vol. 13 no. 3 july - sept 2019 issn: 0972-1096
TRANSCRIPT

Vol. 13 No. 3 JULY - SEPT 2019 ISSN: 0972-1096


JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
1© JIMI • JULY - SEPT 2019 • VOL. 13
ContentsORIGINAL ARTICLE
1. A Hospital based Observational Study to establish the cause of Ascites using Serum Ascites Cholesterol Gradient in North Indian patientsShri Krishna Gautam, Brijesh Kumar, Surya Prakash Jha, Richa Giri, J.S.Kushwaha, Anita, Santosh Burman
10- 14
2. Study of Pregnancy Induced Hypertension and Associated Factors among women attending delivery service at Tertiary Care Centre in Gujarat, IndiaVaishali N. Vegada, Hiren N. Makwana
15 - 23
3. Role of Human Papilloma Virus in Head and Neck CarcinomaAfsana Shah, Deepak K Mittal, Gowhar Ahmad Shigan, Nihar Kant Ajena, Dinesh Kumar, Pragya Shukla
24 - 29
4. A Correlation of Mean Platelet Volume (MPV) and Red Cell Distribution Width (RDW) in Type 2 Diabetic Patients in a Tertiary Care Center of Northern IndiaAnubha Srivastava, Anurag varma, Rajneesh Tiwari
30 - 33
5. Awareness about Lifestyle, Diet & Physical Activity among Diabetic Patients in a Tertiary Care Teaching HospitalRavikant, Vinita Thapliyal, Shweta verma, Shikha Saini, Shruti Barnwal
34 - 38
6. A Study of Clinical outcome and analysis of 50 Cases of Snake BiteVaishali N. Vegada, Hiren N. Makvana
39 - 41
REVIEW ARTICLE
7. Treatment of Allergic Bronchopulmonary Aspergillosis Rajendra Prasad, Rishabh Kacker, Nikhil Gupta
42 - 45
8. Beyond Diabetes, Metformin may prove to be a ‘Wonder Drug’Rakesh Kumar
46 - 51
9. Tuberculous MyocarditisAmitesh Aggarwal, Prabhat Gautam Roy, Rohit Gupta
52 - 55
10. Tuberculosis in Diabetes Mellitus : A Systematic ReviewYakshita Goyal, Chahat Saini, Surbhi Khanna, Shivam Nagpal, Ashish Goel
56 - 61
CASE REPORT
11. Early Detection - Need of The Hour: A Case Report of Swallowed Fishbone causing PneumomediastinumAmitesh Aggarwal, Rakshit R. bhardwaj
62 - 64
12. A Rare Presentation of Hemophilia A in a female PatientTejas D. Sailor, Subhashchandra K.Gadhvicharan
65 - 68

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
2 © JIMI • JULY - SEPT 2019 • VOL. 13
JIMIJOURNAL OF INTERNAL MEDICINE OF INDIA
Editor-in-Chief: Dr. S. Chakravorty
Editorial Board
www.upjimi.com
Associate Editors Prof.(Dr.)SaritaBajaj•Prof.(Dr.)OmKumariGuptaAssistant Editors Prof.(Dr.)MadhukarRai•Prof.(Dr.)KauserUsman•Dr.D.HimanshuEditorial Secretary Prof.(Dr.)AmiteshAggarwal•Dr.A.K.Shukla•Dr.MeenakshiJainPeer Reviewer Prof.(Dr.)SaritaBajaj•RichaGiri•Dr.JayaChakravorty
Subscription InformationUttar Pradesh Journal of Internal Medicine of India (ISSN: 0972-1096). For 2019, Volume 13 (3 issue) is scheduled for publication. Subscription prices are available upon request from UP Journal of Internal Medicine of India or from this Journal website (www.upjimi.com)
Copyright PolicyThe content and context of the papers are written by authors and compiled in this volume. The originality and authenticity of the papers and the interpretation of information and views expressed therein are the sole responsibility of the authors. The publishers or editors do not take any responsibility for the same in any manner. Although every care has been taken to avoid errors and omissions, JIMI is being published on the condition and undertaking that the information given in this Journal is merely for reference and must not be taken having authority of, or binding in any manner on the editors or publisher.
Editorial & Publishing Office Dr. S. ChakravortyT-21, SECTOR-11, NOIDA-201301 (UP). INDIAE-mail: [email protected]: 9810210479, 9667668146
Dr. N.K. Soni
Dr. Arvind Mishra
Dr. Virendra Atam
Dr. Veerendra Singh
Dr. R.R. Singh
Dr. Anuj Maheshwari
Dr. K.K. Salwani
Dr. Praveen Kumar Bass
Dr. K.C. Lohani
Dr. Jalees Fatima
Dr. Mahim Mittal
Dr. Balvir Singh
Dr. Sudhir Agarwal
Dr. Sanjay Tandon
Dr. Atul Mehrotra
Dr. Nirupam Prakash
Dr. Sandeep Chaudhary
Dr. Sanjay Singh
Dr. A.K. Singh
Dr. Sameer Gupta
Dr. Abha Gupta
Dr. Saurabh Shrivastava
Dr. S.K. Sahoo
Dr. Ravi Kant

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
3© JIMI • JULY - SEPT 2019 • VOL. 13
GoverningBodyMembers Co-optedMembers
GoverningBodyASSOCIATIONOFPHYSICIANSOFINDIA
UPCHAPTER
GoverningBodyASSOCIATIONOFPHYSICIANSOFINDIA
NOIDACHAPTER
Chairman Dr.VeerendraSinghVice-Chairman Dr.K.K.Sawlani Dr. S. C. ChaudharyHon.Secretary Dr.SanjayTandonTreasurer Dr.D.HimanshuJointSecretaries Dr.S.Chakravorty Dr.NirupamPrakash
Dr.AtulMehrotraDr.AnupamWakhluDr.SandeepChaudharyDr.JaleesFatimaDr.S.K.GautamDr.SmitaGupta
PatronProf. (Dr.) B. C. BansalProf. (Dr.) Om Kumari GuptaDr. S. K. PlahaFormerChairmanDr. Subodh ChandraDr. K.C. SoodDr. G.C. VaishnavaDr. S. ChakravortyChairmanDr. R. K. GattaniViceChairmanDr. G.C. Gupta
SecretaryDr. Meenakshi JainTreasurerDr. A.K. ShuklaJointSecretaryDr. Kuldeep DharProf. (Dr.)Amitesh AggarwalDr. Kiran SethScientificAdvisorDr. Neeru GeraDr. L.K. JhaDr. Amitabh YaduvanshiDr. R.K. PrasadProf. (Dr.) Saurabh SrivastavaDr. Amit Kumar Gupta
CoreCommitteeMemberDr. Sanjay WadhawanDr. Vandana GargDr. Ajay AggarwalDr. N. K. SharmaDr. K.D. KotliaDr. S.K. SahooDr. P.K. GuptaDr. Sanjay MahajanDr. Manju TyagiDr. Vinay LabrooDr. Zeenat Ahmad
Dr.RichaGiriDr.T.P.SinghDr. Jaya ChakrovartyDr.AnubhaSrivastavaDr.AbhaGupta
JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
4 © JIMI • JULY - SEPT 2019 • VOL. 13
Editorial
Dear All,Journal of Internal Medicine of India-UP Chapter is about to complete 4 years. It had been a tedious journey to maintain and upkeep the standard of the journal over such a long period of time. The journal acts as an academic representative for all of us especially those who are engaged as a teaching faculty. I request your utmost cooperation to maintain and smoothly run the journal in future.
Hydroxychloroquine is available as antimalarial medication over 60 years and is still prescribed today for treatment and prophylaxis.Later USFDA approved it for other indications like discoid lupus, systemic lupus erythematosus, and rheumatoid arthritis.1Hydroxychloroquine differs from chloroquine by presence of hydroxyl group at the end of side chain but no difference in pharmacokinetic property.
The present world is experiencing a pandemic (Covid 19) caused by novel strain of coronavirus. Diversion of all healthcare facilities towards the Covid 19 pandemic is likely to increase the morbidity and mortality due to other health problems. Another conundrum faced is a high secondary infection rate among high-risk healthcare workers annexing the already burdened healthcare system. In the absence of specific treatment against Covid 19, prevention is the best strategy not only to prevent more spread and deaths but also to unburden the healthcare system. Prophylaxis in the present context refers to the use of short - term therapy to prevent acquisition of SARS-Co-V-2 infection. Currently there is lot of speculation on chemoprophylaxis stemming from the available data on the use of hydroxychloroquine, which has been tried for the treatment of Covid 19.2
In vitro activity of chloroquine and hydroxychloroquine in Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection.3
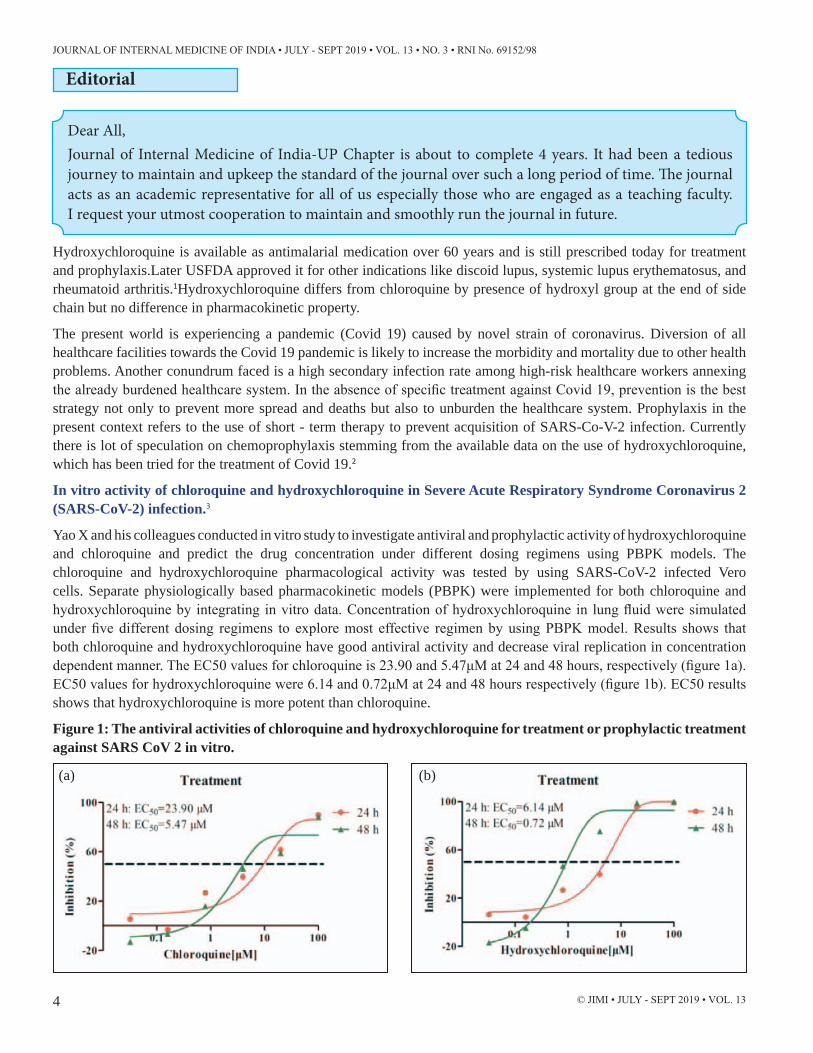
Yao X and his colleagues conducted in vitro study to investigate antiviral and prophylactic activity of hydroxychloroquine and chloroquine and predict the drug concentration under different dosing regimens using PBPK models. The chloroquine and hydroxychloroquine pharmacological activity was tested by using SARS-CoV-2 infected Vero cells. Separate physiologically based pharmacokinetic models (PBPK) were implemented for both chloroquine and hydroxychloroquine by integrating in vitro data. Concentration of hydroxychloroquine in lung fluid were simulated under five different dosing regimens to explore most effective regimen by using PBPK model. Results shows that both chloroquine and hydroxychloroquine have good antiviral activity and decrease viral replication in concentration dependent manner. The EC50 values for chloroquine is 23.90 and 5.47μM at 24 and 48 hours, respectively (figure 1a). EC50 values for hydroxychloroquine were 6.14 and 0.72μM at 24 and 48 hours respectively (figure 1b). EC50 results shows that hydroxychloroquine is more potent than chloroquine.
Figure 1: The antiviral activities of chloroquine and hydroxychloroquine for treatment or prophylactic treatment against SARS CoV 2 in vitro.
(a) (b)

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
5© JIMI • JULY - SEPT 2019 • VOL. 13
Antiviral Pre-treatment (prophylaxis) activity in vitro
Prophylactic treatment of hydroxychloroquine shows superior in vitro antiviral effect compared to chloroquine. EC50 value for chloroquine is >100 and 18.01μM at 24 and 48 hours, respectively. EC 50 valuesfor hydroxychloroquine were 6.25 and 5.85 μM at 24 and 48 hours, respectively (figure 1c and 1d).
(c) (d)
Dose regimen optimization done by using PBPK models to predict the lung tissue concentration of chloroquine and hydroxychloroquine under different dosing regimens. The RLTEC values of hydroxychloroquine were found tobe higher than the RLTEC values of chloroquine on days 1, 3, 5 and 10. This suggest that hydroxychloroquine may achieve ideal clinical efficacy under the simulateddosing regimens (Table 1).Based on PBPK models results, a loading doseof 400 mg twice daily of hydroxychloroquine sulfate given orally, followed by amaintenance dose of 200 mg given twice daily for 4 days is recommended forSARS CoV 2 infection, as it reached three times the potency of chloroquinephosphate when given 500 mg twice daily 5 days in advance.
Table 1: Ratios of free lung tissue trough concentration/EC50 (RLTEC) under different dosage regimens
In conclusion, hydroxychloroquine found to be more potent than chloroquine in SARS-CoV-2 infection. The recommended dose is 400 mg twice daily on day 1, followed by 200 mg twice daily for 4 more days.
Effect of Hydroxychloroquine in Covid 19 patients.
Zhaowei Chen and his colleagues has conducted study on Hydroxychloroquine in patients with Covid 19 corona virus infection at Wuhan University. Around 62 Covid 19 confirmed patients (mean age of 45 years with no difference in sex

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
6 © JIMI • JULY - SEPT 2019 • VOL. 13
and age distribution) were randomized to receive standard treatment (n=31) including oxygen therapy, antiviral agents, antibacterial agents, and immunoglobulins with or without corticosteroids and patients in intervention group (n=31) received Hydroxychloroquine tablets 400 mg/day on day 1-5.
Changes intime to clinical recovery (TTCR), clinical characteristics of patients and any severe adverse effects observed after 5 days of treatment were taken as endpoints lost to follow up.
The clinical recovery, defined as return to body temperature (Body temperature ≤36.6 °C on the surface, ≤ 37.2 °C under the armpit and mouth or ≤ 37.8 °C in the rectum and tympanicMembrane) and cough relief (patients’ reports, slight or no cough was in the asymptomatic range), which is maintained for 72 hours, was taken as primary endpoint. For radiological changes, chest CT has done on one day before (day 0) and one day after (day 6).
The patients received Hydroxychloroquine group has shown significant shorter time to body temperature recovery vs. control group (2.2 days vs. 3.2 days, p=0.0008) and time taken for cough remission also less with hydroxychloroquine group compared to control group (2.0 vs. 3.1 days, p=0.0016). Further effect of HCQ on pneumonia evaluated with help of Chest CT, which shows 80.6% (25/31) improvement in pneumonia in hydroxychloroquine received groups compared to 54.8% (17/31) in control group. Besides, 61.3% of patients in the HCQ treatment group had a significant pneumonia remission.
In conclusion: Hydroxychloroquine has shown promising results in the treatment of Covid 19 corona virus infection. However,large-scale study is still required to clarify its specific mechanism and to optimize the treatment.4
Hydroxychloroquine and azithromycin as a treatment of COVID-19: A open label, non-randomized trial5
Gautret P et al conducted open label study to evaluate the role of hydroxychloroquine on respiratory viral loads. 42 French patients (26 patients received hydroxychloroquine and 16 patients were control, mean age is 45.1 years) confirmed with Covid 19 infection were included in the study. Patients received 600mg of hydroxychloroquine daily and their viral load in nasopharyngeal swabs was tested daily in hospital setting. Azithromycin 500 mg was added to treatment based on clinical presentation of the patients. Presence or absence of virus at day 6 was considered the endpoint. The results presented for only 36 patients (20 patients treated with hydroxychloroquine and 16 patients were control) as six patients were lost follow-up. Results: 70% of the patients treated with hydroxychloroquine shows virologically cured compared to 12.5% on control group (P=0.001) after day 6 post inclusion. While, 100% patients treated with combination of hydroxychloroquine and azithromycin shows virologically cure compared to 57.1% in patients treated with only hydroxychloroquine and 12.5% in control group (p<0.001) (figure 2&4).
Figure 2: Percentage of patients with PCR-positive nasopharyngeal samples in COVID-19 patients treated with hydroxychloroquine and in control patients.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
7© JIMI • JULY - SEPT 2019 • VOL. 13
Figure 3: Percentage of patients with PCR-positive nasopharyngeal samples in COVID-19 patients treated with hydroxychloroquine only, hydroxychloroquine and azithomycin combination, and in control group.
This study shows that hydroxychloroquine treatment significantly decreases the viral load /disappearance of virus in Covid 19 patients and its effect is reinforced by azithromycin.
Hydroxychloroquine in Health care workers and SARS-CoV-19 – Case control study2
Pranab Chatterjee and his team developed (ICMR Covid 19 research team) case control study proposal to investigate risks and protective factor against SARS-CoV-2 infection among HCWs, which is approved by central ethics committee. Participant undergoing testing for SARS-Co-V-2 infection (during May 8-23, 2020) across India was used as study participants. Health care workers tested between 1st week of April 2020 and the end of the first week of May 2020 formed the sample pool from which cases and control were drawn. Around 21,402 individuals data were obtained with 1073 (5%) confirmed SARS-Cov-2 infected HCWs. Only 624 and 549 individuals are completed interview schedules of which 60.58% of cases (378/624) and 67.94% of controls (373/549) available for analysis. The number of maintenance doses taken by HCWs following intake of loading dose revealed protective dose response relationship. Consumption of 4 or more maintenance doses was associated with significant decline in the risk of SARS-CoV-2 infection among the study participants (P<0.001) (figure 4).
Figure 4: Dose-response relationship between hydroxychloroquine(HCQ) exposure and severe acute respiratory syndrome coronavirus2 (SARS-CoV-2) infection.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
8 © JIMI • JULY - SEPT 2019 • VOL. 13
Use of PPE, endotracheal intubation, prophylactic hydroxychlorquine and intake of 4-5 maintenance doses of HCQs were found independently impart the protective effect against SARS-CoV-2 infection among Health care workers. > 80% of protective effects seen against SARS-CoV-2 infection those who have used more than six doses of HCQs. Of the 172 cases and 193 controls reporting HCQ intake, no significant difference in the occurrence of adverse drug reactions was noted.Nausea (5 vs. 8%), headache (6vs5%) and diarrhea (5vs4%) are the common adverse events reported with hydroxychloroquine treated case and controls.
In conclusion, this study shows the consideration of HCQ as prophylaxis for the prevention of SARS-CoV-2 infection among healthcare workers.
Investigation from 3 central government hospitals in New Delhi
An investigation conducted in three central government hospitals in New Delhi to investigate the effect of hydroxychloroquine in healthcare workers in Covid 19 care. The people who have taken hydroxychloroquine as prophylaxis show less likely to develop SARS-CoV—2 infection compared to those who have not taken prophylaxis treatment.
Another prospective observational study conducted at AIIMS hospital to investigate the effect of hydroxychloroquine in healthcare workers. Total 334 healthcare workers involved in this study, out of which 248 individuals taken hydroxychloroquine as prophylaxis (median 6 weeks of follow up). Those individuals taken HCQ prophylaxis had lower incidences of SARS-CoV-2 infection compared to those who have not taken prophylaxis.
Precautions to be taken before using hydroxychloroquine1• Measure glucose-6 phosphate dehydrogenase if indicated
• Take ocular history and order baseline ophthalmologic evaluation
• Screen for digoxin use
• Screen for history of cardiomyopathy or severe heart failure
• Counsel patient on risks of use, including permanent loss of vision and recommended frequency of screening retinal examination
• Counsel on risks of skin rashes, gastrointestinal upset, increased hair and skin pigmentation
• Obtain baseline laboratory testing
Revised advisory on the use of Hydroxychloroquine (HCQ) as prophylaxis for SARS-CoV-2 infection6
Eligibility criteria for HCQ prophylaxis1. All asymptomatic healthcare workers involved in containment and treatment of COVID19 and asymptomatic
healthcare workers working in non-COVID hospitals/non-COVID areas of COVID hospitals/blocks
2. Asymptomatic frontline workers, such as surveillance workers deployed in containment zones and paramilitary/police personnel involved in COVID-19 related activities.
3. Asymptomatic household contacts of laboratory confirmed cases.
Dosage:
Category of personnel DosageAsymptomatic household contacts of laboratory confirmed cases
400 mg twice a day on Day 1, followed by 400 mg once weekly for next 3 weeks; to be taken with meals.
All asymptomatic healthcare workers involved in containment and treatment of COVID-19 and asymptomatic healthcare workers working in non-COVID hospitals/non-COVID areas of COVID hospitals/blocks
400 mg twice a day on Day 1, followed by 400 mg once weekly for next 7 weeks; to be taken with meals.
Asymptomatic frontline workers, such as surveillance workers deployed in containment zones and paramilitary/police personnel involved in COVID-19 related activities
ICMR further recommend its use beyond 8 weeks as weekly doses with strict monitoring of clinical and ECG parameters.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
9© JIMI • JULY - SEPT 2019 • VOL. 13
Exclusion/contraindications:
• The drug is contraindicated in persons with known case of:
1. Retinopathy,
2. Hypersensitivity to HCQ or 4-aminoquinoline compounds
3. G6PD deficiency
4. Pre-existing cardiomyopathy and cardiac rhythm disorders
• The drug is not recommended for prophylaxis in children under 15 years of age and in pregnancy and lactation.
Rarely the drug causes cardiovascular side effects such as cardiomyopathy and rhythm (heart rate) disorders. In that situation the drug needs to be discontinued. The drug can rarely cause visual disturbance including blurring of vision which usually self-limiting and improves on discontinuation of the drug. For the above cited reasons the drug has to be given under strict medical supervision with an informed consent.
REFERENCES:
1 Shippey EA et al. Hydroxychloroquine: An old drug with new relevance. Cleveland clinic journal of medicine. 2018;85(6): 459-467
2 Chatterjee P et al. Healthcare workers & SARS-CoV-2 infection in India: A case-control investigation in the time of COVID-19. Indian J Med Res. 2020. DOI: 10.4103/ijmr.IJMR_2234_20.
3 Yao X et al,Published by Oxford University Press for the Infectious Diseases Society of America. Accessed on 04/06/2020.
4 Chen Z, et al “Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial” medRxiv 2020; DOI: 10.1101/2020.03.22.20040758.
5 Gautret p et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020 Mar 20 : 105949.doi: 10.1016/j.ijantimicag.2020.105949.
6 https://www.icmr.gov.in/pdf/covid/techdoc/V5_Revised_advisory_on_the_use_of_HCQ_SARS_CoV2_infection.pdf. Accessed on 04/06/2020.
7. Chen Z, et al “Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial” medRxiv 2020; DOI: 10.1101/2020.03.22.20040758.
8. Gautret p et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020 Mar 20 : 105949. doi: 10.1016/j.ijantimicag.2020.105949.
9. https://www.icmr.gov.in/pdf/covid/techdoc/V5_Revised_advisory_on_the_use_of_HCQ_SARS_CoV2_infection.pdf. Accessed on 04/06/2020.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
10 © JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
A Hospital based Observational Study to establish the cause of Ascites using Serum Ascites Cholesterol Gradient in
North Indian patients
ABSTRACT:
Background: Ascites is manifestations of many diseases besides liver cirrhosis like tubercular ascites, congestive heart failure, bacterial peritonitis, pancreatic ascites and malignancy related ascites. SAAG is an effective parameter to identify ascites due to portal hypertension. But establishing the cause of low SAAG ascites remains difficult.
Aims and objective: To establish the cause of ascites with reference to Serum Ascitic Cholesterol Gradient (SACG) and assess the validity of Serum Ascites Cholesterol Gradient in diagnosis of malignant ascites.
Methods: 106 patients of ascites were investigated for ascitic fluid cholesterol, and SACG, USG Abdomen and other investigation.
Results: The mean SACG was 81.2722.07 mg/dl in the malignant ascites and in the non malignat group was 113.66, p value <0.001 which shows that SACG was highly significant in differentiating malignant ascites from the non-malignant ascites. The sensitivity and specificity of Serum Ascites Cholesterol Gradient at cut off value of 90mg/dl was 94.44% and 91.46% respectively. The mean value of SACG in tubercular ascites was 115.5±33.22 and in malignant group was 75.55±16.69, p value<0.001 There was significant difference in SACG in tubercular and malignant ascites.
Conclusion: Ascitic fluid cholesterol and SACG can be used as an effective parameter to differentiate malignant ascites from tubercular ascites. It is cost effective method even at small centers with limited diagnostic facilities.
Keywords: Ascites, malignant ascites, tubercular ascites, ascitic fluid cholesterol, SACG.
1. Associate Professor of Medicine, GSVM Medical College, Kanpur, Uttar Pradesh, India.2. Associate Professor of Medicine, GSVM Medical College, Kanpur, Uttar Pradesh, India.
(Corresponding Author) E-mail: [email protected]. Junior Resident of Medicine, GSVM Medical College, Kanpur, Uttar Pradesh, India.4, 5. Professor of Medicine, GSVM Medical College, Kanpur, Uttar Pradesh, India.6. Medical Officer Family Planning, GSVM Medical College, Kanpur, Uttar Pradesh, India.7. Associate Professor of PSM, GSVM Medical College, Kanpur, Uttar Pradesh, India.
Shri Krishna Gautam1, Brijesh Kumar2, Surya Prakash Jha3, Richa Giri4, J.S. Kushwaha5, Anita6, Santosh Burman7
INTRODUCTION:
Ascites occurs as a manifestation of various of disease. Liver cirrhosis (80%) is the most common cause of ascites. Beside this malignancy related ascites (10%), tubercular peritonitis (2%), congestive cardiac failure, nephrotic syndrome, others (3%) are important causes of ascites.1,2 Diagnostic ascitic fluid analysis is central to the
diagnosis of cause of ascites. Initially etiology of ascites was based on the value of ascitic fluid protein.
Ascitic fluid protein value≤2.5 g% is considered transudative and exudative if >2.5 g%.3,4,5 Presently SAAG (serum ascites albumin gradient) is used to classify ascites in place of ascitic fluid protein. Differential diagnosis of low SAAG (<1.1) includes

