the role of voice analysis in the recovery process of...
TRANSCRIPT

Theses of the PhD Dissertation
EÖTVÖS LORAND UNIVERSITY OF SCIENCES FACULTY OF HUMANITIES
Doctoral School of Linguistics
Head: Prof. Dr. Janusz Bańczerowski DSc, university professor
Doctoral Programme of Hungarian Linguistics Head: Prof. Dr. Jenő Kiss, Member of the Academy
THE ROLE OF VOICE ANALYSIS IN THE RECOVERY
PROCESS OF CERTAIN OTO-RHINO-LARYNGOLOGICAL
DISEASES
Dr Zoltán Fent
Consultant: Prof. Dr. Mária Gósy DSc, university professor
Budapest 2010

1. Introduction
The most important means of human communication is speech.
In recent years quality of life has become an ever more important factor
during individual oncological interventions, thus during the treatment of
head-and neck tumors, as well.
In Hungary the number of malignant head-and-neck tumors, including
hypopharyngeal and laryngeal tumors has increased significantly. A portion
of recognized tumors can only be treated with total laryngeal extirpation.
Recently, with developing surgical techniques, the approach of functional
preservation has come to the foreground: more and more patients undergo
only partial laryngectomy, and these patients would have previously
undergone total laryngeal extirpation.
We cannot be satisfied by curing the disease, and removing the tumor in
itself: the quality of verbal communication crucially affects the patient’s
quality of life as well as his/her readaptation to civil life. If this is not
successful – considering the tight relationship between physical and mental
processes – then frustration deteriorates the recovery and survival potential
of the patient.
Facial nerve paresis – due to its obvious nature – severely damages
interpersonal relations. Starting the adequate treatment as soon as possible
depending on the etiology is extremely important with regards to recovery.
2
Objectives of the dissertation:
1) To study the effect of surgical interventions performed as the
treatment for malignant laryngeal tumors on the quality of voice and
quality of life,
2) To establish the relationship between the self-assessment of speech
of partial- and total laryngeal extirpated patients and the
assessment of the listeners
3) To study the significant alterations in the quality of voice after
supracricoid horizontal laryngeal surgical intervention
4) To study the limitations of voice analysis in patients who underwent
laryngeal operations; can the self-assessment of patients’ speech
based on the quality of life test be matched with the value obtained
during their voice analysis?
5) Will articulation change during peripheral facial nerve paresis?
6) Is there any relationship between the temporal changes of paralyzed
facial nerve excitability, and the change in results obtained during
voice analysis?
7) Which parameter(s) tested during voice analysis of which vowels are
most suitable to monitor the recovery process of facial nerve paresis?
3

2. Structure of the dissertation
The dissertation consists of 14 chapters.
Chapter 1, the introduction describes the subject and its actuality, as well as
the general aim of the research.
Chapter 2 is an anatomical overview. It outlines the knowledge that is
indispensable to interpret the research summarized in the dissertation. The
first subchapter details the structure of organs involved in voice formation,
while the second subchapter discusses the facial nerve.
Chapter 3 summarizes the physiology of voice formation, as well as the
acoustic and phonetic characteristics of human voice and speech.
The first subchapter of Chapter 4 introduces everyday and experimental
testing methods of organs of speech. The second subchapter discusses the
testing methods of the facial nerve and the reasons of peripheral facial
nerve paresis, as well as the most frequent associated clinical pictures.
Chapter 5 overviews laryngeal- and hypopharyngeal surgical treatment
options. Consequences of total laryngectomy and the method of voice
rehabilitation are detailed. It also outlines laryngeal operations performed
as part of my research later presented in the dissertation.
Chapter 6 provides a literature review of the effect of partial laryngeal
operations on voice formation and speech.
Chapter 7 examines parameters influencing quality of life in patients who
underwent surgical intervention due to a laryngeal or pharyngeal tumor.
Chapter 8 describes comparative testing of the speech of patients who
underwent a partial laryngeal operation. It compares and discusses the
opinion of the listeners of the perception test and the patients’ self-
assessment grouped according to the type of surgical intervention.
Chapter 9 demonstrates the acoustic analysis of the speech sound developed
after supracricoid horizontal laryngeal resection. It investigates the reasons
4
of significantly different speech production of the two types of
reconstructional options after surgery.
Chapter 10 provides a comparison of the speech of patients who underwent
laryngeal operations both on objective and subjective bases. It also
elucidates the potentials and limitations of voice analysis.
Chapter 11 details the perception tests of patients after total laryngectomy.
The self-assessment of patients communicating with esophageal speech and
of those using electrolarynx is compared with the impression of the
listeners.
Chapter 12 details the monitoring of recovery processes of facial pareses
using voice analysis. Results obtained during voice analysis are compared
with results of the widely used NET test.
Chapter 13 summarizes the results.
Chapter 14 lists the references used.
5

