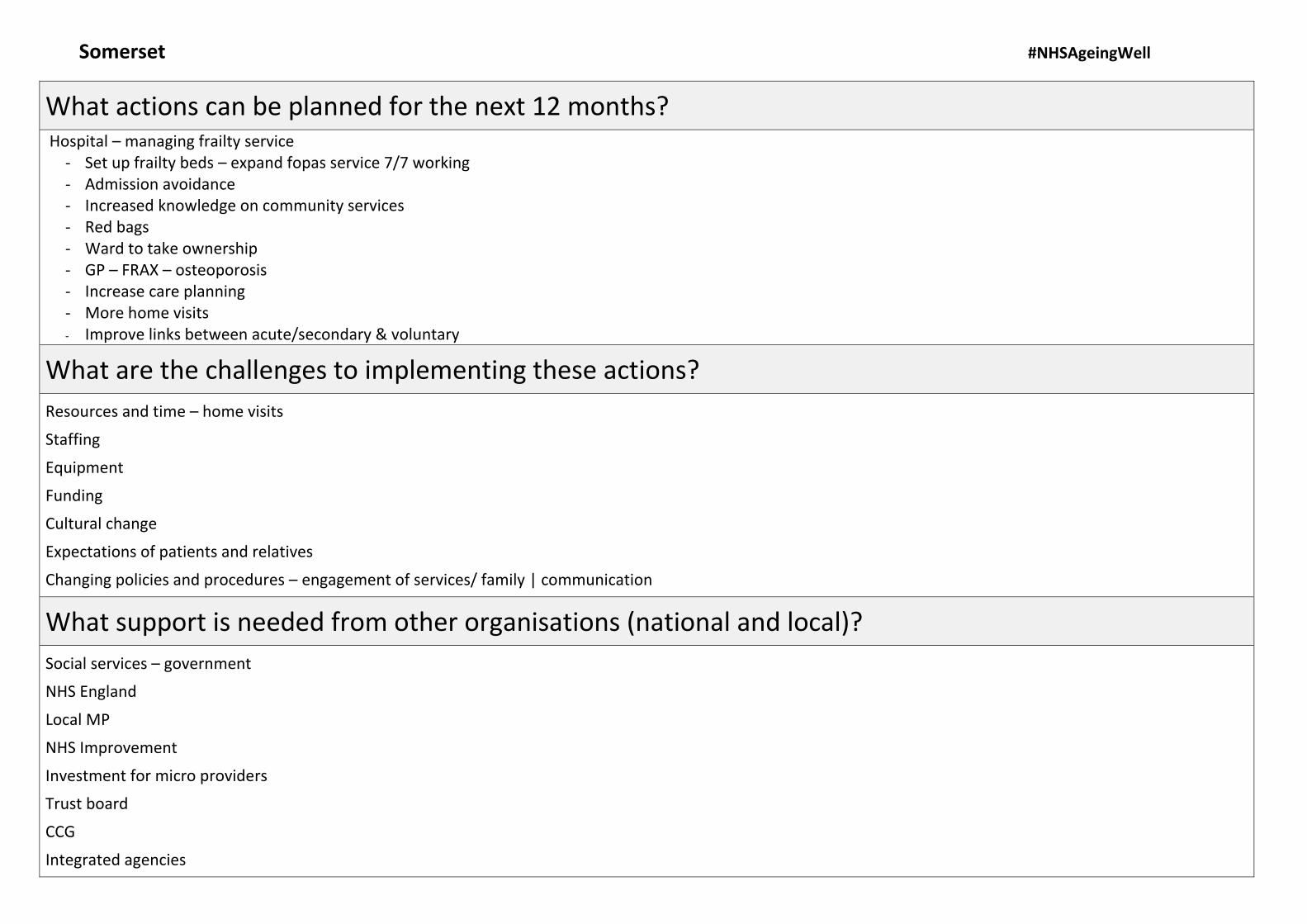
What actions can be planned for the next 12 months? Hospital – managing frailty service
- Set up frailty beds – expand fopas service 7/7 working- Admission avoidance- Increased knowledge on community services- Red bags- Ward to take ownership- GP – FRAX – osteoporosis- Increase care planning- More home visits- Improve links between acute/secondary & voluntary
What are the challenges to implementing these actions?
