theoretical framework - teaediciones theoretical framework: general concepts 5 in neuronup we design...
TRANSCRIPT

NeuronUP Theoretical framework: General Concepts
1
Theoretical framework:General Concepts

NeuronUP Theoretical framework: General Concepts
2
NEURONUP
Theoretical framework:General Concepts

NeuronUP Theoretical framework: General Concepts
3
Introduction
Bases of rehabilitationHierarchical model of the CNS
Plasticity
Intervention: How to rehabilitate
Cognitive Functions Orientation
Attention
Agnosias
Apraxias
Visuospatial skills
Memory
Language
Executive functions
Social cognition
Activities of Daily LivingBasic activities of daily living.
Instrumental activities of daily living
Education
Work
Social skillsReferences
INDEX
3
10
11
13
15
18
19
22
25
32
37
40
46
51
61
65
66
67
68
68
71
72
Page

NeuronUP Theoretical framework: General Concepts
4
IntroductionThe goal of neuropsychological rehabilitation is to improve an individ-
ual’s performance and to compensate for the impairments resulting from brain injury in order to reduce functional limitations and increase the ability of the person to perform activities of daily living (Bernabéu & Roig, 1999) with the purpose of improving quality of life (Christensen, 1988; Prigatano, 1984; Sohlberg, & Mateer, 1989).
Cognitive functions are interrelated, and interdepend-ent on a functional and anatomical level. Functional activi-ties involve multiple types and levels of processing. When an activity of daily living is carried out, neural combina-tions that recruit specific neuropsychological processes to perform it are put into play. From those motivations that initiate behavior, all the way through to visual recognition, impulse control or the development of cognitive strate-gies to resolve these impulses, to plan behavior or to learn. Therefore, from a professional approach, it is logical to formulate rehabilitation activities from an ecological per-spective.
The goal of NeuronUP is to identify those processes in order to calibrate and design useful activities for neu-
ropsychological rehabilitation and occupational therapy, as well as providing a platform and flexible materials for neuropsychology professionals. Neu-ronUP was founded in response to several urgent questions in the field of neuropsychological rehabilitation in general, and clinical and experimental practice in particular. In line with the urgent need to carry out a more eco-logical neuropsychological assessment (Tirapu, 2007) that allows clinicians to assess the accurate functional condition of individuals who come for a consultation, there has emerged a school of thought that seeks to use more ecological, motivational and personalized contents in the process of cogni-tive stimulation and rehabilitation. Therefore, in addition to the assessed functions, an ecological approach can be applied to neuropsychological re-habilitation (Wilson; 1987, 1989).
Ecological validity refers to—Kvavilashvili & Ellis (2004)—both the representativeness of a task (the degree of correspondence in form and context in regards to a real life situation), and the generalizability of the results produced by that task. There are three different levels of generaliz-ability:
Level 1. Keeping the outcomes from session to session, using the same situations and materials.
Level 2. The achieved progress has to reflect in similar tasks.
Level 3. Transferring the skills acquired during training sessions to activities of daily living.
BEHAVIORAL INTERVENTION
ADJUSTMENTTO COGNITIVE
PROFILE
FUNCIONAL INDEPENDENCE
WeakSkills
Strong Skills
PHARMACOLOGY
EXTERNAL AIDS & SUPPORT
OCUPATIONALTHERAPY
COMMUNITY
COGNITIVE
PROFILE
QUALITYOF
LIFE
- GOALS- EXPECTATIONS- FEELINGS
ADL ADL
ADL

NeuronUP Theoretical framework: General Concepts
5
In NeuronUP we design materials involving activities and situations of daily living that are related not only to basic neuropsychological functions—since they are multifaceted activities—but also to variables of daily function-ing (Yantz, Johnson-Greene, Higginson, & Emmerson, 2010).
Taking advantage of the “cognitive profile” (weak and strong cognitive points) requires our scheme of rehabilitation to be at least as comprehensive as the neuropsychological tests used to establish a baseline (we have 40 neuropsychological pro-cesses divided among 11 cognitive functions). This com-prehensiveness allows an accurate analysis of the neu-ropsychological processes involved in activities of daily living.
“The planning of the rehabilitation activities and times is under the control of the therapist”. Thus, the therapist decides which type of activities each patient must per-form, the duration of each activity, and at which level of difficulty the tasks will be adjusted (Muñoz-Céspedes &
Tirapu, 2004). NeuronUP adopts this principle as one of the basis of its approach, and the activities have been designed so that the therapist can adjust the parameters of those activities without compromising the record of the data.
Incorporating the general observations on neuropsychological rehabilita-tion given by Muñoz-Céspedes & Tirapu (2001), NeuronUP:
- Calibrates the complexity of the tasks.
- Divides tasks into their different component parts.
- Gives simple and clear instructions that help give structure to the task and its performance. If the therapist considers the language sug-gested by NeuronUP inappropriate for the person undergoing reha-bilitation, we give the option to customize the instructions of the activities.
- Makes resources more accessible for the patient in terms of under-standing while also saving expenses and travel.
Computer-assisted rehabilitation benefits
Why use a web platform of computer-assisted rehabilitation? Although it would be incorrect to conceptualize NeuronUP as solely computer-based (since many materials can be printed out), below we propose some advan-tages in the use of computer format (Ginarte-Arias, 2002; Lynch, 2002; Roig & Sánchez Carrión, 2005):
- It enables the accurate control of certain variables such as stimulus-exposure time and reaction time. This allows suitable control of
The planning of the rehabilitation
activities and times is under
the control of the therapist”

NeuronUP Theoretical framework: General Concepts
6
patient evolution and his/her monitoring.
- Data collection is more reliable and consistent, and its analysis is facilitated. In this way, it is possible to plan a strategic neuropsy-chological rehabilitation.
- The stimuli presented are more attractive, which increases the moti-vation of the individual. Customization of activities.
- Integration of multimedia materials.
- Provides quick and accurate feedback because it allows the con-struction of an interactive system of changing images depending on whether the answers are correct or not while allowing for independ-
ent work from home. This helps build awareness of the deficit.
- Connection of peripheral devices for motor or visual problems.
- Allows flexibility since computer-based materials can be programmed to permit alteration of different vari-ables such as the type of stimulus used, the level of difficulty, or exposure time in such a way that alterna-tive procedures can be selected in accordance with the specific needs of each patient. In fact, one of the ad-vantages of NeuronUP is that it adapts to the pa-tient based on the decisions of the therapist, and it is not the patient who has to adapt to the level or
the materials of the activities.
- Some programs and platforms have a reasonable cost–benefit since they save the therapist time. NeuronUP allows access to the platform and data from any place.
How have we corrected problems associated with computer-assisted neu-ropsychological rehabilitation?
1. We have developed a flexible system so that it is not applied in a rigid and inappropriate manner (Ginarte Arias, 2002).
2. We adapt the contents to the evolutionary moment of the persons undergoing rehabilitation (Tam & Man, 2004). Additionally, this ex-pert system can adapt to language, educational level, or the type of brain injury of patients.
We believe that the use of cognitive rehabilitation platforms and pro-grams cannot replace the contact, support, effort and supervision of the therapists. The programs must be continually revised and updated based on patient evolution and performance (Sánchez Carrión, Gómez Pulido, García Molina, Rodríguez Rajo, & Roig Rovira, 2011). To consider an intervention that only takes into consideration the cognitive sphere without acknowledg-ing psychosocial, emotional and behavioral disorders is an insufficient ap-proach (Salas, Báez, Garreaud, & Daccarett, 2007).
Benefits of a computer-based platform: data tracking, motivating
materials,accurate feedback, flexible
approach, adjustment, planning...

NeuronUP Theoretical framework: General Concepts
7
Assistive technologies for cognition (ATC) are being used to support a wide range of activities, from communication to social participation (Gillespie, Best & O´Neill, 2012). This is due to different improvements and changes in the concept of “technologies for cognitive rehabilitation along the last 40 years”. From first generation computers to videogames and fi-nally to “social communication” devices, the use of technology for cognitive rehabilitation has evolved from isolated (lab) use to functional and ecologi-cal intervention in which ATC are a part of a holistic model that empowers
functional and emotional outcomes.
Computer-Based Cognitive Rehabilitation Technolo-gies may be used in a wide range of populations. Cole (1999) has already shown that cognitive orthoses should be highly customizable to the needs of the person. More-over, the use of “therapist-friendly” and “user-friendly” interfaces (Cole, Ziegmann, Wu, Yonker, Gustafson &
Cirwithen, 2000) should be used. These interfaces should provide a simpli-fied file access, save and print commands for word processing to increase the ability to access, modify, and print longer, detailed amounts of informa-tion. According to Lynch (2002), these types of activities should be used to train tasks related to Activities of Daily Living, including work.
Due to heterogeneity in cognitive profiles (strengths and weak-nesses), materials and guides used in computer-based technologies must be adapted in terms of complexity–number and difficulty of decision-making points-presentation of information sequentially, and others (LoPresti, Mi-hailidis & Kirsch, 2004). For that purpose, users must be included in the design process, according to the concept of “user sensitive inclusive design” proposed by Newell & Gregor (2000). These recommendations point to the need for a computer-based personalized cognitive training in neuropsycho-logical rehabilitation. Peretz, Korczyn, Shatil, Aharonson, Birnboim & Giladi (2011) compared a computer-based personalized cognitive training group with a group that received a classical computer games training. Improvements in the personalized condition were significant in all the cognitive domains trained (focused attention, sustained attention, recognition, recall, visuospa-tial learning, visuospatial working memory, executive functions, and mental flexibility), while classical computer games group improved significantly only in four domains (focused attention, sustained attention, memory recognition and mental flexibility).
For a more extensive review, the reader can consult the following: Gillespie et al. (2012); Kueider, Parisi, Gross & Rebok (2012); Cicerone et al. (2011); Stahmer, Schreibman & Cunningham (2010); Faucounau, Wu, Bou-lay, De Rotrou, Rigaud (2009); Lange, Flynn & Rizzo (2009); Tang & Pos-ner (2009); LoPresti et al. (2004), Kapur, Glisky & Wilson (2004), Bergman (2002) and Lynch (2002).
In relation to specific neuropsychological functions, a broad amount of research has been done to date. Computer-based interventions have proved effective in the rehabilitation of different domains such as atten-
Taking onlyinto consideration the cognitive sphere is an insufficient approach”
NeuronUP Theoretical framework: General Concepts
8
tion (Borghesse, Bottini & Sedda, 2013; Jiang et al., 2011; Flavia, Stampa-tori, Zanotti, Parrinello & Capra, 2010; Barker-Collo et al., 2009; Dye, Green & Bavelier, 2009; Green & Bavelier, 2003; Cho et al., 2002; Grealy, John-son & Rushton, 1999; Gray, Robertson, Pentland, Anderson, 1992; Sturm & Wilkes, 1991; Niemann, Ruff & Baser, 1990; Sohlberg & Mateer, 1987), memory (Caglio et al., 2012, 2009; das Nair & Lincoln, 2012; McDonald, Haslam, Yates, Gurr, Leeder & Sayers, 2011; Bergquist et al., 2009; Gillette & DePompei, 2008; Wilson, Emslie, Quirk, Evans & Watson, 2005; Ehlhardt, Sohlberg, Glang & Albin, 2005; Glisky, Schacter & Tulving, 2004; Kapur, Glisky & Wilson, 2004; Tam & Man, 2004; Webster et al., 2001; Wilson, Emslie, Quirk & Evans, 2001; van der Broek, Downes, Johnson, Dayus & Hilton, 2000), visuospatial skills (Boot, Kramer, Simons, Fabiani & Grat-ton, 2008), language (Allen, Mehta, McClure & Teasell, 2012; Fink, Brecher, Sobel & Schwartz, 2010; Lee, Fowler, Rodney, Cherney & Small, 2009; Kirsch et al., 2004b; Wertz & Katz, 2004; Katz & Wertz, 1997), social cognition (Grynszpan et al., 2010; Bernard-Opitz, Srira & Nakhoda-Sapuan, 2001), and executive functions (Nouchi et al., 2013; Johansson & Tornmalm 2012; López Martinez et al., 2011; O´Neill, Moran & Gillespie, 2010; Westerberg et al., 2007; Ehlhardt et al., 2005; Kirsch et al., 2004a; Gorman, Dayle, Hood & Rumrell, 2003).
Computer-based interventions (and micro-computing interven-tions) have also been applied with positive outcomes to a wide range of psy-chological impaired profiles such as those occurring due to TBI (Cernich et al., 2010; Gentry, Wallace, Kvarfordt & Lynch, 2008; Thornton & Carmody, 2008; Michel & Mateer, 2006), stroke (Cha & Kim, 2013; Lauterbach, Fore-man & Engsberg, 2013; Akinwuntan, Wachtel & Rosen, 2012; Cameirão, Bermúdez I Badia, Duarte Oller & Verschure, 2009; Michel & Mateer, 2006; Deutsch, Merians, Adamovich, Poizner & Burdea, 2004; Teasel et al., 2003; Wood et al., 2004), dementia (Crete-Nishihata et al., 2012; Mihailidis, Fernie & Barbenel, 2010; Cipriani, Bianchetti &Trabucchi, 2006; Cohene, Baecker & Marziali, 2005; Alm et al., 2004; Hofman et al., 2003; Zanetti et al., 2000), multiple sclerosis (Flavia et al., 2010; Shatil, Metzer, Horvitz & Miller, 2010; Vogt et al., 2009; Gentry, 2008), autism spectrum disorders (Sitdhisanguan, Chotikakamthorn, Dechaboon & Out, 2012; Wainer & In-gersoll, 2011; Tanaka et al., 2010; Beaumont & Sofronoff, 2008; Sansosti & Powell-Smith, 2008; Stromer, Kimball, Kinney & Taylor, 2006; Goldsmith & LeBlanc, 2004; Silver & Oakes, 2001; Werry, Dautenhahn, Ogden & Harwin, 2001; Lane & Mistrett, 1996), ADHD (Steiner, Sheldrick, Gotthelf & Perrin, 2011; Rabiner, Murray, Skinner & Malone, 2010; Shalev, Tsal & Mevorach, 2007; Mautone, DuPaul & Jitendra, 2005; Shaw & Lewis, 2005), learning disabilities (Nisha & Kumar, 2013; Seo & Bryant, 2009 –with recommen-dations regarding effectiveness-; Kim, Vaughn, Klingner & Woodruff, 2006; Hasselbring & Bausch, 2005; Lee & Vail, 2005; Maccini, Gagnon & Hughes, 2002; MacArthur, Ferretti, Okolo & Cavalier, 2001; Hall, Hughes & Filbert, 2000), intellectual disabilities (Cihak, Kessler & Alberto, 2008; Mechling & Ortega-Hurndon, 2007; Ayres, Langone, Boon & Norman, 2006; Ortega-

NeuronUP Theoretical framework: General Concepts
9
Tudela & Gómez-Ariza, 2006; Standen & Brown, 2005; Furniss et al., 1999), schizophrenia (Sablier et al., 2011; Suslow, Schonauer & Arolt, 2008 –with recommendations for future research-; Medalia, Aluma, Tryon & Merriam, 1998; Hermanutz & Gestrich, 1991), or social phobia (Neubauer, von Auer, Murray, Petermann, Helbig-Lang & Gerlach, 2013; Schmidt, Richey, Buckner & Timpano, 2009). Computer-based interventions can also be a tool for training of cognitive skills in normal aging (Kueider, Parisi, Gross & Rebok, 2012; Cassavaugh & Kramer, 2009; Basak, Boot, Voss & Kramer, 2008; Flnkel & Yesavage, 2007; Rebok, Carlson & Langbaum, 2007; Jobe et al., 2001).
Some experimental and clinical issues should be con-trolled to adequately assess the factors and effect of computer-based cognitive rehabilitation. Santaguida, Oremus, Walker, Wishart, Siegel & Raina (2012) recently identified some methodological flaws in stroke rehabili-tation reviews. These aspects extend to computer-based studies and therefore must be addressed. They showed that primary studies had problems with randomization, allocation concealment, and blinding. Also, baseline com-parability, adverse events, and co-intervention or contami-nation were not consistently assessed in all studies. Ore-mus, Santaguida, Walker, Wishart, Siegel & Raina (2012)
recommend that researchers rationalize the number of outcome measure instruments used in their studies. The control of additive effects of other coadjutant therapies must also be taken into account. Jack, Seelye & Jurick (2013) have already addressed the generalization of trained tasks versus to untrained tasks in computer-based cognitive rehabilitation. According to their results, “fewer studies have demonstrated improvements in untrained tasks within the trained cognitive domain, non-trained cognitive domains, or on measures of everyday function. Successful cognitive training programs will elicit effects that generalize to untrained, practical tasks for extended periods of time”. Reviews of meta-analysis recommend stronger methodo-logical designs. For a good review of the principles that should be taken into account in computer-based learning research, we recommend Cook (2012, 2005). Van Heugten, Gregório & Wade (2012) suggest the development of “an international checklist to make standardised description of non-phar-macological complex interventions possible”.
In conclusion, computer-based interventions can effectively facilitate improvement in many activities that would otherwise not be possible, but future research must control relevant parameters in computer-based cogni-tive rehabilitation studies.
Future research of computer-based
interventions should control relevant
parameters to enhance validity”

NeuronUP Theoretical framework: General Concepts
10
BASES OF REHABILITATION

NeuronUP Theoretical framework: General Concepts
11
Hierarchical model of the CNSThe central nervous system can be divided into three hierarchical axes with functional specialization.
Anterior-posterior or rostral-caudal axis In which anterior or frontal areas manage abstract
content rather than specific, and more complex types of information possibly involved in the monitoring and integration of contents and processes. In this respect, we can observe control processes in cognitive and emo-tional functions. While the anterior regions contain more complex representations of the emotional contents, re-garding emotional functions, the insula, the posterior re-gions—posterior cingulate cortex, posterior insula—and the middle cingulate cortex, all support the functionality of first-order processes that manage sensory informa-tion. In general, this happens too with attentional and cognitive contents. In attentional processes we can see how the most frontal areas monitor and guide the search based on complex contents (for example, goals), while the most posterior cortical regions (for example, the pa-rietal lobe) guide the process based on the stimuli and not on reflective process.
The cognitive content of the anterior regions is more complex as well. The anterior frontal regions, for in-stance, control conscious and reflective processes, moni-tor the actions that we perform and use modality-specific information that is received from different areas of the brain directly (communication between frontal areas), and through association areas.
On the whole, the complexity of the representations contained in the rostral regions is greater, and is used to develop abstract schemata, higher-level cognitive func-tions and conscious and volitional action commands. In addition, the rostral regions in this plane are capable of integrating different kinds of information from other more posterior parts of the brain, for example, simple inputs about locations or luminance.
ANTERIORAbstract contentsComplexityControlMonitoringIntegration of processesHigh-order FunctionsVolitionSocial CognitionOperative-driven processes
POSTERIORStimulus-driven processesLow-Order FunctionsModality-specific informationPerceptual IntegrationAutomatic processes
DORSALReflective processCold funtionsReappraisalSelf-based strategies
VENTRAL Autonomies responsesEmotional processing “Hot” functionsSituation-based strategies
LATERAL External worldSpatial info“Others” info
MEDIALInternal Cues Processing
Personal informationNext to emotion areas

NeuronUP Theoretical framework: General Concepts
12
Cortical-limbic or dorsal-ventral axisIn which dorsal regions are responsible for reflective or cognitive pro-
cessing. By contrast, the ventral regions are responsible for a stimulus-driven or emotional processing. Among the more dorsal structures we find the an-terior cingulate cortex or ACC—especially the rostral ACC—and in ventral regions we find the amygdala”, which is an automatic node of emotion. It is logical to think that these have a more automatic processing such as, for example, situation-based strategies, as is the case with the implication of the rostral ACC in modulating the amygdala in the resolution of conflict. On the other hand, the reappraisal, which is a cognitive control of the emotional processing, a reflective strategy based on oneself.
Medial-lateral axisIn which medial structures are responsible for processing focused on the
individual and his/her internal cues, while lateral structures are responsible for visual and spatial aspects and the representation of characteristics of the external world. In this sense, medial areas are closer to the emotional
centers, and as a result, they have a greater number of in-terconnections due to the cytoarchitectonic organization and therefore, both influence or regulate each other. In fact, the emotional structures are those responsible for giving information to the subject about his/her internal states, thus the further we move away (cytoarchitectur-ally) from these areas, the functional relationship grows smaller. Structures with more depth have connections with the autonomic nervous system and, therefore with the arousal, these structures influence those data-driven events. By contrast, more superficial structures in some way modulate the structures that belong to the autonomic nervous system with reflective processes.
Anterior (frontal) regions control conscious and
reflective processes, monitor actions and
use information from different points of the
brain
NeuronUP Theoretical framework: General Concepts
13
PlasticityBrain plasticity refers to the brain’s capacity to reorganize its patterns of
neuronal connectivity and readjust its functionality. Neural plasticity is not only found in acquired brain injury but also in active aging and even in Alz-heimer’s dementia (though neuronal degeneration attacks new hippocampal structures that reduce the ratio of neurogenesis).
Functional rehabilitation takes advantage of this phenomenon to generate new synapses, even though the effect may be limited in the recovery of func-tional deficits. As of today, there are no param-eters that guarantee a permanent therapeutic win-dow for this phenomenon because it depends on
factors such as the type of injury, age and others such as recovery. Brain-computer interfaces have been used to augment plasticity and out-comes for neurological rehabilitation. Skill learning after brain injury and other diseases draws upon spared neural networks for movement, sensation, perception and cognitive functions. Physiological basis for neurorehabilita-tion depends on these mechanisms (Dobkin, 2007):
- Changes in neuronal tuning to parameters of movement,
- Variability of neuronal firing as practice and reward proceed,
- Hebbian strengthening of neural ensembles with remapping of representations for movements,
- Recruitment of remote or correlated activity from ensembles within a network,
- Other self-regulation and learning-associated processes.
New neurons are continuously generated in the adult human brain (Ming & Song, 2011; Boyke, Driemeyer, Gaser, Büchel & May, 2008; Ge, Sailor, Ming & Song, 2008; Fuchs & Gould, 2000; Gross, 2000; Eriksson, Per-filieva, Björk-Eriksson, Alborn, Nordborg et al., 1998). From this point of view, plasticity may result from two potential different mechanisms (Ming & Song, 2011): renewing neurons and/or multi-potential differentiation of neurons. Rates of these processes are significantly slower in the adult brain than in the child brain.
But, how can a small number of neurons affect the global functioning of a brain? Ming & Song (2011) mention that the answer may reside in the capacity of adult-born neurons both as encoding units and as active modifi-ers of mature neuron firing, synchronization, and network oscillations. They propose some principles by which this can be possible:
1. Adult-born neurons are preferentially activated by specific inputs
2. Adult-born neurons actively inhibit local circuitry output
3. Adult-born neurons also modify the local circuitry through selec-tive activation of modulatory pathways, and
Adult human brain is continuosly generating
new neurons

