the immune landscape of colon cancer -...
TRANSCRIPT

Jérôme GALON
INSERM, Laboratory of Integrative Cancer ImmunologyCordeliers Research Center, Paris, France
LabEx
The immune landscape of colon cancer
ESMO Immuno-Oncology
Prague, Czech Republic,
October 2nd 2015

Disclosure
Co-founder and Chairman of the Scientific Council: HalioDx
Collaborative Research Agreement (grant) : MedImmune, Janssen, Perkin Elmer, IO biotech
Participation to Scientific Advisory Boards: ImmunID, MedImmune, Astra Zeneca, Definiens, Actelion,
HalioDx, Incyte
Consultant : BMS, Roche, GSK, MedImmune, Janssen, ImmunID,
Nanostring, Compugen

What is the relationship between tumor genotype andimmunophenotype ?
Lessons learned after 15 years of systems immunology in humantumors ? And how important is the immune system against cancer ?
How to explain “Hot” and “Cold” immune infiltrated tumors ?

Anti-PD1 treatment in CRC patients
Le et al. NEJM 2015

Cancer is one of the most complex biological system of all
“The whole is greater than the sum of its parts”, Aristotle
-> Systems biology in human cancer
Molecule X
Pathway Y
Cell Z

-> Tumor aggressiveness, progression, invasion and recurrence define early and late
stage cancers, and the severity of the disease
Definition of cancer
1) A tumor cell DNA disease – Cell-centric paradigm2) Due to the acquisition of secondary key behavioral characteristics following tumor genomic changes (Hanahan & Weinberg, Cell 2001)
TisT1 T2 T3 T4
T-Stage
N-Stage
M-Stage
Tumor invasion
Tumor progression
-> Tumor recurrence
Early-metastasis (venous emboli)
Tumor grade differentiationTumor aggressiveness(driver mutations, CIN, MSI, CIMP…)

Tumor progression, invasion and recurrence are dependent on immunity and theImmunoscore
Pre-existing immunity is determining the fate and survival of the patient, and thelikelihood of response to immunotherapy
Novel paradigm
TisT1 T2 T3 T4
T-Stage
N-Stage
M-Stage
Tumor invasion
Tumor progression
-> Tumor recurrence-> death
Early-metastasis (venous emboli)
Tumor grade differentiationTumor aggressiveness(driver mutations, CIN, MSI, CIMP…)
ImmunoscoreImmune contexture

Role of immune infiltrates in the promotion/control of early-metastatic invasion(VELIPI) in human cancers ? Impact on clinical outcome ?
Venous Emboli (VE)Lymphatic Invasion (LI) Perineural Invasion (PI)
Question
blood vessels (Endoglin)
Lymphatic vessels (PDPN)
-> Global analysis of tumor microenvironment in Human tumors
promotion control
? ?
BeneficialDetrimental No impact
?
immune
959 colorectal cancer patientsLymphatic emboli / Tumor

Memory T cells, in particular, TEM correlate with the absenceof early-metastatic invasion, and improved clinical outcomein colorectal carcinoma.
Pagès F, et al. N Engl J Med. 2005
Pagès F & Galon J. N Engl J Med. 2006

Quantification of immune cell densities (n=415 Patients, 6640 IHC) revealed themajor positive role of cytotoxic and memory T cells for patient’s survival
Galon J et al. Science 2006
ImmunoscoreImmune contexture
The foundation a new concept

