the urinary system assessment & disorders
DESCRIPTION
The Urinary System Assessment & Disorders. The kidneys, ureters, and bladder. (Source: Dorling Kindersley Media Library). An illustration of the internal structures of the kidney. The structure of the nephron and the processes of urine formation. Age-Related Changes. Nephrons lost with aging - PowerPoint PPT PresentationTRANSCRIPT

The Urinary System Assessment & Disorders
1

The kidneys, ureters, and bladder. (Source: Dorling Kindersley Media Library)
2

An illustration of the internal structures of the kidney.
3
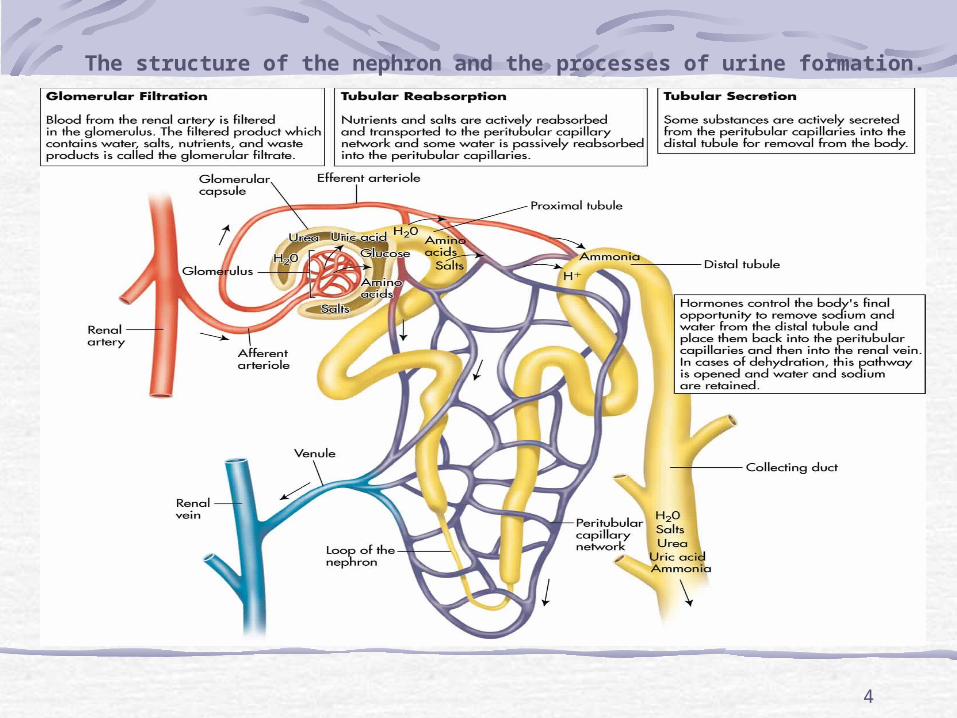
The structure of the nephron and the processes of urine formation.
4

5

Age-Related ChangesNephrons lost with aging
Reduces kidney mass and GFR
Less urine concentrationRisk for dehydration
6
AssessmentUse simple languageAssess for incontinence (esp. muliparous)Family historyChief concernLocation and character of painPrevious UTI, stones, urinary problemsPattern or urination
7

AssessmentColor, clarity, amount of urineDifficulty initiating urination or changes in streamChanges in urinary patternDysuria, nocturia, hematuria, pyuria
8

AssessmentHistory of urinary problemsUrinary or abdominal surgeriesSmoking, alcohol useChance of pregnancyHistory of diabetes or other endocrine disordersUnexplained anemia
9

Diagnostic TestsClean-catch urine24-hour urine collectionCulture and sensitivityBUN, creatinine and creatinine clearance = {Vol. of urine (ML/hr) x urine creatine}/serum creatinine IVP, Retrograde Pyelography
10

Diagnostic TestsCystography, voiding cystogramCT scan, MRIRenal scanUltrasound
X-ray (KUB)CystoscopyRenal AngiographyKidney biopsy (by needle or open procedure)
11