NeuronUP Theoretical framework: General Concepts
14
4. Newborn neurons could contact several distinct subtypes of local interneurons
Plasticity could enhance learning processes in three levels (Berlucchi, 2011): a neuronal level, a synaptic level (changing connectivity spines or newly formed neurons as a consequence of experience and adaptation) and a network level (changes in functional connectivity as a result of the modifi-cation of existing synapses or the formation of novel synaptic connections). These levels are not mutually excluding. Short-term and long-term spine re-modeling, including formation, elimination and shape and size changing, as well as axonal sprouting, are principal means by which both maturation and
experience can organize neuronal connectivity (Álvarez & Sabatini, 2007) through long-term potentiation and de-pression of synaptic transmission caused by neurotrophic factors, which modulate synaptic strength. Neurotrophic factors are also influenced by experience through epige-netic regulation of genes (Cowasange, LeDoux & Mon-fils, cited by Berlucchi, 2011).
Plasticity is a natural phenomenon that entails brain adaptation to tasks and age. In older brains, compensatory mechanisms are required for a better performance in spe-cific working memory tasks: elder brains show widespread
activity, with a diffuse cortical activation. This may represent a compensato-ry response (Dennis & Cabeza, 2011). Regardless, plasticity as a maturation and learning phenomenon and plasticity that takes place after brain injury are not the same, and differences among these processes should be clarified before making any conclusion.
There are diverse environmental factors that can affect plasticity. Among others, stress or insulin deficiency syndromes (a profile that could be related to Alzheimer’s disease) decrease the rate of neuroplasticity in adult brains. On the other hand, physical exercise increases cell proliferation (van Praag et al., 1996; cited by Ming & Song, 2011). Learning modulates adult neuro-genesis in a specific fashion (Zhao, Deng & Gage, 2008). For example, some types of adult neurogenesis are only influenced by learning tasks that de-pend on the hippocampus. Studies have suggested significant contribution of adult hippocampal neurogenesis to (Deng et al., 2010):
• Spatial-navigation learning and long-term spatial memory retention,
• Spatial pattern discrimination,
• Trace conditioning and contextual fear conditioning,
• Clearance of hippocampal memory traces, and
• Reorganization of memory to extrahippocampal substrates
Plasticity entails brain adaptation to tasks and age.
Enviromental factors influence
plasticity ”

NeuronUP Theoretical framework: General Concepts
15
Intervention: How to rehabilitate
The therapeutic strategy will be selected based on the severity of defi-cits, the elapsed time since injury, and the profile of the cognitive deficit. But in a general manner we can establish the following distinctions (Lubrini, Periáñez, & Ríos-Lago, 2009):
• Re-establishing previously learned patterns of behavior and cog-nitive activity.
• Establishing new patterns of cognitive activity by means of sub-stitution strategies.
• The introduction of new patterns of activity thanks to internal and external compensatory mechanisms.
• Rehabilitation helps patients and their families to adapt to the new condition of disability in order to improve the patients’ overall level of functioning.
Zangwill (1947) distinguished compensation, a reorganization of behav-ior aimed at minimizing a particular disability, from substitution, the accom-plishment of a task by new methods different from those naturally employed by the intact brain in the performance of that particular task.
The evolution of functional recovery following brain injury may be as-cribed to four basic events and principles (Edelman & Gally, 2001):
(1) a spontaneous disappearance of the acute effects of traumatic or ischaemic lesions;
(2) a reversal of diaschisis, that is, a reversal of the temporary depres-sion of activity in uninjured brain regions following their discon-nection from the injured region;
(3) the principle of vicarious function, that is, the taking over of the functions of the injured part of the brain by distant back-up areas endowed, inherently or by acquisition, with the same functional capacity;
(4) the principle of redundancy, that is, the maintenance of the func-tion of a damaged system by those parts of the same system that have escaped injury; and
(5) the principle of degeneracy, that is, the performance of the same function by multiple differentiated neuronal systems either through similar mechanisms or by applying different strategies.
The essence of therapy is progressive practice of subtasks and more complete intended goals using physical and cognitive cues with feedback about performance and results (Dobkin, 2005).Nonetheless, we have to take care of the strategy implied in our therapy because the potential for func-

NeuronUP Theoretical framework: General Concepts
16
tional recovery of a damaged neuronal system may be suppressed through a disuse process caused by compensation and substitution strategies (Belucchi, 2011).
Cognitive rehabilitation should be guided by the following principles:
- Be based on theoretical models and scientific evidence.
- Have a multidisciplinary perspective.
- To establish a priority of objectives.
- Use tools as a help to get objectives, not as a solution by itself.
- Adjust time and intensity of the treatment according to the patient´s characteristics and evolution.
- Consider autonomy as the main goal instead of cognitive deficits.
- Be focused on preserved skills whit the objective to enhance weak
cognitive skills, functional outcomes, and behavior.
- Take care about motivational intervention. Identify significant
reinforcers for the patient.
- Include tasks that help generalization
- Design a flexible rehabilitation schedule that allows objective
modification.

NeuronUP Theoretical framework: General Concepts
17
Personalized, systematic planning of therapy sessions
Attractive materials for the patient, adapted to his/her real evolution / actual condition / current functional status
Constant updating of rehabilitation tools (Evidence-based practice)
NEURONUPMETHOD
Applicability:
Dementias Acquired brain damage
Adaptive psychological disorders
ADHDDevelopmental and learning disorders
Normal aging
etc...
Based on models of cognitive functioning and neuropsychological rehabilitation……and of the specific nature of the cognitive domains, based on competences and abilities in specific activities
Approach to cognitive functioning
conceptualizationof rehabilitation
Restoration
Compensation
Substitution
Integration
of functions
Ongoing practice
Education in biopsychosocialaspects
Specific processtraining
Training in generalizablestrategiesRehabilitation
mechanisms
Orientation Control
Monitoring
Self-control
Executive metacognition(external and internal)
Basic cognitive function (Attention,Perception, Memory, Language, Praxis, Executive functions ….)
Emotionalcontrol
Social skills and competences
Daily life activities
Adaptive conceptualization of behavior in functional andpsychosocial environments
NEURONUPMETHOD
Goals:
Significant functional improvement of the user
Models of independent living
Improvement in quality of life
Modular andMulti-modal
Basic and ecological
Issues in cognitive rehabilitation. Applying NeuronUP

NeuronUP Theoretical framework: General Concepts
18
COGNITIVE FUNCTIONS
f(x)

NeuronUP Theoretical framework: General Concepts
19
- Environment of the patient should be analyzed to find significant reinforcers.
OrientationOrientation is a cognitive function whose goal is to locate the subject
in a specific parameter of his/her environment. As a result, it requires in-formation relating to spatial location, in addition to functions of attention,
memory (episodic and semantic), and working memory.
Orientation is defined as the awareness of oneself in relation to the characteristics of one’s surround-ings: place, time, and personal history. It requires the integration of attention, perception and memory (Lezak, 2004). Deficits in perception or memory can result in mild impairments in orientation, while alterations in the subsystems of attention can result in severe impairment in orientation at all levels. The dependence on other sys-tems makes orientation especially vulnerable (however, its presence does not rule out cognitive damage since orien-
tation is also influenced by routine). There are three types of orientation:
• Temporal orientation: are updating processes whose output in-forms about situations related to the day, time, month, year, mo-ment of performing behaviors, public official holidays, seasons, etc. Temporal orientation depends largely upon sustained atten-tion and semantic memory, while selective attention captures the changes in the environment that determine an organized pro-cess of time—the moment of performing an action (to have din-ner, to get up), what does it mean (in relation to the weather) that it is snowing, etc—. Temporal orientation differs from temporal estimation, since this metacognitive process entails:
- Either an estimate of elapsed time (vigilance, decision mak-ing, perception).
- Or an estimate of the amount of time we can spend on an activity (which depends on planning and prospective memory).
• Spatial orientation: are updating processes in which the subject is able to locate himself/herself in a spatial continuity (where he/she is coming from, where he/she is at a specific moment, where he/she is going). Spatial orientation depends, in the first place, on the orientation of visual attention, sustained atten-tion, selective attention and memory.
• Personal orientation: personal orientation is
Orientation requires a integration of
information from different brain
networks
Updating processes require retrieval of
recent and old stored information about
place, time and identity

NeuronUP Theoretical framework: General Concepts
20
the most complex process out of the three, as it usually requires multimodal information that involves personal identity, and a mechanism of control that verifies the information (in case of failure, confabulations could occur). Some authors have referred to this type of orientation as autonoetic consciousness (Tulving, 2002). Autonoetic consciousness involves the reorganization of contents of the autobiographical episodic memory in relation to the present moment, involving a sense of self-continuity. In order to have access to this type of information, encoding algorithms are required in the first place and then, the working memory up-dates that content, thereby connecting it to the present time and moment resulting in a sense of self-continuity.
Dependence of functional systemsOrientation involves remembering. Therefore, it is a system whose traces
are cortically distributed throughout the whole central nervous system but with special relevance for the hippocampus. The influence of some hip-pocampal structures differs depending on the type of orientation, but it is a function particularly linked to this structure. In fact, orientation tasks are
usually used mainly with persons with dementias associ-ated to this structure. There are several reasons for this:
In the first place, the type of information that is re-quired changes quite often (especially temporary informa-tion) and depends on very recent memory traces. If the hippocampus has not been able to develop algorithms that connect mnestic information to cortical traces as a result of brain injury, those neural traces disappear. Sec-ondly, the update of contents depends largely upon work-ing memory. Though it is true that working memory is an executive process widely distributed throughout the cen-tral nervous system (although with functional predomi-
nance of the dorsolateral prefrontal cortex), in dementias there is usually a general alteration in white matter tracts that affect the integrity of the task-positive network (in opposition to the default-mode network). This al-teration causes a disconnection between systems responsible for retrieving and updating information (prefrontal cortex, longitudinal fasciculi), memory traces (grey matter), and mechanisms that generate algorithms to facilitate access to those traces (hippocampus).
This disconnection is progressive and decline in orientation occurs in parallel to it. Thus, the most recent and variable data (day, time, new place, recent births within the family, names of people we recently met, age…) is
Orientation is the most vulnerable function
in disconnection syndromes, as it
relies on widespread networks of the brain

NeuronUP Theoretical framework: General Concepts
21
the first lost, while older data is more resistant to decay because neural algo-rithms belong to more consolidated networks.
Models used to design materialsThe principles used in the design of orientation activities are primarily
based on two models: the Reality Orientation and Reminiscence Therapy—a flexible model that relies on external aids—and the Orientation Remedia-
tion Module developed by Ben-Yishay (Ben-Yishay et al., 1987) that is based on Posner and Petersen’s model of attention (1990).
The Reality Orientation and Reminiscence Therapy has as its objective temporospatial re-orientation and the reinforcement of the foundations of the patient’s person-al identity by repetitively presenting information regarding orientation with the use of various external aids (Arroyo-Anlló, Poveda Díaz-Marta, & Chamorro Sánchez, 2012). The materials are designed based on two factors: an indi-vidual one, with activities that the therapist administers
to the patient daily, and a group one, with activities that can be performed by several subjects using interactive scoreboards. Specifically, reminiscence interventions manage similar age groups and encourage the sharing of au-tobiographical stories that promote group cooperation to build meanings from the biography (personal and shared) of the persons in the group. In order to do so, it is necessary to integrate content such as photographs, vid-eos, songs, words, etc. NeuronUP provides user-friendly and easy-to-use (by both therapists and patients) interfaces to share those contents.
The Orientation Remediation Module created by Ben-Yishay possesses a more defined attentional nature and a significant theoretical structure that agrees with the general premises we use in NeuronUP, especially the concept of functional hierarchy. In functional hierarchy, activities designed for ori-entation stem from the first hierarchical stage of the modules developed by Ben-Yishay that focuses on increasing the level of alertness.
Additionally, some concepts from the Montessori Intervention Model have been adapted to design the activities in this area. This is due to the fact
Posterior attentionsystem
Anteriorattentionsystem
Reticularsystem
Posterior parietal cortex Superior colliculus Thalamic pulvinar
Anterior cingulate
Attentional orienting Target detection
Arousal
Petersen & Posner Attentional Model
(1990), in which Ben Yishay´s Orientation
Remediation Model is based.
Rehabilitation of orientation requires
increasing alertness, teaching coding
strategies and retrieval external aids

NeuronUP Theoretical framework: General Concepts
22
that orientation activities are mainly formulated (although not exclusively) for intervention in dementias.
AttentionAttention is a complex cognitive function involving several subsystems
and has been explained in different manners. Next, I will briefly explain Pos-ner’s definition (1995). For Posner, attention is “the selection of informa-tion for conscious processing and action, as well as maintaining an alert state required for attentional processing” (Posner & Bourke, 1999, mentioned by Benedet, 2002.). Attention is a limited capacity function that distributes cognitive resources of the central nervous system based on situation sche-mata (ORIENTATION), and according to information priority. It has two main functions: maintaining a vigilant or alert state, and the selection of relevant information that the resources are going to manage (MONITOR-ING AND CONTROL). The characteristics of attention are the following (Posner, 1995):
A. Attention does not process information; it either allows or inhibits that processing. Attention is anatomically separate from the informa-tion processing systems.
B. Attention utilizes a network of anatomical areas. It is neither the property of a specific area of the brain, nor a general result of the brain.
C. The brain areas involved in attention do not have the same function, but different areas carry out different functions. Attention is not a unitary function.
Which anatomical networks underlie attention?
In attention there are three anatomical networks that function as “small-world networks” connected on a large scale.
- Ascending reticular activating system (Posner, 1995): controls tasks of tonicity, regulates the sleep-wake cycle and the state of arousal. Its main nuclei are found in the brainstem although its networks extend through the ascending pathways throughout the cerebral cortex. Its main neurotransmitter is the norepinephrine (NE). The main NE inputs of the locus coeruleus project to the parietal area, the pulvinar nucleus of the thalamus and the culliculi, that is, the areas that constitute the poste-rior attentional network.
- Cingulo-opercular network (Dosenbach et al., 2008): consists of the anterior prefrontal cortex, anterior insula, dorsal ACC, and thalamus. It provides stable set-maintenance throughout task execution.
- Frontoparietal network (Dosenbach et al., 2008): includes the dor-

NeuronUP Theoretical framework: General Concepts
23
solateral prefrontal cortex, inferior parietal lobule, dorsal frontal cortex, intraparietal sulcus, precuneus, and midcin-gulate cortex. It plays a role in initiating and adjusting cognitive control responding differentially depending on the feedback that is received from our behaviors.
The frontoparietal and cingulo-opercular networks work in parallel and are connected through the cerebel-lum, which functions as a hub between the thalamus (cinguloopercular) and the precuneus, the inferior parietal cortex, and the dorsolateral prefrontal cortex (frontopari-etal), acts as an error-detecting mechanism, and connects with those areas that detect (anterior cingulate cortex) and adopt strategies (frontoparietal network) for the perceived
error.
These anatomical networks are integrated in two different ways or forms (Corbetta et al., 2008), creating a double network of attentional execution:
• A ventral network, dedicated to detecting salience of envi-ronmental stimuli,
• And a dorsal network that is activated during focal attention tasks sustaining attention over time and that also acts by being directed by the ventral network.
Both networks are indirectly related through the prefrontal cortex.
Which cognitive processes define attention?
We have established a hierarchical model similar to the one developed by Ben-Yishay but focused on functional concepts. Each one of the processes involves a different complexity because the tasks (activities) designed by NeuronUP start from simple levels in which the activity in its most isolated form is put into play, while in complex levels of those same activities, the neurocognitive processes are combined depending on internal attentional control (demand) that the subject must maintain. We have distinguished the
Cerebellum functions as a hub between
cinguloopercular and frontoparietal
networks, acting as an error-detecting
mechanism
Default-mode network

NeuronUP Theoretical framework: General Concepts
24
following functions:
• Perceptual speed: refers to the speed of processing. While origi-nally this variable was included in the visuospatial skills, the fac-torialization carried out by Miyake et al. (2000) demonstrates that the executive demand in this kind of tasks is very low in compari-son to other visuospatial processes that require working memory.
• Sustained attention: is the ability to maintain a continuous focus of attention.
• Selective attention: is the ability to focus on a stimulus while dis-criminating other environmental stimuli.
• Alternating attention: is the ability to alternate two (or more) cognitive sets, which in turn requires the ability to maintain them in the phonological loop.
• Heminegligence: Inability to alternate, orient, and/or direct the focus of attention from a sensory hemifield—visual, auditory, body, etc.—to the oppo-site (usually the affected hemisphere is the left one). We consider that, although heminegligence can be considered a problem of spatial orientation (Lezak, 2004), there is also literature that considers it an atten-tional disorder for its therapeutic approach (Sohlberg
& Mateer, 1987, among others). We distinguish this disorder from those problems in the orientation of somatic hemifields that in-volve a lack of recognition of the body schema.
Models used to design materialsThere are several main models we use to base our rehabilitation of atten-
tion on. Before explaining these models, it is necessary to remember that at-tentional processes are not separated from other functions such as memory, executive functions or social cognition, and they are the anatomic functional basis to all of those:
• Orientation Remediation Module developed by Ben-Yishay (1987): reaction time tasks; attentional control and awareness of attentional processes; maintenance of attentional processes; atten-tional control processes and alternation.
• Attention Process Training Programs (Sohlberg & Mateer, 1987): we utilize a concept in which tasks are hierarchically ordered ac-cording to their difficulty levels that finally include complex com-ponents of attentional control and working memory. The authors conceptualize the rehabilitation of attention from specific sub-processes that define it.
• Specific attentional skills training
• Time Pressure Management Fasotti, Kovacs, Eling & Brouwer (2000)
• Metacognitive strategies (Ehlhardt, Sohlberg, Glang, & Albin, 2005)
Neurocognitive processes are combined
depending on internal attentional control (demand) that the
subject must maintain

NeuronUP Theoretical framework: General Concepts
25
AgnosiasClinical syndromes characterized by a failure of recognition that cannot
be attributed to the loss of primary sensory function, inattentiveness, gen-eral mental impairment, or lack of familiarity with the stimulus (Frederiks, 1969), and neither attributed to deficits in aphasia. Agnosias are sensory modality specific: the access to recognition can occur through a different sensory modality.
In Neuropsychology there is a problem in the conceptualization of per-ceptual disorders that could be labeled as historical. Since the concept was formulated, it has not yet been clarified whether the gnostic problem or dis-order is due to an alteration in the memory store, to a perceptual alteration, or even to an attentional problem.
In this section we will principally focus on visual agnosias for we con-sider them as the most disabling since we are beings that process the external world mainly through vision.
Visual agnosias The difficulties in the formulation of a theory of visual recognition have
not been resolved, despite attempts by several authors to develop approach-es regarding the phenomenon. This dichotomy derives from two schools of thought: one based on a computational analysis of visual perception, and another based on neuropsychological data that seeks to corroborate a theory of visual perception.
Thus, Marr and Nishihara’s representational model (1978; Marr & Vai-na, 1982) proposes a computational solution that has received empirical sup-port, but not enough to be completely corroborated. Biederman’s “geons” (geometric ions) model has more psychophysical support than Marr and Nishihara’s, but the theory is not clear in regards to the quantity of existing primitive geons and this makes it less accessible. During the era of compu-tational theories of vision, there are references to the high-level analysis but not to the lower levels of visual processing.
At NeuronUP we accept as valid (due to the amount of empirical sup-port) an extension of Marr and Nishihara’s model, specifically, Humphreys and Riddoch (2001). We also consider that there is enough empirical evi-dence to take into account alternative models such as Farah (2004), or War-rington and Taylor (1978).
Warrington and Taylor propose a model that overlaps in some way with the apperceptive and associative agnosias proposed by Lissauer. A visual analysis takes place during the first stage of the perception process and is carried out in the same way in both hemispheres. The next stage is termed perceptual categorization and represents those processes that enable object constancy by establishing that two different views of an object are in fact

NeuronUP Theoretical framework: General Concepts
26
representations of the same thing. After perceptual categorization comes semantic categorization. This involves the attribution of meaning to the percept.
To Farah, there are two independent recognition systems: one based on part-based processing (that analyzes the parts of the object based on stored representations of such characteristics) and another system based on holistic processing (that analyzes the match between the stored holistic representations and the input). This is compatible with the structural-de-scription models—part-based system—and with the view-based models—holistic system—. Farah uses these two systems to explain the evidence of disorders of recognition, which are explained based on the dysfunction of these two systems:
- Prosopagnosia responds to a dysfunction in the ho-listic system.
- Alexia responds to a dysfunction in the part-based system.
- Object agnosia is explained based on a partial dete-rioration of one or both systems. The deterioration is defined by the degree to which an object is recognized on the basis of configural or featural information.
Therefore, Farah proposes a viewpoint continuum in which the extremes are the analysis systems that explain pure syndromes. The difference in intensity between both extremes would explain the diversity of gnostic deficits.
According to Kolb and Wishaw, there are several theo-ries that establish relations between neural networks and specific aspects of spatial behavior. Thus, the dorsal stream subserves “vision for action”, un-consciously guiding the actions in space in relation to the distribution of the objects and ourselves in space (thereby involving egocentric spatial behavior). On the other hand, the ventral stream subserves “vision for perception”, consciously guiding the actions in relation to the identity of the objects (in-volving allocentric spatial behavior).
Humphreys and Riddoch’s model (2001) is an extension of Marr and Ni-shihara’s, complementing it with a series of intermediate steps and including the integration of top-down and bottom-up perceptual processes. In the first stage there is a processing of the basic features of the stimuli (color, form, depth, motion) generating a primal sketch (from the perceptual representa-tion systems—see Schacter, 1994). In the second stage, a general contour of the object is sketched in 21/2D to afterwards represent a 3D sketch to per-ceive the object in a canonical view (although objects can be also recognized by salient features in non-canonical views). Once we gain access to stored knowledge about the features of the object, we search in the memory traces for two types of information: one regarding the object’s form, and the other regarding its semantic characteristics.
A special case of visual processing is that of face processing, for which the reader can refer to Ellis and Young (2000) and to Marta Farah’s theory.
7
21
19
V5(MT)
V1
V2V3
V4VP
18
17
22
‘What’ v
entral s
tream
‘Where’ dorsal stream