Dis
ease
Fre
e S
urv
ival
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180
Survival (months)
I
II
III
AJCC/UICC-TNMCurrent prognosis classification
Tumor Histopathologic Findings
NSIII
III
High-CD45ROCT/IM High-CD3CT/IM
Dis
ease
Fre
e S
urv
ival
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180
Survival (months)
CD3CT/CD3IM evaluationplus
CD45ROCT/CD45ROIM evaluation
Immune cells analysis
II
III
Low-CD45ROCT/IM
Low-CD3CT/IMIV
IV
**
NS
I
Coordinated adaptive immune reaction more than tumor invasion predictsclinical outcome
->
Importance of the distribution of the adaptive immunereaction compared to tumor invasion
Galon J et al. Science 2006
Parameter
• T-stage • N-stage • Differentiation • Immune
HR
1.21.41.11.9
P value
0.250.150.840.00001
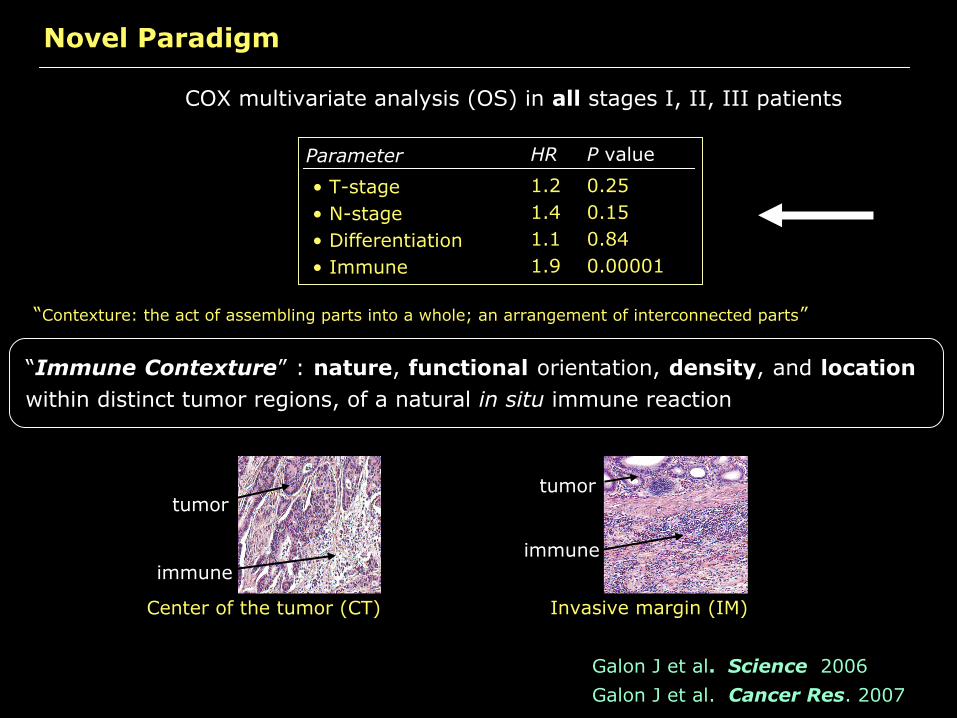
COX multivariate analysis (OS) in all stages I, II, III patients
Novel Paradigm
Galon J et al. Science 2006Galon J et al. Cancer Res. 2007
“Immune Contexture” : nature, functional orientation, density, and location within distinct tumor regions, of a natural in situ immune reaction
“Contexture: the act of assembling parts into a whole; an arrangement of interconnected parts”
Invasive margin (IM)
immune
tumor
Center of the tumor (CT)
immune
tumor

