value based care: a system overhaul - anzca.edu.au · value based care: a system overhaul lee a....
TRANSCRIPT

Value based care: A system overhaul
Lee A. Fleisher, M.D.
Robert D. Dripps Professor and Chair of Anesthesiology
Perelman School of Medicine at the University of Pennsylvania
Email: [email protected]


Unexplained Variation
Dartmouth Atlas of Healthcare


Value
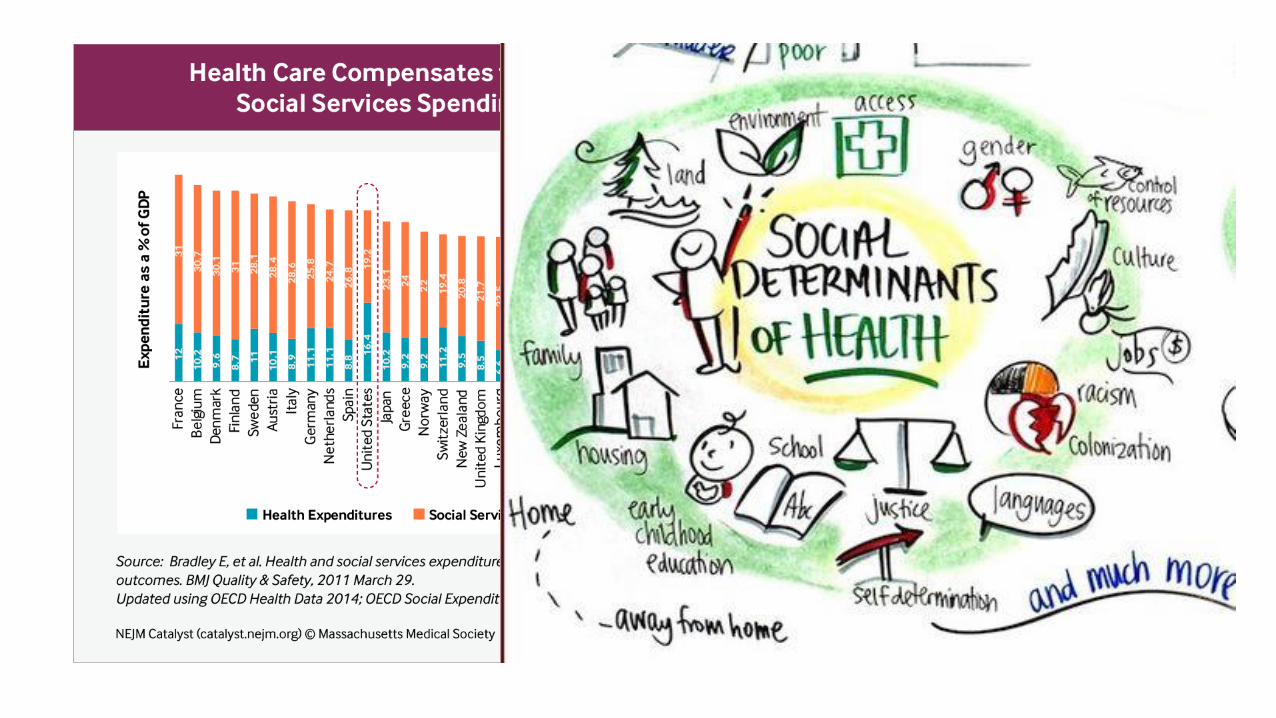
• The core issue in health care is the value of health care delivered
• Value is the only goal that can unite the interests of all system participants
Value = Patient health outcomes per dollar spent