NeuronUP Theoretical framework: General Concepts
27
Types of agnosias
Apperceptive • Characteristics
- No access to the perceptual structure of visual sensations.
- Subject can neither draw nor match.
- Awareness of the deficit.
- Search for features of the object that can lead to recognition but are usually sources of constant error.
- In mild forms (of apperceptive agnosia): errors in the identifi-cation of overlapped images.
- Location: heterogeneous, unilateral or bilateral posterior le-sions; damage can be extensive and diffuse—lesions are local-ized in the posterior parieto-temporo-occipital area bilaterally although sometimes lesions are focal, and affect the inferior temporooccipital gyri, the lingual gyrus and the fusiform gyrus.
The apperceptive nomenclature for all deficits observed is not exhaustive. Many patients show specific deficits and can perform some perceptual tasks while not others (e.g., the patient can discriminate forms and not object-depth discrimination).
- Form agnosia
- Transformation agnosia / Perceptual categorization deficit: in-ability to recognize objects from their non-canonical or unu-sual view.
- Integrative agnosia: inability to recognize the overall relation between the details of a whole. Object-decision tasks with sim-ple line drawings and silhouettes.
- Simultanagnosia: inability to recognize complex images while perceiving the details, parts or the isolated objects but without being able to integrate the parts into a coherent whole; subjects cannot see more than one object at the same time.
• Dorsal: results from bilateral parieto-occipital lesions; related to oculomotor disorders.
• Ventral: due to left temporooccipital lesions; associated to perceptual problems.
Objet
Sensorial treatment
Feature analysisand shape analysis
Egocentric representation
Primary sketch
21/2 Sketch
3D representation
Object-centered representation
Memory structural representation
Semantic representation
Semantic representation
Perceptive stagesAssociative
and semantic stages
Humphreys and Riddoch´s (2001) Model for visual perception
NeuronUP Theoretical framework: General Concepts
28
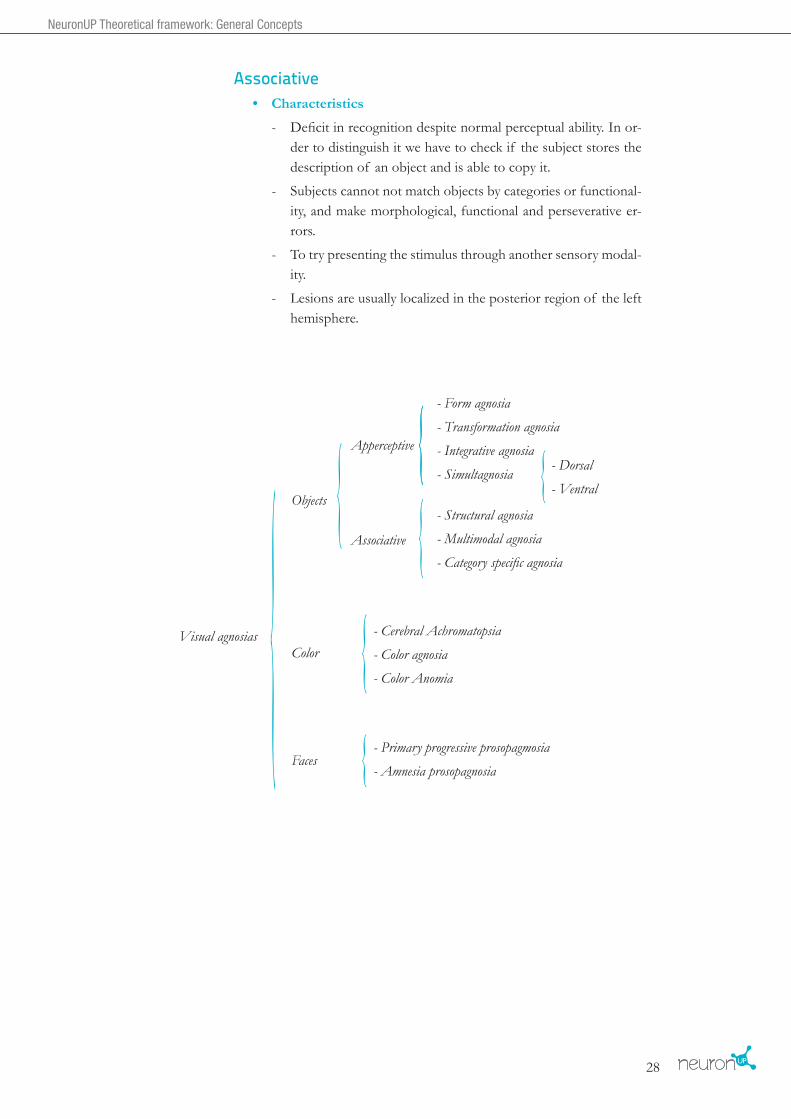
Associative• Characteristics
- Deficit in recognition despite normal perceptual ability. In or-der to distinguish it we have to check if the subject stores the description of an object and is able to copy it.
- Subjects cannot not match objects by categories or functional-ity, and make morphological, functional and perseverative er-rors.
- To try presenting the stimulus through another sensory modal-ity.
- Lesions are usually localized in the posterior region of the left hemisphere.
{ { {
{ {
{ {Visual agnosias
Apperceptive
- Form agnosia
- Transformation agnosia
- Integrative agnosia
- Simultagnosia
- Structural agnosia
- Multimodal agnosia
- Category specific agnosia
- Dorsal
- Ventral
- Cerebral Achromatopsia
- Color agnosia
- Color Anomia
- Primary progressive prosopagmosia
- Amnesia prosopagnosia
Associative
Color
Faces
Objects

NeuronUP Theoretical framework: General Concepts
29
• Structural: failures in the structural representation of objects. Tac-tile recognition is preserved. Subject can make copies of drawings. Real objects better recognized than images. Bilateral lesion of lin-gual and fusiform gyri.
• Multimodal: failures in the recognition of objects and their func-tions. Perseverative and semantic errors in naming. On verbal command, the subject is unable to mime the use of objects. It is typical that access does not occur through other sensory modali-ties. Drawing performance is poor, as well as the descriptions of objects in contrast to the abstract words. Lesion in BA39—left angular gyrus—or in its afferent pathways, the lingual and fusi-form lobes.
• Category-specific: deficit at the level of structural description sys-tem or at the level of accessing such system. Dissociation between object recognition and action recognition. The deficit contrasts with the preservation of verbal knowledge in object naming from its verbal definition. Deficit in semantic memory may exist.
Disorders of color recognition and cerebral achromatopsiaSubject is unable to name colors visually presented or unable to select a
color named by the examiner.
- Cerebral achromatopsia: inability to perceive color in all or in a part of the visual field. It results from unilateral or bilateral lesions in the inferior ventromedial sector of the occipital lobe, the lingual and fusiform gyri, specialized regions of the brain for the encoding of color.
- Color agnosia: failure to match colors with objects.
- Color anomia
ProsopagnosiaInability to recognize and/or integrate facial features into a recognizable
or coherent whole.
- Usually bilateral temporo-occipital lesions, although it can result from right unilateral lesion of the occipito-temporal junction in connection with the right parahippocampal region.
• Primary progressive prosopagnosia
• Amnesic prosopagnosia

NeuronUP Theoretical framework: General Concepts
30
Other types of agnosia based on sensory modality
{ {
{ {
{
Agnosia based on sensory modality
A. Tactile agnosia- Apperceptive
- Associative
- Digital agnosia
- Asomatognosia and hemiasomatognosia
- Autotopagnosia
- Verbal
- Non-verbal:
B. Olfactory agnosia or anosmia
C. Auditory agnosias
D. Gustatory agnosia
E. Supramodal spatial defects
F. Anosognosia: relation between agnosias and awareness [see in executive functions]
G. Imaginative pro cesses (multimodal, dependent on working memory).
- Cortical deafness
- Cortical auditory disorders
- Pure word deafness
- Sound agnosias
- Amusias
- Paralinguistic agnosias. {

NeuronUP Theoretical framework: General Concepts
31
Models used to design materialsThere is not a specific model to rehabilitate agnosias, since they depend
on each specific modality. However, there are specific techniques for the compensation of functional deficits caused by agnosia. In this sense, al-
though it is probable that the rehabilitation models based on virtual reality and hardware may improve the rehabili-tation of some types of specific agnosia (especially spatial and tactile agnosias, and imaginative processes), software can also be applied to the rehabilitation of visual and au-ditory agnosias, and even helps in the interventions of other modalities.
The goal of our activities is to favor visual scanning and discrimination of visual features (visual agnosias); construction and discrimination in 3D; to
associate auditory stimuli and specific forms/objects/persons by means of discrimination strategies; to differentiate words from non-words, etc.
To that end, we carry out specific training of visual exploration by design-ing materials that can be analyzed by using self-instructions.
- Design of cutout materials that can be used to discriminate forms, to make a step-analysis of the differential features of the object, to estimate depth, etc.
- Discrimination of shades of colors.
- Hue-discrimination tasks.
- 3D construction tasks.
- Discrimination between similar salient stimuli.
- Activities in which there can be recognizable stimuli in order to discriminate similar objects of different na-ture (dangerous vs. safe objects).
- Design of drawings and maps for spatial orientation.
- 3D puzzles.
- Design of programmes for discrimination within and between spatial hemifields.
- Design of instructions and guidelines for object analysis.
The goal of our activities is to favor visual scanning and
discrimination of visual features
We carry out specific training of visual
exploration by designing materials
that can be analyzed by using self-instructions.

NeuronUP Theoretical framework: General Concepts
32
ApraxiasClarification: Those disorders apparently praxic that are due to a deficit or im-
pairment of the conceptual system (involving knowledge) of objects (i.e., the subject does not know that X is a tool) are not included. Other aspects of the conceptual sys-tem involved in praxis are included: motor act schemas using tools, objects, or ex-ecution of movement with body parts, recognition of gestures and motor planning (Sequencing in motor execution). In addition, deficits in executing motor com-mands in relation to space-time are included—production system. Sensory deficits or deficits due to bradykinesia or other motor disturbances are not included, nor are disturbances in comprehension, executive functioning (planning), or deficits in intelligence.
Apraxia is not a disorder due to the loss of the ability to find meaning in objects, nor to a primary motor dysfunction. Apraxia is a heterogeneous deficit of cognitive-motor nature, in which the ability to execute or carry out purposeful movements is disturbed, not attributable to deficiencies in understanding, agnosia or motor problems (tremor, ataxia, posture distur-bances).
Apraxia is strongly associated with corticobasal degeneration, lesions in the left hemisphere, and dementia.
Despite its importance in clinical reality, the problem in the formulation of apraxias is much worse than in the formulation of agnosias, as previ-ously mentioned. This is due to two aspects: on the one hand, the original description of the concept (Liepmann, 1900); and on the other hand, the extensive distribution of the main anatomical networks that support this function (frontotemporal and frontoparietal circuits—“mirror neuron sys-tem”—, basal ganglia, cerebellum and white matter).
Apraxia modelsA model widely used in the explanation of apraxias
is the one proposed by Rothi, Ochipa and Heilman (Jun-qué, 1999); this model distinguishes two visual pathways to access information (imitation and object action) and one verbal pathway (action performed to command). Vis-ual and auditory analyses enable access to input lexicons, while the output action lexicon is responsible for the pro-duction and execution of movement. The types of motor actions that are altered in apraxia are:
o Transitive movements: related to the use of objects.
o Intransitive movements: related to the execution of symbolic gestures, nonverbal communication [meaning-ful], or intransitive meaningless gestures [imitation].
Visual / ObjectInput
Auditory / VerbalInput
Visual / GestualInput
Visual Analysis
Verbal OutputLexicon
Action OutputLexicon
Auditory Analysis
Phonological Buffer Innervatory Patterns
Motor Systems Motor Systems
Visual Analysis
Object Recognition System
Semantics(action)
Phonological InputLexicon
Action InputLexicon
Apraxia Model by Rothi, Ochipa & Heilman (Junqué, 2009)

NeuronUP Theoretical framework: General Concepts
33
Types of apraxia
IdeomotorSpatial and temporal components of motor execution: action programs,
execution of motor act (spatial and temporal).
IdeationalConceptual component of motor execution: knowledge of object’s pur-
pose, knowledge of actions, and knowledge about the organization of ac-tions into sequences.
Buccofacial and ocular
Buccofacial: ability to perform intentional movements with facial struc-tures including the cheeks, lips, tongue and eyebrows.
Ocular: eyelid apraxia and ocular apraxia are included. Eyelid: ability to perform eyelid movements. Ocular: ability to perform saccadic eye move-ments on command.
VisuoconstructionIt is the ability to perform the motor act, correctly distributing (the
whole-part relationship) the execution of movement in its spatial and tem-poral parameters. It requires planning—in relation to visuospatial estimates of the object made by the subject—to execute the action. The difference with planning (in EF) is that this is a specific case that involves the motor act and its execution, while that (EF) involves semantic and temporal estimates of acts, but not necessarily the execution of motor engrams. In this section are included Visuospatial Skills that involve motor execution and mental transformations with objects, as long as they have no relation to transforma-tion agnosia.
Brief considerations on apraxias: An alternative classification accord-ing to neuropsychological assessment may be established (transitive gestures, intransitive gestures, gestures to imitation, gestures to command, with tools, spontaneous gestures, single acts, serial acts). This classification could also be complemented with the models proposed by Cubelli et al. (2000) or with the model of Buxbaum & Coslett (2001).
Clarification: Language disorders such as apraxia of speech and apraxic agraphia are not included in this section, although some authors conceptualize them as dis-turbances in the execution and/or conceptualization of the motor engrams for speech production. This type of disorder is discussed in the section of Language.

NeuronUP Theoretical framework: General Concepts
34
• Basal ganglia: they are important nodes for movements, and their function is to regulate and filter neuronal information from oth-er areas (i.e. thalamus) to be processed in cerebral cortex. Basal ganglia have an opposite effect on movement depending on the pathway involved in it. The direct pathway increases the excita-tory drive from thalamus to cortex, turning up motor activity. The indirect pathway decreases the excitatory input from thalamus to cortex, turning down motor activity. Also, basal ganglia have an important role in the reward system, taking part in the prediction of immediate and future rewards (Tanaka, Doya, Okada, Ueda, Okamoto, & Yamawaki, 2004)
• Parietal lobe (areas 5 and 7): area 5 is especially involved in the manipulation of objects, while area 7 is involved in visuospatial skills regarding movement.
• Left inferior parietal lobe: stores engrams that are automatized with each experience; when we per-form automatic movements in order to make deci-sions, these areas are a “store” where patterns of pre-viously learned movement can be found.
• Brodmann areas 39 and 40 (left angular and supremarginal gyri): are multimodal or polymodal ar-eas that are important for the integration of sensory information which allows to transform the representa-tions into movement.
As we move towards an anterior pole of the brain, functions become less automatized and involve high-level cognitive processes (planning, temporal sequencing, re-trieval of memory schemas, decision making, flexibility).
Functional systems in apraxiaThe functional systems involved in apraxia are diverse. We can distin-
guish up to six systems involved in movement. Each one of those systems has a functional specificity, but as in the case with attention, movement is an activity composed of interrelated subprocesses.
• Cerebellum: is involved in the fine-tuning of movements and its temporospatial execution. It is a node that contains motor learning and assists in correcting movements, by carrying out monitoring.
96
64
45
7a
7b40
39
4446
4547
11
9
Prefrontal cortex:
Precentral gyrus
Motor Cortex
Parietal lobe
Cerebellum
Brodmann areas 39 and 40
(left angular and supremarginal gyri)
{ { { { {Basal Ganglia
- Corpus Striatum
- Substantia nigra
- Subthalamic nucleus
(Amygdala = Limbic)
Striatum (Neostriatum)
Globus pallidus
Caudate
Putamen
- External segment
- Internal segment
Lenticular nucleus
Basal Ganglia (a) and Neocortical Areas involved in movement

NeuronUP Theoretical framework: General Concepts
35
• Cortico-thalamic-basal ganglia loop: supplementary motor area, premotor cortex and primary motor cortex. It is an articulatory loop of motor nature, a network that processes movements at a high cognitive level to send them to the different nuclei responsi-ble for motor execution.
• Prefrontal cortex: carries out the necessary computations for deci-sion making regarding movement, adapts motor strategies, monitors the feedback of the motor act, and generates patterns of movement.
Strategies for the rehabilitation of apraxias
Analysis of motor execution in each patient enables the establishment of the specific cognitive processes that are altered. Depending on the al-tered process, during rehabilitation an emphasis is put on one or another technique. It is also relevant to establish the type of behavior to be reha-bilitated. In some occasions, the goal of rehabilitation is the imitation of gestures, while in other cases the goals are to carry out purposeful sequences or rehabilitation involving the use of a particular tool. In any case, the goal (Buxbaum et al., 2008) should not be to cure apraxia, but to compensate for impairments, to aim at enabling independent function, and to minimize the extent to which apraxia influences performance of daily life.
The treatment of apraxia (and other deficits involving spatial functions) usually includes proprioceptive stimulation.
There are two main approaches in the rehabilitation of apraxia (Edman, Webster, & Lincoln, 2000): generaliza-tion of the training, and functional approximations. Generalization of the training begins with the notion that a patient can generalize the training in a functional area that is characterized by simple content and functional ac-tivities more complex but similar.
Functional approximation aims at rehabilitating or compensating the symptom rather than the cause, and
employs specific activities of daily living. Both models have been used in the activities that we have designed.
The materials are designed with the purpose of being meaningful and entertaining for the subject undergoing rehabilitation, establishing the se-quentiality of actions, and the adaptation of those motor sequences to changing contexts.
For behavioral rehabilitation we have conceived a project in which the subject can see his/her actions simultaneously on the computer through axes that divide space, so that the subject receives immediate feedback about his/her performance.
The goal should be to compensate for
impairments, to aim at enabling independent
function

NeuronUP Theoretical framework: General Concepts
36
The principles that guide the design of materials are shaping, chaining, successive approximations, and errorless learning (although in many apraxias, the cerebellum is preserved and capable of storing new learnt in-formation, so that in order to receive feedback and train movements errorful learning may be required).
We have also incorporated some techniques and aids into the activities and are considering the possibility of introducing personalization into the
instructions used for the analysis of movement sequenc-es, the cues in the execution of movement sequences, the use of imitation and the possibility to incorporate in the platform videos featuring imitation and repetition. One of the future goal in the rehabilitation of apraxia is the systematization of multiple behaviors with the possibility of personalizing the successive approximations.
Functional approximation employs
specific activities of daily living
NeuronUP Theoretical framework: General Concepts
37
Visuospatial skills
Visuospatial skills are the abilities to perceive, apprehend and manipulate an object mentally. Since they are abilities requiring intrapsychic orienta-tion and mental manipulation of spatial elements, we distinguish them from perceptual skills—addressed under visual agnosias—location in space—ad-dressed under orientation and body agnosias—and from the spatial compo-nent of movement—addressed under apraxias.
Therefore, visuospatial skills are a specific component of visuospatial function that deals exclusively with perception, apprehension and manipula-tion of mental objects. Alterations in visuoconstructive skills are “distur-bances in formulative activities, in which the spatial form of the product proves to be unsuccessful without there being an apraxia of single move-ments” (Benton, 1969). They are associated with lesions of the nonspeech hemisphere of the brain, and frequently appear with defects of spatial per-ception. These deficits are among the most probable dysfunctions following damage to the parietal lobe, independently of the hemisphere. They involve an alteration in the ability to construct two-dimensional or three-dimension-al forms. Occasionally they seem to be associated with defects in perception. Lesions of the right and left hemisphere tend to have different effects on construction.
Visuospatial skills: Visuoespatial working memory
Visuospatial working memory is considered a subcomponent of working memory, related but not overlapped with executive functions. The visuos-patial sketchpad serves as a working system with limited storage capacity, is not specific (of a sensory modality), and is capable of integrating visual and spatial information into a unitary representation (Baddeley, 2007). Visuos-patial processes (less automatized than verbal processes, composed of less familiar items, and with a more complex verification process of the result)
demand greater executive involvement and therefore are more sensitive to disruption during the performance of other tasks that require greater attentional/executive load.
Miyake, Friedman, Rettinger, Shah, & Hegarty (2001) have proposed a triple functional model composed of: spatial visualization, spatial relations, and visuospatial perception. Spatial visualization comprises processes of apprehending, encoding, and mentally manipulating spatial forms (3D). Spatial relations (rotation) are men-tal transformations that involve manipulations of two-
Visuospatial processes demand greater executive involvement and are more
sensitive to disruption during the performance of
other tasks

NeuronUP Theoretical framework: General Concepts
38
dimensional objects, and in which speed is a relevant factor. Mental rotation involves two processes: first, the representation of an object; and second, the mental transformation of that representation, so that the resulting fig-ure is compared with the original. Finally, visuospatial perceptual speed is the speed and efficiency to make perceptual judgements involving no spatial transformations. The three factors are separable but they are correlated.
These processes differ in the degree in which they demand executive components (factorially determined by oxygen concentration in brain areas). Spatial rotation tasks are found at a halfway point of executive demand. By contrast, spatial visualization tasks require greater executive control while visuospatial perception tasks require lesser executive demand. The greater the executive demand of the process is—in terms of attentional control and mental manipulation—the greater the relationship with reasoning and psy-chometric intelligence (Conway, Kane, & Engle, 2003).
Due to the aforementioned, we have included the first of the three factors in the function of attention, since it requires low executive demand and are processes dependent on reaction times.
Anatomical bases of visuospatial skillsVisual imagery and retention of objects are crucial
to understand the anatomical bases of visuospatial skills. Although the current consensus is that visuospatial func-tions share the neural substrates of visual functions, there is also a visuospatial function that manipulates stable visu-al representations independent of visual inputs (Moulton & Kosslyn, 2009), transforms them and verifies the re-sponses to the situations. This skill is strongly related to working memory.
Therefore due to its multifactorial nature it is necessary to understand that these functions are found throughout large-scale neural networks that involve the entire brain. Because visuospatial skills depend on working memory com-ponents, we consider that the dorsolateral prefrontal cortex is fundamental to execute this type of processes. Besides, the right parietal cortex contains spatial schemas that allow the spatial analysis of objects and even the spatial component of numerical sequences. Left hemisphere lesions cause distur-bances in the sequence of the necessary movements for constructional ac-tivity. Right hemisphere lesions result in the alteration of spatial relations or mental manipulation of spatial relations.
Finally, since this type of cognitive deficits needs to be treated (sometimes even before motor rehabilitation), all the structures involved in movement should be taken into account (i.e., the cerebellum, an important component in mental spatial rotation) (Molinari, Petrosini, Misciagna, & Leggio, 2003).
Visuospatial function manipulates stable visual
representations, transforms them and verifies the
responses to the situations

NeuronUP Theoretical framework: General Concepts
39
Rehabilitation of visuospatial skillsThe materials designed for the rehabilitation of visuospatial abilities are
hierarchical (in terms of analytical complexity) and are based on techniques that have demonstrated effectiveness (Cicerone et al., 2000). As mentioned by Weinberg et al. (1979), deficits in visuospatial skills can improve with treatment on multiple levels of visuospatial processing, and can be benefi-cial to use tasks involving complex academic skills, visual processing tasks, and manipulative tasks in order to yield solid, generalizable results. Some of the techniques that we have used to design our materials are:
- Visual scanning training and visual analysis.
- Rotations of three-dimensional objects.
- Aids for the analysis of visual components.
- Training in the analysis of the stimuli main features such as depth, size and distance between objects.
- Training in visuospatial orientation.
- Simple and complex visuospatial organization training.
- Somatosensory awareness training (recommendations).
- Training in spatial organization skills.
- Visual imagery techniques.
Materials allow the training of visuospatial skills at various levels. In ad-dition, materials include not only entertaining tasks involving abstract ele-ments, but that are also meaningful to the subject performing them. Thus, we design activities that also integrate visuoconstruction with dimensional materials (3D) to form real elements and spatial cues for reading, among others.
As can happen with praxis, many of these materials are used to acquire strategies with which to compensate for the deficits rather than to cure the problems, and to aim at teaching generalizable strategies for daily life. The training of visuospatial skills in persons with heminegligence, accompanied by training in visual scanning, is a recognized and effective practice that allows for generalizing results in various areas of life (educational, employ-ment, reading, activities of daily living, etc.) (Gordon, Hibbard, Egelko, Diller, Shaver, & Lieberman, 1985), being the stage-by-stage intensive prac-tice the best strategy possible.