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
11© JIMI • JULY - SEPT 2019 • VOL. 13
malignancy related ascites, abdominal tuberculosis.3,5,7 Ascitic fluid microscopy and ascitic fluid ADA can help in diagnosis of tubercular ascites.6 The most definitive test for diagnosis of malignancy related ascites is ascitic fluid cytology. But it has low sensitivity (64%)8. Beside this collection and processing of ascitic fluid sample for cytology is cumbersome and identification of malignant cells in ascitic fluid requires expert pathologist. So, we are in search of new marker that can help to differentiate malignancy related ascites.
Previous studies have shown increased ascitic fluid cholesterol in malignancy related ascites as well as in tubercular ascites. So, we perform the following study usefulness of serum ascites cholesterol gradient in differential diagnosis of ascites.
AIM AND OBJECTIVES:
1. To establish the cause of ascites with reference to Serum Ascitic Cholesterol Gradient (SACG).
MATERIAL & METHODS:
This hospital based prospective observational study has been carried out in PG Department of Medicine, LLR & associated hospitals, GSVM Medical College, Kanpur during July 2018 to June2019. The study was approved by ethical committee of GSVM Medical college Kanpur.
Inclusion Criteria: -
• Age>18 yrs.
• Clinical features suggestive of ascites or ultrasonography suggestive of ascites
• Willing to participate in the study and gave consent.
Exclusion Criteria: -
Patient with bacterial peritonitis.
Patient on drug therapy that would alter Serum Cholesterol.
Methodology:
An informed consent was taken either from the patient or their relatives before interview, examination and investigation.
After examination of patient following diagnostic tests were performed-
CBC, LFT, KFT, PT/INR, Lipid profile and ultrasonography of abdomen.
Diagnostic paracentesis9,10,11 was done with prior written consent using 20-22-gauge 2.5-inch disposable needles under sterile precautions using Z tract technique. Around 50ml fluid is aspirated and fluid is immediately sent for
physical, chemical, biochemical analysis, ascitic fluid cholesterol ascitic fluid ADA, cytological analysis for cell counts and differential count, malignant cells and ZN staining.
Serum samples and ascitic fluid sample were drawn simultaneously. CT scan abdomen and Pelvis, upper GI endoscopy were done in selected cases where it is needed.
• Diagnosis of liver cirrhosis confirmed by clinical features of Portal HTN and Hepato-cellular failure, alcohol history, and ultra sound (Coarse hepatic echotexture with nodularity, Dilated collaterals around the gastroesophageal junction and splenic hilum, splenomegaly and dilated portal vein >12.5 mm in diameter.
• Congestive heart failure confirmed by clinical history, ECG, 2D echo, X ray chest.
• Diagnosis of tubercular ascites:
Mesenteric lymphadenopathy >10mm (on USG abdomen/CT abdomen)Ascitic fluid analysisTotal cells >500Polymorphonuclear<50%ADA >40Acid fast bacilli staining positive.
Nephrotic syndrome and chronic kidney disease confirmed by clinical history, ultra sound abdomen, Urine Albumin, 24 hours urinary protein, lipid profile, blood urea, serum creatinine.
Pancreatitis confirmed by clinical history, ultra sound abdomen, CT abdomen, serum amylase, serum lipase, ascetic fluid amylase.
Diagnosis of malignancy related ascites-
Ultrasonography or CT scan abdomen suggestive of intra-abdominal,pelvic malignancy or peritoneal metastasis
Ascitic fluid analysisTotal cell >500Polymorphonuclear cells<50%Positive cytology for malignant cells
Statistical analysis:
The data was collected and entered in MS Excel and a master chart was made. The data was analyzed using appropriate statistical tools i.e. SPSS (23rd version) like percentage, mean, SD by using chi-square test and z test and results were drawn accordingly.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
12 © JIMI • JULY - SEPT 2019 • VOL. 13
RESULTS:We studied 106 patients of ascites age above 18 years. 6 patients were excluded from the study. 4 of them had bacterial peritonitis and 2 of them were taking lipid lowering drugs. Out of remaining 100, 64% were males and 34% females. Majority of the cases i.e. 87% were aged above 30 years and highest no. of cases in above 60 years age group (24%).). The mean age of the patients who took part in study was 48.6914.37. The lowest age is 22 years and the highest age was 70 years.
TABLE 1: AGE WISE SEX DISTRIBUTIONAge(years) Male Female Total18-30 7(7%) 6(6%) 13(13%)31-40 13(13%) 10(10%) 23(23%)41-50 12(12%) 6(6%) 18(18%)51-60 16(16%) 6(6%) 22(22%)>60 16(16%) 8(8%) 24(24%)Total 64(64%) 36(36%) 100(100%)
TABLE 2: DISTRIBUTION OF PATIENTS ACCORDING TO ETIOLOGYEtiology Male Female TotalChronic liver disease
41(41%) 17(17%) 58(58%)
Tubercular effusion
8(8%) 4(4%) 12(12%)
Malignant ascites
8(8%) 10(10%) 18(18%)
Other causes 7(7%) 5(5%) 12(12%)
Out of 100 patients, 82(82%) patients were diagnosed as non-malignant ascites and 18(18%) were diagnosed with malignancy.
82 non-malignant patients were further sub divided into 3 groups based on etiology. 58(58%) patients were of chronic liver disease, 12(12%) of tubercular ascites and 12(12%) patients with ascites of other cause. Other causes of ascites are decompensated heart failure, chronic kidney disease, nephrotic syndrome.
TABLE 3: ASCITIC FLUID CHOLESTEROL AND SACG VALUE IN MALIGNANT AND NON-MALIGNANT GROUP
Non-malig-nant (n=82)
Malignant (n=18)
P value
Ascites Cholesterol (mg/dl) (mean SD)
17.98±13.35 74.83±32.47 0.001
SACG (mg/dl) 113.66±31.24 81.27±22.07 0.001
The mean value of ascitic fluid cholesterol in the non-malignant group was 17.98±13.35 mg/dl and in malignant group was 74.83±32.47mg/dl(p<0.001). The mean SACG was 81.2722.07 mg/dl in the malignant ascites and in the non-malignant group was 113.66 , p value <0.001 which shows that SACG was highly significant in differentiating malignant ascites from the non-malignant ascites.
TABLE 4: ASCITIC FLUID CHOLESTEROL AND SACG VALUE IN MALIGNANT AND TUBERCULAR GROUP
Malignant (n=18)
Tubercular (n=12)
P value
Ascitic-fluid Cholesterol (mean SD) (mg/dl)
74.8332.47 21.66 0.001
SACG (mg/dl) (mean SD)
75.55±16.69 115.5±33.22 0.001
The mean value of ascites fluid cholesterol in the tubercular group was 21.66mg/dl and 74.83±32.47mg/dl in the malignant group (p-value <0.001).The mean value of SACG in tubercular ascites was 115.5±33.22 and in malignant group was 75.55±16.69, p value<0.001 There was significant difference in SACG in tubercular and malignant ascites.
TABLE 5: Sensitivity, specificity, PPV and NPV of SACG
Specific-ity
Sensitiv-ity
Positive predic-
tive value (PPV)
Negative predic-
tive value (NPV)
Serum ascitic Cholester-ol Gradi-ent(90mg/dl)
91.46% 94.44% 70.83% 98.68%
The sensitivity and specificity of Serum Ascites Cholesterol Gradient at cut off value of 90mg/dl was 94.44% and 91.46% respectively. The PPV was 70.83% and NPV was and 98.68% respectively.
DISCUSSION:
Many diseases are complicated by ascites. Its appropriate treatment depends on proper diagnosis.12 SAAG is of no value in differentiating malignant from tubercular ascites.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
13© JIMI • JULY - SEPT 2019 • VOL. 13
The search for novel biochemical markers in the serum and ascitic fluid is still under investigation. In this approach cholesterol have shown to be a promising marker.
This study showed that ascitic fluid cholesterol and serum ascites cholesterol gradient to be reliable parameters to differentiate cirrhotic and malignancy related ascites. A number of previous workers have shown the relation between high ascitic fluid cholesterol and the _occurrence of malignant ascites.13,14,15,16 The etiology for the elevated cholesterol level in malignancy is due to the increased vascular permeability increased cholesterol synthesis and release from malignant cell implanted on peritoneum.17
The ascitic fluid cholesterol was compared in malignant and non-malignant group the mean cholesterol level was found to be 74.83mg/dl in the malignant group and 17.98mg/dl in non-malignant group, p-value of <0.001. The mean SACG was 81.2722.07 mg/dl in the malignant ascites and in the non malignat group was 113.66 , p value <0.001 The sensitivity and specificity of Serum Ascites Cholesterol Gradient at cut off value of 90mg/dl was 94.44% and 91.46% respectively in differentiating malignant and non-malignant ascites. The mean value of serum ascites fluid cholesterol in the tubercular group was 21.66mg/dl and 74.83±32.47 mg/dl in the malignant group, p value 0.001. The mean value of SACG in tubercular ascites was 115.5±33.22 and in malignant group was 75.55±16.69, p value<0.001.
Prieto et al18 showed that ascitic fluid cholesterol concentrations were significantly higher in patients with peritoneal metastases and was superior to ascitic fluid total protein, lactate dehydrogenase and SAAG for discriminating ascites from that due to liver disease. Similar results were found by Chelliah Dharmaraj1 et al24 found the mean (±SD) of serum ascites cholesterol gradient (SACG) for cirrhosis group was 67.52 (±4.46) and that for MRA group was 60.16 (±3.38).
T. N. Dubey et al25 also showed that these values are significantly higher in cirrhosis than tuberculosis or malignancy. Sharatchandra, LK et al20also reported that the mean ascitic cholesterol level was significantly higher in malignant ascites (100 mg/dl) than in non-malignant ascites(31.44mg/dl). SACG values in cirrhosis, tuberculosis, and malignant group as 99.2 ± 27.8, 54.16 ± 36.26, and 50 ± 23 respectively and with a cut-off value of 65 mg% the gradient was significantly higher in cirrhotic ascites compared to malignant and tubercular ascites but with a lower sensitivity (80%) and specificity (80%).
Mukhyaprana P et al21calculated ascitic fluid cholesterol in ascites patients. Ascitic fluid cholesterol value in
cirrhotic, malignant and tubercular ascites was 17.75mg/dl, 93.15mg/dl and 63.15mg/dl respectively. The results were similar to our study in cirrhotic and malignant ascites but in tubercular group they observed a higher ascitic fluid cholesterol.
Study performed Vyakaranam S et19also observed that the malignant group had lowest SACG (44.3mg %) when compared with cirrhosis (96.48mg %) and tuberculosis (86.13mg%) (p=0.0001, p=0.001 respectively). The difference between cirrhosis and tuberculosis group was not significant (p >0.05).
Almost similar result also reported by Sastry AS et al22, Serum Ascitic Cholesterol Gradient was found lower in malignant Ascites 36.4mg/dl vs 72.4mg/dl in non-malignant group. With SACG cut off value of 54mg/dl sensitivity was 90% and specificity of 95%.
CONCLUSION:
This study has shown that increased levels of ascitic fluid cholesterol, serum ascites fluid cholesterol gradient are very good indicators of malignant ascites. They hold promises to be reliable and yet simple and cost-effective parameter even at small centers with limited diagnostic facilities.
A large multicenter study will be required to validate the significance of the above values. In view of good diagnostic efficiency, we propose that ascitic fluid cholesterol and SACG can be used as an effective parameter to differentiate malignant ascites. These are simple and cost-effective method for diagnosing the etiology of ascites in developing countries.
REFERENCES :
1. Runyon ba. Management of adult patients with ascites due to cirrhosis. Aasld practice guideline. Hepatology 2004; 39:1-16
2. Moore kp, aithalgp. Guidelines on management of ascites in cirrhosis .gut 2006; 55 (suppl.vi):vi1-12.
3. Pare p, talbot j, hoefsjc. Serum ascites albumin gradient- a Rector WG. An improved diagnostic approach to ascites. Arch Intern Med 1987; 147: 215. physiological approach to differential diagnosis of ascites. Gastroenterology 1983; 85(2):240-4
4. Sampliner R, Iber F. High protein ascites in patients with uncomplicated hepaticcirrhosis. American journal of medical science, 1974; 267: 275-9.
5. Rector wg, reynoldstb. Superiority of serum ascites albumin difference over the ascites total protein

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
14 © JIMI • JULY - SEPT 2019 • VOL. 13
concentration in separation of transudative and exudative ascites. Am j med1984; 77:83-5.
6. Dwivedi M, Misra SP, Misra V. Value of adenosine deaminase estimation in the diagnosis of tuberculous peritonitis. American Journal of Gastroenterology1990; 9:1123-5
7. Rector wg. An improved diagnostic approach to ascites. Arch intern med 1987; 147: 215.
8. Rana sv, babu sgvetal. Usefulness of ascetic fluid cholesterol as a marker for malignant ascites. Med scimon 2005; 11:136-42.
9. Hoefsjc. Diagnostic paracentesis: a potent clinical tool. Gastroenterology1990; 98:230-6.
10. Runyon ba. Paracentesis of ascitic fluid: a safe procedure. Arch intern med 1986; 146:225961.
11. Romney r, mathurin p, ganne-carrie n, etal. Usefulness of routine analysis of ascitic fluid at the time of therapeutic paracentesis in asymptomatic out patients. Results of multicenter prospective study. Gasterolclinbiol 2005; 29:275-9.
12. Menon VP, Jiandani PG, et al. Ascitic fluid analysis--the yet new investigation. J Assoc Physicians India. 1995;43: 743-744
13. Halpedn, R., Hadas, E., Bukovsky, I., Schneider, D. (1999) Peritoneal fluid analysis in the differentiation of ovarian cancer and benign ovarian tumor. Eur-J-GynaecokOncol. 20(1), 40-44.
14. Bansal, S., Kaur, K., and Bansal, A.K. (1998) Diagnosing ascitic etiology on a bio chemical basis. Hepatogastroentemiogy. 45 (23~,1673-1677.
15. Castaldo, G., Oriani, G., Cimino, L, Topa, M., Mostarda, I. and Castallano, L. (1994) Total discrimination of peritoneal malignant ascites from cirhosis- and hepatocaminoma - associated ascites by assays of ascitic cholesterol and lactate dehydrogenase. Clin-Chem. Mar: 40(3), 478-483.
16. Garg, R., Sood, A., Arora, S., Bhatia, K.L., Chawia, L.A., Gupta, R. and Chawla, LS.(1993) Asoiticfluid cholesterol in differential diagnosis of ascites. J.Assoc.Physicians.lndia. 41(10), 644-646.
17. Lu CW, Wang SS, Lee SD, et al. Ascitic fluid analysis in peritoneal carcinomatosis: comparison of various biochemical tests with ascitic cirrhotics. Zhonghua Yi Xue Za Zhi (Taipei). 1991;47:350-356.
18. Prieto M, Gómez-Lechón MJ, Hoyos M, et al. Diagnosis of malignant ascites. Comparison of ascitic fibronectin, cholesterol,and serum-ascites albumin difference. Dig Dis Sci. 1988;33:833-838.
19. Vyakaranam S, Nori S, Sastry GM, Vyakaranam SB, Bhongir AV. Serum - Ascites Albumin and Cholesterol Gradients in Differential Diagnosis of Ascites. NJIRM. 2011;2(3):22-8.
20. Sharath Chandra LK, Mingsen T, Singh YI. Serum ascites lipid gradients in alcoholic liver cirrhosis, tuberculosis and malignancy. JIACM. 2005;6:106-9.
21. Prabhu, Mukhyaprana, Rahul Sai Gangula, and Weena Stanley. “Diagnostic Utility of Serum Ascites Lipid and Protein Gradients in Differentiation of Ascites.” Research article. International Journal of Hepatology, 2019. https://doi.org/10.1155/2019/8546010
22. Sastry AS, Mahapatra SC, Dumpula V. Ascitic fluid analysis with special reference to serum ascites cholesterol gradient and serum ascites albumin gradient. Int J Res Med Sci 2017;5:429-36
23. B.a.runyon,a.a.montano,e.a.akriviadis,m.r.antillon, m. A. Irving, and j. G. Mchutchison, “the serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites,” annals of internal medicine,vol.117,no.3,pp.215–220,1992
24. Chelliah Dharmaraj, Sigamani Saranya, Hibu Juli. A study on serum ascitic fluid cholesterol gradient in differentiating cirrhotic and malignancy related ascites. IAIM, 2017; 4(7): 139-143.
25. T. N. Dubey, Shyam Dawane. Diagnostic value of serum ascites lipid gradients in patients with ascites. International Journal of Contemporary Medical Research 2016;3(9):2572-2577.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
15© JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
Study of Pregnancy Induced Hypertension and Associated Factors among women attending delivery service
at Tertiary Care Centre in Gujarat, India
Vaishali N. Vegada1, Hiren N. Makwana2
ABSTRACT:
Background: Hypertensive disorders of pregnancy & their complications are one of the most common cause of maternal morbidity in world. In India the incidence of hypertension is reported to be 8-10% of the pregnancies. The World Health Organization estimates that at least one woman dies every seven minutes from complications of hypertensive disorders of pregnancy. The objective of this study is to assess pregnancy induced hypertension and its associated factors among women attending delivery service at zanana hospital, p.d.u. medical college, Rajkot.
Materials and Methods: Prospective study of 70 cases of hypertension in pregnancy during the period from July 2015 to July 2017.
Aims of study: To study the incidence of hypertension, its complication in pregnancy, factors affecting pregnancy induced hypertension and see how early management can decrease maternal morbidity and mortality.
Results: Regular ANC visits and follow up in patients of pregnancy with hypertension will reduce the morbidity and mortality in nearly 70-75%.
Key words: Pregnancy, Hypertension, Pregnancy Induced Hypertension (PIH), associated factors.
1. Assistant Professor in Dept of Medicine, Pramukhswami Medical College, Karamsad, Anand, Gujarat.2. Assistant Professor in Dept of Medicine, Government Medical College, Surat, Gujarat.
(Corresponding Author), Email: [email protected]
INTRODUCTION:Hypertensive disorders of pregnancy & their complications ranks as one of the major cause of maternal morbidity in the world. It occurs in the women with pre-existing primary or secondary chronic Hypertension. Hypertension in pregnancy is a systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or both. Both systolic and diastolic blood pressure raises are important in the identification of Pregnancy induced hypertension. Pregnancy induced hypertension (PIH) is hypertension that occurs after 20 weeks of gestation in women with previously normal blood pressure. The broad classification of pregnancy-induced hypertension during pregnancy is gestational hypertension, pre-eclampsia and eclampsia.Severe preeclampsia in pregnancy is a systolic blood pressure ≥160 mmHg or diastolic blood pressure ≥110 mmHg or both. Eclampsia is a severe type of pregnancy
induced hypertension, and it happens in about one in 1,600 pregnancies and develops near the end of pregnancy. The three primary characteristics of pregnancy induced hypertension conditions are high blood pressure, protein in the urine and pathologic edema.Pregnancy induced hypertension is a major contributors to maternal and perinatal morbidity and mortality. In the United States, about 15% of maternal deaths are attributable to hypertension,making it the second leading cause of maternal mortality. Severe hypertension increases the mother’s risk of cardiac failure, heart attack, renal failure and cerebral vascular accidents. In addition, the fetus is at increased risk from complications like poor placental transfer of oxygen, growth restriction, preterm birth, placental abruption, stillbirth and neonatal death. Hypertensive disorders represent the most common medical complications of pregnancy with a reported incidence of 5–10%.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
16 © JIMI • JULY - SEPT 2019 • VOL. 13
Globally, preeclampsia is a leading cause of maternal and neonatal mortality and morbidity, predominantly in developing countries. The disorder is usually diagnosed in late pregnancy by the presence of high blood pressure with proteinuria and/or edema. Prevention of any disease process needs awareness of its prevalence, etiology and pathogenesis. The World Health Organization estimates that at least one woman dies every seven minutes from complications of pregnancy induced hypertension disorders. Pregnancy complicated with hypertensive disorder is related with increased risk of adverse fetal, neonatal and maternal outcome.Null parity, multiple pregnancies, history of chronic hypertension, gestational diabetes, fetal malformation, obesity, extreme maternal age (less than 20 or over 40 years), history of PIH in previous pregnancies and chronic diseases like renal disease, diabetes mellitus, cardiac disease, unrecognized chronic hypertension, positive family history of PIH which shows genetic susceptibility, psychological stress, alcohol use, rheumatic arthritis, extreme underweight and overweight, asthma and low level of socioeconomic status are the risk factors for PIH. According to a study in South Africa, the incidence of hypertensive disorders of pregnancy was 12%, and it was the commonest cause of maternal death which contributed 20.7% of maternal deaths.The Federal Ministry of Health has applied multi-pronged approaches to reducing maternal and newborn morbidity and mortality by improving access to and strengthening facility-based maternal and newborn services but the maternal morbidity and mortality due to pregnancy induced hypertension was in an increasing trend.Despite the fact that pregnancy induced hypertension is a leading causes of maternal morbidity and mortality during pregnancy, little is known about the current magnitude of PIH, its associated factors among women attending delivery service in India and specifically in study areas. Therefore, the objective of this study was to assess pregnancy induced hypertension and its associated factors among women attending delivery service at zanana hospital, civil hospital and p.d.u. medical college, Rajkot, Gujarat.MATERIALS AND METHODS:• The present study was conducted in indoor patients at
civil hospital and Zanana Hospital Rajkot.• Study carried out in pregnant patient with hypertension.• All the patients presented with hypertension in
pregnancy/Eclampsia were included in this study.
• Hypertension controlled by antihypertensive drugs like Nifedipine (10mg), Methyldopa (250mg) & Labetalol (100mg ) & convulsion by Mgso4, Heart failure by diuretics monthly.
• Follow up was done in all patients with Hypertension in pregnancy.
• A detailed history with clinical symptoms & signs, vitals, laboratory investigation & diagnosis were recorded in performa. USG findings of increased cortical echogenecity was considered significant.
• In some patients serum electrolytes were done in this study.
• All the patients are examined in detail including clinical medical history and detail cardiovascular & medical examination and they are subjected to neccessory investigations available in government set up
INCLUSION CRITERIA:
1) All the patient who come to outdoor antenatal clinics & indoor patients of civil & zanana hospital, and pregnant patient visiting to medical OPD are included in this study.
2) The pregnant patient > 20 weeks & BP >140mmHg, minimum for 2 frequent time or visit.
3) Patient with past history of gestational hypertension, pre-eclampsia & eclampsia.
4) Pregnant patient who are already on antihypertensive.
5) Patient with hypertension & pre-existing medical illness.
EXCLUSION CRITERIA:
1) Gestational age <20weeks
2) Pregnancy at the age >42 years
OBSERVATION AND RESULTS:
Table No :01
Age Distribution in Hypertension in Pregnancy
Sr. No Age Group No. of Cases
1 <20 3 (5%)
2 20-25 40(57%)
3 26-30 15(21%)
4 >30 12(17%)
TOTAL 70

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
17© JIMI • JULY - SEPT 2019 • VOL. 13
• Table shows the age distribution in pregnant females patients.
• 40(57%) of patients are between the age group of 20-25 years.
• 15(21%) patients are between 26-30 years.
• So, 55(78%) of patients are between 20-30 years.
• It shows that more than 3/4th of the young pregnant hypertensive females are between 20 & 30 years.
• Whereas, 12(17%) patients are above 30 years.
• This indicates the incidence of hypertension remarkably decrease above the age of 30 years.
• Late Pregnancy above 30 years, do not usually are having much risk of developing hypertension.
Table No :02Socioeconomic class in relation to
Hypertension in pregnancy
Socioeconomic class No. of cases
L-Lower 46(65%)
M-Middle 20 (28%)
U-Upper 4(7%)
Total 70
• The Socioeconomic classification is decided according to educational, status, income & percapita Space.
• 46(65%) of patients are of lower Socioeconomic group .
• 20(28%) of patients are of middle Socioeconomic class .
• Whereas 4(7%) of patients are belonging to upper SC group.
• This shows that the incidence of hypertension is in pregnancy is highest in lower socioeconomic group to the extent of 46 (65%) followed by 20 (28%) from middle Socioeconomic group.
• This shows that incidence of hypertension in pregnancy in lower SE group is double than that of middle SE group.
• Only 4(7%) of upper SE group had hypertension during pregnancy.
• This shows that the incidence of hypertension in pregnancy in upper SE group is very less 4(7%) that is < 10% of patients.
• This is because of increased awareness and better antenatal care taken during pregnancy.
Table No :03Residence of the Patient
Sr. No Residence No. of Cases
1 R-Rural 50 (71%)
2 U-Urban 20 (29%)
TOTAL 70
• Table shows the Socioeconomic class of patients of hypertension in pregnancy.
• Table shows the area or residential locality of the patient.
• 50(71%) of the patient are from the rural areas and 20(29%) patients are coming from urban areas.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
18 © JIMI • JULY - SEPT 2019 • VOL. 13
• This indicates that occurrence of hypertension during pregnancy is approx. 70% in rural areas which is very less in urban area.
• This may be due to better health facilities available at urban region.
Table No :04Literacy in Relation to Hypertension in Pregnancy
Sr. No Literacy No. of Cases1 L-Literate 28 (40%)2 I-Illiterate 42 (60%)
TOTAL 70
• Table-04 shows the literacy status of pregnant patient, 42(60%) patient were illiterate & 28(40%) patients were literate.
• This shows that illiteracy in female is a major cause of complications occurring because of hypertension during pregnancy. This reflects high maternal mortality or development of post-partum complications.
Table No :05Parity in Relation to Hypertension in Pregnancy
Sr. No Parity No. of Cases1 PRIMI 37(52%)2 SECOND 17(24%)3 MULTI 16(24%)
TOTAL 70
• Table 06- shows that the incidence of hypertension in term pregnancy are 48(69%) of the young hypertensive pregnant patients.
• That is almost double than the incidence in pre term and post term pregnancy, which is only 22(31%) of the young hypertensive patients.
Table No :07Antenatal visits in Relation to Hypertension in
Pregnancy
Sr. No Antenatal Visit No. of Cases1 <3 VISIT 53 (76%)2 >3 VISIT 17 (24%)
TOTAL 70
• Table -05 shows the parity in relation to development of hypertension in pregnancy.
• 37(52%) young hypertensive pregnant patient were primipara & 17(24%) patients were second para & multipara who develop hypertension.
• Above finding concludes that development of hypertension is almost double in primipara than multipara (or second para). So judicious screening for hypertension is required to prevent maternal complication during pregnancy.
• The incidence of hypertension decreases as the parity increases.
Table No :06Gestational Age in Relation to Hypertension in
Pregnancy
Sr. No Gestational Age (in Weeks)
No. of Cases
1 PRE-TERM (<37WKS) 20 (30%)2 TERM (37-42 WKS) 48 (69%)3 POST-TERM
(>42 WKS)02 (1%)
TOTAL 70

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
19© JIMI • JULY - SEPT 2019 • VOL. 13
• Table -08 shows the clinical presentation of the patient of hypertension in pregnancy.
• 44(31%) patients complain of headache• 28(20%) patients complain of swelling of feet• Whereas giddiness occurs in 21(15%) of the patients• The most common presentation is headache &
swelling of feet in pregnant hypertensive patients.
Table No :09Gestational Age in Relation to Hypertension in
Pregnancy
Sr. No Severity of Hypertension No. of Cases
1 SBP-140-159mmHg DBP-90-109mmHg
43(62%)
2 SBP->160mmHg DBP->110mmHg
27(38%)
TOTAL 70
• Table 09-shows mild hypertension (SBP-140 to 159mmhg) and (DBP 90 to 109 mmhg).
• It occurs in 43(62%) of the patients, it is more common and almost 1.5 times more common than severe hypertension.
Table No :10Relation of Albuminuria with Hypertension in Pregnancy
Sr. No Urine Albumin No. of Cases
1 NIL 14(20%)
2 TRACE 07(10%)
3 +1 21(30%)4 +2 15(21%)5 +3 13(19%)
TOTAL 70
• Table -05 shows the parity in relation to development Table -07 shows the development of occurrence of hypertension in relation to visits to antenatal clinic.
• If patient is irregular in ANC visit of less than 3, 53(76%) develops hypertension during any stage of their pregnancy and if patient is regularly visiting to ANC 17(24%) patients had developed hypertension.
• This shows that the development of hypertension almost approximately 2.5-3 times higher in pregnant patients those who are not regularly visiting to ANC.
• This also shows that regular visit to ANC, will held early screening of hypertension and maternal mortality in young pregnant hypertensive patients.
Table No :08Presenting Complain in Cases of Hypertension in Pregnancy
Sr. No Presenting Complain No. of Cases1 Headache 44 (31%)2 Swelling of Feet 28 (20%)3 Giddiness 21 (15%)4 Epigastric Pain 18 (12%)5 Vomitting 16 (12%)6 Brethlessness 05 (4%)7 Decreased Urine Output 05 (4%)8 Blurring of Vision 04 (2%)9 Convulsion 01
10 Bleeding 01