Immune ContextureParameters with major positive impact on patient’ survival
Type
Density
Functional orientation
Location • TLS (Presence and quality)
IFNGIL12TBX21IRF1STAT1
• Cytotoxic T cells (CD3, CD8)• Memory T cells (CD45RO)
TH1 cells
Associated factors
CX3CL1CXCL9CXCL10CCL5CCL2
• Center of the Tumor (CT) • Invasive Margin (IM)
CD3CT
CD3IM
CD8CT
CD8IM
CD45ROCT
CD45ROIM
1 10 100 1000 10000
Number of cells/mm2
(TH17, Treg, TH2 cells havevariable impact on survivaldepending on tumor types)
MADCAM1ICAM1VCAM1
GZMAGZMBGZMH PRFGLNY
Pages F NEJM 2005 ; Galon J. Science 2006 ; Galon J. Cancer Res. 2007 ; Camus M. Cancer Res 2009 ; Pages FJCO 2011; Mlecnik B Gastroenterology 2011; Tosolini M. Cancer Res 2011 ; Mlecnik B JCO 2011; Fridman H. Nat RevCancer 2012 ; Galon J. Immunity 2013 ; Galon J. Immunity 2013
CXCL13IL21
IL15
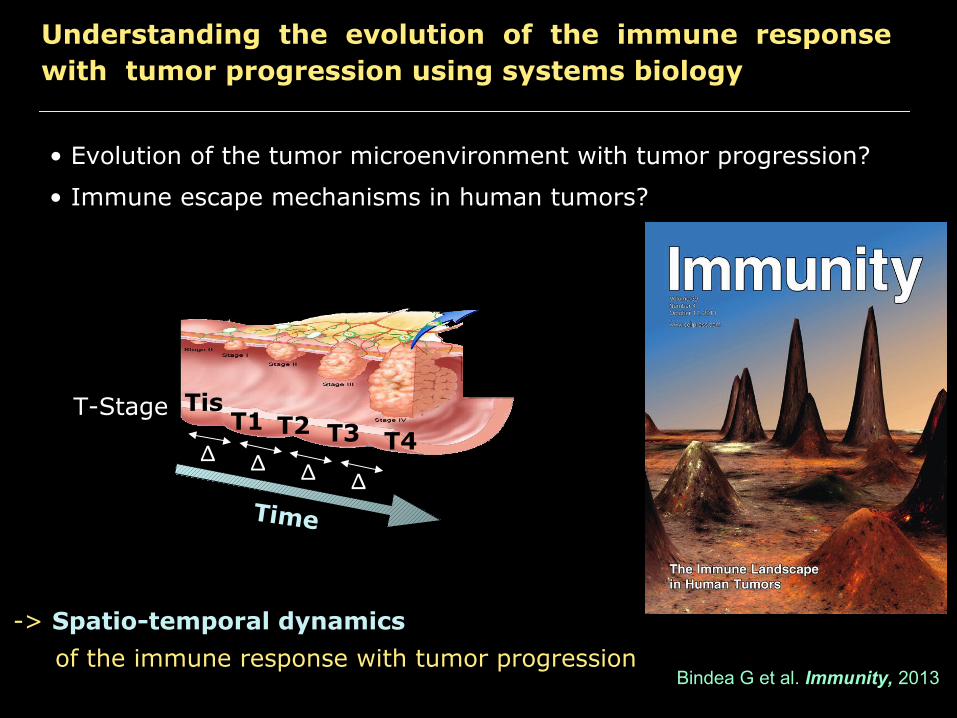
• Evolution of the tumor microenvironment with tumor progression?
Understanding the evolution of the immune responsewith tumor progression using systems biology
-> Spatio-temporal dynamics of the immune response with tumor progression
TisT1 T2 T3 T4∆ ∆ ∆ ∆
T-Stage
Time
• Immune escape mechanisms in human tumors?
Bindea G et al. Immunity, 2013

Neutrophils
Eosinophils
Basophils
Mast cells
Red cells
T-lymphocytes
PlasmaB cells
B-lymphocytes
NK cells
NKT cells
Macrophages
mDC
TH1
TH2
TH17
TH3
Treg
TEM
Tmemory
TEMRA
T-cytotoxic
iDC
Tumor cells
pDC
Lymph vessels
Blood vessels
Tumor microenvironment