3. Materials, methods, research subjects
In the dissertation – first in Hungary – we applied the QLQ-C30 quality of
life test of the European Organization for Research on Treatment of Cancer
(EORTC), as well as the head-and-neck-tumor specific H&N35 quality of life
test.
Statistical analyses were performed with SPSS version 13.0 and 15.0
software.
Voice analysis was performed using Praat software version 4.3, 4.4, and 4.5.
Research subjects were selected from patients treated at the Department of
Oto-Rhino-Laryngology and Head-and Neck Surgery.
4. Testing quality of life in patients who underwent a laryngeal
operation
The study included 54 patients who had undergone hemilaryngectomy,
supraglottic horizontal-, supracricoid horizontal, or supracricoid lateral
laryngeal resection or total laryngectomy, with or without voice-prosthesis
implantation.
Our objective was to establish: which parameters influence mostly general
quality of life and subjective health status in the period after the surgical
intervention.
Statistical analysis of data was performed using discriminant analysis („canonical variate analysis” = CVA). Results are represented on a biplot that
graphically illustrates the relationship of the variables and the axis (Figure 1).
6

Axis 120151050-5-10-15-20-25-30-35
Axi
s 2
30
28
26
24
22
20
18
16
14
12
10
8
6
4
2
0
-2
-4
-6
-8
-10
-12
-14
-16
-18
TL4TL6TL3
TL1
TL5TL2
SCL6SCL1
TLV2
SCL2SCL3SCL4SCL9SCL8
SCL5
SCL10SCL7
TLV1
TLV4
TLV3
HL3HL2HL1
SCH1HL5HL4SCH3SCH2SCH4SCH8
SCH5SCH6
SCH7
SGH6
SGH3SGH1SGH2SGH5SGH4
HNSE
FI
HNSP
HNSS
HNDR
SL
HNPK HNTE
HNOM
DI
NV
HNSC
PF2
HNPAFA
PA
DYHNFI
CO
RF2
EF
HNSO
AP
HNSW
CF
HNCO
HNWL
HNSX
HNWG
HNNU
SF
Figure 1. Discriminant analysis of parameters determining quality of life and of the type of surgical intervention in patients with pharyngeal and laryngeal tumors. Signs: parameters determining quality of life: PF2: physical functions, RF2: performing activities, EF: Emotional functions, CF: cognitive functions, SF: social functions, FA: fatigability, NV: nausea, vomiting, PA: pain, DY: dyspnoe, SL: sleeplessness, AP: anorexia, CO: constipation, DI: diarrhea, FI: financial difficulties, HNPA: pain, HNSW: swallowing, HNSE: sensory organs, HNSP: speech, HNSO: social eating, HNSC: social contacts, HNSX: sex, HNTE: teeth, HNOM: opening the mouth, HNDR: dry mouth, HNSS: