welcome building a healthier hawaii island-- together dec. 7, 2011, tutu’s house hawaii island...
TRANSCRIPT
Welcome
Building a Healthier Hawaii Island-- Together
DEC. 7, 2011, Tutu’s HouseHawaii Island Healthcare Alliance
www.hawaiihealthcarealliance.org

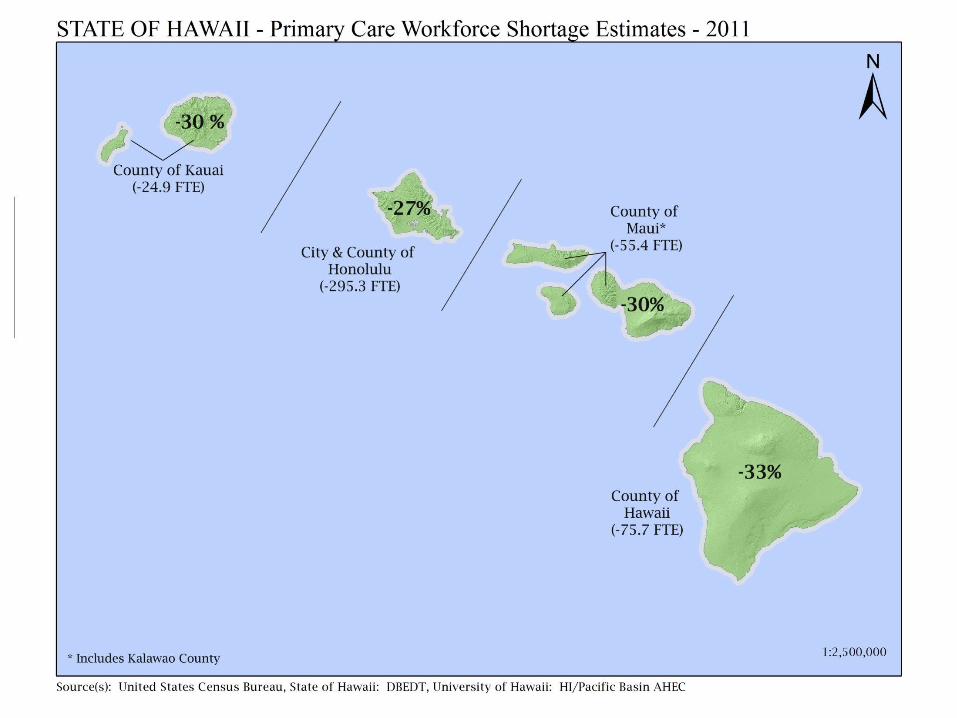
Hawaii Island - Health Problems• Higher death rates, lower life expectancy• Large & increasing workforce shortages,
– Primary Care
• Aging facilities & lack of capital • Higher costs,
– Higher hospital, Emergency Room use rates, – Higher Emergency Room rates
Health Disparities & Workforce Shortages are in a
Larger Economic Context
• Partly Result of poorer rural economy
AND • Contribute to more
economic challenges for business & government
AND • Barrier to economic
growth
However•Growing the health workforce is an OPPORTUNITY to stimulate economic growth
•Job multiplier effect of Physicians is ~1 to 5
Our Assumptions
• Need to reduce costs– Business as usual is Pau– Do more with less
• Collaboration is even more essential now
• We can’t (won’t) wait for someone else to solve our problems
Improving Health & Healthcare Is Our Monkey
Hawaii Island Healthcare AllianceSupports Solutions
Growing Our Primary Care Workforce Family Medcine Residency in HiloGrowing effective use of mid-level providersImproving recruitment & retention of providers
Increase effective use of technology - Beacon Collaboration and leveraging resources
Regional planning Aligning high leverage policy change.
