urachal cysthhh
DESCRIPTION
tgggTRANSCRIPT

Treatment of Infected Urachal CystsKoo Han Yoo, Sun-Ju Lee, and Sung-Goo Chang
Author information ► Article notes ► Copyright and License information ►
This article has been cited by other articles in PMC.
Go to:
Abstract
The urachus is a fibrous cord that arises from the anterior bladder wall and extends cranially to the umbilicus. Traditionally, infection has been treated using a two-stage procedure that includes an initial incision and drainage which is then followed by elective excision. More recently, it has been suggested that a single-stage excision with improved antibiotics is a safe option. Thus, we intended to compare the effects of the two-stage procedure and the single-stage excision. We performed a retrospective review on nine patients treated between May 1990 and September 2005. The methods used in diagnosis were ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and cystoscopy. The study group was comprised of three males and six females with a mean age of 28.2 years (with a range from three to 71 years). Symptoms consisted of abdominal pain, abdominal mass, fever, and dysuria. The primary incision and drainage followed by a urachal remnant excision with a bladder cuff excision (two-stage procedure) was performed in four patients. The mean postoperative hospitalization lasted 5.8 days (with a range of three to seven days), and there were no reported complications. A primary excision of the infected urachal cyst and bladder cuff (single-stage excision) was performed in the other five patients. These patients had a mean postoperative hospitalization time of 9.2 days (with a range of four to 15 days), and complications included an enterocutaneous fistula, which required additional operative treatment. The best method of treating an infected urachal cyst remains a matter of debate. However, based on our results, the two-stage procedure is associated with a shorter hospital stay and no complications. Thus, when infection is extensive and severe, we suggest that the two-stage procedure offers a more effective treatment option.
Keywords: Urachal cyst, infectionGo to:
INTRODUCTION
The urachus is a fibrous cord that arises from the anterior bladder wall and extends cranially to the umbilicus.1 Urachal cysts are rare anomalies that occur from the urachus. Most urachal cysts are not detected until adulthood, although they are detected rarely in asymptomatic children.2,3 A urachal cyst presents four anomalies: a patent urachus, a vesicourachal diverticulum, urachal cysts, and a urachal sinus.4-8
The treatment of urachal cysts involves primary excision of the cyst. However, the traditional treatment of an infected urachal cyst is composed of a two-stage approach, i.e., an incision and then drainage of the infected cyst followed by secondary excision.2-4 Recently, Newman et al.9 suggested that with the advent of improved antimicrobials and earlier detection, a single-stage procedure can be safely accomplished. However, studies which compared the two different treatments reported that single-stage excisions result in complications and longer postoperative hospitalizations, and that the two-stage procedure is complication-free.4,10 We conducted this study to evaluate the comparative effectiveness of both the single-stage excision and the two-stage procedure.
Go to:
MATERIALS AND METHODS
We performed a retrospective review of nine patients who had been diagnosed with an infected urachal cyst and who were treated at our institution from May 1990 to September 2005. We reviewed imaging studies, pathological specimens and hospital records, and checked patients' symptoms, diagnoses, treatments, and results. The study group was comprised of three males and six females, with a mean age of 28.2 years (with a range of three to 71 years). Laboratory studies included urinalysis, urine cultures, wound cultures, and blood cultures. Pyuria was defined as more than five white blood cells per high power field on urinalysis. The imaging studies used were ultrasonography, computed
tomography (CT), magnetic resonance imaging (MRI), fistulography, voiding cystourethrography and cystoscopy.
The single-stage excision involves a primary excision of the infected urachal cyst and bladder cuff, whereas the two-stage procedure involves a primary incision and drainage, a delay to ensure that the infection has cleared, and then a later excision of the urachal remnant and bladder cuff.
Go to:
RESULTS
Of the nine patients, the most common symptom associated with an infected urachal cyst was abdominal pain (seen in eight cases); other symptoms included fever in six cases, dysuria in four patients, and umbilical discharge in one. In our study, seven infected urachal cysts were diagnosed in the nine patients by ultrasonography, which means the success rate of this diagnostic method was 77.8%. CT (four cases) and MRI (three cases) were used to determine the sizes of the infected urachal cysts, and fistulography (one case), voiding cystourethrography (one case) and cystoscopy (one case) were also performed (Table 1).
Table 1Patient Presentation Details
Four patients presented with pyuria by urinalysis, and E. coli was found by urine culture in one patient and by blood culture in another patient. Wound cultures discovered E. faecium in one patient and K. pneumonia in another patient (Table 2).

Table 2Results of Urinalysis, Urine Culture, Blood and Wound Culture
The primary excision of an infected urachal cyst and bladder cuff (single-stage excision) was performed in five patients. The mean number of postoperative hospitalization days was 9.2 (with a range of four to 15 days), and a complication was present in one patient: the patient developed an enterocutaneous fistula that required additional operative treatment (Table 3).
Table 3Results of the Single-Stage and Two-Stage Procedures
The two-stage procedure was performed in four patients. The interval of incision and drainage and secondary excision was 12.5 days (with a range of five to 14 days). The mean number of postoperative hospitalization days was 5.8 (with a range of three to seven), and there were no complications (Table 3).
Go to:
DISCUSSION
The optimal treatment method for infected urachal cysts remains a subject of debate. The present study shows that the two-stage procedure was complication-free (zero vs. one case) and involved a short postoperative hospitalization stay (5.8 vs. 9.2 days) compared with the single-stage excision. Although the introduction of improved antimicrobials and earlier detection by abdominal ultrasonography has improved the effectiveness of infected urachal cyst treatment, our results
suggest that the two-stage procedure remains a more effective treatment option.
Newman et al.9 suggested that improved antimicrobials and earlier detection allow the single-stage excision to be accomplished safely, and that the risks of this procedure compare with those of complication development during the two admissions and two operations of the two-stage procedure. However, McCollum et al.10 performed five single-stage excisions and six two-stage procedures, and found that two of the five single-stage excision patients experienced complications, but that all two-stage procedure patients were complication-free. Similarly, Minevich et al.4 reported that three of nine single-stage excision patients had complications, but all patients who had the two-stage procedure had no complications at all. Moreover, they reported mean postoperative hospital stays of 14 and 11.5 days for the single-stage excision and the two-stage procedure, respectively.
An infected urachal cyst can cause abdominal pain, abdominal tenderness, fever, nausea, vomiting, dysuria, voiding difficulty, N. gonorrhea urethritis, epididymitis, and orchitis at presentation.11-13 In our study, patients presented with abdominal pain (eight cases), fever (six cases), voiding difficulty (four cases), an abdominal mass (three cases), and umbilical discharge (one case).
The luminal wall of a urachal cyst is composed of transitional epithelium, and infection may occur due to the accumulation of materials within the cyst.14 Infected urachal cysts can disseminate infection by hematogenous or lympatic spread or through direct invasion of the bladder and umbilicus.15 Newman et al.9 and MacMillian et al.16 reported that S. aureus is the most common bacteria found in cystic fluid, and that other bacteria found were aerobic or anaerobic, such as E. coli. In our study, E. faecium and K. pneumonia were also cultured, and E. coli was grown from both urine and blood cultures.
Allen et al.5 and Ozbek et al.11 suggested that ultrasonography is an ideal modality for diagnosing urachal cysts, since these entities are cystic, extraperitoneal, and are directly related to the bladder. Nagasaki et al.17 reported a 75% diagnostic success rate for ultrasound, whereas

