the pharmacokinetic effects of coadministration of morphine and trovafloxacin in healthy subjects
TRANSCRIPT

The Pharmacokinetic Effects ofCoadministration of Morphine andTrovafloxacin in Healthy Subjects
John Vincent, MD, PhD, Thomas Hunt, MD, PhD,* Renli Teng, PhD,† Lisa Robarge,Susan A. Willavize, PhD, Hylar L. Friedman, MD, Groton, Connecticut
BACKGROUND: Morphine and antibiotics are fre-quently coadministered in the surgical setting.These agents may interact, reducing the efficacyof the antibiotic or increasing the toxicity of mor-phine. It is therefore important to determinewhether antibiotics that might be used for surgi-cal prophylaxis have the potential to change thepharmacokinetics of morphine. It is equally im-portant to learn whether morphine affects theplasma levels of antibiotics and thus may poten-tially influence their efficacy or tolerability.
METHODS: This open, randomized, placebo-con-trolled, three-treatment, three-period cross-overstudy enrolled 19 healthy volunteers. Oral trova-floxacin (200 mg), a novel fluoroquinolone antibi-otic, and intravenous morphine (0.15 mg/kg)were coadministered, and the effects on thepharmacokinetics of each drug and on changesin the pharmacologic action of morphine, esti-mated from its effects on respiratory rate andlevel of sedation, were examined.
RESULTS: When trovafloxacin was coadministeredwith morphine, the half-life of trovafloxacin wasunchanged; however, the ratio of the area underthe serum concentration versus time curve(AUC0–`) estimates for trovafloxacin/morphineversus trovafloxacin/placebo was 63.8% (95%confidence interval [CI], 40.7% to 100.3%), indi-cating a 36% reduction in the bioavailability oftrovafloxacin. The ratio of the mean maximumserum concentration (Cmax) estimates of trova-floxacin for the two treatments was 53.8% (95%CI: 36.1% to 80.1%), indicating a 46% reductionin Cmax. The time to Cmax was delayed by4 hours. With trovafloxacin coadministration,there were no statistically significant changes ineither the mean relative bioavailability of mor-phine or that of its metabolite, 6b-glucuronide-morphine. Coadministration of trovafloxacin didnot exacerbate the reduction in respiratory rateor increase the number of side effects associ-ated with morphine administration.
CONCLUSIONS: Coadministration of trovafloxacinand morphine reduces the bioavailability andmaximum serum concentrations of trovafloxacin.However, elimination of oral trovafloxacin is notimpaired, suggesting that the efficacy of trova-floxacin could be maintained in many patientswho receive concomitant morphine. Morphineplasma levels and pharmacologic effects are notsignificantly altered by coadministration of trova-floxacin. Despite their similar metabolic path-ways, the trovafloxacin/morphine combinationneither exacerbates the respiratory depressanteffects of morphine nor increases the frequencyof side effects when compared with placebo/morphine treatment. These results suggest thatthe efficacy of trovafloxacin may be maintainedwhen coadministered with morphine. Concurrentadministration of trovafloxacin and morphine isunlikely to alter the pharmacologic effects ofmorphine. Am J Surg. 1998;176(Suppl 6A):32S–38S. © 1998 by Excerpta Medica, Inc.
The early quinolone antibiotics, such as nalidixicacid, had limited clinical utility because of a narrowspectrum of activity, low potency, high frequency of
spontaneous bacterial resistance, poor bioavailability, andshort half-lives.1 The widely used fluoroquinolone antimi-crobials, including ciprofloxacin and norfloxacin, haveovercome many of these shortcomings2 but have their ownclinically significant limitations, including only modestefficacy against anaerobes and gram-positive bacteria, par-ticularly methicillin-resistant Staphylococcus aureus andpenicillin-resistant Streptococcus pneumoniae.3,4
Trovafloxacin, a novel fourth-generation synthetic tri-fluorinated quinolone antibiotic, is structurally differentfrom other fluoroquinolones. Trovafloxacin contains a C-7ring moiety, 7-(3-azabicyclo[3.1.0]-hex-3-yl), on a basicnaphthyridone configuration (Figure 1).5
Trovafloxacin broadens the spectrum of activity of thefluoroquinolones. Although, as a class, quinolones displayexcellent activity against most gram-negative bacteria,these agents have only modest activity against gram-posi-tive bacteria.6 In contrast, trovafloxacin has in vitro activ-ity against both gram-negative and gram-positive bacteriaas well as against atypical pathogens.7–9 Trovafloxacin hasbeen shown to be more effective than ciprofloxacin andofloxacin against acute infections in animal models in-volving gram-positive bacteria, such as Streptococcuspneumoniae, while maintaining activity similar to that ofciprofloxacin against gram-negative organisms.8 Trova-floxacin has also been shown to be more active than
From the Department of Clinical Research, Pfizer Central Re-search, Groton, Connecticut.
