the standard of care for chronic type b disclosures …€¦ · estrera al, sandhu h, afifi ro,...
TRANSCRIPT
April 6, 2017
Copyright UPM-Kymmene Group 1
The Standard of Care for Chronic Type B Dissection is Endovascular Repair
Benjamin W. Starnes MD, FACSThe Alexander Whitehill Clowes MD Endowed Chair of Vascular Surgery
Professor of SurgeryChief, Division of Vascular Surgery
University of WashingtonSeattle, WA
Disclosures
• Co-Founder: AORTICA Corporation
Will the REAL Michael Conte please stand up!
Scientist Open Surgeon
Endovascular Surgeon
What do we know about Conte?
• Extremely Smart
• Very Charismatic
• Good Looking
• Fit
• Great Technical Surgeon
• Good Common Sense
April 6, 2017
Copyright UPM-Kymmene Group 2
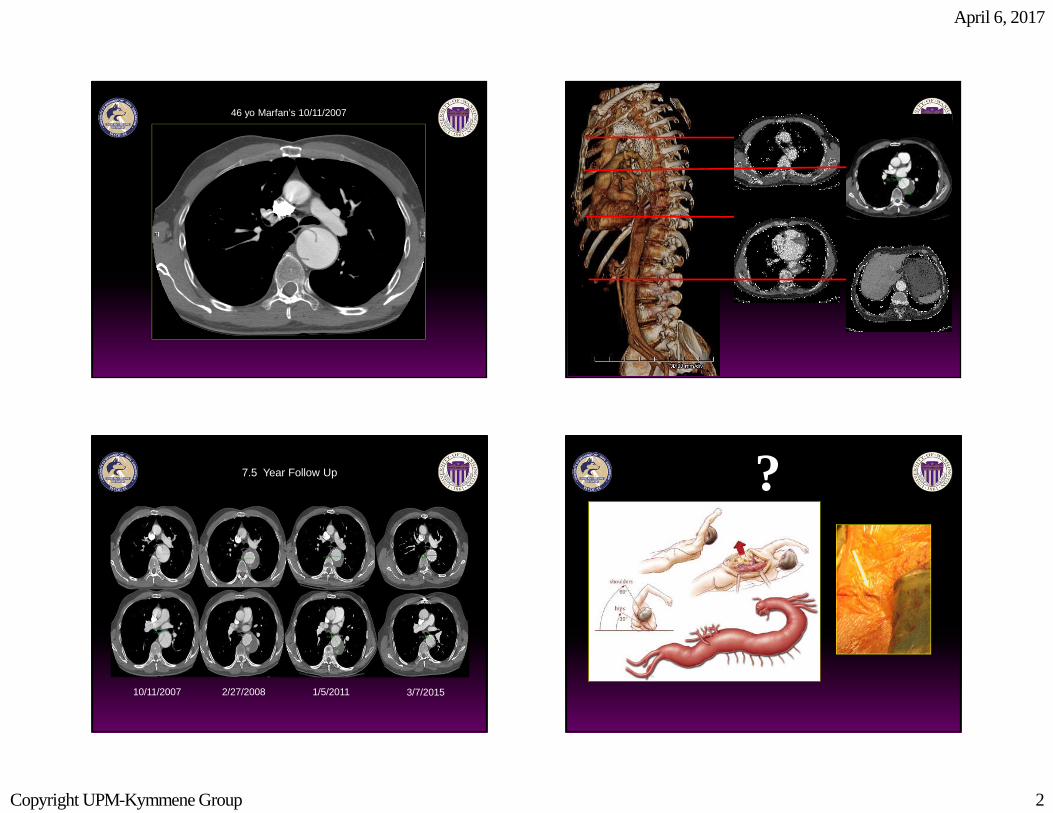
46 yo Marfan’s 10/11/2007
10/11/2007 2/27/2008 1/5/2011 3/7/2015
7.5 Year Follow Up ?
April 6, 2017
Copyright UPM-Kymmene Group 3
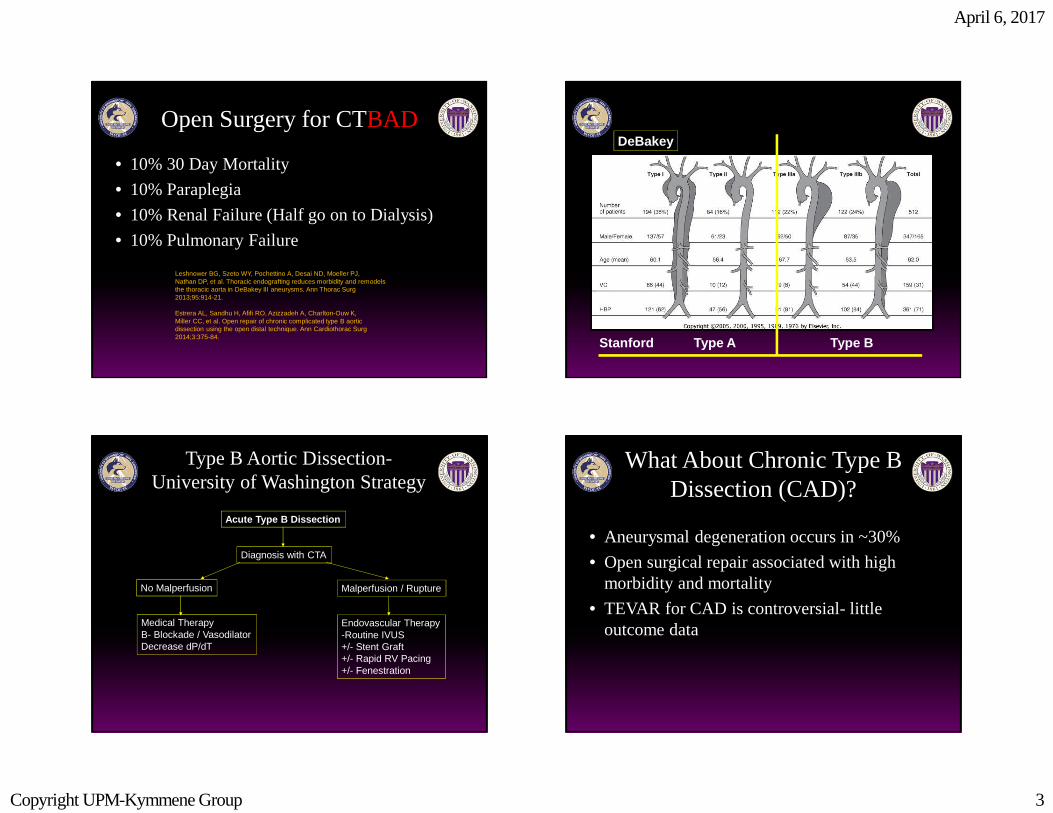
Open Surgery for CTBAD
• 10% 30 Day Mortality
• 10% Paraplegia
• 10% Renal Failure (Half go on to Dialysis)
• 10% Pulmonary Failure
Leshnower BG, Szeto WY, Pochettino A, Desai ND, Moeller PJ,Nathan DP, et al. Thoracic endografting reduces morbidity and remodelsthe thoracic aorta in DeBakey III aneurysms. Ann Thorac Surg2013;95:914-21.
Estrera AL, Sandhu H, Afifi RO, Azizzadeh A, Charlton-Ouw K,Miller CC, et al. Open repair of chronic complicated type B aorticdissection using the open distal technique. Ann Cardiothorac Surg2014;3:375-84.
Aortic Dissection- Classification
Stanford Type A Type B
DeBakey
Type B Aortic Dissection-University of Washington Strategy
Diagnosis with CTA
No Malperfusion
Medical TherapyB- Blockade / VasodilatorDecrease dP/dT
Malperfusion / Rupture
Endovascular Therapy-Routine IVUS+/- Stent Graft+/- Rapid RV Pacing+/- Fenestration
Acute Type B Dissection
What About Chronic Type B Dissection (CAD)?