Michael Porter NEJM 2010
7
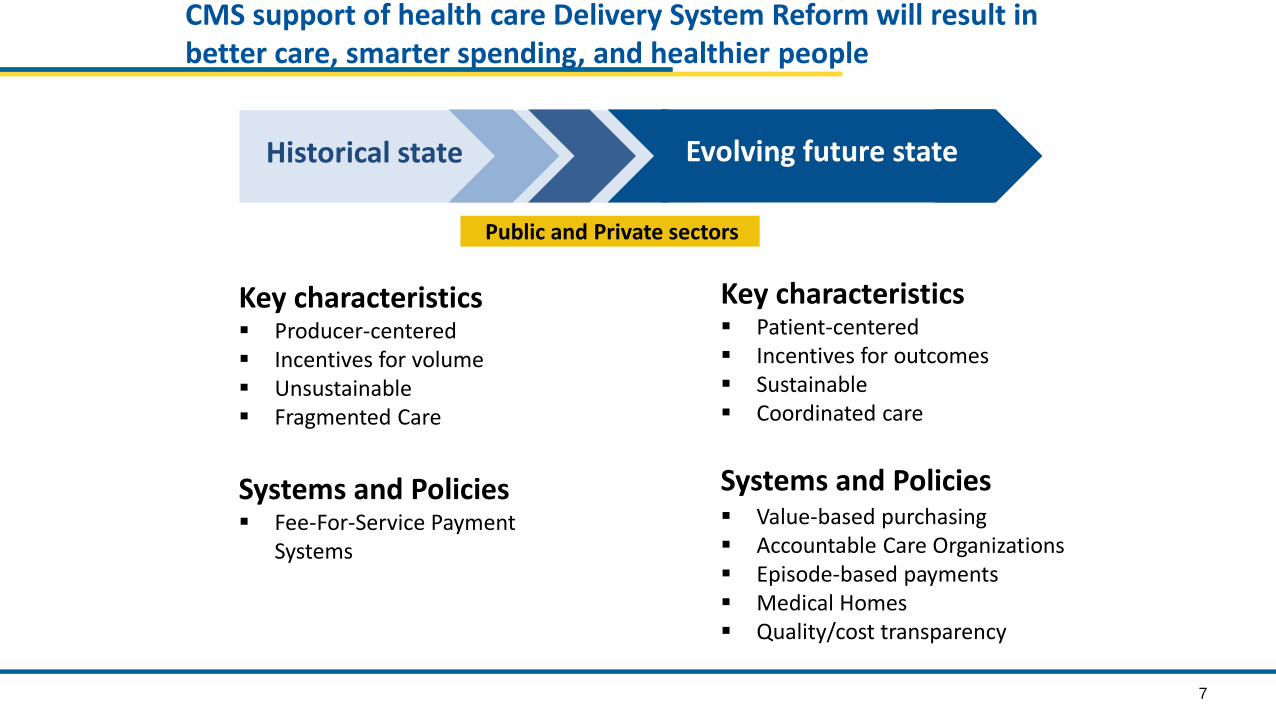
CMS support of health care Delivery System Reform will result in better care, smarter spending, and healthier people
Key characteristics▪ Producer-centered▪ Incentives for volume▪ Unsustainable▪ Fragmented Care
Systems and Policies▪ Fee-For-Service Payment
Systems
Key characteristics▪ Patient-centered▪ Incentives for outcomes▪ Sustainable▪ Coordinated care
Systems and Policies▪ Value-based purchasing▪ Accountable Care Organizations▪ Episode-based payments▪ Medical Homes▪ Quality/cost transparency
Public and Private sectors
Evolving future stateHistorical state