* Current affiliation: PPD Pharmaco, Austin, Texas.† Current affiliation: Astra Merck, Wayne, Pennsylvania.Requests for reprints should be addressed to John Vincent,
MD, PhD, Department of Clinical Research, Pfizer Central Re-search, Eastern Point Road, Groton, Connecticut 06340.
32S © 1998 by Excerpta Medica, Inc. 0002-9610/98/$19.00All rights reserved. PII S0002-9610(98)00218-9

ciprofloxacin or ofloxacin against Bacteroides species, suchas B. fragilis, the most important anaerobic organism asso-ciated with intra-abdominal abscesses.10,11
The pharmacokinetic characteristics of single and multi-ple doses of trovafloxacin are unique among fluoroquino-lone antibiotics.12,13 In studies with fasting healthy volun-teers, oral trovafloxacin at doses of 100, 200, or 300 mg wasrapidly absorbed, reaching maximum serum concentrations(Cmax) 1 to 2 hours after administration.13,14 The meanhalf-life and area under the serum concentration versustime curve (AUC) of trovafloxacin after a single, 200-mgdose were 11.3 hours and 30.4 mg z hour/L, respectively,14
or approximately twofold longer and threefold greater thanthose observed for ciprofloxacin after a single, 500-mgdose.12,15 After multiple dosing, the renal clearance (0.43L/hour), half-life, and unbound fraction (23.8%) of trova-floxacin did not change.13 The half-life of trovafloxacin islong relative to other fluoroquinolones, permitting once-daily administration.13
A daily oral dose of 200 mg trovafloxacin is well toleratedand, unlike other quinolones such as ofloxacin, its phar-macokinetics are not altered by a patient’s age, gender, orrenal status.16 Moreover, unlike enoxacin and ciprofloxa-cin,1 the coadministration of trovafloxacin with methyl-xanthines, such as theophylline, is not associated withclinically significant drug–drug interactions.17
Prophylactic antibiotics and agents used to control post-operative pain are often administered concomitantly topatients undergoing surgery.18 Morphine and relatedagents have relatively narrow therapeutic indexes, anddrug interactions that alter their plasma levels may com-promise their efficacy or intensify adverse events.18 It istherefore important to determine whether antibiotics usedfor surgical prophylaxis have the potential to change thepharmacokinetics of analgesics. It is equally important todetermine whether commonly used analgesics change an-tibiotic plasma levels potentially affecting the antibiotic’sefficacy and toxicity.
With its broad spectrum of antimicrobial activity and apharmacokinetically equivalent intravenous formulation,19
trovafloxacin is a logical candidate for prophylaxis in pa-tients undergoing surgical procedures. However, morphineand trovafloxacin are both eliminated by glucuronidation.When coadministered, trovafloxacin could potentiallymodify the toxicity and sedation profile of morphine, in-
creasing the risk of esophageal reflux, excessive sedation,and respiratory depression.
In this study, the pharmacokinetics of coadministeredtrovafloxacin and morphine were evaluated and the effectof trovafloxacin on the pharmacologic actions of morphinewere examined by measuring the respiratory rate and seda-tion induced by the opiate.
METHODSSubjects
Normal, healthy subjects of either sex between the ages of18 and 45 years were eligible for participation providedbody weight and laboratory parameters were within 10% ofnormal and urine drug screen and ethanol breath tests werenegative. Written informed consent was obtained from allparticipants, and the study was approved by the local ethicscommittee.
Subjects were included if they had taken no prescriptiondrugs (except oral contraceptives), over-the-counter drugs,or recreational drugs for at least 2 weeks before studyparticipation, and no investigational drugs within 4 weeksof the study. Women were included if they were notbreastfeeding and were either surgically sterilized, at least 2years postmenopausal, or using appropriate contraceptivemethods.
Subjects with any condition affecting drug absorption,those requiring concomitant drug therapy (except oralcontraceptives), and those with evidence or history ofclinically significant allergic, hematologic, renal, endo-crine, pulmonary, gastrointestinal, cardiovascular, hepatic,psychiatric, or neurologic diseases, including all forms ofepilepsy, were excluded. Subjects with supine diastolic/systolic blood pressures .140/90 mm Hg or ,90/60 mmHg or heart rate .100 beats/min or ,50 beats/min on thescreening electrocardiogram were also excluded.