“Immunome” of purified immune cell subpopulations
normalmucosa
Ad
ap
tive I
mm
un
ity
Inn
ate
Im
mu
nit
y
Exp
ress
ion
of
57
7 c
ell
typ
esp
eci
fic
gen
es
coloncancer
aDC
Cell types (n=28)
DC
CD8 T cellsTreg
B cells
Lymph vessels
T cells
Blood vessels
SW480 cancer cells
Normal mucosa
pDCiDC
Macrophages
Neutrophils
Eosinophils
Mast cells
NK CD56bright cells
NK cells
NK CD56dim cells
TgdCytotoxic cells
TFH
T helper cells
Tcm
TemTh1 cells
Th2 cells
Th17 cells
B c
ells
#1
B c
ells
#2
Tcm
Te
mT
h1
cells
#1
Th
1 ce
lls #
2T
h2
cells
#1
Th
2 ce
lls #
2T
FH
ce
lls #
1T
FH
ce
lls #
2T
FH
ce
lls #
3C
D8
T c
ells
#1
CD
8 T
ce
lls #
2C
D8
T c
ells
#3
CD
8 T
ce
lls #
4C
D8
T c
ells
#5
Tg
d #
1T
gd
#2
NK
CD
56d
im c
ells
#1
NK
CD
56d
im c
ells
#2
NK
CD
56b
righ
t ce
lls #
1N
K C
D56
bri
ght
cells
#2
iDC
#1
iDC
#2
aDC
#1
aDC
#2
aDC
#3
aDC
#4
aDC
#5
aDC
#6
aDC
#7
aDC
#8
Eo
sino
ph
ils #
1E
osi
nop
hils
#2
Ma
cro
ph
age
s #1
Ma
cro
ph
age
s #2
Ma
cro
ph
age
s #3
Ma
cro
ph
age
s #4
Ma
cro
ph
age
s #5
Ma
cro
ph
age
s #6
Ma
st c
ells
#1
Ma
st c
ells
#2
Ma
st c
ells
#3
Ma
st c
ells
#4
Neu
tro
ph
ils #
1N
eutr
op
hils
#2
Neu
tro
ph
ils #
3S
W4
80 c
anc
er
cells
#1
SW
480
ca
nce
r ce
lls #
2S
W4
80 c
anc
er
cells
#3
Nor
ma
l muc
osa
#1
Nor
ma
l muc
osa
#2
Nor
ma
l muc
osa
#3
Nor
ma
l muc
osa
#4
Nor
ma
l muc
osa
#5
Nor
ma
l muc
osa
#6
Nor
ma
l muc
osa
#7
Nor
ma
l muc
osa
#8
Nor
ma
l muc
osa
#9
Nor
ma
l muc
osa
#1
0N
orm
al m
uco
sa #
11
Nor
ma
l muc
osa
#1
2N
orm
al m
uco
sa #
13
Nor
ma
l muc
osa
#1
4N
orm
al m
uco
sa #
15
Nor
ma
l muc
osa
#1
6N
orm
al m
uco
sa #
17
Nor
ma
l muc
osa
#1
8N
orm
al m
uco
sa #
19
Nor
ma
l muc
osa
#2
0N
orm
al m
uco
sa #
21
Nor
ma
l muc
osa
#2
2Purified immune cell subpopulations : “Immunome”
Bindea G et al. Immunity 2013

Intratumor “immunome” clustering within CRC
Cluster 1 Cluster 2NC
Exp
ress
ion
of 3
72 s
igni
fican
t gen
es
with
in C
RC
tum
ors
Cluster 1 (n=60)
Cluster 2 (n=45)
Survival (Months)

Intratumor “immunome” clustering within CRC
T cellsCytotoxicityTh1
B cellsMHC Cl II
TFH cells
MHC Cl IInflammation
Group 1 Group 2P-value
CD3E <0.00001CD3G <0.0001CD4 <0.00001CD8A <0.00001GNLY <0.01GZMA <0.0001GZMB <0.01GZMH <0.0001GZMK <0.00001IFNG 0.01TBX21 <0.00001
CD19 <0.00001CD40 <0.001CD86 <0.00001HLA-DMA <0.00001HLA-DMB <0.00001HLA-DOA <0.00001HLA-DOB <0.00001HLA-DPA1 <0.00001HLA-DQA2 0.03HLA-DRA <0.00001LTA <0.00001
CXCR5 <0.0001CXCL13 <0.0001
HLA-B 0.94HLA-C 0.34IFNA1 0.23IFNA2 0.48IL1A 0.72IL1B 0.81IL8 0.84IL8RA 0.50
-> “Immunome” analysis from CRC tumors reveals functional association of Tcells, cytotoxicity, B cells, MHC Cl II molecules, and TFH cells
Bindea G et al. Immunity 2013