NeuronUP Theoretical framework: General Concepts
40
MemoryMemory is the ability to effectively retrieve previously learned informa-
tion (encoded and stored). According to Wilson (2009), memory can be conceptualized in different terms: as memory dependent on time; as mem-ory dependent on the type of information; as modality-specific memories; as stages of recall, retrieval or recognition; as implicit or explicit memory; or as retrograde or anterograde memory. Next, we briefly present the model developed by Larry Squire. Nevertheless, we would like to emphasize that models focused on memory processes also play an important role (since
they complement system models) and that even if this approach is not explicit in the conceptual framework of the platform, it has been taken into account in the design of materials.
SystemsSquire (1987) proposes a schematic representation
in which memory systems are broken down based on whether theirs contents can be verbalized (declarative memory), in contrast to a procedural knowledge without the need for conscious retrieval processes (non-declara-tive memory).
Declarative memory distinguishes between facts (se-mantic memory) and events (episodic memory).
The properties of each system are:
• Declarative memory: conscious recollection of events and facts; allows information to be compared and contrasted; encodes memories in terms of the relation-ships among multiple items and events; is composed of flexible representations, and autobiographical experienc-es and knowledge about the world. Declarative memory is either true or false. Propositional. Principle of exclusivity (what is distinctive about the item or the event).
• Procedural memory: is neither true nor false (it does not possess that characteristic); is dispositional and does not recollect events but performs and processes be-
haviors. This type of memory occurs as modifications within spe-cialized performance systems; is activated through reactivation of the systems involved in the original learning. Principle of common-ality (extraction of common elements). Procedural memory is an automatic process, an implicit knowledge that facilitates the execu-tion of motor tasks.
Basal forebrain
Mamillary body
Prefrontal cortex
Fornix
Thalamus
Rhinal cortex
Hippocampus
Amygdala

NeuronUP Theoretical framework: General Concepts
41
Both types of memory serve distinct purposes and are functionally in-compatible despite being related, which satisfies the criteria for postulating memory systems formulated by Tulving. They operate in parallel to support behavior in such a way that if one form of knowledge is damaged, the other
can take control to maintain the necessary learning in a different format. For other proposals on this topic, the reader can consult the Moscovitch (1994), who proposes three modular, domain-specific components of memory and a frontal central-system, each of which mediates pro-cesses that dominate performance on different memory tasks (see model below).
According to Damasio´s Theory of Convergence Zones (1989), the early and intermediate posterior sensory cortices “contain fragmentary records of featural components which can be reactivated, on the basis of appropri-ate combinatorial arrangements”. The patterns of neural activity that cor-respond to distinct physical properties of entities are recorded in the same neural ensembles in which they occur during perception, but the binding codes that describe their spatial and temporal coincidences are stored in sep-arate neural ensembles called convergence zones. Convergence zones trigger and synchronize neural activity patterns corresponding to topographically organized fragment representations of physical structure, that were perti-nently associated in experience, on the basis of similarity, spatial placement, temporal sequence, or temporal coincidence, or combinations thereof.
Processes
Models focused on memory processes
complement system models
{ { { {
{
}Memory
Medial temporal lobe diencephalon
Reflex pathways
Neocortex
Striatum
Cerebellum
Amygdala
- Declarative
- Nondeclarative
- Facts
- Events
- Emotional responses
- Skeletal responses
- Nonassociative learning
- Simple classical conditioning
- Priming and perceptual learning
- Procedural (Skills and habits)
Memory Systems
Memory Systems (II) according to tasks, another interpretation of
memory function distribution.Event / Cue
Conscious Awareness
Enconding/Ecphory(Hippocampus and related limbic structures)
Non-ConsciousProcedural
Systems
Control or Executive Systems
(Frontal Lobes and Related Structures)
PerceptualAnd Other Modules(Non-Frontal Cortex)

NeuronUP Theoretical framework: General Concepts
42
Memory processes are carried out in order to learn/encode, store or re-trieve information which is done through, from or for the memory systems. Memory processes are divided into:
• Processes of acquisition and storage: implicit, associative, procedur-al, elaborative, and constructive processes.
• Processes of retrieval: activation and fluency, familiarity, associative search, constructive, and inferential retrieval.
• Processes of forgetting: decay, interference, inhibition, distortions.
• Processes of consolidation and reconsolidation.
Functional systems of memoryOur conception is similar to the memory trace theory proposed by
Damasio.
Medial temporal lobe structures are necessary to archive declarative in-formation and to recall it during a limited period of time. However, con-solidated declarative information ends up being independent of the hip-pocampus, distributing itself throughout the cerebral cortex, and depending upon every characteristic of the encoded information. Different areas of the brain are involved in remembering. In the first place, the hippocampus is responsible for implementing an algorithm that is a storage code of the distributed information. In Squire’s model, declarative memory depends on the hippocampus while non-declarative memory does not. In this model, the prefrontal and parietal cortices would be involved in working memory processes; procedural memory would depend on the basal ganglia; instru-
mental conditioning on the basal ganglia and cerebellum, and classical conditioning might depend on emotional priming, in such way that the activation of the amygdala triggers a rapid associative memory process.
Junqué (2009) provides an anatomical model for the explanation of memory. For information processing to persist as long-term memory, medial temporal lobe struc-tures must mediate the process. Damage to this structure could result in retrograde amnesia. Projections from the neocortex arrive in the hippocampal cortex and perirhinal cortex; further processing occurs next at the entorhinal cortex, and in the several stages of the hippocampal for-
mation (CA3 and CA1, dentate gyrus). This connectivity provides the hip-pocampus with access to cortical activity at widespread sites throughout the neocortex. The information can then return to neocortex via the subiculum and entorhinal cortex.
Information processed in the medial temporal lobe is also sent to critical areas for memory in the diencephalon and from here to the anterior nucleus of the thalamus via the mammillothalamic tract. The dorsomedial thalamic nucleus and the projections from the amygdala receive information from
HIppocampal fissure
Optic tract
Tail of the caudate nucleus
Inferior portion of the temporal lobe
Hippocampus
Inferior horn of
the lateral ventricle

NeuronUP Theoretical framework: General Concepts
43
perirhinal cortex.
The prefrontal lobe is an important target of diencephalic and medial temporal lobe structures. The anterior thalamic nucleus and the dorsome-dial thalamic nucleus send projections to both ventromedial and dorsolateral frontal cortex. Additionally, the entorhinal cortex and the subiculum send prominent projections to ventromedial cortex.
Medial temporal lobe structures and the medial thalamus are compo-nents of the memory system that is essential for long-term declarative mem-ory. This system is required at the time of learning and during a period of time thereafter, while the process of consolidation slowly develops in the neocortex, presumably thanks to sleep.
Short-term memory is independent of this system. Habits, skills, prim-ing and some forms of conditioning are also independent of the medial temporal structures and the medial thalamus. Procedural memory depends on the frontoparietal system, the neostriatum and the cerebellum. Perceptual priming depends on posterior cortical areas.
Principles and techniques for the rehabilitation of memory
PrinciplesUsing specific techniques to design rehabilitation materials requires
knowledge of some basic principles of memory training that serve to im-prove the process of information acquisition and its retrieval in every sub-ject. To employ any technique on any subject is neither useful nor practical for the professional. The first thing to be done is we have to adapt the strate-gies and materials to our subjects. According to Wilson (1989):
- Material must be simple, with reduced load of information—at least, in the initial phases, we believe.
- Instructions must be clear and concise.
- Subject must understand the instructions.
- Material must be adapted, both in form and language employed.
- Associations must be established between elements previously known (persons, songs, contexts, dates, activities) and elements to be learned.
In addition, at NeuronUP we follow the levels of pro-cessing theory proposed by Craik & Lockhart (1972), by which we consider subjects to be active manipulators and not passive recipients of learning. To design significant material that is linked to daily life situations is a principle that can also adapt to the levels of processing postulates.
TechniquesOn the one hand, there is the training in internal mem-
We have to adapt the strategies and
materials because we consider subjects active
manipulators

NeuronUP Theoretical framework: General Concepts
44
ory strategies; on the other hand, the environmental adaptations and exter-nal aids. The activities we design are based on both realities but also have different treatment depending on the type of activity or tool that is going to be designed.
Training in internal strategies of encoding, storage and retrieval
• Verbal
- Organization: encoding strategies such as grouping words/items into distinct categories, or phonetic strategies—less ef-fective. To adapt the stimuli to the patient.
- Association: to give a semantic context to the processed infor-mation, to make up stories, rhymes, songs (auditory process-ing), contextual association, etc.
- Acronyms (a word formed from the initial letters of a name or thing) and mnemonics.
- Errorless learning.
- Backward chaining (the method of vanishing cues).
- The spaced retrieval technique (Landauer & Bjork, 1978) with distributed practice (Baddeley, 1999).
- Repetition.
- Trial-and-error (is not the most effective method but occasion-ally can generate results).
• Visual
- Visualization: paired-associate technique in order to form im-ages. Words and drawings. Generation of visual strategies for memory improvement.
- Method of loci (places or locations).
Environmental adaptations and external aidsThey are methods and devices aimed at establishing adaptations in the
environment, so that demands on memory are reduced to more manageable levels.
- Training in the use of labels with images, colors, names, words, etc.
- Devices that facilitate access to previously stored information: alarms, timers.
- To record information: tape recorders or personal digital assis-tants (PDAs). Design of memory aids through which to easily access relevant information.
- Sometimes the use of these strategies requires training the pa-tient’s immediate environment.
The main characteristics of these kinds of adaptations are:

NeuronUP Theoretical framework: General Concepts
45
- Active, timely and specific (simple commands)
- Easy-to-train.
- Generalization to other situations is easier.
- More effective than internal strategies: aimed at reducing the de-mands on the patient’s memory.
- Very useful in the most severely impaired patients. Notebooks and PDAs (personal digital assistants)
- It is more effective when the patient, despite memory problems, has:
o Average or above average intelligence
o Reasoning (ability)
o Awareness of deficits
o Skills to initiate behaviors
Training in the use of a memory notebookSohlberg & Mateer (1989): orientation (autobiographical information),
memory (activities to be performed), calendar, tasks, transport, names of known people, work activities, maps. Training stages:
- Acquisition: learning sections, purposes and use of the notebook.
- Application: where and when to use the notebook.
- Adaptation: demonstration of appropriate use of the notebook in naturalistic situations.
Schmitter-Edgecombe, Fahy, Whelan, & Long (1995): personal notes (autobiographical information), diary, calendar, names, work activities…
Training stages:
- Anticipation: identifying memory weaknesses and the need for ex-ternal aids.
- Acquisition: learning the purpose of each notebook section.
- Application: how to take notes.

NeuronUP Theoretical framework: General Concepts
46
LanguageLanguage is the ability to produce and communicate thought processes
through motor execution of a system of gestures (nonverbal communica-tion), symbols (writing and reading), and sounds (speech). It is a phenom-enon that requires the coordination of a distributed neural network, with areas that change regarding their functional specificity. Even though the left hemisphere (in right-handers) is dominant for language, lesions of the right hemisphere can also cause language disturbances such as aprosody or the inability to detect intent (ironies). Lesion in each one of the nodes necessary for efficient functioning can cause disturbances in a specific aspect of the linguistic process; these can occur in:
- Encoding
- Production (articulation, execution, modulation)
- Comprehension
- Naming
- Elaboration and organization
- Contextualization
- Motivation
Language disturbances can occur on four levels: syntactic, semantic, pho-nological and morphological.
Language disturbancesTo carry out an exhaustive classification of these dis-
turbances is not the goal of this document. For an ex-haustive classification of the different communication disorders (excluding the autism spectrum disorders) con-sult Junqué & Barroso (2009), or Martinell Gispert-Saúch (2012). Next, we define the main deficits observed in lan-guage: aphasia, alexia, agraphia and aprosody.
Aphasia: loss or disturbance of speech as a conse-quence of acquired brain injury. Deterioration of lin-guistic production and comprehension. The severity of the disorder varies in every area. The main disturbance is found in linguistic processing. It is not a perceptual or motor problem, nor an alteration in the thought pro-cesses. Rather, aphasia occurs when a lesion damages the neural network that allows the transformation of the in-ternal images or thoughts into symbols and appropriate linguistic structures, or prevents the translation of heard words or written text into nonverbal ideas and thoughts.
pIF/dPM (LEFT)
Articulatory-based
speech codes
Area Spt (LEFT)
Articulatory-motor interface
pITL (LEFT)
Sound-meaning interface
STL (bilateral)
acoustic-phonetic
speech codes
articulatory-basedspeech codes
auditory-motorinterface
sound-meaninginterfaceauditory
input
acoustic-phoneticspeech codes
Dorsal stream
Vental stream
abc...
Language processing streams (a) and neocortical areas involved in language (b)

NeuronUP Theoretical framework: General Concepts
47
Alexia: is a disorder of reading subsequent to brain injury in individuals who had previously acquired the ability to read. Thus, it can be distinguished from dyslexia, a disorder that occurs during the acquisition of reading.
Agraphia: a loss, to a greater or lesser degree, of the ability to produce written language as a result of brain injury. In most aphasic patients, the deterioration of writing properties has similar characteristics to the deterio-ration of oral expression.
Aprosody: language disorders that affect normal speech characteristics such as intonation, melody, cadence and accentuations. There are three types of aprosody: hyperprosody (excessive use of prosody), dysprosody (or ataxic prosody, a change in the quality of voice which can result in a “for-eign accent”; this deterioration remains even after recovery from non-fluent aphasia), and aprosodia (limited capacity to modulate intonation).
Classification of language functions
We have partially followed the classification of language functions devel-oped by Lezak (2004).
ReadingAbility to identify and transform written symbols—in a code—into in-
ternal representations. Reading involves the discrimination of symbols and words, their phonetic association, and the comprehension of grammatical relation schemes (phonemes, words, phrases, paragraphs, and texts) in writ-ten language. Reading does not include comprehension, nor is included in Repetition or Spontaneous Language when spoken language is read aloud. It is not form agnosia either (subject is capable of recognizing two identical letters or numbers).
WritingAbility to produce written language that does not include comprehen-
sion. There are three main variants: copying of texts, words or writing texts to dictation, or spontaneous writing.
ComprehensionAbility to understand the semantic meaning when combining sym-
bols (written) or phonemes (spoken language) into grammatical structures (words, phrases, texts, clauses, etc). It does not include the interpretation of linguistic formulas—ironies, double meanings, etc—nor alternative mean-ings of the message (these require Abstraction, such as in the meaning of
¿?

NeuronUP Theoretical framework: General Concepts
48
proverbs). It does not include prosody and does not extent to the perception of emotional tone of the speech.
NamingAbility to name and/or identify objects, persons, activities or actions pre-
sented on visual (drawings or pictures) or verbal confrontation (definitions). The alteration of this ability can arise as a consequence of the total or partial destruction of the semantic storage, or as a consequence of an alteration in word-retrieval abilities (for example, in the phenomenon of linguistic ap-proximation). Anomias which are due to difficulties in comprehension, lan-guage production or recognition failures are not included.
VocabularyQuantity of information relating to words in the semantic storage (quan-
tity of words that the subject possesses).
RepetitionAbility to transform phonemes and activate the representations and mo-
tor engrams of language to produce the same sounds that the subject hears. Sounds can be vocal and non-vocal.
FluencyAbility to produce language (written and spoken) in a rapid and effec-
tive manner. This production depends on two main strategies: a semantic (semantic fluency) or phonetic (phonetic fluency). It entails the preservation of the semantic storage, as well as the representations of the phonological pathway. It also involves Flexibility. There are three types of fluency: spoken
Fluency (spontaneous or not), written fluency, and reading fluency. We do not consider fluency as a main measure of processing speed (therefore reading is excluded), but of production speed. Fluency is not included either as a production measure of complex spontaneous language (in this case it is included in the section of spontaneous Speech), but of words.
DiscriminationAbility to recognize different frequencies, intensities and tones that help
us to identify phonemes, phrases, or identical words –always as a result of linguistic processes- without the need of understanding.
MIAU!
ABC
BLABLE
BLABLE
l FR
P
A
M S
T
¿T?¿D?
¿E?
T
NeuronUP Theoretical framework: General Concepts
49
Anatomofunctional models of languageAccording to Damasio and Damasio (1992),there are 3 major functional
systems in language:
- Conceptual representation system: activates the concepts associated with the record of words. This system depends on extensive cortical areas of different hierarchies and modalities that are distributed in the parietal, temporal and frontal areas bidirectionally (arcuate fasciculus).
- Linguistic representation system (phonemes, words and syntactic rules for combining words): is located in the left hemisphere and in-cludes various areas. The anterior perisylvian sector contains struc-tures that are responsible for the assembly of phonemes into words, and of words into sentences; by contrast, the systems in the posterior perisylvian sector hold auditory and kinesthetic records of the pho-nemes and phoneme sequences that make up words. Comprehension begins in this system, although depends on the access to representa-tion and association areas.
- The mediation system: the left temporal cortex, outside the classical language areas, is the intermediary between the other two systems, the mediator in lexical retrieval. It is involved in the access to the names of people, things, animals, etc.
The authors also insist on the involvement of other areas in this lan-guage system: the basal ganglia and the thalamus, the supplementary motor area and the anterior cingulate gyrus (medial frontal cortex), involved in the initiation and maintenance of speech; and the right hemisphere, involved in verbal automatisms, narrative aspects and prosody.
In addition to the model of Damasio and Damasio, we use the model developed by Marcel Mesulam. For a cognitive model of language, consult the model by Ellis & Young (1992).
Techniques for the rehabilitation of language
Language depends on and supports other cognitive functions. Therefore, language rehabilitation must rely on the preserved processes and functions, while also adapting treatment individually. It is necessary to take into account that language rehabilitation must comprise different cognitive modules and occasionally, neuromuscular training, so that a multidisciplinary interven-tion is important for significant improvement. In addition, language deficits
produce social isolation, so it is necessary to integrate the intervention into the community, without forgetting func-tional communication strategies.
The intervention must be functional but must also fo-cus on the deficits, thus rehabilitation materials must meet both demands; they must focus on situations and activi-
Interventions in language must comprise different
cognitive modules and multidisciplinary intervention

NeuronUP Theoretical framework: General Concepts
50
ties of daily living but combining these tasks with basic aspects of language processing. Daily living situations are usually very useful in the rehabilitation of language, as well as motivating.
The designed materials must fulfill certain principles, especially the re-quired aids to begin treatment. The formulation of written, phonetic, and/or iconic instructions and prompts must be always clear and concise with augmentative communication boards if necessary, and multimedia material.
According to Cuetos (1998), the main language rehabilitation techniques can be divided into:
• Techniques directed at functional recovery: cueing, relearning, reor-ganization based on preserved functions.
• Compensatory techniques: alternative communication techniques and language processing strategies.
We design materials that are based on different stages of language pro-cessing. From the basic stages of language processing (letter discrimination) to the use of metacognition for discourse production.
- Gradual articulation training by means of auditory examples.
- Auditory discrimination.
- Letter-phoneme association and word-picture association.
- Lexical decision tasks.
- Phonological judgements.
- Rhyme training.
- Identification of lexical words.
- Production and identification of meanings.
- Word association.
- Discrimination between phonetically similar words.
- Word articulation tasks (syllables and letters).
- Modulation of prosody with visual external feedback from the sound wave.
- Generalization of repeated words.
- Analysis of conversational topics.
- Arrangement of sentences.
- Gradual acquisition of vocabulary.
- Verb-action-result matching tasks.
- Text analysis activities.
- Text production activities.
- Identification of sentence constituents.
- Repetition by approximation.
- Functional definitions of words.
- Training in taking turns in conversation.
In order to carry out these activities, there are utilities and tools at the subject’s disposal that the therapist can personalize for rehabilitation.

NeuronUP Theoretical framework: General Concepts
51
Executive functionsNo consensus has been reached concerning the definition of executive
functions. We will now outline some of the existing definitions. Executive functions (EFs) are cognitive processes or capacities that control and regulate thought and action (Friedman et al., 2006). Lezak (1999) defines executive functions as mental abilities essential for carrying out effective, creative and socially accepted conduct. According to this author, these executive func-tions can be grouped around a series of components: the necessary capaci-ties to formulate goals (motivation, self-awareness, and way in which one perceives one’s relationship to the world), the abilities employed in the plan-ning of processes, and the strategies to achieve goals (the ability to adopt an abstract attitude—Abstraction—to evaluate different possibilities—Decision making— and to develop a conceptual framework that enables
managing activity—Reasoning), the abilities involved in the execution of plans (the capacity to initiate, continue and stop complex behavioral sequences in an orderly and integrated manner), and the abilities to perform those ac-tivities affectively (monitoring, correcting and self-reg-ulating time—time estimations—intensity, and other qualitative aspects of performance—such as Dual-task Performance and Branching-Multitasking).
According to Banich’s definition (2004), the main goal of executive functions is the intentional, purpose-ful, and coordinated organization of behavior. Executive functions have been even considered as a construct that encompasses a series of control processes of thought,
emotions and behavior. Some authors consider that that they are modular in nature and depend on multiple control processes that have a high correla-tion with intelligence (Tirapu-Ustárroz & Luna-Lario, 2009).
According to Verdejo-García & Bechara (2010), executive functions are higher-order skills involved in the energization, regulation, sound execution and on-line readjustment of goal-directed behaviors. They constitute mech-anisms of inter-modal and inter-temporal integration that allow us to project cognitions and emotions towards future scenarios in order to best resolve novel complex situations (Fuster, 2004).
Miyake et al. (2000), by means of a structural equation model, found that executive functions can be grouped in three latent aspects:
• Shifting: related to the ability to shift the attentional set. This vari-able allows the person to disengage his/her attention from irrel-evant tasks and to maintain attention on tasks that are relevant.
• Updating: is the ability to code and monitor representations in memory. It refers to both the update of content—understood as the insertion or elimination of that information in the short-
Executive functions have been even considered
as a construct that encompasses a series
of control processes of thought, emotions and
behavior

NeuronUP Theoretical framework: General Concepts
52
term memory—and also refers to the manipulation of content in memory. Due to this last reason, the dimension Updating can be considered most similar to Working Memory.
• Inhibition: refers to the ability to inhibit dominant or prepotent responses and to ignore irrelevant information.
Working memoryWorking memory is a mental workspace that can be flexibly used to
perform cognitive activities that require processing, retrieval, storage, and decision-making. Its storage capacity is limited and an overload in any di-mension results in the loss of information in continuous performance tasks (Gathercole & Alloway, 2006).
Working memory is supported by a series of limited attentional resourc-es. Baddeley proposes a structure composed of multiple subsystems: a cen-tral executive and three “slave” subsystems (Tulving, 1999)—the phono-
logical loop, the visuospatial sketchpad, and the episodic buffer—although initially he only suggested two, not tak-ing into account the episodic buffer.
The central executive is a supervisory attentional sys-tem of limited capacity that coordinates the “slave” sys-tems, manipulates contents, and updates them.
The phonological loop is a system dedicated to the re-trieval, temporary storage, and rehearsal of auditory rep-resentations, while the visuospatial sketchpad performs analogous functions for visual representations of stimuli and their location in space.
The phonological loop has two components: a short-term store that is subject to rapid decay, whose function is maintaining the auditory representations, and a subvocal rehearsal process that helps to maintain and update those
representations.
The visuospatial sketchpad is a system specialized in the temporary stor-age of that kind of information.
The episodic buffer integrates information from working memory and from long-term memory systems in multimodal representations.
Baddeley proposes a Working Memory that:
- Is multimodal with regard to the type of information that is managed and integrated.
- Is composed of autonomic processes of maintenance, suppression and monitoring (which implies certain independence from other memory types).
Multimodal Store
Rehearsal
2
EPISODIC BUFFER
PHonological Store
Articulatory Rehearsal
+
PHONOLOGICAL LOOP
Visual Cache
Inner Scribe
+
VISUO-SPATIAL SKETCHPAD
Semantic Visual Memory
Semantic Verbal Memory
Episodic Memory3
CENTRAL EXECUTIVE+
- Switching- Updating- Inhibition- Divided Attention
Working Memory Model (Baddeley, 2007)