Study DesignThe study was an open, randomized, placebo-controlled,
three-treatment, three-period, cross-over design. Subjectsreceived the following regimens on days 1, 8, and 15according to one of six treatment sequences: normal saline(placebo) administered intravenously over 10 minutes fol-lowed by 200 mg oral trovafloxacin (2 3 100 mg), 0.15mg/kg intravenous morphine administered over a 10-minute period followed by 200 mg oral trovafloxacin, and0.15 mg/kg intravenous morphine administered over a 10-minute period followed by oral placebo (two tablets). Oneach treatment day, subjects fasted for at least 8 hours priorto the morning dosing and for 4 hours thereafter. Subjectswere confined to the clinical research facility for at least12 hours before and released no earlier than 24 hours afteradministration of study drug. They returned for blood sam-pling at 36 and 48 hours after dosing.
Pharmacokinetic SamplesBlood samples were collected from each subject before
administration of the study drug, immediately after intra-venous drug administration, and at 0.08, 0.25, 0.5, 0.75, 1,1.5, 2, 3, 4, 6, 8, 12, 18, 24, 36, and 48 hours after dosingon days 1, 8, and 15. Samples sufficient to yield 2.5 mL ofserum for determination of trovafloxacin concentration
Figure 1. The chemical structure of trovafloxacin.
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998 33S

were collected in evacuated tubes free of anticoagulants,phase separators, or preservatives and allowed to clot for 45minutes. Blood samples sufficient to yield 2 mL of plasmafor determination of morphine concentration were col-lected in heparinized tubes. Serum and plasma were sepa-rated from whole blood by refrigerated centrifugation,transferred into labeled plastic vials, and frozen immedi-ately at 220°C.
Pharmacokinetic AnalysisSerum concentrations of trovafloxacin and plasma con-
centrations of morphine and its metabolite, 6b-glucuro-nide-morphine, were determined by high performanceliquid chromatography methods using ultraviolet and elec-trochemical detection, respectively. The following param-eters were determined for trovafloxacin, morphine, and6b-glucuronide-morphine: Cmax, time to maximum serumconcentration (Tmax), terminal phase rate constant (Kel),serum half-life (t1/2), and area under the concentration-time curve from zero to infinity (AUC0–`) and from zero tothe last sampling time (AUC0–t). Kel was estimated usingleast squares regression analysis of the serum concentra-tion-time curve obtained over the terminal log-linearphase. Individual terminal phase t1/2 was calculated as0.693/Kel. The AUC0–t was calculated by the linear trap-ezoidal rule, and the AUCt–` was calculated as Cest(t)/Kel,where Cest(t) is the estimated serum concentration at timet based on the regression analysis described above.AUC0–` was estimated as the sum of AUC0–t andAUCt–`. Cmax and Tmax were derived directly from theexperimental data.
Pharmacodynamic AssessmentsResting respiratory rate was measured over 60 seconds
with subjects supine in a quiet room, prior to blood drawingand drug administration, and 1, 2, 3, 4, 6, 8, 10, and12 hours after dosing on days 1, 8, and 15. Two measure-ments were made at each time point and averaged.
Safety AnalysisStudy drug-induced sedation was evaluated by having
subjects place a mark on an ungraded 100-mm line markedwith ‘‘wide awake’’ on the left and ‘‘almost asleep’’ on theright. These Visual Analog Scale (VAS) estimates wereobtained at times corresponding to when blood had beendrawn. Subjects were not permitted to review their previ-ous sedation estimates when subsequent estimates wereobtained.
All observed or volunteered adverse events were recordedin terms of severity, duration, and possible relationship tostudy drug. Serious adverse events occurring at any timefrom the start of the study through 30 days after the studywere also recorded.
Laboratory tests (hematology, urinalysis, clinical chemis-try) and an electrocardiogram were obtained at baseline.Blood pressure and pulse were monitored on study days 1,8, and 15.
Statistical AnalysisAnalysis of variance (ANOVA) was performed on the
natural log-transformed AUC0–`, Cmax, and untrans-
formed Tmax and Kel. Both respiratory rate and sedation(VAS) were analyzed with a mixed effects model repeatedmeasures analysis with baseline included as a covariate.Overall treatment effects were summarized by their means,standard errors, differences between treatments, and 95%confidence intervals (CI). Statistical significance was de-fined as P #0.05.
RESULTSDemographics
A total of 19 healthy subjects, nine men and 10 women,participated in the study. Subjects ranged in age from 18 to41 years, with a mean age of 29.3 (30.3 in men, 28.7 inwomen). Seventeen of the subjects were white and twowere Hispanic. Their weight ranged from 65.9 to 87.7 kg inmen (mean 76.0 kg) and from 53.9 to 84.1 kg in women(mean 66.2 kg).