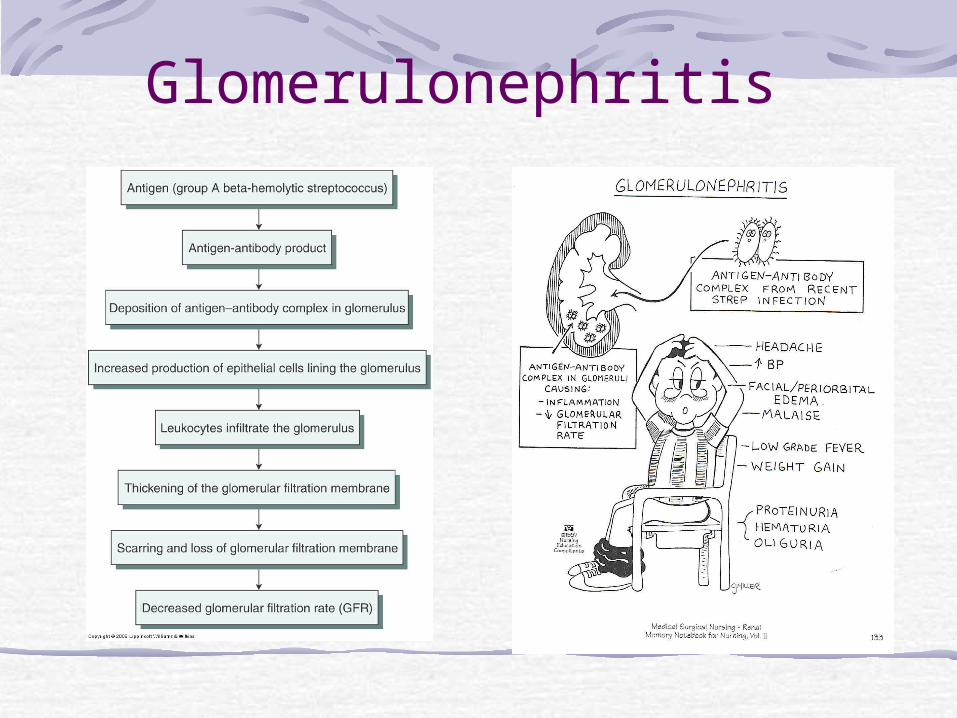
GlomerulonephritisInflammatory condition of glomerulusAntigen–antibody complexes form in the blood and become trapped in the glomerular capillaries, inducing an inflammatory response. Damages capillary membrane
Blood cells and proteins escape into filtrateHematuria, proteinuria, azotemia (increase BUN & Creatinin)
Acute or chronic
12
Acute Glomerulonephritis - Manifestations
Usually follows infection of group A beta-hemolytic StreptococcusAffect children > 2 yearsManifestations develop abruptly
Hematuria (? Microscopic, or frank, urine is cola color), proteinuria, edema, azotemia (High BUN and Creatineine) hypertension, fatigue, hypoalbuminemia, hyperlipidemia? headache, malaise and flank pain
13
Glomerulonephritis

Glomerulonephritis – Diagnostic Tests
ASO titer (anti streptolysine O)BUNSerum creatinine
Serum electrolytesUrinalysisKUB x-rayKidney scan or biopsy
15

Complications of acute glomerulonephritis
Hypertensive encephalopathy, Heart failure, Pulmonary edema,Without treatment, end-stage renal disease (ESRD) develops in a matter of weeks or months.
16
Glomerulonephritis – Treatment
Focus is on identifying and treating underlying disease process and preserving kidney functionIf residual streptococcal infection is suspected, penicillin. Corticosteroids and immunosuppressant medications may be prescribed for patients with rapidly progressive acute glomerulonephritis.
17

Glomerulonephritis –Treatment
Dietary protein is restricted when renal insufficiency (elevated BUN) develop. Sodium is restricted when the patient has hypertension, edema, and heart failure. Loop diuretic and antihypertensive medications may be prescribed to control hypertension. Bed rest during acute phase.18

Glomerulonephritis –Nursing Care
Decrease protein and increase CHO to prevent protein breakdown.Accurate I & O (consider insensible loss)
19