Resources and time – home visits
Staffing
Equipment
Funding
Cultural change
Expectations of patients and relatives
Changing policies and procedures – engagement of services/ family | communication
What support is needed from other organisations (national and local)?
Social services – government
NHS England
Local MP
NHS Improvement
Investment for micro providers
Trust board
CCG
Integrated agencies

Somerset #NHSAgeingWell
Name
Sharon Field
Anita Howe
Jacqui Dally
Jenny Perris
Darren Cox
Vikki Vose
Cathy Fone
Rebecca Sutton

#NHSAgeingWell
Sustainability and transformation partnership area: Somerset 2
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Health coaches Dementia service
Dementia service Community mental health teams Older people
Dementia service
Moderate
Taunton and area wellbeing service
District nursing Sompar complex care hubs FOPAS – acute hospital OPAL – acute hospital District nursing
Taunton and area wellbeing service
South Sompar complex care Severe
Somerset 2 #NHSAgeingWell
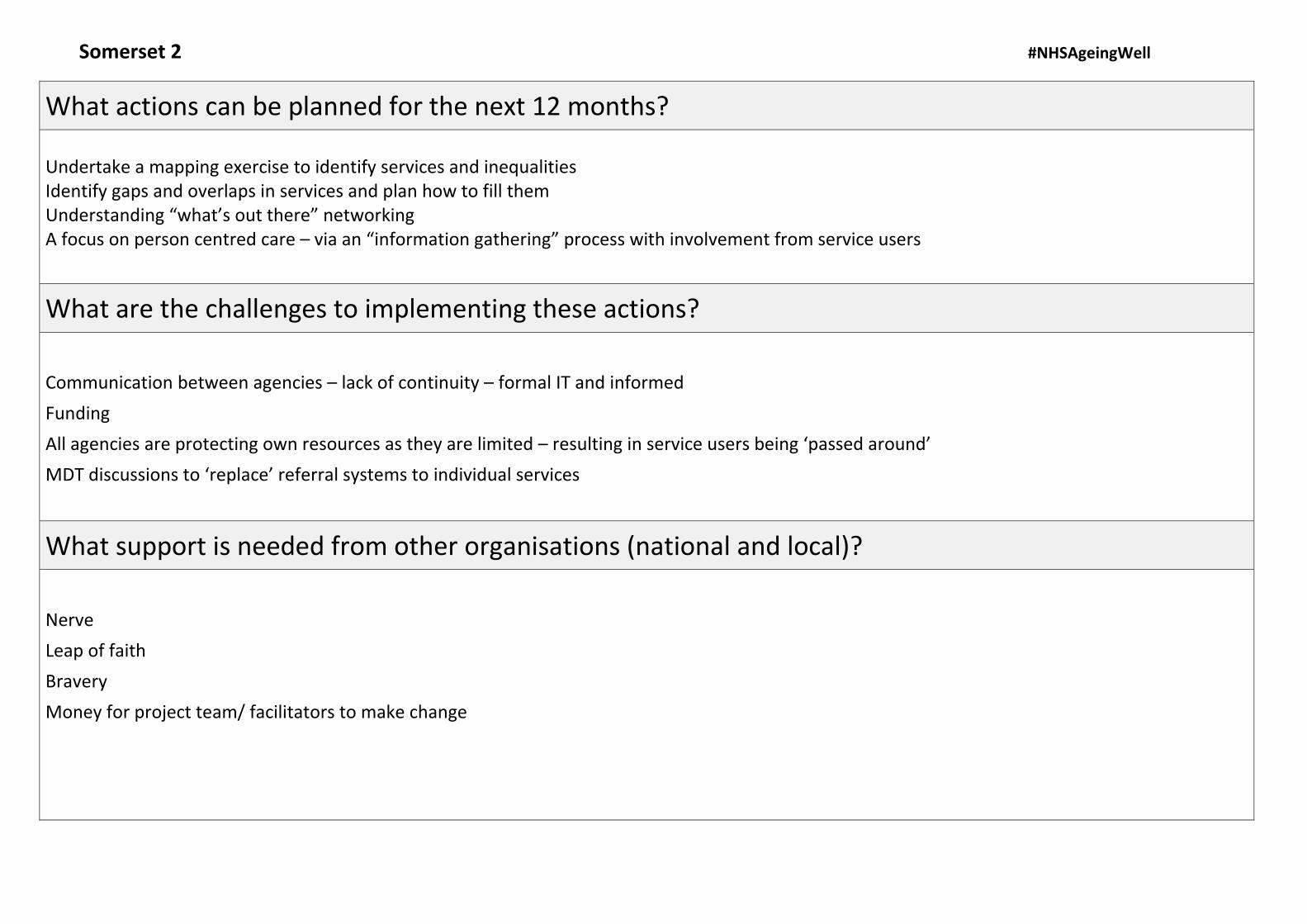
What actions can be planned for the next 12 months?