sticky saliva, HNCO: coughing, HNFI: sense of disease, HNPK: pain killers, HNNU: dietary supplements, HNFE: nutrition probe, HNWL: weight loss, HNWG: weight gain; type of surgery. HL: hemilaryngectomy, SGH: supraglottic horizontal-, SCH: supracricoid horizontal-, SCL: supracricoid lateral laryngeal resection, TL: laryngectomy, TLV: voice-prosthesis implantation, the numbers indicated next to the type of surgery indicate the number of specific patients.
General health- and quality of life values correlate with the extent of
intervention. The subjective health state and quality of life of subjects
eligible for voice-prosthesis implantation is significantly higher than that of
those living without a voice-prosthesis.
After surgery, on the long run communication skills significantly influence
the patient’s quality of life. Recidivation- and metastasis free survival can
be evaluated only together with quality of life, this latter can only be
7
improved by bringing organ- and function preserving oncological treatment
methods into the foreground.
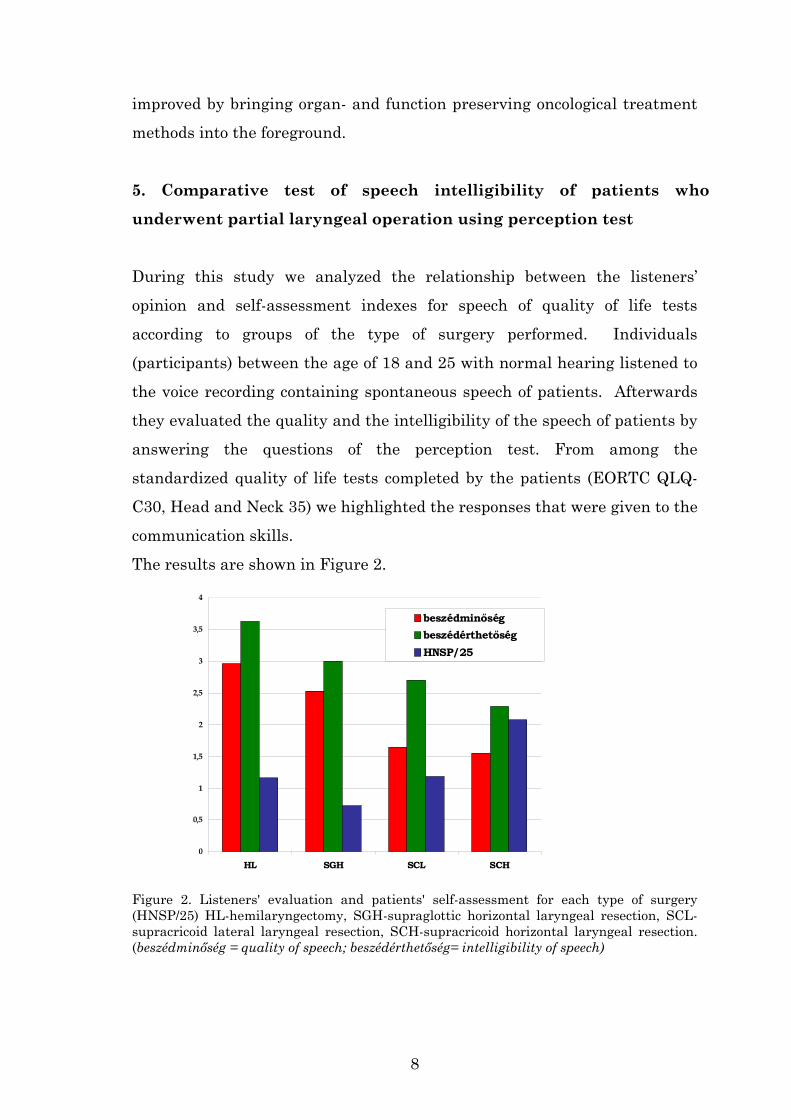
5. Comparative test of speech intelligibility of patients who
underwent partial laryngeal operation using perception test
During this study we analyzed the relationship between the listeners’
opinion and self-assessment indexes for speech of quality of life tests
according to groups of the type of surgery performed. Individuals
(participants) between the age of 18 and 25 with normal hearing listened to
the voice recording containing spontaneous speech of patients. Afterwards
they evaluated the quality and the intelligibility of the speech of patients by
answering the questions of the perception test. From among the
standardized quality of life tests completed by the patients (EORTC QLQ-
C30, Head and Neck 35) we highlighted the responses that were given to the
communication skills.
The results are shown in Figure 2.
0
0,5
1
1,5
2
2,5
3
3,5
4
HL SGH SCL SCH
beszédminőségbeszédérthetőségHNSP/25
Figure 2. Listeners' evaluation and patients' self-assessment for each type of surgery (HNSP/25) HL-hemilaryngectomy, SGH-supraglottic horizontal laryngeal resection, SCL-supracricoid lateral laryngeal resection, SCH-supracricoid horizontal laryngeal resection. (beszédminőség = quality of speech; beszédérthetőség= intelligibility of speech)
8

