congenital genito urinary disorders
TRANSCRIPT
CONGENITAL GENITO URINARY DISORDERS
introduction
Disorders of kidney and urinary tract are commonly seen in pediatric units as medical and surgical problems.
Incidence: 3 to 6 per 1000 live births
Congenital abnormalities of the kidney and urinary tract
These problems usually required surgical correction.
Some of them are producing no clinical symptoms.
25% cases of CRF are due to congenital anomalies
8 to 10 % of children affected with congenital anomalies of urinary tract.

enKidney and Ureter Bladder and
Urethra•Renal agenesis•Renal hypoplasia•Horse-shoe kidney•Poly cystic renal disease•Ectopic kidney•Duplication of renal pelvis and ureter•Hydronephrosis•Pelvi-ureteric obstruction•Congenital renal neoplasm•ureterocele
•Ectopia vesicaehus•Patent urachus•Bladder and neck obstruction•Posterior urethral valves•Neurogenic bladder•Hypospadias•Epispadias•Phimosis•Urethral stenosis•Meatal stenosis
Renal agenesis
Definition :It is the absence of kidney due to failure of ureteric bud formation.
Type: Bilateral Unilateral
Renal hypoplasia and dysplasia
it occurs due to reduction of renal mass affecting the nephron.
It may be unilateral or bilateralIt may be segmental, simpleRENAL DYSPLASIA :Disorganization of lung parenchyma with
immature nephron and ductal elements resulting in large or small kidney.
It may be multicystic , hypo plastic or aplastic
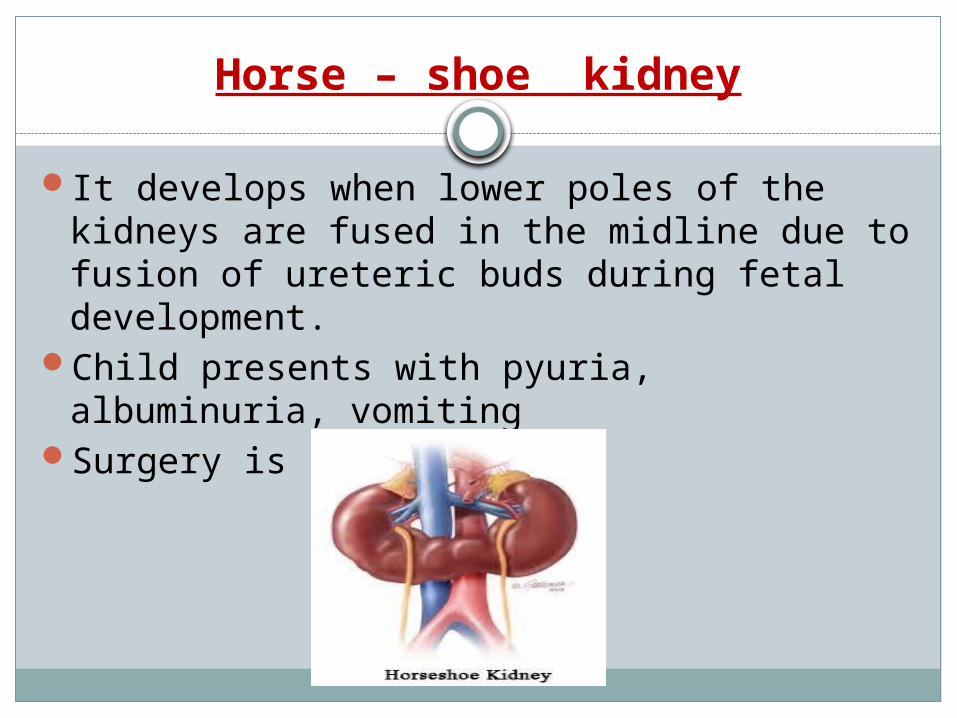
Horse – shoe kidney
It develops when lower poles of the kidneys are fused in the midline due to fusion of ureteric buds during fetal development.