Minevich et al.4reported 57.1% and Cilento et al.18 reported 100%. However, cases of concomitant abscess and cellulitis were misinterpreted by ultrasonography. During primary diagnosis, ultrasonography, CT and MRI were performed to determine the size of the cyst and also the relationship between the peripheral tissue and the cyst.17 In the presence of an umbilical discharge, fistulography was performed to confirm the existence of a fistula, voiding cystourethrography was performed for reflux,9 and cystography was also carried out to investigate bladder cancer. In our study, seven infected urachal cysts were diagnosed in the nine patients that underwent ultrasonography. CT and MRI were used to confirm the extent of infection.
In one of our nine cases, an extensive and severely infected urachal cyst was excised using the single-stage procedure, and an enterocutaneous fistula developed during the postoperative period and became operatively manageable. However, since the urachal cyst was extensive and severe, the two-stage procedure should have been considered.
The optimal treatment method for infected urachal cysts remains a subject of debate. Based on our results, the two-stage procedure produces a shorter postoperative hospital stay and no complications. However, in the case of small and localized infections, a single-stage excision can be considered in young adults without comorbidity. Thus, when evaluating complication frequencies alone, we determined that the two-stage procedure presents a more-effective treatment option.
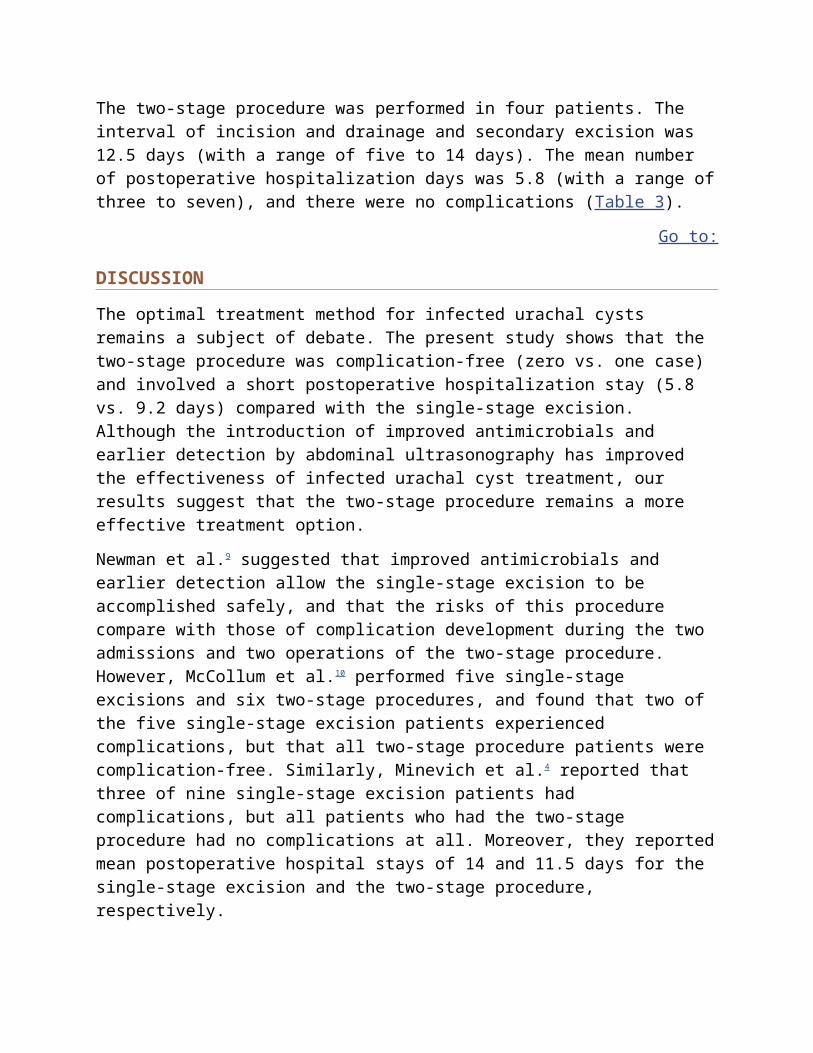
Fig. 1Abdominal ultrasonographic finding of a urachal cyst (longitudinal view). A cystic lesion is shown on the dome area of the urinary bladder (arrow).
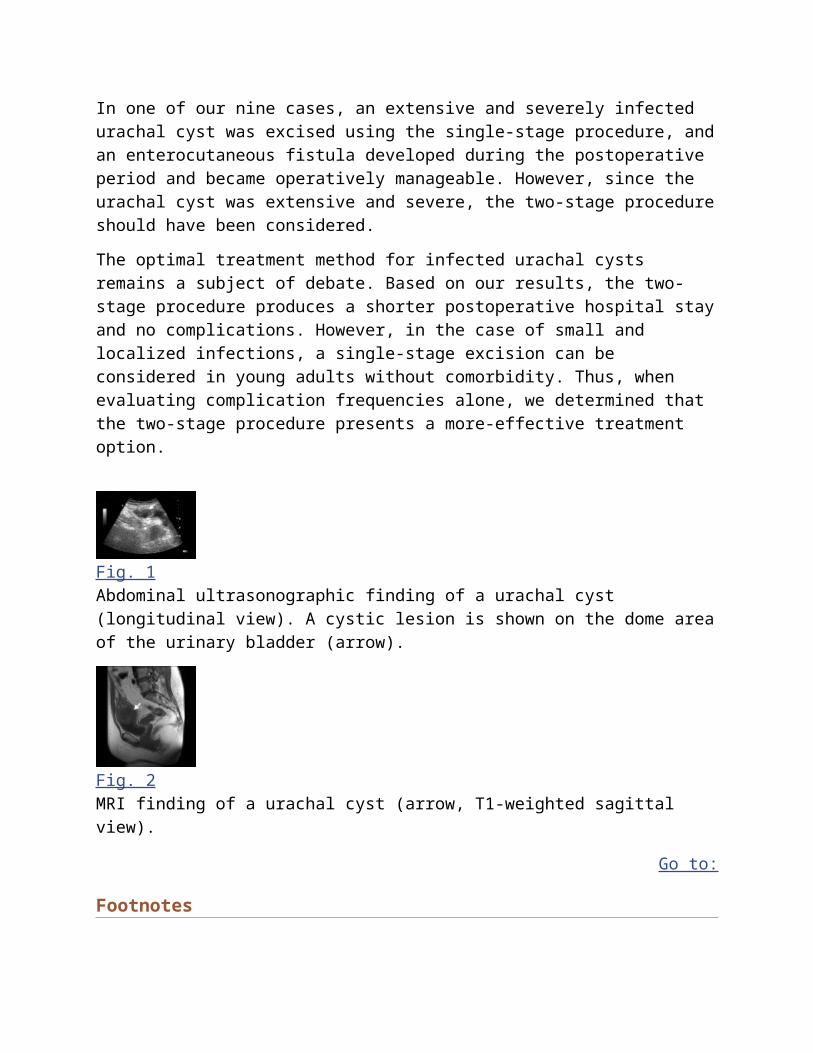
Fig. 2MRI finding of a urachal cyst (arrow, T1-weighted sagittal view).
Go to:
FootnotesThis work was supported by a grant R13-2002-020-01001-0 from the Korea Science & Engineering Foundation.
Go to:
References1. Gearhart JP. Exstrophy, epispadias, and other bladder anomalies. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, editors. Campbell's Urology. 8th ed. Philadelphia: Saunders; 2002. pp. 2136–2196.
2. Iuchtman M, Rahav S, Zer M, Mogilner J, Siplohttp://www.ncbi.nlm.nih.gov/pmc/articles/PMC2688164/
Urachal cystFrom Wikipedia, the free encyclopedia
Urachal cyst
Classification and external resources
ICD-10 Q 64.4
ICD-9 753.7
DiseasesDB 32765
MeSH D014496
A urachal cyst is a sinus remaining from the allantois during embryogenesis. It is a cyst which
occurs in the remnants between the umbilicus andbladder.[1] This is a type of cyst occurring in a
persistent portion of the urachus, presenting as an extraperitoneal mass in the umbilical region.
It is characterized by abdominal pain, and fever if infected. It may rupture, leading to peritonitis,
or it may drain through the umbilicus.[1] Urachal cysts are usually silent clinically until
infection, calculi or adenocarcinoma develop.[2]
Contents
[hide]
1 Symptoms
2 See also
3 References
4 External links
Symptoms[edit]
Lower abdominal pain
Pain on urination
Persistent umbilical discharge
Fever
UTI (Urinary Tract Infection)
Lump
Hematuria
http://en.wikipedia.org/wiki/Urachal_cyst
urachal cyst occurs when a pocket of air or fluid develops in the urachus. Before birth, the urachus is a primitive structure that connects the umbilical cord to the bladder in the developing fetus. The urachus normally disappears before birth, but part of the urachus may remain in some people after they are born. Urachal cysts can develop at any age, but typically affect older children and adults. Symptoms of a urachal cyst include pain in the abdomen, fever, or a lump that can be felt near the bellybutton. A urachal cyst is most often benign, but it can sometimes turn into
a cancer. For this reason, it is recommended that surgery be done to remove a urachal cyst.[1][5889]
http://rarediseases.info.nih.gov/gard/5425/urachal-cyst/resources/1
URACHAL ABNORMALITIESBefore birth, there is a connection between the bellybutton and the bladder. This connection, called the urachus, normally disappears before birth. But what happens if part of the urachus remains after birth? Read on to learn more about what problems can arise.What happens under normal conditions?
The bladder, located in the lower abdomen, is formed from structures located in the lower half of the developing fetus that are directly connected to the umbilical cord. After the first few weeks of gestation, this thick pathway to and from the placenta contains blood vessels, a merged channel to the future intestine and a tubular structure called the allantois. The internal part of the allantois is connected to the top of the developing bladder, and in ordinary circumstances, collapses and becomes a cord-like structure called the urachus. The formation and regression of this connection from the top of the bladder to the bellybutton are completed by the middle of the second trimester of pregnancy (approximately 20 weeks).Although the urachus is easily seen by a surgeon whenever an operation inside the abdomen or around the bladder is performed, it is a remnant of development that serves no further purpose but can be a source of specific health problems. Such problems are rare and usually seen in childhood, but occasionally can be seen for the first time in adults.What are the symptoms of urachal abnormalities?
Because this remnant of early development is found between the bellybutton and the top of the bladder, diseases of the urachus can appear anywhere in that space. In newborns and infants, persistent drainage or "wetness" of the bellybutton can be a sign of an urachal problem. However, the most common detectable problem at the bellybutton is a granuloma, a reddened area that is present because the base of the umbilical cord stump did not heal properly.Urachal abnormalities can also be seen without persistent umbilical drainage — 35 percent of urachal problems are manifestations of an enclosed urachal cyst or infected urachal cyst (abscess). This type of problem is seen more often in older children and adults. Instead of visible bellybutton drainage, the symptoms of such a cyst consist of lower abdominal pain, fever, a lump that can be felt, pain with urination, urinary tract infection or hematuria.How are urachal abnormalities treated?