The comparisons reveal that qualification by patients and by participants do
not correlate for each type of surgery; one possible explanation is different
expectation by patients with regards to post-surgery quality of voice.
Self-assessment of speech function is influenced by the type of laryngeal
operation performed. The larger the extent of residual defect in the larynx
is, the worse the value of their evaluation is.
The results obtained demonstrate that patients who underwent partial
laryngeal operation communicate well in everyday life, and this is not only
based on self-assessment, but also on the opinion of their environment.
6. “Zönge” (tone produced by the vibration of the vocal cords) voice
formation potentials after supracricoid horizontal laryngeal
resection
Significant differences can be observed in the quality of voice of patients
who underwent supracricoid horizontal resection. Some patients are only
able to form a weak, whispering-type voice, while others produce a voice of
satisfactory volume, but hoarse. Based on our investigations performed on
the group of 11 patients, differences of the place for forming the "zönge"
voice (tone produced by the vibration of the vocal cords) constitute the
background of voice quality differences. If the epiglottis can be preserved
(CHEP), the place for forming the “zönge” voice will be between the edge of
the epiglottis and the posterior pharyngeal wall (Figure 3). If the arytenoid
region is preserved, the place of “zönge” voice formation will be between the
arytenoid region and the epiglottis (Figure 4). After a reconstruction with
epiglottis removal (CHP), in certain cases no “zönge” voice is formed at all;
air flows unarrested through the glottis (Figure 5). During their speech
these patients try to use the “friction” of the air passing through the
strictures of the hypopharynx as primary voice. In other cases of
reconstruction with epiglottis removal the place for “zönge” voice formation
9

is the substitute vocal cord formed between the preserved arytenoid region
and the root of the tongue.
Figure 3. The place of “zönge” voice formation is between the epiglottis and the posterior
pharyngeal wall
Figure 4. The place of “zönge” voice formation is between the epiglottis and the arytenoid
region
Figure 5. The place for forming “zönge” voice is missing
10
During the acoustic analysis of patients’ voice recordings, we established the
basic frequency, and during the examination of a sustained vowel we
measured the extent of frequency- an amplitude fluctuation, as well as the
signal/noise ratio. By comparing the results obtained with those obtained for
a voice formed with a normal larynx, we established that the harsh tone of
the voice formed with the epiglottis is explained by a higher than normal