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
20 © JIMI • JULY - SEPT 2019 • VOL. 13
• Table 10-shows almost 2/3rd patients of young hypertensive pregnancy 42(60%) had non significant albuminuria.
• And only 28(40%) patients had significant albuminuria.
Table No :11Relation of Maternal Complication to Hypertension
Sr. No Maternal Complication No. of Cases
1 SEPTICEMIA 07 (10%)
2 ACUTE RENAL FAILURE 06 (8.5%)
3 ECLAMPSIA 04 (5.7%)
4 HEART FAILURE 02
5 HTN RETIOPATHY 02
6 DIC 01
7 NO COMPLICATION 49TOTAL 70
• Table 11-shows the complications of hypertension came across are:
• Septicemia 07(10%).• Acute renal failure 06 (8.5%).• Eclampsia 04(5.7%).
• The other complications like heart failure, hypertensive retinopathy and DIC are rare.
• But majority of the young hypertensive pregnant patients 49(70%) cases usually do not have any maternal complications.
Table No :12Effect of follow up on Hypertension in Pregnancy
Sr. No FOLLOW UP No. of Cases
1 R-REGULAR 27(38%)
2 I-IRREGULAR 43(62%)
TOTAL 70
• Table 12-shows those who are under regular follow up 27(38%) has good antenatal and peri partum period.
DISCUSSION:
The present clinical study of “Study of Pregnancy Induced Hypertension and Associated Factors among women attending delivery service at tertiary care centre in Gujarat, India”, 70 Cases was carried out at Civil Hospital and Zanana hospital, Rajkot during period of July 2015 to July 2017 with following discussion.
1) A Similar clinical study to determine the incidence of hypertension related to parity, in BMC-RI AT Banglore by proff.Bharathi K.N.
Total women of hypertension in pregnancy:- 904
Primigravida:- 20.9% had hypertension
Multigravida:- 15.4% had hypertension
Gravida Study in Banglore
Our study
Primigravida 20.9% 52%Multigravida 15.4% 24%

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
21© JIMI • JULY - SEPT 2019 • VOL. 13
In our clinical study, the incidence of primigravida is 52% and 24% in muligravida.
Here in our clinical study, both the incidence are increased as compared to study conducted in south, this could be explained on the basis of increased salt intake, relative less health awareness and less awareness regarding hypertension in ANC period. And our patient are selected randomly, irrespective of their socioeconomic status.
2) A case control study was carried out in the dept. of OBGY in King George Hospital, Andhra Pradesh.
LITERACY Total cases in AP
Total cases in our study
Literate 13(26%) 28(40%)Illiterate 37(74%) 42(60%)
Table shows that study carried out in hospital Andhra pradesh, the literacy rate is 26% and in our study literacy rate is 40%. The incidence of hypertension during pregnancy in literate person is higher in present clinical study than in King George Hospital, it is 26% of literate patient, whereas the present study 40% in literate patient. Whereas incidence in illiterate patient is 74% in king George hospital, where as it is 60% in our study. All over incidence of hypertension is higher in illiterate patients in both studies
In same region socioeconomic status in patient of hypertension in pregnancy was carried out. The incidence of pregnancy induced hypertension is 22% in upper SEC and 68% in lower SEC group in King George Hospital, Andhra Pradesh. Whereas in our study incidence is 35% in upper SEC and 65% in lower SEC group.
In both studies, the incidence of pregnancy induced hypertension is higher in lower SEC group of patients.
Socioeconomic status
In Andhra Pradesh
In our study
Upper SEC (APL)
11(22%) 24(35%)
Lower SEC (BPL)
39(68%) 46(65%)
3) A study by Zenebe wolbe(2010) residential area of the mothers (rural/urban) was found to have statistically significant association with occurence of hypertension in pregnancy.
Area Zenebe wolbe study
Our study
Rural 74.7% 71%Urban 26% 29%
In Zenebe wolbe study, the incidence of hypertension in rural patient was 74.7%, whereas in present clinical study 71% which is almost comparable. Also in urban 20% in Zenebe wolbe study, whereas in present study it is 29%, which is also almost comparable. So incidence of PIH is higher in rural area as compared to urban area.
4) A study by Teklu S Gayus et al (2006) in Addis (Tinkur hospital) showed that more than 78% cases had mild hypertension and 22% cases had severe hypertension and 1.99% patient had complication like eclampsia and 40% patients had other complication.
Hypertension in pregnancy
Teklu study Our study
Mild Hyertension 78% 62%Severe Hypertension 22% 38%
Complication Teklu study Our studyEclampsia 1.99% 5.71%Other 40% 30%
The study carried out in Tinkur al et, the mild hypertension occur in 78% ,where as in present clinical study it is 62%, where as severe hypertension occurred in 22% in Tinkur At el and in present study it is 38% which is explained on the basis of high occurence of hypertension in this region.
The complication in Teklu study, eclampsia occurred in 1.99% of patients, where as in present clinical study it is 5.71% of patients.This is high because of (1)taking less care during antenatal period (2)defaulter in taking medications (3)less care in dietery modification because of dietery taboos during pregnancy(routinely advised more ghee and salt during pregnancy),which may be one of the major factor that increases the complications.
The other complications like hypertensive retinopathy, acute renal failure and heart failure occurred in 40% in Teklu study and 30% in present study, it is almost comparable.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
22 © JIMI • JULY - SEPT 2019 • VOL. 13
CONCLUSION:
We have done a prospective observation study of “Study of Pregnancy Induced Hypertension and Associated Factors among women attending delivery service at tertiary care centre in Gujarat, India” at civil Hospital & zanana hospital, Rajkot during the period of July 2015 to July 2017.
Clinical profile of hypertension in pregnancy can be affected by factors as follow:-
1) Age group:- Hypertension common in younger age group between 20-25 years of age, which is about 57% of total cases.
2) Socioeconomic class:- Hypertension common in the women belonging to lower socioeconomic class, which is 65% of total cases.
3) Residence:- Hypertension is common in the women belonging to rural area, which is 71% of total cases.
4) Literacy:- Hypertension is common in illiterate women, which is 60% of total cases.
5) Parity:- Incidence of hypertension common in primigravida group, which is 52% of total cases.
6) Gestational age:- Incidence of hypertension was more in term pregnancy than preterm & post-term, which is 69% in term pregnancy.
7) Antenatal visits:- Incidence of hypertension was more in the women who had less antenatal follow up,76% of cases had less than 3 antenatal visits.
8) Severity of Hypertension:- Majority of women were suffering from mild hypertension, which is 62% of total cases.
9) Maternal complication:- Maternal complications were less in the women who had adequate , regular treatment & follow up, about 70% cases had no any maternal complication related to hypertension.
From our study, we concluded that, with early detection of Hypertension, timely treatment & regular follow up can improve maternal morbidity & decrease the incidence of hypertension & prevention of complication related to Hypertension.
REFERENCES:
1. Geographic variation in the incidence of hypertension in pregnancy. Am J. Obstet Gynecol 1988;158:80-3. World health organization International collaborative study of Hypertensive Disorder of Pregnancy.
2. Hypertensive disorder in pregnancy; F Gary Cunningham ,Keneth J Leveno, Steven L. Bloom, John C. Hauth, Larry Gilstrap III, Katharine D. Wenstrom(eds), Williams obstetrics,22nd ed, New York,2005:761-809.
3. Kar J Srivastava k ,Mishra R K, Sharma N, Pandey O N, Gupta S-J Obestet. Gynecol.India2002:52(2):39-42
4. Seon Ac Yeo,RNC, PhD, Pamella J Wells, MSN:Edith C.Kieffer, PhD:George.H. Nolan MD, MP. Preeclampsia among Hispanic women in Detroit health system ,Ethnicity and disease,Vol 17. Winter 2007Pp118
5. Indian Council of Medical Research women and health (1992)
6. Reingardiene D Pregnancy induced hypertension related complication medicine 2003 Mar 14:39 (12) ;1244-52
7. Lee CJ , Hsieh TT , Chiu TH,Chen KC,Lo LM, Hung TH. Risk factor for pre-eclampsia in an Asian population.Int J Gynaecol.Obstet.2000;70:327-33.(PubMed)
8. Eskenzi B, Fenster L, Sidney S. A multivariate analysis of risk factor for hypertension in pregnancy JAMA, 1991; 266-237-41.(PubMed).
9. Mohmad K, Williams MA Woelk GB, Jenkins-Woelk L, Mudzamiri S : Risk factor for hypertension in pregnancy among Zimbabwean women:Recurrence risk and familial tendency towards hypertension. J Obstet Gynaecol.1998:18:218-22.(PubMed).
10. Lowdermilk DL. Perry ES, Boback MI.Maternity and Womens Health care.6th ed.Edinburgh:Mosby:2000.
11. Shenoy K Pregnancy in women.JAMA 2004Feb 12:30 (12):7-8.
12. Government of India- Goals and targets for Maternal and Child Health under various National and International commitments. PARK’S Text book of preventive and social medicine.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
23© JIMI • JULY - SEPT 2019 • VOL. 13
13. Chang J Elams-Evans LD,Berg CJ,Herndon J, Flowers L. Seed KA,Et Al. Pregnancy related mortality surveillance –United states, 1991-1999. MMWR Surveill sum Feb 21 2003:52(2):1-8
14. Kumar S Ganesh B. Unnikrishnan , k. Nagaraj and Jayaram ,Et Al:Determinants of hypertension in pregnancy. A case-control study in a District Hospital. Indian J Community Med 2010 oct-Dec; 35(4): 502 505 doi: A 10.4103/0970-0218.74360.
15. Teklu S Gaym A. Prevalence and clinical correlates of the hypertensive disorders of pregnancy at Tikur Anbessa Hospital,Addis Ababa,Ethiopia,Ethiop Med J,2006 Jan:44(1): 18-26.
16. Dr.OlumideOjodun and Prof. PJT De Villiers, Et Al: The prevalence complications of pregnancy in Dora Nginza Hospital, Port Elizabeth, Eastern Cape.
17. Cronje G, Grobler CJF, Chronic and gestational hypertension. Obstetrics in Southern Africa. 2nd ed.2003;58:489-512.
18. Assis TR, Viana FP. Study on major maternal risk factors in hypertensive syndrome. Arq Bras cardiol 2008;91:11-17.
19. Majhi AK, Mondal A, Mukherjee G G. Maternal Mortality associated with pregnancy. India Journal of Medical Associations 2001 Mar 4:99(3):132-7
20. Vidyadhar B Bangal , Purushottam A. Giri, Aditi S.Mahajan,Et al:Maternal and Foetal outcome in pregnancy induced hypertension: A study from rural tertiary care teaching hospital in India.
21. Helena Salonen Ros,Sven Cnattinguis, and loren lipworth,Et al.Comparison of risk factors for hypertension in pregnancy and gestational hypertension in apopulation based cohort study.
22. Indian Council of Medical Research studies-Women and Child Health.
23. Zhang Zeisler and Berkowits(1999),et al: Epidemiological Investigations of hypertension in pregnancy.
24. Bodole, Fetal growth associations with maternal artey intake hemoglobin and antenatal care in reral area. Journal of Indian Obstetrics and Gynaecology;1992.vol (42).
25. Zenebe Wolde, Hailemariam segni, Mirkuzie Woldie,Et al: Hypertensive disorders of pregnancy in Jimma University specialized Hospital.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
24 © JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
Role of Human Papilloma Virus in Head and Neck Carcinoma
ABSTRACT:Background: The aim of our study was to prospectively evaluate the association of tumor hpv status with response to treatment in patients with hnscc.
Material & Method: A prospective study was conducted, from june 2010 to june 2011. 53 patients suffering from hnscc were included mainly of the site of oral cavity & oropharynx, and were advised a combination treatment of chemotherapy and radiotherapy. the tissue collected from patients through punch biopsy and, were processed by rt-pcr technique for hpv status.
Results: Out of 53 patient 6(11.32%) were hpv positive. four(21.1%) cases of oropharyngeal tumor, and 2(5.9%) cases of oral cavity tumor were hpv positive. 50% of hpv positive patient had smoking as the onlyhabit,33% hpv positive patient had all three habit(smoking,tobacco,alcohol), and 16% hpv positive patient had 2 habits(smoking,tobacco).as for treatment response to chemo-radiation 66% of hpv positive patient have complete response and 33% hpv positive patient have partial response.
Conclusion: The tumorigenic potential of hpv in hnscc is now evident in many prospective & retrospective studies. hnscc is a multifactorial disease,to know interaction between hpv& other risk factor and their effect on treatment, need furthur large group study.the association of tumor hpv status with better response to treatment consistent with prior studies reflect that hpv status should be considered in the design and analysis of current and future clinical trials for treatment of head and neck cancer patients
Keywords: head & neck carcinoma, human papilloma virus, risk factors, chemo-radiotherapy, treatment response.
1. Department of Clinical Oncology, Delhi State Cancer Institute
2, 3, 4, 5. Department of Clinical Oncology, Delhi State Cancer Institute
6. Department of Clinical Oncology, Delhi State Cancer Institute
(Corresponding Author) Email: [email protected]
Afsana Shah1, Deepak K Mittal2, Gowhar Ahmad Shigan3, Nihar Kant Ajena4, Dinesh Kumar5, Pragya Shukla6
INTRODUCTION:
Most HNSCCs arise in the epithelial lining of the oral cavity, oropharynx, larynx, and hypopharynx (1, 2). About 90% of all head and neck cancers are squamous cell carcinomas (HNSCC). The incidence of HNSCC has been gradually increasing over the last 3 decades (3), making it the sixth leading cancer by incidence worldwide. The annual incidence of head and neck cancers worldwide is more than 550,000 cases with around 300,000 deaths each year (4). Overall 57.5% of global Head & neck cancers reported from Asia, especially in India (5). HNSCC disproportionality affects male population and male to female ratio ranges from 2:1 to 4:1.
These cancers are strongly associated with certain environmental and lifestyle risk factors such as tobacco and alcohol consumption. Tobacco use alone has been linked to eighty-five percent of head and neck cancers & the risk of developing these cancers is more in people consuming both than those who use either tobacco or alcohol alone (6).
It is widely accepted that HPV infection is a risk factor for cervical cancer (7). The similarity of the morphologic features of genital and oral HPV-associated lesions was one of the early findings that raised the possibility that HPV might be associated with oral and laryngeal squamous-cell carcinomas (8,9).
Human papillomavirus (HPV) is a circular, double-stranded DNA virus. More than 100 unique HPV types are known, but these different types are generally divided into those with a predilection to infect the skin versus mucosal surfaces (10). Mucosal HPV infections are well known to associate with a spectrum of human diseases from benign papillomas (or warts) to invasive carcinomas including

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
25© JIMI • JULY - SEPT 2019 • VOL. 13
cervical, vulvar, vaginal, anal, penile, and more recently head and neck squamous cell carcinoma (3,7,11). Until recently, however, the role of HPV in the pathogenesis of head and neck squamous-cell carcinoma has been uncertain, mainly because detection of HPV DNA has been highly variable, with rates ranging from 0 to 100% (12). Our study is one such effort to find the association of Human papilloma virus with head and neck carcinoma & treatment response in the context of definitive (CTRT) chemo-radiotherapy.
MATERIAL & METHODS:
A prospective study was conducted, from June 2010 to June 2011. 53 patients, suffering from HNSCC were included, mainly of the region of oral cavity and oropharynx, which were confirmed by histopathological examinations. All cases were advised combination treatment of chemotherapy and radiotherapy. The tissue collected from patients through punch biopsy. The samples were processed by Real-time polymerase reaction (RT-PCR) technique for HPV status.
All the patient included in the study belonged to the same ethnic group (Indo-European community) of North India based on geographical location and linguistic basis.
Informed consents of the patients were obtained before inclusion in the study. All study subjects completed a questionnaire covering medical, residential and occupational history. Information pertaining to dietary habits, family history of cancer, smoking, tobacco chewing and alcohol drinking was also obtained.
INCLUSION CRITERIA:
We included newly diagnosed cases of histologically proven head & neck squamous cell carcinoma, from age group 20-70 years with karnofsky performance status (KPS) > 70 and with normal liver, renal, cardiac, CNS, lung function and normal hematologic & biochemical parameters with no second malignancy and planned for definitive CT+RT.
EXCLUSION CRITERIA:
Patients with any concurrent systemic illness, any other malignancy, having distant metastasis, KPS< 70 and with prior chemotherapy or radiotherapy were excluded.
THE FOLLOWING TREATMENT DESIGN WAS ADOPTED:
The Presenting history & chief complaints were taken with a special inquiry about, history of a predisposing factor. Patient’s local, general & systemic examination done.
After initial workup patients underwent work-up to assess the extent of primary malignancy and to rule out secondary malignancy and metastasis (chest X-ray, CT head & neck, MRI & PET). Patients staged according to TNM staging (AJCC 2002). The sample was collected from patients through punch biopsy. The HPV status was assessed by RT-PCR technique. Treatment consisted of definitive concurrent chemo-radiotherapy. All patients received external beam radiotherapy 70 Gy in 35 fractions by 2 fields in 2 phases delivered using the cobalt-60 unit, with weekly cisplatin 35mg/m2. The response was categorized as complete response, partial response or no response based on WHO assessment criteria after 1 month of completion of treatment. Weekly follow-up during treatment, monthly thereafter, & routine investigations were done to assess the radiation & systemic toxicity according to RTOG Toxicity criteria & NCI-CTC, criteria. Adverse effects were managed symptomatically. The treatment was stopped in the patient showing toxicity grade 3 & 4, treatment started again after toxicity decreased by at least grade 2. Patients, who defaulted, were taken out of the study.
RESULTS:
The results are discussed and shown in table 1, with reference to the site of involvement, age of presentation, stage at presentation, demographic distribution, association of use of tobacco and alcohol with head and neck carcinoma, association of HPV status and tobacco and alcohol use and finally association of HPV status and response to treatment
Out of 53 patients, 6(11.32%) were HPV positive. In <60year age group 4(10.8%) were HPV positive and in >60year age group 2(12.5%) were HPV positive. All 6 HPV positive patients were male. 4 (21.1%) cases of the oropharyngeal tumor were HPV positive, and 2(5.9%) cases of oral cavity tumor were HPV positive which was found to be statistically significant. In respect of stage, 4(15.4%) HPV positive tumor were of stage 4 and 2(9.1%) HPV positive tumor were stage 2. According to HPE differentiation, 50% of the poorly differentiated tumor were HPV positive, 8.7% were well differentiated, and 7.7% were moderately differentiated. 50% of HPV positive patient had smoke as the only habit,33% HPV positive patient had all three habit (smoking, tobacco, alcohol), and 16% HPV positive patient had two habits (smoking, tobacco). As for treatment response to chemo-radiation, 66% of HPV positive patient has complete response (100% for who had 1 or 2 habits) and 33% HPV positive patient have partial response (100% who had more than 2 habits).
JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
26 © JIMI • JULY - SEPT 2019 • VOL. 13
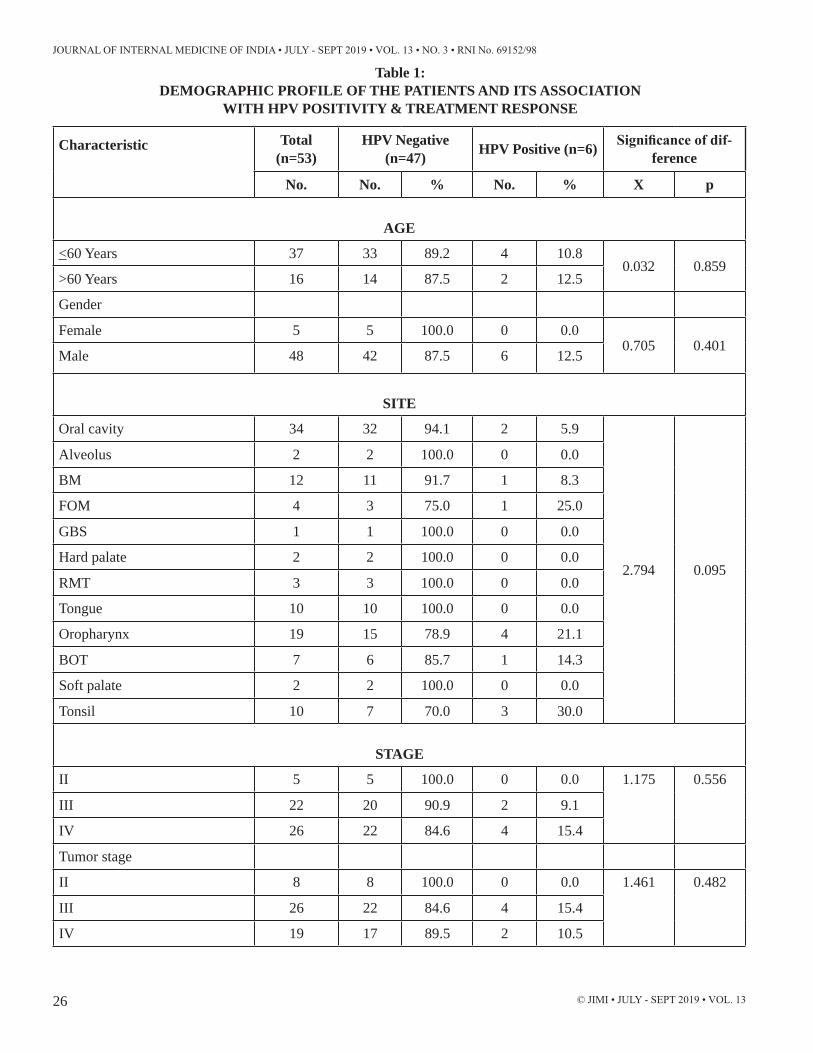
Table 1: DEMOGRAPHIC PROFILE OF THE PATIENTS AND ITS ASSOCIATION
WITH HPV POSITIVITY & TREATMENT RESPONSE
Characteristic Total (n=53)
HPV Negative (n=47) HPV Positive (n=6) Significance of dif-
ference
No. No. % No. % X p
AGE
<60 Years 37 33 89.2 4 10.80.032 0.859
>60 Years 16 14 87.5 2 12.5
Gender
Female 5 5 100.0 0 0.00.705 0.401
Male 48 42 87.5 6 12.5
SITE
Oral cavity 34 32 94.1 2 5.9
2.794 0.095
Alveolus 2 2 100.0 0 0.0
BM 12 11 91.7 1 8.3
FOM 4 3 75.0 1 25.0
GBS 1 1 100.0 0 0.0
Hard palate 2 2 100.0 0 0.0
RMT 3 3 100.0 0 0.0
Tongue 10 10 100.0 0 0.0
Oropharynx 19 15 78.9 4 21.1
BOT 7 6 85.7 1 14.3
Soft palate 2 2 100.0 0 0.0
Tonsil 10 7 70.0 3 30.0
STAGE
II 5 5 100.0 0 0.0 1.175 0.556
III 22 20 90.9 2 9.1
IV 26 22 84.6 4 15.4
Tumor stage
II 8 8 100.0 0 0.0 1.461 0.482
III 26 22 84.6 4 15.4
IV 19 17 89.5 2 10.5

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
27© JIMI • JULY - SEPT 2019 • VOL. 13
NODAL STATUS
0 14 13 92.9 1 7.1 0.596 0.897
1 25 22 88.0 3 12.0
2 13 11 84.6 2 15.4
3 1 1 100.0 0 0.0
HPE
WD 23 21 91.3 2 8.7
6.460 0.091MD 26 24 92.3 2 7.7
PD 2 1 50.0 1 50.0
Verrucous 2 1 50.0 1 50.0
HABITS
No habit 2 2 100.0 0 0.0
4.481 0.482
Smoking only 12 9 75.0 3 25.0
Tobacco only 10 10 100.0 0 0.0
Smoking + Tobacco 14 13 92.9 1 7.1
Tobacco + Alcohol 2 2 100.0 0 0.0
All three 13 11 84.6 2 15.4
No habit 2 2 100.0 0 0.0
TREATMENT RESPONSE
CR 21 17 81.0 4 19.0
2.249 0.325PR 25 23 92.0 2 8.0
NR 6 6 100.0 0 0.0
DISCUSSION:
The aim of our study was to prospectively evaluate the association of tumor HPV status with response to treatment in patients with HNSCC. Accumulating evidence suggests that HPV positive (+) status is an important prognostic factor associated with a favorable outcome in head and neck cancers (13-17). In a recent prospective multi-center clinical study demonstrated that patients with HPV+ tumors had better response rates after induction chemotherapy (82% vs. 55%), and after chemoradiation treatment (84% vs. 57%) compared to patients with HPV negative (-) tumors (18). Similarly, our study also showed a trend towards improved treatment outcome for patients with HPV positive tumors.
Numerous studies have shown HPV positive and HPV negative HNSCC are two different entities with different risk factors, demographic variables and tumor
characteristics (19).
HPV-positive tumors were more likely than HPV-negative tumors to arise from the oropharynx, to be poorly differentiated, and to have basaloid features. Additionally, patients with HPV-positive tumors had less cumulative exposure to multiple risk factors (tobacco chewing, alcohol, smoking). In our study also we have found a similar trend.
The proportion of oropharynx cancers attributable to HPV infection is variable in different studies. The International Agency on Treatment of Cancer (IARC) Multicenter Study estimated that 18% of the oropharynx and 3.9% of oral cavity (20) cancers worldwide are HPV associated. In a separate IARC literature summary, this proportion was estimated to be 38%, and that study found that oropharynx cancer patients in North America were more likely than those in Europe to be HPV positive (47%