Child presents with pyuria, albuminuria, vomiting
Surgery is indicated
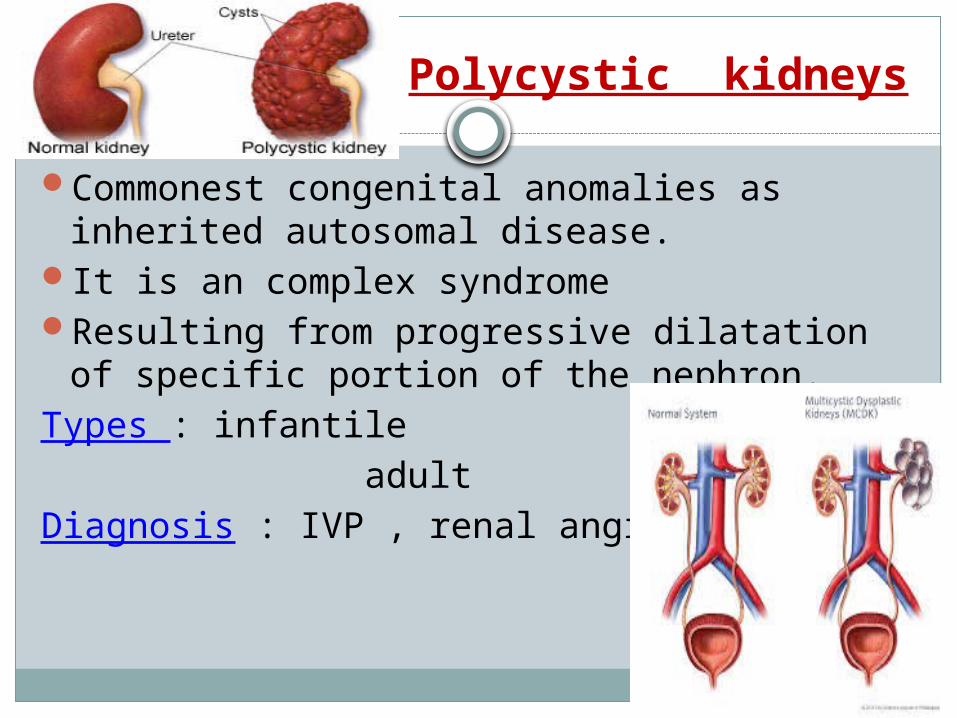
Polycystic kidneys
Commonest congenital anomalies as inherited autosomal disease.
It is an complex syndromeResulting from progressive dilatation of
specific portion of the nephron.Types : infantile adult Diagnosis : IVP , renal angiography
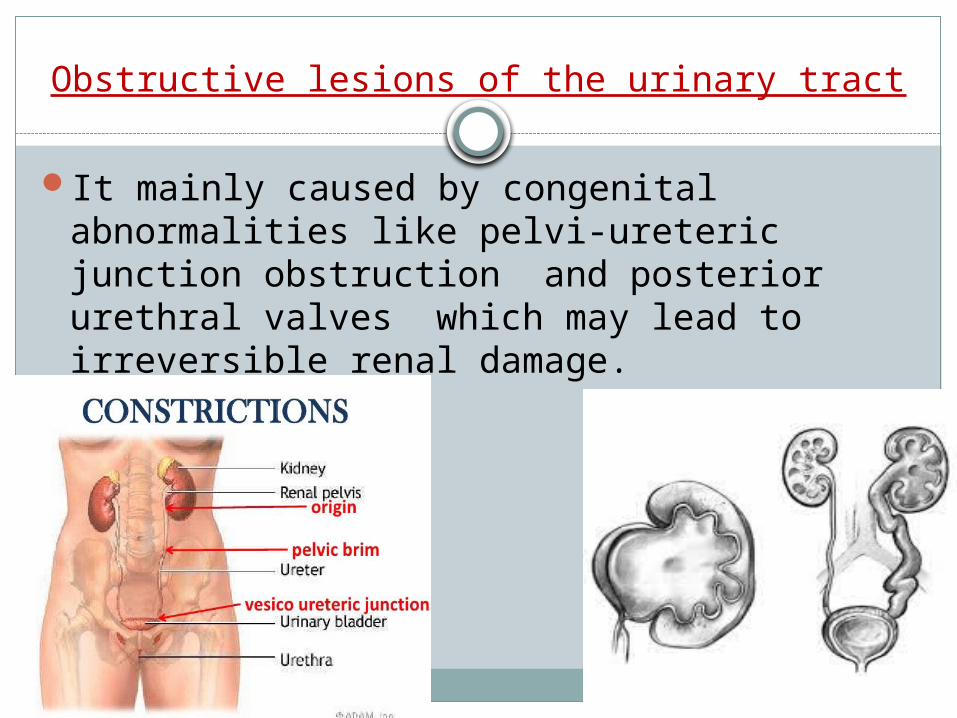
Obstructive lesions of the urinary tract
It mainly caused by congenital abnormalities like pelvi-ureteric junction obstruction and posterior urethral valves which may lead to irreversible renal damage.