Undertake a mapping exercise to identify services and inequalities Identify gaps and overlaps in services and plan how to fill them Understanding “what’s out there” networking A focus on person centred care – via an “information gathering” process with involvement from service users
What are the challenges to implementing these actions?
Communication between agencies – lack of continuity – formal IT and informed
Funding
All agencies are protecting own resources as they are limited – resulting in service users being ‘passed around’
MDT discussions to ‘replace’ referral systems to individual services
What support is needed from other organisations (national and local)?
Nerve
Leap of faith
Bravery
Money for project team/ facilitators to make change

Somerset 2 #NHSAgeingWell
Name
Helen Hughes
Marie Spink
Lyme Carey
Sue Payne
Kay Griffin
Helen McEvansoneya
Jeremy Martin

#NHSAgeingWell
Sustainability and transformation partnership area: Somerset: CMHTs, Primary Care, IRT
Milbrook Community, Equipment Services Emma Norton, based at Magnolia House
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
CAB Better living Symphony Health coaches Stay strong, stay steady Village agents Voluntary services Fire safety checks
Community care agents Carer support (HMH)
OOH ||| services
Moderate
Referral to specialist services eg. Dieticians Home first Continence services DNs FOPAS Red gross Support at home Safe guarding IRT
RUSS POPS Consultant and urgent connect Interweave dementia specialist service (Yeovil) OPAL #NoFPathways SWAST Fire services EDRed Cross
Severe

Somerset: CMHTs, Primary Care, IRT #NHSAgeingWell
What actions can be planned for the next 12 months? Implement a frailty pathway. Strategy. Standardisation of identifiers. Introduce comprehensive assessments. Education/training – frailty – public message. ACPs. Shared e-documentation. Individualised care plan at patient’s home – for use by all – one folder.
What are the challenges to implementing these actions?
Technology – data sharing. Myth busting (TEPs, DNAR)
Central co-ordination at CGAs
Financial
Avoid duplication
What support is needed from other organisations (national and local)?
Networking. Building relationships. Understanding roles and areas of expertise.
Data. Patient participation.

#NHSAgeingWell
Name
Sarah Bevan
Katy Richards
Sandra Firth
Fiona Grant
Jenny Pickhaver
Jane Jacobi
Susie Davis
Somerset: CMHTs, Primary Care, IRT
#NHSAgeingWell
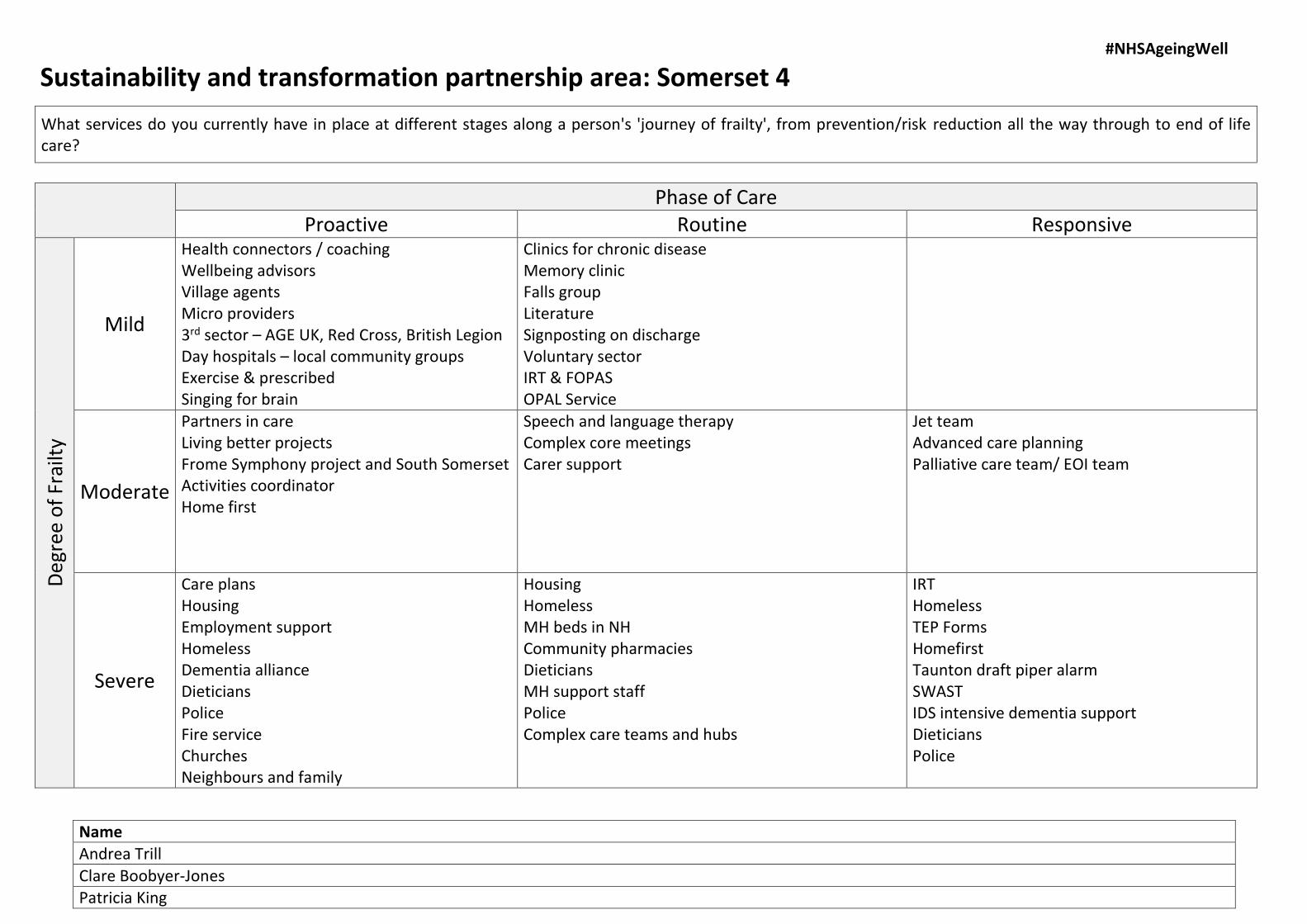
Sustainability and transformation partnership area: Somerset 4
Name
Andrea Trill
Clare Boobyer-Jones Patricia King
What services do you currently have in place at different stages along a person's 'journey of frailty', from prevention/risk reduction all the way through to end of life care?
Phase of Care Proactive Routine Responsive
Deg
ree
of
Frai
lty
Mild
Health connectors / coaching Wellbeing advisors Village agents Micro providers 3rd sector – AGE UK, Red Cross, British Legion Day hospitals – local community groups Exercise & prescribed Singing for brain