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
28 © JIMI • JULY - SEPT 2019 • VOL. 13
vs. 28%) (21). These studies have also shown (19,20,21), that the overwhelming majority (~ 95%) of HPV-positive tumors were HPV16 positive. In our study also we have found that out of 19 patients of oropharynx 4 (21.1%) are positive for HPV, & out of 34 patients of oral cavity 2 (5.9%) are positive for HPV.
D’Souza and colleagues present data suggesting that smoking and alcohol uses, which are important risk factors for oropharyngeal cancer, may not act as cofactors in HPV mediated carcinogenesis in the oropharynx (22).
Another study examined the synergistic effect of the HPV Virus-like particle (VLP) serology and smoking (23), and reported an additive effect of smoking and alcohol with HPV VLP serology.
Our study showed a trend that if multiple risk factors are present, treatment outcome might be grave even if HPV status is positive. However, we found no evidence in our statistical analysis that the association of tumor HPV status with treatment response could be attributed to confounding by tobacco use.
Additional variables of potential prognostic importance, such as TNM stage, HPE differentiation, Age, and sex may be associated with tumor HPV status. But the small sample size limited the number of variables that could be discussed in our study. Hence, factors not discussed in our study may be important.
The association of tumor HPV status with treatment response observed in our study showed a trend of better treatment outcome, consistent with prior studies, and reflect that HPV status should be considered in the design and analysis of current and future clinical trials of treatments for head and neck cancer patients.
CONCLUSION
The tumorigenic potential of HPV in HNSCC is now evident in many prospective and retrospective studies. Although a viral association within a subset of HNSCC has been shown, the molecular and histopathological characteristics of these tumors have yet to be clearly defined. Evidence supports the idea that HNSCC is a multifactorial disease with at least two, possibly distinct, pathways, one driven by smoking and alcohol consumption, and another driven by HPV. There have been several studies in which HPV infection and smoking are not mutually exclusive. Others and we have observed that HNSCC from smokers may contain transcriptionally active HPV. Further studies are warranted for a clearer definition of whether these tumors may have developed due to the interactions between these two risk factors &
to see the treatment response if multiple risk factors are present.
The association of tumor HPV status with better response to treatment observed in our study is consistent with prior studies and reflect that HPV status should be considered in the design and analysis of current and future clinical trials for the treatment of head and neck cancer patients.
REFERENCES:
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin.;57(1): 43-66.
2. Boyle P and Bernard Levin. World Cancer Report 2008. International Agency for Research on Cancer.
3. Parkin DM, Bray F: Chapter 2: The burden of HPV-related cancers. Vaccine 2006, 24 (Suppl 3):11-25.
4. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61(2):69-90.
5. Chaturvedi P.Head & neck surgery.J Can Res Ther 2009; 5:143
6. Sankaranarayanan R, Masuyer E, Swaminathan R, Ferlay J, Whelan S. Head and neck cancer: a global perspective on epidemiology and survival. Anticancer Res 1998;18:4779–86.
7. Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer 2002;2:342-350.
8. Syrjänen K, Syrjänen S, Pyrhönen S. Human papilloma virus (HPV) antigens in lesions of laryngeal squamous cell carcinomas. ORL J Otorhinolaryngol Relat Spec 1982;44:323-334.
9. Syrjänen K, Syrjänen S, Lamberg M, Pyrhönen S, Nuutinen J. Morphological and immunohistochemical evidence suggesting human papillomavirus (HPV) involvement in oral squamous cell carcinogenesis. Int J Oral Surg 1983;12:418-424.
10. McLaughlin-Drubin ME, Munger K. Oncogenic activities of human papillomaviruses. Virus Res 2009;143:195–208.
11. De Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen Classification of papillomaviruses.Virology 2004;324:17–27.
12. Syrjänen KJ, Syrjänen SM. Papillomavirus infections in human pathology. New York: John Wiley, 2000.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
29© JIMI • JULY - SEPT 2019 • VOL. 13
13. Mellin H, et al.: Human papillomavirus type 16 is episomal and a high viral load may be correlated to better prognosis in tonsillar cancer. Int J Cancer 2002, 102(2):152-8.
14. Weinberger PM, et al.: Molecular classification identifies a subset of human papillomavirus-associated oropharyngeal cancers with favorable prognosis. J Clin Oncol 2006, 24(5):736-47.
15. Licitra L, et al.: High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J Clin Oncol 2006, 24(36):5630-6.
16. Gillison ML, et al.: Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 2000, 92(9):709-20.
17. Schwartz SR, et al.: Human papillomavirus infection and survival in oral squamous cell cancer: a population-based study. Otolaryngol Head Neck Surg 2001, 125(1):1-9.
18. Fakhry C, et al.: Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 2008, 100(4):261-9.
19. Kumar B, EGFR, p16, HPV Titer, Bcl-xL and p53, sex, and smoking as indicators of response to therapy and survival in oropharyngeal cancer. J Clin Oncol. 2008 Jul 1;26(19):3128-37.
20. Herrero R, Castellsague X, Pawlita M, et al. Human papillomavirus and oral cancer: the International Agency for Research on Cancer multicenter study. J Natl Cancer Inst 2003;95:1772-1783.
21. Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev 2005; 14:467-475.
22. D’Souza G, et al.: Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 2007, 356(19):1944-56.
23. Schwartz SM, Daling JR, Doody DR, Wipf GC, Carter JJ, Madeleine MM, et al. (1998). Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst 90:1626-1636.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
30 © JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
A Correlation of Mean Platelet Volume (MPV) and Red Cell Distribution Width (RDW) in Type 2 Diabetic Patients in a
Tertiary Care Center of Northern India
ABSTRACT:Objective: To study the Mean Platelet Volume (MPV) and Red Distribution Width (RDW) in type 2 diabetic patients(T2DM), in comparison with non-diabetic healthy controls. This study is novel in our environment and will serve as a foundation for other researchers in this field.Methods: This case control study included 146 T2DM patients and 156 healthy control subjects. Sex, age, weight, height, blood pressure, complete blood count, fasting plasma glucose, hemoglobin A1c (A1C), and lipid profile were done for all of the study population. For diabetic patients, data on duration of diabetes were also included.Results: A positive correlation between MPV with HbA1c ( R2 value 0.304) and MPV with FPG (R2value 0.623) was found among diabetic subgroup which was statistically significant. Also RDW with HbA1c (R2 value -0.289) and RDW with FPG (R2 value 0.481) were found to be statistically significant (p<0.05). The strongest correlation between RDW and MPV was with FPG followed by A1C.Conclusion: RDW which is recently considered as an inflammatory marker with a significant predictive value of mortality is higher in T2DM patients than healthy subjects and is particularly higher in uncontrolled hyperglycemia. Hence, to conclude a simple, low cost, easily available test in T2DM patients can asses control of hyperglycemia and it’s complications. Keywords: Red cell distribution width, Mean platelet volume, T2DM, Inflammation
1. Associate Professor, Medicine MLN Medical College, Prayagraj (UP) (Corresponding Author) E-mail: [email protected]
2. Consultant Psychiatry, MLN Medical College, Prayagraj (UP)
2. Department of Medicine MLN Medical College, Prayagraj (UP)
Anubha Srivastava1, Anurag Varma2, Rajneesh Tiwari3
INTRODUCTION:
T2DM patients have an increased risk of developing micro- and macro vascular disease. The increased platelet activity is emphasized to play a role in the development of vascular complications of diabetes1,2. RDW, defined as the heterogeneity of circulating erythrocytes (anisocytosis), was used to distinguish the variable pathogenesis of anemia together with the MPV. RDW is considered to be an inflammatory marker in certain conditions3,4 with an association between RDW and cardiovascular diseases, ESRD, stroke and celiac disease 5,6
A significant association between higher MPV and increased incidence of cardiovascular events and risk factors like diabetes mellitus, obesity, and metabolic
syndrome has been described in literature7-11. RDW is considered as a prognostic marker which may reflect an underlying inflammatory process. It is calculated by both impedance and flow cystometric analysers as a part of routine complete blood count analysis.
This study aimed to compare RDW and MPV values of the patients with diabetes to normal population. This study was an observational case-control study. Ethical Committee approval was taken from Institutional Ethics Committee. The study was conducted in the Department of Medicine, MLN Medical College and SRN Hospital, Prayagraj (formerly Allahabad) from Jan 2017 to June 2018.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
31© JIMI • JULY - SEPT 2019 • VOL. 13
Figure 1 : Comparison of mean FPG in between cases and controls
Figure 2 : Comparison of mean HbA1c between cases and controls
Figure 3 : Scatter plot (MPV and FPG)
MATERIALS & METHODS:
Patients aged 18-70 years who were diagnosed as T2DM as per ADA 2019 were included in this study with healthy controls.
All patients with known Heart Disease, Chronic liver disease, Chronic renal failure, Hypothyroidism, Malignancy, Secondary hypertension, Anaemia (haemoglobin <10g/dl), Medication affecting platelet volume, (eg Isotretinoin, Statin) were excluded from the study.
Patients underwent a morning fasting glucose estimation. (after 8 hours of fasting) along with A1C with fasting lipid profile. Blood pressure and weight was recorded with Waist circumference (measured at midway between lower thoracic bony cage and brim of iliac crest ) as per the protocol for Diabetes patients in our institute.
After obtaining written informed consent, patient qualifying inclusion criteria were included in the study. Demographic data was recorded and subjects were interviewed about medical history, education, family medical history, and intake of medications.
Anthropometric Measures like Weight, height, body mass index (BMI), and waist circumferences were measured.
The data was entered in MS EXCEL spreadsheet and analysis was done using Statistical Package for Social Sciences (SPSS) version 19.
RESULTS & CONCLUSIONS:
145 Cases and 156 age and sex matched controls were included in our study.
The FPG amongst the cases were 114.5+_12.45 mg/dl as compared to controls 90.25+_ 7.5 mg/dl and A1C was 6.29+_0.88 % as compared to controls 5.34+_ 0.41. Figure 1 shows the comparison of mean FPG in between cases and controls which was 114.55±12.45 mmHg in case group and 90.25± 7.50 mmHg in control group and this was statistically significant (p <0.05). Figure 2 shows the comparison of mean A1C between cases and controls. The mean A1C in case group was 6.29 ±0.88 mmHg and in control group was 5.34 ±0.41 mmHg which was statistically significant (p <0.05). Figure 3 shows the correlation of MPV and FPG which shows a positive correlation between FPG and MPV with R2 value 0.623 which is statistically significant ( p<0.5 ). Figure 4 shows correlation of MPV and A1C and there is weak positive correlation between A1C and MPV with R2 value 0.304
which is statistically significant (p<0.5). Figure 5 shows Scatter Plot diagram of RDW & A1C which shows a weak positive correlation between A1C and RDW with R2 value 0.289 and is statistically significant ( p<0.5 ). Figure 6 shows correlation between RDW and FPG and there is positive correlation between FPG and RDW with R2 value 0.481 which is statistically significant ( p<0.5 ).

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
32 © JIMI • JULY - SEPT 2019 • VOL. 13
DISCUSSION:
Red cell distribution width is considered as a prognostic marker which may reflect an underlying inflammatory process. The MPV is a marker of platelet size that is easily determined on routine automated hemograms and routinely available at low cost. Subjects with a higher MPV have large platelets that are metabolically and enzymatically more active and have greater prothrombotic potential than small platelets.
In this study out of 145 cases maximum study subjects were in between 41-50 years of age. In the case groups there were 77 males and 68 females whereas in the control groups there were 99 males and 57 females. In the cases male : female ratio was 1.13 : 1 and male : female ratio was 1.7 : 1 in controls. In cases the mean age of males and females were 43.53 ± 11.06 and 43.976±11.97 years respectively, which was statistically not significant (p value >0.05). In the present study, higher RDW in T2DM patients than healthy controls (P=0.008) indicates the presence of anisocytosis, which is related to impairment of erythropoiesis and degradation of erythrocytes by fragmentation or agglutination.9,10 This occurs in the presence of chronic inflammation and increased level of oxidative stress.11
Nada et al.12 have also shown that RDW was significantly higher in diabetic patients than healthy controls (P=0.008) Comparing patients with A1C ≤7% (47 patients) and with A1C >7% (213 patients) showed higher RDW (P=0.035) that is similar to our study. Most of the studies shows significant correlation of RDW and MPV with underlying inflammatory condition as found in our study too, this provides a low cost easily available test to help prevent microvascular complications of Diabetes which is rampant and rapidly increasing all over India and the whole world.
Jaman et al13 in his study included 87 T2DM patients, which divided into two groups, A (n=41, presence in diabetics≤6.5-6.9%) and B (n=46, target in diabetes≥7.0%), according to A1C values. Spearsman correlation co-efficient were calculated to evaluate the relationship between RBC count, MCHC, RDW with random blood sugar (RBS) and PCV, MCV, MCHC with A1C value. Binominal logistic regression analysis was performed to estimate the relationship between glycemic control, as dichotomous outcome of MCHC, RDW, PCV, and MCV as the main prognosticator. MCHC and RDW were significantly higher in the group B compared to the
Figure 4 : Scatter plot (MPV & HbA1c)
Figure 5 : Scatter Plot (RDW & HbA1c)
Figure 6: Scatter plot showing correlation between RDW and FPG

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
33© JIMI • JULY - SEPT 2019 • VOL. 13
group A. RDW and MCHC may be applied as the auxiliary indicators of deterioration of glucoregulation.
CONCLUSIONS:
The mean RDW and MPV values in patients with diabetes were statistically significant (p<0.05) in comparison to controls.
A positive correlation between RDW and MPV with A1C, FPG was also found to be statistically significant (p<0.05).
The strongest correlation between RDW and MPV was with FPG followed by A1C.
REFERENCES:
1. Thompson CB, Jakubowski JA, Quinn PG, Deykin D, Valeri CR. Platelet Size as a Determinant of Platelet-Function. J Lab Clin Med. 1983;101(2): 205-13.
2. Bath PMW, Butterworth RJ. Platelet size: Measurement, physiology and vascular disease. Blood Coagul Fibrin. 1996;7(2):157-61.
3. Cakal B, Akoz AG, Ustundag Y, Yalinkilic M, Ulker A, AnkaraliH. Red Cell Distribution Width for Assessment of Activity of Inflammatory Bowel Disease. Digest Dis Sci. 2009;54(4):842-7.
4. Clarke K, Sagunarthy R, Kansal S. RDW as an additionalmarkerin inflammatory bowel Disease/Undifferentiated colitis. Digest Dis Sci. 2008;53(9):2521-3.
5. Anderson JL, Ronnow BS, Horne BD, Carlquist JF, May HT, Bair TL, et al. Usefulness of a complete blood count-
derived riskscore to predict incident mortality in patients with suspectedcardiovascular disease. Am J Cardiol. 2007;99(2):169-74.
6. Brusco G, Di Stefano M, Corazza GR. Increased red celldistribution width and coeliac disease. Digest Liver Dis.2000;32(2):128-30.
7. Hekimsoy Z, Payzin B, Ornek T, Kandogan G. Mean platelet volume in type 2 diabetic patients. J Diabetes Complicat.2004;18(3):173-6.
8. Coban E, Bostan F, Ozdogan M. The mean platelet volume in subjects with impaired fasting glucose. Platelets. 2006;17(1):67-9.
9. Coban E, Ozdogan M, Yazicioglu G, Akcit F. The mean platelet volume in patients with obesity. Int J Clin Pract. 2005;59(8):981-2.
10. Coban E, Afacan B. The effect of rosuvastatin treatment on themean platelet volume in patients with uncontrolled primarydyslipidemia with hypolipidemic diet treatment. Platelets. 2008; 19(2):111-4.
11. Coban E, Yazicioglu G, Avci AB, Akcit F. The mean plateletvolume in patients with essential and white coat hypertension.Platelets. 2005;16(7):435-8.
12. Nada AM. Red cell distribution width in type 2 diabetic patients. Diabetes Metab Syndr Obes. 2015;8:525-33.
13. Jaman MS, Rahman MS, Swarna RR, Mahato J, Miah MM, et al. Diabetes and red blood cell parameters. Ann Clin Endocrinol Metabol. 2018; 2: 001-009.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
34 © JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
Awareness about Lifestyle, Diet & Physical Activity among Diabetic Patients in a Tertiary Care Teaching Hospital
ABSTRACT:Background: High rates of diabetes in India are due to many factors such as poor lifestyle, dietary habits & low level of physical exercise.
Objective: The objective of this research was to assess the level of awareness about lifestyle, dietary habits, and low level of physical activity among diabetic patients in a tertiary care teaching hospital.
Methodology: A cross sectional study was conducted using self-prepared questionnaire among 200 patients coming to diabetic clinic at medicine OPD at AIIMS Rishikesh.
Results: Of the total population, 57% were male & 43% were females, only 28% of the respondents had good overall awareness.
Conlusion: Despite having clear attitude among respondents the practice & awareness were poor among the patient.
Key words: - Diabetes, awareness, lifestyle.
1. Additional Professor & Head, Division of Diabetes Mellitus, Department of General Medicine, AIIMS Rishikesh (Corresponding Author) E-mail: [email protected]
2. Dietician, AIIMS Rishikesh, Department of Dietetics3, 4. Intern Dietician, AIIMS Rishikesh, Department of dietetics5. Associate Professor, Dermatology GDMC, Dehradun
Ravikant1, Vinita Thapliyal2, Shweta Verma3, Shikha Saini4 , Shruti Barnwal4
INTRODUCTION:
Diabetes is a metabolic disorder with an increasing global prevalence & incidence. [1-5] it is presumably an oldest disease. It is known as Black Death from the 14th centenary. [6] The prevalence rate of the disease is now assumed to go on the higher side and the disease has now crossed the epidemic proportions. It is estimated that more than 170 million of population across the world will have this disease and the burden is assumed to be double by 2030[6] diabetes mellitus is the growing major concern in the developing countries like India. Significant modifications in diet & life style of urban Indians have major contribution in increasing incidence of diabetes. As per WHO by 2030 there will be 2.48 million of total diabetic population in India compared to 0.94 million which is 164% increases [7-8]. The high prevalence rate is due to transition (nutrition transition, epidemiological transition, economic & demographical transition) [9]
Keys to self-management of diabetes are dietary modification & lifestyle changes.[10] Several studies
report that knowledge of Diabetes is poor in developing and under-developed countries and health care professionals like pharmacists, nurses and physicians should improve knowledge through continuous education. Knowledge of disease is of utmost importance to meet the challenge of increasing healthcare costs. [11-13]The required lifestyle changes in managing DM are influenced by one’ knowledge, attitudes and practices (KAP) and one’s culture and values [14]. Hence, these important psychosocial determinants need to be incorporated in effective strategies to manage diabetes since they are major determinants in treatment regimens [15]. According to the International Diabetes Federation, at present 39.5 million people in India have pre- diabetes, and up to seven million will develop diabetes every year [16].The American Diabetes Association recognises the integral role of nutrition therapy in overall diabetes

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
35© JIMI • JULY - SEPT 2019 • VOL. 13
management& recommended that each person with diabetes receive an individualised eating plan that has been developed in collaboration with his or her health care provider.
A balanced diet makes a difference not only in managing diabetes but also help to manage the energy requirement. As diet is one of the crucial aspects of the management of diabetes, every individual with diabetes must be aware of the importance of the balanced diet [17-18].
METHODOLOGY:
Data collection
The data was collected using self-prepared questionnaire on knowledge attitude and practices. Interview technique was used by ensuring the confidentiality of information. After filling the questionnaire, the respondents called to a separate room for anthropometric measurement and variables such as weight (kg) & height in (cm) recorded using standard protocols.
In this study the modified classification of BMI for Asian populations was used to define overweight (23-24.99) and obesity (>25kg/m2).
200 patients with T2DM recruited from diabetic clinic, All India Institute of Medical Science, Rishikesh, Uttarakhand, India between August 2018 to October 2018.
Sample Size
The Sample Size Calculated Was 200 With A Confidence Interval Of 90% And Margin Of Error 5%.
Data Analysis
Inclusion criteria =All T2 DM patients coming to OPD above the age of 20 years were included in the study.
Exclusion criteria = Pregnant & lactating women were excluded from the study.
The analysis of data was performed by using spss17 computer statistical software package. Cross-tabulation and frequency distribution was done to find the relationship with categorical variables.
RESULTS:
The present study was conducted to assess the dietary pattern food habits and nutritional status of type 2 DM patient. The sample composed of 200 diabetic patients. For the study 200 patients were selected the overall response of the study was 100% of the 200 adults 114(57%) were male & 86 (43%) were female , 150 (75%) respondents were Hindu.
Table:-1 General characteristics of patients
Variables Sub group N % P value
Gender MaleFemale
11486
57%43%
<0.01
ReligionHindu MuslimSikh
1503020
75%15%10% <0.01
Food habits VegetarianNon-vegetarian
68132
34%66% <0.01
Marital status
MarriedUnmarried
19010
95%5% <0.01
OccupationServiceBusinessHousewife
762896
38%14%48%
<0.01
Figure:-1 BMI of study population.
Table: - 2 Anthropometric characteristics of study population
The mean age of the adults in the current study was 51.6 + 8.9 years. The mean height was 157.87 + -5.7 cm, weight was 64.1 + 9.2 kg , Mean BMI was 24.13 + 26 kg/m2
, Mean waist circumference was 89.4+ 9.3 cm & Mean HbA1c was 8.8 + 1.2%.
Risk factors
Variable Mean + S.D P value
Age 51.6 + 8.4 0.73Height 157.87 + 5.4 0.001Weight 64.1 + 9.2 0.001
BMI 24.13 + 2.6 0.534
W.C 89.4 + 9.3 0.001HbA1c 8.8 + 1.2 0.528

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
36 © JIMI • JULY - SEPT 2019 • VOL. 13
Data presented as Mean + Standard deviation.
AWARENESS ITEMS:
The study shows that only 59% of population was aware of balanced diet. The daily-recommended intake of fruits was very low only 18% of the population was consuming fruits on regular basis. 90% of the population still feels that eating excess of sugar & its products causes diabetes. Awareness regarding the brisk walking exist among 56% of population. Female respondents were non-smokers and non-alcoholic, 23% of male smoke on daily basis & 31% of male consumes alcohol. Scoring was done for awareness & practice regarding the diet, exercise & health education the median for the awareness score was above 6.4 & median score for practice was 61. Graded scoring system was adopted for assessment score (0-3 , poor, 4-7 , fair & 8-10, as good score). Figure3 shows that 28% of population has good awareness score 31% of population had only fair awareness score.
In present study, more than 60% of diabetic patients with low income have difficulty in following the practice, though they were aware of dietary modification & health check-up but the main constraint was affordability. Even having the good positive attitude participants were not following proper life-style management.
Table: 3 Awareness of diet, exercise & other practices among diabetic patients.
Awareness Item Responses%
DietAwareness of balanced diet?
Yes 59%No 41%
Daily recommended fruit intake. Yes- 18%No -82%
Eating too much of sugar causes diabetes.
Yes -90%No -10%
Awareness of different types of fat. Yes –No -100%
Awareness about carbohydrate sources
Yes -37%No -63%
Do you know what are starchy food Yes -35%No -65%
Foods to be avoided Yes -68%No -32%
Exercise Aware of brisk walking
Yes -56%No -44%
Behavior characteristics Smoking habits
Yes -23%No -77%
Alcohol consumption Yes -31%No -69%
Figure: 2 Type of exercises done by study group
Table: 4 Correlation of Awareness, Attitude & Practices among type 2 Diabetes
Parameters Person’s correlation
P value
Awareness & attitude 0.15 0.01
Awareness & practices -0.53 0.02
Attitude & practices -0.83 0.01
Figure: 3 Overall awareness of diet, physical activity & health education

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
37© JIMI • JULY - SEPT 2019 • VOL. 13
DISCUSSION:
In the past years many countries, has been experiencing a nutritional transition in food choices. [19] The rapid change in physical activity and food habits has led to the co-existence of many nutritional problems that underlines many chronic diseases. As population has become more urbanized and as lifestyles shifts towards reduced physical activities and increased food consumption, the prevalence of obesity expected to rise.
In this study, we found that the patients did not have a good knowledge about dietary management and food habits. Other studies have similar findings. [20]
This is comparable to the results of a study conducted by Kiren J et al in Tamilnadu, India reported that the majority of the participants 65 (86.7%) have heard about balanced diet, there are still a few of them who have not heard and understand the importance of balanced diet and there is still a need for promotion of awareness on balanced diet among the diabetic patients to prevent complications of diabetes mellitus in the future.
In a study conducted in Amman, Jordan by Jafar M.F.El-Qudah reported that more than half of patients gave wrong answers for meal recommended for diabetes/day (56.1%). The dietary knowledge of diabetic patients among female Ordains is inadequate and need improvement. Education and counselling about all aspects of diabetes are needed.
In other study, 90% of patients answered 50% of the knowledge questions correctly. Still a large proportion of population that is almost 40.3% were not able to score above 10%. In another study, reported that only 40% of diabetic patients had compliance with their diet. [21] Improving the knowledge of the diabetics in our society will not be an easy task. Mansour- ghanaei etal.reported low level of knowledge in Iran [22], Kuwait [23], Nigeria [24], and in United Arab Emirates [25]. On the other hand a good level of knowledge was found among patients in Malaysia [26], Pakistan [27] Qatar [28] and in Hong Kong study. Khattab MS etal (1999) conducted a study among the community of Saudi Arabia, and reported that only 40% of diabetic patients had good compliance with their diet. [30]
CONCLUSION:
According to the results, the dietary knowledge of diabetic patients is inadequate and need improvement. It was considered to be poor & the practice of dietary pattern is found to be inadequate study recommends that there is a
need to set up a healthy education programme on diabetes mellitus that would also include a self-monitoring programme.
REFERENCES:
1. Kumar PJ, Clark M (2002) Textbook of clinical Medicine. Pub: Saunders (London), pp:1099-1121.
2. Clinical Pharmacy and Therapeutics (2011) Roger walker and cate whittlesed (5th edn.).
3. Evaluation of the characteristics of safety withdrawal of prescription drugs from worldwide pharmaceutical markets- 1990 to 1999. Therapeutic innovation & regulatory science 35: 293-317.
4. Ford ES, Zhao G (2010) Prevalence and correlated of metabolic syndrome based on a harmonious definition among in the VS.J Diabetes Z: 180-193.
5. Utku N, Pape VF (2016) Neuroendowine Tumors.J Mult Scaler 3:193.
6. Jahan S, Fariduddin M, Sultana N, Aktar Y, Hasan M, etal. (2015) predictors of post-partum persistence of glucose intolerance and its association with cardio-metabolic risk factors in gestational diabetes mellitus. J Diabetes Metab 6:609.
7. Mafauzy, M. Diabetes mellitus in Malaysia. Med. J. Malays 2006, 61,397-398.
8. Murata, G.H;, Shah, J.H; Adam, K.D; Wendel, C.S; Bokhari, S.U; Solvas, P.A; Hoffman, R.M; Duckworth, W.C. Factors affecting diabetes knowledge in type 2 diabetes veterans. Diabetologia 2003, 46, 1170-1178 [PubMED].
9. Thapliyal.Vinita ; Singh. Karuna, ‘Nutrition Transition’ : A paradigm shift in Uttarakhand, Nutrition and Food Sciences, Amity Institute of Food Technology, Amity University, Noida, Sector – 125 India.
10. K.Ravi ; Thapliyal. Vinita,Knowledge attitude and practice of type 2 diabetic paitents in a tertiary care teaching hospital in India , Oat ,DOI : 10.11761/ IFNM .1000115.
11. Palani samly s; Arulkumaran, K.S.G; Rajasekaran, A. Knowledge assessment in adverse drug reactions and reporting: Arch. Pharma pract. 2013, 4.104-119.
12. Singh. A; Shenoy, S.; Sandhu, J.s prevalence of type 2 diabetes mellitus among urban Sikh population Amritsar. Ind. J. Common Med.2016, 41, 263-267. [Cross Ref] [PubMed].
JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
38 © JIMI • JULY - SEPT 2019 • VOL. 13
13. Acharya, K.G; Shah, K.N; Solanki, N.D; prescriptions, cost and adherence to treatment guidelines: A prospective, cross-sectional study at a tertiary care teaching hospital. J. Basic, Clin. Pharm 2013, 4, 82-87 [PubMed].
14. Ardena GJRA, Pa2-Pacheco E, Jimeno CA, Lantion- AngFL, persons with type 2 diabetes in a rural community phase 1 of the community-based diabetes self-management education (DSME) program in San Jaun, Batangas, Phillippines, Diabetes Research Clinical practice. 2010; 90(2): 160-166.
15. Hawthorne K, Robles Y, Canning-John R, Edwards AGK. Culturally appropriate health education for type 2 diabetes in ethnics’ minority groups: A systematic and narrative review of randomized controlled trials. Diabetes Medicine. 2010; 27(6); 613-623.
16. World Health Organization/International Diabetes Federation. Report of WHO/IDF consultation. Definition and diagnosis of diabetes mellitus and intermediate of hyperglycaemia. Geneva: WHO press, 2006:1-46?
17. Kiren J. etal/J. Pharm. Sci & Res. Vol. 9(2), 207, 245-247.
18. Kishore J etal, Awareness, practices and treatment seeking behaviour of Type2Diabetes Mellitus patients in Delhi. Ann Med Health sci. Res.2015, 5(4), 266-273.
19. Musaiger, A.O.; Lloyd, O.L.; Al-Neyadi, S.M.; Bener, A.B. Lifestyle factors associated with obesity among male university students in the United Arab Emirates. Nutrition & Food science. , 33(4) 145-14 2003.
20. Green A.J., Bazat D, Fox M et al. Health related Behaviours of people with Diabetes and those with cardio metabolic risk factors: results from SHIELD. International journal of clinical practice. November 2007; 67(11): 1791-1797.
21. Khattab, M.S.; Aboifotouh, M.A.; Khan, M.Y.; Humaidi, M.A.; al- Kaldi, Y.M. Compliance and control of diabetes in a family practice setting, Saudi Arabia. East Mediterr Health J.5 (4) 755-765 1999.
22. Mansour- ghanaei, R.; Joukar, F.; Soati, F.; Khanegha, A. Association between knowledge, Iocus of control and health belief with selfmangement, HbA1c level; and number of attendance in type 1 diabetes mellitus patients. Int J Clin Exp Med, 6 (6)470-477 2013.
23. Al-Adsani, A.; Moussa, M.; Al-Jasem, L.; Abdella, N.; Al-Hamad, N. The level and determinant of diabetes knowledge in Kuwaiti adults with type 2 diabetes. Diabetes Metab J, 35 (2) 121- 128 2009.
24. Yusuf, K.; Obe, O.; Joseph, B. Adherence to anti-diabetic drug therapy and self-management practices among type-2 diabetics in Nigeria. Pharm World Sci, 30 (6) 876- 883 2008.
25. Al-Maskari, F.; El-Sadig, M.; Al-Kaabi, J.; Afandi, B.; Nagelkerke, N.; Yeatts, K. Knowledge, attitude and practices of diabetic patients in the united Arab emirates . PLoS One, 8 (1) e52857 2013.
a. Cross Ref
26. Ng, S.; Chan, K.; Lian, Z.; C hauh, Y.; Waseem, A.; Kadirvelu, A. Reality vs. illusion: knowledge, attitude and practice mong diabetic patients. Int J Collab Res Internal Med, 4 (5)723-732 2012.
27. Hawthorne, K.; Tomlinson, S. Pakistani Muslims with type 2 diabetes mellitus: effect of sex, literacy skills, known diabetic complications and place of care on diabetic knowledge, reported self-monitoring management and glycemic control. Diabetic Med, 16(7): 591-7 1999.
a. Cross Ref
28. Mesmar, M.; Eljiack, A.; Al-Kuwari, M. Knowledge and practice of type 2 diabetic patients attending primary health care in Qatar. Middle East J Fam Med, 9 (4) 3- 10 2011.
29. Khattab MS, Aboifotouh MA, Khan MY, Humaidi MA, al- Kaldi YM. Compliance and control of diabetes in a family practice setting, Saudi Arabia. East. Mediterr Health J. 1999, 5(4), 755-765.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
39© JIMI • JULY - SEPT 2019 • VOL. 13
Original Article
A Study of Clinical outcome and analysis of 50 Cases of Snake Bite
1. Assistant Professor, Department of Medicine, Pramukhswami Medical College, Karamsad, Anand, Gujarat, India2. Assistant Professor, Department of Medicine, Government Medical College, Surat, Gujarat, India.
(Corresponding Author) E-mail: [email protected]
Vaishali N. Vegada1, Hiren N. Makvana2
INTRODUCTION:
India has always been a land of common and exotic snakes. Snake bite has become a very important preventable public health hazard as a result of urbanization and cutting down of forests. It is believed that in India about 2 millions people are bitten by snake and about 35000-50000 cases prove fatal. This amply reflects the magnitude of the
problem. Snakes are ubiquitous species of reptiles, around 216 varieties are found in India, of which about 52 are venomous. Only four varieties of snakes are commonly encountered as a cause of snake bite poisoning[6].
• Russell’s viper • Saw scaled viper• Krait • Cobra
ABSTRACT:
Background: Snake bite has become a very important preventable public health hazard. Snake bite usually take place in villages and forests. About 2 million people are bitten by snake and about 35000-50000 cases prove fatal showed the mortality of about 1.75% to 2.5% due to snake bite.
Objective of Study: 1. To study the various complications of snake bite
2. To study the overall outcome of snake bite.
3. To study the cause of death in snake bite patients.
Methodology: 50 cases of snake bite admitted at P.D.U hospital, Rajkot were studied, from December 2015 to July 2017 during the season of monsoon and post monsoon starting from june 2016. The clinical history and examinations were carried out in detail, all necessary investigations done,their clinical course and development of complications were studied, then outcome and analysis of cause of death were recorded.
Observations: Most of cases of snake bite occurred in rural areas with 70 % of cases whereas only 30 % cases in urban areas. The highest incidence of snake bite is between May to August 37(72%) and the incidence in post monsoon is 26%. In clinical evaluation 44(88%) had symptoms of toxic snake bite within 3 hours and 6(12%cases) took >3 hours to develop symptoms .On examination local pain was reported in almost all cases 42(84%) out of 50 cases and local swelling was reported in 34(68%) cases. Local bleeding occurred in 24 (48%) cases which is the commonest manifestation, whereas other haematological manifestations like Heamaturia, Heamoptysis, Hemetemesis and Epistaxis occurred in 1 (2%) cases. Neurological manifestation like blurring of vision 23 (46%) cases, difficulty in breathing 20 (40%) cases and ptosis 20 (40%) cases. Local complications like cellulitis occurred in 29(58%) cases and systemic complications like bulbar palsy in 20(40%) cases, respiratory paralysis in 20(40%) cases, DIC occurred in 3(6%) cases. In outcome highest mortality noted in 2 cases out of 9 cases (22%) of cobra bite whereas 1 case died out of 9 cases of krait bite.in analysis of cause of death 2 cases were died due to respiratory paralysis and 1 case due to haematological toxicity.
Conclusion: Most common presentation was cellulitis and bulbar and respiratory paralysis. Majority of the patients complicated and died due to respiratory failure.
Keywords : Snake bite