CMS framework for measurement maps to the six national priorities
Greatest commonality of measure concepts across domains
– Measures should be patient-centered and outcome-oriented whenever possible
– Measure concepts in each of the six domains that are common across providers and settings can form a core set of measures
Person- and Caregiver-centered experience and
engagment
•CAHPS or equivalent measures for each settings•Shared decision-making
Efficiency and cost reduction
•Spend per beneficiary measures•Episode cost measures•Quality to cost measures
Care coordination
•Transition of care measures•Admission and readmission measures•Other measures of care coordination
Clinical quality of care
•HHS primary care and CV quality measures•Prevention measures•Setting-specific measures•Specialty-specific measures
Population/ community health
•Measures that assess health of the community•Measures that reduce health disparities•Access to care and equitability measures
Safety
•Healthcare Acquired Infections•Healthcare acquired conditions• Harm

CMS has adopted a framework that categorizes payments to providers
Description
Medicare Fee-for-Service examples
▪ Payments are based on volume of services and not linked to quality or efficiency
Category 1:
Fee for Service –No Link to Value
Category 2:
Fee for Service –Link to Quality
Category 3:
Alternative Payment Models Built on Fee-for-Service Architecture
Category 4:
Population-Based Payment
▪ At least a portion of payments vary based on the quality or efficiency of health care delivery
▪ Some payment is linked to the effective management of a population or an episode of care
▪ Payments still triggered by delivery of services, but opportunities for shared savings or 2-sided risk
▪ Payment is not directly triggered by service delivery so volume is not linked to payment
▪ Clinicians and organizations are paid and responsible for the care of a beneficiary for a long period (e.g., ≥1 year)
▪ Limited in Medicare fee-for-service
▪Majority of Medicare payments now are linked to quality
▪ Hospital value-based purchasing
▪ Physician Value Modifier
▪ Readmissions / Hospital Acquired Condition Reduction Program
▪ Accountable Care Organizations▪Medical homes▪ Bundled payments ▪ Comprehensive Primary Care
initiative▪ Comprehensive ESRD▪Medicare-Medicaid Financial
Alignment Initiative Fee-For-Service Model
▪ Eligible Pioneer Accountable Care Organizations in years 3-5
▪Maryland hospitals
Source: Rajkumar R, Conway PH, Tavenner M. CMS ─ engaging multiple payers in payment reform. JAMA 2014; 311: 1967-8.

The CMS Innovation Center
The purpose of the [Center] is to test innovative
payment and service delivery models to reduce
program expenditures…while preserving or
enhancing the quality of care furnished to
individuals under such titles.
- The Affordable Care Act
Identify, Test, Evaluate, Scale

CMS Innovations Portfolio: Testing New Models to Improve Quality
Accountable Care Organizations (ACOs)
• Medicare Shared Savings Program (Center for
Medicare)
• Pioneer ACO Model
• Advance Payment ACO Model
• Comprehensive ERSD Care Initiative
Primary Care Transformation
• Comprehensive Primary Care Initiative (CPC)
• Multi-Payer Advanced Primary Care Practice (MAPCP)
Demonstration
• Federally Qualified Health Center (FQHC) Advanced
Primary Care Practice Demonstration
• Independence at Home Demonstration
• Graduate Nurse Education Demonstration
Bundled Payment for Care Improvement
• Model 1: Retrospective Acute Care
• Model 2: Retrospective Acute Care Episode &
Post Acute
• Model 3: Retrospective Post Acute Care
• Model 4: Prospective Acute Care
Capacity to Spread Innovation
• Partnership for Patients
• Community-Based Care Transitions
• Million Hearts
Health Care Innovation Awards
State Innovation Models Initiative
Initiatives Focused on the Medicaid Population
• Medicaid Emergency Psychiatric Demonstration
• Medicaid Incentives for Prevention of Chronic
Diseases
• Strong Start Initiative
Medicare-Medicaid Enrollees
• Financial Alignment Initiative
• Initiative to Reduce Avoidable Hospitalizations of
Nursing Facility Residents

2016
30%
85%
2018
50%
90%
Target percentage of payments in ‘FFS linked to quality’ and ‘alternative payment models’ by 2016 and 2018
2014
~20%
>80%
2011
0%
~70%
GoalsHistorical Performance
All Medicare FFS (Categories 1-4)
FFS linked to quality (Categories 2-4)
Alternative payment models (Categories 3-4)

Partnership for Patients contributes to quality improvements
Data shows from 2010 to 2014…
Ventilator-
Associated
Pneumonia
Early
Elective
Delivery
Central Line-
Associated
Blood Stream
Infections
Venous
thromboembolic
complications
Re-
admissions
Leading Indicators, change from 2010 to 2013
62.4% ↓ 70.4% ↓ 12.3% ↓ 14.2% ↓ 7.3% ↓
87,000
2.1 million
PATIENT HARM
EVENTS AVOIDED
$20 billion
IN SAVINGS

Payment reform
• Traditional fee-for-service
– Reduced reimbursement
• Bundled payments
• Accountable Care Organizations