Pelvi – ureteric junction stenosis
Unilateral or bilateralUrinary tract infections and upper abdominal
painDiagnosis : ultrasound, IVP , renal function test
Management:Surgery is indicated for removal of
obstruction
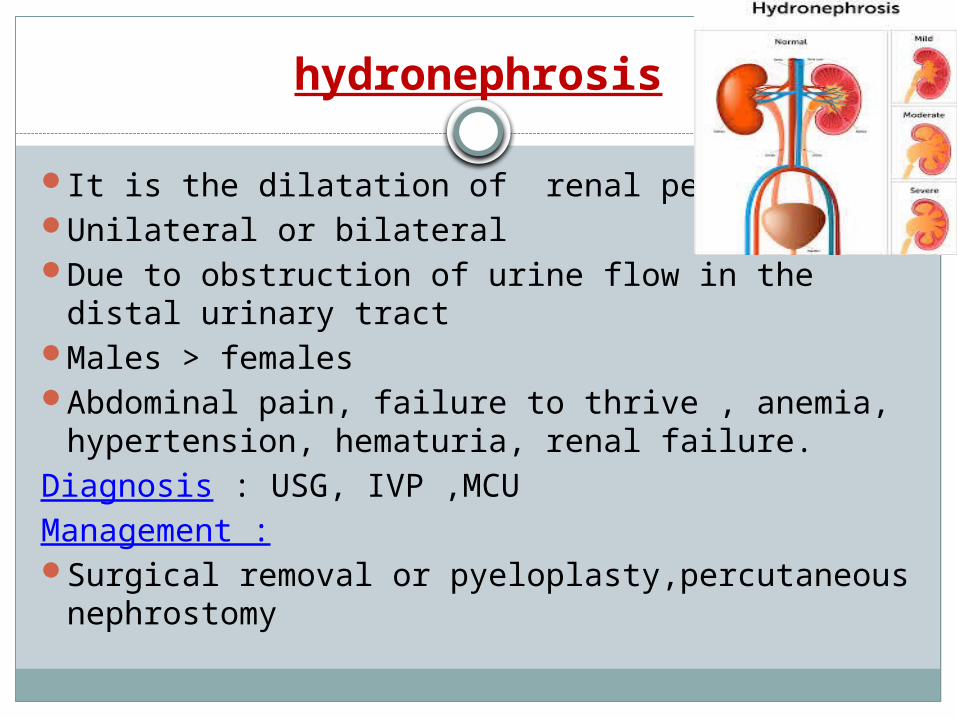
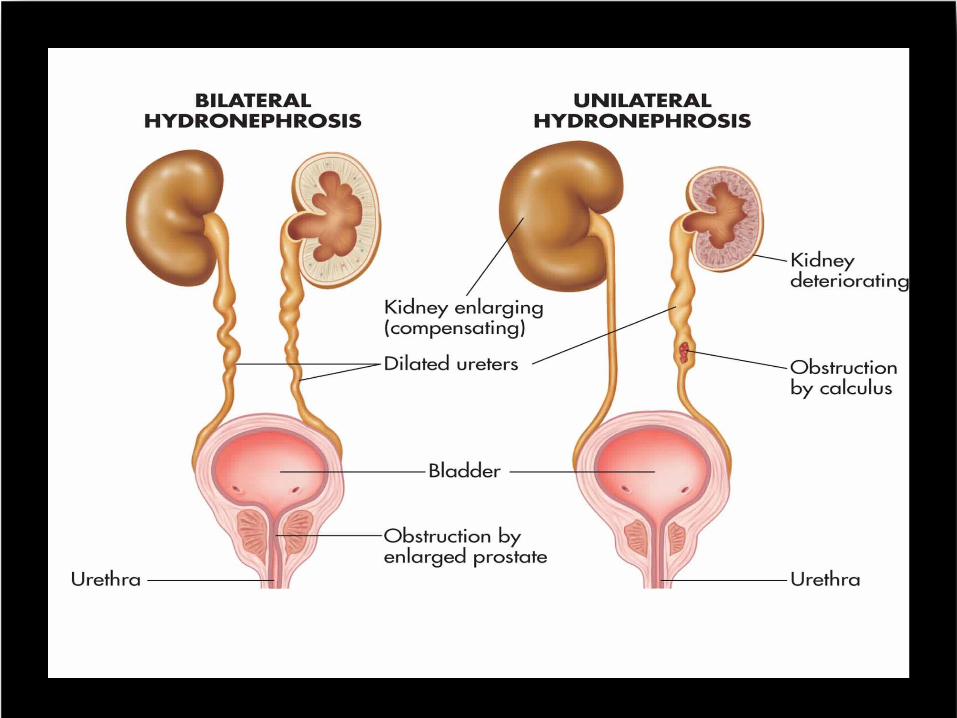
hydronephrosis
It is the dilatation of renal pelvisUnilateral or bilateralDue to obstruction of urine flow in the distal
urinary tractMales > femalesAbdominal pain, failure to thrive , anemia,
hypertension, hematuria, renal failure.Diagnosis : USG, IVP ,MCUManagement :Surgical removal or pyeloplasty,percutaneous
nephrostomy
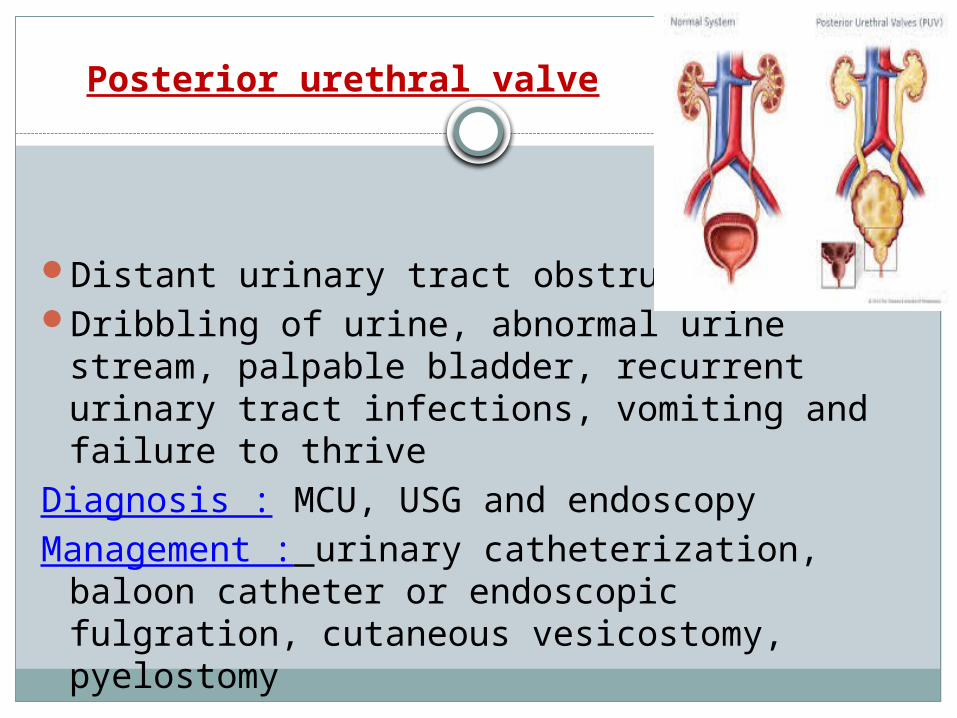