CD1A ENGGranulocyteIL3RA PDPN /csCD20 /cs CD68 /Tum
CD45RO FoxP3 TryptaseCD3 / Tum CD57 /cs CXCR5CD8 /Tum
Intratumor innate cells, adaptive cells, and vessels
IHC enzymatic stainings: -> Quantification (cells/mm2)Cohort 1 (n=120 patients), cohort 2 (n=415 patients)
Bindea G et al. Immunity 2013

Intratumor B cells, T cells and TFH cells
CD20
CD3 CXCR5
Bindea G et al. Immunity 2013

CD3
FoxP3
CD20
CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD3
FoxP3
CD20
CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD8
CD8
Invasive margin (IM)Center of the tumor (CT)
Cell density
x-y-Force Directed Topology
Cell density(cells/mm2)
tumor progression
Understanding the evolution of the immune responsewith tumor progression : The immune landscape
Bindea G et al. Immunity 2013
TFH
B-cells

CD3
FoxP3
CD20
CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD3
FoxP3
CD20
CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD8
CD8
Invasive margin (IM)
Center of the tumour (CT)
Cell density
x-y-Force Directed Topology
CD3
FoxP3
CD20CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD3
FoxP3
CD20
CD8extra
CD8intra
CD68intra
CD68
CD45RO
PDPN
CD57
CXCR5
Granulocyte
IL17
ENG
Tryptase
IL3RA
CD1A
CD8
CD8
Invasive margin (IM)Center of the tumor (CT)
Impact on DFS
x-y-Force Directed Topology
Hazard ratiotumor recurrence
Understanding the evolution of the immune responsewith tumor progression : The immune landscape
GoodBad
Bindea G et al. Immunity 2013
TFH
B-cells
TH17

TH1
Tumor
TFH
CXCL13
Tmemory
T-cytotoxic
B cells
IL21
TLS
Immune contexture associated with prolonged survival
TLSInvasivemargin
Tumor
Tumor
Tumorstroma
Bindea G et al. Immunity 2013

• Mutation, immunogenicity and immune microenvironment?
Relationship between molecular phenotypes andimmunophenotypes of CRC tumors using systems biology
-> Rationale for an immune classification of tumors
• Immune escape mechanisms in human tumors?
Angelova M et al. Genome Biol, 2015
Mutations Immune

Spin chart from (n=460 patients)
Molecular phenotypes and immunophenotypes of CRC tumors
Molecular phenotype
Angelova M et al. Genome Biol. 2015
Immunome of CRC tumors

Molecular phenotype
Spin chart from (n=460 patients)
Molecular phenotypes and immunophenotypes of CRC tumors
Angelova M et al. Genome Biol. 2015

Spin chart from (n=460 patients)
Molecular phenotypes and immunophenotypes of CRC tumors
Innate immunity
Adaptive immunity
Enrichment of immune subpopulations : TILs in 97% of tumors, and T-cells in 69% of tumors
metagenes expression profiles

Enriched and depleted immune subpopulations in hypermutated(MSI-H and MSS^)
Volcano plots for enriched (blue) and depleted (yellow) TIL subpopulations in the distinctpatient groups compared to normal samples (n=50).
MSI-H MSS^
Tregs and MDSCs are depleted
EnrichedDepleted
Act CD4Act CD8Tem CD4Tem CD8Tregs MDSCs
MSI-HMSS^
Angelova M et al. Genome Biol. 2015

Patient 1 (weak) Patient 2 (moderate) Patient 3 (strong)
How to explain “Hot” and “Cold” immune infiltrated tumors ?
CD3Tumor
Median OS (death)
< 2 years 4.9 years > 15 years
Im0 Im2 Im4ImmunoscoreCD3/CD8Center/Margin

Mechanisms associated with T cells infiltration
Attraction Adhesion
MADCAM1VCAM1ICAM1
T cells
TH1Cytotoxic
MemoryT cells
CXCL9CXCL10
CCL2CCL5
CX3CL1 CXCL13
TFHB cells
Mlecnik et al. Gastroenterology 2010
Bindea et al. Immunity 2013