Chronic Glomerulonephritis
Could be due to repeated episodes of acute glomerulonephritis, hypertensive nephrosclerosis, hyperlipidemia, glomerular sclerosisOther causes include SLE, DMKidney size reduce to 1/5th of original size and many scar tissue formed leading to ESRF.
20

Chronic Glomerulonephritis/ S&S
Many are asymptomatic? Discovered when patient diagnosed with Hypertension.? severe nosebleed, a stroke, or a seizure, swollen feet at night. Heneral symptoms, such as loss of weight and strength, increasing irritability, nocturia, Headaches, dizziness, and digestive disturbances.Finally, S&S of renal failure.
21

Medical Management
Control BP: Na & water restriction, antihypertensive drugMonitor weight.Diuretics. Adequate CHO diet to spare protienTreat UTI? Dialysis.
22

Nephrotic Syndrome
Is a cluster of clinical findings, including:1. Marked increase in protein
(particularly albumin) in the urine (proteinuria)
2. Decrease in albumin in the blood (hypoalbuminemia)
3. Edema (periorbital, ascites, and dependent edema)
4. High serum cholesterol and low-density lipoproteins (hyperlipidemia)
23

Treatment Diuretics (be careful not to cause sever hypovolemia as it may lead to ARF)Loop diuretics + ACE inhibitors lead to decreasing protienuria. Immunosuppresive agents (i.e. cytoxan).Coriticosteroids.
Restrict protein and sodium.
24

Nephrotic Syndrome

Acute Renal Failure (ARF)Is a reversible clinical syndrome where there is a sudden and almost complete loss of kidney function (decreased GFR) over a period of hours to days with failure to excrete nitrogenous waste products and to maintain fluid and electrolyte homeostasisMay progress to end stage renal disease, uremic syndrome, and death without treatment
26

Acute Renal FailurePersons at Risks
Major surgeryMajor traumaReceiving nephrotoxic medicationsElderly
ARF mostly occur within hospital settings
27

Causes of ARF
1. Prerenal Failure
2. Intrarenal Failure
3. Postrenal Failure
28

Prerenal Failure
Volume depletion resulting from:HemorrhageRenal losses (diuretics, osmotic diuresis)Gastrointestinal losses (vomiting, diarrhea, nasogastric suction)
Impaired cardiac efficiency resulting from:
Myocardial infarctionHeart failureDysrhythmiasCardiogenic shock
29

Prerenal FailureVasodilation resulting from:
SepsisAnaphylaxisAntihypertensive medications or other medications that cause vasodilation
30
Intrarenal Failure
Prolonged renal ischemia resulting from:Pigment nephropathy (associated with the break-down of blood cells containing pigments that in turn occlude kidney structures)Myoglobinuria (trauma, crush injuries, burns)Hemoglobinuria (transfusion reaction, hemolytic anemia)
31

Intrarenal FailureNephrotoxic agents such as:
Aminoglycoside antibiotics (gentamicin, tobramycin, amicacin)Radiopaque contrast agentsHeavy metals (lead, mercury)Solvents and chemicals (ethylene glycol, carbon tetrachloride, arsenic)Nonsteroidal anti-inflammatory drugs (NSAIDs)Angiotensin-converting enzyme inhibitors (ACE inhibitors)
32

Intrarenal FailureInfectious processes such as:
Acute pyelonephritisAcute glomerulonephritis
33

Postrenal failure
Urinary tract obstruction, including:
Calculi (stones)TumorsBenign prostatic hyperplasiaStricturesBlood clots
34

Phases of Acute Renal Failure
Initiation period: begins with the initial insult and ends when oliguria develops. Oliguria period: UOP < 400 ml/day, increase in urea, creatinine, uric acid, K & magnesium. Some people have normal urine output (2 L/d)Diuretic – UOP ^ to as much as 4000 mL/d but BUN & Cretinine still high, at end of this stage may begin to see improvement Recovery – things go back to normal. It may take up to 3-12 months
35
Acute Renal Failure S & SThe patient may appear critically ill and lethargic. The skin and mucous membranes are dry from dehydration. Central nervous system signs and symptoms include drowsiness, headache, muscle twitching, and seizures.Urine output varies (scanty to normal volume), ? hematuria & urine has a low specific gravity
36