fluctuation of frequency- and amplitude, as well as by the deterioration of
the signal/noise ratio.
7. Relationships of objective and subjective assessments of speech
in patients who underwent a laryngeal operation
In our study we examined the acoustic parameters of the speech of 95
patients operated for laryngeal- or hypopharyngeal tumors, and compared
them with answers related to quality of life of EORTC questionnaires. 10
adult males with normal larynx served as the control group.
We aimed to establish in patients who underwent various types of partial
laryngectomy or total laryngectomy due to a malignant tumor and
rehabilitated using various methods, to what extent can communication
abilities experienced by the patients be objectivized with acoustic
parameters measured during their voice analysis.
From among the responses given to the questions we pay special attention
to those that were provided related to general health state, quality of life, as
well as speech, social contacts and social functions.
From among the acoustic parameters we analyzed the phonation time,
speech rate, articulation speed, fundamental frequency, number of
detectable formants, the rate of frequency and intensity fluctuation, as well
as the signal/noise ratio. The results are shown in Table 1 and 2.
11
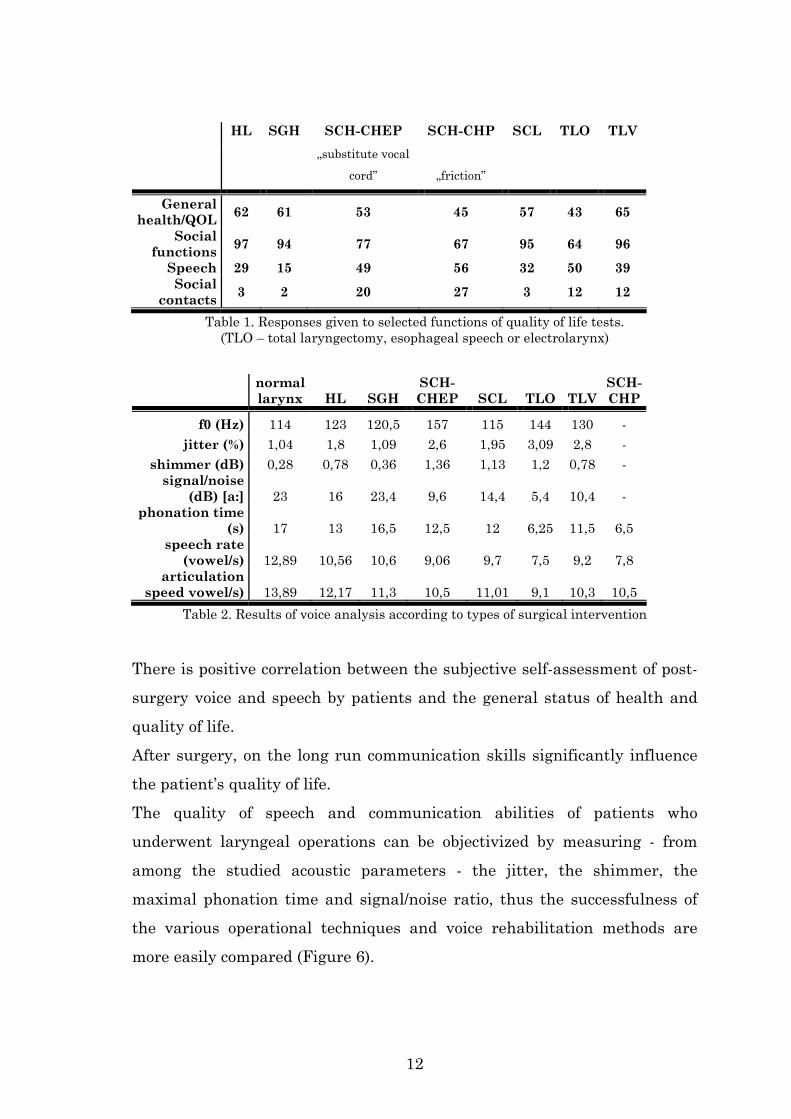
HL SGH SCH-CHEP SCH-CHP SCL TLO TLV
„substitute vocal
cord” „friction”
General health/QOL 62 61 53 45 57 43 65
Social functions 97 94 77 67 95 64 96
Speech 29 15 49 56 32 50 39 Social
contacts 3 2 20 27 3 12 12
Table 1. Responses given to selected functions of quality of life tests. (TLO – total laryngectomy, esophageal speech or electrolarynx)
normal larynx HL SGH
SCH-CHEP SCL TLO TLV
SCH-CHP
f0 (Hz) 114 123 120,5 157 115 144 130 - jitter (%) 1,04 1,8 1,09 2,6 1,95 3,09 2,8 -
shimmer (dB) 0,28 0,78 0,36 1,36 1,13 1,2 0,78 - signal/noise
(dB) [a:] 23 16 23,4 9,6 14,4 5,4 10,4 - phonation time
(s) 17 13 16,5 12,5 12 6,25 11,5 6,5 speech rate
(vowel/s) 12,89 10,56 10,6 9,06 9,7 7,5 9,2 7,8 articulation
speed vowel/s) 13,89 12,17 11,3 10,5 11,01 9,1 10,3 10,5 Table 2. Results of voice analysis according to types of surgical intervention
There is positive correlation between the subjective self-assessment of post-
surgery voice and speech by patients and the general status of health and
quality of life.
After surgery, on the long run communication skills significantly influence
the patient’s quality of life.
The quality of speech and communication abilities of patients who
underwent laryngeal operations can be objectivized by measuring - from
among the studied acoustic parameters - the jitter, the shimmer, the
maximal phonation time and signal/noise ratio, thus the successfulness of
the various operational techniques and voice rehabilitation methods are
more easily compared (Figure 6).
12