• Aneurysmal degeneration occurs in ~30%
• Open surgical repair associated with high morbidity and mortality
• TEVAR for CAD is controversial- little outcome data
April 6, 2017
Copyright UPM-Kymmene Group 4
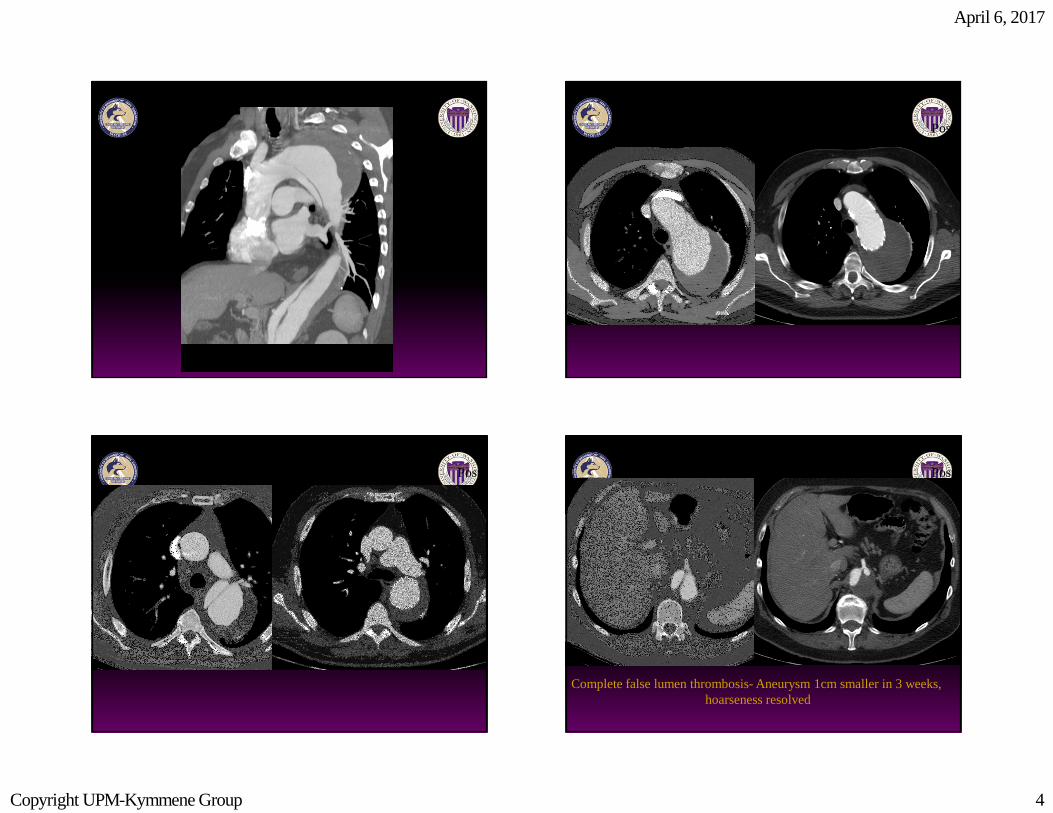
Pre Post
Pre Post Pre Post
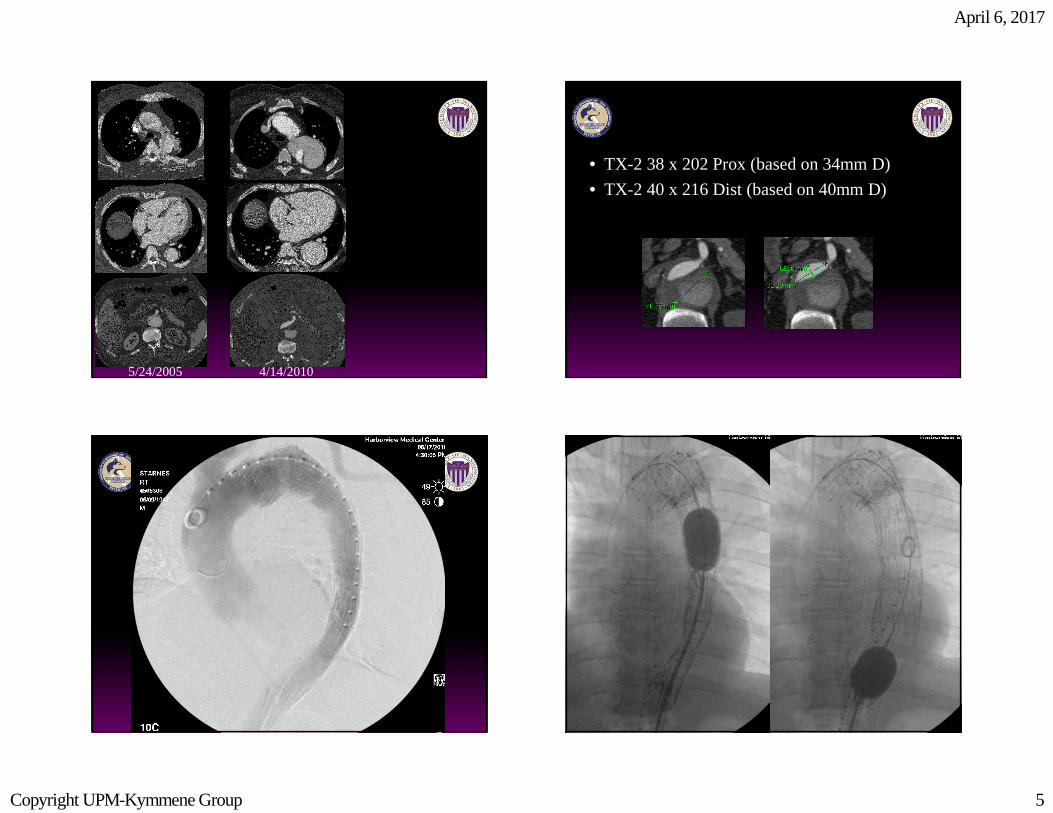
Complete false lumen thrombosis- Aneurysm 1cm smaller in 3 weeks, hoarseness resolved