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
40 © JIMI • JULY - SEPT 2019 • VOL. 13
MATERIALS AND METHOD:
50 cases of snake bite admitted at P.D.U hospital, Rajkot were studied, from December 2015 to July 2017 during the season of monsoon and post monsoon starting from June 2016. The clinical history and examinations were carried out in detail, all necessary investigations done, their clinical course and development of complications were studied, then outcome and analysis of cause of death were recorded.
OBSERVATIONS:
Most of cases of snake bite occurred in rural areas with 70 % of cases whereas only 30 % cases in urban areas. The highest incidence of snake bite is between May to August 37(72%) and the incidence in post monsoon is 26%. In clinical evaluation 44(88%) had symptoms of toxic snake bite within 3 hours and 6 (12%) cases took >3 hours to develop symptoms. On examination local pain was reported in 42(84%) out of 50 cases and local swelling was reported in 34(68%) cases. Local bleeding occurred in 24(48%) cases which is the commonest manifestation, whereas other haematological manifestations like Heamaturia, Heamoptysis, Hemetemesis and Epistaxis occurred in 1(2%) cases. Neurological manifestation like blurring of vision 23 (46%) cases, difficulty in breathing 20 (40%) cases and ptosis 20(40%) cases. Local complications like cellulitis occurred in 29(58%) cases and systemic complications like bulbar palsy in 20(40%) cases, respiratory paralysis in 20(40%) cases, DIC occurred in 3(6%) cases. In outcome highest mortality noted in 2 cases out of 9 cases (22%) of cobra bite whereas
1 case died out of 9 cases of krait bite.in analysis of cause of death 2 cases were died due to respiratory paralysis and 1 case due to haematological toxicity.
Figure 1 : complications of Snake Bite
Table 1 : Outcome and Type Specific Mortality
Type of Snake No. of Cases
Expired % of Type Specific Snake
MortalitySaw Scalded Viper (Paidka)
24 0 0
Russell’s Viper 2 0 0Cobra 9 2 22 %Krait 9 1 11 %Unidentified 6 0 0
Table 1 shows the outcome and type specific mortality, the highest mortality noted in 2 cases out of 9 cases of cobra bite which is 22% whereas 1case died out of 9 cases of krait bite.Table 2: Cause of Death
Cause of Death No. of CasesRespiratory paralysis 2Periphery circulatory failure shock 1Cardio toxicity 0
Table 2 shows the cause of death. 2 cases are of respiratory paralysis due to cobra bite and died in spite of ventilatory support. 1 case died due to haematological toxicity.Cardio toxicity is not reported because of snake biteDISCUSSION :In present study 50 cases of toxic snake bite were studied, who were admitted at P.D.U hospital Rajkot. The data
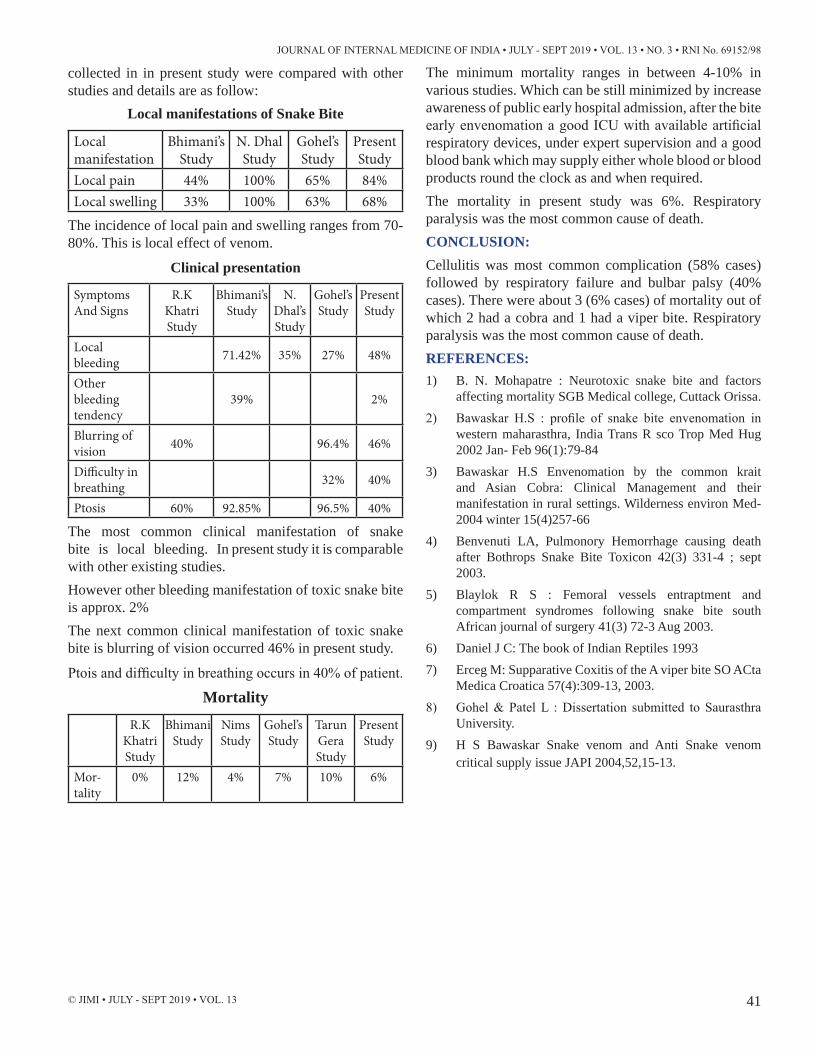
JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
41© JIMI • JULY - SEPT 2019 • VOL. 13
collected in in present study were compared with other studies and details are as follow:
Local manifestations of Snake Bite
Local manifestation
Bhimani’s Study
N. Dhal Study
Gohel’s Study
Present Study
Local pain 44% 100% 65% 84%Local swelling 33% 100% 63% 68%
The incidence of local pain and swelling ranges from 70-80%. This is local effect of venom.
Clinical presentation
Symptoms And Signs
R.K Khatri Study
Bhimani’s Study
N. Dhal’s Study
Gohel’s Study
Present Study
Local bleeding 71.42% 35% 27% 48%
Other bleeding tendency
39% 2%
Blurring of vision 40% 96.4% 46%
Difficulty in breathing 32% 40%
Ptosis 60% 92.85% 96.5% 40%
The most common clinical manifestation of snake bite is local bleeding. In present study it is comparable with other existing studies.However other bleeding manifestation of toxic snake bite is approx. 2%The next common clinical manifestation of toxic snake bite is blurring of vision occurred 46% in present study.
Ptois and difficulty in breathing occurs in 40% of patient.
Mortality
R.K Khatri Study
Bhimani Study
Nims Study
Gohel’s Study
Tarun Gera Study
Present Study
Mor-tality
0% 12% 4% 7% 10% 6%
The minimum mortality ranges in between 4-10% in various studies. Which can be still minimized by increase awareness of public early hospital admission, after the bite early envenomation a good ICU with available artificial respiratory devices, under expert supervision and a good blood bank which may supply either whole blood or blood products round the clock as and when required.The mortality in present study was 6%. Respiratory paralysis was the most common cause of death.CONCLUSION:Cellulitis was most common complication (58% cases) followed by respiratory failure and bulbar palsy (40% cases). There were about 3 (6% cases) of mortality out of which 2 had a cobra and 1 had a viper bite. Respiratory paralysis was the most common cause of death.REFERENCES:1) B. N. Mohapatre : Neurotoxic snake bite and factors
affecting mortality SGB Medical college, Cuttack Orissa.2) Bawaskar H.S : profile of snake bite envenomation in
western maharasthra, India Trans R sco Trop Med Hug 2002 Jan- Feb 96(1):79-84
3) Bawaskar H.S Envenomation by the common krait and Asian Cobra: Clinical Management and their manifestation in rural settings. Wilderness environ Med- 2004 winter 15(4)257-66
4) Benvenuti LA, Pulmonory Hemorrhage causing death after Bothrops Snake Bite Toxicon 42(3) 331-4 ; sept 2003.
5) Blaylok R S : Femoral vessels entraptment and compartment syndromes following snake bite south African journal of surgery 41(3) 72-3 Aug 2003.
6) Daniel J C: The book of Indian Reptiles 19937) Erceg M: Supparative Coxitis of the A viper bite SO ACta
Medica Croatica 57(4):309-13, 2003.8) Gohel & Patel L : Dissertation submitted to Saurasthra
University.9) H S Bawaskar Snake venom and Anti Snake venom
critical supply issue JAPI 2004,52,15-13.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
42 © JIMI • JULY - SEPT 2019 • VOL. 13
Treatment of Allergic Bronchopulmonary Aspergillosis Rajendra Prasad1, Rishabh Kacker2, Nikhil Gupta3
1. Department of Pulmonary Medicine, Era’s Lucknow Medical College & Hospital, Era University, Lucknow
2. Department of Pulmonary Medicine, Era’s Lucknow Medical College & Hospital, Era University, Lucknow
3. Department of General Medicine, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow (Corresponding Author) E-mail : [email protected]
INTRODUCTION:
Pulmonary aspergillosis is a clinical spectrum of lung disease caused by the fungus Aspergillus. The classification of pulmonary aspergillosis includes saprophytic aspergillosis in the form of pulmonary aspergilloma, immune disease in the form of allergic bronchopulmonary aspergillosis (ABPA), IgE mediated asthma, hypersensitivity pneumonitis, allergic Aspergillus sinusitis (AAS) and infectious disease in the form of invasive and semi-invasive pulmonary aspergillosis.[1] Allergic bronchopulmonary aspergillosis complicates asthma and cystic fibrosis in 1%–2% and 5%–15% of patients, respectively[2]. ABPA is suspected in any patient with asthma with lung shadows on chest X-Ray and peripheral blood eosinophilia. All the features are not necessary to diagnose ABPA. The important diagnostic criteria are the presence of recurrent pulmonary infiltrates, peripheral blood eosinophilia and positive skin test to Aspergillus antigen[3]. Radiological features in patients of ABPA may be transient or permanent. Fleeting shadows are characteristic of ABPA and is also termed as “Walking Pneumonia”[4]. In a study by Prasad et al around 66.7% patients of ABPA had fleeting opacities. Early diagnosis and treatment is necessary in order to prevent end stage lung fibrosis. Despite several published series from various parts of the country, this disease is still under recognized and misdiagnosed as pulmonary tuberculosis.
In a study conducted by Prasad et al 91% of patients were misdiagnosed as pulmonary tuberculosis, and they had been treated with antitubercular therapy before a diagnosis of ABPA could be made[5]. Management of allergic bronchopulmonary aspergillosis includes corticosteroids to control the host immune response while azoles are frequently used to decrease the burden of the organism. As chronic steroid therapy is associated with a number of adverse effects, other therapies are being constantly explored in order to treat the disease as effectively as possible with fewer number of adverse reactions. This article, aims to review these newer treatment options in order to help the physician to provide with the best treatment available.
ORAL CORTICOSTEROIDS:
Oral corticosteroid remains the cornerstone for the treatment of ABPA.[6] The goal of therapy is to achieve symptom resolution, clearance of radiographic infiltrates, and establishment of a stable baseline serum level of total IgE. There are two dose schedules of oral glucocorticoid therapy, low dose and high dose. In low dose oral glucocorticoid therapy, Prednisolone 0.5 mg/kg/d is given for 2 weeks, then on alternate day for 6–8 weeks and then tapered 5–10 mg every 2 weeks and then discontinued. In high dose glucocorticoid therapy, Prednisolone 0.75 mg/kg is given for 6 weeks, followed by 0.5 mg/kg for 6 weeks,
ABSTRACT:Pulmonary aspergillosis is a clinical spectrum of lung disease caused by the fungus Aspergillus. Oral corticosteroids remain the mainstay treatment of ABPA. In recent decade antifungals have emerged as a remarkable adjunctive treatment which aids in resolution of symptoms, decreasing IgE levels and exacerbations. Inhaled corticosteroids though useful for the management of asthma in patients with ABPA, have minimal role in regards to controlling the clinical manifestations of ABPA. Newer anti-fungal drugs such as voriconazole and posaconazole appears to be promising as a monotherapy in the management of ABPA. Alternatives to azoles such as amphotericin B and Omalizumab have also shown efficacy in reducing symptoms and exacerbations along with corticosteroid therapy.
Review Article

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
43© JIMI • JULY - SEPT 2019 • VOL. 13
then taper 5 mg every 6 weeks to continue for a total of atleast 6–12 months. A RCT in adults with asthma had shown that medium and high dose of steroids were equally effective for ABPA, though high-dose steroids had more side effects.[7] During the acute episode, usual starting dose of prednisone is 0.5 mg/kg daily for 2 weeks then reduced to an alternate day regime for 2–3 months, after that it should be tapered off in next 2–3 months. Repeat chest X ray in 1 month should demonstrate clearing of the infiltrates. The total serum IgE level also regresses along with the infiltrates. The failure of the total serum IgE level to decrease suggests continuation of active disease and requires additional corticosteroids. Following successful infiltrate clearing there is a reduction in total serum IgE and remission of the patient’s symptoms. The total serum IgE level, chest x ray, absolute eosinophil count should then be followed at 6–8 weeks intervals regularly. The goal of glucocorticoid therapy is not normalization of total Serum. IgE but reduction in total Serum. IgE by 35%–50% from baseline that defines remission by 6 weeks Serial total serum IgE levels are important for follow up care.[2] A sudden doubling of total serum IgE levels over baseline usually heralds activity of disease. Such activity can be aborted or even prevented with increased dose of prednisone at the time when the elevated level of IgE is noted.
Patients who have remission of ABPA may discontinue prednisone. The remission may last for years or may be permanent. In patients with recurrent flares of ABPA or in those with severe persistent asthma, long term corticosteroid therapy may be necessary to control their symptoms. Patients in the fibrotic stage of ABPA may have increased sputum volume as a result of infection. Measures such as postural drainage and antibiotics may be useful, but with deterioration, exercise tolerance decreases and oxygen therapy may be needed.
Optimization of baseline asthma therapy is essential with inhaled corticosteroid and β2 agonists. In addition, prophylactic measures should be instituted when indicated to prevent the adverse effects of long term corticosteroid treatment such as osteoporosis. Thus, patients who will be taking prednisolone for more than 2–3 months should be considered for bone mineral density analysis to direct commencement of calcium/Vitamin D supplementation with or without bisphosphonates.[8]
ALTERNATIVE TO CORTECOSTEROID TREATMENT:
Even though oral corticosteroids is the treatment of choice in ABPA, the fact that it is associated with numerous adverse effects cannot be neglected. Inhaled
corticosteroids are associated with fewer side effects and hence considering them as a viable treatment option for ABPA seems appropriate. Not a lot of studies have been conducted to evaluate the role of inhaled corticosteroids in the management of ABPA. Inhaled corticosteroids, while useful for concomitant asthma management in patients with ABPA, do not control the pathophysiology or clinical manifestations of ABPA.[9-13] In contrast to the inhaled corticosteroid therapy “pulse” therapy(10-20mg/kg/day i.v. methylprednisolone infused on three consecutive days every 3-4 weeks) was found out to be generally safe and effective in two open labelled series of thirteen steroid dependent ABPA CF patients.[14-15]
ANTI-FUNGAL DRUGS:
The most efficacious alternative to long term oral corticosteroids is the use of antifungal agents either in conjunction to the steroid therapy or even as a standalone therapy. Use of antifungal therapy in the treatment of ABPA is based on the assumption that allergic inflammatory responses arise in part from non-invasive airway fungal infection. Pooled analysis showed that itraconazole could significantly decrease IgE levels by >25% when compared to placebo, reduction in steroid dose by ≥50%; increase in exercise tolerance by ≥25%, improvement of ≥25% in results of spirometry, resolution of pulmonary opacities but failed to reach statistical significance, and did not cause significant improvement in lung function. Itraconazole modified the immunologic activation associated with ABPA and improve clinical outcome at least over the period of 16 wks. The effectiveness of itraconazole in the treatment of ABPA was also demonstrated in two randomised, double-blind, placebo controlled trials in patients with asthma.[16-17] At present, itraconazole should be limited in cases where oral steroids are contraindicated or refused by patients. In patients requiring high doses of oral steroid, itraconazole may allow reduction in steroid doses, but should not replace the need of steroid; the major concern being no long term trials and adrenal suppression with itraconazole. Thus, long term trials are required before firm recommendation can be made for the use of itraconazole in ABPA. In a recent randomized trial of itraconazole vs prednisolone in acute stage ABPA, it was found that oral glucocorticoids were more effective than itraconazole monotherapy in producing treatment response in patients with acute stage ABPA complicating asthma. However, time to first exacerbation and the number of subjects experiencing exacerbations were similar in both groups[18]. An important concern with azole therapy is emerging risk of azole resistant Aspergillus species.[19] The use of azoles for ABPA in asthma patients was reviewed by the Cochrane