Posterior urethral valve
Distant urinary tract obstructionDribbling of urine, abnormal urine stream,
palpable bladder, recurrent urinary tract infections, vomiting and failure to thrive
Diagnosis : MCU, USG and endoscopyManagement : urinary catheterization, baloon
catheter or endoscopic fulgration, cutaneous vesicostomy, pyelostomy
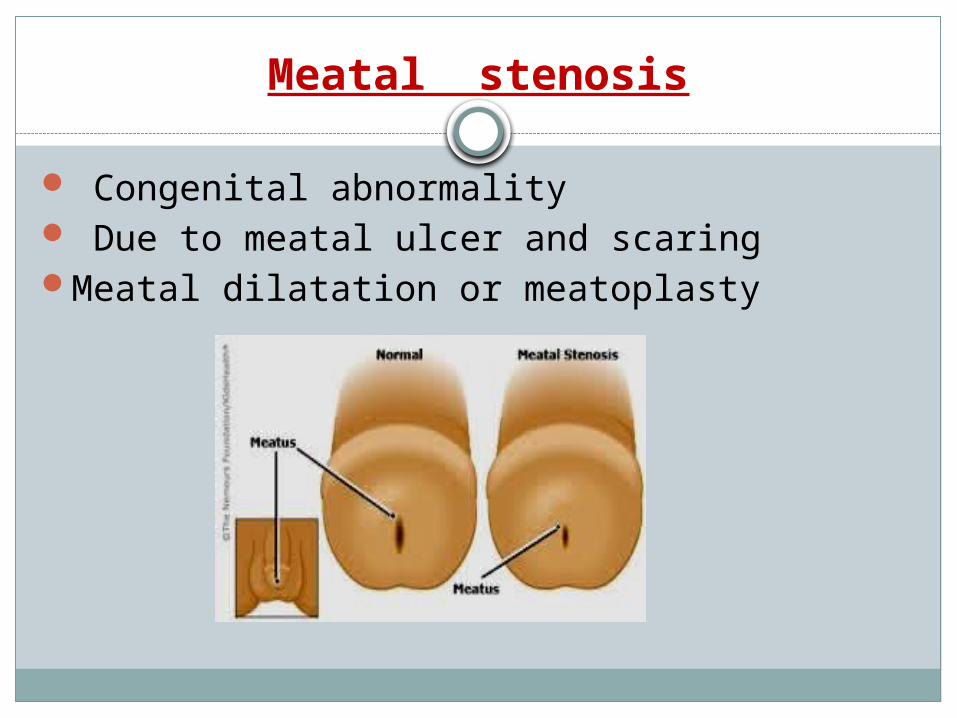
Meatal stenosis
Congenital abnormality Due to meatal ulcer and scaringMeatal dilatation or meatoplasty

Exstrophy of bladder( ectopia vesicae)
It is a congenital malformationLower portion of the abdominal wall and the
