two red flag symptoms in urology: haematuria and ... · pdf filethe royal marsden two red flag...
TRANSCRIPT
The Royal Marsden
Two red flag symptoms in urology: haematuria and testicular lumps Mr Erik Mayer, Consultant Surgeon
Change Presentation title and date in Footer dd.mm.yyyy 1

The Royal Marsden
Contents
− Referral Guidelines
− Diagnostics
− Differential Diagnosis
2

The Royal Marsden
Haematuria

The Royal Marsden
Causes of Haematuria
– Infection (cystitis, prostatitis).
– Tumour (renal cell, Wilms' tumour, bladder, prostate).
– Trauma.
– Inflammation (glomerulonephritis, IgA nephropathy, Henoch-Schonlein purpura, systemic lupus erythematosus).
– Structural (calculi, polycystic kidney disease).
– Haematological.
– Surgery.
– Toxins (NSAIDs, sulphonamides, cyclophosphamide).
The Royal Marsden
Why the NICE Guidance?
– UK has worse survival than other countries
– New guidance to broaden (lower threshold) for
referral – actually more confusing
5

The Royal Marsden
NICE Guidance 6

The Royal Marsden
‘Unexplained’
Unexplained Symptoms or signs that have not led to a
diagnosis being made by the healthcare professional in
primary care after initial assessment (including history,
examination and any primary care investigations)
– Primary care investigations:
– History/examination
– Bloods
– BP
– Urine Dipstick/culture
– Urine cytology
– Ultrasound
7

The Royal Marsden 8
• Dipstick versus microscopy (high-false negative rate)
• Trace versus 1+ (Trace considered negative)
• Haemolysed versus non-haemolysed (No difference)
• Persistence NVH is defined as 2 out of 3 dipsticks positive for NVH.
• Haematuria does not result from anti-coagulants or anti-platelets
Non-visible Haematuria
• Exclude UTI and/or other transient cause.
• Plasma creatinine/eGFR.
• Measure proteinuria on a random sample.
Send urine for protein:creatinine ratio
(PCR) or albumin:creatinine ratio (ACR)
on a random sample
• Blood pressure
Visible Haematuria
• Exclude UTI and/or other
transient cause.

The Royal Marsden 9

The Royal Marsden
Bladder TCC
80% of patients with a bladder tumour will present with painless
visible haematuria

The Royal Marsden 11

The Royal Marsden
Lessons Learnt
– Bladder cancer most frequent diagnosis after NO
DIAGNOSIS and UTI – 1 in 20 risk for Non-visible
haematuria and 1 in 5 risk for Visible haematuria
– Cancer diagnosis in 1 in 4 for Visible Haematuria and
1 in 10 for Non-visible Haematuria
– Ultrasound or IVU alone would have missed 50% of
upper tract tumours
– Cystoscopy recommended for all patients
12

The Royal Marsden
Projected Age-standardised Rates
13

The Royal Marsden
Risk Factors
– Smoking
– 37% of bladder cancers in the UK are linked to
tobacco smoking
– Bladder cancer risk is 73-80% lower in ex-smokers
who quit 25 years previously
– Aromatic Amines
– Production of dyes, rubber, and textiles
– Hairdressers/Barbers
14

The Royal Marsden
Increases risk ('sufficient' or
'convincing' evidence) – Aluminium production
– 4-Aminobiphenyl
– Arsenic and inorganic arsenic compounds
– Auramine production
– Benzidine
– Chlornaphazine
– Cyclophosphamide
– Magenta production
– 2-Naphthylamine
– Painting
– Rubber production industry
– Schistosoma haematobium
– Tobacco smoking
– ortho-Toluidine
– X-radiation, gamma-radiation
– 4-Chloro-ortho-toluidine
– Coal-tar pitch
– Coffee
– Dry cleaning
– Engine exhaust, diesel
– Hairdressers and barbers (occupational exposure)
– Pioglitazone
– Printing processes
– Soot
– Textile manufacturing
– Tetrachloroethylene
15
May increase risk ('limited' or
'probable' evidence)