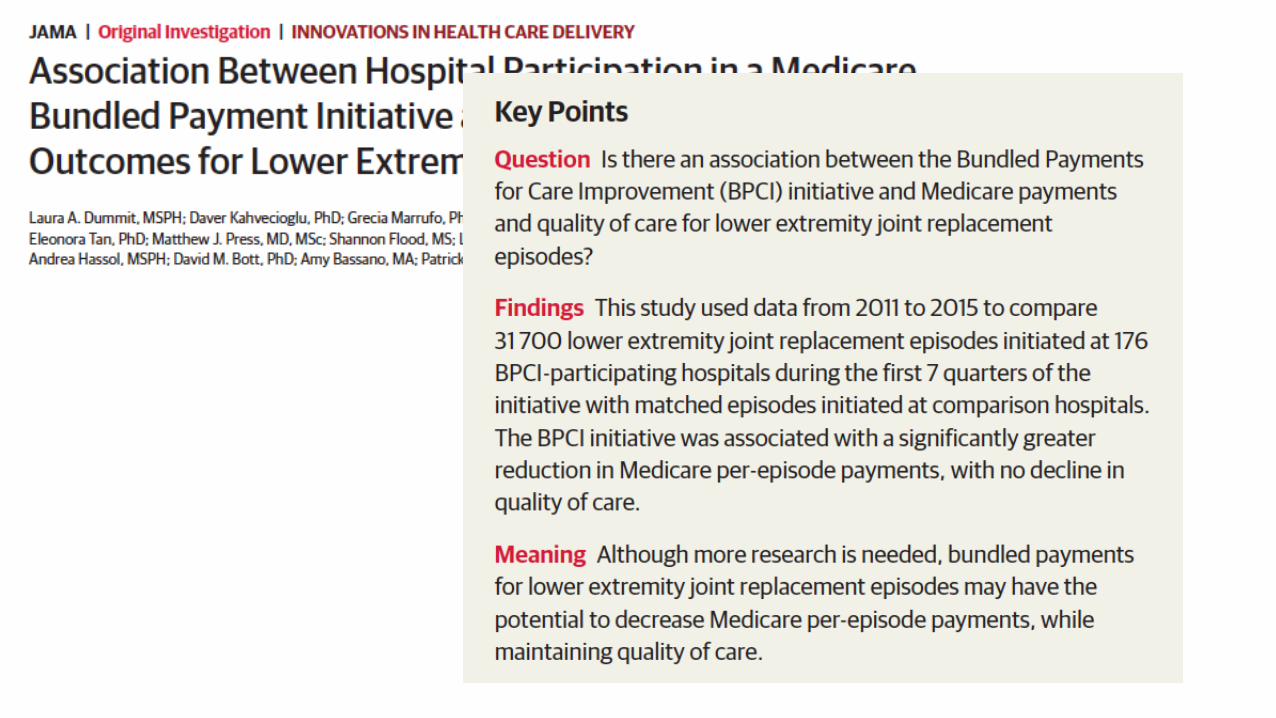
The bundled payment model targets 48 conditions with a single payment for an episode of care
➢ Incentivizes providers to take accountability for both cost and quality of care
➢ Four Models - Model 1: Retrospective acute care hospital stay only
- Model 2: Retrospective acute care hospital stay plus post-acute care
- Model 3: Retrospective post-acute care only
- Model 4: Prospective acute care hospital stay only
▪ 337 Awardees and over 1500 Episode Initiators as of January 2016
Bundled Payments for Care Improvement is also growing rapidly
▪ Duration of model is scheduled for 5 years:▪ Model 1: Awardees began Period of Performance in
April 2013▪ Models 2, 3, 4: Awardees began Period of
Performance in October 2013

Healthcare Consumerism



Is Policy Reform Good for Anesthesiologists/Perioperative Physicians
Bundled care-
How do we divvy up the pie?
Traditional FFS
Fixed payment
Lower fixed payment and share in any profit margin
Should the anesthesiologist be allowed to share in potential reward?
Does the anesthesiologist want to assume any risk?

What is shared accountability?