IL15 and intratumoral immune reaction
In situ densities of proliferating B and T cells
CD20+ CD3+ Ki67+
-> Quantification in tumor core (CT), invasive margin (IM), and lymphoid ilets (LI)

Mechanisms associated with T cells infiltration
Attraction Adhesion
MADCAM1VCAM1ICAM1
T cells
TH1Cytotoxic
MemoryT cells
CXCL9CXCL10
CCL2CCL5
CX3CL1 CXCL13
TFHB cells
Mlecnik et al. Gastroenterology 2010
Local lymphocyteproliferation
IL15
Mlecnik et al. Science Transl Med 2014
Bindea et al. Immunity 2013

Implications for cancer classification and therapies
To the Immunoscore
From the Immune contexture
(A simple and powerfull Immune Test)
(Complexity of intratumor immune reaction)

T-STAGE N-STAGE M-STAGETumor cell extension and invasion
CD3+ T cells CD8+ T cells Density Locaton (CT, IM)ImmunoscoreHost immune response
Mucinous CCS1
CCS2Medullary
Adeno. NOS
Serrated
Signet ring cell
Enterocyte
Goblet-like
Transit-amplifying-S
Infammatory
Stem-like
CIN
MSI
CIMP CCS3Transit-amplifying-R
BRAF
APC
KRAS
TP53
Morphology Cell of origin Molecular pathway Mutaton status Gene expression
Tumor cell characteristcs
Ways to classify
CTNNB1
Micropapillary
Cribriform comedo-type
Galon et al. J Pathol. 2014
Colorectal cancer classifications

Prolonged survival in patients with high Immunoscore (Im) based on the evaluation of CD45RO-CT/IM and CD8-CT/IM
Mlecnik et al. J Clin Oncol 2011
Survival (months)
P<0.0001
Dis
ease
-Fre
e Sur
viva
l (%
)
0
20
40
60
80
100
0 20 40 60 80 100 120 140 160 180
Im4
Im2
Im1Im0
Im3
AJCC/UICC-Stage I-III
Dis
ease
-Fre
e Sur
viva
l (%
)
Im4
Im2
Im1Im0
Im3
0
20
40
60
80
100
0 20 40 60 80 100 120 140 160 180
Survival (months)
P<0.0001
AJCC/ UICC-Stage I-IV

Multivariate proportional hazard COX analysis among all patients with AJCC/UICC-TNM Stage I/II/III colorectal cancer
Tumor (T) stageN StageGenderNumber of total lymph nodesHistological gradeMucinous ColloideOcclusionPerforationImmunoscore
Log Rank P-values
1.241.311.471.130.691.291.034.030.65
0.290.170.180.680.290.470.940.00840.0003
HRCOX analysis for DFS
According to clinical parameters and immune parameters
DFS OS DSS
1.38
0.64
0.09 ns
<0.0001
1.18
0.71
0.29 ns
<0.0001
1.43
0.63
0.10 ns
<0.0001
HR P-value HR P-value HR P-value
AJCC/UICC-TNM
Immunoscore
COX analysis
According to AJCC/UICC-TNM classification and immune score
-> Validation in 2 independent cohorts of colorectal cancer patientsMlecnik et al. J Clin Oncol 2011

Metastasis analysis
Colorectal cancer
Liver Metastasis Lung Metastasis
One primary tumor
Multiple metastatic sites
Immunoscore within multple metastases at diferent sites Death at years: Low Immunoscore: 76% vs High Immunoscore: 15%

THE IMMUNOSCOREAS A NEW POSSIBLE APPROACH IN THECLASSIFICATION OFCANCER
Naples, Italy, Feb 2012Principal investigator: J. Galon
Galon J et al. J. Transl. Med. 2012Galon J et al. J. Pathol. 2014