The Royal Marsden
Routes to Diagnosis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Stage 1 Stage 2 Stage 3 Stage 4 Stage unknown
Stage
Percentage of tumour stages by presentation route, Bladder, 2012-2013
Death certificate only & unknown
Emergency presentation
Other managed
GP referral
Two week wait
Screen detected
Presentation route
Perc
enta
ge
of
dia
gno
ses
16

Bladder Cancer (C67 D090 D414): 2002-2006 Five-Year Relative Survival (%) by Stage, Adults Aged 15-99, Former Anglia Cancer Network
Prepared by Cancer Research UK Original data source: The National Cancer Registration Service, Eastern Office. Personal communication. http://ecric.org.uk/

The Royal Marsden
Haematuria
– Visible versus Non-visible
– Painful or painless
– Initial/mid/end/throughout
– Trauma
– Previous history
Dysuria/smelly urine
Pain on ejaculation
Haematuria/haematospermia
STD’s/UTI’s
Previous urological history/surgery
Family history of urinary tract malignancy/stones
Smoker
Occupation
(Sexual history)

The Royal Marsden
Haematuria
– 2WW pathway
– Typically one stop:
– Investigations:
– Urine Culture/Urine Cytology
– US KUB or CT IVU
– Flexible Cystoscopy

The Royal Marsden
Flexible Cystoscopy

The Royal Marsden 21
Rate is no different to background incident rate

The Royal Marsden
Urgent (2WW) referral
Urgent referral is required for:
– All adult patients with painless visible haematuria.
– Patients >50 years with unexplained non-visible
haematuria (Greater than trace)
– Patients >40 years with recurrent/persistent UTI
associated with haematuria.
– Symptoms of UTI with persistent sterile pyuria >50
years old
22

The Royal Marsden
Take home messages
– 2WW Referral for haematuria very acceptable
– As Urologists we try and funnel most through one-
stop haematuria clinic as best environment for
diagnosis of several pathologies
– Two patient groups to be wary of:
– Squamous Cell Carcinoma and long-term
catheters (spinal cord injury patients)
– Female with recurrent UTIs
23

The Royal Marsden
Take home messages
24

The Royal Marsden
Male vs. Female
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Male
s
Fe
male
s
Male
s
Fe
male
s
Male
s
Fe
male
s
Male
s
Fe
male
s
Male
s
Fe
male
s
Male
s
Fe
male
s
Screen detected Two week wait GP referral Other managed Emergency presentation
Death certificate
only &
unknown
Presentation route and sex
Percentage of presentation routes and sex by tumour stage, Bladder, 2012-2013
Stage unknown
Stage 4
Stage 3
Stage 2
Stage 1
Stages
Perc
enta
ge o
f dia
gno
ses
25

The Royal Marsden 26

The Royal Marsden
Testicular lumps

The Royal Marsden
Referral Guidelines
28

The Royal Marsden
Diagnosis

The Royal Marsden
Diagnostics
– History
– Clinical Examination
– Genitals
– Abdomen
– Supraclavicular Lymphadenopathy
– Urine Dipstick & Pregnancy Test
– Tumour Markers
– Ultrasound
30

The Royal Marsden
History
Symptoms
• Hard, painless lump
- Partner detection
• 5-10% scrotal pain
• - Intra-tumoural haemorrhage
- Trauma brings attention to abnormality
• Metastatic
- Weight loss
- Shortness of Breath
- Back/abdominal pain
- Neck lumps
31

The Royal Marsden
Key Points in a Scrotal Mass History
– The Lump
– How was it detected (in the bath etc.)?
– How long has it been there?
– Is it changing in size?
– Painful or painless
– Sexual history – Any recent STIs
– Any lower urinary tract symptoms
– Any recent testicular trauma
32

The Royal Marsden
Key points continued
− Any abdominal or neck lumps (lymphadenopathy)
− Any SOB or abdominal pain
− PMH
− Previous orchidopexy/maldescent of testicle
− Have they had testicular US scan before/been encouraged to regularly self examine
− FH of testicular Cancer
33

The Royal Marsden
Clinical Examination
34

The Royal Marsden
Which tumour markers might be raised in testicular cancer?
A. CA 19-9, CA 125
B. CEA, B-HCG
C. AFP, B-HCG, LDH
D. CA 125, AFP
E. None of the above
35