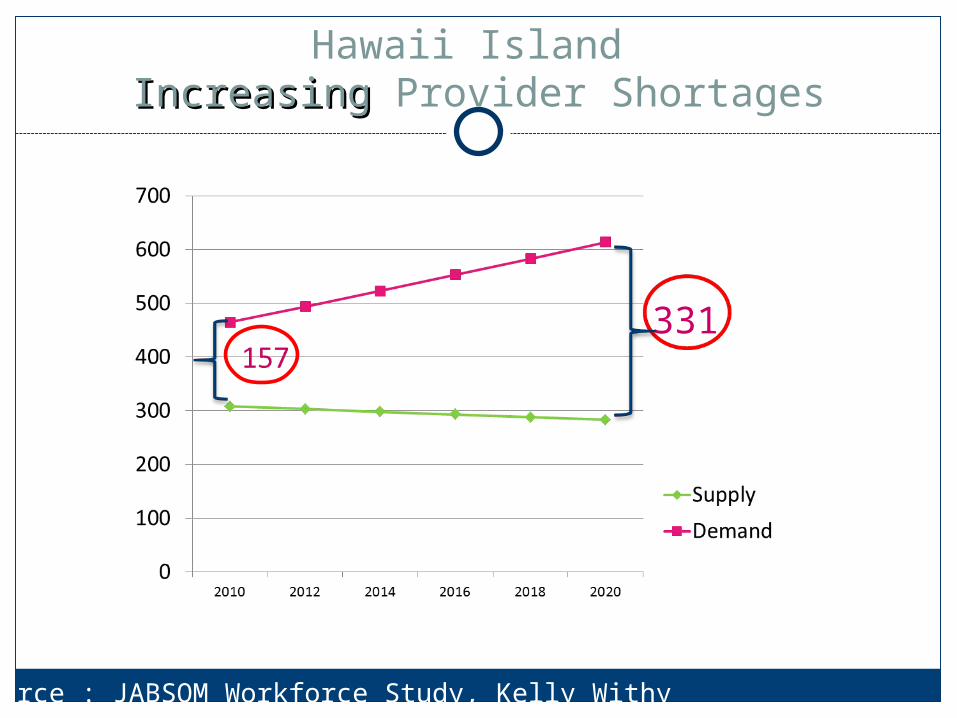
Hawaii Island IncreasingIncreasing Provider Shortages
331
Source : JABSOM Workforce Study, Kelly Withy
Why Action is Crucial Now
Verge of provider crisis
Neglected capital equipment is obsolete
Beacon provides new opportunities
UH JOHN A. BURNS SCHOOL OF MEDICINEAREA HEALTH EDUCATION CENTER
Hawaii Physician Workforce Assessment
Project, Act 219, SLH, 2007
Kelley Withy, MD, [email protected]
David Sakamoto, MD, MBA
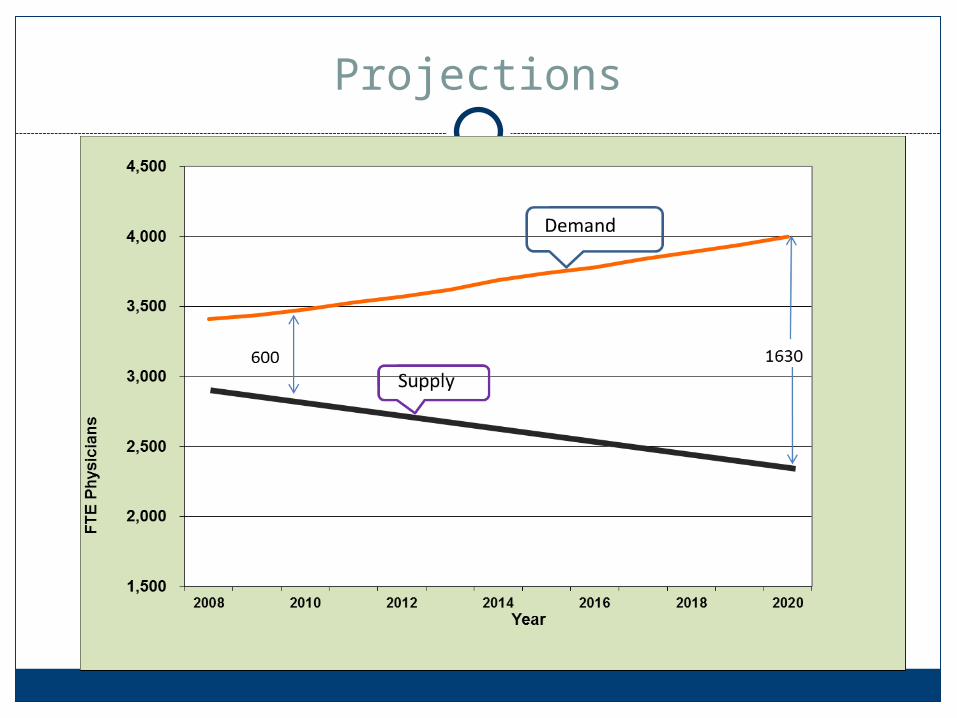
Projections
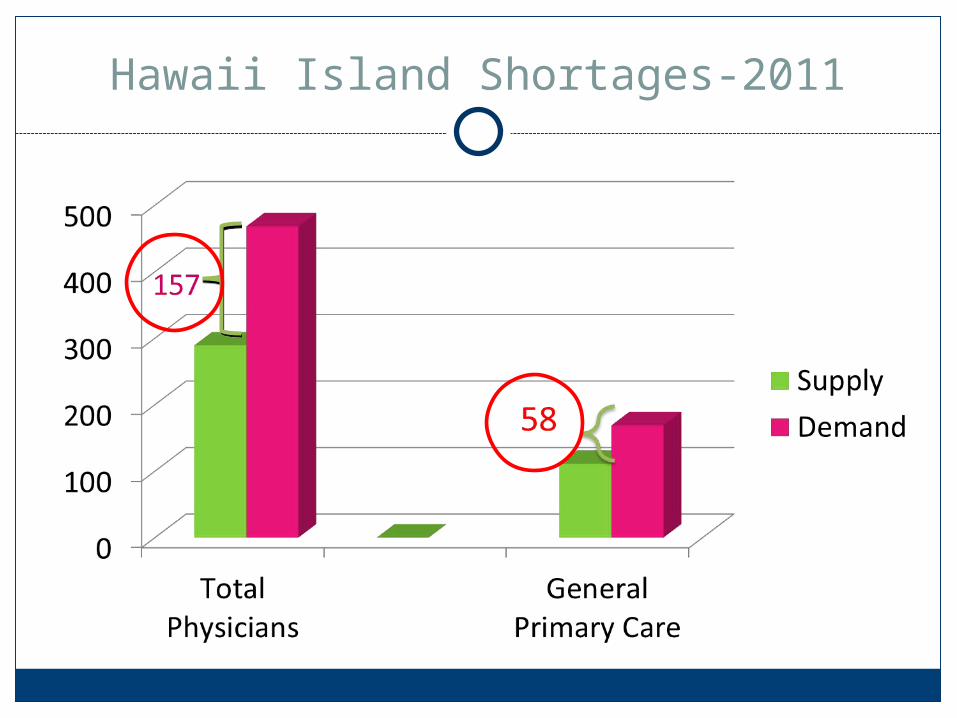
Hawaii Island Shortages-2011