anterior wall of the bladder are missing so that bladder is everted through the opening and may found on the lower abdomen with continuous passage of urine to the outside.
Male are more commonly affected
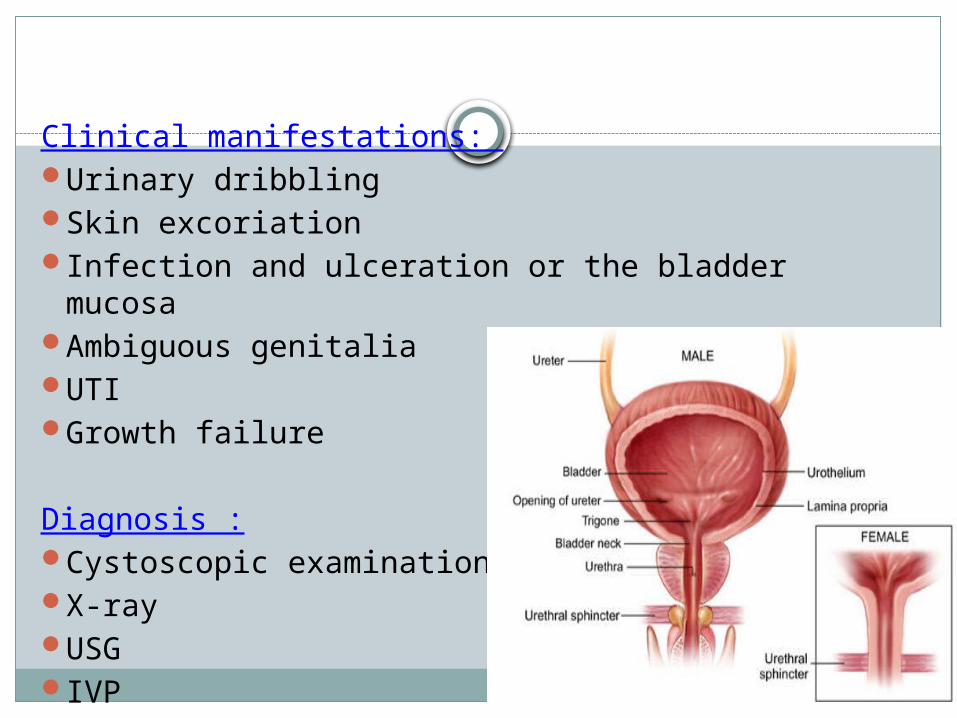
Clinical manifestations: Urinary dribblingSkin excoriationInfection and ulceration or the bladder mucosaAmbiguous genitaliaUTIGrowth failure
Diagnosis :Cystoscopic examinationX-rayUSGIVP
Management :Surgical closure of the bladder within 48
hoursUrinary conversion before reconstructive
surgeryOrthopedic surgerySupportive nursing carePre operative carePost operative careFollow up
epispadias
Abnormal urethral opening on the dorsal aspect of penis.