The Royal Marsden
Tumour Markers
AFP - raised in 50-70% of NSGCT – May be elevated with:
– hepatic dysfunction, cirrhosis, and – drug or alcohol abuse
- normal <10ng/mL – βhCG - raised in:
• 100% Choriocarcinoma • 60% Embryonal carcinoma • 55% Teratocarcinoma • 25% Yolk Cell Tumour • 7% Seminomas
- normal <5mIU/mL – False positive elevations - marijuana use – LDH- ↑in 30% to 80% of pure seminoma and 60% of
nonseminomas.
Useful in diagnosis, risk stratification & monitoring
36

The Royal Marsden
Ultrasound
37

The Royal Marsden
What I discuss with the patient
− Diagnosis
− Prognosis
− CxR/CT scan/tumour markers
− Need for Surgery as first line treatment
− Testicular Prosthesis
− Fertility/Sperm Storage
− Possible further treatment
38
The Royal Marsden
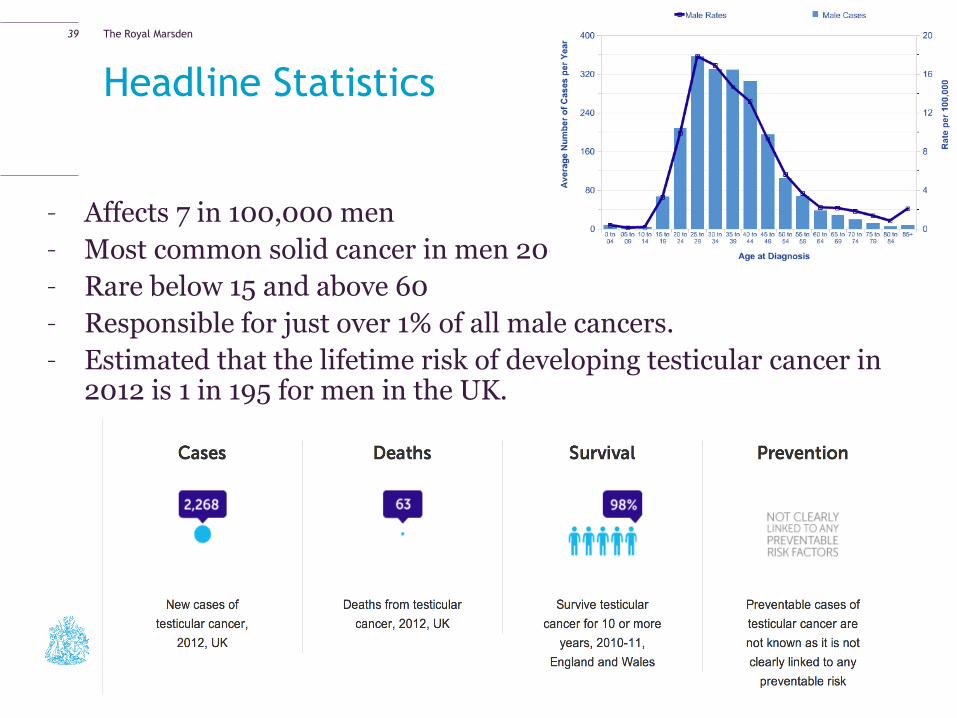
Headline Statistics
– Affects 7 in 100,000 men
– Most common solid cancer in men 20-45
– Rare below 15 and above 60
– Responsible for just over 1% of all male cancers.
– Estimated that the lifetime risk of developing testicular cancer in 2012 is 1 in 195 for men in the UK.
39

The Royal Marsden
European Age-Standardised Incidence Rates per 100,000
Population, Males, Great Britain
Headline Statistics
40

The Royal Marsden
Headline Statistics European Age-Standardised Mortality Rates per
100,000 Population, Males, UK
One-, Five- and Ten-Year Net Survival (%), Adults Aged 15-99, England & Wales
1-Year Survival (%)
5-Year Survival (%)
10-Year Survival (%)
Men
Net Survival 99.1 98.3 98.2
95% LCL 99.1 98.3 98.2
95% UCL 99.1 98.3 98.2
41