Clinics for chronic disease Memory clinic Falls group Literature Signposting on discharge Voluntary sector IRT & FOPAS OPAL Service
Moderate
Partners in care Living better projects Frome Symphony project and South Somerset Activities coordinator Home first
Speech and language therapy Complex core meetings Carer support
Jet team Advanced care planning Palliative care team/ EOI team
Severe
Care plans Housing Employment support Homeless Dementia alliance Dieticians Police Fire service Churches Neighbours and family
Housing Homeless MH beds in NH Community pharmacies Dieticians MH support staff Police Complex care teams and hubs
IRT Homeless TEP Forms Homefirst Taunton draft piper alarm SWAST IDS intensive dementia support Dieticians Police
#NHSAgeingWell
Sarah Mead
Anita Turner
Katie Hart
Shaun Charthew
Liz Harper
Beth Blackwell
Fiona Devonport
Debbie Bennett
Somerset 4
Somerset 4 #NHSAgeingWell
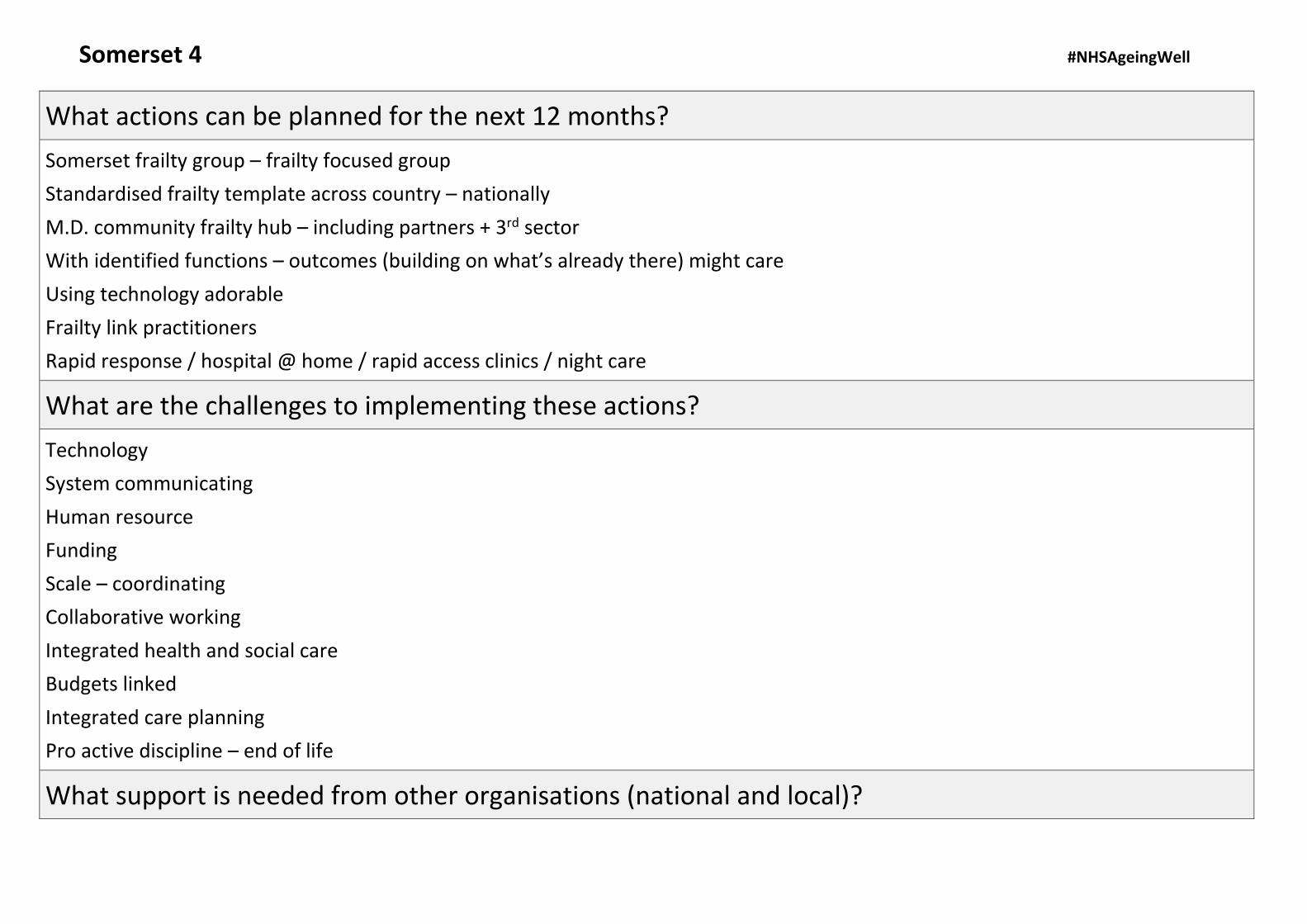
What actions can be planned for the next 12 months?
Somerset frailty group – frailty focused group
Standardised frailty template across country – nationally
M.D. community frailty hub – including partners + 3rd sector
With identified functions – outcomes (building on what’s already there) might care
Using technology adorable
Frailty link practitioners
Rapid response / hospital @ home / rapid access clinics / night care
What are the challenges to implementing these actions?