So how do we fix it from a policy perspective?

NOTES: Current status for each state is based on KCMU tracking and analysis of state executive activity. *AR, AZ, IA, IN, MI, MT, and NH have approved Section 1115 waivers. WI covers adults up to 100% FPL in Medicaid, but did not adopt the ACA expansion. SOURCE: “Status of State Action on the Medicaid Expansion Decision,” KFF State Health Facts, updated January 1, 2017.http://kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/
Current Status of State Medicaid Expansion Decisions
WY
WI*
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI
PA
OR
OK
OH
ND
NC
NY
NM
NJ
NH*
NVNE
MT*
MO
MS
MN
MI*
MA
MD
ME
LA
KYKS
IA*
IN*IL
ID
HI
GA
FL
DC
DE
CT
COCA
AR*AZ*
AK
AL
Adopted (32 States including DC)
Not Adopting At This Time (19 States)



Summary
• The US healthcare system is transitioning from volume to value, but lives in both worlds
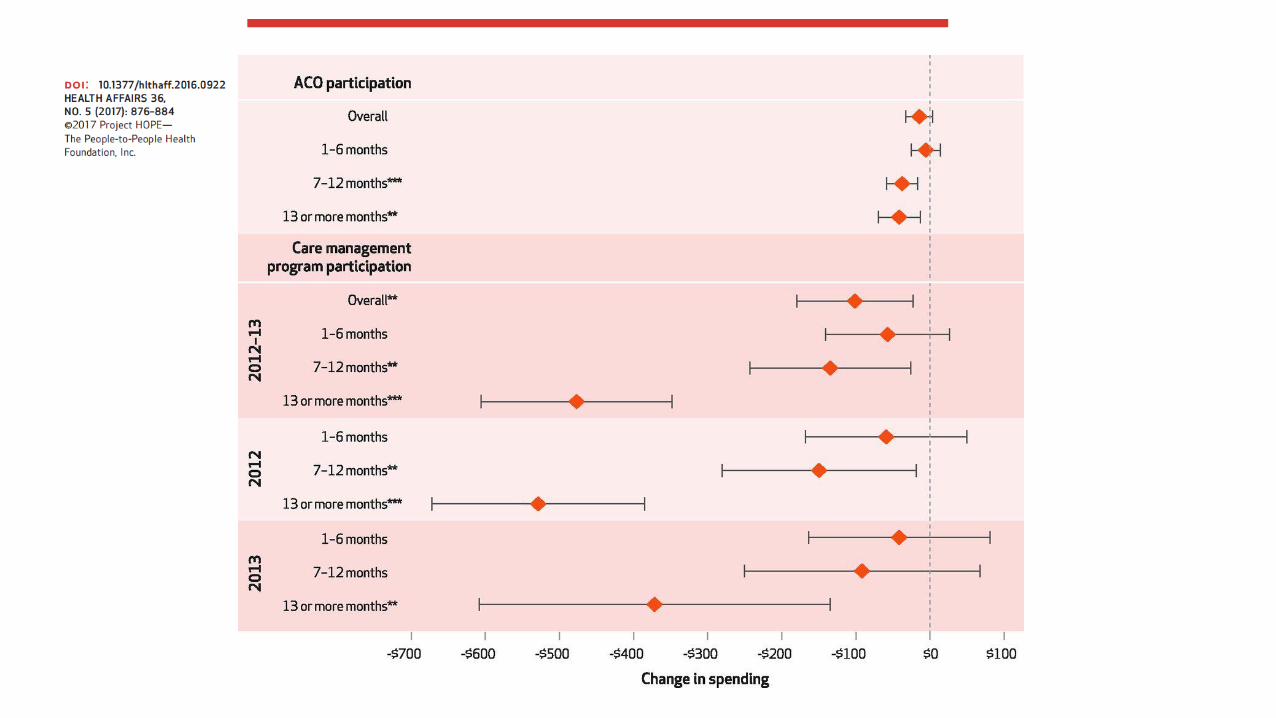
• Bundled payment is one of the few measures that improves quality and reduces cost
• Perioperative physicians must be engaged in the care.