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
44 © JIMI • JULY - SEPT 2019 • VOL. 13
collaboration which suggested that itraconazole modifies the immunologic activation associated with ABPA and improves the clinical outcome, at least over a period of 16 weeks, though adrenal suppression with inhaled corticosteroids and itraconazole is a potential concern.[20] Another Cochrane review was done which aimed to test the hypothesis that antifungal therapy improved the clinical status in patients of ABPA associated with cystic fibrosis, concluded that at present there are no randomized controlled trials to evaluate the use of antifungal therapies for the treatment of ABPA in people with cystic fibrosis and trials with clear outcome measures are needed to properly evaluate this potentially useful treatment of ABPA in cystic fibrosis[21]. Newer generation triazoles such as voriconazole and posaconazole have also been reported as beneficial in the treatment of ABPA. Treatment with voriconazole as a monotherapy was shown to be associated with improvements in clinical status, lung function and serologies.[22] In another study, 10 out of 11 steroid-dependent patients were able to reduce oral steroid needs while having a marked drop in IgE levels.[23] Voriconazole has the advantage of excellent oral bioavailability but is associated with a greater number of adverse drug reactions when compared to itraconazole.[24-25] A newer agent, posaconazole has been shown to have higher activity against Aspergillus and also has fewer side effects when compared to voriconazole, though is much more expensive. A newer agent isavuconazole, a broad spectrum antifungal azole with potent activity against Aspergillus species has been shown to be effective in a study conducted by Jacobs et al in a patient of ABPA who was successfully treated with marked improvement and minimal adverse effects.[26]
ALTERNATIVES TO AZOLES:
As azoles are frequently associated with potential issues of metabolism, tolerance and resistance, further alternative approaches have been investigated.
Amphotericin B
Amphotericin deoxycholate has been frequently used via inhalational route in the treatment of pulmonary fungal infection, primarily in the setting of cancer treatment and lung transplantation. Amphotericin B can be delivered via nebulization to the lower respiratory tract in doses which are capable enough to exceed the minimal inhibitory concentration of Aspergillus in the epithelial lining.[27] Since the systemic levels are low which in turn reduces the risk of renal toxicities it is a plausible therapy for the treatment of recurrent non invasive infections associated with ABPA. However, data regarding the efficacy of amphotericin B is pretty scarce as of now and thus more
studies needs to be conducted in order to determine its actual role in the treatment of ABPA. As of now two studies utilizing Amphotericin deoxycholate or liposomal amphotericin in aerosol doses of 10 mg twice daily or 20 mg thrice weekly, respectively with success. [28-29]. Use of amphotericin has been associated with cough and bronchospasm and hence, observation after drug delivery is warranted. [30]
OMALIZUMAB:
Omalizumab, a monoclonal antibody to IgE has been associated with improvement in symptoms, reduction in exacerbations and asthma hospitalizations, improvement in lung function and reduction in dose of oral steroids.[2] However, a recent retrospective series conducted in France has found variable results in 32 patients of ABPA with cystic fibrosis, which though reported a reduction in the steroid need over a 21 month observation period but there was no significant improvement in the lung function or the use of antibiotics.[31]
CONCLUSION:
Corticosteroids remains the validated mainstay pharmacological treatment in ABPA. Use of azoles may allow reduction in steroid doses but should not replace the need the of steroid. More long term trials are neccisitated before firm recommendation can be made for the use of itraconazole in ABPA. Inhaled corticosteroids though useful for the management of asthma in patients with ABPA, they have minimal role in regards to controlling the clinical manifestations of ABPA. Newer anti-fungal drugs such as voriconazole and posaconazole appears to be promising as a monotherapy in the management of ABPA but more trial needs to be conducted before they can be recommended as a sole treatment in ABPA.
REFERENCES:1. Binder RE, Faling LJ, Pugatch RD, Mahasaen C, Snider
GL. Chronic necrotizing pulmonary aspergillosis: A discrete clinical entity. Medicine (Baltimore) 1982;61:109-24.
2. Agarwal R, Chakrabarti A, Shah A, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy 2013; 43:850–73.
3. Prasad R, Kacker R, Gupta N. Allergic bronchopulmonary aspergillosis: Indian scenario. Indian J Allergy Asthma Immunol 2019;33:63-9.
4. Prasad R, Garg R, Sanjay. Walking pneumonia in a patient of bronchial asthma: A clue to the diagnosis of allergic bronchopulmonary aspergillosis. Pulmon 2007; 9:120-23.
5. Prasad R, Garg R, Sanjay, Shukla AD. Allergic broncho-pulmonary aspergillosis: A review of 42 patients from a tertiary care center in India. Lung India 2009;26:38-40.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
45© JIMI • JULY - SEPT 2019 • VOL. 13
6. Fink JN. Therapy of allergic bronchopulmonary aspergillosis. Indian J Chest Dis Allied Sci 2000;42:221-4
7. Agarwal R, Aggarwal AN, Dhooria S, Singh Sehgal I, Garg M, Saikia B, et al. A randomised trial of glucocorticoids in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J 2016;47:490-8.
8. Recommendations for the prevention and treatment of glucocorticoid induced osteoporosis. American College of Rheumatology Task Force on Osteoporosis Guidelines. Arthritis Rheum 1996;39:1791 801
9. Inhaled beclomethasone dipropionate in allergic bronchopulmonary aspergillosis. Report to the Research Committee of the British Thoracic Association. Br J Dis Chest 1979; 73: 349–56.
10. Heinig JH, Weeke ER, Groth S, et al. High-dose local steroid treatment in bronchopulmonary aspergillosis. A pilot study. Allergy 1988; 43: 24–31
11. Imbeault B, Cormier Y. Usefulness of inhaled high-dose corticosteroids in allergic bronchopulmonary aspergillosis. Chest 1993; 103: 1614–17
12. Seaton A, Seaton RA, Wightman AJ. Management of allergic bronchopulmonary aspergillosis without maintenance oral corticosteroids: a fifteen-year follow-up. QJM 1994; 87: 529–37.
13. Agarwal R, Khan A, Aggarwal AN, et al. Role of inhaled corticosteroids in the management of serological allergic bronchopulmonary aspergillosis (ABPA). Intern Med 2011; 50: 855–60.
14. Thomson JM, Wesley A, Byrnes CA, et al. Pulse intravenous methylprednisolone for resistant allergic bronchopulmonary aspergillosis in cystic fibrosis. Pediatr Pulmonol 2006; 41: 164-70.
15. Cohen-Cymberknoh M, Blau H, Shoseyov D, et al. Intravenous monthly pulse methylprednisolone treatment for ABPA in patients with cystic fibrosis. J Cyst Fibros 2009; 8: 253–57.
16. Stevens DA, Schwartz HJ, Lee JY, et al. A randomized trial of itraconazole in allergic bronchopulmonary aspergillosis. N Engl J Med 2000; 342: 756–62.
17. Wark PA, Hensley MJ, Saltos N, et al. Anti-inflammatory effect of itraconazole in stable allergic bronchopulmonary aspergillosis: a randomized controlled trial. J Allergy Clin Immunol 2003; 111: 952–57.
18. Agarwal R, Dhooria S, Singh Sehgal I, Aggarwal AN, Garg M, Saikia B, Behera D, Chakrabarti A. A randomised trial of Itraconazole vs Prednisolone in Acute-Stage Allergic Bronchopulmonary Aspergillosis Complicating Asthma. Chest. 2018;153(3):656-64
19. Tucker RM, Haq Y, Denning DW, Stevens DA. Adverse events associated with itraconazole in 189 patients on chronic therapy. J Antimicrob Chemother 1990;26:561-6
20. Wark PA, Gibson PG, Wilson AJ. Azoles for allergic bronchopulmonary aspergillosis associated with asthma. Cochrane Database Syst Rev 2004; 3: CD001108.
21. Elphick HE, Southern KW. Antifungal therapies for allergic bronchopulmonary aspergillosis in people with cystic fibrosis. Cochrane Database of Systematic Reviews 2016, Issue 11. Art. No.: CD002204.
22. Hilliard T, Edwards S, Buchdahl R, et al. Voriconazole therapy in children with cystic fibrosis. J Cyst Fibros 2005; 4:215–20
23. Glackin L, Leen G, Elnazir B, et al. Voriconazole in the treatment of allergic bronchopulmonary aspergillosis in cystic fibrosis. Ir Med J 2009; 102: 29.
24. Markantonis SL, Katelari A, Pappa E, et al. Voriconazole pharmacokinetics and photosensitivity in children with cystic fibrosis. J Cyst Fibros 2012; 11: 246–252
25. Jain LR, Denning DW. The efficacy and tolerability of voriconazole in the treatment of chronic cavitary pulmonary aspergillosis. J Infect 2006; 52: e133–e137.
26. Jacobs SE, Saez-Lacy D, Wynkoop W, Walsh TJ. Successful Treatment of Allergic Bronchopulmonary Aspergillosis With Isavuconazole: Case Report and Review of the Literature. Open Forum Infect Dis. 2017;4(2):ofx040. Published 2017 May 5. doi:10.1093/ofid/ofx040
27. Kuiper L, Ruijgrok EJ. A review on the clinical use of inhaled amphotericin B. J Aerosol Med Pulm Drug Deliv 2009;22: 213–227
28. Proesmans M, Vermeulen F, Vreys M, et al. Use of nebulized amphotericin B in the treatment of allergic bronchopulmonary aspergillosis in cystic fibrosis. Int J Pediatr 2010; 2010: 376287
29. Hayes D Jr, Murphy BS, Lynch JE, et al. Aerosolized amphotericin for the treatment of allergic bronchopulmonary aspergillosis. Pediatr Pulmonol 2010; 45: 1145–48.
30. Slobbe L, Boersma E, Rjinders BJ. Tolerability of prophylactic aerosolized liposomal amphotericin-B and impact on pulmonary function: data from a randomized placebo-controlled trial. Pulm Pharmacol Ther 2008; 21: 855–59
31. Grard S, Auzou L, Nove-Josserand R, et al. Omalizumab (Xolair1) in the treatment of ABPA in 32 patients with cystic fibrosis. J Cystic Fibros 2013; 12: Suppl. 1, S96.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
46 © JIMI • JULY - SEPT 2019 • VOL. 13
Beyond Diabetes, Metformin may prove to be a ‘Wonder Drug’Review Article
Rakesh Kumar
1. Senior Consultant Internal Medicine, Indraprastha Apollo Hospitals, Sarita Vihar, Delhi Mathura Road, New Delhi-110076. (Corresponding Author) E-mail : [email protected]
INTRODUCTION:
Inthe past 2 decades, metformin has become a mainstay of type 2 diabetes management and is now the recommended first line drug for treating the disease in the United States and worldwide.
Available in the United States since 1995, metformn is an attractive therapy forclinicians and patients alike. Studies have found the agent to be safe and effectiveand at about $4 for a 1 month supply of the generic, that option is affordable at a time when many prescription drugs are being priced out of reach for some patients.
Metformin is most commonly used to treat type 2 diabetes, either alone or combined with other agents, but is also used off label as a treatment for prediabetes, gestational diabetes and PCOS. [1]
Metformin (a biguanide derivative), by controlling blood glucose level decreases these complications. Metformin works by helping to restore the body’s response to insulin. It decreases the amount of blood sugar that the liver produces and that the intestines or stomach absorb.[2] Metformin, other than hypoglycaemic activity, has been taken with diet and exercise changes to prevent diabetes in people who are at high risk for becoming diabetic. It is also used in women with polycystic ovarian syndrome. Metformin may make menstrual cycles more regular and increase fertility.[3]
ABOUT PCOD
Metformin has been used for PCOS treatment since 1994,[4] by which most of the metabolic abnormalities of PCOS can be reversed. [5]
ABSTRACT:
Metformin has been proven to be one of the most safe and effective antihyperglycemic agents. Through more than six decades of metformin use, it became the most studied hypoglycemic agent; through these studies, it showed a marvellous non-glycemic related effect. These effects include modulation of different points of cancer timeline, weight reduction, cardiovascular health, thyroid diseases, polycystic ovaries disease and many other medical conditions like aging. Aging has been targeted by genetic and dietary manipulation and by drugs in order to increase lifespan and health span in numerous models. Metformin, which has demonstrated protective effects against several age-related diseases in humans, will be tested in the TAME (Targeting Aging with Metformin) trial, as the initial step in the development of increasingly effective next-generation drugs. The aim of this review was to assess the effect of metformin on non-diabetes related medical diseases. We have examined the studies published in PubMed and summarized different randomized controlled trials, observational trials and review articles. This review has summarized most of the non-glycemic effects of metformin. Metformin has been solidly shown to be effective in weight control with certain medications, effective in neuroprotection, in endothelial health, in control of anti-HIV agent side effects and many other crucial health jeopardies. The effects in cancer timeline modulation have taken the biggest part, since it was the most studied area outside the diabetes field. Having mentioned all the above privileges, and in addition to the robust evidence in glycemic control, this consolidates the position of metformin as a first line agent in treatment of diabetes and pre-diabetes. Perhaps in the near future, we may see other indications to use metformin in non-diabetes patients.
Keywords: metformin, antitumor effect, antiaging effect, cardiovascular protective, HIV associated diabetes, neuroprotective effect, PCOS.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
47© JIMI • JULY - SEPT 2019 • VOL. 13
Metformin dose ranged from 850 to 1,700 mg in different studies (Table 1). The mechanism is thought to be mediated through increased insulin sensitivity, increased ovarian secretion of estrogen, decreased ovarian production of androgen and augmentation of the production of sex hormone binding globulin.[5,6] A recent meta-analysis shows that metformin can reduce testosterone and insulin in PCOS women.[7]“Metformin is the first drug of choice, by all standards. It is time tested, proven, has good efficacy, a good safety profile and it’s cheap.
MECHANISM OF ACTION OF METFORMINThe metformin molecule works in the human’ bodies at the level of the liver and peripheral tissues, basically, by downsizing the glucose output from the liver, as well as by enhancing the utilization at the peripheral tissues (muscles). This process takes place through the activation of adenosine monophosphate-activated protein kinase (AMPK). The AMPK is the cell regulatory pathway that reduces the energy expenditure at the cellular level. In humans, AMPK is essential for the metabolism of glucose and fatty acids, through reduction of the gluconeogenesis and fatty acids synthesis in the liver, and enhancing glucose uptake, and the fatty acids oxidation by peripheral tissues.[8]
METFORMIN & OBESITYThe efficacy of metformin for the treatment of obesity has been evaluated in few clinical trials and it shows that the patient loseweight in a year, including attempting life style modification.Ultimately, a combination of metformin and lorcaserin worked for the patient, who has since maintained a 50 lb weight loss.
When metformin used in a group of 10 patients, about seven of them either lose no weight or lose marginal amounts of weight, “But the three that do respond very dramatically. It may have something to do with central effects of metformin when it is able to get across the blood–brain barrier via the organic cation transporter (OCT2). [9]
HIV-ASSOCIATED DIABETESAntiretroviral therapies with protease inhibitors inhibit glucose transporter (GLUT)-4 mediated glucose transport.[10] They are likely to be, in part, responsible for the insulin resistance and body composition changes in HIV-infected patients. Metformin has been shown to reduce visceral adiposity and insulin resistance after 8 weeks of drug therapy at dose of 850 mg, 3 times per day. [11]
NEPHROTOXICITY PREVENTIONRecent studies have suggested that metformin may have therapeutic or renoprotective effects against nephrotoxic
agents. [10, 11] It has also been shown to have a good efficacy in diabetic nephropathy. Furthermore, it significantly decreases albuminuria in patients with diabetes mellitus. [12, 13, 14, 15, 16] However, the exact mechanism beyond these effects is still unknown. Recent studies have shown that therapeutic effect of metformin is mediated through its action on adenosine monophosphate (AMP)-activated kinase in tissues.[15,16 ,17,18,19,20] Various studies have shown that metformin is capable of decreasing intracellular reactive oxygen species (ROS).[17,18,19,20,21] It protects tubular injury through regulation of oxidative stress and restoring the biochemical alterations on renal tubules. Metformin may also protect the podocytes in diabetic nephropathy.[19, 20, 21, 22, 23]
CARDIOVASCULAR PROTECTIVE EFFECTS OF METFORMIN
Diabetic patients mainly die of cardiovascular complications,[24] including macrovascular complications (such as stroke, coronary artery disease [CAD] and myocardial infarction) and microvascular complications (such as kidney disease, retinal injury and peripheral nerve disease), of which approximately 70% of all diabetic patients die of heart and brain macrovascular diseases. In addition, a 10-year post-interventional follow-up of the UKPDS survivor cohort further examined that metformin treatment had a long-term benefit on cardiovascular risk in overweight patients. Compared with sulfonylurea and insulin treatment, metformin treatment can effectively reduce the risk of myocardial infarction and death.[25]
CANCER RELATED MORTALITY
Epidemiologic studies suggest that metformin use may be associated with both reduced cancer incidence and mortality. Although patients with diabetes had a higher risk for developing colon cancer, patients assigned metformin had a 27% reduced risk, according to researchers. Comparing patients with diabetes for less than 1 year, between 1 and 2 years, and at least 3 years with patientswithout diabetes, adjusted RRs were 1.308 (95% CI, 1.02 1.679), 1.087 (95%CI, 0.9 1.313) and 1.185 (95% CI, 1.055 1.33), respectively. The duration of metformin use showed an inverse trend, according to researchers, with an RR of 0.643 (95% CI, 0.49 0.845) in users for at least 3 years vs. nonusers.
“Metformin clearly affects AMP – activated protein kinase, which effect mitochondrial energy generation and may deprive malignant, inefficient cells of energy and therefore reduce their potential growth rate. Although some of the observations [with metformin] imply not just

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
48 © JIMI • JULY - SEPT 2019 • VOL. 13
[preventing] a progression of cancer but an incident of the cancer, which might suggest broader effect than merely energy deprivation. [26]
METFORMIN AND THYROID CANCER
It shows in the studies that metformin act as anti-proliferative effects on differentiated thyroid cancers when they examined 34 patients with differentiated thyroid cancer (DTC) taking metformin versus 21 non-metformin using patients, tumor size was smaller, and progression was slower in the metformin group. One of the theories in DTC response to metformin is the p70S6K/pS6 pathway that induces the cancer cell metabolic stress and the autophagy later. [27] Similar experimental findings shown that medullary thyroid cancer (MTC) cells found slowness of cellular progression in metformin-treated patients. They stated that cyclin D1 (usually overexpressed in cancer cells) was remarkably inhibited, through inhibition of mTOR/p70S6K/pS6 signaling and down-regulation of pERK. Out of this sophisticated process, they concluded metformin could have a potential additional role in treating MTC [28], therefore adding thyroid cancer to the list of cancers showing a decreased cancer-specific mortality with the use of metformin.
METFORMIN AND MELANOMA
An article in 2011 by Tomic et al entertained an additional anti-proliferative effect of metformin in addition to AMPK activation. The activation of the AMPK ends cell proliferation, and subsequently, apoptosis develops within 96 h. Interestingly this article illustrated two findings one is how metformin leads to phagocytosis of cells containing AMPK, which are malignantly mutated, whilst sparing the healthy cells containing AMPK. Secondly, metformin can reduce proliferation of tumor cells effectively in an AMPK-independent manner as well [29].
METFORMIN & THE BLOOD HOMEOSTASIS
It was mentioned earlier that metformin reduces the incidence of cardiovascular events in diabetes patients. This takes place through various cascades (glycemia and non-glycemia related cascades). Metformin, in high doses, was shown to various coagulation factors in humans. Metformin reduces the systemic production of the tissue type plasminogen activator, Von Willibrand factor, and plasminogen activator inhibitor [30]. In addition to that, metformin was found to modulate the fibrin threads formation; this takes place by reducing the factor XIII functions and structural modeling of the fibrin threads [31]. Nonetheless, metformin was found to reduce the levels of plasminogen activator inhibitor-1, and Von
Willibrand factor from the unhealthy endothelium in patients with no underlying diabetes mellitus [32].
METFORMIN AS AN ANTI-OXIDANT
This privilege is still to be explained by scientists. The hypotheses include lowering the reactive oxygen species, up-regulation of uncoupled protein 2 in the fat cells, as well as the AMPK system activation [33, 34, 35]. This as mentioned above reduces gluconeogenesis, and increase fatty acids metabolism, as well as B-oxidation in the fat tissues.
METFORMIN MODULATES THE BIOLOGY OF AGING
Metformin is a drug approved to treat diabetes but appears to target a number of aging-related mechanisms. Some mechanisms are relevant to glucose metabolism, but with respect to aging these may not be the most important ones. Metformin’s multiple aging-relevant actions at the cellular and organismal levels are depicted in figure 1.[36]
Specifically for aging, metformin leads to decreased insulin levels, decreased IGF-1 signaling[37],inhibition of mTOR [38], inhibition of mitochondrial complex 1 in the electron transport chain and reduction of endogenous production of reactive oxygen species (ROS) [39], activation of AMP-activated kinase (AMPK)[40], and reduction in DNA damage[41]. Metformin favorably influences metabolic and cellular processes closely associated with the development of age-related conditions, such as inflammation[42],autophagy[43], and cellular senescence[44]. In C. elegans metformin extends lifespan by several possible mechanisms including the alteration of the microbiome, specifically by changing microbial folate and methionine metabolism. [45]

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
49© JIMI • JULY - SEPT 2019 • VOL. 13
Figure 1 : Metformin Targets Multiple Pathways of Aging
The figure depicts schematically the current consensus within the biology of aging community as to pathways that are important in order to target aging and indicates at which points metformin has been shown to have effects (see text). Key take-away: outside of the cell (1, top), metformin has been shown to affect the receptors for cytokines, insulin, IGF-1, and adiponectin, all pathways that are activated with aging and, when modulated, are associated with longevity. (1) Intracellular (2,middle) metformin inhibits the inflammatory pathway and activates AMPK, increasing inhibition of mtor, which seems to be a major target to modulate aging. Through some of these mechanisms, it also modulates oxidative stress and removes senescent cells (the mitochondrial pathways are not shown, and the mechanisms by which metformin induces senescent cell removal remain unclear). (2) These processes jointly (3, bottom) affect inflammation, cellular survival, stress defense, autophagy, and protein synthesis, which are major biological outcomes associated with aging/longevity. [36
TABLE -1SUMMARY OF EFFECTIVE DOSE OF
METFORMIN IN STUDIESAntitumor effect of metformin
500mg/day.[46]The greater the metformin exposure, the stronger the risk reduction. [47]
Cardiovascular protective effects of metformin
Starting with one 850 mg tablet per day, then 850 mg twice a day, and then 1,700 mg in the morning and 850 mg with the evening meal (maximum dose =2,550 mg)[48] 1.4±0.2 g10
Polycystic ovary syndrome
Range from 850 to 1,700 mg
Neuroprotective effect of metformin
Starting with 0.5 g tablet, two tablets a day with meals. If the blood glucose level is not controlled for 7 days after taking metformin, it should be increased to 1.5 g/day over 2 weeks (maximum dose <2.0 g/day) [49] 1,000 mg twice a day. [50]
An Obesity Range from 850 to 1,700 mg
SUMMARY
Metformin is the most commonly prescribed therapy for patients with T2DM. It has a good safety profile and is associated with low cost. With further exploration of the clinical effect and possible mechanism of metformin, its indications have been extended to antitumor effect, HIV-associated diabetes, cardiovascular protective effects, neuroprotective effects, anti-oxidant, cancer and an optional treatment for PCOS.Beyond its impact on glycaemic control and diabetes-related outcomes, metformin has pleotropic effects targeting multiple age-related mechanismsalso. Furthermore, many questions such as whether these potential indications of metformin can be observed in non-diabetics and whether genetic factors have an influence on the effect of metformin need to be clarified by substantial basic experiments and clinical trials.
REFRENCE
1. Oluwaranti Akiyode, pharmd, rph, BCPS, CDE, can be reached at Howard University College of Pharmacy, 2300 Fourth St., NW, Washington, D.C. 20059~ email: [email protected]
2. Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes research and Clinical practice. 2012;97(3):359–67. 10.1016/j.diabres.2012.06.001 [pubmed] [crossref] [Google Scholar].
3. Group UPDS. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). The Lancet. 1998;352(9131):854–65. [pubmed] [Google Scholar].
4. Velazquez EM, Mendoza S, Hamer T, Sosa F, Glueck CJ. Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy. Metabolism. 1994;43(5):647–6.
5. Moghetti P, Castello R, Negri C, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab. 2000;85(1):139–146.
6. Glueck CJ, Wang P, Fontaine R, Tracy T, Sieve-Smith L. Metformin to restore normal menses in oligo-amenorrheic teenage girls with polycystic ovary syndrome (PCOS). J Adolesc Health. 2001;29(3):160–169.
7. Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
50 © JIMI • JULY - SEPT 2019 • VOL. 13
sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2012;5:CD003053.
8. Kahn BB, Alquier T, Carling D, Hardie DG. AMP-activated protein kinase: ancient energy gauge provides clues to modern understanding of metabolism. Cell Metab. 2005;1(1):15–25. Doi: 10.1016/j.cmet.2004.12.003. [pubmed] [crossref] [Google Scholar]
9. Sriram Machineni, MD, can be reached at Massachusetts General Hospital, 55 Fruit St., Boston, MA 02114~ email: [email protected].
10. Murata H, Hruz PW, Mueckler M. The mechanism of insulin resistance caused by HIV protease inhibitor therapy. J Biol Chem. 2000;275:20251–4. [pubmed] [Google Scholar]
11. Saint-Marc T, Touraine JL. Effects of metformin on insulin resistance and central adiposity in patients receiving effective protease inhibitor therapy. AIDS. 1999;13:1000–2. [pubmed] [Google Scholar]
12. Rafieian-Kopaei M, Nasri H. Ginger and diabetic nephropathy. J Ren Inj Prev. 2012;2:9–10. [PMC free article] [pubmed] [Google Scholar]
13. Baradaran A. Lipoprotein (a), type 2 diabetes and nephropathy; the mystery continues. J Nephropathol. 2012;1:126–9. [PMC free article] [pubmed] [Google Scholar].
14. Nasri H. Renoprotective effects of garlic. J Ren Inj Prev. 2012;2:27–8. [PMC free article] [pubmed] [Google Scholar]
15. Nasri H, Behradmanesh S, Maghsoudi AR, Ahmadi A, Nasri P, Rafieian-Kopaei M. Efficacy of supplementary vitamin D on improvement of glycemic parameters in patients with type 2 diabetes mellitus: A randomized double blind clinical trial. J Ren Inj Prev. 2014;3:31–4. [PMC free article] [pubmed] [Google Scholar].
16. Tavafi M. Complexity of diabetic nephropathy pathogenesis and design of investigations. J Ren Inj Prev. 2013;2:61–5. [PMC free article] [pubmed] [Google Scholar].
17. Behradmanesh S, Nasri P. Serum cholesterol and LDL-C in association with level of diastolic blood pressure in type 2 diabetic patients. J Ren Inj Prev. 2012;1:23–6. [PMC free article] [pubmed] [Google Scholar]
18. Rahimi Z. ACE insertion/deletion (I/D) polymorphism and diabetic nephropathy. J Nephropathol. 2012;1:143–51. [PMC free article] [pubmed] [Google Scholar]
19. Nasri H. Comment on: Serum cholesterol and LDL-C in association with level of diastolic blood pressure in type 2
diabetic patients. J Ren Inj Prev. 2012;1:13–4. [PMC free article] [pubmed] [Google Scholar]
20. Nasri H. Acute kidney injury and beyond. J Ren Inj Prev. 2012;21:1–2. [PMC free article] [pubmed] [Google Scholar].
21. Rouhi H, Ganji F. Effect of N-acetyl cysteine on serum Lipoprotein (a) and proteinuria in type 2 diabetic patients. J Nephropathol. 2013;2:61–6. [PMC free article] [pubmed] [Google Scholar].
22. Tavafi M. Diabetic nephropathy and antioxidants. J Nephropathol. 2013;2:20–7. [PMC free article] [pubmed] [Google Scholar].
23. Behradmanesh S, Derees F, Rafieian-kopaei M. Effect of Salvia officinalis on diabetic patients. J Ren Inj Prev. 2013;2:57–9. [PMC free article] [pubmed] [Google Scholar]
24. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603.
25. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589.
26. Andrew T. Chan, MD, MPH, can be reached at Massachusetts General Hospital, Gastrointestinal Unit, GRJ 722, 55 Fruit St., Boston, MA 02114~ email: [email protected].
27. Klubo-Gwiezdzinska J, Costello J Jr, Patel A, Bauer A, Jensen K, Mete M, Burman KD. Et al. Treatment with metformin is associated with higher remission rate in diabetic patients with thyroid cancer. J Clin Endocrinol Metab. 2013;98(8):3269–3279. Doi: 10.1210/jc.2012-3799. [pubmed] [crossref] [Google Scholar].
28. Klubo-Gwiezdzinska J, Jensen K, Costello J, Patel A, Hoperia V, Bauer A, Burman KD. Et al. Metformin inhibits growth and decreases resistance to anoikis in medullary thyroid cancer cells. Endocr Relat Cancer. 2012;19(3):447–456. Doi: 10.1530/ERC-12-0046. [pubmed] [crossref] [Google Scholar].
29. Tomic T, Botton T, Cerezo M, Robert G, Luciano F, Puissant A, Gounon P. Et al. Metformin inhibits melanoma development through autophagy and apoptosis mechanisms. Cell Death Dis. 2011;2:e199. Doi: 10.1038/cddis.2011.86. [PMC free article] [pubmed] [crossref] [Google Scholar].
30. Grant PJ. Beneficial effects of metformin on haemostasis and vascular function in man. Diabetes Metab. 2003;29(4

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
51© JIMI • JULY - SEPT 2019 • VOL. 13
Pt 2):6S44–52. [pubmed] [Google Scholar].
31. De Jager J, Kooy A, Lehert P, Bets D, Wulffele MG, Teerlink T, Scheffer PG. Et al. Effects of short-term treatment with metformin on markers of endothelial function and inflammatory activity in type 2 diabetes mellitus: a randomized, placebo-controlled trial. J Intern Med. 2005;257(1):100–109. Doi: 10.1111/j.1365-2796.2004.01420.x. [pubmed] [crossref] [Google Scholar].
32. Charles MA, Morange P, Eschwege E, Andre P, Vague P, Juhan-Vague I. Effect of weight change and metformin on fibrinolysis and the von Willebrand factor in obese nondiabetic subjects: the BIGPRO1 Study. Biguanides and the Prevention of the Risk of Obesity. Diabetes Care. 1998;21(11):1967–1972. Doi: 10.2337/diacare.21.11.1967. [pubmed] [crossref] [Google Scholar].
33. Kahn BB, Alquier T, Carling D, Hardie DG. AMP-activated protein kinase: ancient energy gauge provides clues to modern understanding of metabolism. Cell Metab. 2005;1(1):15–25. Doi: 10.1016/j.cmet.2004.12.003. [pubmed] [crossref] [Google Scholar].
34. Faure P, Rossini E, Wiernsperger N, Richard MJ, Favier A, Halimi S. An insulin sensitizer improves the free radical defense system potential and insulin sensitivity in high fructose-fed rats. Diabetes. 1999;48(2):353–357. Doi: 10.2337/diabetes.48.2.353. [pubmed] [crossref] [Google Scholar].
35. Anedda A, Rial E, Gonzalez-Barroso MM. Metformin induces oxidative stress in white adipocytes and raises uncoupling protein 2 levels. J Endocrinol. 2008;199(1):33–40. Doi: 10.1677/JOE-08-0278. [pubmed] [crossref] [Google Scholar].
36. The critical role of metabolic pathways in aging. Barzilai N, Huffman DM, Muzumdar RH, Bartke A, Diabetes. 2012 Jun; 61(6):1315-22.[pubmed] [Ref list].
37. Liu B, Fan Z, Edgerton SM, Yang X, Lind SE, Thor AD Cell Cycle. 2011 Sep 1; 10(17):2959-66.[pubmed] [Ref list].
38. Kickstein E, Krauss S, Thornhill P, Rutschow D, Zeller R, Sharkey J, Williamson R, Fuchs M, Köhler A, Glossmann H, Schneider R, Sutherland C, Schweiger sproc Natl Acad Sci U S A. 2010 Dec 14; 107(50):21830-5.[pubmed] [Ref list].
39. Batandier C, Guigas B, Detaille D, El-Mir MY, Fontaine E, Rigoulet M, Leverve XM J Bioenerg Biomembr. 2006 Feb; 38(1):33-42.[pubmed] [Ref list].
40. Cho K, Chung JY, Cho SK, Shin HW, Jang IJ, Park JW, Yu KS, Cho JY Sci Rep. 2015 Jan 30; 5():8145.[pubmed] [Ref list].
41. Algire C, Moiseeva O, Deschênes-Simard X, Amrein L, Petruccelli L, Birman E, Viollet B, Ferbeyre G, Pollak MN Cancer Prev Res (Phila). 2012 Apr; 5(4):536-43.[pubmed] [Ref list].
42. Saisho Y Endocr Metab Immune Disord Drug Targets. 2015; 15(3):196-205.[pubmed] [Ref list].
43. Song YM, Lee YH, Kim JW, Ham DS, Kang ES, Cha BS, Lee HC, Lee BW Autophagy. 2015; 11(1):46-59.[pubmed] [Ref list].
44. Jadhav KS, Dungan CM, Williamson DL Mech Ageing Dev. 2013 Nov-Dec; 134(11-12):548-59.[pubmed] [Ref list].
45. Cabreiro F, Au C, Leung KY, Vergara-Irigaray N, Cochemé HM, Noori T, Weinkove D, Schuster E, Greene ND, Gems D Cell. 2013 Mar 28; 153(1):228-39.[pubmed] [Ref list].
46. Lee MS, Hsu CC, Wahlqvist ML, Tsai HN, Chang YH, Huang YC. Type 2 diabetes increases and metformin reduces total, colorectal, liver and pancreatic cancer incidences in Taiwanese: a representative population prospective cohort study of 800,000 individuals. BMC Cancer. 2011;11:20. [PMC free article] [pubmed] [Google Scholar].
47. Landman GW, Kleefstra N, van Hateren KJ, Groenier KH, Gans RO, Bilo HJ. Metformin associated with lower cancer mortality in type 2 diabetes: ZODIAC-16. Diabetes Care. 2010;33(2):322–326. [PMC free article] [pubmed] [Google Scholar].
48. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34).UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):854–865. [pubmed] [Google Scholar].
49. Guo M, Mi J, Jiang QM, et al. Metformin may produce antidepressant effects through improvement of cognitive function among depressed patients with diabetes mellitus. Clin Exp Pharmacol Physiol. 2014;41(9):650–656. [pubmed] [Google Scholar].
50. Luchsinger JA, Perez T, Chang H, et al. Metformin in amnestic mild cognitive impairment: results of a pilot randomized placebo controlled clinical trial. J Alzheimers Dis. 2016;51(2):501–514. [PMC free article] [pubmed] [Google Scholar].