An umbilical granuloma is usually treated by chemical cauterization in the office of the primary care provider. The condition is a superficial abdominal wall problem that heals after treatment and has no long-term implications; it is not caused by an urachal problem.In contrast to the simple granuloma, persistent umbilical wetness needs to be further evaluated. Approximately 65 percent of all urachal problems appear as a sinus or drainage opening at the bellybutton. Most of those are not connected all the way to the bladder, but a small percentage represents an open pathway from the bladder to bellybutton, called a patent urachus. The drainage can be analyzed for urea and creatinine levels, which would be high if the fluid was primarily made of urine from a bladder connection instead of inflammatory tissue fluid. There can be associated redness from the drainage itself. Skin infection – indicated by tenderness, fever or spreading redness of the surrounding skin – can occur and requires prompt antibiotic treatment and possible hospitalization. This is called omphalitis and can be caused by bacteria that have become involved with an urachal sinus or the other embryologicstructure in the bellybutton that was once connected to the intestinal system and might also be persistent. Once inflammation is controlled, the nature and extent of an opening at the bellybutton can be determined by a sinogram. This involves placing a small tube into the sinus opening and allowing contrast material to flow in while taking X-rays to determine the direction and extent of the channel. If the channel follows the expected pathway toward the top of the bladder, the diagnosis is urachal sinus. Treatment should be directed toward complete surgical removal of the urachus and all of its connections, including a small amount of the top of the bladder. Leaving any portion of the structure allows for the possible development of a future malignancy. Less than 1 percent of all bladder malignancies occur in the urachus, but once the urachus has become a potential problem, it should be removed.When there is no draining sinus to investigate, an ultrasound of the lower abdomen will show the typical findings of a fluid-filled, enclosed lump in the location of the urachus. In an adult, where the rare possibility of malignancy could be present, an abdominal and pelvic CT
scanmight be helpful. Again, complete removal of the urachus is important. Simple needle or other drainage of the cyst will result in recurrence in at least one-third of patients, since the linings and structures are still present. About 80 percent of infected cysts are populated bystaphylococcus aureus, and one-third contains multiple types of bacteria. Almost all the time, such an infected cyst stays confined to its predetermined anatomical location; rarely, an infected cyst can drain into the peritoneal cavity and present with additional signs of peritonitisand febrile illness.Therefore, most urachal problems can be characterized by the physical examination and a sinogram or ultrasound. Sometimes a combination of these is needed, and occasionally it is
useful to obtain a voiding cystourethrogram. This is done when the draining urachus is associated with outlet obstruction of the bladder, which would also need to be treated. This possibility is usually determined by the age, gender and physical examination of the patient. There are also situations where a direct look inside the bladder (cystoscopy) can add a bit more information to the diagnostic picture, but most urologists recommend that the basic course of action be determined by the previously described approach.What can be expected after treatment for urachal abnormalities?
After complete surgical removal of a troublesome urachus with no immediate postoperative problems, there should be no further issues and no need for follow-up or evaluation on a regular basis.Frequently asked questions:
Besides the problems that have already been outlined, are there other diseases that appear at the
bellybutton?
As you might expect, there have been rare reports of other inflammatory problems involving the structures that are contained in the umbilical cord. These include infections of the remnant blood vessels. In addition, the vitelline duct, which is supposed to regress in its course between the bellybutton and the small intestine, sometimes has its own remnant problems. Thesinogram that is useful for identifying urachal problems will also serve to identify a likely vitelline duct problem.Occasionally, an intra-abdominal process such as appendicitis or ovarian cyst can mimic some of the symptoms of an urachal problem.Are urachal abnormalities hereditary?
No. There is no evidence that they are inherited.After my baby's umbilical cord stump came off, his bellybutton was extremely red. Is this normal
or does he need immediate evaluation?
Some redness is expected after the stump falls away. Dabbing a small amount of alcohol on the site with a Q-tip twice a day will usually allow complete healing in two to three days. If the redness fails to improve or worsens, contact your primary care provider.
http://www.urologyhealth.org/urology/index.cfm?article=41
BackgroundA stark contrast is observed between the physiologic importance of the umbilicus during development and after birth. During development, the umbilicus functions as a channel that allows blood flow between the placenta and fetus. It also serves an important role in the development of the intestine and the urinary system. After birth, once the umbilical cord falls off, no evidence of these connections should be present. Nevertheless, umbilical disorders are
frequently encountered in pediatric surgery. These disorders range from the very common umbilical hernia to infections such as omphalitis, which can be life threatening. Most patients with umbilical problems present with a mass or drainage from the umbilicus. An understanding of the anatomy and embryology of the abdominal wall and umbilicus is important to identify and properly treat these conditions.
he embryology of the umbilicus and the developmental basis for surgical abnormalities has been well described for more than one hundred years. Umbilical hernias, abdominal wall defects, umbilical polyps and drainage,[1] and omphalomesenteric remnants are well described. Methods of management in some disorders, such as treating umbilical granulomas with silver nitrate, have changed little over the last century. In the early 1900s, umbilical hernia repair was a challenging procedure. Spontaneous closure of these hernias and preservation of the appearance of the natural umbilicus were recognized. Today, umbilical hernia repair is one of the most common procedures performed by pediatric surgeons.
Problem
atients with umbilical disorders present with drainage, a mass, or both. Most umbilical disorders result from failure of normal embryologic or physiologic processes. Unusual umbilical anatomy, such as a single umbilical artery or abnormal position of the umbilicus, may be associated with other congenital anomalies or syndromes. Omphalocele and gastroschisis, which are common abdominal wall defects associated with the umbilicus, are discussed in other Medscape Reference articles (see Pediatric Omphalocele and Gastroschisis). Masses of the umbilicus may be related to lesions of the skin, embryologic remnants, or an umbilical hernia. Masses associated with the skin include dermoid cysts, hemangiomas, and inclusion cysts. Umbilical drainage is associated with granulomas and embryologic remnants. Note the following:
Delayed separation of the umbilical cord: The umbilical cord usually separates from the umbilicus 1-8 weeks postnatally. Topical antimicrobials are usually applied after delivery, followed by isopropyl alcohol until cord separation. Delayed separation may signify an underlying immune disorder.
Umbilical granuloma: Granulation tissue may persist at the base of the umbilicus after cord separation. The tissue is composed of fibroblasts and capillaries and can grow to more than 1 cm. Umbilical granulomas must be differentiated from umbilical polyps, which do not respond to silver nitrate cauterization.
Umbilical infections: Patients with omphalitis may present with purulent umbilical discharge or periumbilical cellulitis. Although infections may be associated with retained umbilical cord or ectopic tissue, in the past, infections were often related to poor hygiene. Current aseptic practices and the routine use of antimicrobials on the umbilical cord have reduced the incidence to less than 1%. Cellulitis may become severe within hours and progress to necrotizing fasciitis and generalized sepsis.
Omphalomesenteric remnants: Persistence of all or portions of the omphalomesenteric duct can result in fistulas, sinus tracts, cysts, congenital bands, and mucosal remnants. Patients with mucosal remnants can present with an umbilical polyp or within an umbilical cyst.
Urachal remnants: The developing bladder remains connected to the allantois through the urachus. Remnants of this connection include a patent urachus, urachal sinus, and urachal cyst. Umbilical polyps can also be observed in association with a urachal remnant.
Umbilical hernia: Umbilical hernias result when persistence of a patent umbilical ring occurs. Umbilical hernias may spontaneously close, but many require surgical repair.[2]