NeuronUP Theoretical framework: General Concepts
53
Explanatory models of executive functions
Formal modelsAmong formal models that aim at explaining executive functions, we can
find various proposals (Verdejo- García & Bechara, 2010):
- Models of multiple control processes based on hierarchical process with top-down modulation.
- Models of action-oriented temporal integration related to the con-struct of working memory.
- Models that assume that executive functions comprise specific repre-sentations related to goal-oriented action sequences, and
- Models that address specific aspects of executive functioning omitted by other models.
Our approach approximates most the third group of models, without denying evidence emerging from the other models.
Neuroanatomical models: the frontal lobesThe frontal lobe is a theoretical classification that serves to define a brain
area specialized in higher-level cognitive functions and is characterized by a spatial localization with unique cytoarchitectonic structure. It is a theoretical structure because the brain functions as a whole and the classification gives us an approximate idea of the functional and anatomical specificity. The hierarchical organization of the brain proposed by several authors spatially divides the organ both into functional specificity and connective specificity.
Functionally, the frontal lobe presents three spatial components and one spatial limitation: it occupies a lim-ited space; its posterior limit is defined by the central sul-cus; it is bounded by the Sylvian fissure or lateral sulcus inferiorly; and the cingulate sulcus, just above the corpus callosum, is its medial limit. Functionally, it is possible to assume a hierarchy of control and contents. In the first place, by establishing an anterior-posterior axis, the fron-tal lobe contains the most abstract representations, and is responsible for exerting significant control over specific contents, monitoring them, integrating information into
more complex contents, establishing control strategies, and guiding complex behaviors. Therefore, the frontal lobe contains complex commands from a cognitive point of view, although this does not have to be seen as a defense of the modular model of the brain. From a dorsal-ventral axis, dorsal areas refer to aspects of the external world and also to cold cognitive functions while medial and ventral regions show associations with content of internal cues and emotions. We can draw a parallel with the cortical-limbic classifica-
The frontal lobe is a theoretical classification
that serves to define a brain area specialized
in higher-level cognitive functions

NeuronUP Theoretical framework: General Concepts
54
tion by establishing that cortical areas are characterized by more reflective processes while limbic zones are characterized by stimulus-driven processes. Finally, from a medial-lateral axis, while medial areas show a relationship be-tween internal contents, lateral areas represent spatial relations, and aspects and representations of the external world.
Regarding connections, the frontal lobe receives two types of connec-tions: the cortico-cortical, that are associations with other regions of the cortex; and the cortico-limbic, that occur between the limbic and sublimbic structures. With respect to the cortico-cortical connections, the frontal cor-tex, and especially the prefrontal cortex, contains a great number of inter-nal connections. Thereby, functionally, the prefrontal cortex is subdivided into several areas: a dorsal area, that has connections with cortical centers responsible for motor action and spatial processing; a medial area, with in-direct connections towards the parietal lobe; and a ventral or inferior area, that has direct connections with the cingulate cortex and the emotional and memory centers of the brain.
There are several classifications of the functional anatomy of the frontal lobe. An acceptable definition dissociates the prefrontal system from the motor and premotor cortices. Stern and Prohaska (196) describe three dif-ferentiated areas within the prefrontal system: dorsolateral, orbital, and me-dial. In this explanation we will include the orbital and the medial as one system, the ventromedial system.
• The dorsolateral system is mainly occupied by areas 9, 9/46 and 46, belongs to an extensive circuit that includes the posterior pari-etal cortex, the caudate nucleus, and connections with the caudate nucleus and lateral dorsal nucleus of the thalamus. This system is responsible for monitoring attention, possibly by managing work-ing memory, retrieval, and spatial attention. However, this system’s most important function is the integration of complex cognitive processes involved in planning and behavioral control.
• The ventromedial system is integrated in a main network, the so-called paralimbic system. In addition to the orbitofrontal cor-tex, this system is composed of the cingulate gyrus, the parahip-pocampal cortex, the temporal pole, the insula, and the amygdala. It is a system implicated in emotional and motivational processes,
Cortex
Striatum
Thalamus
Pallidum
SNr
Supplementary motor area
Putamen
Motor ‘loop’
VLoVLm
Vl -Gpi
Cl - SNr
Dorsolateralprefrontal
cortex
dorsolareralcaudate
Dorsolateralprefrontal ‘loop’
VapcMDpc
Idm -GPi
rl - SNr
Lateralorbitofrontal
cortex
ventromedialcaudate
LaterlaOrbitifrontal ‘loop’
m- VAmcMDmc
mdm - GPi
rm - SNr
Anterirocingulate
area
ventralstriatum
LaterlaOrbitifrontal ‘loop’
pm - MD
rl - GPi, VP
rd - SNr
Fronto-subcortical loops, according to Alexander et al. (1986)

NeuronUP Theoretical framework: General Concepts
55
hence we also have to keep in mind that memory con-tains all information related to the learning that mod-ulates the multiple aspects that make up personality. Some authors have suggested that both systems con-verge in Brodmann area 10 (or frontopolar prefrontal area), this being an area specialized in the coordination of complex processes that entail very abstract cogni-tive and emotional representations. BA10, which is the most rostral area of the brain, is a prefrontal region of maximum integration, modulation, and coordination that manages the most reflective contents that guide behavior. BA10 has direct connections with prefrontal areas but very few connections with other frontal ar-eas, and no direct connection with the parietal, occipi-tal, and temporal lobes. The ventromedial system is, therefore, an afferent system of information, and of control over the rest of processes that require reflec-tion and control not driven by stimuli.
In addition to the aforementioned, for more infor-mation about the extensive neural network implicated in executive functioning we recommend Dosenbach et al. (2008) where the default mode network and the task-positive network are explained.
Rehabilitation of executive functioning
Executive functions gain importance in rehabilitation because they are quite sensitive to acquired brain injury, and essential for the execution of activities of daily living because they are responsible for managing preserved functions. Considering that, we want to emphasize that they are functions whose deficit directly affects the independence of individuals even if they preserve the rest of functions intact.
The rehabilitation of executive function must be as ecological as possi-ble. In practice, we conceptualize that, in the beginning of the rehabilitation process, the therapist acts as an external control mechanism of the activities carried out by the subject, and gradually that control is ceded to the subject as his/her capacities improve. If this is not possible, we train compensatory strategies involving the use of external aids. Among all possible models, in addition to the rehabilitation model of executive functioning developed by Sohlberg & Mateer (2001), in the rehabilitation materials we propose a meta-cognitive approach for the execution of activities of daily living.
How must be the instructional techniques in functional behavioral reha-bilitation?
Mid-dorsolateral PFC
• Task switching
• Super-sequence selection
• Sequence categorization
• Win-stay, lose-shift strategy
• Maintaining cross-temporal contingencies
• March-non-match rule
PFC
• Subgoaling
• Relational integration
• Episodic goal monitoring
• Shifting from internal to external attention
Pre-PMd/caudal PFC
• Response-sequence selection
• Sequence categorization
• S-R rule learning
• Win-stay, lose-shift strategy
• Match-non-match rule
PMd
• Response selection
• S-R rule execution
• Match-non-match rule
Main Processes in Prefrontal Cortex (PFC). Adapted from Badre & D´Esposito (2009).

NeuronUP Theoretical framework: General Concepts
56
Systematic instructional methods:• Vanishing cues
• Errorless learning:
- Dividing tasks into smaller components
- Pre-rehearsal and rehearsal models
- Do not question decisions
- Immediate correction of errors
• Distributed practice
• Instructions (strategy)
Conventional instructional methods:
Trial-and-error + reinforcement
Social/Group methods:
- Social skills (training)
- Action observation
- Role playing
- Educational approaches in community
- Etc.
Domain-specific maintenance
Domain general monitoring
Abstract plan/schema / internal monitoring
Sensory Control
Contextual control
Episodic control
Branching control
Response concflict
Feature concflict
Dimension conflict
Context conflict
Concrete features
First order relationships
Second order relationships
Theoretical accounts of the rostro–caudal gradient in the PFC. (a) From a working memory perspective, rostral and caudal PFC can be distinguished on the basis of processing domain general versus specific representations. Hierarchical versions of this perspective propose that domain-specific posterior frontal regions can be modulated by the maintenance domain general rules in anterior DLPFC and FPC (b) Relational complexity proposes a gradient in the PFC with respect to evaluation of simple stimulus properties, first-order relationships among the properties, and second-order relationships among relationships (c) The cascade model proposes four levels of control that are distinguished by temporally disparate control signals, either sensory, context, episodic or branching (d) Abstract representational hierarchy proposes that regions of the PFC are distinguished by the level of abstraction at which representations compete in a hierarchy of action representations. Adapted from Badre (2008).

NeuronUP Theoretical framework: General Concepts
57
Some explicit direct instructions:
- Task analysis
- Errorless learning
- Cumulative reviews of performance
- Rehearsal
- Metacognitive strategies
To Ehlhardt, Sohlberg, Glang, & Albin (2005), most effective is estab-lishing a direct instruction based on metacognitive strategies. They allow training in the management of self-regulation.
Instructional modelsModels of systematic, explicit instruction (techniques):• Direct instruction
- Step-analysis (sequences)
- Modeling: errorless or guided
- Comprehensive feedback
- Massed practice: massed, mixed and spaced
- Diagrams of spaced practice
- Action observation
{ - Plan prediction
- Monitoring
- Evaluation
{ { {
{
{
{Techniques
Systematic
- Vanishing cues
- Distributed practice
- Instructions (Models & strategy)
- Expliat instructions
- Strategy-based Instructions
- Trial-Error reinforcement
- Social training
- Procedural facilitators
- Scaffolded instruction
- Metacognitive strategies
- Social Skills
- Action Observation
- Role-Playing
- Educational communities
Conventional
- Step—Always
- Errorless learning
- Comprehensive feedback
- Massed practice
- Diagrams

NeuronUP Theoretical framework: General Concepts
58
Models of strategy-based instruction (goal: to monitor thinking)- Procedural facilitators
- Scaffolded instruction
- Metacognitive strategies
• Estimates (of skills)
• Self-monitoring and self-regulation processes (comparison)
• Attributes
• Problem analysis
• Goal management training
• Self-instructional sequences
• Verbal self-regulation
• The prediction-reflection technique
Design of instructions (Sohlberg, Ehlhardt, & Kennedy, 2005)
1. Analysis of content to identify “big ideas”, concepts, rules, and generalizable strategies.
2. Determine necessary skills and prerequisites.
3. Sequence skills from simple to more complex.
4. Develop task analyses.
5. Develop and sequence a broad range of training examples to fa-cilitate generalization.
6. Develop simple, consistent, clear instructions and scripts to re-duce confusion and focus learner on relevant content.
7. Clearly establish learning objectives.
8. Establish high mastery criteria.
9. Provide models and gradually fade cues and prompts to facilitate errorless learning.
10. Pre-correct by instructing prerequisite skills first, or isolating dif-ficult steps for instruction.
11. Provide consistent, rapid feedback (immediately provide the cor-rect model if the patient makes a mistake).
12. Provide high amounts of correct, massed practice followed by distributed practice.
13. Provide sufficient, cumulative review (integration of new and old material).
14. Individualize instruction (language, pacing, time, capacities…).
15. Conduct ongoing assessment to gauge skill retention.
The combined model (direct instruction and programmed instruction) yields the best results. Afterwards come strategy instruction, direct instruc-tion, and then, nondirect instruction (such as social skills training or trial-and-error).

NeuronUP Theoretical framework: General Concepts
59
Which instructions yield the best result?1. Explicit practice: distributed practice and review, repeated practice,
sequenced review, daily feedback, and daily reviews.
2. Orientation to task/advanced organizers: establishment of instruc-tional objectives, review of materials prior to instruction, instruc-tion to focus on particular information, providing prior informa-tion about the task.
3. Presentation of new learning material: diagrams, mental represen-tations, curriculum implemented in the task, information from previous lessons that are related.
4. Modeling of steps to complete the task.
5. Sequencing.
6. Systematic Investigation/Validation and reinforcement: use of probes and daily feedback.
Errorless learningPrimary goal: eliminating errors during the acquisition phase of learning by:
1. Breaking down the activity into discrete and small steps or units.
2. Providing sufficient models before the client performs the target task.
3. Instructing the client to avoid guessing about the causes or reasons regarding the task.
4. Immediately correcting errors.
5. Carefully fading prompts.
Errorless learning is normally applied to persons with impaired procedural memory and declarative memory loss. Errorful learn-ing (for example, trial-and-error learning or discovery learning) consists of encouraging the patient to guess about the targeted response before being provided with the correct information.
Possible applications of errorless learning (according to Barbara Wilson) to ADLs:
• Face-name associations
• Programming an electronic organizer
• Memorizing telephone numbers
Conditions that facilitate errorless learning- High amounts of correct practice. The patient correctly executes
a task if given the opportunity to put it into practice repeatedly. And also vice versa—Pay attention, this does not involve generali-zation and maintenance, just execution.
- Distributed practice—and spaced retrieval.
- To use forward and backward chaining. Chaining is used in multi-step techniques to improve recall of complex guidelines. It

NeuronUP Theoretical framework: General Concepts
60
can be done in a “direct” (to begin with the first step) or reverse manner (to begin with the last step). A form of backward chaining is the technique of vanishing cues. This method can also be direct (fading cues) or reverse (adding cues).
- Effortful processing and Self-Generation. Effortful processing fa-cilitates the mnesic trace, but it is not error-free. Therefore, there must be regulation regarding the administration of this technique. Self-generation refers to cues or prompts self-generated by the in-dividual and not by the therapist (for example, questions generated by the therapist vs questions generated by the client about relevant factors —i.e., about a face).
- To apply the technique during the acquisition phase.
- The prediction-reflection technique (metacognitive) can be useful to generate active processing of the material or to generate new strategies.
Scaffolded instructionScaffolding is a metacognitive method. (Other metacognitive methods:
self-instructional sequences, verbal self-regulation, prediction techniques).
Two important characteristics of any effective metacognitive strategy are:
- Feedback given to the patient must maintain focus on the task.
- Metacognitive strategy training must involve ambiguous situations, for example, in Social Skills must manage ambiguity and planning.
Scaffolded instruction consists of mental representations or knowledge structures that establish relationships between concepts such as diagrams, abstracts, representation of results (real or estimated, etc…). Improve in-structional efficiency (which is the relation between mental effort—re-cruited resources by executive demand—and task performance in a particu-lar learning condition). This method relies on two aspects:
1. A dual processing (Paivio), visual and verbal, that boosts the men-tal representations that establish relationships between concepts. This theory is evident in transfer tasks that require integration of information. It provides graphical representation of mental reality with schematic and semantic representation.
2. Reduction of the amount of information on working memory. Mental models enable the reduction of the cognitive load associ-ated with complex tasks by making relations between structural components in a clear and efficient manner.
Cuevas, Fiore, & Oser (2002) propose a model of metacomprehension (an aspect of metacognition). There are various aspects that correlate meta-cognition and the ability to transfer knowledge and learning.
Beyond the proposed classification, we want to mention a program that has been a pioneer in the rehabilitation of executive functioning and has served as a model for some of the activities that we have designed.

NeuronUP Theoretical framework: General Concepts
61
TEACH-M (Ehlhardt, Sohlberg, Glang, & Albin, 2005)1. Task Analysis: break the task into small steps. Chain the necessary
steps together.
2. Errorless learning: keep errors to a minimum during the acquisi-tion phase. Gradually fade support.
3. Assessment of performance: assess skills before initiating the task (prerequisites). On-going performance. Assess before introducing a new step.
4. Cumulative review: regularly assess previously learned skills.
5. High rates of correct practice.
6. Training in metacognitive strategies: the prediction technique is used to encourage active processing of the material.
Other characteristics:
- Pre-exposure to stimuli that are going to be employed.
- Screenshots that reflect performance.
- Guided practice with multiple opportunities.
- Spaced retrieval.
- Varied training examples
- Training to stipulated and always updated criteria.
Social cognitionSocial cognition is a neurobiological, psychological, and social process
through which social phenomena are perceived, recognized and evaluated in order to construct a representation of the environment where individu-als interact, and to subsequently generate social behavior, that is, the most appropriate response according to the specific circumstance. Social cogni-tion is related to aspects ranging from social perception (initial stages of evaluating the intentions of others by their behavior—gaze direction and body movement) to attributional style (how the behavior of other people is
explained) (Sánchez Cubillo, 2011).
In order to explain social cognition, we base from the model of social-emotional processing stream (Ochsner, 2008). This model enables considering social cognition as a multi-factorial reality that depends on various levels of processing that differ in complexity and interrelation of components. As argued by Adolphs (2001), social cognition is based on a distributed set of neural mechanisms for perceiving, recognizing, and evaluating stimuli, which are then used to construct central representations of the social environment.
Social cognition involves cold executive functions (for they
Social cognition depends on
various levels of processing that
differ in complexity and interrelation of
components

NeuronUP Theoretical framework: General Concepts
62
are responsible for neutral neuropsychological contents and processes) and hot executive functions (which in-volve the management of emotional evaluative compo-nents). This dichotomy is explanatory since emotion and cognition form a continuum in which both influence each other by bottom-up processes (emotional interference) and top-down processes (for example, in the reformula-tion of emotions—see Ochsner & Gross, 2005).
Ochsner’s “Processing Stream” comprises five con-structs (from lowest to highest level of complexity):
- Acquisition of social-affective values and responses
- Recognizing and responding to social-affective stimuli
- Low-level mental state inferences
- High-level mental state inferences
- Context-sensitive emotion regulation
We include Theory of Mind (Baron Cohen, Leslie, & Frith, 1985) within the low and high-level inferences. The concept ‘theory of mind’ (ToM) re-fers to the ability to understand and predict other people’s behavior, their knowledge, their intentions, and their beliefs. Accordingly, this concept re-fers to a metacognitive ability, since we refer to how a cognitive system is able to understand the contents of another cognitive system that is different from the one carrying out the knowledge (Tirapu-Ustárroz, Pérez-Sayes, Erekatxo-Bilbao, & Pelegrín-Valero, 2007).
Empathy is the ability to carry out the theory of mind in its different levels. There are two types of empathy, emotional and cognitive.
Functional models on which social cognition relies
Social cognition is a complex process whose components recruit dif-ferent nodes of processing in order to achieve effective output. Drawing a parallel between the “Processing Stream” components and the main neuro-anatomical nodes that support them, we find that:
- Acquisition of social-affective values and responses: amygdala, stria-tum and hippocampus.
- Recognizing and responding to social-affective stimuli: superior tem-poral sulcus, inferior parietal cortex, amygdala and insula.
- Low-level mental state inferences: mirror-neuron system.
- High-level mental state inferences: mirror-neuron system, superior temporal sulcus, medial prefrontal cortex and temporal poles of the frontal lobe.
- Context-sensitive emotion regulation: dorsolateral prefrontal cortex, ventral prefrontal cortex and orbitofrontal cortex, amygdala and stria-tum.
Theory of Mind refers to a metacognitive ability,
since we refer to how a cognitive system is
able to understand the contents of another
cognitive system

NeuronUP Theoretical framework: General Concepts
63
The mirror- neuron systemThere are two main neural networks that make up the mirror-neuron
system (Cattaneo & Rizzolatti, 2009): a network comprised of areas of the parietal lobe and premotor cortex, as well as the caudal part of the inferior frontal gyrus; and another network comprised of the insula and the an-
terior medial frontal cortex. The first mirror system in-volves learning based on observation and imitation. The second mirror system is the emotional, and is involved in the adoption of empathic attitudes but it does not neces-sarily work separately from the first system. The role of mirror neurons in empathic attitudes such as the adoption of facial expressions and postures in interactive imitative behaviors is essential in association with emotional em-pathy (limbic system). Mirror neuron computations are guided by consequences of action and goals. This knowl-edge serves as a base for social cognition, together with the second system of emotional integration.
To learn more about the networks that make up the mirror-neuron system, there is an open access document downloadable from our website. Click on the link:
https://www.neuronup.com/ftp/Neuronas_espejo_NeuronUP.pdf
Rehabilitation of social cognitionWhen social cognition fails, some of the following changes can occur:
- We are not capable of establishing or inferring intentions, thoughts, desires, etc. in others (mentalization).
- We are not capable of recognizing an emotion or nuanced look, a tone of voice, or a situation (recognition of emotions in different formats).
- We are not capable of coping with a situation because we do not know how to/cannot gather information of the environment (working memory, problem solving).
- We cannot initiate conversations or requests with others out of fear or because we do not have the required skills (communicative and/or expressive language).
- We create false theories about reality that are usually based on er-roneous ideas.
- We cannot envision social situations as a whole, focusing instead on specific details.
- Negative emotional responses to situations of social interaction.
Social cognition is a function composed of various levels of process-ing; hence the intervention must be carried out based on analysis of the
F
B
CG
D
E
A
Mirror-Neuron Systems. Adapted from: Southgate & Hamilton (2008), and Iacoboni & Dapretto (2006)*. a) Inferior Frontal Gyrus and Ventral Premotor Cor-tex; b) Rostral Inferior Parietal Cortex; c) Secondary Somatosensory Cortex; d) Anterior Insula; e) Anterior Cingulate Cortex; *f) Posterior Superior Temporal Sulcus and g) Amygdala. Furthermo-re, there are 2 systems in empathy: emotional empathy system -BA 44 and Amiygdala- and a perspective taking system -BA 10 and BA 11-.