Technology
System communicating
Human resource
Funding
Scale – coordinating
Collaborative working
Integrated health and social care
Budgets linked
Integrated care planning
Pro active discipline – end of life
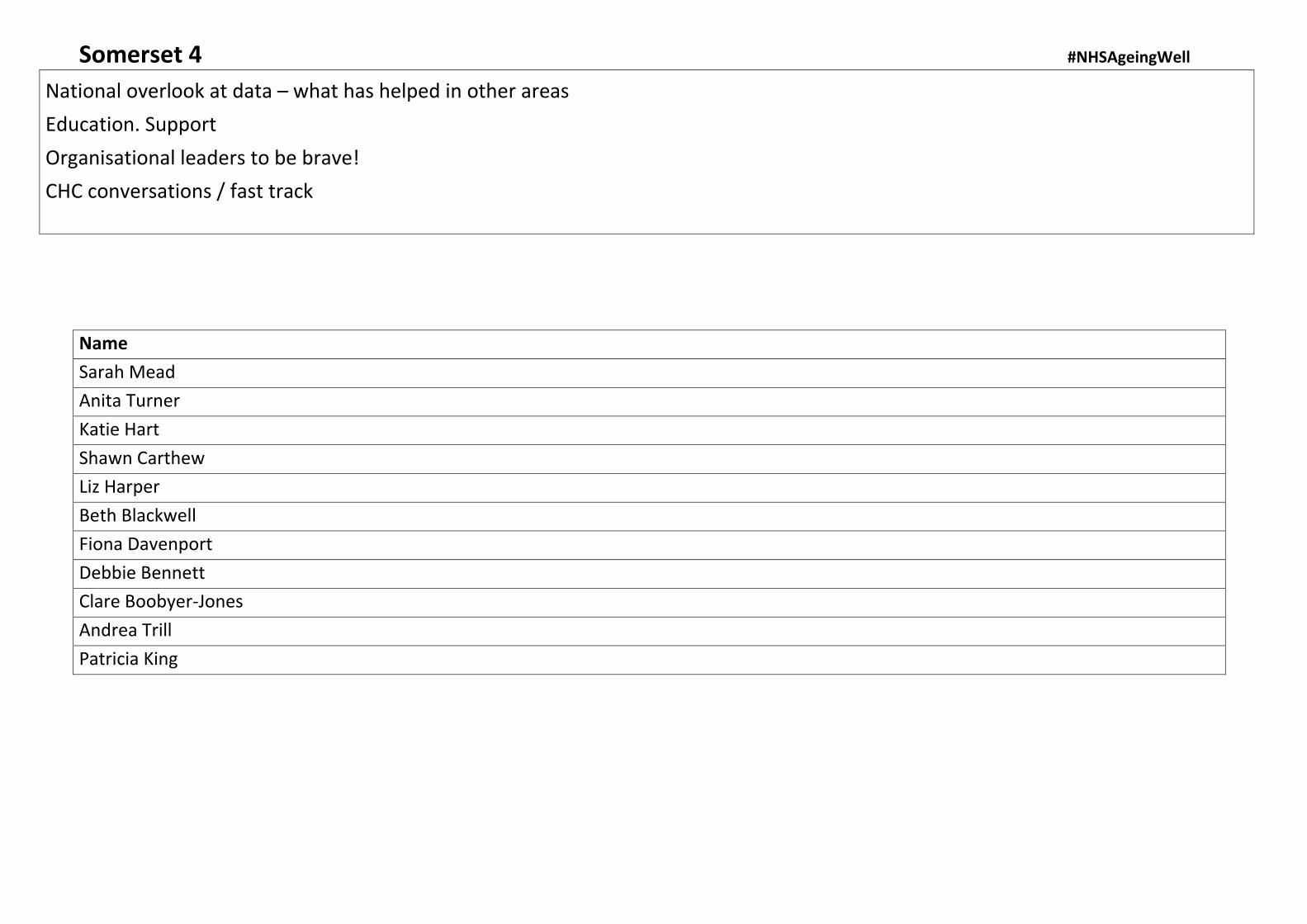
What support is needed from other organisations (national and local)?
Somerset 4 #NHSAgeingWell
Name
Sarah Mead
Anita Turner
Katie Hart
Shawn Carthew
Liz Harper
Beth Blackwell
Fiona Davenport
Debbie Bennett
Clare Boobyer-Jones
Andrea Trill
Patricia King
National overlook at data – what has helped in other areas
Education. Support
Organisational leaders to be brave!
CHC conversations / fast track