The Royal Marsden
Operating is not always best for the patient
42

The Royal Marsden
Orchidectomy: Inguinal vs. Scrotal approach
– Meta-analysis
– Scrotal violation → ↑ local recurrence from 0.4 – 2.9%
Capelouto et al., 1995
43

The Royal Marsden
Prosthesis
– Infection risk
– Think Chemotherapy
– Long-term safety
– Cosmesis/Migration
– About 25% uptake
44

The Royal Marsden
Sperm Storage
– Andrology Lab - Hammersmith
– Hep B/C, HIV & CMV screening
– No desperate need to do pre-op although is recommended in
EAU guidelines (3 samples/3 day abstinence)
– Cost associated after year one
– Collecting and freezing the samples can cost between £200
and £400. Then you pay about £300 a year to store them
– Standard storage period 10 years
– Quality of the sperm not guaranteed
45

The Royal Marsden
Further Treatment
– Oncological outcomes – overall survival
– Reducing burden of follow-up
– Minimising ‘overtreatment’ and treatment related morbidity
46

The Royal Marsden
So it’s NOT Cancer
Most testicular lumps are NOT cancer. At a testicular clinic at the Queen Elizabeth Hospital in Birmingham, only 76 cancers were found out of 2,000 men seen with a testicular lump. This means that fewer than 4 in every
100 testicular lumps (4%) are cancer
The awkward Scrotum
47

The Royal Marsden
Differential Diagnosis
– Any cause of scrotal lump/pain
– Testicular torsion
– Torted hydatid of Morgagni
– Epididymal cyst(s)
– Hydrocoele
– Varicocoele
– Epididymitis (orchitis)
– Hernia
– Adenomatoid Tumour
Other findings on Ultrasound
Microlithiasis
Varicocoele
48

The Royal Marsden
Microlithiasis
– Common – up to 10% men referred for Ultrasound
– Increasingly detected with higher frequency US
– Is it Premalignant?
49
The Royal Marsden
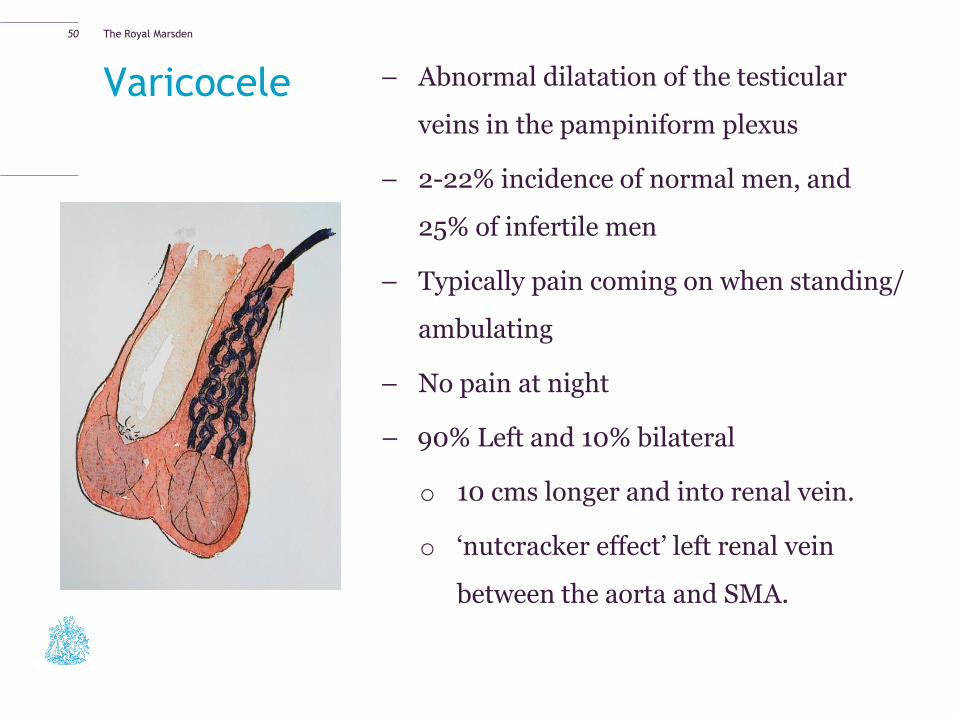
Varicocele – Abnormal dilatation of the testicular
veins in the pampiniform plexus
– 2-22% incidence of normal men, and
25% of infertile men
– Typically pain coming on when standing/
ambulating
– No pain at night
– 90% Left and 10% bilateral
o 10 cms longer and into renal vein.
o ‘nutcracker effect’ left renal vein
between the aorta and SMA.
50