Subject DispositionA total of 18 subjects completed the study. One female
subject discontinued the study after the initial dose oftrovafloxacin with morphine. This subject was not in-cluded in the pharmacokinetic or pharmacodynamic anal-ysis but was included in the safety analysis.
PharmacokineticsFigures 2 and 3 illustrate the mean serum concentration
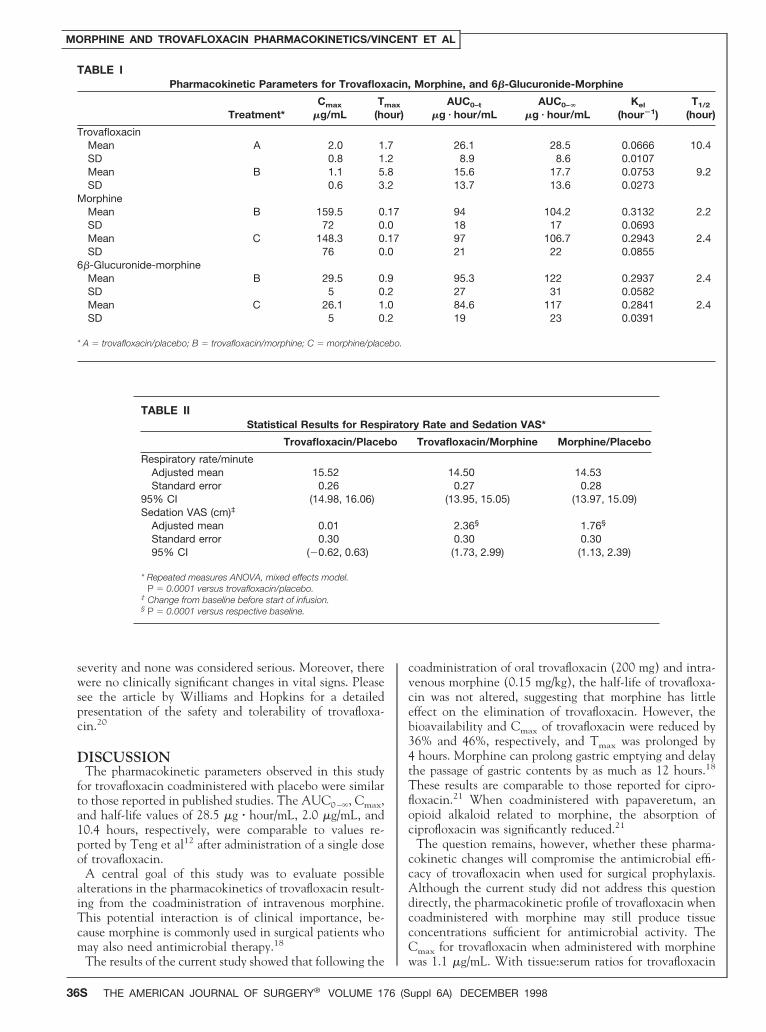
profiles of trovafloxacin and morphine when taken indi-vidually with placebo or together. Mean trovafloxacinAUC0–` and Cmax estimates following trovafloxacin/mor-phine treatment were 18.2 mg z hour/mL and 1.1 mg/mL,respectively, compared with values of 28.5 mg z hour/mLand 2.0 mg/mL following trovafloxacin/placebo treatment(Table I). The ratio of the mean trovafloxacin AUC0–`
estimates for trovafloxacin/morphine versus trovafloxacin/placebo was 63.8% (95% CI: 40.7%, 100.3%), indicating a36% reduction in bioavailability. The ratio of the meanCmax estimates of trovafloxacin for the two treatments was53.8% (95% CI: 36.1%, 80.1%), indicating a 46% reduc-tion.
The mean trovafloxacin Tmax was prolonged by approx-imately 4 hours for trovafloxacin/morphine (5.8 hours) ascompared with trovafloxacin/placebo (1.7 hours) (Table I).The mean t1/2 estimates for trovafloxacin/morphine andtrovafloxacin/placebo were 9.2 hours and 10.4 hours, re-spectively.