April 6, 2017
Copyright UPM-Kymmene Group 5
5/24/2005 4/14/2010
• TX-2 38 x 202 Prox (based on 34mm D)
• TX-2 40 x 216 Dist (based on 40mm D)
April 6, 2017
Copyright UPM-Kymmene Group 6
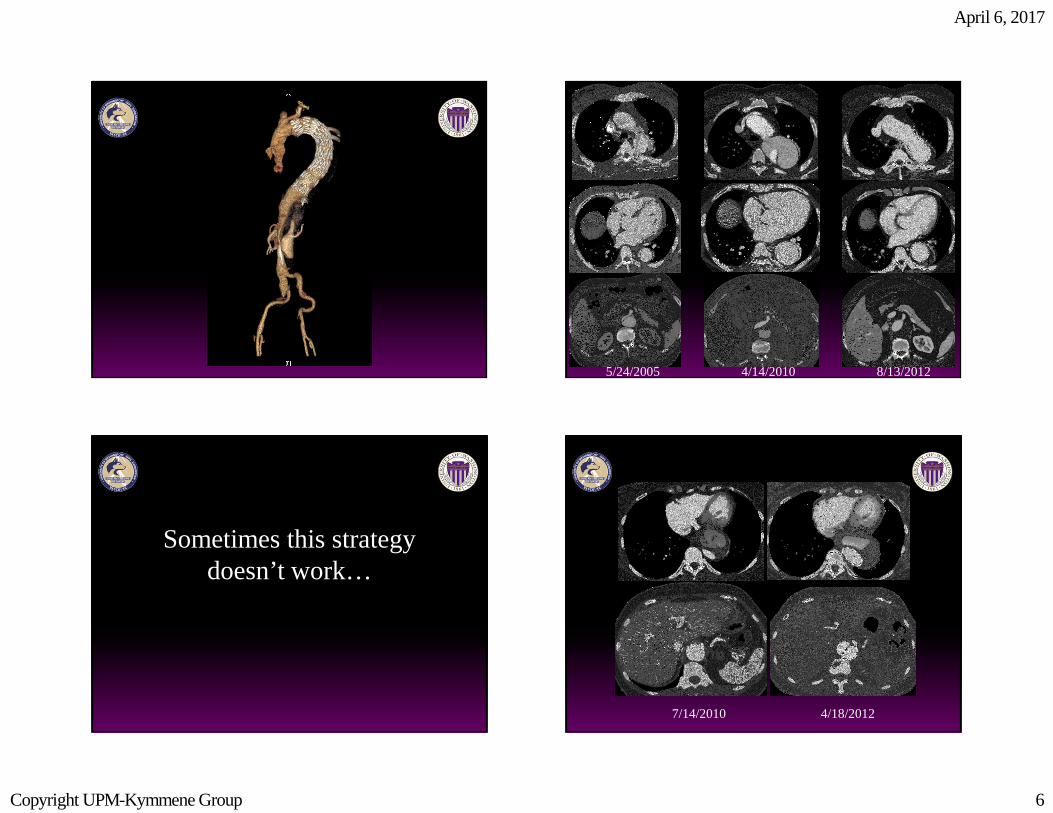
5/24/2005 8/13/20124/14/2010
Sometimes this strategy doesn’t work…
7/14/2010 4/18/2012
April 6, 2017