The Royal Marsden
Varicocoele
– Consider underlying cause if:
• Sudden onset of varicocoele
• Right sided varicocoele
• Does not collapse on being supine
51
– Grade 0:
– subclinical varicocoele.
– Grade 1:
– palpable only with valsalva.
– Grade 2:
– Clinically palpable in upright position.
– Grade 3:
– Gross varicocoele with ‘bag of worms’ visible through skin.

The Royal Marsden
Varicocoeles and fertility
– Varicocoeles do not cause infertility
– Routine testing of semen parameters not
required
– Do not require treatment unless associated
with abnormal semen parameters and low
testicular volume in the context of infertility
– Always consider female infertility factors
52

The Royal Marsden
Treatment
– Treatment Conservative/embolisation/ ligation
– Be guarded about outcome
– Natural History may demonstrate improvement
53

The Royal Marsden
Torsion
– Testicular torsion
– Torsion of a testicular appendage (appendix testis, Hydatid of Morgagni)
– Torsion
– Acute testicular pain (unilateral)
– Radiation to lower abdomen
– Nausea & vomiting
– Negative urine dipstick
– Main investigation is scrotal exploration
– (Ultrasound)
54

The Royal Marsden
Torsion
− Immediate referral to A&E
− No investigation needed
− Scrotal exploration, untwisting of testicle and bilateral 3-point
fixation with non-absorbable sutures in adult, dartos pouch in
children
− Warm ischaemia time 6 hours
− Torted Hydatid of Morgagni – conservative treatment an option
if diagnosis clear
55

The Royal Marsden
Infection
–Acute epididymitis/Epididymo-orchitis
– Bacterial
– In older men, UTI organisms
– In younger men, Chlamydia and Gonococcus
History
– Examination; tender swelling of epididymis +/- secondary
hydrocoele
– 21 days of appropriate antibiotic but warn patient that swelling
may persist >6 weeks
– Scrotal support
– Patient typically ends up with repeat ultrasound
56

The Royal Marsden 57

The Royal Marsden
Follow-up Ultrasound
– Epididymal/Testicular abscess
– Testicular infarction
– Underlying tumour
58

The Royal Marsden
Infection
–Orchitis
Can be extension of epididymorchitis
Viral
• Mumps, ?other viruses
• History of parotitis
• Supportive measures – analgesia, bed rest
• Steroids? Tunical incision
If bilateral, mumps orchitis post-puberty may lead to
atrophy and subfertility
59

The Royal Marsden
Epididymal cysts and hydroceles
60

The Royal Marsden
Aetiology
Epididymal Cyst
– Possible results from
epididymal tube
obstruction
Hydrocoele
-Excess fluid production
Inflammation
Tumours
-Decreased fluid absorption
Post treatment for varicocoele
-Congenital
Patent Processus Vaginalis
61

The Royal Marsden
Clinical Appearance
62

The Royal Marsden
Epididymal Cyst
63

The Royal Marsden
Management
Epididymal Cyst
– Conservative
- Why not to operate:
– Pain does not improve
– Pain can be made worse
– Recurrence
– Epididymal obstruction
Hydrocoele
– Conservative
– Aspiration
– Aspiration + Sclerotherapy
64

The Royal Marsden
Inguino-scrotal Hernia
65
The Royal Marsden
Take Home Messages
− Scrotal Lumps and Bumps can be difficult to confidently
diagnose
− Always get an Ultrasound (urgent vs. routine)
− If in doubt 2WW referral
− Elements of managing new testicular cancer patient
− Benign scrotal pathology can generally be managed
conservatively
− Except torsion
66