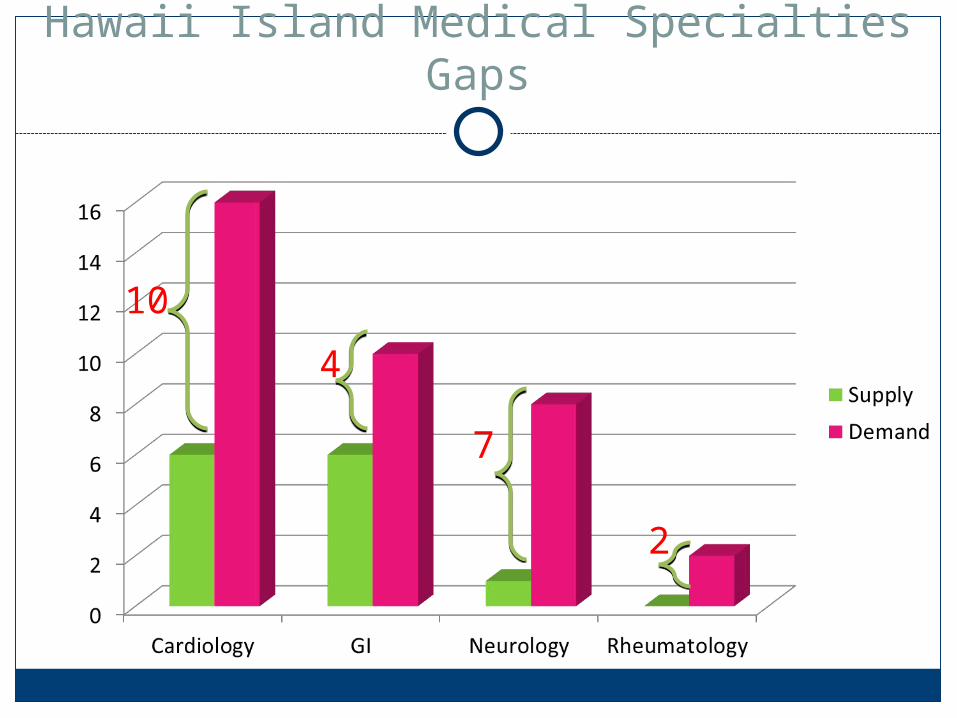
Hawaii Island Medical Specialties Gaps
7
4
10
2
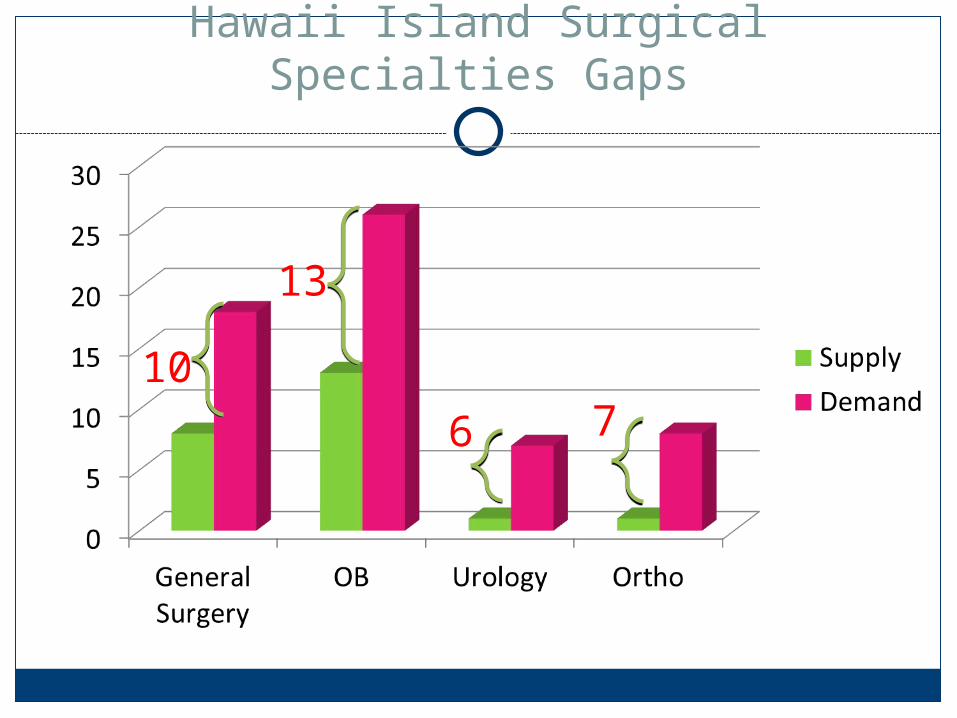
Hawaii Island Surgical Specialties Gaps
13
6 710
Act 18, SSLH 2009 Progress
10 priority areas identified at 2010 Workforce Summit
Support Training-Hilo FM Residency (interdisciplinary), SON/JABSOM joint training, increased rural training for nursing and med
Expand Pipeline-Increasing activities in rural areas, mentoring, coaching [email protected]
Act 18, SSLH 2009 Progress
Tort Reform Lawyers and doctors met monthly for 1 year and are finalizing
recommendations for MCCP changes
Community Involvement in Building Workforce: 2011 Hawaii State Rural Health Association Meeting to bring
resources to communities
Local hosts needed for visiting students/welcoming committee
Possible telemedicine presentations at community health fairs
Act 18, SSLH 2009 Progress
Systems Change, Teamwork, Administrative Simplification, Payment reform, Electronic Health Records: Patient Centered Medical Home Conference 3/3/12-all welcome!
Continuing research Update findings with current licensure numbers
Where do docs come from and go to?