Mean morphine AUC0–` and Cmax estimates followingtrovafloxacin/morphine treatment were 104.2 ng z hour/mLand 159.5 ng/mL, respectively, compared with correspond-ing values of 106.7 ng z hour/mL and 148.3 ng/mL follow-ing morphine/placebo treatment (Table I). The ratio of themean morphine AUC0–` estimates for trovafloxacin/mor-phine versus morphine/placebo was 97.7% (95% CI:88.2%, 108.3%), whereas the ratio of the mean Cmaxestimates of morphine for the two treatments was 107.5%(95% CI: 83.6%, 138.3%). Figure 4 illustrates the mean6b-glucuronide-morphine plasma concentrations after co-administration of morphine with either trovafloxacin orplacebo. Mean 6b-glucuronide-morphine AUC0–t andCmax estimates following trovafloxacin/morphine treat-ment were 95.3 ng z hour/mL and 29.5 ng/mL, respec-
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
34S THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998

tively, compared with AUC0–t and Cmax values of 84.6 ngz hour/mL and 26.1 ng/mL following morphine/placebotreatment (Table I). The ratio of the mean 6b-glucuro-nide-morphine AUC0–t estimates of trovafloxacin/mor-phine versus morphine/placebo was 112.6% (95% CI:99.3%, 127.7%). The ratio of the mean Cmax estimates of6b-glucuronide-morphine for the two treatments was113.1% (95% CI: 102.5%, 124.8%).
The Tmax for morphine occurred at 10 minutes (end ofinfusion) for all subjects. No appreciable change in meanTmax for 6b-glucuronide-morphine was observed for trova-floxacin/morphine compared with morphine/placebo (0.9hour and 1.0 hour, respectively). The mean t1/2 estimatesfor morphine and 6b-glucuronide-morphine were 2.2 and2.4 hours, respectively, for trovafloxacin/morphine, and 2.4and 2.4 hours, respectively, for morphine/placebo (TableI).
PharmacodynamicsA statistically significant difference in overall mean re-
spiratory rate was found between the trovafloxacin/mor-phine and trovafloxacin/placebo treatments (adjustedmean 5 21.02 [21.51, 20.54; P 5 0.0001]; Table II).However, there was no significant difference in mean re-
spiratory rate between trovafloxacin/morphine and mor-phine/placebo treatments (P 5 0.8928).
Quantification of SedationThe mean change in sedation VAS increased postdose in
patients treated with trovafloxacin/morphine and mor-phine/placebo (Figure 5). VAS scores indicated significantincreases in sedation from baseline for the trovafloxacin/morphine and morphine/placebo treatments (P 5 0.0001)but not for the trovafloxacin/placebo treatment (P 50.9846; Table II).
Adverse EventsOne subject was discontinued on day 1 following the
initial treatment (trovafloxacin/morphine) due to adverseevents (mild anxiety, and moderate nausea and vomiting).The investigator considered these events, which resolvedon the same day, to be related to morphine.
The most frequently reported treatment-related adverseevents were dizziness, headache, and nausea during trova-floxacin/placebo treatment; nausea, vomiting, and head-ache during trovafloxacin/morphine treatment; and nau-sea, dizziness, and vomiting during morphine/placebotreatment. All adverse events were mild to moderate in
Figure 2. Mean trovafloxacin serum concentrations after coad-ministration of trovafloxacin with either placebo or morphine tohealthy subjects.
Figure 3. Mean morphine plasma concentrations after coadmin-istration of morphine with either trovafloxacin or placebo tohealthy subjects.
Figure 4. Mean 6b-glucuronide-morphine plasma concentrationsafter coadministration of morphine with either trovafloxacin orplacebo to healthy subjects.
Figure 5. Mean change in sedation VAS (cm) versus time post-dose (hours).
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998 35S
severity and none was considered serious. Moreover, therewere no clinically significant changes in vital signs. Pleasesee the article by Williams and Hopkins for a detailedpresentation of the safety and tolerability of trovafloxa-cin.20
DISCUSSIONThe pharmacokinetic parameters observed in this study
for trovafloxacin coadministered with placebo were similarto those reported in published studies. The AUC0–`, Cmax,and half-life values of 28.5 mg z hour/mL, 2.0 mg/mL, and10.4 hours, respectively, were comparable to values re-ported by Teng et al12 after administration of a single doseof trovafloxacin.