ép gé
ge HLSGH
SCH-CHEP(C
HP)
SCLTLO TLV
SCH-CHP
Általános eg./QOL
szociális funkciók
jitter (%) x10
shimmer (dB) x10
Figure 6. The relation ship of jitter and shimmer to social functions and quality of life
The rate of frequency and amplitude fluctuations is inversely proportional to the subjective quality of life: QOL/jitter - [r= -0,68, p<0,05] QOL/shimmer - [r= -0,76, p<0,05] („általános eg” = general health, „szociális funkciók” = social functions)
8. Studying esophageal speech and fundamental frequency formed
with an electric artificial larynx after total laryngectomy
During the perception test performed with the inclusion of 11 patients we
compare the impressions of the listeners of speech quality and intelligibility
with the self assessment of speech provided by total laryngeal extirpated
patients. Objectives:
To establish if there is any relationship between the assessment of the
speaker and that of the conversation partner. Are there any differences in
this respect between those using an electric larynx and those with
esophageal speech?
Based on the self-assessment of speakers, those using an electric larynx are
more satisfied with their speech and communication efficiency than those
applying esophageal speech. However, according to the assessment provided
by the listeners, esophageal speech proved to be significantly better both
with respect to speech quality and speech intelligibility. The results show
13

that esophageal speech allows for a more successful communication, thus for
a more efficient re-adaptation to society.
9. Monitoring of recovery processes of facial pareses using voice
analysis
In our study we compared NET (nerve excitability testing) test results of
patients suffering from peripheral facial nerve paresis with the results of
their voice analysis, by which we monitor their voice formation.
Our objective was to establish:
• Will articulation change during peripheral facial nerve paresis?
• Is there any relationship between the results of the NET test
(excitability of the paralyzed facial nerve) and the results of voice
analysis?
• Which parameter(s) tested during voice analysis of which vowels are
most suitable to monitor the recovery process of facial nerve paresis?
• In case of the 3 examined branches (temporal, zygomatic, and
marginal mandibular) which, to what extent and in case of which
vowels show a significant relationship with the changes of NET
values?
We asked the 30 study participant patients to repeat 1-2-syllable,
vocabulary form words containing mostly front-formed, labial articulation
vowels and sentences after hearing them read out. We randomly selected 3-
3 identical vowel from the voice recorded during patient visits. We analyzed
the 8 tested vowels from the voice record, taking care to analyze the vowel
coming from the same word or sentence when the specific patient performs
his/her next visit.
14

We compared the results of the voice analysis of the voice record (F0, jitter,
shimmer, signal/noise ratio) with the NET results.
In order to show correlation when comparing the mean of the NET values
and of acoustic measurements we calculated Pearson’s correlation
coefficient. The results are shown in Table 3.
15

NET value temp.
NET value zyg.
NET value marg.
NET value temp.
NET value zyg.
NET value marg.
fundamental frequency
fundamental frequency
jitter % jitter %
jitter (µs) jitter (µs)
shimmer % shimmer %
shimmer (dB) shimmer (dB)
i
signal/noise ratio (dB)
y
signal/noise ratio (dB)
NET value temp.
NET value zyg.
NET value marg.
NET value temp.
NET value zyg.
NET value marg.
fundamental frequency
fundamental frequency
jitter % jitter %
jitter (µs) jitter (µs)
shimmer % shimmer %
shimmer (dB) shimmer (dB)
i:
signal/noise ratio (dB)
y:
signal/noise ratio (dB)
NET value temp.
NET value zyg.
NET value marg.
NET value temp.
NET value zyg.
NET value marg.
fundamental frequency
fundamental frequency
jitter % jitter %
jitter (µs) jitter (µs)
shimmer % shimmer %
shimmer (dB) shimmer (dB)
ɛ
signal/noise ratio (dB)
ø
signal/noise ratio (dB)
NET value temp.
NET value zyg.
NET value marg.
NET value temp.
NET value zyg.
NET value marg.
fundamental frequency
fundamental frequency
jitter % jitter %
jitter (µs) jitter (µs)
shimmer % shimmer %
shimmer (dB) shimmer (dB)
e:
signal/noise ratio (dB)
ø:
signal/noise ratio (dB)
Table 3. Correlations of front formed, rounded vowels. A yellow field indicates which acoustic parameter change of the specific vowel correlates with NET value changes
measured on the defined facial nerve branches
16

Based on the results we can establish that during facial nerve paresis
articulation changes can be observed in each case.
From among the tested parameters of voice analysis, NET test results show
correlation with fundamental frequency (F0), jitter, shimmer and the
signal/noise ratio.
From the three facial nerve branches tested by us in the majority of cases
we observed a correlation with regards to articulation change on the
zygomatic branch and on the marginal mandibular branch.
We could reveal most correlations in case of these 2 branches and for the
front formed long vowels.
For each tested vowel F0 change correlates with NET values in case of the
zygomatic branch and marginal brand.
17

10. Results and Conclusions
1. In Hungary we were the first to perform a comprehensive quality of
life testing according to international standards in 2 periods on a
total number of 149 patients who underwent total- and partial
laryngectomy by using the QLQ-C30 quality of life test of the
European Organization for Research on Treatment of Cancer
(EORTC), as well as the head-and-neck-tumor specific H&N35
quality of life test. We established that on the long run
communication skills are decisive with regards to patients’ quality of
life.
2. By using the perception test we established that the larger the extent
of the defect remaining after the surgery in the larynx, the worse is
the listeners’ assessment for speech quality and speech intelligibility.
Patients who underwent partial laryngeal operation communicate
well in everyday life, and this is not only based on self-assessment,
but also on the opinion of their environment.
3. By testing the reasons of significant voice quality alterations
observed after supracricoid horizontal laryngeal operations, we
revealed potential ways of primary voice formation and their acoustic
consequences.
4. We established that after total- or partial laryngectomy, there is a
positive correlation between the subjective assessment of post-
surgery voice and speech by patients and general status of health,
and quality of life. The quality of speech and communication abilities
of patients who underwent laryngeal operations can be objectivized
by measuring - from among the acoustic parameters - the jitter, the
18