Copyright UPM-Kymmene Group 7
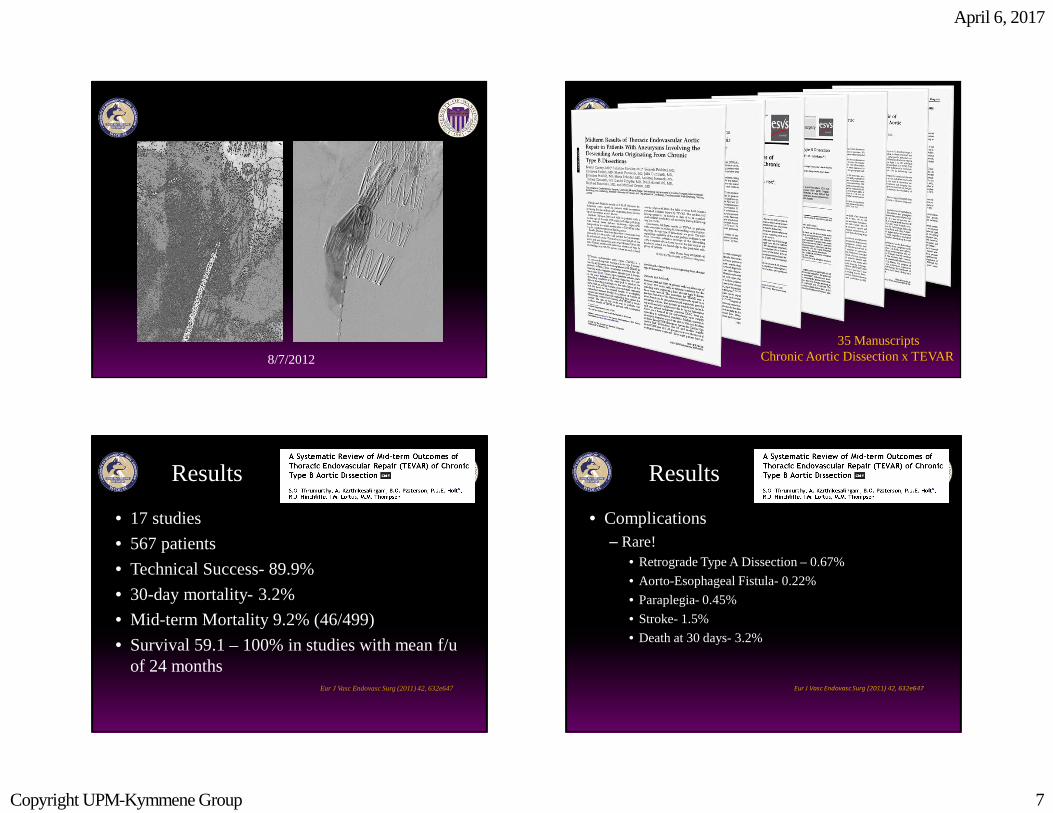
8/7/2012
35 ManuscriptsChronic Aortic Dissection x TEVAR
Results
• 17 studies
• 567 patients
• Technical Success- 89.9%
• 30-day mortality- 3.2%
• Mid-term Mortality 9.2% (46/499)
• Survival 59.1 – 100% in studies with mean f/u of 24 months
Eur J Vasc Endovasc Surg (2011) 42, 632e647
Results
• Complications– Rare!