A central goal of this study was to evaluate possiblealterations in the pharmacokinetics of trovafloxacin result-ing from the coadministration of intravenous morphine.This potential interaction is of clinical importance, be-cause morphine is commonly used in surgical patients whomay also need antimicrobial therapy.18
The results of the current study showed that following the
coadministration of oral trovafloxacin (200 mg) and intra-venous morphine (0.15 mg/kg), the half-life of trovafloxa-cin was not altered, suggesting that morphine has littleeffect on the elimination of trovafloxacin. However, thebioavailability and Cmax of trovafloxacin were reduced by36% and 46%, respectively, and Tmax was prolonged by4 hours. Morphine can prolong gastric emptying and delaythe passage of gastric contents by as much as 12 hours.18
These results are comparable to those reported for cipro-floxacin.21 When coadministered with papaveretum, anopioid alkaloid related to morphine, the absorption ofciprofloxacin was significantly reduced.21
The question remains, however, whether these pharma-cokinetic changes will compromise the antimicrobial effi-cacy of trovafloxacin when used for surgical prophylaxis.Although the current study did not address this questiondirectly, the pharmacokinetic profile of trovafloxacin whencoadministered with morphine may still produce tissueconcentrations sufficient for antimicrobial activity. TheCmax for trovafloxacin when administered with morphinewas 1.1 mg/mL. With tissue:serum ratios for trovafloxacin
TABLE IPharmacokinetic Parameters for Trovafloxacin, Morphine, and 6b-Glucuronide-Morphine
Treatment*Cmax
mg/mLTmax
(hour)AUC0–t
mg z hour/mLAUC0–`
mg z hour/mLKel
(hour21)T1/2
(hour)
TrovafloxacinMean A 2.0 1.7 26.1 28.5 0.0666 10.4SD 0.8 1.2 8.9 8.6 0.0107Mean B 1.1 5.8 15.6 17.7 0.0753 9.2SD 0.6 3.2 13.7 13.6 0.0273
MorphineMean B 159.5 0.17 94 104.2 0.3132 2.2SD 72 0.0 18 17 0.0693Mean C 148.3 0.17 97 106.7 0.2943 2.4SD 76 0.0 21 22 0.0855
6b-Glucuronide-morphineMean B 29.5 0.9 95.3 122 0.2937 2.4SD 5 0.2 27 31 0.0582Mean C 26.1 1.0 84.6 117 0.2841 2.4SD 5 0.2 19 23 0.0391
* A 5 trovafloxacin/placebo; B 5 trovafloxacin/morphine; C 5 morphine/placebo.
TABLE IIStatistical Results for Respiratory Rate and Sedation VAS*
Trovafloxacin/Placebo Trovafloxacin/Morphine Morphine/Placebo
Respiratory rate/minuteAdjusted mean 15.52 14.50† 14.53Standard error 0.26 0.27 0.28
95% CI (14.98, 16.06) (13.95, 15.05) (13.97, 15.09)Sedation VAS (cm)‡
Adjusted mean 0.01 2.36§ 1.76§
Standard error 0.30 0.30 0.3095% CI (20.62, 0.63) (1.73, 2.99) (1.13, 2.39)
* Repeated measures ANOVA, mixed effects model.† P 5 0.0001 versus trovafloxacin/placebo.‡ Change from baseline before start of infusion.§ P 5 0.0001 versus respective baseline.
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
36S THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998

between 0.8 and 1.5 in colon tissue after intravenousadministration,22 expected tissue concentrations of trova-floxacin, even when administered with morphine, wouldbe .1.5 mg/mL. Minimum inhibitory concentrations re-quired to inhibit 90% of microorganisms (MIC90) of trova-floxacin against the following clinically important patho-gens are all #1.0 mg/mL: Escherichia coli (0.06), Klebsiellapneumoniae (0.12), Pseudomonas aeruginosa (1.0), Hae-mophilus influenzae (0.015), Neisseria gonorrhoeae (0.25),Moraxella catarrhalis (0.06), methicillin-resistant Staphylo-coccus aureus (1.0), methicillin-susceptible S. aureus(0.06), Enterococcus faecalis (0.5), viridans group strepto-cocci (0.25), vancomycin-resistant enterococci (1.0),Streptococcus pneumoniae (0.06–0.25), Bacteroides fragilis(0.5), and Mycoplasma pneumoniae (0.25).2,23–26 Conse-quently, even when combined with morphine, the relativebioavailability of trovafloxacin should remain sufficientlyhigh to ensure effective prophylaxis against postsurgicalinfection.
When oral trovafloxacin and intravenous morphine werecoadministered, absorption of the antibiotic was delayed,with the time to achieve initial maximum trovafloxacinserum levels lengthened by 4 hours. However, the potentialfor delayed antibiotic absorption can be minimized byadministering trovafloxacin at least 2 hours prior to initi-ation of morphine therapy in fasting patients or 4 hoursprior in fed patients. Alternatively, for many surgical pa-tients intravenous administration of trovafloxacin may bepreferred. The intravenous formulation, alatrofloxacin, is aprodrug of trovafloxacin that is rapidly converted to theparent compound in vivo and shares a similar pharmaco-kinetic profile in normal volunteers to the oral formula-tion.19
The other objectives of this investigation were to evalu-ate the pharmacokinetics of morphine, particularly theformation and clearance of the active metabolite, 6b-glucuronide-morphine, after coadministration with trova-floxacin, and to assess the impact of pharmacokineticchanges on the subjects’ response to morphine. Both trova-floxacin and morphine are metabolized by glucuronidation,and competition between these compounds for this meta-bolic pathway could have an important impact on theefficacy and toxicity of morphine. The analgesic potency ofmorphine is predominantly due to the 6b-glucuronide me-tabolite of morphine.27
The clearance (CL) of 6b-glucuronide-morphine can beinferred from the relationship
AUC(m)
AUC(d)5
fm z FH(m) z CL(d)
CL(m)
where fm is the fraction of morphine converted to metab-olite, FH(m) is the systemic availability of the metabolite6b-glucuronide-morphine, (m) is metabolite, and (d) isparent drug. Since neither of these fractions can exceed 1,a value of this ratio in excess of 1 suggests that the clear-ance of the metabolite is lower than that of the parentdrug.28 The mean ratio of the AUC of 6b-glucuronide-morphine to the AUC of morphine was unchanged by thecoadministration of trovafloxacin, indicating that trova-floxacin did not alter the clearance of the active metabo-lite.