HMJ Physician Workforce Edition, Feb 2012
Hawaii Island Healthcare AlliancePolicy Priorities for 2012
UH Family Practice Rural Residency Hospital Capital Requirements Improvements to allow Health
Information Exchange (HIE)
What information do Legislators need to support policy priorities for 2012?
Family Medicine Residency in Hilo Hospital Capital Requirements Improvements to allow Health
Information Exchange (HIE)
Collaboration Is Even More Essential NowProgress on Solutions
• Family Medicine Rural Residency in Hilo• Beacon • Increasing use of “mid-level”/ non physician
clinicians • Hospital Collaboration• Policy Alignment
Family Medicine Residency - Hilo
Why:– Rural residencies grow the local provider work force– Growing Primary Care reduces death rates– Growing Primary Care reduces costs– Growing Primary Care grows the economy
Recent progress:Timeline:What's different now:
– Critical Success Factors are in place:
Family Medicine ExpansionHilo, Hawaii
Meeting the health care needs of the Big Island
COGME 20th Report to Congress
• There is compelling evidence that health care outcomes and costs in the United States are strongly linked to the availability of primary care physicians.
• For each incremental primary care physician, there are 1.44 fewer deaths per 10,000 persons.
• Patients with a regular primary care physician have lower overall health care costs than those without one.
COGME 20th Report to CongressRole for legislators:
• Provide increased incentives for physicians who practice primary care or other critical specialties in designated health workforce shortage areas.
• Substantially enhance funding for scholarships, loans, loan repayment, and tuition waiver programs to lower financial obligations for students who plan and pursue careers in primary care.

HAWAII ISLAND FAMILY HEALTH CENTER
Accomplishments
• Education– Numerous medical students, as well as nursing
and pharmacy students have rotated in the office.
– UH Family Medicine residents spend two months training at the Hilo Medical Center and in the community
• Six UH Family Medicine Residency Program graduates have settled to practice in Hilo.

Timeline
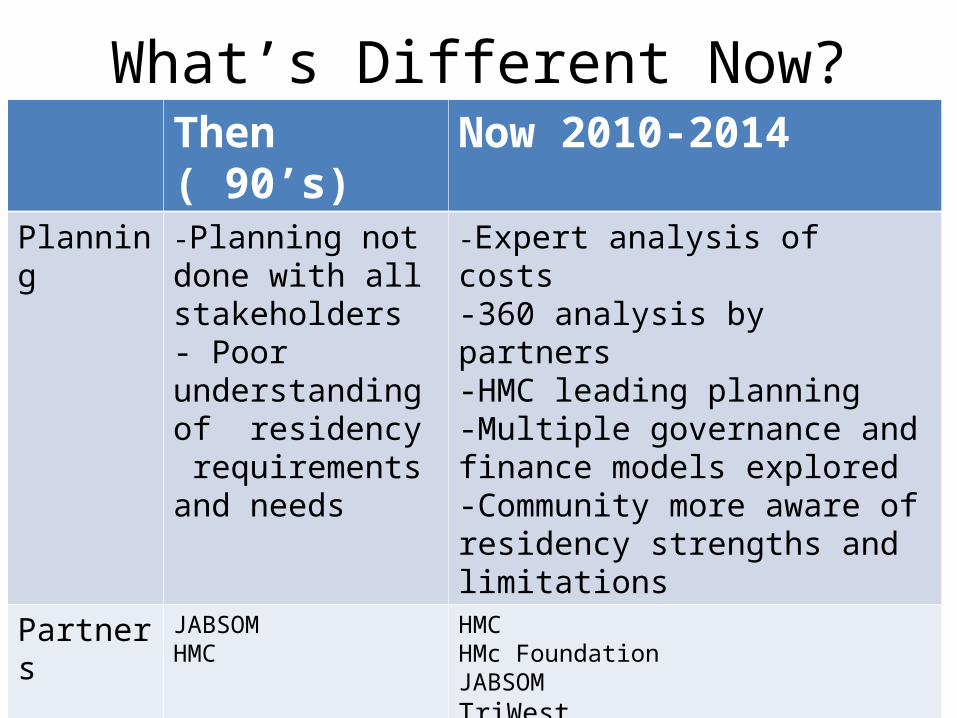
What’s Different Now?Then ( 90’s) Now 2010-2014
Planning -Planning not done with all stakeholders- Poor understanding of residency requirements and needs
-Expert analysis of costs -360 analysis by partners-HMC leading planning -Multiple governance and finance models explored -Community more aware of residency strengths and limitations
Partners JABSOMHMC
HMCHMc FoundationJABSOMTriWestHMSALegislatureSchool Of NursingSchool of Pharmacy