Epidemiology
Frequency
The frequency of the many different umbilical disorders varies. Umbilical infections are now identified in less than 1% of hospitalized newborns.
Umbilical hernias are commonly identified in early infancy; however, most spontaneously close. No sex predilection is noted. The incidence at age 1 year ranges from 2-15%. Incidence is increased in infants who are black and in infants with low birthweight, Down syndrome, trisomy 13, trisomy 18, or Beckwith-Wiedemann syndrome.
Etiology
he development of the anterior abdominal wall depends on differential growth of embryonic tissues, shown below. As the embryo grows, the yolk sac is divided into an intracoelomic portion and an extracoelomic portion. The intracoelomic portion becomes the primitive alimentary canal and communicates with the extracoelomic portion through the vitelline duct, also known as the omphalomesenteric duct. This communication is lost at 5-7 weeks' gestation. Persistence of part or all of this connection results in omphalomesenteric anomalies.
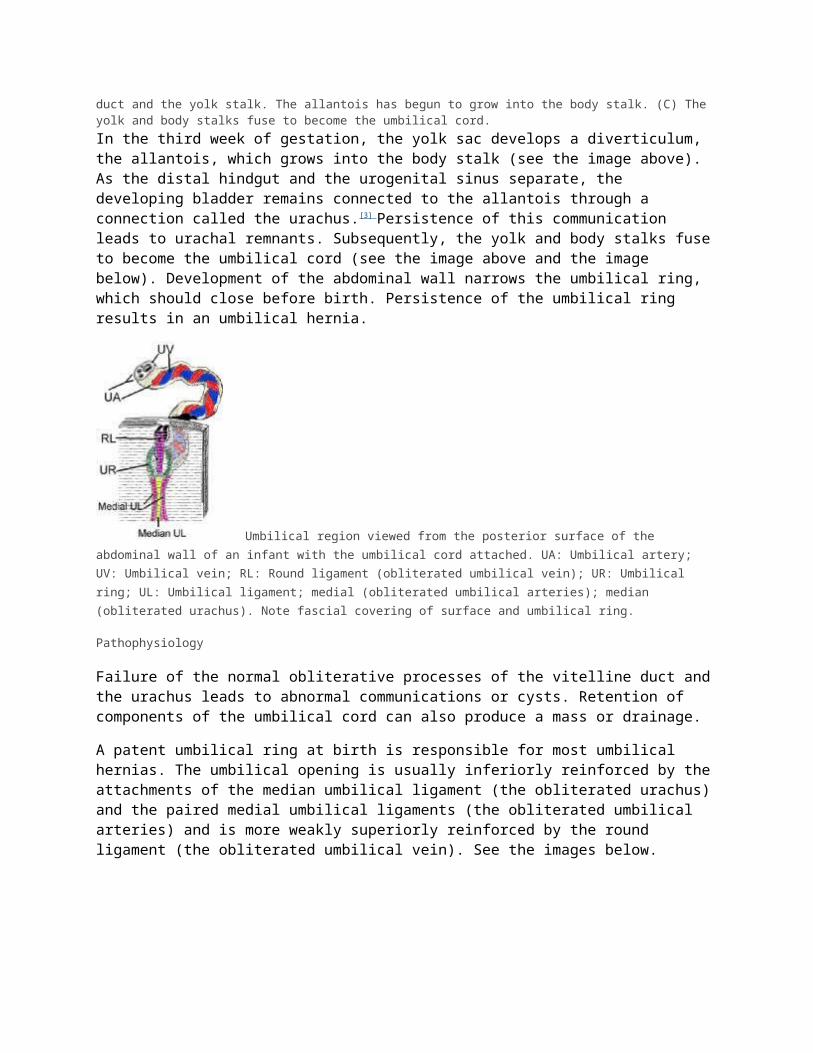
Cartoon illustrating the developing umbilical cord. (A) Embryonic disk: At this stage, the ventral surface of the fetus is in contact with the yolk sac. (B) The yolk sac narrows as the fetus grows and folds. The intracoelomic yolk sac forms the intestine and communicates with the extracoelomic yolk sac through the vitelline duct. The vitelline duct is also referred to as the omphalomesenteric duct and the yolk stalk. The allantois has begun to grow into the body stalk. (C) The yolk and body stalks fuse to become the umbilical cord.In the third week of gestation, the yolk sac develops a diverticulum, the allantois, which grows into the body stalk (see the image above). As the distal hindgut and the urogenital sinus separate, the developing bladder remains connected to the allantois through a connection called the urachus.[3] Persistence of this communication leads to urachal remnants. Subsequently, the yolk and body stalks fuse to become the umbilical cord (see the image above and the image below). Development of the abdominal wall narrows the umbilical ring, which should close before birth. Persistence of the umbilical ring results in an umbilical hernia.
Umbilical region viewed from the posterior surface of the abdominal wall of an infant with the umbilical cord attached. UA: Umbilical artery; UV: Umbilical vein; RL: Round ligament (obliterated umbilical vein); UR: Umbilical ring; UL: Umbilical ligament; medial (obliterated umbilical arteries); median (obliterated urachus). Note fascial covering of surface and umbilical ring.
Pathophysiology
Failure of the normal obliterative processes of the vitelline duct and the urachus leads to abnormal communications or cysts. Retention of components of the umbilical cord can also produce a mass or drainage.
A patent umbilical ring at birth is responsible for most umbilical hernias. The umbilical opening is usually inferiorly reinforced by the attachments of the median umbilical ligament (the obliterated urachus) and the paired medial umbilical ligaments (the obliterated umbilical arteries) and is more weakly superiorly reinforced by the round ligament (the obliterated umbilical vein). See the images below.
Umbilical region viewed from the posterior surface of the abdominal wall of an infant with the umbilical cord attached. UA: Umbilical artery; UV: Umbilical vein; RL: Round ligament (obliterated umbilical vein); UR: Umbilical ring; UL: Umbilical ligament; medial (obliterated umbilical arteries); median (obliterated urachus). Note