• Retrograde Type A Dissection – 0.67%
• Aorto-Esophageal Fistula- 0.22%
• Paraplegia- 0.45%
• Stroke- 1.5%
• Death at 30 days- 3.2%
Eur J Vasc Endovasc Surg (2011) 42, 632e647
April 6, 2017
Copyright UPM-Kymmene Group 8
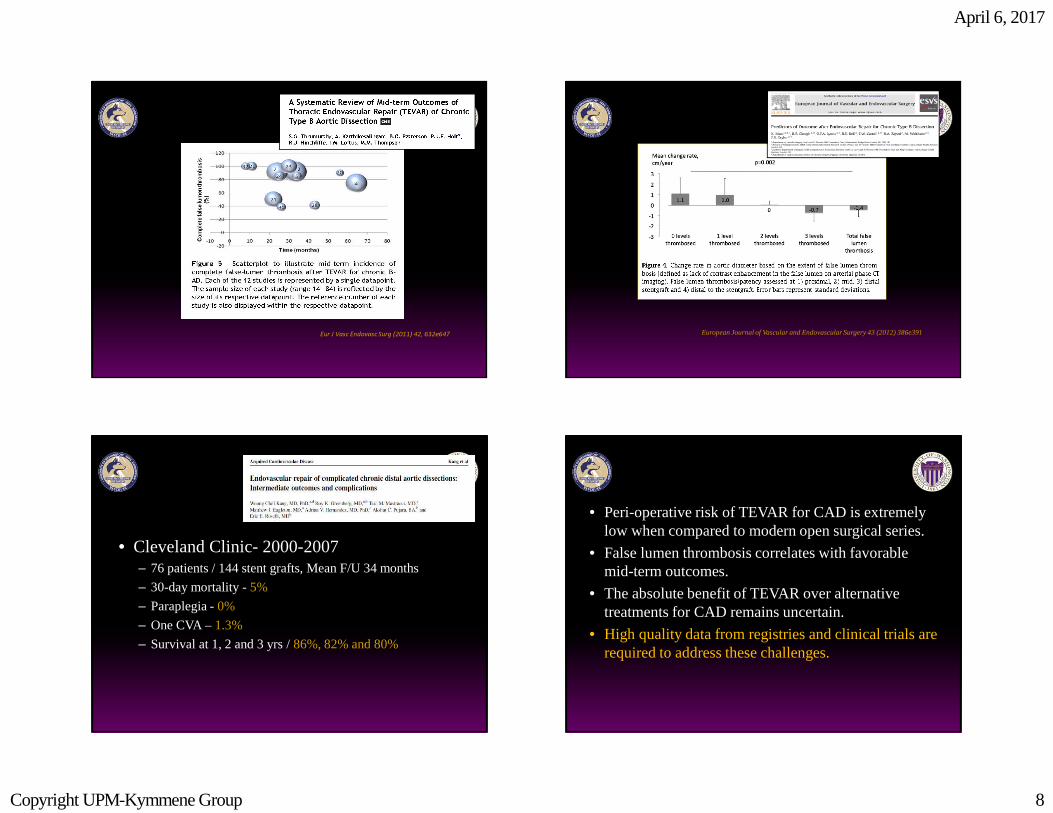
Eur J Vasc Endovasc Surg (2011) 42, 632e647 European Journal of Vascular and Endovascular Surgery 43 (2012) 386e391
• Cleveland Clinic- 2000-2007– 76 patients / 144 stent grafts, Mean F/U 34 months
– 30-day mortality -5%
– Paraplegia -0%
– One CVA –1.3%
– Survival at 1, 2 and 3 yrs / 86%, 82% and 80%
• Peri-operative risk of TEVAR for CAD is extremely low when compared to modern open surgical series.
• False lumen thrombosis correlates with favorable mid-term outcomes.
• The absolute benefit of TEVAR over alternative treatments for CAD remains uncertain.
• High quality data from registries and clinical trials are required to address these challenges.