The IMMUNOSCORE
FaisabilityIHC automate High-resolution scanner
whole slide quantification
Digital pathology
Immunoscore
-> Standardized Operating Procedure-> Today’s tools for modern pathologists
Galon J et al. J. Transl. Med. 2012Galon J et al. J. Pathol. 2014

Immunoscore (I) using whole slide FFPE
Routine whole slide stainings & precise image quantification
CT
IM
Tissue
Immunostaining Definition of Tumor Regions
Density plots
I
CD3

World Immunotherapy Council inaugural meeting (Feb 2012)
Support (moral) from the World Immunotherapy Council (WIC), and supportfrom societies including, EATI, BDA, CCIC, CIC, CRI, CIMT, CSCO, TIBT,DTIWP, ESCII, NIBIT, JACI, NCV-network, PIVAC, ATTACK, TVACT…
Worldwide Immunoscore consortium (PI: J Galon)
The Immunoscore as a New Possible Approach for theClassification of Cancer
Assay harmonization
Immunoscore meetings :-Feb 2012, Italy-Dec 2012, Italy-Nov 2013, SITC, USA-Dec 2013, Italy-Jan 2014, Qatar-Jul 2014, Paris, France-Nov 2014, SITC, USA-Nov 2015, SITC, USA-Dec 2015, Italy
Switzerland
Australia
Netherland
Spain
Qatar
Canada
Japan
China
Immunoscore
Italy
Austria
Germany
Sweden
FranceUSA
UKCzech R
India
Switzerland
(23 Centers, 17 countries: >3000 patients)

PI: J Galon SITC, EATI23 Centers, 17 countries
National Prospective Immunoscore Consortium
Worldwide Immunoscore Consortium
European Immunoscore Consortium
PI: J Galon ERAnet H20205 European countries
PI: F PagèsPHRC, INCa6 hospitals
Switzerland
Australia
Netherland
Spain
Qatar
Canada
Japan China
Immunoscore
Italy
Austria
Germany
Sweden
France
USA
UKCzech
India
Ongoing international consortia on Immunoscore
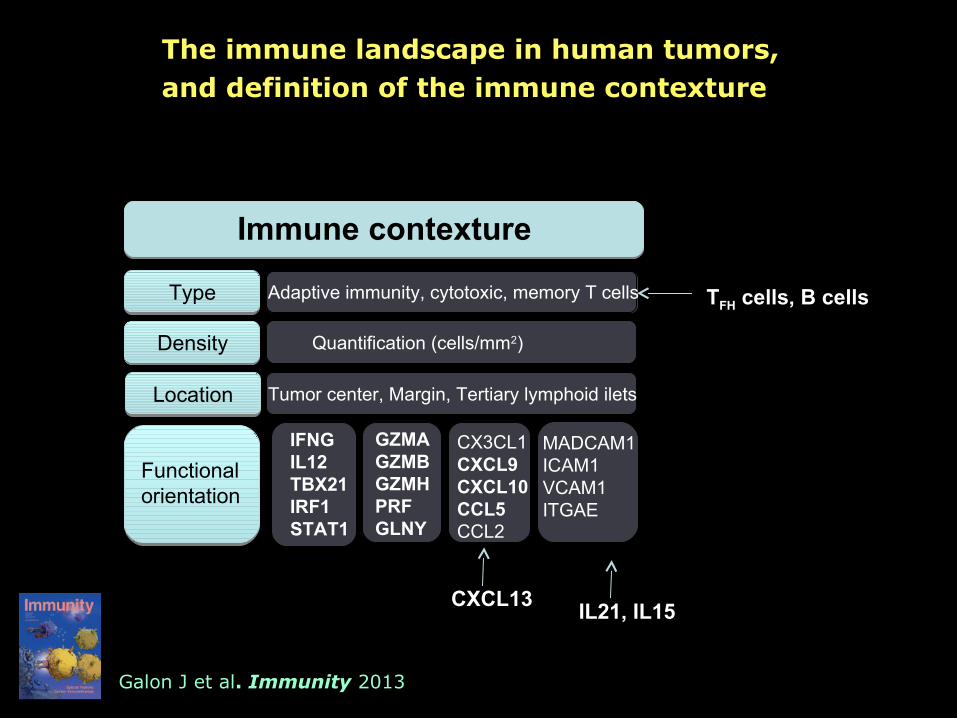
Functional orientation
IFNGIL12TBX21IRF1STAT1
MADCAM1ICAM1VCAM1ITGAE
Quantification (cells/mm2)
Adaptive immunity, cytotoxic, memory T cells
Tumor center, Margin, Tertiary lymphoid ilets
Immune contexture
CX3CL1CXCL9CXCL10CCL5CCL2
GZMAGZMBGZMH PRFGLNY
Type
Density
Location
The immune landscape in human tumors, and definition of the immune contexture
CXCL13
Galon J et al. Immunity 2013
TFH cells, B cells
IL21, IL15