fascial covering of surface and umbilical ring. Variations in the umbilical ring structure. (A) Usual configuration of the round ligament and urachus. (B) Less common configuration that can result in weakness at the umbilical ring.Richet fascia, derived from the transversalis fascia, covers the ring, as shown above. The peritoneum covers the innermost portion of the ring. Variability in the attachment of the ligaments and the covering by Richet fascia may predispose some children to developing umbilical hernias, as shown below. However, many children undergo spontaneous closure in the first few years of life. The pressure exerted on the umbilical skin, even when a small umbilical defect is present, can result in marked stretching of the skin and a proboscis appearance, shown below.
Animation demonstrating variability in the covering of the umbilical ring by the umbilical fascia. (A) Complete cover of the umbilical ring (36%). (B) Umbilical fascia is present but does not cover the umbilical ring (4%), or fascia is absent (16%). (C) Umbilical fascia covers the superior portion of the umbilical ring only (38%). (D) Umbilical fascia covers the inferior portion only (6%). Incomplete coverage of the umbilical ring may predispose individuals to formation of
umbilical hernias. Preoperative photograph demonstrating umbilical hernia with redundant skin.Previous
Next Section: PresentationFailure of the normal obliterative processes of the vitelline duct and the urachus leads to abnormal communications or cysts. Retention of components of the umbilical cord can also produce a mass or drainage.
A patent umbilical ring at birth is responsible for most umbilical hernias. The umbilical opening is usually inferiorly reinforced by the attachments of the median umbilical ligament (the obliterated urachus) and the paired medial umbilical ligaments (the obliterated umbilical arteries) and is more weakly superiorly reinforced by the round ligament (the obliterated umbilical vein). See the images below.
Umbilical region viewed from the posterior surface of the abdominal wall of an infant with the umbilical cord attached. UA: Umbilical artery; UV: Umbilical vein; RL: Round ligament (obliterated umbilical vein); UR: Umbilical ring; UL: Umbilical ligament; medial (obliterated umbilical arteries); median (obliterated urachus). Note
fascial covering of surface and umbilical ring. Variations in the umbilical ring structure. (A) Usual configuration of the round ligament and urachus. (B) Less common configuration that can result in weakness at the umbilical ring.Richet fascia, derived from the transversalis fascia, covers the ring, as shown above. The peritoneum covers the innermost portion of the ring. Variability in the attachment of the ligaments and the covering by Richet fascia may predispose some children to developing umbilical hernias, as shown below. However, many children undergo spontaneous closure in the first few years of life. The pressure exerted on the umbilical skin, even when a small umbilical defect is present, can result in marked stretching of the skin and a proboscis appearance, shown below.
Animation demonstrating variability in the covering of the umbilical ring by the umbilical fascia. (A) Complete cover of the umbilical ring (36%). (B) Umbilical fascia is present but does not cover the umbilical ring (4%), or fascia is absent (16%). (C) Umbilical fascia covers the superior portion of the umbilical ring only (38%). (D) Umbilical fascia covers the inferior portion only (6%). Incomplete coverage of the umbilical ring may predispose individuals to formation of
umbilical hernias. Preoperative photograph demonstrating umbilical hernia with redundant skin.Previous
Next Section: PresentationPresentation

Umbilical infections can occur because of an embryologic remnant or poor hygiene. Traditionally, gram-positive organisms, such as Staphylococcus aureusand Streptococcus pyogens, were most commonly identified. Gram-negative and polymicrobial infections are seen today, especially in rapidly progressing cellulitis and necrotizing fasciitis.
Umbilical granulomas appear as 1-mm to 1-cm, pink, friable lesions at the base of the umbilicus. They produce variable amounts of drainage that can irritate the surrounding skin. An umbilical polyp is brighter red than a granuloma and represents retained intestinal or gastric mucosa from the vitelline duct.
The presentation of omphalomesenteric remnants depends on the specific type of defect, as shown below. If a communication persists from the terminal ileum to the umbilicus, intestinal contents or stool can be observed leaking from the umbilicus. Prolapse of intestine through an omphalomesenteric fistula can also be observed (see the image below). The drainage from a fistula that does not communicate with the ileum varies; it may be clear, bloody, or purulent. Cystic remnants may become infected and manifest with pain and swelling.
Omphalomesenteric duct remnants. (A) Meckel diverticulum. Note feeding vessel. (B) Meckel diverticulum attached to posterior surface of anterior abdominal wall by a fibrous cord. (C) Fibrous cord attaching ileum to abdominal wall. (D) Intestinal-umbilical fistula. Intestinal mucosa extends to skin surface. (E) Omphalomesenteric cyst arising in a fibrous cord. The cyst may contain intestinal or gastric mucosa. (F) Umbilical sinus ending in a fibrous cord attaching to the ileum. (G, H) Omphalomesenteric cyst and sinus without intestinal
attachments. Photograph of newborn with intestinal prolapse through a patent omphalomesenteric duct. Both the proximal and distal limbs of the intestine have prolapsed. The umbilicus was explored, the bowel was easily reduced, and the patent duct was excised. The child was discharged from the hospital 2 days later.The presentation of urachal remnants also varies. Clear drainage from the umbilicus is characteristic of a urachal fistula. Drainage of urine from the umbilicus may suggest bladder outlet obstruction and warrants further investigation. A urachal cyst is usually discovered as a painful mass between the umbilicus and suprapubic area when it becomes infected. Pain and retraction of the umbilicus during urination may suggest a urachal anomaly. A urachal sinus manifests with drainage that can be clear or purulent and occurs through the umbilicus or midline skin below the umbilicus. See the image below.