NeuronUP Theoretical framework: General Concepts
64
entire process (selective attention, recognition, language, memory, executive functions). Therefore, the first level of intervention corresponds with the identification of internal emotional states (estimation of attributed valence) and external environmental factors that produce such valence. Afterwards, we have created a series of activities aimed at the identification of emotional states in others, first by using body gestures and then, with elements that become more subtle and ambiguous.
We have created a variety of activities to train how to infer both internal and external emotional states, and thought processes in others. The compo-nents have a significant visual load, since on many occasions disturbances in social communication are accompanied by deficits in language, and there-fore, the materials must fulfill certain requirements that we have stipulated.
The goal is to train processes of inference about others and social skills (which also involve the contextualization of language in the form of detec-tion of ironies, lies, etc.). Social skills focus on two main aspects: on the one hand, they are directed towards managing behaviors of interaction in social situations; on the other hand, they are directed towards self-regulation and management of internal emotional states in diverse contexts.
Among the intervention activities, we would like to mention a specific one that we have used to design the most complex materials: the social stories.
Social stories.The social stories are a script for training persons with impaired social
cognition and theory of mind to acquire skills at the moment of interaction with other people that indicate the appropriate behavior expected in social situations. Social stories attempt to be “social translations”. This training
can focus on interaction behaviors, self-regulation, infer-ence of intentionality, reading and management of some-one else’s emotions, etc.
It is necessary to differentiate the social stories from other two types of training:
- Social cognition, which involves more basic aspects of theory of mind that have to do with perceptive or linguistic aspects. It is true that social scripts entail social cognition, but they are com-bined with more complex processes (unlike social cognition tasks, which usually are more simple).
- Training in routines such as self-care, housework, dressing, etc. that do not require social involvement.
There are different formats in social stories. These stories can be de-signed with pictograms (drawings that represent the context that we are going to work on), with words, or with mixed formats. It seems that among all subjects with whom we train these activities, persons with ASD in any degree usually benefit more from pictograms. It is important that situations
Social stories attempt to be social
translations
NeuronUP Theoretical framework: General Concepts
65
catch the selective attention of patients but without distracting them.
The contexts that we will use will be diverse and will be useful in grading activities, depending on the quantity of ambiguity, number of interactions, quantity of employed concepts and complexity of emitted social behavior.
Situations are as diverse as life, but we can begin with the following cat-egories that are non-exclusive:
- Self-regulation
- Interactions with close people (relatives/friends/teachers/etc.)
- Rules for specific places of social activity (hospitals, school, theat-er, cinema, park, train…)
- Explicit prohibitions regarding behavior
- Housework
- Personal care (AS LONG AS IT REQUIRES INTERACTION, for example, to go shopping for clothes)
- Exceptions to a rule
- Impatience
- Violent / embarrassing / awkward situations
- Exceptional situations
- Emotional situations (meaning of gestures, e.g., crying=sadness)
- Inferences of internal states in others
In addition to these categories, we must take into account the language employed in the activity, even in tasks whose only purpose is the acquisition of language.
Activities of daily livingWhen a neuropsychological deficit occurs, this can have a variable im-
pact on the functionality of the people. Functionality is related to the per-formance of ADLs. Independece has an impact on emotional aspects and quality of life and has a direct impact on the construction of personality and people’s environment. The primary goal in any neuropsychological or occupational therapy intervention is to help the person achieve the highest
level of function possible. Thus, a significant impact in a specific area of the brain may have little or no impact in the functionality of the person, which is generally deter-mined by the context.
Activities of daily living are tasks performed by indi-viduals on a daily basis. Following brain injury (whether acquired or not), the priority and nature of those activities need to be reformulated. In many cases, those activities
Functionality is related to the performance of
ADLs. independece has an impact on emotional
aspects and quality of life

NeuronUP Theoretical framework: General Concepts
66
will be taken up again, while in other cases, the activities will be replaced with new ones or with techniques of substitution and compensation, de-pending on the person’s preserved abilities.
The main types of activities of daily living have been extracted from Rogers & Holm (1994).
Basic activities of daily living. They are activities oriented toward taking care of one’s own body.
• Bathing, showering— Obtaining and using supplies; soaping, rinsing, and drying body parts; maintaining bathing position; and transferring to and from bathing positions.
• Bowel and bladder management— Includes completing inten-tional control of bowel movements and urinary bladder and, if necessary, using equipment or agents for bladder control (Uni-form Data System for Medical Rehabilitation, 1996, pp. III–20, III–24).
• Dressing— Selecting clothing and accessories appropriate to time of day, weather, and occasion; obtaining clothing from storage area; dressing and undressing in a sequential fashion; fastening and adjusting clothing and shoes; and applying and removing per-sonal devices, prostheses, or orthoses.
• Eating— “The ability to keep and manipulate food or fluid in the mouth and swallow it; eating and swallowing are often used inter-changeably” (AOTA, 2008).
• Feeding— “The process of setting up, arranging, and bringing food [or fluid] from the plate or cup to the mouth; sometimes called self-feeding” (AOTA, 2008).
• Functional mobility— Moving from one position or place to an-other (during performance of everyday activities), such as in-bed mobility, wheelchair mobility, and transfers (e.g., wheelchair, bed, car, tub, toilet, tub/shower, chair, floor). Includes functional am-bulation and transporting objects.
• Personal device care— Using, cleaning, and maintaining personal care items, such as hearing aids, contact lenses, glasses, orthot-ics, prosthetics, adaptive equipment, and contraceptive and sexual devices.
• Personal hygiene and grooming— Obtaining and using supplies; removing body hair (e.g., use of razors, tweezers, lotions); apply-ing and removing cosmetics; washing, drying, combing, styling, brushing, and trimming hair; caring for nails (hands and feet); car-ing for skin, ears, eyes, and nose; applying deodorant; cleaning mouth; brushing and flossing teeth; or removing, cleaning, and reinserting dental orthotics and prosthetics.
NeuronUP Theoretical framework: General Concepts
67
• Sexual activity— Engaging in activities that result in sexual satis-faction.
• Toilet hygiene— Obtaining and using supplies; clothing management; maintaining toileting position; transferring to and from toileting posi-tion; cleaning body; and caring for menstrual and continence needs (including catheters, colostomies, and suppository management).
Instrumental activities of daily living (iadls)
They are activities to support daily life within the home and community that often require more complex interactions than self-care used in ADL.
• Care of others (including selecting and supervising caregivers)—Arranging, supervising, or providing the care for others.
• Care of pets—Arranging, supervising, or providing the care for pets and service animals.
• Child rearing—Providing the care and supervision to support the developmental needs of a child.
• Communication management—Sending, receiving, and interpret-ing information using a variety of systems and equipment, includ-ing writing tools, telephones, typewriters, audiovisual recorders, computers, communication boards, call lights, emergency systems, Braille writers, telecommunication devices for the deaf, augmenta-tive communication systems, and personal digital assistants.
• Community mobility—Moving around in the community and us-ing public or private transportation, such as driving, walking, bicy-cling, or accessing and riding in buses, taxi cabs, or other transpor-tation systems.
• Financial management—Using fiscal resources, including alternate methods of financial transaction and planning and using finances with long-term and short-term goals.
• Health management and maintenance—Developing, managing, and maintaining routines for health and wellness promotion, such as physical fitness, nutrition, decreasing health risk behaviors, and medication routines.
• Home establishment and management—Obtaining and maintain-ing personal and household possessions and environment (e.g., home, yard, garden, appliances, vehicles), including maintaining and repairing personal possessions (clothing and household items) and knowing how to seek help or whom to contact.
• Meal preparation and cleanup—Planning, preparing, and serving well-balanced, nutritional meals and cleaning up food and utensils after meals.

NeuronUP Theoretical framework: General Concepts
68
• Religious observance—Participating in religion, an organized sys-tem of beliefs, practices, rituals, and symbols designed to facilitate closeness to the sacred or transcendent.
• Safety and emergency maintenance— Knowing and performing preventive procedures to maintain a safe environment as well as recognizing sudden, unexpected hazardous situations and initiat-ing emergency action to reduce the threat to health and safety.
• Shopping—Preparing shopping lists (grocery and other); select-ing, purchasing, and transporting items; selecting method of pay-ment; and completing money transactions.
Education Includes activities needed for learning and participating in the environ-
ment.
• Formal educational participation—Including the categories of academic (e.g., math, reading, working on a degree), nonacadem-ic (e.g., recess, lunchroom, hallway), extracurricular (e.g., sports, band, cheerleading, dances), and vocational (prevocational and vocational) participation.
• Informal personal educational needs or interests exploration (be-yond formal education)—Identifying topics and methods for ob-taining topic-related information or skills.
• Informal personal education participation— Participating in classes, programs, and activities that provide instruction/training in identified areas of interest.
Work• Includes activities needed for engaging in remunerative employ-
ment or volunteer activities (Mosey, 1996, p. 341).
• Employment interests and pursuits—Identifying and selecting work opportunities based on assets, limitations, likes, and dislikes relative to work.
• Employment seeking and acquisition—Identifying and recruit-ing for job opportunities; completing, submitting, and reviewing appropriate application materials; preparing for interviews; par-ticipating in interviews and following up afterward; discussing job benefits; and finalizing negotiations.
• Job performance—Job performance including work skills and pat-terns; time management; relationships with co-workers, managers, and customers; creation, production, and distribution of products and services; initiation, sustainment, and completion of work; and compliance with work norms and procedures.

NeuronUP Theoretical framework: General Concepts
69
• Retirement preparation and adjustment—Determining aptitudes, developing interests and skills, and selecting appropriate avoca-tional pursuits.
• Volunteer exploration—Determining community causes, organi-zations, or opportunities for unpaid “work” in relationship to per-sonal skills, interests, location, and time available.
• Volunteer participation—Performing unpaid “work” activities for the benefit of identified selected causes, organizations, or facilities.
Play Any spontaneous or organized activity that provides enjoyment, enter-
tainment, amusement, or diversion.
• Play exploration—Identifying appropriate play activities, which can include exploration play, practice play, pretend play, games with rules, constructive play, and symbolic play (adapted from Ber-gen,1988, pp. 64–65).
• • Play participation—Participating in play; maintaining a balance of play with other areas of occupation; and obtaining, using, and maintaining toys, equipment, and supplies appropriately.
Leisure • A nonobligatory activity that is intrinsically motivated and engaged
in during discretionary time, that is, time not committed to obliga-tory occupations such as work, self-care, or sleep (Parham & Fazio, 1997, p. 250).
• Leisure exploration—Identifying interests, skills, opportunities, and appropriate leisure activities.
• Leisure participation—Planning and participating in appropriate leisure activities; maintaining a balance of leisure activities with other areas of occupation; and obtaining, using, and maintaining equipment and supplies as appropriate.
Social participation
Organized patterns of behavior that are characteristic and expected of an individual or a given position within a social system (Mosey, 1996, p. 340).
• Community—Engaging in activities that result in successful inter-action at the community level (i.e., neighborhood, organizations, work, school).

NeuronUP Theoretical framework: General Concepts
70
• Family—Engaging in “[activities that result in] successful inter-action in specific required and/or desired familial roles” (Mosey, 1996, p. 340).
• Peer, friend—Engaging in activities at different levels of intimacy, including engaging in desired sexual activity.
The goal is to increase autonomy of brain-injured people or to maintain it at an optimal level for as much time as possible. NeuronUP integrates the characteristics of occupational therapy and neuropsychology by carry-ing out a comprehensive analysis of the activities that constitute these fields, but without denying a detailed analysis of the neuropsychological processes involved in each and every behavior. By implementing sequences, an exhaus-tive analysis of the neuropsychological processes involved in the activities
can be conducted. The purpose is to establish an appro-priate classification of the complexity levels.
NeuronUP approaches the rehabilitation of the activi-ties of daily living in a gradual and operative manner but without being less ecological. We integrate everyday ob-jects in simulators that people can use to train the use of objects and the sequence of activities with the therapist and therefore have a number of cognitive resources when facing real contexts that they may find complex in some cases. We have also designed interactive games and pencil and paper tasks (also available in digital format) in which the contents are ecological and personalized. As a result
of using real objects as material, the possibility that an effective generaliza-tion exists can increase and the motivational effect is verifiable.
In general, we use many of the metacognitive strategies that we have outlined in the rehabilitation of executive functioning, adapting the activity, the materials, and the instructions to the patient’s current functional status. The functional analysis of sequences is a priority in our approach.
The record of results and the accuracy in the formation of behavioral and cognitive sequences that integrate this type of activities are aspects that occupational therapists recommend, and whose purpose is to evaluate the effectiveness of treatments, achieving a higher level of evidence.
The goal is to increase autonomy of
brain-injured people or to maintain it at an optimal level for
as much time as possible

NeuronUP Theoretical framework: General Concepts
71
Social SkillsAccording to Beauchamp & Anderson (2010), social skills must be in-
tegrated into a comprehensive framework that “incorporates the biological underpinnings and socio-cognitive skills that underlie social function (atten-tion/executive function, communication, socio-emotional skills), as well as the internal and external (environmental) factors that mediate these skills”. We can consider that social skills are the implementation of social cognition abilities in a socio-emotional context, emitting and maintaining effective be-haviors and strategies.
Parsons & Mitchell (2002) consider two ways to promote social skills in ASD:
- Behavioral, structured one-to-one settings of behaviors. They are very effective in teaching children new behaviours or skills, but suffer from a lack of generalization in terms of transferring learned behaviours to new tasks or contexts.
- Embedding interventions within the child’s natural settings, such as home and school.
The goal for social skills in NeuronUP is to develop a system that would be integrated into different contexts. By now, we have developed con-textual simulations that allow the patients to learn and put into in practice basic social cognition processes –learnt in cognitive functions areas-, as well as get an automatic feedback to correct their behavior. Social skills exercises are more complex than media as they contain flexible aspects of behavior (contexts change depending on the patient´s answers).
Social Skills are directly related to quality of life, and treatment has to be comprehensive by providing a wide range of contexts that require complex and diverse neuropsychological processes. These complex processes entan-gle widespread neural mechanisms (such as language, perception, motor and memory). Working memory, flexibility and social cognition are the key pro-cesses in this area.
The specific contents of this area are those which are not already in-cluded in basic neuropsychological processes:
- Proxemic aspects of social interaction.
- Paralinguistic issues of communication.
- Complex social cognition aspects.
- Conversational issues such as adequate themes of conversation, initiation, etc.
- Ecological tools and activities regarding changeling changing con-texts.
NeuronUP Theoretical framework: General Concepts
72
References

NeuronUP Theoretical framework: General Concepts
73
Adolphs, R. (2001). The neurobiology of social
cognition. Current opinion in neurobiology, 11(2),
231-239.
Akinwuntan, A. E., Wachtel, J., & Rosen, P. N.
(2012). Driving Simulation for Evaluation and
Rehabilitation of Driving After Stroke. Journal of
Stroke and Cerebrovascular Diseases, 21(6), 478-486.
doi:10.1016/j.jstrokecerebrovasdis.2010.12.001
Alexander, G. E., DeLong, M. R. & Strick, P.
L. (1986) Parallel Organization of Functionally
Segregated Circuits Linking Basal Ganglia and
Cortex. Annual Review of Neuroscience, Vol.
9: 357-381
Allen, L., Mehta, S., McClure, J., & Teasell, R.
(2012). Therapeutic Interventions for Aphasia
Initiated More than Six Months Post Stroke: A
Review of the Evidence. Topics in Stroke Rehabili-
tation, 19(6), 523-535. doi:10.1310/tsr1906-523
Alm, N., Astell, A., Ellis, M., Dye, R., Gowans,
G., & Campbell, J. (2004). A cognitive prosthe-
sis and communication support for people with
dementia. Neuropsychological Rehabilitation, 14(1-
2), 117-134. doi:10.1080/09602010343000147
Alvarez, V. A., & Sabatini, B. L. (2007). Ana-
tomical and physiological plasticity of dendritic
spines. Annual review of neuroscience, 30, 79-97.
doi:10.1146/annurev.neuro.30.051606.094222
Arroyo-Anlló, E. M., Díaz-Marta, J. P., &
Sánchez, J. C. (2012). Técnicas de rehabilitación
neuropsicológica en demencias: hacia la ciber-
rehabilitación neuropsicológica. Pensamiento
Psicológico, 10(1), 107-127.
Assistive technology: Matching device and consumer for
successful rehabilitation. (2002) (Vol. xiii). Washing-
ton, DC, US: American Psychological Associa-
tion.
Ayres, K. M., Langone, J., Boon, R. T., & Nor-
man, A. (2006). Computer-Based Instruction
for Purchasing Skills. Education and Training in
Developmental Disabilities, 41(3), 253-263.
Baddeley, A. (2007). Working memory, thought, and
action (Vol. xviii). New York, NY, US: Oxford
University Press.
Baddeley, A. D. (1999). Essentials of human memo-
ry (Vol. xi). Hove, England: Psychology Press/
Taylor & Francis (UK).
Badre, D. (2008) Cognitive control, hierarchy,
and the rostro–caudal organization of the fron-
tal lobes. Trends in Cognitive Sciences, Vol. 12,
Issue 5: 193-200
Badre, D. & D´Esposito, M. (2009) Is the ros-
tro-caudal axis of the frontal lobe hierarchical?
Nat Rev Neuroscience, Vol. 10, Issue 9: 659-
669
Banich, M.T. (2004). Cognitive Neuroscience
and Neuropsychology (second edition). Boston:
Houghton-Mifflin.
Barker-Collo, S. L., Feigin, V. L., Lawes, C. M.
M., Parag, V., Senior, H., & Rodgers, A. (2009).
Reducing Attention Deficits After Stroke Us-
ing Attention Process Training A Randomized
Controlled Trial. Stroke, 40(10), 3293-3298.
doi:10.1161/STROKEAHA.109.558239
Baron-Cohen, S., Leslie, A. M., & Frith, U.
(1985). Does the autistic child have a «theory of
mind»? Cognition, 21(1), 37-46.
Basak, C., Boot, W. R., Voss, M. W., & Kramer,
A. F. (2008). Can training in a real-time strat-
egy video game attenuate cognitive decline in
older adults? Psychology and aging, 23(4), 765-777.
doi:10.1037/a0013494
Beauchamp, M. H., & Anderson, V. (2010). SO-
CIAL: An Integrative Framework for the De-
velopment of Social Skills. Psychological Bulletin,
136(1), 39-64.
Beaumont, R., & Sofronoff, K. (2008). A multi-
component social skills intervention for children
with Asperger syndrome: The Junior Detective
Training Program. Journal of Child Psychology and
Psychiatry, 49(7), 743-753. doi:10.1111/j.1469-
7610.2008.01920.x
Benedet Alvarez, M. J. (2002). Fundamento teórico
y metodológico de la neuropsicologia cognitiva. IMSER-
SO
Ben-Yishay, Y., Piasetsky, E., and Rattok, J. A
(1987) Systematic Method for Ameliorating
Disorders in Basic Attention. In: Meier, M.,
Benton, A., and Diller, L., (Ed.), Neuropsycho-
logical Rehabilitation. (pp. 165-181). The Guilford
Press, New York.
Bergman, M. M. (2002). The benefits of a cog-
nitive orthotic in brain injury rehabilitation. The
Journal of head trauma rehabilitation, 17(5), 431-
445.
Bergquist, T., Gehl, C., Mandrekar, J., Lepore, S.,
Hanna, S., Osten, A., & Beaulieu, W. (2009). The
effect of internet-based cognitive rehabilitation
in persons with memory impairments after se-
vere traumatic brain injury. Brain Injury, 23(10),
790-799. doi:10.1080/02699050903196688
Berlucchi, G. (2011). Brain plasticity and cogni-
tive neurorehabilitation. Neuropsychological reha-
bilitation, 21(5), 560-578. doi:10.1080/0960201
1.2011.573255
Bernabeu M., Roig T. (1999). La rehabilitación
del traumatismo craneoencefálico: un enfoque
rehabilitador. Barcelona. Fundació Institut
Guttmann.
Bernard-Opitz, V., Sriram, N., & Nakhoda-
Sapuan, S. (2001). Enhancing social problem
solving in children with autism and normal
children through computer-assisted instruction.
Journal of autism and developmental disorders, 31(4),
377-384.
Bonder, B., Haas, V. D. B., & Wagner, M. B.
(2008). Functional Performance in Older Adults (3rd
Revised edition.). F.A. Davis Company.
Boot, W. R., Kramer, A. F., Simons, D. J., Fabi-
ani, M., & Gratton, G. (2008). The effects of
video game playing on attention, memory, and
executive control. Acta Psychologica, 129(3), 387-
398. doi:10.1016/j.actpsy.2008.09.005
NeuronUP Theoretical framework: General Concepts
74
Borghese, N. A., Bottini, G., & Sedda, A. (2013).
Videogame Based Neglect Rehabilitation: A
Role for Spatial Remapping and Multisensory
Integration? Frontiers in Human Neuroscience, 7.
doi:10.3389/fnhum.2013.00116
Boyke, J., Driemeyer, J., Gaser, C., Büchel, C., &
May, A. (2008). Training-Induced Brain Struc-
ture Changes in the Elderly. The Journal of Neu-
roscience, 28(28), 7031-7035. doi:10.1523/JNEU-
ROSCI.0742-08.2008
Bruna, O., Roig, T., Puyuelo, M., Junqué, C. &
Ruano, A. (Eds.) Rehabilitación neuropsicológica.
Intervención y práctica clínica. (2011). Barcelona:
Masson.
Buxbaum, L. J., & Coslett, H. (2001). Spe-
cialised structural descriptions for human
body parts: Evidence from autotopagno-
sia. Cognitive Neuropsychology, 18(4), 289-306.
doi:10.1080/02643290126172
Buxbaum, L. J., Haaland, K. Y., Hallett, M.,
Wheaton, L., Heilman, K. M., Rodriguez, A.,
& Rothi, L. J. G. (2008). Treatment of Limb
Apraxia. American Journal of Physical Medicine
& Rehabilitation, 87(2), 149-161. doi:10.1097/
PHM.0b013e31815e6727
Caglio, M., Latini-Corazzini, L., D’Agata, F.,
Cauda, F., Sacco, K., Monteverdi, S., … Gemi-
niani, G. (2012). Virtual navigation for memory
rehabilitation in a traumatic brain injured pa-
tient. Neurocase, 18(2), 123-131. doi:10.1080/13
554794.2011.568499
Caglio, Marcella, Latini-Corazzini, L., D’agata,
F., Cauda, F., Sacco, K., Monteverdi, S., …
Geminiani, G. (2009). Video game play changes
spatial and verbal memory: rehabilitation of a
single case with traumatic brain injury. Cognitive
Processing, 10(2), 195-197. doi:10.1007/s10339-
009-0295-6
Cameirão, M. S., Bermúdez I Badia, S., Duarte
Oller, E., & Verschure, P. F. M. J. (2009). The
rehabilitation gaming system: a review. Studies in
health technology and informatics, 145, 65-83.
Cassavaugh, N. D., & Kramer, A. F. (2009).
Transfer of computer-based training to simu-
lated driving in older adults. Applied Ergo-
nomics, 40(5), 943-952. doi:10.1016/j.aper-
go.2009.02.001
Cattaneo, L., & Rizzolatti, G. (2009). The mir-
ror neuron system. Archives of neurology, 66(5),
557-560. doi:10.1001/archneurol.2009.41
Cernich, PhD, S. M. K., PhD, K. L. M., & PhD,
P. B. R. (2010). Cognitive Rehabilitation in Trau-
matic Brain Injury. Current Treatment Options in
Neurology, 12(5), 412-423. doi:10.1007/s11940-
010-0085-6
Cha, Y.-J., & Kim, H. (2013). Effect of com-
puter-based cognitive rehabilitation (CBCR) for
people with stroke: A systematic review and
meta-analysis. NeuroRehabilitation, 32(2), 359-
368. doi:10.3233/NRE-130856
Cho, B.-H., Ku, J., Jang, D. P., Kim, S., Lee, Y. H.,
Kim, I. Y., … Kim, S. I. (2002). The Effect of
Virtual Reality Cognitive Training for Attention
Enhancement. CyberPsychology & Behavior, 5(2),
129-137. doi:10.1089/109493102753770516
Christensen, A.-L., & Uzzell, B. P. (2000). Inter-
national Handbook of Neuropsychological Rehabilita-
tion. Springer.
Cicerone, K D, Dahlberg, C., Kalmar, K.,
Langenbahn, D. M., Malec, J. F., Bergquist,
T. F., … Morse, P. A. (2000). Evidence-based
cognitive rehabilitation: recommendations for
clinical practice. Archives of physical medicine and
rehabilitation, 81(12), 1596-1615. doi:10.1053/
apmr.2000.19240
Cicerone, Keith D, Langenbahn, D. M., Braden,
C., Malec, J. F., Kalmar, K., Fraas, M., … Ash-
man, T. (2011). Evidence-based cognitive reha-
bilitation: updated review of the literature from
2003 through 2008. Archives of physical medicine
and rehabilitation, 92(4), 519-530. doi:10.1016/j.
apmr.2010.11.015
Cihak, D. F., Kessler, K., & Alberto, P. A.
(2008). Use of a Handheld Prompting System
to Transition Independently through Vocation-
al Tasks for Students with Moderate and Severe
Intellectual Disabilities. Education and Training in
Developmental Disabilities, 43(1), 102-110.
Cipriani, G., Bianchetti, A., & Trabucchi, M.
(2006). Outcomes of a computer-based cogni-
tive rehabilitation program on Alzheimer’s dis-
ease patients compared with those on patients
affected by mild cognitive impairment. Archives
of Gerontology and Geriatrics, 43(3), 327-335.
doi:10.1016/j.archger.2005.12.003
Cohene, T., Baecker, R., & Marziali, E. (2005).
Designing Interactive Life Story Multimedia
for a Family Affected by Alzheimer’s Disease:
A Case Study. En Proceedings of ACM CHI (pp.
2–7).
Cole, E. (1999). Cognitive prosthetics: an over-
view to a method of treatment. NeuroRehabilita-
tion, 12(1), 39-51.
Cole, E., Ziegmann, M., Wu, Y., Yonker, V.,
Gustafson, C., & Cirwithen, S. (2000). Use of
“therapist-friendly” tools in cognitive assistive
technology and telerehabilitation. In: Proceedings
of the RESNA 2000 Annual Conference: Technology
for the New Millennium, June 28-July 2, 2000, Omni
Rosen Hotel, Orlando, Florida (p. 31). RESNA
Press.
Conway, A. R. A., Kane, M. J., & Engle, R. W.
(2003). Working memory capacity and its rela-
tion to general intelligence. Trends in cognitive sci-
ences, 7(12), 547-552.
Cook, D. A. (2005). The research we still are not
doing: an agenda for the study of computer-
based learning. Academic medicine: journal of the
Association of American Medical Colleges, 80(6),
541-548.