shimmer, the maximal phonation time and signal/noise ratio, thus
the successfulness of the various operational techniques and voice
rehabilitation methods are more easily compared.
5. Even internationally we were the first to test the effect of facial
nerve paresis on articulation using the method of voice analysis.
From among the tested parameters of voice analysis, NET test
results show correlation with fundamental frequency (F0), jitter,
shimmer and the signal/noise ratio. We could reveal most
correlations in case of the front formed, long vowels.
6. Based on the results of this research the effect of paresis severity on
articulation would worth to be investigated further with a modified
set of words. Based on the results of these studies, voice analysis
could be used in a new, practical way in the future.
19

Presentations related to the dissertation Speech after total laryngectomy: the oesophageal and voice prosthesis sound Fent Z., Kiefer G., Répássy G. 4th European Congress of Oto-Rhino-Laryngology Head and Neck Surgery Berlin, 2000. Tapasztalataink a percutan endoscopos gastrostoma alkalmazásával előrehaladott fej-nyaki tumoros betegeken Lőrincz T., Fent Z., Szirmai Á., Répássy G. Fül-orr-gégegyógyászat 2003/2.109-113. Az életminőséget meghatározó paraméterek garat és gégerákos betegeknél Fent Z., Kiefer G., Jósa V., Répássy G. MFOE 39. Kongresszusa, 2004. május 26-29., Sopron A supracricoid horisontalis gégeresectio utáni beszédhang akusztikai analízise Kiefer G., Fent Z., Répássy G.: MFOE 39. Kongresszusa, 2004. május 26-29., Sopron Supracricoid lateralis gégeresectio után képzett hang akusztikai analízise Kiefer Gábor dr., Fent Zoltán dr., Bajnóczyné Szucsák Klára, Répássy Gábor dr. MFFLT és a MAGYE Kongresszusa, 2004. június 24-26., Pécs A hangrehabilitáció eredményeinek összehasonlító fonetikai vizsgálata Kiefer G., Fent Z.,Gósy M. VII. Nemzetközi Magyar Nyelvtudományi Kongresszus, 2004. augusztus 29-31. MTA, Budapest Factors Defining Quality of Life in Patients with Pharyngeal and Laryngeal Cancer (poster) Fent, Zoltan; Kiefer, Gabor; Josa, Valeria; Repassy, Gabor; 5th European Congress of Oto-Rhino-Laryngology Head and Neck Surgery, Rhodos, 2004.
20

Comparative Acoustic Analysis of the Voice Rehabilitation After Partial and Total Laryngectomy Kiefer, Gabor; Fent, Zoltan; Repassy, Gabor; 5th European Congress of Oto-Rhino-Laryngology Head and Neck Surgery, Rhodos, 2004. A beszéd objektív és szubjektív minősítésének összefüggései gégeműtötteknél Fent Zoltán – Kiefer Gábor – Gósy Mária XV. Magyar Alkalmazott Nyelvészeti Kongresszus Miskolc, 2005. április 7-9. Részleges- és teljes gégeeltávolításon átesett betegek beszédakusztikai paraméterei, szubjektív beszédminősége Fent Zoltán – Kiefer Gábor – Gósy Mária MFFLT és a MAGYE Kongresszusa, 2005. június 16-18., Kőszeg A gége betegségei és a zöngeképzés Fent Zoltán PhD kurzus előadás, 2005.november 17., ELTE BTK Fonetika Tanszék Részleges gégeműtéten átesett betegek nyelési funkciója Fent Zoltán dr, Bajnócziné Szucsák Klára, Tóth Krisztina dr., Szabó Balázs dr., Répássy Gábor dr. MFFLT és a MAGYE Kongresszusa, 2006. június 22-24., Hódmezővásárhely Részleges gégeműtéten átesett betegek nyelés rehabilitációja Bajnócziné Szucsák Klára, Fent Zoltán dr., Halmos György dr., Répássy Gábor dr. MFFLT és a MAGYE Kongresszusa, 2006. június 22-24., Hódmezővásárhely Eltérő fonációjú beszédmódok percepciós vizsgálata Markó Alexandra, Gráczi Tekla Etelka, Fent Zoltán dr. MFFLT és a MAGYE Kongresszusa, 2006. június 22-24., Hódmezővásárhely Supracricoid horisontális gégeresectio 1997 és 2006 között. Retrospektív elemzés Szabó B., Fent Z., Halmos Gy., Kiefer G., Tóth K., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 39. Nemzeti Kongresszusa 2006. szeptember 6-9., Debrecen Parciális gégeműtétek rövid- és hosszútávú eredményeinek értékelése Tóth K., Halmos Gy., Fent Z., Szabó B., Bódis F., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 39. Nemzeti Kongresszusa 2006. szeptember 6-9., Debrecen
21