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
52 © JIMI • JULY - SEPT 2019 • VOL. 13
Tuberculous MyocarditisAmitesh Aggarwal1, Prabhat Gautam Roy2, Rohit Gupta3
ABSTRACT:
Tuberculous Myocarditis (TM) is defined as inflammation of the myocardium secondary to Mycobacterium tuberculosis infection. It is characterized by manifestations varying from acute fulminant conditions like arrythmias and sudden cardiac death to chronic presentations like slowly progressive heart failure and incidentally detected myocarditis during workup of disseminated tuberculosis (TB). TM carries a poor prognosis if not treated early in the course of disease. Even though considerable data is available on TM, it is scattered in the form of individual case reports. With this article we present a compiled data on TM which gives an overview of salient clinical features, course of illness, complications, diagnostic modalities and management of this disease. Such a document is desirable, both from a clinical point of view-since it will act as a ready reckoner for clinicians managing TM as well as from a research perspective where this document can be used as a baseline article for reference based on which further studies can be planned.
1. Associate Professor, Department of Medicine, University College of Medical Sciences & GTB Hospital, Delhi (Corresponding Author) Email: [email protected]
2. Post Graduate Student, Department of Medicine, University College of Medical Sciences & GTB Hospital, Delhi
3. Intern, Department of Medicine, University College of Medical Sciences & GTB Hospital, Delhi
METHODOLOGY
This report about TM is a Systematic Review. All articles published before May 2020 were considered for the review taking care to include only those studies which had ‘Humans’ as their patients and which were published in English language. No preference was given to any particular article type.
A PubMed search using the keywords ‘tuberculosis myocardium’ and ‘tuberculous myocarditis’ was conducted which yielded 337 articles in total. A comprehensive review of each article and their references was done taking care to exclude overlapping results. Forty three articles were selected as being highly relevant to the topic. Intervention in the form of treating the myocarditis was done in each patient by the respective authors. The outcomes were recorded and compiled. Due to lack of personal contact with either the patient or the author, we had to rely completely on the information given in these articles.
Review Article

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
53© JIMI • JULY - SEPT 2019 • VOL. 13
INTRODUCTION:
Tuberculosis (TB) accounted for 1.5 million deaths worldwide in 2018.1 It is one of the top ten leading causes of death worldwide. Cardiac tuberculosis is a rare disease affecting 1% of tuberculosis patients.2 Pericardium is most commonly involved structure in heart. Isolated tuberculous myocarditis is a rare entity. In 1664, Maurocadat reported the first ever case of isolated tuberculous myocarditis. He was followed by Morgagni who reported the second case nearly a century later in 1761. In 1987, Rose et al studied 19 cases of TB myocardium and estimated it’s prevalence to be 0.14%.3 Other studies have estimated the prevalence varying from 0.2 to 2%.3,4
It has been seen that tuberculosis generally spares pancreas, thyroid, heart and skeletal muscles.5 The constant movement of myocardium is suggested to be protective against lodging of tubercle bacilli in myocardium. Lactic acid production by muscular activity in heart has also been proposed to offer protection to cardiac muscle against tubercle bacilli.6 These factors make tuberculous myocarditis a rare entity.
PATHOLOGY
The most common method of myocardial involvement is by direct extension followed by retrograde lymphatic drainage from tubercular lymph nodes. Haematogenous spread may occur in those suffering from miliary TB.7
The right atrium is the most commonly affected area of myocardium due to its proximity to right mediastinal lymph nodes which are frequently affected.5
Histologically, three patterns of myocardial tuberculosis have been proposed by Horn and Saphir which are:
• Nodular tubercles or tuberculomas of myocardium varying from pea to egg size with central caseation,
• Miliary tubercles of myocardium complicating generalized miliary disease and
• The uncommon diffuse infiltrative type usually associated with tuberculous pericarditis in which the myocardium is diffusely infiltrated by granulation tissue containing giant cells, endothelial cells and lymphocytes.6
CLINICAL PRESENTATION
Myocardial tuberculosis is seldom diagnosed ante-mortem and most of the case reports and systematic reviews are based on autopsy results8.
The most common presentation of TM in our review (33% of total cases) was that of slowly progressive dyspnea,
pain in right hypochondrium, jaundice and pedal edema which is consistent with congestive heart failure. This was followed by rhythm disturbances (28% of total cases) like supraventricular arrhythmias, ventricular arrhythmias and varying degrees of conduction blocks. Third most common presentation (20% of total cases) was that of sudden cardiac death.
Around 7% patients were asymptomatic. Myocardial tuberculosis was detected in them as a part of workup of pulmonary tuberculosis. Another 7% presented with angina9. Other rare presentations included isolated right heart failure (5%), generalized lymphadenopathy with myocarditis (2%), right ventricular outflow tract obstruction (<1%), ventricular aneurysm (<1%), ventricular pseudo-aneurysm (<1%), aortic insufficiency (<1%) and coronary arteritis (<1%).5
DIAGNOSIS
Clinical Diagnosis
A diagnosis of myocarditis is suspected by taking a detailed history and conducting a comprehensive physical examination on the patient. Further, investigations like a 12 lead electrocardiogram, cardiac biomarkers and cardiac imaging in the form of echocardiography, coronary angiography and cardiac magnetic resonance imaging are usually conducted to confirm the diagnosis. There have been case reports highlighting the utility of 18-fluoro deoxyglucose positron emission tomography scan in diagnosing granulomatous myocarditis10. Rarely, a diagnosis can’t be reached upon even after the aforementioned investigations. In such instances endomyocardial biopsy is indicated to arrive at a diagnosis of myocarditis.
Etiological diagnosis
In a diagnosed case of myocarditis where Myocardial Tuberculosis is suspected, various biochemical and imaging studies may support the diagnosis and help in determining the extent of disease, however, the definitive diagnosis can only be made by Zeihl-Neelsen (ZN) staining of endomyocardial biopsy specimens.
Findings favouring tuberculous myocarditis include characteristic histological changes seen upon ZN Staining and demonstration of tuberculosis bacilli by culture or Polymerase Chain Reaction (PCR).11
Diagnostic criteria for Tubercular Myocarditis were proposed by Liu et al in 2012. Major criteria included positive PCR on myocardial tissue, positive TB culture from myocardial tissue sampling and positive acid fast

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
54 © JIMI • JULY - SEPT 2019 • VOL. 13
bacilli on myocardial tissue. Minor criteria included granulomata in myocardial tissue, miliary TB in more than one organ and positive radiological image (MRI). The presence of two major criteria or a major and two or more minor criteria justify the diagnosis of myocardial TB12.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of Tubercular Myocarditis include other causes of granulomatous myocarditis like sarcoidosis, fungal infections, syphilis, tularemia, brucellosis, Systemic Lupus Erythematosus, drug hypersensitivity, thyrotoxicosis, thymoma, inflammatory bowel disease, rheumatoid arthritis, rheumatic fever, Farber’s disease, gout and idiopathic giant cell myocarditis13.
TREATMENT
Treatment of TB myocarditis is aimed at achieving two major goals: Treating Myocarditis and Treating Tuberculosis.
Treatment of Myocarditis
Treatment of myocarditis includes general nonspecific measures to treat the sequelae of heart disease which include treatment for heart failure (HF), arrhythmias, and in select cases, anticoagulation14.
Candidacy for cardiac transplantation should be considered in patients with chronic myocarditis presenting as an intractable cardiomyopathy with refractory HF15.
Patients with TB myocarditis can develop arrhythmias. Because these arrhythmias often resolve after the acute phase of myocarditis, therapy is generally supportive. Electrocardiographic monitoring can permit early detection of asymptomatic yet potentially life-threatening arrhythmias and/ or conduction defects.
Implantable Cardioverter Defibrillator (ICD) implantation is generally deferred in patients with acute myocarditis since myocarditis and arrhythmia risk may resolve. A potential role for a wearable cardioverter-defibrillator for patients at risk for sudden cardiac arrest has been suggested but the evidence to support such therapy is scanty16.
Indications for anticoagulation in patients with myocarditis include standard general indications such as evidence of systemic embolism or presence of acute left ventricular thrombus.
Treatment of Tuberculosis
No separate guidelines for therapy are available for
myocardial tuberculosis and most of the available studies have treated their patients using regimens validated for commoner forms of cardiac tuberculosis (Pericardial TB). A commonly used regime includes 2 months of Isoniazid, Rifampicin, Pyrazinamide and Ethambutol followed by 4 months of Isoniazid, Rifampicin and Pyrazinamide17.
Response to treatment is assessed at 4 months from initiation of Anti-tubercular therapy. Treatment failure is considered in patients who deteriorate after initial improvement – this requires diagnostic investigations, a drug sensitivity testing and warrants a change of treatment. However, it must be appreciated that deterioration in the first 3 months may be due to a paradoxical reaction to treatment and this does not require repeat diagnostic tests or a change of treatment.
Role of corticosteroids is controversial. However, it may be given to patients developing pericardial effusion who also have concomitant TB Pericarditis. Pericardiocentesis is indicated as an urgent intervention if pericardial effusion progresses to Cardiac tamponade and impedes venous return to the heart. Few case reports suggest high chances for successful treatment if treatment is started well in time18.
Surgical intervention in the form of Pericardectomy is sometimes indicated in patients who develop constrictive pericardial disease as a late complication. Some of these patients may improve without surgery, but others may develop progressive cardiac failure and require Pericardectomy.17
CONCLUSION
Tuberculous myocarditis is a rare manifestation of tuberculosis which is characterized by presentations varying from acute fulminant conditions like arrythmias and sudden cardiac death to chronic conditions like slowly progressive heart failure and incidentally detected myocarditis during workup of disseminated tuberculosis. Diagnosis depends on demonstration of Mycobacterium tuberculosis and characteristic histological findings on myocardial biopsy, suggestive changes on cardiac MRI and evidence of concomitant spread of TB to other organs. TM carries a poor prognosis if not treated early in the course of disease. Besides general measures comprising treatment for heart failure and arrythmias, treatment for TM includes 2 months of Isoniazid, Rifampicin, Pyrazinamide and Ethambutol followed by 4 months of Isoniazid, Rifampicin and Pyrazinamide. Role of corticosteroids is controversial. Surgical intervention in the form of pericardiectomy may be reserved for patients who develop complications like constrictive pericarditis.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
55© JIMI • JULY - SEPT 2019 • VOL. 13
REFERENCES:
1. Tuberculosis [Internet]. [cited 2020 May 17]. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
2. Fowler NO. Tuberculous pericarditis. Jama 1991; 266:99-103.
3. Rose AG. Cardiac tuberculosis. A study of 19 patients. Archives of pathology & laboratory medicine 1987; 111:422-6.
4. Fairley CK, Ryan M, Wall PG, Weinberg J. The organisms reported to cause infective myocarditis and pericarditis in England and Wales. The Journal of infection 1996; 32:223-5.
5. Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D. Tuberculous dilated cardiomyopathy: an under-recognized entity? BMC infectious diseases 2005; 5:29.
6. Horn H, Saphir O. The involvement of the myocardium in tuberculosis: a review of the literature and report of three cases. Am Rev Tuberc 1935; 32:492-506.
7. Wallis P, Branfoot A, Emerson P. Sudden death due to myocardial tuberculosis. Thorax 1984; 39:155-6.
8. Kumar S, Bhutani N, Kataria SP, Sen R. Tuberculous myocarditis on autopsy: a rare underdiagnosed entity. Cardiovasc Pathol. 2018 Nov 1; 37:5–7.
9. Cowley A, Dobson L, Kurian J, Saunderson C. Acute myocarditis secondary to cardiac tuberculosis: a case report. Echo Res Pract. 2017 Sep; 4(3):K25–9
10. Danwade TA, Devidutta S, Shelke AB, Saggu DK, Yalagudri SD, Sridevi C, et al. Prognostic value of fluorine-18 fluoro-2-deoxyglucose positron emission computed tomography
in patients with unexplained atrioventricular block. Hear Rhythm. 2018 Feb 1; 15(2):234–9
11. Khurana R, Shalhoub J, Verma A, et al. presenting with ventricular tachycardia. Nature Reviews Cardiology 2008; 5:169.
12. Liu A, Hu Y, Coates A. Sudden cardiac death and tuberculosis–how much do we know? Tuberculosis 2012; 92:307-13.
13. Kanchan T, Nagesh K, Lobo F, Menezes R. Tubercular granuloma in the myocardium: an autopsy report. Singapore Med J 2010; 51:e15-e7.
14. Caforio ALP, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, Felix SB, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013; 34(33):2636–48.
15. O’Connell JB, Breen TJ, Hosenpud JD. Heart transplantation in dilated heart muscle disease and myocarditis. Eur Heart J. 1995; 16:137–9.
16. Prochnau D, Surber R, Kuehnert H, Heinke M, Klein HU, Figulla HR. Successful use of a wearable cardioverter-defibrillator in myocarditis with normal ejection fraction. Clin Res Cardiol. 2010; 99(2):129-31.
17. Sharma SK, Ryan H, Khaparde S, Sachdeva KS, Singh AD, Mohan A, et al. Index-TB guidelines: Guidelines on extrapulmonary tuberculosis for India. Indian J Med Res. 2017; 145(April):448–63.
18. Al-Jahdali F, Al-Harbi A, Baharoon S, Al-Gamdi M, Al-Jahdali H. Tuberculous myocarditis is not always fatal: Report of three confirmed cases with uneventful outcome. Int J Mycobacteriology. 2017 Jan 1; 6(1):111–5.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
56 © JIMI • JULY - SEPT 2019 • VOL. 13
Tuberculosis in Diabetes Mellitus : A Systematic ReviewYakshita Goyal1, Chahat Saini2, Surbhi Khanna3, Shivam Nagpal4, Ashish Goel5
ABSTRACT:Introduction: Diabetes mellitus and tuberculosis are major killer of mankind across the globe. The rising prevalence of diabetes is a potential threat to tuberculosis control. It shows some significant changes to clinical feature like involvement of lower lobe of lung and make management more complicated as metformin resist the cellular growth but still fatality rate is high when comes together.
Methodology: A systematic literature search performed during January 2020 in compliance with article selection process was based on Preferred Reporting Item for Systemic review & Meta Analyses (PRISMA). 141 articleswere found from which 24 article were selected after applying inclusion and exclusion criteria.
Observation: Diabetes mellitus and tuberculosis account for major burden of health globally, affecting millions of lives. Their co-occurrence is even more dangerous, by perpetuating each other’s progression, leading to significant morbidity and mortality. The increased susceptibility at acquiring the infection, becoming more prone for dissemination and leading to enhanced chances of treatment failure and mortality has been linked to an impaired immune system in the diabetics and poor sugar control lies at its epicentre. This has been attributed to increased number and severity of symptoms like cough, dyspnea, fever, night sweats and weight loss. The radiographic profile showed lower lung involvement and multiple cavities as opposed to upper lung involvement in conventional cases. InDiabetic patients receiving Metformin, the cellular growth of bacteria was found to be inhibited but itseffect on response of standard tuberculosis drugs like Rifampicinwas found to be variable.
Key word: Diabetes mellitus, tuberculosis
1,2,3,4.University College of Medical Sciences, University of Delhi, Dilshad Garden, Delhi-110095, India.
5. Department of Medicine, University College of Medical Sciences, University of Delhi, Dilshad Garden, Delhi-110095, India. (Corresponding Author) Email: yakshita [email protected]
INTRODUCTION:
Diabetes mellitus and tuberculosis are major killers of mankind across the globe.(1) Globally, an estimated 10.0 million (range, 9.0–11.1 million) people fell ill with tuberculosis in 2018, a number that has been relatively stable in recent years. There were an estimated 1.2 million (range, 1.1–1.3 million) tuberculosis deaths among HIV-negative people in 2018 (a 27% reduction from 1.7 million in 2000), and an additional 251 000 deaths among HIV positive people (a 60% reduction from 620 000 in 2000).(2)
WHO estimates that, globally, 422 million adults aged over 18 years were living with diabetes in 2014.(3) The largest numbers of people with diabetes were estimated for the WHO South-East Asia and Western-Pacific Regions accounting for approximately half the diabetes cases in the world. Worldwide, the number of people with diabetes has substantially increased between 1980 and 2014, rising from 108 million to current numbers that are around four
times higher. Forty per cent of this increase is estimated to result from population growth and ageing, 28% from a rise in age-specific prevalence, and 32% from the interaction of the two. The global prevalence of diabetes has grown from 4.7% in 1980 to 8.5% in 2014, during which time prevalence has increased or at best remained unchanged in every country.(3)
About 95% of tuberculosis and 75% of the diabetes cases live in low and middle-income countries. The rising prevalence of diabetes is a potential threat to tuberculosis control. Poorly controlled diabetes increases the risk of tuberculosis and leads to unfavourable treatment outcomes.(4)especially in low-to-middle income countries where tuberculosis (TB(5) There is robust evidence to support an association between diabetes mellitus and tuberculosis. A recent meta-analysis showed that diabetes increases the risk of tuberculosis development three-fold compared to non-diabetic.(6) This association was confirmed as early
Review Article

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
57© JIMI • JULY - SEPT 2019 • VOL. 13
as in 1934, when Root found that adolescents with diabetes contracted tuberculosis ten times more frequently.(7)
The absolute number of tuberculosis cases has been falling since 2006 and dropped at a rate of 2.2% between 2010 and 2011.(8) The prevalence of diabetes is projected to double from 171 million in 2000 to 552 million patients in 2030.(9) Half of people with diabetes are undiagnosed and the vast majority of the diabetic population lives in the ‘developing world’ countries which are well known to be endemic for tuberculosis. In view of the steady rise in diabetes worldwide, especially in these low-income countries, the importance of the TB-DM association cannot be overemphasized. In the year 2000 developing countries were expected to share around 67% of the global diabetes burden.(9)
A country with one of the largest number of tuberculosis cases is India. In this highly endemic country, over 25% of tuberculosis patients were found to have diabetes and 24% pre-diabetes.(10) Altogether almost 50% of tuberculosis patients had some form of hyperglycaemia. The odds ratio (OR) for diabetes was estimated as 3.06 (95% CI: 1.69–5.52, p < 0.001) and was especially high for positive smear patients. Of interest, among tuberculosis patients with diabetes, almost 60% had been diagnosed with diabetes before. It is most likely that long-term diabetes has a negative effect on the immune response and may enhance tuberculosis morbidity. In another study from India, the number of tuberculosis patients needed to screen (NNS) to find one newly diagnosed diabetic case was 4.(11) In another retrospective study from India, diabetes was found as the most frequent risk factor for pulmonary tuberculosis, far more common (30.9%) than classic risk factors for tuberculosis such as smoking (16.9%), alcoholism (12.6%), human immunodeficiency virus (HIV) (10.6%), malignancy (5.8%) as well as history of contact with tuberculosis (3.4%) and chronic corticosteroid therapy (2.9%).(12)alcoholism (12.6% The strength of diabetes as a risk factor for tuberculosis appears to be equivalent to that of HIV infection. In a case-control study conducted in California, Pablos-Mendez et al. found that among Hispanics aged 25–54 the estimated risk due to diabetes was 25.2% whereas that due to HIV infection was 25.5%.(13)and 37 366 control subjects who had a primary discharge diagnosis of deep venous thrombosis, pulmonary embolism, or acute appendicitis. Risk of tuberculosis was estimated as the odds ratio (OR Here, we discuss diverse findings ranging from in vitro studies to clinical research, which support the connection between diabetes progression and tuberculosis susceptibility in a metabolic-dependent way and present a global connection of feasible events that may occur during this comorbidity, which might create
an appropriate environment to tuberculosis infection, and we also present evidences of the role of the treatment of diabetes on this response.PATHOLOGY
The increased risk of acquiring a primary infection or reactivation of a latent infection, increased chances of dissemination and an increase in treatment failure in diabetic patients has been attributed to a compromised immune system.(14).
A competent immune system works to suppress the Mycobacterium growth and replication, prevent its dissemination and kill the bacilli.(15) The effective communication between the immune cells for attaining migration to concerned site and performing specific functions is made possible by the cytokines and chemokines released when the host immune cells like the macrophages, by virtue of their recognition receptors, interact with the inhaled bacilli and it has been seen that diabetes mellitus affects the course of tuberculosis by affecting this aspect.
In diabetes, the hyperglycemia lies at the heart of an impaired immune system.(16) When glucose is in excess, it is shunted to the polyol pathway instead of being oxidized. The polyol pathway is a two-step process where glucose is first converted to sorbitol by aldose reductase, with NADPH as the co-factor for it. Sorbitol dehydrogenase with NAD+ as its co-factor, ultimately converts it to fructose, a more potent nonenzymatic glycation agent than glucose.(25) This promotes the non-enzymatic glycosylation of proteins and matrix molecules, leading to the formation of Advanced Glycation End Products(AGE).(17) Additionally, the excess glucose forms diacylglycerol (DAG) in the cell, which can cause protein kinase-C (PKC) activation.(25)
This has multiple consequences; stimulation of NF-κB pathway and an increase in TGF-β being the prominent ones.(25) The cellular receptor of TGF-β autophosphorylates its Smad 2 and Smad 3 subunits, which then forms a heterodimer with the Smad 4 subunit. The heterodimer is translocated to the nucleus to down regulate the genes of glutamine-cysteine ligase (GCL); the rate limiting enzyme for glutathione synthesis and its modifier protein. To compensate for the decreased glutathione synthesis, an increased levels of glutathione reductase is seen in diabetic subjects. But this ultimately proves to be futile as its co-factor, NADPH, is diverted towards the polyol pathway.
Glutathione deficiency stimulates the NF-κB pathway further, leading to the production of IL-1, IL-6 and TNF-α. Normally, IL-6 helps in proper functioning of the macrophages.(18) Similarly, TNF-α has a crucial role

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
58 © JIMI • JULY - SEPT 2019 • VOL. 13
in the granuloma formation to contain the bacilli and suppress its growth and replication. But the cytokines and the chemokines cannot be grouped rigidly as either beneficial or harmful. A desired effect is achieved by the right amount at the correct time and site. Hence, the shifting of the balance between an anti-inflammatory and a pro-inflammatory state towards the latter leads to a disarray and malfunction of the immune response.(13)
IL-1 and IL-6, being pro-inflammatory, exacerbate the inflammation.(14)phagocytic activity, and cellular activation which results in impaired production of chemokines and cytokines. The initiation of adaptive immunity is delayed by impaired antigen-presenting cell (APC This is assisted by the AGE-RAGE binding as it starts a cascade of NF-κB pathway activation and reactive oxygen species generation (ROS). Moreover, the NADH produced as a by-product of polyol pathway acts as a substrate for NADH oxidase, causing an additional increase in the ROS.(25) Thus, in the wake of GSH deficiency, an oxidative stress ensues, leading to tissue damage, bacterial escape and dissemination. The role of GSH deficiency is further strengthened by its negative impact on vitamin D binding protein and receptor expression as the activation of vitamin D by
the bacilli-macrophage interaction induces transcription of human cathelicidin and β-defensin, which are crucial for the mycobactericidal activity.(25) The killing ability is additionally hampered by the ineffective migration of the neutrophils through the glycated collagen due to the AGE-RAGE binding with the collagen.(14)
Impaired immune cells also implicate that the dendritic cells, a link between innate and adaptive immunity are not able to effectively activate the naïve T-cell conversion to TH
1 cell, upon draining into the lymph nodes. Even
here, the GSH deficiency contributes by shifting the bias towards conversion into TH
2 cells.(14) IL-4 , thus secreted
by TH2 cells antagonizes the differentiation of TH
1 and
TH17
cells resulting in a defective interferon (IFN-γ) mediated killing of the bacilli by the macrophages.(18) Henceforth, a rapid progression of the disease occurs before the proper development of adaptive immunity. Additionally, the impact of hyperglycemia is also seen in the humoral response as the glycation of antibodies cause a loss of their biological functions.(14)
Hence, it can be appreciated that at the core of the TB-DM comorbidity lies a disturbed immunological system which, altered by the metabolic state of diabetes mellitus, starts acting against the host. (Figure 1)

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
59© JIMI • JULY - SEPT 2019 • VOL. 13
CLINICAL FEATURES
The increase in the number of tuberculosis cases in the diabetic population has been attributed to a poor control of blood sugar in diabetics.(19) A descriptive observational study by Ogbera et al in Nigeria in 2011-12 signifies the importance of immunosuppression in diabetes in the reactivation of latent TB infection and recurrent tuberculosis as a consequence.(20)
A higher BMI commonly associated with diabetics also plays a role in modifying the clinical picture of the affected population.(18) TB in diabetic patients usually presents with greater number and severity of symptoms like cough, hemoptysis, dyspnoea, fever, night sweats and weight loss. In a retrospective analysis of 692 tuberculosis patients by Skowronski et al, DM-TB patients presented to the hospital earlier due to increased severity of symptoms and enhanced pulmonary involvement leading to a shorter incubation period and making it easy to detect.(18)
Radiographic picture of tuberculosis in the presence of diabetes has shown lower lung involvement more commonly in contrast to upper lung being affected in a patient suffering from TB alone.(19) In a systematic review by Dooley et al lower lung involvement in DM-TB patients, 20% patients were found to have this type of finding, while other studies suggested this proportion to be as low as 1.8% (8 of 438 patients) and 8.3% (1 of 12 patients).(19) This finding can be attributed to the fact that Mycobacterium tuberculosis prefers high oxygen tension for its growth and replication and the lower lobes have a higher alveolar oxygen pressure in elderly and diabetics thus serving as a favourable ground.(18) Also, the lung is affected diffusely and not a specific local involvement.(21) Diabetes also increases the chances of multiple cavities in the lungs of the patients.(19)
The risk of treatment failure came out to be 3.9 times more in DM-TB patients than in patients with TB alone in a study in Egypt where 119 patients with treatment failure were compared to 119 controls.(19) Treatment failure and death as a consequence was seen in 41% of DM-TB patients and 13% of only TB patients in a descriptive case- control study.(19) Out of the total deaths in DM-TB patients, 87.5% (7 out of 8) died due to respiratory failure and 12.5% (1 out of 8) due to diabetic coma.(19)
TREATMENT
Duration of treatment
According to WHO guidelines 2019 for treatment of tuberculosis. Treatment is divided into two phases 1. Intensive for two months 2. Continuous phase for four
months which varies with type of resistivity same for drugs.
DM-TB patients and TB alone patients showed similar sputum-culture conversion proportions after two months of treatment in one of the studies. In Saudi Arabia, out of 692 smear positive TB patients, after 3 months, sputum cultures were found to be negative in 98.9% of DM-TB patients and 94.7% of patients with TB alone. But when time to sputum culture conversion was assessed various studies revealed that negativity appeared late in patients with diabetes. Similar observation was seen in a study by Dooly et al in Turkey where sputum culture conversion time was more in DM-TB patients.(19) This higher smear positivity can be attributed to immune suppression seen in diabetes.(18)
Agent of choice
Worldwide there are some standard drugs for tuberculosis like metformin and for type 2 diabetes it is metformin.
Diabetes makes it quite challenging and difficult to treat tuberculosis. Metformin prescription evidently lowers the risk of TB in patient with diabetes. Metformin is first line drug for type-2 DM therefore it could be used to improve treatment outcomes. It may shorten the standard course duration of anti-tuberculosis therapy & lower the ability of drug resistance by limiting the cellular growth of Mycobacterium tuberculosis by acting on AMPK (adenosine monophosphate activated phosphokinase) anti tuberculosis effect the risk of tuberculosis is still nebulous. After analysing different articles, it is found that TB mortality could be reduced by metformin usage (OR, 0.47; 95%CI, 0.27 to 0.83), and the sputum culture conversion at two months of TB disease was highly favourable in metformin users compared to non-users (OR, 2.72; 95%CI, 1.11 to 6.69). Contrarily, the pooled result of the relapse of TB within 3 years was not statistically different (OR, 0.55; 95% CI, 0.04 to 8.25) between the metformin group and the control group.(22)
DM-TB patients increase chances of TB transmission in low-TB burden countries and after observing broader cross sectional and prospective data it found that it may help in assessing the feasibility and cost effectiveness of DM-TB bi-directional screening.(23
In a descriptive case-control study by Dooley and colleague, it was found that treatment failure was seen in 41% of the patients who had diabetes but reduce to 13% in alone case tuberculosis. Out of eight patient those who died in DM-TB group, seven patients died due to pulmonary failure while one due to diabetic coma.(19)