NeuronUP Theoretical framework: General Concepts
75
Cook, D. A. (2012). Revisiting cognitive and
learning styles in computer-assisted instruction:
not so useful after all. Academic medicine: journal of
the Association of American Medical Colleges, 87(6),
778-784. doi:10.1097/ACM.0b013e3182541286
Corbetta, M., Patel, G., & Shulman, G. L.
(2008). The reorienting system of the human
brain: from environment to theory of mind.
Neuron, 58(3), 306-324. doi:10.1016/j.neu-
ron.2008.04.017
Craik, F. I. M., & Lockhart, R. S. (1972). Lev-
els of processing: A framework for memory
research. Journal of Verbal Learning and Verbal
Behavior, 11(6), 671-684. doi:10.1016/S0022-
5371(72)80001-X
Crete-Nishihata, M., Baecker, R. M., Massimi,
M., Ptak, D., Campigotto, R., Kaufman, L. D.,
… Black, S. E. (2012). Reconstructing the Past:
Personal Memory Technologies Are Not Just
Personal and Not Just for Memory. Human–
Computer Interaction, 27(1-2), 92-123. doi:10.108
0/07370024.2012.656062
Cubelli, R., Marchetti, C., Boscolo, G., & Della
Sala, S. (2000). Cognition in Action: Testing a
Model of Limb Apraxia. Brain and Cognition,
44(2), 144-165. doi:10.1006/brcg.2000.1226
Cuevas, H. M., Fiore, S. M., & Oser, R. L.
(2002). Scaffolding cognitive and metacogni-
tive processes in low verbal ability learners: Use
of diagrams in computer-based training envi-
ronments. Instructional Science, 30(6), 433-464.
doi:10.1023/A:1020516301541
Damasio, A. R. (1989). The Brain Binds Entities
and Events by Multiregional Activation from
Convergence Zones. Neural Computation, 1(1),
123-132. doi:10.1162/neco.1989.1.1.123
Damasio, A.R. & Damasio, H. (1992), Cerebro
y Lenguaje. Investigación y Ciencia, 194, 59-66.
Das Nair, R., Ferguson, H., Stark, D. L., & Lin-
coln, N. B. (2012). Memory Rehabilitation for
people with multiple sclerosis. Cochrane data-
base of systematic reviews (Online), 3, CD008754.
doi:10.1002/14651858.CD008754.pub2
Deng, W., Aimone, J. B., & Gage, F. H. (2010).
New neurons and new memories: how does
adult hippocampal neurogenesis affect learning
and memory? Nature reviews. Neuroscience, 11(5),
339-350. doi:10.1038/nrn2822
Dennis, N. A., & Cabeza, R. (2011). Age-re-
lated dedifferentiation of learning systems: an
fMRI study of implicit and explicit learning.
Neurobiology of aging, 32(12), 2318.e17-2318.e30.
doi:10.1016/j.neurobiolaging.2010.04.004
Deutsch, J. E., Merians, A. S., Adamovich, S.,
Poizner, H., & Burdea, G. C. (2004). Develop-
ment and application of virtual reality technol-
ogy to improve hand use and gait of individuals
post-stroke. Restorative neurology and neuroscience,
22(3-5), 371-386.
Dobkin, B. H. (2005). Rehabilitation after
Stroke. New England Journal of Medicine, 352(16),
1677-1684. doi:10.1056/NEJMcp043511
Dobkin, B. H. (2007). Brain–computer inter-
face technology as a tool to augment plastic-
ity and outcomes for neurological rehabilita-
tion. The Journal of Physiology, 579(3), 637–642.
doi:10.1113/jphysiol.2006.123067
Dosenbach, N. U. F., Fair, D. A., Cohen, A.
L., Schlaggar, B. L., & Petersen, S. E. (2008).
A dual-networks architecture of top-down
control. Trends in cognitive sciences, 12(3), 99-105.
doi:10.1016/j.tics.2008.01.001
Dye, M. W. G., Green, C. S., & Bavelier, D.
(2009). The development of attention skills
in action video game players. Neuropsychologia,
47(8–9), 1780-1789. doi:10.1016/j.neuropsy-
chologia.2009.02.002
Edelman, G. M., & Gally, J. A. (2001). Degen-
eracy and complexity in biological systems. Pro-
ceedings of the National Academy of Sciences, 98(24),
13763-13768. doi:10.1073/pnas.231499798
Edmans, J. A., Webster, J., & Lincoln, N. B.
(2000). A comparison of two approaches in
the treatment of perceptual problems after
stroke. Clinical Rehabilitation, 14(3), 230-243.
doi:10.1191/026921500673333145
Ehlhardt, L. A., Sohlberg, M. M., Glang, A., &
Albin, R. (2005). TEACH-M: A pilot study eval-
uating an instructional sequence for persons
with impaired memory and executive functions.
Brain injury: [BI], 19(8), 569-583.
Ellis, A. W., & Young, A. W. (1996). Human Cog-
nitive Neuropsychology: A Textbook with Readings.
Psychology Press.
Eriksson, P. S., Perfilieva, E., Björk-Eriksson,
T., Alborn, A. M., Nordborg, C., Peterson,
D. A., & Gage, F. H. (1998). Neurogenesis in
the adult human hippocampus. Nature medicine,
4(11), 1313-1317. doi:10.1038/3305
Farah, M. (2004). Visual agnosia. MIT Press.
Fasotti, L., Kovacs, F., Eling, P. A. T. M., & Brou-
wer, W. H. (2000). Time Pressure Management as
a Compensatory Strategy Training after Closed
Head Injury. Neuropsychological Rehabilitation,
10(1), 47-65. doi:10.1080/096020100389291
Faucounau, V., Wu, Y. H., Boulay, M., De Ro-
trou, J., & Rigaud, A. S. (2010). Cognitive in-
tervention programmes on patients affected by
Mild Cognitive Impairment: a promising inter-
vention tool for MCI? The journal of nutrition,
health & aging, 14(1), 31-35.
Fink, R., Brecher, A., Sobel, P., & Schwartz, M.
(2005). Computer-assisted treatment of word
retrieval deficits in aphasia. Aphasiology, 19(10-
11), 943-954. doi:10.1080/02687030544000155
Flavia, M., Stampatori, C., Zanotti, D., Par-
rinello, G., & Capra, R. (2010). Efficacy and
specificity of intensive cognitive rehabilitation
of attention and executive functions in multiple
sclerosis. Journal of the Neurological Sciences, 288(1–
2), 101-105. doi:10.1016/j.jns.2009.09.024

NeuronUP Theoretical framework: General Concepts
76
Flnkel, S. I., & Yesavage, J. A. (1989). Learn-
ing mnemonics: A preliminary evaluation of
a computer-aided instruction package for the
elderly. Experimental Aging Research, 15(4), 199-
201. doi:10.1080/03610738908259776
Fox, M. D., Snyder, A. Z., Vincent, J. L., Corbet-
ta, M., Essen, D. C. V., & Raichle, M. E. (2005).
The human brain is intrinsically organized into
dynamic, anticorrelated functional networks.
Proceedings of the National Academy of Sciences of
the United States of America, 102(27), 9673-9678.
doi:10.1073/pnas.0504136102
Fredericks J.A.M. (1969) The agnosias. In: Bru-
in, G. W. (Ed.) Handbook of Clinical Neurology.
Vol. 3 Amsterdam: Nother-Holland
Friedman, N P, & Miyake, A. (2000). Differ-
ential roles for visuospatial and verbal working
memory in situation model construction. Journal
of experimental psychology. General, 129(1), 61-83.
Friedman, Naomi P, Miyake, A., Corley, R.
P., Young, S. E., Defries, J. C., & Hewitt, J. K.
(2006). Not all executive functions are related to
intelligence. Psychological science, 17(2), 172-179.
doi:10.1111/j.1467-9280.2006.01681.x
Fuchs, E., & Gould, E. (2000). In vivo neu-
rogenesis in the adult brain: regulation and
functional implications. European Journal of Neu-
roscience, 12(7), 2211–2214. doi:10.1046/j.1460-
9568.2000.00130.x
Furniss, F., Lancioni, G., Rocha, N., Cunha,
B., Seedhouse, P., Morato, P., & O’Reilly, M.
F. (2001). VICAID: Development and evalu-
ation of a palmtop-based job aid for workers
with severe developmental disabilities. British
Journal of Educational Technology, 32(3), 277–287.
doi:10.1111/1467-8535.00198
Fuster, J. M. (2004). Upper processing stages
of the perception–action cycle. Trends in Cog-
nitive Sciences, 8(4), 143-145. doi:10.1016/j.
tics.2004.02.004
Gathercole, S. E., & Alloway, T. (s. f.). Practi-
tioner review: Short-term and working memory
impairments in neurodevelopmental disorders :
diagnosis and remedial support. Journal of child
psychology and psychiatry and allied disciplines, 47(1),
4-15.
Ge, S., Sailor, K. A., Ming, G., & Song, H. (2008).
Synaptic integration and plasticity of new neu-
rons in the adult hippocampus. The Journal of
Physiology, 586(16), 3759-3765. doi:10.1113/
jphysiol.2008.155655
Gentry, T. (2008). PDAs as Cognitive Aids
for People With Multiple Sclerosis. The Ameri-
can Journal of Occupational Therapy, 62(1), 18-27.
doi:10.5014/ajot.62.1.18
Gentry, T., Wallace, J., Kvarfordt, C., & Lynch, K.
B. (2008). Personal digital assistants as cognitive
aids for individuals with severe traumatic brain
injury: a community-based trial. Brain injury: [BI],
22(1), 19-24. doi:10.1080/02699050701810688
Gillespie, A., Best, C., & O’Neill, B. (2012).
Cognitive function and assistive technology for
cognition: a systematic review. Journal of the In-
ternational Neuropsychological Society: JINS, 18(1),
1-19. doi:10.1017/S1355617711001548
Gillette, Y., & Depompei, R. (2008). Do PDAs
enhance the organization and memory skills
of students with cognitive disabilities? Psychol-
ogy in the Schools, 45(7), 665–677. doi:10.1002/
pits.20316
Ginarte-Arias, Y. (2002). [Cognitive rehabilita-
tion. Theoretical and methodological aspects].
Revista de neurologia, 35(9), 870-876.
Glisky, E. L., Schacter, D. L., & Tulving, E.
(1986). Computer learning by memory-im-
paired patients: Acquisition and retention of
complex knowledge. Neuropsychologia, 24(3),
313-328. doi:10.1016/0028-3932(86)90017-5
Goldsmith, T. R., & LeBlanc, L. A. (2004). Use
of Technology in Interventions for Children
with Autism. Journal of Early and Intensive Behav-
ior Intervention, 1(2), 166-178.
Gordon, W. A., Hibbard, M. R., Egelko, S.,
Diller, L., Shaver, M. S., Lieberman, A., & Rag-
narsson, K. (1985). Perceptual remediation in
patients with right brain damage: a comprehen-
sive program. Archives of physical medicine and re-
habilitation, 66(6), 353-359.
Gorman, P., Dayle, R., Hood, C.-A., & Rumrell,
L. (2003). Effectiveness of the ISAAC cognitive
prosthetic system for improving rehabilitation
outcomes with neurofunctional impairment.
NeuroRehabilitation, 18(1), 57-67.
Green, C. S., & Bavelier, D. (2003). Action video
game modifies visual selective attention. Nature,
423(6939), 534-537. doi:10.1038/nature01647
Gross, C. G. (2000). Neurogenesis in the adult
brain: death of a dogma. Nature Reviews Neurosci-
ence, 1(1), 67-73. doi:10.1038/35036235
Grynszpan, O., Perbal, S., Pelissolo, A., Fossati,
P., Jouvent, R., Dubal, S., & Perez-Diaz, F. (2010).
Efficacy and specificity of computer-assisted
cognitive remediation in schizophrenia: a me-
ta-analytical study. Psychological Medicine, 41(01),
163-173. doi:10.1017/S0033291710000607
Hall, T. E., Hughes, C. A., & Filbert, M. (2000).
Computer Assisted Instruction in Reading for
Students with Learning Disabilities: A Research
Synthesis. Education and Treatment of Children,
23(2), 173-93.
Hasselbring, T. S., & Bausch, M. E. (2006). As-
sistive Technologies for Reading. Educational
Leadership, 63(4), 72-75.
Hermanutz, M., & Gestrich, J. (1991). Comput-
er-assisted attention training in schizophren-
ics. European Archives of Psychiatry and Clinical
Neuroscience, 240(4-5), 282-287. doi:10.1007/
BF02189541
Hofmann, M., Rösler, A., Schwarz, W., Müller-
Spahn, F., Kräuchi, K., Hock, C., & Seifritz, E.
(2003). Interactive computer-training as a thera-
peutic tool in Alzheimer’s disease. Comprehensive
Psychiatry, 44(3), 213-219. doi:10.1016/S0010-
440X(03)00006-3

NeuronUP Theoretical framework: General Concepts
77
Humphreys, G. W., & Riddoch, M. J. (2006).
Features, objects, action: The cognitive neu-
ropsychology of visual object processing, 1984-
2004. Cognitive neuropsychology, 23(1), 156-183.
doi:10.1080/02643290542000030
Iacoboni, M. & Dapretto, M. (2006) The mir-
ror Neuron System and the consequences of its
dysfunction. Nat Rev Neuroscience, 7(12):942-
951
Jak, A. J., Seelye, A. M., & Jurick, S. M. (2013).
Crosswords to computers: a critical review of
popular approaches to cognitive enhancement.
Neuropsychology review, 23(1), 13-26. doi:10.1007/
s11065-013-9226-5
Jiang, L., Guan, C., Zhang, H., Wang, C., & Ji-
ang, B. (2011). Brain computer interface based
3D game for attention training and rehabilita-
tion. En 2011 6th IEEE Conference on Industrial
Electronics and Applications (ICIEA) (pp. 124-
127). Presentado en 2011 6th IEEE Confer-
ence on Industrial Electronics and Applications
(ICIEA). doi:10.1109/ICIEA.2011.5975562
Jobe, J. B., Smith, D. M., Ball, K., Tennstedt, S.
L., Marsiske, M., Willis, S. L., … Kleinman, K.
(2001). Active: A cognitive intervention trial to
promote independence in older adults. Controlled
Clinical Trials, 22(4), 453-479. doi:10.1016/
S0197-2456(01)00139-8
Johansson, B., & Tornmalm, M. (2012). Work-
ing memory training for patients with acquired
brain injury: effects in daily life. Scandinavian
Journal of Occupational Therapy, 19(2), 176-183.
doi:10.3109/11038128.2011.603352
Junqué, C. & Barroso, J. (1999). Neuropsi-
cología. Madrid: Síntesis.
Kapur, N., Glisky, E. L., & Wilson, B. A. (s. f.).
Technological memory aids for people with
memory deficits. Neuropsychological rehabilitation,
14(1-2), 41-60.
Kim, A.-H., Vaughn, S., Klingner, J. K., Wood-
ruff, A. L., Reutebuch, C. K., & Kouzekanani,
K. (2006). Improving the Reading Comprehen-
sion of Middle School Students With Disabili-
ties Through Computer-Assisted Collaborative
Strategic Reading. Remedial and Special Education,
27(4), 235-249. doi:10.1177/074193250602700
40401
Kueider, A. M., Parisi, J. M., Gross, A. L., &
Rebok, G. W. (2012). Computerized Cogni-
tive Training with Older Adults: A Systematic
Review. PLoS ONE, 7(7). doi:10.1371/journal.
pone.0040588
Kvavilashvili, L., & Ellis, J. (2004). Ecological
validity and twenty years of real-life/laboratory
controversy in memory research: A critical (and
historical) review. History and Philosophy of Psy-
chology , vol 6 , pp. 59-80.
Landauer, T. K., & Bjork, R. A. (1978). Opti-
mum rehearsal patterns and name learning. In:
M. M. Gruneberg, P. E. Morris, & R. N. Sykes
(Eds.) Practical aspects of memory (pp. 625-632).
London: Academic Press.
Lane, S. J., & Mistrett, S. G. (1996). Play and
Assistive Technology Issues for Infants and
Young Children with Disabilities A Pre-
liminary Examination. Focus on Autism and
Other Developmental Disabilities, 11(2), 96-104.
doi:10.1177/108835769601100205
Lange, B., Flynn, S. M., & Rizzo, A. A. (2009).
Game-based telerehabilitation. European journal
of physical and rehabilitation medicine, 45(1), 143-
151.
Lauterbach, S. A., Foreman, M. H., & Engsberg,
J. R. (2013). Computer Games as Therapy for
Persons with Stroke. Games for Health Journal,
2(1), 24-28. doi:10.1089/g4h.2012.0032
Lee, J., Fowler, R., Rodney, D., Cher-
ney, L., & Small, S. L. (2010). IMITATE:
An intensive computer-based treatment
for aphasia based on action observation
and imitation. Aphasiology, 24(4), 449-465.
doi:10.1080/02687030802714157
Lee, Y., & Vail, C. O. (2005). Computer-Based
Reading Instruction for Young Children with
Disabilities. Journal of Special Education Technol-
ogy, 20(1), 5-18.
Lezak, M. D. (2004). Neuropsychological assessment,
4 Ed. Oxford University Press.
Liepmann H. (1990) Das Krankheitsbild der
Apraxia auf Grund eines Falles von einseitiger
Apraxie. Mschr Psychiat Neurol 8: 15-44, 102-132,
188-197.
Lopez-Martinez, A., Santiago-Ramajo, S., Cara-
cuel, A., Valls-Serrano, C., Hornos, M. J., &
Rodriguez-Fortiz, M. J. (2011). Game of gifts
purchase: Computer-based training of execu-
tive functions for the elderly (pp. 1-8). IEEE.
doi:10.1109/SeGAH.2011.6165448
LoPresti, E. F., Bodine, C., & Lewis, C. (2008).
Assistive technology for cognition. IEEE
engineering in medicine and biology magazine: the
quarterly magazine of the Engineering in Medicine
& Biology Society, 27(2), 29-39. doi:10.1109/
EMB.2007.907396
LoPresti, E., Mihailidis, A., & Kirsch, N. (2004).
Assistive technology for cognitive rehabilitation:
State of the art. Neuropsychological Rehabilitation,
14(1-2), 5-39. doi:10.1080/09602010343000101
Lubrini, G., Periañez , J. A., & Rios-Lago, M.
(2009). Introducción a la estimulación cognitiva
y la rehabilitación neuropsicológica. In: Muñoz-
Marrón, E. (Ed.), Estimulación cognitiva y reha-
bilitación neuropsicológica (pp. 13-34). Barcelona:
Editoria UOC.
Lynch, B. (2002). Historical review of comput-
er-assisted cognitive retraining. The Journal of
head trauma rehabilitation, 17(5), 446-457.