Urachal sinus with purulent drainage in midline below the umbilicus (black arrow). A laparoscope was placed in the supraumbilical crease (red arrow) for mobilization of the internal portion of the urachal remnant as depicted in the next image.Patients with umbilical hernias present early in life with bulging at the umbilicus. The swelling is most prominent when the infant or child is crying or straining. Umbilical hernias are usually asymptomatic and rarely cause pain. The skin can become severely stretched, which may be alarming to parents and physicians. Parents often mention that the child plays with the redundant skin. Incarceration, strangulation, bowel obstruction, erosion of the overlying skin, and bowel perforation are rare events in infants and small children. The risk of incarceration increases significantly in adults with umbilical hernias.
Patients with umbilical infections can present with drainage from the umbilicus, swelling, and redness. Cellulitis may rapidly progress and lead to necrotizing fasciitis. Necrotizing fasciitis is characterized by abdominal distention, tachycardia, purpura, leukocytosis, and other signs of sepsis despite antibiotic therapy.
Indication
Small umbilical granulomas usually respond to silver nitrate application. Large umbilical granulomas or those that persist after silver nitrate treatment require surgical excision.
Omphalomesenteric remnants and urachal remnants require surgical excision. The precise diagnosis is often not confirmed until surgery is performed and the anatomy of the umbilicus is established.
The diameter of the umbilical ring defect is predictive of spontaneous closure. The length of the protruding skin is not prognostically significant. Umbilical hernias with ring diameters less than 1 cm are more likely to spontaneously close than those with ring diameters more than 1.5 cm. Surgery is indicated for all symptomatic umbilical hernias. Incarceration, strangulation, skin erosion, and bowel perforation are indications for immediate surgery. Similarly, patients presenting with pain should be repaired on an elective basis.
Asymptomatic umbilical hernias can be safely monitored until the child is aged 4-5 years to allow spontaneous closure, especially if the ring defect is small. Because umbilical hernias with larger defects (ie, >1.5 cm) are unlikely to spontaneously close, surgery can be performed at an earlier age. Similarly, closing umbilical hernias with large ring defects is reasonable in younger children if the child is having a general anesthetic for another procedure, such as an inguinal hernia repair. Considering surgery in younger children who have a large protrusion of the umbilical skin that is causing distress to the parents is also reasonable.
Necrotizing fasciitis and gangrene of the umbilical skin requires emergency surgical debridement and can be life saving.

Relevant anatomy
During development, the embryonic disk is in contact with the yolk sac anteriorly, shown in A below. As the embryo grows and differential growth of tissues leads to the folding appearance of the embryo, the ventral attachment of the yolk sac narrows.
The intracoelomic portion of the yolk sac becomes the primitive alimentary canal and attaches to the extracoelomic portion through the vitelline duct. The allantois buds from the hindgut and grows into the body stalk, shown in B below. The yolk stalk and the body stalk eventually fuse to become the umbilical cord, shown in C below.
Cartoon illustrating the developing umbilical cord. (A) Embryonic disk: At this stage, the ventral surface of the fetus is in contact with the yolk sac. (B) The yolk sac narrows as the fetus grows and folds. The intracoelomic yolk sac forms the intestine and communicates with the extracoelomic yolk sac through the vitelline duct. The vitelline duct is also referred to as the omphalomesenteric duct and the yolk stalk. The allantois has begun to grow into the body stalk. (C) The yolk and body stalks fuse to become the umbilical cord.As the abdominal wall forms, the umbilical ring is narrowed. The vitelline and umbilical vessels, vitelline duct, and allantois should be absent in the umbilicus at term, shown below. Residual tissue leads to remnants that require surgical intervention, as shown below.
During exploration for a sinus or fistula, all structures, including the round ligament, median, and medial umbilical ligaments, must be identified (see the images below). An omphalomesenteric or urachal sinus or fistula must be dissected back to its origin in the ileum or bladder, respectively.
Umbilical region viewed from the posterior surface of the abdominal wall of an infant with the umbilical cord attached. UA: Umbilical artery; UV: Umbilical vein; RL: Round ligament (obliterated umbilical vein); UR: Umbilical ring; UL: Umbilical ligament; medial (obliterated umbilical arteries); median (obliterated urachus). Note