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
60 © JIMI • JULY - SEPT 2019 • VOL. 13
Rifampicin is a key drug used in tuberculosis treatment. It is found in a study by Jacob et al during December 2017 it reaches its recommended dose in both cases either Tuberculosis alone or tuberculosis with diabetes mellitus. Therefore requisite to use high doses of rifampicin & perform routine check-up & proper follow up of serum level. (24)
REFERENCES:
1. Syal K, Srinivasan A, Banerjee D. VDR, RXR, Coronin-1 and Interferonã Levels in PBMCs of Type-2 Diabetes Patients: Molecular Link between Diabetes and Tuberculosis. Indian J Clin Biochem. 2015 Jul 17;30(3):323–8.
2. WHO | Global tuberculosis report 2019. WHO. 2020;
3. Zhou B, Lu Y, Hajifathalian K, Bentham J, Di Cesare M, Danaei G, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. Lancet [Internet]. 2016 Apr [cited 2020 Feb 6];387(10027):1513–30. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673616006188
4. Jeon CY, Murray MB, Baker MA. Managing tuberculosis in patients with diabetes mellitus: Why we care and what we know. Vol. 10, Expert Review of Anti-Infective Therapy. 2012. p. 863–8.
5. Riza AL, Pearson F, Ugarte-Gil C, Alisjahbana B, Van de Vijver S, Panduru NM, et al. Clinical management of concurrent diabetes and tuberculosis and the implications for patient services. Vol. 2, The Lancet Diabetes and Endocrinology. Lancet Publishing Group; 2014. p. 740–53.
6. Jeon CY, Murray MB. Diabetes Mellitus Increases the Risk of Active Tuberculosis: A Systematic Review of 13 Observational Studies. Williams B, editor. PLoS Med [Internet]. 2008 Jul 15 [cited 2020 Feb 6];5(7):e152. Available from: http://dx.plos.org/10.1371/journal.pmed.0050152
7. Root H. The association of diabetes and tuberculosis. N Engl J Med 1934; 210: 1-13. - Google Search [Internet]. [cited 2020 Feb 6]. Available from: https://www.google.com/search?q= Root+H.+The+association+ of+diabetes+and+tuberculosis.+N+Engl+J+Med+1934%3B+210%3A+1-13.&rlz=1C5CHFA_enIN844IN844&oq=Root+H.+ The+association+of+diabetes+and+tuberculosis.+ N+Engl+J+Med+1934%3B+210%3A+1-13.&aqs= chrome..69i57.1702j0j4 & sourceid=chrome & ie=UTF-8
8. World Health Organization. Global Tuberculosis Report. WHO report 2012, Geneva 2012.-Google Search [Internet]. [cited 2020 Feb 6]. Available from: https://www.google.
com/search?q=World+Health+Organization.+Global+ Tuberculosis+Report .+WHO+report+2012%2C+ Geneva+2012.&rlz=1C5CHFAenIN844IN844&oq= World+Health+Organization.+Global+Tuberculosis+ Report. + WHO+report+2012%2C+Geneva+2012. & aqs= chrome..69i57.733j0j9 & sourceid=chrome&ie=UTF-8
9. IDF Diabetes atlas. 5th ed. International Diabetes Feder- ation, Brussels 2012.-Google Search [Internet]. [cited 2020 Feb 6]. Available from:https://www.google.com/search?q=IDF+Diabetes+atlas.+5th+ed.+ International+Diabetes+Feder-+ation%2C+Brussels +2012. & rlz=1 C5CHFA_enIN844IN844 & oq=IDF+ Diabetes+atlas.+5th+ed. +International+ Diabetes+ Feder-+ation%2C+Brussels+2012. & aqs=chrome..69i57.658j0j9 & sourceid=chrome & ie=UTF-8
10. Ferlita S, Yegiazaryan A, Noori N, Lal G, Nguyen T, To K, et al. Clinical Medicine Type 2 Diabetes Mellitus and Altered Immune System Leading to Susceptibility to Pathogens, Especially Mycobacterium tuberculosis. [cited 2020 Jan 30]; Available from: www.mdpi.com/journal/jcm
11. Balakrishnan S, Vijayan S, Nair S, Subramoniapillai J, Mrithyunjayan S, Wilson N, et al. High Diabetes Prevalence among Tuberculosis Cases in Kerala, India. Gordon S V., editor. PLoS One [Internet]. 2012 Oct 15 [cited 2020 Feb 6];7(10):e46502. Available from: https://dx.plos.org/10.1371/journal.pone.0046502
12. Gupta S, Shenoy VP, Mukhopadhyay C, Bairy I, Muralidharan S. Role of risk factors and socio-economic status in pulmonary tuberculosis: A search for the root cause in patients in a tertiary care hospital, South India. Trop Med Int Heal. 2011 Jan;16(1):74–8.
13. Pablos-Méndez A, Blustein J, Knirsch CA. The role of diabetes mellitus in the higher prevalence of tuberculosis among Hispanics. Am J Public Health. 1997;87(4):574–9.
14. Ayelign B, Negash M, Genetu M, Wondmagegn T, Shibabaw T. Immunological Impacts of Diabetes on the Susceptibility of Mycobacterium tuberculosis. Vol. 2019, Journal of Immunology Research. Hindawi Limited; 2019.
15. Kumar NP, Banurekha V V., Nair D, Sridhar R, Kornfeld H, Nutman TB, et al. Coincident pre-diabetes is associated with dysregulated cytokine responses in pulmonary tuberculosis. PLoS One. 2014 Nov;9(11).
16. Podell BK, Ackart DF, Obregon-Henao A, Eck SP, Henao-Tamayo M, Richardson M, et al. Increased severity of tuberculosis in guinea pigs with type 2 diabetes: A model of diabetes-tuberculosis comorbidity. Am J Pathol. 2014;184(4):1104–18.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
61© JIMI • JULY - SEPT 2019 • VOL. 13
17. Nowotny K, Jung T, Höhn A, Weber D, Grune T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Vol. 5, Biomolecules. MDPI AG; 2015. p. 194–222.
18. Skowroñski M, Zozuliñska-Ziólkiewicz D, Barinow-Wojewódzki A. Tuberculosis and diabetes mellitus - An under appreciated association. Arch Med Sci. 2014 Oct;10(5):1019–27.
19. Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. 2009 Dec;9(12):737–46.
20. Ogbera AO, Kapur A, Abdur-Razzaq H, Harries AD, Ramaiya K, Adeleye O, et al. Clinical profile of diabetes mellitus in tuberculosis. BMJ open diabetes Res care. 2015;3(1):e000112.
21. Dousa KM, Hamad A, Albirair M, Al Soub H, Elzouki A-N, Alwakeel MI, et al. Impact of Diabetes Mellitus on the Presentation and Response to Treatment of Adults With Pulmonary Tuberculosis in Qatar. Open forum Infect Dis. 2019 Jan;6(1):ofy335.
22. Yu X, Li L, Xia L, Feng X, Chen F, Cao S, et al. Impact of metformin on the risk and treatment outcomes of
tuberculosis in diabetics: a systematic review. BMC Infect Dis [Internet]. 2019/10/19. 2019;19(1):859. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6796338/pdf/12879_2019_Article_4548.pdf
23. Sane Schepisi M, Navarra A, Altet Gomez MN, Dudnyk A, Dyrhol-Riise AM, Esteban J, et al. Burden and Characteristics of the Comorbidity Tuberculosis-Diabetes in Europe: TBnet Prevalence Survey and Case-Control Study. Open Forum Infect Dis [Internet]. 2019/01/31. 2019;6(1):ofy337. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6330516/pdf/ofy337.pdf
24. Perea-Jacobo R, Muniz-Salazar R, Laniado-Laborin R, Cabello-Pasini A, Zenteno-Cuevas R, Ochoa-Teran A. Rifampin pharmacokinetics in tuberculosis-diabetes mellitus patients: a pilot study from Baja California, Mexico. Int J Tuberc Lung Dis. 2019 Sep;23(9):1012–6.
25. Ferlita S, Yegiazaryan A, Noori N, Lal G, Nguyen T, To K, et al. Clinical Medicine Type 2 Diabetes Mellitus and Altered Immune System Leading to Susceptibility to Pathogens, Especially Mycobacterium tuberculosis.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
62 © JIMI • JULY - SEPT 2019 • VOL. 13
Early Detection - Need of The Hour: A Case Report of Swallowed Fishbone causing Pneumomediastinum
Amitesh Aggarwal1, Rakshit R. Bhardwaj2
ABSTRACT:
Background: Accidental ingestion of fishbone is a common condition in fish eating communities. Majority (of the ingested foreign bodies usually pass through the gastrointestinal tract spontaneously, without complications while 10%-20% require endoscopic interventions and about 1% of them require surgery.Case report: A 30-year male patient with intellectual disability and seizure disorder was brought to the medical emergency with 2-day history of fever, recurrent vomiting and left sided neck pain and swelling. On probing, there was history of fishbone ingestion 10 days back for which X-ray lateral neck was found normal and he was reassured and sent home. The case complicated to develop oesophageal perforation and pneumomediastinum leading to sepsis and death of the patient.Why should an emergency physician be aware of this? A high level of suspicion, diligent search and timely intervention can make a difference between life and death.
1. Department of Medicine, University College of Medical Sciences & GTB Hospital, Delhi, India (Corresponding Author) Email: [email protected]
2. Department of Medicine, University College of Medical Sciences & GTB Hospital, Delhi, India
INTRODUCTION:
Accidental ingestion of fishbone is a common condition in fish eating communities. Majority (about 90%) of the ingested foreign bodies usually pass through the gastrointestinal tract spontaneously, without complications while 10%-20% require endoscopic interventions and about 1% of them require surgery.1,2,3 There are many case reports of fishbone causing complications such as penetration of oesophagus, gastric4, small bowel5 and colonic perforation6, retropharyngoesophageal abscess7, epidural abscess8, mediastinal abscess9 and even penetrating the atrium10 or the pericardium11. A high level of suspicion, diligent search and timely intervention can make a difference between life and death. We report the present case of oesophageal perforation leading to pneumomediastinum due to fishbone.
CASE PRESENTATION:
A 30-year-old male patient, known case of mental retardation with seizure disorder, presented to emergency
with complaints of fever since 2 days, generalized weakness, recurrent vomiting following meals, left sided neck pain and swelling and associated difficulty in deglutition. He was conscious and co-operative at presentation. General examination revealed tachypnoea and left sided neck swelling with crepitus on palpation. Rest of Systemic examination was normal. Laboratory examination revealed Hb-12.0g/dl, thrombocytopenia (Plt-18,000/μl), a blood urea of 159mg/dl and creatinine of 5.7mg/dl. Urine routine showed 2+ albuminuria with 6-8 pus cells. Chest X-ray showed possible superior mediastinal widening. On further probing, a history of fishbone ingestion about 10 days back was revealed. He had then been to a doctor and an X-ray neck lateral view was done but no foreign body was visualized and hence was sent home with a possibility of spontaneous expulsion.
An immediate ENT examination was done which revealed pus pointing on left side of posterior pharyngeal wall on indirect laryngoscopy. An urgent NCCT neck was then
Case Report

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
63© JIMI • JULY - SEPT 2019 • VOL. 13
performed which showed a foreign body (? fishbone) at C7 vertebral level of oesophagus with subcutaneous emphysema.
Subsequently patient developed hypotension with multi-organ failure and died within few hours.
Figure 1. Image of the foreign body penetrating through the oesophagus at C7 vertebral level.
Figure 2. Subsequent imaging after few hours showing air dissecting through fascial planes causing extensive subcutaneous emphysema and pneumomediastinum.
Patient was started on broad spectrum antibiotics on suspicion of sepsis. A surgery consultation was taken and in view of the poor clinical condition of the patient, a decision to manage sepsis as priority was made. Repeated blood counts showed persistent thrombocytopenia, for which a total of 12 units of platelets were transfused in 3 days. Blood and urine cultures were sterile. His general condition gradually deteriorated and subcutaneous emphysema increased by 3rd day of admission causing respiratory distress and necessitating intubation and ventilator support. A repeat NCCT on day 4 showed air dissecting through fascial planes in the region of left angle of mandible, left side of neck, prevertebral and posterior cervical space and thoracic inlet anterior to thyroid gland causing subcutaneous emphysema and superior pneumomediastinum with multiple enlarged mediastinal lymph nodes with possibility of aspiration pneumonia.
DISCUSSION AND CONCLUSION
Although gut perforation associated with swallowed foreign body is rare, it is not uncommon. The risk factors for accidental fishbone ingestion include use of dentures, fast eating, extremes of age, alcohol abuse and mental retardation.12 Fishbone perforation of the GI tract may have several clinical manifestations, such as acute abdominal pain, vomiting, fever, occasionally melena, bowel obstruction, inflammatory mass, hemorrhage and rarely, uncommon presentation of crepitus due to subcutaneous emphysema, as was the presentation in this patient. In addition, the patients are often unaware of the accidental fishbone ingestion, which makes the diagnosis of fishbone perforation, clinically challenging.
In the diagnostic process, although plain soft tissue neck radiographs are not very useful for detecting fish bones in the throat, they are frequently employed in the management of affected patients.13,14,15 Fish bones tend to be radiolucent and, as a result, many cases of a fishbone stuck in the neck are not visualized on radiographs.15 CT has the best sensitivity in searching for a fish bone.16 On a plain CT, a fish bone often appears as a high-density linear structure like calcification within inflammatory tissue. An ultrasound study of the neck and intraoesophageal probe may also be helpful in some cases.17
To conclude, this case gives us a valuable lesson in that when patients present with complaints of foreign body ingestion, an extra effort such as CT, direct examination

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
64 © JIMI • JULY - SEPT 2019 • VOL. 13
of the pharynx, oesophagus and even the stomach through endoscopy- to trace the foreign body and an early surgical intervention to retrieve it should be made, especially in patients with predisposing risk factors.
REFERENCES:
1. Telford JJ. Management of ingested foreign bodies. Can J Gastroenterol. 2005; 19:599–601.
2. Zhang S, Cui Y, Gong X, Gu F, Chen M, Zhong B. Endoscopic management of foreign bodies in the upper gastrointestinal tract in South China: a retrospective study of 561 cases. Dig Dis Sci. 2010; 55:1305–12.
3. Ribas Y, Ruiz-Luna D, Garrido M, Bargalló J, Campillo F. Ingested foreign bodies: do we need a specific approach when treating inmates? Am Surg. 2014; 80:131–37.
4. Wada Y, Sasao W, Oku T. Gastric Perforation due to Fish Bone Ingestion: A Case Report. J Gen Fam Med 2016; 17:315–18.
5. Pulat H, Karakose O, Benzin MF, Benzin S, Cetin R. Small bowel perforation due to fish bone: A case report. Turk J Emerg Med. 2015; 15: 136–38.
6. Choi PW. Sigmoid Colon Perforation Caused by an Ingested Fish Bone: A Case Report. American Journal of Medical Case Reports. 2016; 4:301-03.
7. BizakisJG, Sega J, Skoulakis H, Voludakis A, Velegrakis G, Christodoulou P, Helidonis E. Retropharyngoesophageal abscess associated with a swallowed bone. Am J Otolaryngology 1993; 14:354–57.
8. Chen JM, Wang ZY, Ni GX. Thoracic spinal epidural abscess caused by fishbone perforation: A case report and review of literature. Medicine 2016; 95:49(e5283)
9. Mateo S, BlazquezC, Ortega J, Cabajo M, Hernandez M, Torre W. Mediastinal abscess secondary to esophageal perforation caused by foreign body. Med Cli (Barc) 1984; 82:779–80.
10. Zhao X-H, Lu Y-Q. Multiple embolisms resulted from a huge fishbone piercing the left atrium. Intensive Care Med. 2014; 40: 621–22.
11. Sharland MG, McCaughan BC. Perforation of the esophagus by fish bone leading to cardiac temponade. Ann Thorac Surg 1993; 56: 969–71.
12. Bathla G, Teo LL, Dhanda S: Pictorial essay: Complications of a swallowed fish bone. Indian J Radiol Imaging. 2011; 21: 63–68.
13. Tong MC, Woo JK, Sham CL, van Hasselt CA. Ingested foreign bodies – a contemporary management approach. J of Laryngology and Otolaryngology 1995; 109: 965-70.
14. Ng SK, Tong MC. A swallowed fishbone. Diagnosis: pharyngo-oesophageal air column. Hong Kong Medical Journal 2009; 15: 73-74.
15. Evans RM, Ahuja A, Rhys WS, van Hasselt CA. The lateral neck radiograph in suspected impacted fish bones – does it have a role? Clin Radiology 1992; 46: 121-3.
16. Goh BK, Tan YM, Lin SE, et al: CT in the preoperative diagnosis of fish bone perforation of the gastrointestinal tract. AJR Am J Roentgenol. 2006; 187: 710–714.
17. Al-Shukry, S. M. A swallowed fishbone penetrating the oesophagus into the sternomastoid muscle. J Sci Res Med Sci. 2003; 5: 51–52.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
65© JIMI • JULY - SEPT 2019 • VOL. 13
Case Report
A Rare Presentation of Hemophilia A in a Female PatientTejas D. Sailor1, Subhashchandra K.Gadhvicharan2
ABSTRACT:
Hemophilia A (HA) in females is rare. Female HA cases are often misdiagnosed as acquired HA (AHA) or as von Willebrand disease type 2N (vWD-2N). Here, we report the case of a 22-year-old female HA patient with a moderate factor VIII (FVIII) deficiency. The patient had personal &family history of bleeding disorders, &presented with heavy upper GI bleeding ,IgG inhibitory antibodies against FVIII were undetected.Patient investigated further having diagnosed as Non-random inactivation of the normal X-chromosome in a female HAcarriers.
1. Resident Doctor, Department of Medicine, P.D.U. Medical College, Rajkot (Corresponding Author) Email: [email protected]
2. Resident Doctor, 2nd Professor & Head, Department of Medicine, P.D.U. Medical College, Rajkot
INTRODUCTION:
Hemophilia A (HA) is an X-linked recessive congenital coagulation disorder caused by afactor VIII (FVIII) deficiency, which results from mutations in the FVIII gene (F8). HA typicallyoccurs in males with an incidence of ~1 in 5000 (1). Female HA patients have rarely beenreported, although they may carry a defective allele.. FVIII synthesized in hepatocytes is secreted intothe plasma in the form of an inactive pro-cofactor (3). FVIII, an essential cofactor forcoagulation factor IX, readily binds to von Willebrand factor (vWF), forming a tightnon-covalent complex that protects against degradation. Furthermore, FVIII may alsointeract with a number of proteins, such as thrombin and factor X. These interactions areindispensable for effective coagulation. Once FVIII is cleaved by thrombin, activated FVIIIdissociates from vWF and participates in the coagulation cascade (4).
In this study, we report the case of a female HA patient with normal karyotype with positivefamily History.
CASE REPORT :-
A 22 year old female patient Named Nitaben presented with chief complaints of black colourstool since 1 day & blood in vomiting 2-3 episode, with past history of uncontrolled bleedingduring childhood while hit by cow and on and off joint swelling followed by minor traumawhich was not concert by her parents with family H/O having similar complains to her twomale siblings
and with no such H/O to both her parents and her female sibling.
On clinical examination patient having tachycardia with feeble pulse, mild pallor, no icterus,clubbing, cyanosis,, Normal RS & CNS examination, P/A Soft, Mild tenderness + in epigastricregion, no hepatosplenomegaly & no ascites. Initial biochemistry and hematology results.
Variable Value Reference range.
Whole blood White blood cell 14,600 cells/
cumm 4000-11,000 cells/cumm
Hemoglobin 6.4 gm/dl 11–16 gm/dlPlatelet 3.67 lacs 1.5-4.5 lacs/
cumm
Coagulation panelPT 15.1 sec 12–16 secINR 1.19 0.8–1.2APTT 58.3 sec 25–35 secBT 2 min upto 5 min CT 7 min upto 11 minFVIII:C 10 % 50–150%vWF-Ag 128% 60–150%Factor VIII antibody
Negative Negative

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
66 © JIMI • JULY - SEPT 2019 • VOL. 13
PT, prothrombin time; INR, international normalized ratio; APTT: activated partial thromboplastin time; Fib, fibrinogen; BT, bleeding time; vWF-Ag, von Willebrand factorantigen.
White blood cell and platelet levels were within the normal ranges. Hemoglobin was reduced ( 6.4 gm/dl). The prothrombin time (PT) and international normalized ratio (INR)were normal, bleeding time (BT) & clotting time were normal but the activated partialthromboplastin time (APTT) were noticeably prolonged, which may be corrected easily by aplasma transfusion. Plasma FVIII levels were significantly decreased (10 %). vWF antigenlevels were within the normal range (128%). Other coagulation tests were also normal,including platelet count and function. USG Abdomen & Chest were normal.
MANAGEMENT
Initially patient managed conservatively, RT - RT lavage with cold water done, lavage fluidscontains blood mixed with fluid with few clots.
Trenaxa, Botophage for Bleeding control, 2 unit of PCV transfused for correction on Anaemia.
Factor VIII level done suggestive of 10% with rest investigation within normal limit.
Patient was given Plasma transfusion & Factor VIII 1000 i.u then bleeding stopped and thenRT- aspirate showing clear fluid, RT was removed and then patientdischarged with stablecondition.
Patients External feature suggestive of Turner’s syndrome, so work-out done to rule outturner’s syndrom.

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
67© JIMI • JULY - SEPT 2019 • VOL. 13
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Based on the clinical manifestations, Family history, laboratory tests, the following diagnoses were considered, in order of decreasing probability:
1. Haemophilia A:
i) Non-random inactivation of the normal X-chromosome in a female HA carriers (the most common cause of female HA )
ii) Homozygous F8 mutations (mostly reported in India where consanguineous marriages are more common)
iii) Compound heterozygous mutations affecting both F8 alleles .
iv) X-chromosome monosomy or gross structural defects, such as a deletion or translocation .
2. Acquired HA (AHA):
AHA is an autoimmune disorder caused by autoantibodies against FVIII, neutralizing itscoagulation functions and resulting in severe, often life- threatening bleeding. It ischaracterized by severe, spontaneous hemorrhaging at sites, such as the skin, muscleand soft tissues, or by excessive bleeding during surgery. Hemarthrosis, the hallmark ofsevere congenital HA, seldom occurs in AHA patients. AHA may be associated withseveral clinical conditions, including pregnancy, autoimmune diseases, malignancies, infections or drugs. Approximately 50% of patients are idiopathic with no knownunderlying disease association. If a patient presents with spontaneous hemorrhaging,then previous personal or family history of bleeding must be ruled out. Once laboratoryresults reveal the isolated prolongation of APTT and reduced FVIII levels, which fail tonormalize following a normal
plasma transfusion, AHA should be suspected. Followingconfirmation that FVIII antibodies are absent and that FVIII levels may be improved by transfusing normal plasma, a diagnosis of AHA was definitively ruled out.
3. Von Willebrand disease type 2N (vWD-Type 2N) :
vWD is the most common inherited bleeding disorder and is caused by deficiency ordysfunction of vWF.
vWD is divided into three types:
Type 1 (partial quantitative deficiency);
Type 2 with four subtypes 2A, 2B, 2M and 2N (qualitative deficiency)
Type 3 (complete quantitative deficiency).
Type 2N vWD show a marked decrease in the vWF binding affinity for FVIII.
Its clinicalmanifestations are similar to that of mild HA: FVIII levels are decreased, but vWF antigen(vWF:Ag) levels are within the normal range . These patients are usually misdiagnosedas HA. When the laboratory results were returned, we need to observed that the vWFbinding affinity for FVIII and the ristocetin-induced platelet agglutination (RIPA) shouldcome to be normal to exclude the diagnosis of vWD-Type 2N.
Differential diagnosis of HA, vWD-Type 2N and AHA.
Variable HA VWD-Type 2N AHA
BT Normal Normal or (↑) Normal
APTT ↑ ↑ ↑FVIII:C ↓ ↓ ↓
vWF-Ag Normal (↓) or Normal Normal
FVIII inhib-itor Negative Negative Positive
vWF-FVIII binding affinity
Normal↓ ↓ Normal
vWF:Rcof Normal (↓) or Normal Normal
DISCUSSION
Due to the X-linked recessive mode of inheritance, HA usually affects males, and femalesusually are carriers who may pass the disease on to their progeny. Thus, female HA

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
68 © JIMI • JULY - SEPT 2019 • VOL. 13
casesare rarely observed. However, in certain cases, there are a variety of potential geneticmechanisms leading to HA in females.
Disease severity in HA patients is classified according to residual plasma FVIII activity(FVIII:C): severe (<1%), moderate (1–5%) and mild (5–35%) . In the severe phenotype, themost prevalent mutations are inversions of introns 1 or 22, accounting for 5% and 40–50%of patients, respectively. Moderate or mild HA are usually caused by missense mutations.
In this study, we presented the case of a female HA patient with a mild clinical phenotype(FVIII: C=10%) Non-random inactivation of the normal X-chromosome in a female HAcarriers.
CONCLUSION
Female HA patients, particularly those without a personal or family history of bleedingdisorders, are often misdiagnosed as AHA or vWD-type 2N. A diagnosis of HA should bemade in a female patient when isolated APTT
is prolonged, FVIII binding capacity for vWFis normal, FVIII levels are decreased and FVIII auto-antibodies are absent. Genetic analysisof F8 using multiplex PCR and DNA sequencing is an essential tool in elucidating thenature of the various molecular mechanisms resulting in HA in females.
REFERENCES:
1. Klinge J, Ananyeva NM, Hauser CA, Saenko EL. Hemophilia A - from basic science toclinical practice. Semin Thromb Hemost. 2002;28:309–322. [PubMed] [Google Scholar]
2. Saenko EL, Ananyeva NM, Tuddenham EG, Kemball-Cook G. Factor VIII - novel insightsinto form and function. Br J Haematol. 2002;119:323–331. [PubMed] [Google Scholar]
3. Lenting PJ, van Mourik JA, Mertens K. The life cycle of coagulation factor VIII in view ofits structure and function. Blood. 1998;92:3983–3996. [PubMed] [Google Scholar]

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
69© JIMI • JULY - SEPT 2019 • VOL. 13

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
70 © JIMI • JULY - SEPT 2019 • VOL. 13

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
71© JIMI • JULY - SEPT 2019 • VOL. 13

JOURNAL OF INTERNAL MEDICINE OF INDIA • JULY - SEPT 2019 • VOL. 13 • NO. 3 • RNI No. 69152/98
72 © JIMI • JULY - SEPT 2019 • VOL. 13
NOTES
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................
...............................................................................................................................................................................................................

Thanks & RegardsEditor-in-Chief UP JIMI
Dr. S. ChakravortyMob: 9810210479, 9667668146
Email: [email protected], [email protected]
Rs. 30000/-
Rs. 20000/-
Rs. 15000/-
Rs. 10000/-
Rs. 5000/-
Back Page
Back Inside
Front Inner Page
Full Page Inside
Half Page Inside
:
:
:
:
:
Journal of Internal Medicine of India (Uttar Pradesh)
Advertisement Tariff