In this study, the pharmacokinetics of morphine and itsmetabolite were not altered following coadministration oftrovafloxacin. Although sedation was increased and therespiratory rate was significantly decreased by the mor-phine/trovafloxacin combination, there was no significantdifference between the morphine/trovafloxacin and themorphine/placebo treatments. Based on these results, in-creased sedation and respiratory depression were predomi-nantly morphine effects and were not exacerbated bytrovafloxacin. There were also no serious adverse eventsnoted in this study, and subjects receiving the trovafloxa-cin/morphine combination experienced side effects similarto those of subjects receiving the morphine/placebo com-bination. These results indicate that trovafloxacin does notexacerbate the respiratory depressant effects produced bymorphine, and that these drugs, when combined, do notresult in an increased number of side effects.
The coadministration of trovafloxacin and morphine re-duces the bioavailability and maximum serum concentra-tions of oral trovafloxacin. However, other pharmacoki-netic parameters of trovafloxacin were comparativelyunchanged, suggesting that the efficacy of trovafloxacincould be maintained in many patients who receive con-comitant morphine. Moreover, the delay in absorption oforal trovafloxacin when coadministered with morphinemay be avoided by administering the antibiotic at least2 hours prior to initiation of morphine therapy in a fastedstate or after at least 4 hours in a fed state, or by using theintravenous formulation alatrofloxacin. The results alsoshow that morphine plasma levels and pharmacologic ef-fects are not significantly altered by coadministration oftrovafloxacin. Despite their similar metabolic pathways,the trovafloxacin/morphine combination neither exacer-bated the respiratory depressant effects of morphine norproduced additional side effects when compared with mor-phine/placebo treatment. These results suggest that theefficacy of trovafloxacin may be maintained when coad-ministered with morphine.
REFERENCES1. von Rosenstiel N, Adam D. Quinolone antibacterials: an updateof their pharmacology and therapeutic use. Drugs. 1994;47:872–901.2. Neu HC, Chin N-X. In vitro activity of the new fluoroquinoloneCP-99,219. Antimicrob Agents Chemother. 1994;38:2615–2622.3. Blumberg HM, Rimland D, Carroll DJ, et al. Rapid developmentof ciprofloxacin resistance in methicillin-susceptible and -resistantStaphylococcus aureus. J Infect Dis. 1991;163:1279–1285.4. Kaatz GW, Seo SM, Ruble CA. Mechanisms of fluoroquinoloneresistance in Staphylococcus aureus. J Infect Dis. 1991;163:1080–1086.5. Jones RN. In vitro antimicrobial activity of CP-99,219, a new7-azabicyclonaphthyridone. Drugs. 1995;49(suppl 2):205–207.6. Moellering RC Jr. Quinolone antimicrobial agents: overviewand conclusions. In: Wolfson JS, Hooper DC, eds. Quinolone An-timicrobial Agents. Washington, DC: American Society forMicrobiology; 1989:273–283.7. Felmingham D, Robbins MJ, Ingley K, et al. In vitro activity oftrovafloxacin, a new fluoroquinolone, against recent clinical iso-lates. J Antimicrob Chemother. 1997;39(suppl B):43–49.8. Girard AE, Girard D, Gootz TD, et al. In vivo efficacy oftrovafloxacin (CP-99,219), a new quinolone with extended activ-ities against gram-positive pathogens, Streptococcus pneumoniae, and
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998 37S