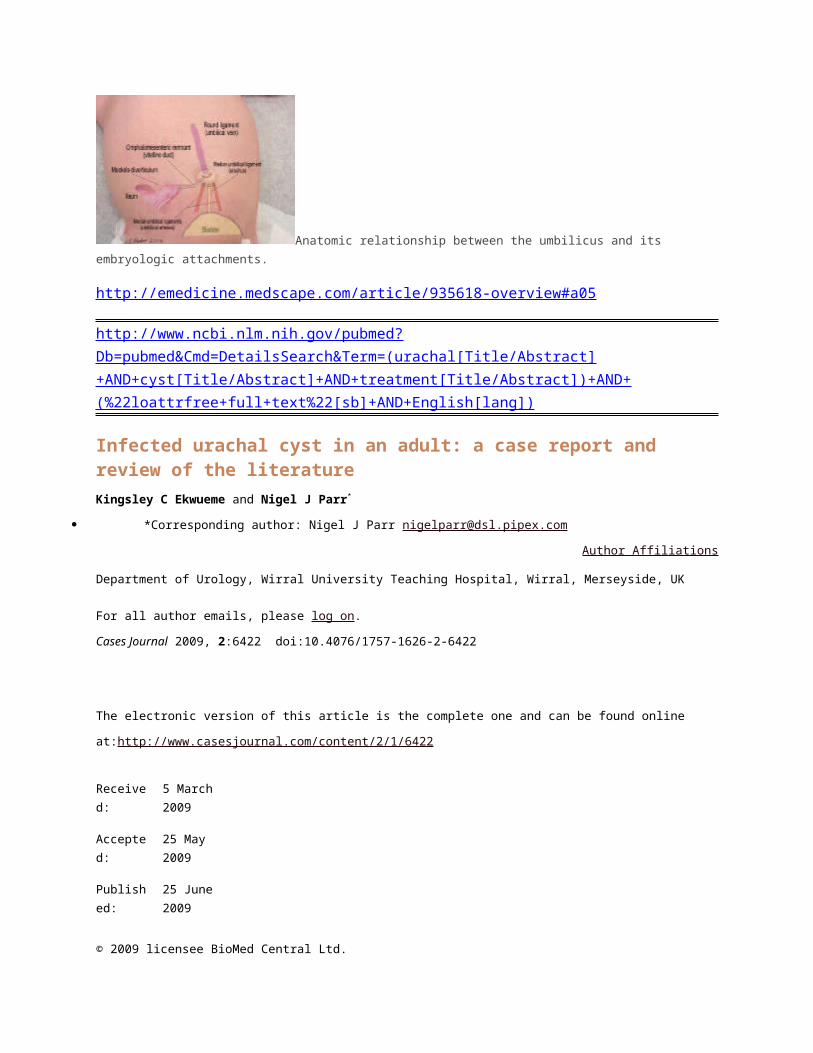
fascial covering of surface and umbilical ring. Anatomic relationship between the umbilicus and its embryologic attachments.
http://emedicine.medscape.com/article/935618-overview#a05
http://www.ncbi.nlm.nih.gov/pubmed?Db=pubmed&Cmd=DetailsSearch&Term=(urachal[Title/Abstract]+AND+cyst[Title/Abstract]+AND+treatment[Title/Abstract])+AND+(%22loattrfree+full+text%22[sb]+AND+English[lang])
Infected urachal cyst in an adult: a case report and review of the literatureKingsley C Ekwueme and Nigel J Parr*
*Corresponding author: Nigel J Parr [email protected]
Author Affiliations
Department of Urology, Wirral University Teaching Hospital, Wirral, Merseyside, UK
For all author emails, please log on.
Cases Journal 2009, 2:6422 doi:10.4076/1757-1626-2-6422
The electronic version of this article is the complete one and can be found online
at:http://www.casesjournal.com/content/2/1/6422
Received:
5 March 2009
Accepted:
25 May 2009
Published:
25 June 2009
© 2009 licensee BioMed Central Ltd.

This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Abstract
IntroductionUrachal cyst is one of a spectrum of urachal abnormalities most commonly found in children. They are very rarely seen in adults because the urachus is normally obliterated in early infancy.
Case presentationWe describe a case of a 32 year old male Caucasian who presented with a tender, midline, infraumbilical mass and purulent umbilical discharge. Diagnosis of an infected urachal cyst was confirmed on magnetic resonance scan. He was treated initially with broad spectrum antibiotics in order to allow sepsis to resolve prior to surgical excision of the cyst and fibrous tract. Cystoscopy was performed intraoperatively to exclude sinus communication with the bladder. Histology of the excised specimen showed chronic inflammation with no evidence of malignancy. Postoperative recovery was uneventful.
ConclusionUrachal abnormalities are rare in adults. Clinical presentation is non-specific; therefore, a high index of suspicion is required in order to make the diagnosis. When diagnosed, surgical excision is advised because of the risk of malignant transformation.
Introduction
Urachal abnormalities result from incomplete regression of the foetal urachus. They are more common in children than in adults, due to urachal obliteration in early infancy [1].In adults, urachal cyst (UC) is the commonest variety, with infection being the usual mode of presentation [2]. Diagnosis remains challenging due to the rarity of this lesion and the non-specific nature of its symptomatology. Since the first description of urachal abnormality by Cabriolus in 1550, few cases have been reported in literature.We describe a case of urachal cyst presenting with a tender infraumbilical mass, purulent umbilical discharge and sepsis, in a previously fit and well man.
Case presentation
A 32 year old male Caucasian was referred after presenting to the accident an emergency department with a 10 day history of persistent purulent umbilical discharge associated with constant lower abdominal pain, chills and rigors. He gave no history of nausea, vomiting or change in bowel habit. Systemic review revealed no abnormality. He had completed a course of antibiotics prescribed by his General Practitioner with little relief.
On examination, he was apyrexial and haemodynamically stable. Abdominal examination, however, revealed purulent umbilical discharge with surrounding erythema and a tender infraumbilical mass. A working differential diagnosis of omphalitis or pilonidal disease of the umbilicus, or patent urachus was made.
Haematology showed a raised C-reactive protein of 112 mg/l, but normal white cell count. Microbiology culture of the pus grew Bacteroides sp.Abdominal ultrasound scan showed a 3.8 cm echogenic collection in a cavity within the anterior abdominal wall in the midline. An MRI scan, confirmed the diagnosis of UC communicating proximally with the umbilicus (Figure 1). The initial MRI scan was carried out on an empty bladder making it difficult to exclude possible distal communication between the UC and the bladder. A repeat MRI scan was subsequently performed with a full bladder, to exclude any distal communication.The patient was initially treated with intravenous antibiotics followed by a 2 week course of oral antibiotics with surgery planned at the end of this period. Cystoscopy and excision of the infected urachal cyst were performed simultaneously. Cystoscopy confirmed no evidence of a sinus into the bladder. A midline incision was used to excise the cyst, together with the omentum adherent to it posteriorly. The sac of the cyst contained white cheesy material (Figure 2). Histopathological analysis of the resected specimen showed chronic inflammation with no evidence of malignancy. Recovery was unremarkable.
Figure 1. MRI scan showing high signal fluid within the umbilicus tracking
into urachal remnant.
Figure 2. The urachal cyst and fibrous tract containing white cheesy material
within its cavity.
Discussion
The urachus, developmentally is the upper part of the bladder, both of which arise from the ventral part of the cloaca [3]. Descent of the bladder from the 5th month of development into the foetal pelvis pulls the urachus with it resulting in the formation of the urachal canal. The lumen of this canal progressively obliterates during foetal life, with eventual formation of a fibrous tract in early adult life.At the end of development, the urachus lies between the transversalis fascia anteriorly and the peritoneum posteriorly (space of Retzius), surrounded by loose areolar tissue and attaches the umbilicus to the dome of the bladder. Histologically, it is composed of 3 layers; an innermost layer of modified transitional epithelium similar to the urothelium, the middle layer of fibroconnective tissue and outermost layer of smooth muscle continuous with the detrusor [1,3].There are five types of urachal abnormalities: 1) patent urachus, in which the entire tubular structure fails to close; 2) urachal cyst, in which both ends of the canal close leaving an open central portion; 3)