Acute Renal FailureDiagnostic tests
BUN, creatinine, potassium increase. pHHgb and HctUrine studiesUS of kidneysHigh phosphorus and low calcium.
37

Prevention of ARF
Provide adequate hydrationPrevent and treat shock promptlyHourly urine output for critical patientsContinuosally assess renal functionPrevent and treat infections promptlyMonitor for effects of toxic drugs
38

Medical treatment of ARFObjectives of treatment are to restore normal chemical balance and prevent complications until repair of renal tissue and restoration of renal function can occur.Management includes
maintaining fluid balance, avoiding fluid excesses, or possibly performing dialysis.
39

Acute Renal FailureMedical treatment
Treat the causeFluid and replacement or restrictionsMonitor for fluid overloadDiuretics Maintain E-lytes May need dialysis (especially with high K)May need to stimulate production of urine with IV fluids, Dopomine, diuretics, etc.
40

Acute Renal FailureMedical treatment
HemodialysisSubclavian approachFemoral approach
Peritoneal dialysisNutritional Therapy
? Decrease Protein (according to BUN level)Increase CHODecrease potassium and phosphrous
41

Acute Renal Failure
Nursing Diagnosis-imbalanced fluid volume= excessAltered electrolyte balanceImpaired tissue perfusion: renalAnxiety Imbalanced nutritionRisk for infectionFatigue Knowledge deficit
42
Acute Renal Failure
Plan-Promote recovery of optimal kidney function.Maintain normal fluid and electrolyte balance.Decrease anxiety.Increase knowledge.
43

Nursing interventions
Monitoring Fluid and Electrolyte BalanceReducing Metabolic RatePromoting Pulmonary FunctionPreventing InfectionProviding Skin Care
44

Chronic Renal FailureChronic renal failure, or ESRD, is a progressive, irreversible deterioration in renal function in which the body's ability to maintain metabolic and fluid and electrolyte balance fails, resulting in uremia or azotemia.Results from gradual, progressive loss of renal functionOccasionally results from rapid progression of acute renal failure
45

Chronic Renal FailureConditions that cause ESRD include systemic diseases, such as diabetes mellitus (leading cause); hypertension; chronic glomerulonephritis; pyelonephritis; obstruction of the urinary tract; hereditary lesions, as in polycystic kidney disease; vascular disorders; infections; medications; or toxic agents.
46

Chronic Renal FailureSymptoms occur when 75% of function is lost but considered chronic if 90-95% loss of functionDialysis is necessary D/T accumulation of uremic toxins, which produce changes in major organs
47
Chronic renal failure/ S&SCardiovascular: the most common cause of death
HypertensionPitting edema (feet, hands, sacrum)Periorbital edemaPericardial friction rubAcidosis (kidney can’t excrete amonia, reabsorb bicarb, high phosphate)
Engorged neck veinsPericarditisPericardial effusionPericardial tamponadeHyperkalemiaHyperlipidemia
48

Chronic renal failure/ S&S Neurologic
Weakness and fatigueConfusionInability to concentrateDisorientationTremors
SeizuresAsterixisRestlessness of legsBurning of soles of feetBehavior changes
49
Chronic renal failure/ S&S Pulmonary Integumentary
CracklesThick, tenacious sputumDepressed cough reflexPleuritic painShortness of breathTachypneaKussmaul-type respirationsUremic pneumonitis
Gray-bronze skin colorDry, flaky (ر TقّشWُم) skinPruritusEcchymosisPurpuraThin, brittle nailsCoarse, thinning hair
50
Chronic renal failure/ S&S Gastrointestinal
HematologicAmmonia odor to breath (“uremic fetor”)Metallic taste
Mouth ulcerations and bleeding
Anorexia, nausea, vomiting
HiccupsConstipation or diarrhea
Bleeding from GI tract
AnemiaThrombocytopenia
51