Bacteroides fragilis. Antimicrob Agents Chemother. 1995;39:2210–2216.9. Coque TM, Singh KV, Murray BE. Comparative in-vitro activ-ity of the new fluoroquinolone trovafloxacin (CP-99,219) againstgram-positive cocci. J Antimicrob Ther. 1996;37:1011–1016.10. Snydman DR, McDermott L. Analysis of the in vitro activityof trovafloxacin (CP-99,219) against Bacteroides species. Infect DisClin Pract. 1996;5(suppl 3):S96–S100.11. Gorbach SL, Bartlett JG. Anaerobic infections. N Engl J Med.1974;290:1177–1184, 1237–1245, 1289–1294.12. Teng R, Harris SC, Nix DE, et al. Pharmacokinetics and safetyof trovafloxacin (CP-99,219), a new quinolone antibiotic, follow-ing administration of single oral doses to healthy male volunteers.J Antimicrob Chemother. 1995;36:385–394.13. Teng R, Liston TE, Harris SC. Multiple-dose pharmacokineticsand safety of trovafloxacin in healthy volunteers. J AntimicrobChemother. 1996;37:955–963.14. Teng R, Dogolo LC, Willavize SA, et al. Oral bioavailability oftrovafloxacin with and without food in healthy male volunteers. JAntimicrob Chemother. 1997;39(suppl B):87–92.15. Bergeron MG. The pharmacokinetics and tissue penetration ofthe fluoroquinolones. Clin Invest Med. 1989;12:20–27.16. Teng R, Dogolo LC, Willavize SA, Vincent J. Effect of age andgender on the pharmacokinetics of CP-99,219, a new quinoloneantibiotic, in healthy volunteers (Abstract F238). In: Abstracts ofthe Thirty-fifth Interscience Conference on Antimicrobial Agents andChemotherapy. Washington, DC: American Society for Microbiol-ogy, 1995:154.17. Vincent J, Teng R, Dogolo LC, et al. Effect of trovafloxacin, anew fluoroquinolone antibiotic, on the steady-state pharmacoki-netics of theophylline in healthy volunteers. J Antimicrob Che-mother. 1997;39(suppl B):81–86.18. Jaffe JH, Martin WR. Opioid analgesics and antagonists. In:Goodman Gilman A, Rall TW, Nies AS, Taylor P, eds. Goodmanand Gilman’s The Pharmacological Basis of Therapeutics. 8th ed.Elmsford, NY: Pergamon Press, 1990:485–521.19. Brighty KE, Gootz TD, Girard A, et al. Prodrugs of CP-99,219
for intravenous administration; synthesis and evaluation resultingin identification of CP-116,517 (Abstract 730). In: Abstracts of the7th European Congress of Clinical Microbiology and Infectious Diseases.Amsterdam: CONIFER, Excerpta Medica Medical Communica-tions b.v.; 1995:141.20. Williams DJ, Hopkins S. Safety and tolerability of intravenousto oral treatment and single dose intravenous or oral prophylaxiswith trovafloxacin. Am J Surg. 1998;176(Suppl 6A):74S–79S.21. Morran C, McArdle CS, Pettit L, et al. Brief report: pharma-cokinetics of orally administered ciprofloxacin in abdominal sur-gery. Am J Med. 1989;87(suppl 5A):86S–88S.22. Melnick G, Schwesinger H, Dogolo LC, et al. Concentrationsof trovafloxacin in colonic tissue and peritoneal fluid after intrave-nous infusion of the prodrug alatrofloxacin in patients undergoingcolorectal surgery. Am J Surg. 1998;176(Suppl 6A):14S–17S.23. Kenny GE, Cartwright FD. Susceptibilities of Mycoplasmapneumoniae, Mycoplasma hominis, and Ureaplasma urealyticum to anew quinolone, trovafloxacin (CP-99,219). Antimicrob Agents Che-mother. 1996;40:1048–1049.24. Endtz HP, Mouton JW, Den Hollander JG, et al. Comparativein vitro activities of trovafloxacin (CP-99,219) against 445 gram-positive isolates from patients with endocarditis and those withother bloodstream infections. Antimicrob Agents Chemother. 1997;41:1146–1149.25. Brighty KE, Gootz TD. The chemistry and biological profile oftrovafloxacin. J Antimicrob Chemother. 1997;39(suppl B):1–14.26. Spangler SK, Jacobs MR, Appelbaum PC. Activity of CP99,219 compared with those of ciprofloxacin, grepafloxacin, met-ronidazole, cefoxitin, piperacillin, and piperacillin-tazobactamagainst 489 anaerobes. Antimicrob Agents Chemother. 1994;38:2471–2476.27. Thompson Pl, Joel SP, John L, et al. Respiratory depressionfollowing morphine and morphine-6-glucuronide in normal sub-jects. Br J Clin Pharmacol. 1995;40:145–152.28. Rowland M, Tozer TN. Clinical Pharmacokinetics: Concepts andApplication. Philadelphia: Lea & Febiger; 1980.
MORPHINE AND TROVAFLOXACIN PHARMACOKINETICS/VINCENT ET AL
38S THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 (Suppl 6A) DECEMBER 1998