April 6, 2017
Copyright UPM-Kymmene Group 9
TEVAR for CAD
• Methods:– Retrospective review of consecutive TEVARs for CAD
– 2008-2013
– Primary Outcome- 30 day Mortality
– Secondary Outcomes-• False Lumen Thrombosis
• Aneurysm Sac Shrinkage
• “Positive” Aortic Remodeling
TEVAR for CAD
• Results:– 45 TAA / CAD cases were treated with TEVAR
• 73% male
• Median Age 60 (37-71)
• Median time to presentation- 56 months
• Five cases secondary to Marfan’s
• Seven Type A CAD with previous ascending repair
• 38 Type B CAD
– Staged approach in 7 cases and Hybrid in 8
TEVAR for CAD- Results
• Adjunctive Procedures– Spinal Drainage (n=42)
– Left C-SCA Bypass (n=21)
• Proximal Landing Zone– Zone 2 (n=24)
– Zone 3 (n=21)
April 6, 2017
Copyright UPM-Kymmene Group 10
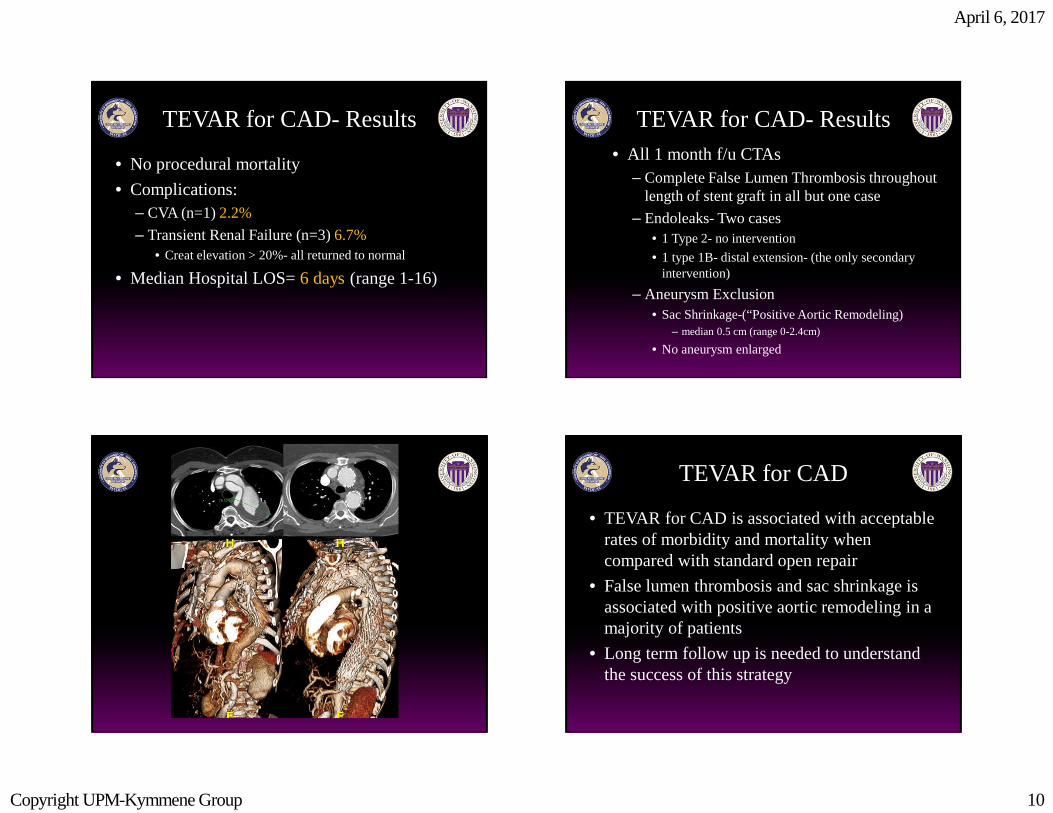
TEVAR for CAD- Results
• No procedural mortality
• Complications:– CVA (n=1) 2.2%
– Transient Renal Failure (n=3) 6.7%• Creat elevation > 20%- all returned to normal
• Median Hospital LOS= 6 days (range 1-16)
TEVAR for CAD- Results• All 1 month f/u CTAs
– Complete False Lumen Thrombosis throughout length of stent graft in all but one case
– Endoleaks- Two cases• 1 Type 2- no intervention
• 1 type 1B- distal extension- (the only secondary intervention)
– Aneurysm Exclusion• Sac Shrinkage-(“Positive Aortic Remodeling)
– median 0.5 cm (range 0-2.4cm)
• No aneurysm enlarged
TEVAR for CAD
• TEVAR for CAD is associated with acceptable rates of morbidity and mortality when compared with standard open repair
• False lumen thrombosis and sac shrinkage is associated with positive aortic remodeling in a majority of patients
• Long term follow up is needed to understand the success of this strategy
April 6, 2017
Copyright UPM-Kymmene Group 11
Will the REAL Michael Conte please stand up!
Scientist Open Surgeon
Endovascular Surgeon