Functional orientation
IFNGIL12TBX21IRF1STAT1
MADCAM1ICAM1VCAM1ITGAE
Quantification (cells/mm2)
Adaptive immunity, cytotoxic, memory T cells
Tumor center, Margin, Tertiary lymphoid ilets
Immune contexture
Immunologic Constant
of Rejection (other diseases)
CX3CL1CXCL9CXCL10CCL5CCL2
GZMAGZMBGZMH PRFGLNY
Cancer
Type
Density
Location
Immunoscore
The overlap between the immune contexture, theimmunologic constant of rejection and the Immunoscore
CXCL13
Galon J et al. Immunity 2013
IL21, IL15

Stratification of cancer based on the immune status
MSI-H MSS^ MSS/CIMP.hi MSS MSS-CIMP.lo
Tumor classification
Immune classification
IMMUNE
-> Importance of having standardized immune Assays

Towards the future
1) Prognostic: ImmunoscoreTM - “I”
Immune Contexture • Nature • Functional orientation • Density• Location
• Cytotoxic & Memory T cells• Prognostic value: “I” > TNM • Tumor invasion parameters (T, N, …) are statistically dependent on “I”
-> Novel cancer classification
2) Predictive markers• Current clinical trials
3) Patient stratification Based on immune contexture defect
4) Novel immunotherapies Adapted to patient’s immune defect
Galon J et al. Immunity 2013


Franck Pagès Angela VasaturoTessa Fredriksen Helen AngellStéphanie Mauger Mihaela Angelova Florence Marliot Sarah ChurchLucie Lafontaine Pauline MabyAmélie Bilocq Marc Van den EyndeAmos Kirilovsky Bernhard MlecnikMarie Tosolini Gabriela Bindea
Anne Berger
Anna ObenaufMichael Speicher
Tchao MeatchiChristine LagorcePatrick Bruneval
Galon lab. INSERM, CRC, Paris, France
Dpt. of General and Digestive Surgery,HEGP, Paris, France
Institute for Genetics, Graz, Austria
Dpt. of Pathology, HEGP, Paris, France
Philippe Wind
Dpt. Digestive Surgery and Pathology, Avicenne, Bobigny, France
Team 13, Cordeliers Research Center, France
Hervé Fridman
Martin Asslaber
Dpt. Pathology, Graz hospital, Graz, Austria
Dpts. of Pathology from the 23 CentersWorldwide
SITC, EATI and all supportive societiesDefiniens, PathForce, MedImmune
Pornpimol CharaoetongZlatko Trajanoski
Institute for Bioinformatics, Innsbruck, Austria
University Clinic, Erlangen, Germany
Christopher BeckerMaximilian Waldner
Jean Baptiste Latouche
Rouen University, France
Anna BerghoffMatthias Preusser
Clinical Division of Oncology, Medical Universityof Vienna, Austria
Team 10, Cordeliers Research Center, France
Gauthier StollGuido Kroemer

Jérôme GALON
INSERM, Laboratory of Integrative Cancer ImmunologyCordeliers Research Center, Paris, France
LabEx
The immune landscape of colon cancer
ESMO Immuno-Oncology
Prague, Czech Republic,
October 2nd 2015