Due to abnormal development of the infraumbilical wall and upper wall of urethra.
Rare in femalesClassification : anterior epispadias posterior epispadias female epispadias – bifid clitoris subsymphyseal with
incontinence of urine
Management : surgical correction1. 1.5 to 2 years of age for penile lengthening,
elongation of urethral strip and chordee correction.
2. operation done at least 6 months after first stage for urethral reconstruction
3. 3 to 4 years of age for bladder neck reconstruction and correction of VUR
Cystoplasty Supportive nursing care
hypospadias
it is the congenital abnormal urethral opening on the ventral aspect( under surface ) of the penis.
Common in male children.Classification : Anterior hypospadias(65 to 70%) : it may found
as glandular or coronal or on distal penile shaftMiddle (10-15%) penile shaft hypospadias.Posterior hypospadias(20%) : it may be found on
proximal penile shaft or as penoscrotal,scortal or perineal type.

Problems related to hypospadias :1. Painful downward curvature of penis2. Deflected stream of urine3. Inability void urine while standingManagement : surgical reconstruction Meatotomy Chordee correction urethroplasty
phimosis
Narrow opening of the prepuce that prevents it being drawn back over the glans penis.
Management:Circumcision apply Betamethasone cream
paraphimosis
It is the retraction of a phimotic foreskin, behind coronal sulcus.
It may develop phimotic child which also need for surgical management by circumcision or reduction with application of lubricant under deep sedation.
Clinical features : edematousSevere pain
Wilm’s tumor (nephroblastoma)
Max wilm’s , German surgeon described this most common renal tumor of childhood.
Chromosomal deletions 11 and 16Highly malignant embryonal tumorTumor develops in kidney parenchyma ,invading the
surrounding tissues.Clinical features :abdominal massMicroscopic hematuriaFeverPallorSuperficial vein engorgement
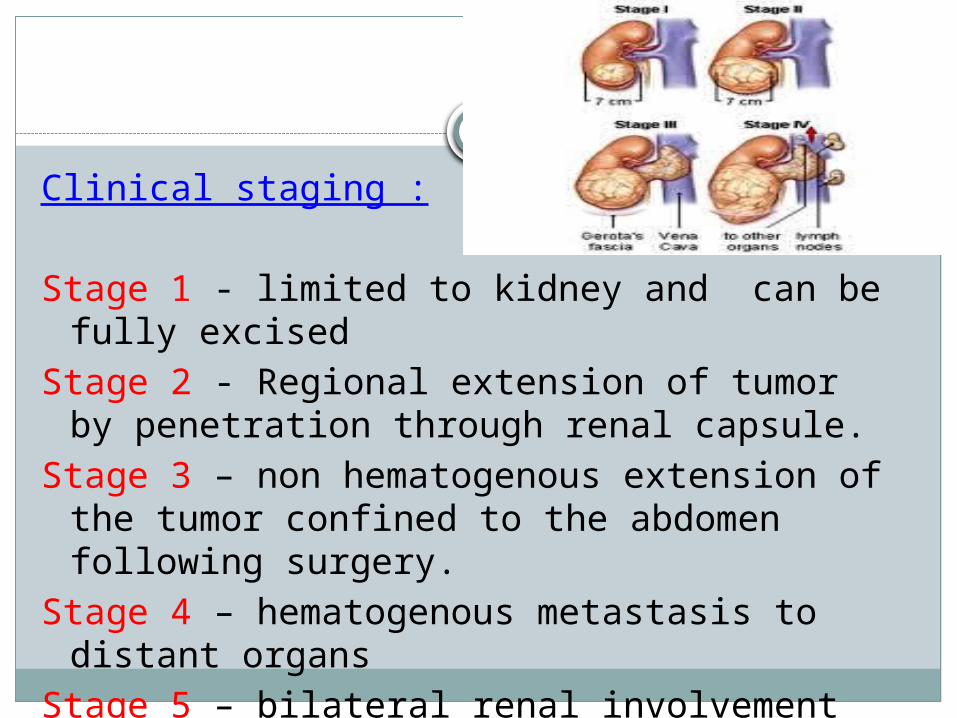
Clinical staging :
Stage 1 - limited to kidney and can be fully excised
Stage 2 - Regional extension of tumor by penetration through renal capsule.