Chronic renal failure/ S&S Reproductive Musculoskeletal
AmenorrheaTesticular atrophyInfertilityDecreased libido
Muscle crampsLoss of muscle strengthRenal osteodystrophyBone painBone fracturesFoot drop
52

53

Chronic Renal FailureLab findings
BUN – indicator of glomerular filtration rate and is affected by the breakdown of protein. Serum creatinine – waste product of skeletal muscle breakdown and is a better indicator of kidney function. Creatinine clearance is best determent of kidney function (GFR). Must be a 24 hour urine collection.
54

Chronic Renal FailureK+
The kidneys are means which K+ is excreted. Normal is 3.5-5.0 ,mEq/L. maintains muscle contraction and is essential for cardiac function. Both elevated and decreased can cause problems with cardiac rhythmHyperkalemia is treated with IV glucose and Na Bicarb which pushes K+ back into the cellKayexalate (Sodium polystyrene sulfonate ) is also used to promote the exchange of sodium and potassium in the body.
55

Chronic Renal FailureCa
With disease in the kidney, the enzyme for utilization of Vit D is absentCa absorption depends upon Vit DAlso, phosphate level increase leading to decreasing level of CaParathyroid hormone level increase in attempt to increase calcium, but because of the high phosphorus level, there is limited response. Body moves Ca out of the bone to compensate.Renal osteodystrophy is the end result
Hypocalcemia = tetany
56

Chronic Renal Failure
Other abnormal findingsMetabolic acidosisFluid imbalanceInsulin resistanceAnemiaImmunoligical problems
57

Complications
HyperkalemiaPericarditis, pericardial effusion, and pericardial tamponadeHypertensionAnemiaBone disease and metastatic and vascular calcifications
58

Medical management Calcium carbonate, or calcium acetate: bind to phosphours and decrease its level. Antihypertensive and Cardiovascular AgentsAntiseizure AgentsErythropoietin
59

Nutritional TherapyProtein is restricted (allowed protein should be of high biologic value)Restrict fluid (500-600 ml/day more than previous day’s urine output).Restrict K, Na, PhosphorusIncrease CHO to meat caloric needsVitamin suplements
60

Treatment Dialysis Transplantation
61

Chronic Renal FailureNursing diagnosis
Excess fluid volume related to decreased urine output, dietary excesses, and retention of sodium and waterImbalanced nutrition: less than body requirements related to anorexia, nausea and vomiting, dietary restrictions, and altered oral mucous membranes
62

Nursing diagnosis
Deficient knowledge regarding condition and treatment regimenActivity intolerance related to fatigue, anemia, retention of waste products, and dialysis procedureRisk for situational low self-esteem related to dependency, role changes, changes in body image, and sexual dysfunction
63

Chronic Renal FailureNursing care : see world document
64

DialysisDialysis is used to remove fluid and uremic waste products from the body when the kidneys are unable to do so.Chronic: in ESRF when the kidney can’t remove waste products. Acute: high level of serum K+, fluid overload, or impending pulmonary edema, acidosis, to remove certain medications or other toxins from the blood.
65
Dialysis½ of patients with CRF eventually require dialysisDiffuse harmful waste out of bodyControl BPKeep safe level of chemicals in body2 types
HemodialysisPeritoneal dialysis
66