Parciális gégeműtéten átesett betegek életminőségének vizsgálata Halmos Gy., Tóth K., Fent Z., Szabó B., Bajor B., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 39. Nemzeti Kongresszusa 2006. szeptember 6-9., Debrecen Gége- és hypopharynxtumoros betegek életminőségének összevetése beszédakusztikai paramétereivel Fent Z., Szabó B., Tóth K., Halmos Gy., Kiefer G., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 39. Nemzeti Kongresszusa 2006. szeptember 6-9., Debrecen Image guidance offers additional benefits in the endoscopic solution of extended cranio-facial malformations. A case report Andor Hirschberg, Zoltán Fent, Károly Hrabák, Ödön Rezek, Ron von Jako, Gábor Répássy International Journal of Pediatric Otorhinolaryngology Extra Volume 1, Issue 3, September 2006, Pages 181-184 Különleges zöngeképzési módok hatása az észlelésre Markó Alexandra PhD, Gráczi Tekla Etelka,dr. Fent Zoltán Magyar Tudomány 167. évfolyam 2007/3. szám A hangképzésben részt vevő szervek anatómiája Fent Z. Magyar Foniátriai, Fonetikai és Logopédiai Társaság Kongresszusa 2007. június 21-23., Eger A klinikánkon 2004-ben bevezetett, komplex foniátriai vizsgálati protokoll alkalmazásával szerzett tapasztalataink Kiefer G., Fent Z. Magyar Foniátriai, Fonetikai és Logopédiai Társaság Kongresszusa 2007. június 21-23., Eger Részleges gégeműtéten átesett betegek beszédének összehasonlító vizsgálata percepciós teszt segítségével Fent Z., Markó A., Gráczi T.E. Magyar Foniátriai, Fonetikai és Logopédiai Társaság Kongresszusa 2007. június 21-23., Eger Beszédészlelési és beszédmegértési zavarok az anyanyelv-elsajátításban Szerk.: Gósy Mária. Fent Z. A hallószerv, a hallás folyamata, zavarok Könyvfejezet, Nikol Kkt., 2007.
22

Az arcidegbénulások gyógyulási folyamatának monitorozása hanganalízis segítségével Fent Z., Bencsik B., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 40. Nemzeti Kongresszusa 2008. október 15-18. Az arcidegbénulások gyógyulási folyamatának monitorozása hanganalízis segítségével – esetismertetés Bencsik B., Fent Z., Szirmai Á. Magyar Fül-orr-gégeorvosok Egyesülete 40. Nemzeti Kongresszusa 2008. október 15-18. Reziduális epipharynx tumor endoszkópos eltávolítása és gamma terápiája Fent Z., Szabó B., Fedorcsák I., Nagy R., Noszek L., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 41. Nemzeti Kongresszusa 2010. október 13-16. Az arcidegbénulások gyógyulási folyamatának monitorozása hanganalízis segítségével – újabb eredmények Bódis F., Fent Z., Bencsik B., Répássy G. Magyar Fül-orr-gégeorvosok Egyesülete 41. Nemzeti Kongresszusa 2010. október 13-16. A supracricoid horisontalis gégeresectio utáni beszédhang akusztikai analízise Kiefer Gábor dr., Fent Zoltán dr., Répássy Gábor dr. Fül-orr-gégegyógyászat, megjelenés alatt Az életminőséget meghatározó paraméterek garat- és gégerákos betegeknél Fent Zoltán dr., Kiefer Gábor dr., Jósa Valéria, Répássy Gábor dr. Magyar Onkológia, megjelenés alatt
23