Stage 3 – non hematogenous extension of the tumor confined to the abdomen following surgery.
Stage 4 – hematogenous metastasis to distant organs
Stage 5 – bilateral renal involvement
Diagnostic evaluation :HistoryPhysical examinationX-ray abdomen ,chestUSGCT scanMRIRenal function testManagement :NephrectomyChemotherapyradiotherapy
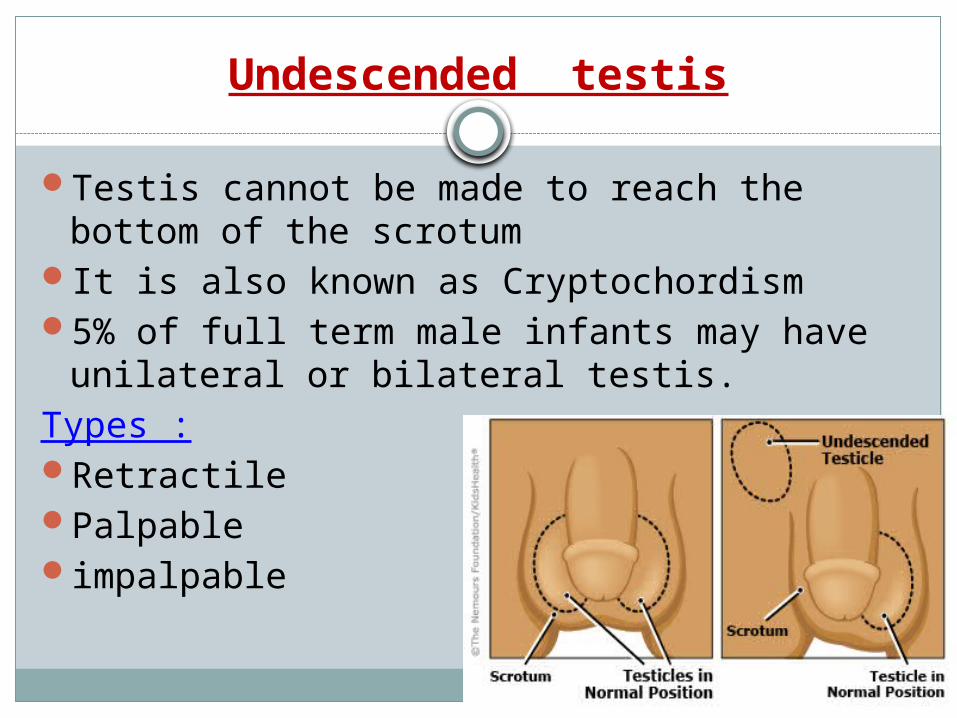
Undescended testis
Testis cannot be made to reach the bottom of the scrotum
It is also known as Cryptochordism 5% of full term male infants may have
unilateral or bilateral testis.Types :RetractilePalpableimpalpable
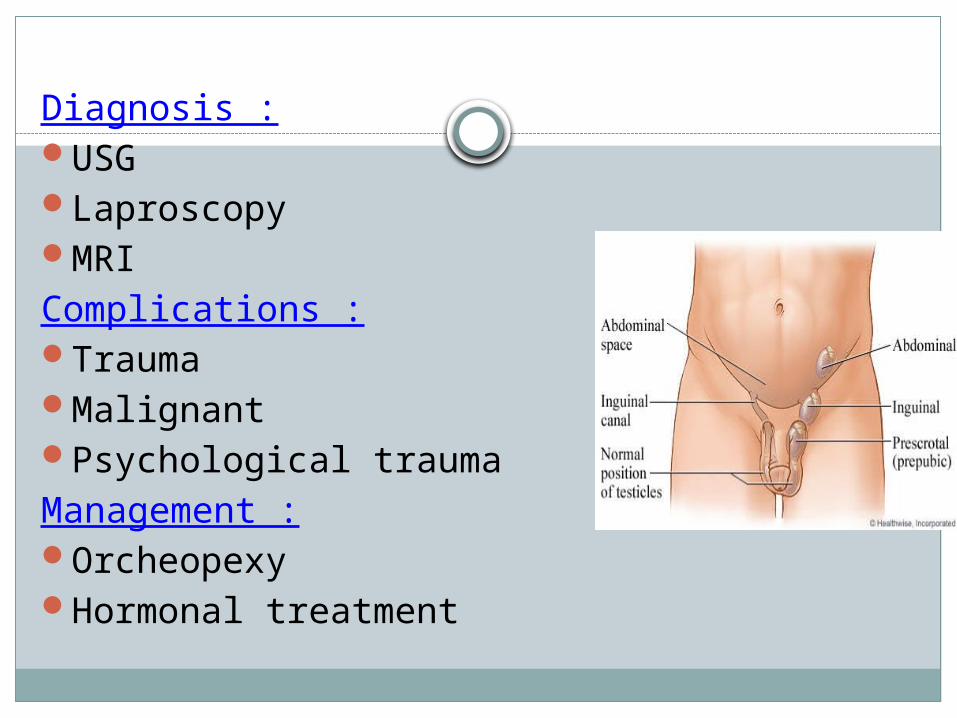
Diagnosis :USGLaproscopyMRIComplications :TraumaMalignantPsychological traumaManagement :OrcheopexyHormonal treatment
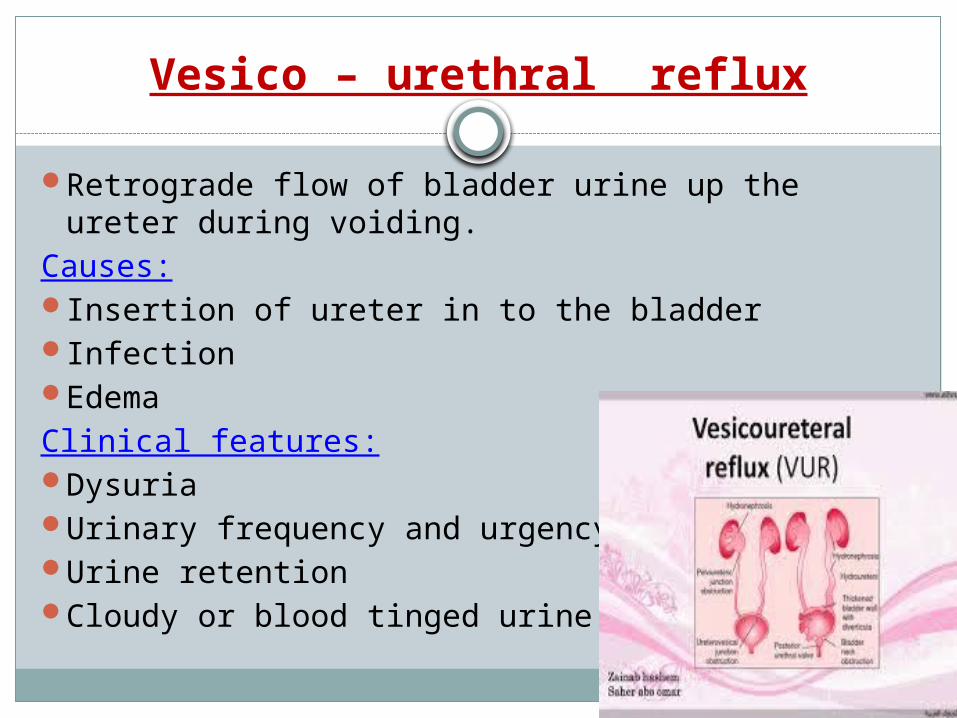
Vesico – urethral reflux
Retrograde flow of bladder urine up the ureter during voiding.
Causes:Insertion of ureter in to the bladderInfectionEdemaClinical features:DysuriaUrinary frequency and urgencyUrine retentionCloudy or blood tinged urine
Management :Correction of structural anomaliesAdministration of low dose antibiotics
Detecting kidney and urinary tract abnormalities before birth
Ultrasound examinationAntenatal screeningScreening of high risk groups
Prevention of congenital genito urinary anomalies
Advice to future parentsTo minimize exposure of pregnant women to
risk factorsTo prevent over weight/ obesityTo promote effective information on dietTo improve folate statusTo avoid contraindicated vaccinationTo include school education programmes
Nursing management of the child with urologic surgery
Promoting understanding of parentsPreparing for diagnostic proceduresInvolving the parents in child careMonitoring intake and outputPreventing infectionsProviding comfortProviding adequate nutritionTeaching the parents about related care
Thank you…