Principles for dialysis Diffusion: toxins and wastes in the blood are removedOsmosis: excess water is removed from the bloodUltrafiltration: helps water to move faster under high pressure to an area of lower pressure
67
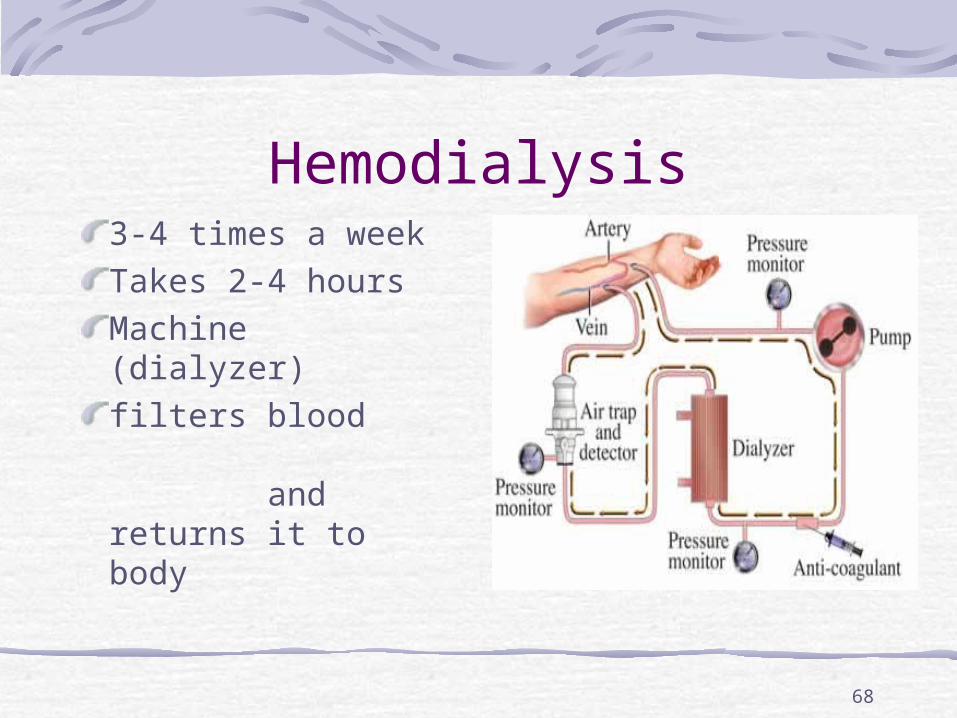
Hemodialysis3-4 times a weekTakes 2-4 hours Machine (dialyzer)filters blood and returns it to body
68

Chronic Renal FailureHemodialysis
Vascular accessTemporary – subclavian or femoralPermanent – shunt, in arm
Care post insertion
Can be done rapidlyTakes about 4 hoursDone 3 x a week
69

Types of AccessTemporary site: subclavian or femoralPermanent: shunt, in armAV fistula
Surgeon constructs by combining an artery and a vein3 to 6 months to matureAV graft
70

What This Means For YouNo BP on same arm as fistulaProtect arm from injuryNever inject anything into catheterControl obvious hemorrhage
Bleeding will be arterialMaintain direct pressure
No IV on same arm as fistulaA thrill will be felt – this is normal
71

Complication of dialysis HypotensionPainful muscle cramping (due to rapid alterations in electrolyte balance)Dysrhythmias may result from electrolyte and pH changes Air embolism Dialysis disequilibrium results from cerebral fluid shifts.
72

Peritoneal Dialysis
73

Peritoneal Dialysis
Abdominal lining filters blood3 types
Continuous ambulatoryContinuous cyclicalIntermittent
74

Dialysis
Peritoneal dialysisSemipermeable membraneCatheter inserted through abdominal wall into peritoneal cavityCost lessFewer restrictionsCan be done at homeRisk of peritonitis3 phases – inflow, dwell and outflow
Automated peritoneal dialysis
Done at home at nightMaybe 6-7 times /week
CAPDContinous ambulatory peritoneal dialysisDone as outpatientUsually 4 X/d
75

Chronic Renal Failure
TransplantMust find donorWaiting period longGood survival rate – 1 year 95-97%Must take immunosuppressant’s for lifeRejection
Watch for fever, elevated B/P, and pain over site of new kidney
76

77

Chronic Renal FailurePost op care
ICUI/OB/PWeight changesElectrolytesMay have fluid volume deficitHigh risk for infection
78

Transplant MedsPatients have decreased resistance to infectionCorticosteroids – anti-inflammarory
DeltosoneMedrolSolu-Medrol
Cytotoxic – inhibit T and B lymphocytesImuranCytoxanCellcept
T-cell depressors - Cyclosporin
79

Renal Trauma? due to rib fractures or fractures vertebrae.80% to 90% of all renal injuries are blunt injuriesS & S: Pain, hematouria, S & S of shockRx: Bed rest, antibiotics. In sever cases, need surgical repair or ? Nephrectomy.
80