urachal sinus, which drains proximally into the umbilicus; 4) vesicourachal diverticulum, where the distal communication to the bladder persists; and 5) alternating sinus, which can drain to either bladder or umbilicus.
The incidence of UC in adults is unknown but it is rare. It is more common in men than women[2,4]. In a 31-year review, Risher et al [2] found 12 adults with urachal anomalies, of which 5 were UC. Modes of presentation of urachal anomalies in adults differ from those seen in children. In adults, the commonest variety is urachal cyst, with infection being usual mode of presentation[2,5]. The route of infection is haematogenous, lymphatic, direct or ascending from the bladder. The commonly cultured microorganisms from the cystic fluid include Escherichia coli, Enterococcus faecium, Klebsiella pneumonia, Proteus, Streptococcus viridans and Fusobacterium[4,5]. In our case, Bacteroides sp was cultured.The clinical signs and symptoms are non-specific, as UC are largely asymptomatic until they become infected. However, the presence of the triad of symptoms including a tender midline infraumbilical mass, umbilical discharge and sepsis should arouse suspicion of UC. If left untreated, UC slowly enlarges and may drain through the umbilicus as was seen in our patient, or drain into the bladder or both, resulting in alternating sinus.
Ultrasound scan can help to make diagnosis in 77% of patients [5]. In our case, ultrasound scan was not specific and MRI scan was used to make diagnosis and define the relationship to surrounding structures.UC can be complicated by rupture into the peritoneal cavity leading to peritonitis. Other reported complications include uracho-colonic fistula, stone formation and neoplastic transformation [6]-[9]. The risk of urachal malignancy in adults is high and the prognosis is poor. Ashley et al [4] in a 54 year retrospective study of 130 adults with urachal abnormalities found that 51% were malignant and 20% presented with metastatic disease. The median age at presentation was 61 years and the 2 common risk factors for malignancy were age and haematuria.Although histologically, the innermost layer of the urachus is mainly transitional cell, adenocarcinoma is the predominant histological type and most are mucinous. This is probably due to metaplasia arising from chronic inflammation.
The treatment of choice for urachal cyst is by complete primary excision. An earlier report suggests a single stage procedure backed with appropriate antibiotic therapy for the treatment of infected UC [10]. However, Yoo et al [5] in their study suggested a 2 stage procedure involving initial incision and drainage, followed by later excision of the urachal remnant. In our case, we adopted a staggered plan of management. Firstly, with administration of broad spectrum antibiotics guided by microbiology sensitivity, and after resolution of sepsis interval primary excision of the cyst, including insertion of a covering corrugated wound drain.
Conclusion
Urachal anomalies are rare in adults. Presentation is atypical; therefore, a high index of suspicion is required in order to achieve a diagnosis. A triad of lower midline mass, umbilical discharge and sepsis is suggestive, although MRI confirms the diagnosis and defines the surrounding anatomical relationship. Complete surgical excision is the treatment of choice due to the risk of malignant
transformation. We recommend a 2 stage treatment with a combination of broad spectrum antibiotics or incision and drainage, followed by interval excision after resolution of sepsis.
Abbreviation
UC: Urachal cyst.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests
Authors' contributions
KCE summarised the case and wrote this article whilst NJP is the primary surgeon and provided the overall supervision in the writing of this article. All authors read and approved this article.
References
http://www.casesjournal.com/content/2/1/6422
Urachal anomalies in children: a single center experience.Choi YJ, Kim JM, Ahn SY, Oh JT, Han SW, Lee JS.
Source
Department of Pediatrics, Yonsei University College of Medicine, Seoul, Korea.
AbstractThe objective of this study is to define optimal diagnosis and treatment strategies for patients with urachal anomalies in the pediatric age group. The medical records of 21 children who had undergone surgery for urachal anomalies at Severance Hospital, Yonsei University College of Medicine from January 1990 to April 2005 were reviewed. The subjects included 14 males and 7 females (M:F 2:1). The four types of urachal anomalies confirmed were a urachal cyst in 10 patients (47.6%), a patent urachus in 6 (28.6%), a urachal sinus in 4 (19.0%) and a urachal diverticulum in 1 (4.8%) patient. The most common presenting complaint was umbilical discharge (n = 10, 40.0%), followed by abdominal mass (n = 9, 36.0%). Urachal anomalies were diagnosed by ultrasonography in 18 patients, and 7 of them were additionally examined by computed tomography. The remaining patients were diagnosed solely by surgical exploration. Excision was performed in all patients and was supplemented by

partial cystectomy in three. Umbilical discharge was the most common clinical manifestation in our patients, suggesting that ultrasonography should be performed in patients with umbilical discharge to differentiate urachal anomalies. We found the most common anomaly to be the urachal cyst, and all patients were successfully treated by surgical excision.
http://www.ncbi.nlm.nih.gov/pubmed/17191305
Urachal AbnormalitiesContact Information
Learn more
What is the urachus?
The urachus is a remnant of a channel between the bladder and the umbilicus (belly button)
where urine initially drains in the fetus during the 1st trimester of pregnancy. The channel of
the urachus usually seals off and obliterates around the 12 thweek of gestation and all that is
left is a small fibrous cord between the bladder and umbilicus called the median umbilical
ligament.
What are the disorders of the urachus and the symptoms?
Disorders of the urachus occur when there are abnormalities with the sealing off of the
channel during fetal development. There are at least 4 types of urachal abnormalities seen
(Figure 1).

Figure 1: Types of urachal anomalies
This occurs when a section of the urachus did not seal off, but there is not a connection
between the bladder and umbilicus. Often, this is asymptomatic and is only detected when
an ultrasound is performed for other reasons. Occasionally urachal cysts can become
infected and could cause abdominal pain or could start to leak cloudy or bloody fluid at the
umbilicus. The average age for urachal cysts to present with an infection is 2-4 years old.
Patent urachus
This occurs when the urachus did not seal off and there is a connection between the
bladder and the umbilicus. A patent urachus can cause varying amounts of clear urine to
leak at the umbilicus.
Urachal sinus
This occurs when the urachus did not seal close to the umbilicus and leads to a blind
ending tract from the umbilicus into the urachus called a sinus. These can be asymptomatic
or present with infection with abdominal pain and drainage of fluid.
Diverticulum
This occurs when the urachus did not seal close to the bladder and leads to a blind ending
tract from the bladder into the urachus called a diverticulum. These also can be
asymptomatic or present with a urinary tract infection.
How are the urachal disorders diagnosed?

Urachal disorders are usually diagnosed when there are symptoms such as: drainage from
the umbilicus, redness around umbilicus, abdominal pain, or urinary tract infection. An
ultrasound can often detect urachal anomalies but occasionally other tests are needed. A
sinogram or sinography is a test where contrast is injected into the umbilicus to see if there
is a patent urachus or urachal sinus. Another test called a VCUG (see voiding
cystourethrogram) is also occasionally performed if there is a urinary tract infection or to
ensure that the bladder drains properly. Rarely tests such as a CT scan or MRI are needed
for diagnosis.
How are the urachal disorders treated?
If the urachal disorder presents with an infection, the infection is treated first. This requires
antibiotics, possible admission for intravenous antibiotics, and occasional surgical drainage
of any infected cyst or poorly draining cavity. Once the infection is under control, excision of
the urachus is usually performed. This can usually be done laparoscopically or with a small
incision on the lower abdomen. Patients usually stay in the hospital 1-2 days after the
surgery. The urachus can be excised because in normal development it usually obliterates
anyway. The umbilicus is not removed.
Why are the urachal disorders treated?
The main reasons for why urachal abnormalities are treated are for symptoms such as
drainage, irritation, or infection.
What happens after treatment?
After control of any infection and surgical removal of the urachal abnormality, your child can
be expected to not have any more problems with the urachus. There is a small risk of
localized infection (< 10%) after removal of the urachus, but this can usually be treated with
just antibiotics.
Link to Urology Care Foundation website for more information:
http://www.urologyhealth.org/urology/index.cfm?article=41
Patient Information

urachal_abnormalities.pdf
renal_bladder_ultrasound.pdf
voiding_cystourethrogram_new.pdf
voiding_cystourethrogram_vcug_original.pdf
vcug_espanol.pdf
http://urology.ucsf.edu/patient-care/children/urachal-abnormalities