NeuronUP Theoretical framework: General Concepts
78
MacArthur, C. A., Ferretti, R. P., Okolo, C.
M., & Cavalier, A. R. (2001). Technology ap-
plications for students with literacy problems:
A critical review. The Elementary School Journal,
101(3), 273-301. doi:10.1086/499669
Maccini, P., Gagnon, J. C., & Hughes, C.
A. (2002). Technology-Based Practices for
Secondary Students with Learning Disabili-
ties. Learning Disability Quarterly, 25(4), 247.
doi:10.2307/1511356
Mangiron. (9999). Accesibilidad a los videojue-
gos: estado actual y perspectivas futuras. Trans:
Revista de Traductología, 15, 53-67.
Marr, D., & Nishihara, H. K. (1978). Represen-
tation and recognition of the spatial organiza-
tion of three-dimensional shapes. Proceedings
of the Royal Society of London. Series B, Containing
papers of a Biological character. Royal Society (Great
Britain), 200(1140), 269-294.
Marr, D., & Vaina, L. (1982). Representation
and recognition of the movements of shapes.
Proceedings of the Royal Society of London. Series B,
Containing papers of a Biological character. Royal So-
ciety (Great Britain), 214(1197), 501-524.
Martinell Gispert-Saúch, M. (2012) Lenguaje,
afasias y trastornos de la comunicación. In:
Bruna, O., Roig, T., Puyuelo, M., Junqué, C. &
Ruano, A. (Eds.) Rehabilitación neuropsicológica. In-
tervención y práctica clínica (pp. 61-82). Barcelona:
Masson
Mateer, C. A., & Sohlberg, M. M. (2001). Cogni-
tive Rehabilitation: An Integrative Neuropsychological
Approach (2.a ed.). Guilford Press.
Mautone, J. A., DuPaul, G. J., & Jitendra, A. K.
(2005). The Effects of Computer-Assisted In-
struction on the Mathematics Performance and
Classroom Behavior of Children With ADHD.
Journal of Attention Disorders, 9(1), 301-312.
doi:10.1177/1087054705278832
McDonald, A., Haslam, C., Yates, P., Gurr,
B., Leeder, G., & Sayers, A. (2011). Google
Calendar: A new memory aid to compensate
for prospective memory deficits following ac-
quired brain injury. Neuropsychological Rehabilita-
tion, 21(6), 784-807. doi:10.1080/09602011.201
1.598405
Mechling, L. C., & Ortega-Hurndon, F. (2007).
Computer-Based Video Instruction to Teach
Young Adults with Moderate Intellectual Dis-
abilities to Perform Multiple Step, Job Tasks in
a Generalized Setting. Education and Training in
Developmental Disabilities, 42(1), 24-37.
Medalia, A., Aluma, M., Tryon, W., & Merriam,
A. E. (1998). Effectiveness of attention train-
ing in schizophrenia. Schizophrenia bulletin, 24(1),
147-152.
Michel, J. A., & Mateer, C. A. (2006). Attention
rehabilitation following stroke and traumatic
brain injury. A review. Europa medicophysica,
42(1), 59-67.
Mihailidis, A., Fernie, G. R., & Barbenel, J. C.
(2001). The use of artificial intelligence in the
design of an intelligent cognitive orthosis for
people with dementia. Assistive technology: the of-
ficial journal of RESNA, 13(1), 23-39. doi:10.10
80/10400435.2001.10132031
Ming, G.-L., & Song, H. (2011). Adult neuro-
genesis in the mammalian brain: significant an-
swers and significant questions. Neuron, 70(4),
687-702. doi:10.1016/j.neuron.2011.05.001
Miyake, A., Emerson, M. J., & Friedman, N. P.
(2000). Assessment of executive functions in
clinical settings: problems and recommenda-
tions. Seminars in speech and language, 21(2), 169-
183.
Miyake, A., Friedman, N. P., Rettinger, D. A.,
Shah, P., & Hegarty, M. (2001). How are visuos-
patial working memory, executive functioning,
and spatial abilities related? A latent-variable
analysis. Journal of experimental psychology. General,
130(4), 621-640.
Molinari, M., Petrosini, L., Misciagna, S., &
Leggio, M. (2004). Visuospatial abilities in cer-
ebellar disorders. Journal of Neurology, Neurosur-
gery, and Psychiatry, 75(2), 235-240.
Morganti, F., Gaggioli, A., Castelnuovo, G.,
Bulla, D., Vettorello, M., & Riva, G. (2003).
The use of technology-supported mental
imagery in neurological rehabilitation: a re-
search protocol. Cyberpsychology & behavior:
the impact of the Internet, multimedia and vir-
tual reality on behavior and society, 6(4), 421-427.
doi:10.1089/109493103322278817
Moulton, S. T., & Kosslyn, S. M. (2009). Im-
agining predictions: mental imagery as mental
emulation. Philosophical Transactions of the Royal
Society B: Biological Sciences, 364(1521), 1273-
1280. doi:10.1098/rstb.2008.0314
Muñoz Cespedes, J. M. M., & Tirapu Ustárroz,
J. (2008). Rehabilitacion neuropsicologica. Sintesis.
Muñoz Céspedes, J. M., & Tirapu Ustárroz, J.
(2004). [Rehabilitation programs for executive
functions]. Revista de neurologia, 38(7), 656-663.
Nair, R. das, & Lincoln, N. B. (2012). Evalu-
ation of Rehabilitation of Memory in Neuro-
logical Disabilities (ReMiND): a randomized
controlled trial. Clinical Rehabilitation, 26(10),
894-903. doi:10.1177/0269215511435424
Neubauer, K., von Auer, M., Murray, E., Pe-
termann, F., Helbig-Lang, S., & Gerlach, A.
L. (2013). Internet-delivered attention modifi-
cation training as a treatment for social pho-
bia: a randomized controlled trial. Behaviour
research and therapy, 51(2), 87-97. doi:10.1016/j.
brat.2012.10.006
Newell, A. F., & Gregor, P. (2000). “User Sensi-
tive Inclusive Design” in search of a new para-
digm. In: Proceedings on the 2000 conference
on Universal Usability (CUU ‘00), John Thom-
as (Ed.). ACM, New York, NY, USA, 39-44.
Association for Computing Machinery.

NeuronUP Theoretical framework: General Concepts
79
Nouchi, R., Taki, Y., Takeuchi, H., Hashizume,
H., Nozawa, T., Kambara, T., … Kawashima,
R. (2013). Brain Training Game Boosts Execu-
tive Functions, Working Memory and Process-
ing Speed in the Young Adults: A Randomized
Controlled Trial. PLoS ONE, 8(2), e55518.
doi:10.1371/journal.pone.0055518
O’Neill, B., Moran, K., & Gillespie, A. (2010).
Scaffolding rehabilitation behaviour using a
voice-mediated assistive technology for cogni-
tion. Neuropsychological Rehabilitation, 20(4), 509-
527. doi:10.1080/09602010903519652
Occupational Therapy Practice Framework:
Domain & Process 2nd Edition. (2008). The
American Journal of Occupational Therapy, 62(6),
625-683. doi:10.5014/ajot.62.6.625
Ochsner, K. N. (2008). The Social-Emotional
Processing Stream: Five Core Constructs and
Their Translational Potential for Schizophrenia
and Beyond. Biological Psychiatry, 64(1), 48-61.
doi:10.1016/j.biopsych.2008.04.024
Ochsner, K. N., & Gross, J. J. (2005). The cogni-
tive control of emotion. Trends in cognitive sciences,
9(5), 242-249. doi:10.1016/j.tics.2005.03.010
Oremus, M., Santaguida, P., Walker, K., Wishart,
L. R., Siegel, K. L., & Raina, P. (2012). Studies
of stroke rehabilitation therapies should re-
port blinding and rationalize use of outcome
measurement instruments. Journal of clinical
epidemiology, 65(4), 368-374. doi:10.1016/j.jcline-
pi.2011.10.013
Ortega-Tudela, J. M., & Gómez-Ariza, C. J.
(2006). Computer-assisted teaching and math-
ematical learning in Down Syndrome children.
Journal of Computer Assisted Learning, 22(4), 298-
307. doi:10.1111/j.1365-2729.2006.00179.x
Parsons, S., & Mitchell, P. (2002). The poten-
tial of virtual reality in social skills training for
people with autistic spectrum disorders. Journal
of Intellectual Disability Research, 46(5), 430–443.
doi:10.1046/j.1365-2788.2002.00425.x
Peretz, C., Korczyn, A. D., Shatil, E., Aha-
ronson, V., Birnboim, S., & Giladi, N. (2011).
Computer-based, personalized cognitive train-
ing versus classical computer games: a rand-
omized double-blind prospective trial of cogni-
tive stimulation. Neuroepidemiology, 36(2), 91-99.
doi:10.1159/000323950
Posner, M.I. (1995). Forward. In: Rugg, M. D.,
& Coles, M. G. H. (Eds.) Electrophysiology of
Mind. Oxford: University Press.
Posner, M. I., & Petersen, S. E. (1990). The
attention system of the human brain. Annual
review of neuroscience, 13, 25-42. doi:10.1146/an-
nurev.ne.13.030190.000325
Prigatano, G. P. (1999). Principles of Neuropsycho-
logical Rehabilitation. Oxford University Press Inc.
Rabiner, D. L., Murray, D. W., Skinner, A. T.,
& Malone, P. S. (2010). A Randomized Trial of
Two Promising Computer-Based Interventions
for Students with Attention Difficulties. Jour-
nal of Abnormal Child Psychology, 38(1), 131-142.
doi:10.1007/s10802-009-9353-x
Rebok, G. W., Carlson, M. C., & Langbaum, J.
B. S. (2007). Training and Maintaining Memory
Abilities in Healthy Older Adults: Traditional
and Novel Approaches. The Journals of Gerontol-
ogy Series B: Psychological Sciences and Social Sciences,
62(Special Issue 1), 53-61.
Riddoch, M., & Humphreys, G. (2001). Object
Recognition. In: B. Rapp (Ed.) Handbook of Cog-
nitive Neuropsychology. Hove: Psychology Press
Roig, T. & Sánchez-Carrión, R. (2005) Apli-
caciones de las nuevas tecnologías en la reha-
bilitación neuropsicológica en los traumatismos
craneoencefálicos (TCE) En: Montagut F.,
Flotats G., Lucas E. Rehabilitación domiciliaria.
Principios, indicaciones y programas terapéuticos. Bar-
celona: Masson.
Sablier, J., Stip, E., Franck, N., Giroux, S.,
Pigot, H., & Nadeau-Marcotte, F. (2011).
Mobus project-assistive technology for im-
proving cognition and autonomy of patients
with schizophrenia. International Clinical Psy-
chopharmacology, 26, e65-e66. doi:10.1097/01.
yic.0000405743.97198.55
Salas, C., Báez, M. T., Garreaud, A. M., & Dac-
carett, C. (2007). Experiences and challenges
in cognitive rehabilitation: towards a model of
contextualized intervention? Rev. chil. neuropsicol.
(Impr.), 2(1), 21-30.
Sánchez-Carrión, R., Gómez Pulido, A., García-
Molina, A., Rodríguez Rajo, P., & Roig Rovira,
T. (2011) Tecnologías aplicadas a la rehabili-
tación neuropsicológica. In: Bruna, O., Roig,
T., Puyuelo, M., Junqué, C. & Ruano, A. (Eds.)
Rehabilitación neuropsicológica. Intervención y práctica
clínica (pp. 131-140). Barcelona: Masson
Sánchez Cubillo, I. (1 de Abril, 2011) Actual-
ización en Cognición Social: a propósito de dos casos
[diapositivas en PowerPoint].
Sansosti, F. J., & Powell-Smith, K. A. (2008).
Using Computer-Presented Social Stories and
Video Models to Increase the Social Commu-
nication Skills of Children With High-Func-
tioning Autism Spectrum Disorders. Journal
of Positive Behavior Interventions, 10(3), 162-178.
doi:10.1177/1098300708316259
Santaguida, P., Oremus, M., Walker, K., Wishart,
L. R., Siegel, K. L., & Raina, P. (2012). System-
atic reviews identify important methodological
flaws in stroke rehabilitation therapy primary
studies: review of reviews. Journal of clinical
epidemiology, 65(4), 358-367. doi:10.1016/j.jcline-
pi.2011.10.012
Schachter, D. L., & Endel, T. (1994). Memory sys-
tems 1994. MIT Press.

NeuronUP Theoretical framework: General Concepts
80
Scherer, M. J., Assistive technology: Matching de-
vice and consumer for successful rehabilitation. (2002)
(Vol. XIII). Washington, DC, US: American
Psychological Association.
Schmidt, N. B., Richey, J. A., Buckner, J. D., &
Timpano, K. R. (2009). Attention training for
generalized social anxiety disorder. Journal of
abnormal psychology, 118(1), 5-14. doi:10.1037/
a0013643
Schmitter-Edgecombe, M., Fahy, J. F., Whelan,
J. P., & Long, C. J. (1995). Memory remediation
after severe closed head injury: notebook train-
ing versus supportive therapy. Journal of consult-
ing and clinical psychology, 63(3), 484-489.
Seo, Y.-J., & Bryant, D. P. (2009). Analysis of
studies of the effects of computer-assisted in-
struction on the mathematics performance of
students with learning disabilities. Computers &
Education, 53(3), 913-928. doi:10.1016/j.com-
pedu.2009.05.002
Sepchat, A., Descarpentries, S., Monmarché,
N., & Slimane, M. (s. f.). MP3 Players and Au-
dio Games: An Alternative to Portable Video
Games Console for Visually Impaired Players.
En K. Miesenberger, J. Klaus, W. Zagler, & A.
Karshmer (Eds.), Computers Helping People with
Special Needs (Vol. 5105, pp. 553-560). Berlin,
Heidelberg: Springer Berlin Heidelberg.
Shalev, L., Tsal, Y., & Mevorach, C.
(2007). Computerized Progressive Atten-
tional Training (CPAT) Program: Effec-
tive Direct Intervention for Children with
ADHD. Child Neuropsychology, 13(4), 382-388.
doi:10.1080/09297040600770787
Shatil, E., Metzer, A., Horvitz, O., & Miller,
A. (2010). Home-based personalized cognitive
training in MS patients: a study of adherence
and cognitive performance. NeuroRehabilitation,
26(2), 143-153. doi:10.3233/NRE-2010-0546
Shaw, R., & Lewis, V. (2005). The impact of
computer-mediated and traditional academic
task presentation on the performance and be-
haviour of children with ADHD. Journal of
Research in Special Educational Needs, 5(2), 47–54.
doi:10.1111/J.1471-3802.2005.00041.x
Silver, M., & Oakes, P. (2001). Evaluation of a
New Computer Intervention to Teach People
with Autism or Asperger Syndrome to Recognize
and Predict Emotions in Others. Autism, 5(3),
299-316. doi:10.1177/1362361301005003007
Sitdhisanguan, K., Chotikakamthorn, N.,
Dechaboon, A., & Out, P. (2012). Using tangi-
ble user interfaces in computer-based training
systems for low-functioning autistic children.
Personal and Ubiquitous Computing, 16(2), 143-155.
doi:10.1007/s00779-011-0382-4
Sohlberg, M M, & Mateer, C. A. (1987). Effec-
tiveness of an attention-training program. Jour-
nal of clinical and experimental neuropsychology, 9(2),
117-130. doi:10.1080/01688638708405352
Sohlberg, M., & Mateer, C. A. (1989). Introduc-
tion to Cognitive Rehabilitation. Guilford Publica-
tions.
Sohlberg, McKay Moore, Ehlhardt, L., & Ken-
nedy, M. (2005). Instructional techniques in
cognitive rehabilitation: a preliminary report.
Seminars in speech and language, 26(4), 268-279.
doi:10.1055/s-2005-922105
Solari, A., Motta, A., Mendozzi, L., Pucci, E.,
Forni, M., Mancardi, G., & Pozzilli, C. (2004).
Computer-aided retraining of memory and
attention in people with multiple sclerosis: a
randomized, double-blind controlled trial. Jour-
nal of the Neurological Sciences, 222(1–2), 99-104.
doi:10.1016/j.jns.2004.04.027
Squire, L. R. (2004). Memory systems of the
brain: A brief history and current perspective.
Neurobiology of Learning and Memory, 82(3), 171-
177. doi:10.1016/j.nlm.2004.06.005
Stahmer, A. C., Schreibman, L., & Cunningham,
A. B. (2011). Toward a technology of treatment
individualization for young children with autism
spectrum disorders. Brain research, 1380, 229-
239. doi:10.1016/j.brainres.2010.09.043
Standen, P. J., & Brown, D. J. (2005). Virtual re-
ality in the rehabilitation of people with intellec-
tual disabilities: review. Cyberpsychology & behav-
ior: the impact of the Internet, multimedia and virtual
reality on behavior and society, 8(3), 272-282; discus-
sion 283-288. doi:10.1089/cpb.2005.8.272
Steiner, N. J., Sheldrick, R. C., Gotthelf, D., &
Perrin, E. C. (2011). Computer-Based Attention
Training in the Schools for Children With At-
tention Deficit/Hyperactivity Disorder: A Pre-
liminary Trial. Clinical Pediatrics, 50(7), 615-622.
doi:10.1177/0009922810397887
Stern, R.A. y Prohaska, M.L. (1996). Neuro-
spychological evaluation of executive function-
ing. In: L.J. Dikstein, M.B. Riba y J.M. Oldham
(eds.): Review of Psychiatry, Neuropsychiatry for clini-
cians. Washington: American Psychiatric Press.
Stromer, R., Kimball, J. W., Kinney, E. M., &
Taylor, B. A. (2006). Activity Schedules, Com-
puter Technology, and Teaching Children With
Autism Spectrum Disorders. Focus on Autism and
Other Developmental Disabilities, 21(1), 14-24. doi:
10.1177/10883576060210010301
Susie R Wood, N. M. (2003). Motivating, game-
based stroke rehabilitation: a brief report. Topics
in stroke rehabilitation, 10(2), 134-40.
NeuronUP Theoretical framework: General Concepts
81
Suslow, T., Schonauer, K., & Arolt, V. (2001).
Attention training in the cognitive rehabilitation
of schizophrenic patients:a review of efficacy
studies. Acta Psychiatrica Scandinavica, 103(1),
15–23. doi:10.1111/j.1600-0447.2001.00016.x
Tam, S.-F., & Man, W.-K. (2004). Evaluating
computer-assisted memory retraining pro-
grammes for people with post-head injury am-
nesia. Brain injury: [BI], 18(5), 461-470. doi:10.1
080/02699050310001646099
Tanaka, S. C., Doya, K., Okada, G., Ueda, K.,
Okamoto, Y., & Yamawaki, S. (2004). Prediction
of immediate and future rewards differentially
recruits cortico-basal ganglia loops. Nature Neu-
roscience, 7(8), 887-893. doi:10.1038/nn1279
Tang, Y.-Y., & Posner, M. I. (2009). Attention
training and attention state training. Trends in
cognitive sciences, 13(5), 222-227. doi:10.1016/j.
tics.2009.01.009
Teasell, R. W., Foley, N. C., Bhogal, S. K., &
Speechley, M. R. (2003). An evidence-based
review of stroke rehabilitation. Topics in stroke
rehabilitation, 10(1), 29-58.
Thornton, K. E., & Carmody, D. P. (2008). Ef-
ficacy of traumatic brain injury rehabilitation:
interventions of QEEG-guided biofeedback,
computers, strategies, and medications. Applied
psychophysiology and biofeedback, 33(2), 101-124.
doi:10.1007/s10484-008-9056-z
Tirapu Ustárroz, J., García Molina , A. & Roig
Rovira, T. (2007). Validez ecológica en la ex-
ploración de las funciones ejecutivas. Anales de
Psicología, 23(2) 289-299.
Tirapu Ustárroz, J., & Luna Lario, P. (2008).
Neuropsicología de las funciones ejecutivas,
221-256.
Tirapu-Ustárroz, J., Pérez-Sayes, G., Erekatxo-
Bilbao, M., & Pelegrín-Valero, C. (2007). [What
is theory of mind?]. Revista de neurologia, 44(8),
479-489.
Tulving, E. (1985). How many memory systems
are there? American Psychologist, 40(4), 385-398.
doi:10.1037/0003-066X.40.4.385
Tulving, E. (1999). Memory, Consciousness,
and the Brain. The Tallinn Conference. (pp. 66-68).
Psychology Press.
Tulving, E. (2002). Episodic Memory:
From Mind to Brain. Annual Review of Psy-
chology, 53(1), 1-25. doi:10.1146/annurev.
psych.53.100901.135114
Van den Broek, M. D., Downes, J., Johnson, Z.,
Dayus, B., & Hilton, N. (2000). Evaluation of
an electronic memory aid in the neuropsycho-
logical rehabilitation of prospective memory
deficits. Brain injury: [BI], 14(5), 455-462.
Van Heugten, C., Wolters Gregório, G., & Wade,
D. (2012). Evidence-based cognitive rehabilita-
tion after acquired brain injury: A systematic re-
view of content of treatment. Neuropsychological
Rehabilitation, 22(5), 653-673. doi:10.1080/0960
2011.2012.680891
Verdejo García, A. V., & Bechara, A. (2010).
Neuropsicología de las funciones ejecutivas.
Psicothema, 22(2), 227-235.
Vogt, A., Kappos, L., Calabrese, P., Stöcklin,
M., Gschwind, L., Opwis, K., & Penner, I.-K.
(2009). Working memory training in patients
with multiple sclerosis - comparison of two dif-
ferent training schedules. Restorative neurology and
neuroscience, 27(3), 225-235. doi:10.3233/RNN-
2009-0473
Wainer, A. L., & Ingersoll, B. R. (2011). The use
of innovative computer technology for teach-
ing social communication to individuals with
autism spectrum disorders. Research in Autism
Spectrum Disorders, 5(1), 96-107. doi:10.1016/j.
rasd.2010.08.002
Warrington, E. K., & Taylor, A. M. (1978). Two
categorical stages of object recognition. Percep-
tion, 7(6), 695-705.
Weinberg, J., Diller, L., Gordon, W. A., Gerst-
man, L. J., Lieberman, A., Lakin, P., … Ezrachi,
O. (1979). Training sensory awareness and spa-
tial organization in people with right brain dam-
age. Archives of physical medicine and rehabilitation,
60(11), 491-496.
Werry, I., Dautenhahn, K., Ogden, B., & Har-
win, W. (2001). Can Social Interaction Skills
Be Taught by a Social Agent? The Role of a
Robotic Mediator in Autism Therapy. En Proc.
CT2001, The Fourth International Conference on Cog-
nitive Technology: Instruments of Mind, LNAI 2117
(pp. 57–74). Springer-Verlag.
Wertz, R., & Katz, R. (2004). Out-
comes of computer-provided treatment
for aphasia. Aphasiology, 18(3), 229-244.
doi:10.1080/02687030444000048
Westerberg, H., Jacobaeus, H., Hirviko-
ski, T., Clevberger, P., Östensson, M.-L.,
Bartfai, A., & Klingberg, T. (2007). Com-
puterized working memory training after
stroke–A pilot study. Brain Injury, 21(1), 21-29.
doi:10.1080/02699050601148726
Wilson, B A, Emslie, H. C., Quirk, K., & Ev-
ans, J. J. (2001). Reducing everyday memory
and planning problems by means of a paging
system: a randomised control crossover study.
Journal of neurology, neurosurgery, and psychiatry,
70(4), 477-482.
Wilson, B. (1987). Single-Case Experimental
Designs in Neuropsychological Rehabilitation.
Journal of Clinical and Experimental Neuropsychology,
9(5), 527-544. doi:10.1080/01688638708410767
Wilson, B. (1989). Models of cognitive reha-
bilitation. En R. L. Wood & P. Eames (Eds.),
Models of brain injury rehabilitation (pp. 117-141).
Baltimore, MD, US: Johns Hopkins University
Press.

NeuronUP Theoretical framework: General Concepts
82
Wilson, Barbara A, Emslie, H., Quirk, K., Evans,
J., & Watson, P. (2005). A randomized control
trial to evaluate a paging system for people with
traumatic brain injury. Brain injury: [BI], 19(11),
891-894.
Wilson, Barbara A. (2009). Memory Rehabilitation:
Integrating Theory and Practice. Guilford Press.
Yantz, C. L., Johnson-Greene, D., Higginson,
C., & Emmerson, L. (2010). Functional cook-
ing skills and neuropsychological functioning in
patients with stroke: an ecological validity study.
Neuropsychological rehabilitation, 20(5), 725-738.
doi:10.1080/09602011003765690
Young, A.W. & Ellis, H.D. (2000) Overt and cov-
ert face recognition. In: Revonsu, A. & Rossetti,
Y., (Eds.) Dissociation but Interaction between Con-
scious and Unconscious Processing. (pp. 195–219) Ed.
John Benjamins.
Zangwill, O. L. (1947). Psychological Aspects of
Rehabilitation in Cases of Brain Injury1. British
Journal of Psychology. General Section, 37(2), 60–69.
doi:10.1111/j.2044-8295.1947.tb01121.x
Zhao, C., Deng, W., & Gage, F. H. (2008). Mech-
anisms and functional implications of adult neu-
rogenesis. Cell, 132(4), 645-660. doi:10.1016/j.
cell.2008.01.033

NeuronUP Theoretical framework: General Concepts
83
NEURONUP
Theoretical framework:General Concepts