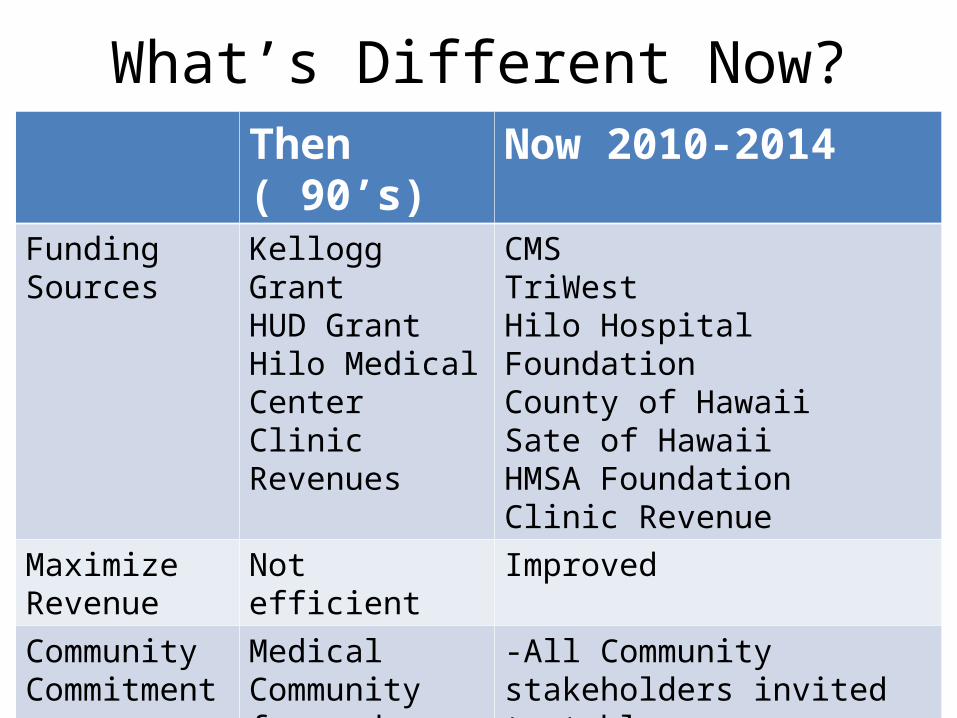
What’s Different Now?Then ( 90’s) Now 2010-2014
Funding Sources
Kellogg Grant HUD GrantHilo Medical CenterClinic Revenues
CMSTriWestHilo Hospital FoundationCounty of HawaiiSate of Hawaii HMSA FoundationClinic Revenue
Maximize Revenue
Not efficient Improved
Community Commitment
Medical Community focused
-All Community stakeholders invited to table-Greater presence of Academic community
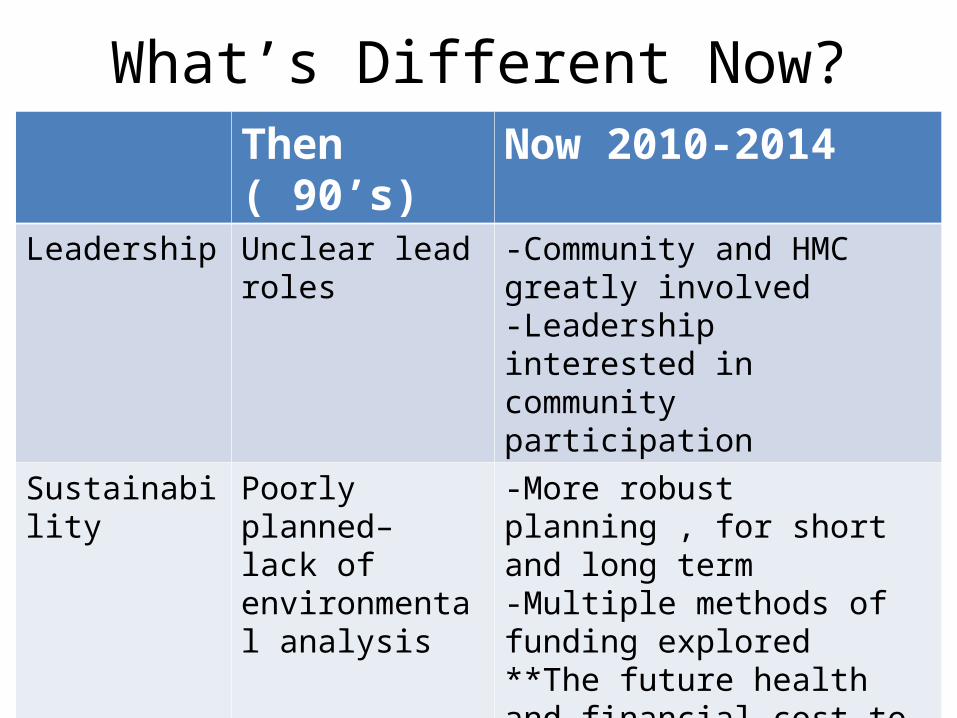
What’s Different Now?Then ( 90’s) Now 2010-2014
Leadership Unclear lead roles -Community and HMC greatly involved-Leadership interested in community participation
Sustainability Poorly planned– lack of environmental analysis
-More robust planning , for short and long term-Multiple methods of funding explored**The future health and financial cost to not develop program is greater than the investment
Hawaii Island Beacon Objectives• Improve access to primary care, specialty care and
behavioral health care• Avert the onset and advancement of diabetes,
hypertension and hyperlipidemia• Reduce health disparities for Native Hawaiians and
other populations at risk• Achieve EHR adoption & meaningful use among >
60% of primary care providers
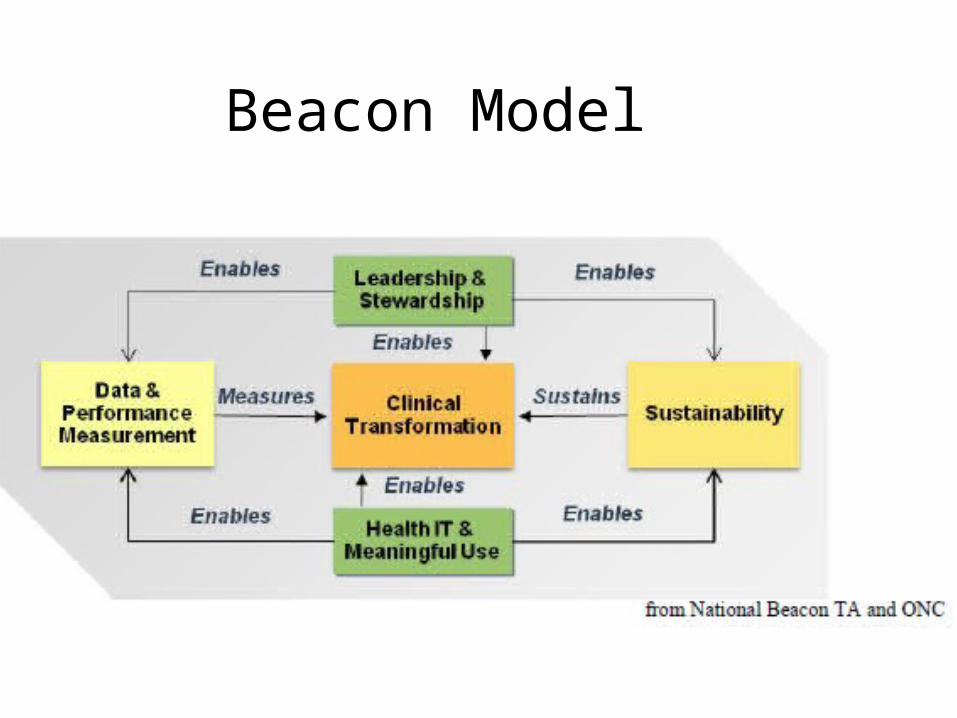
Beacon Model
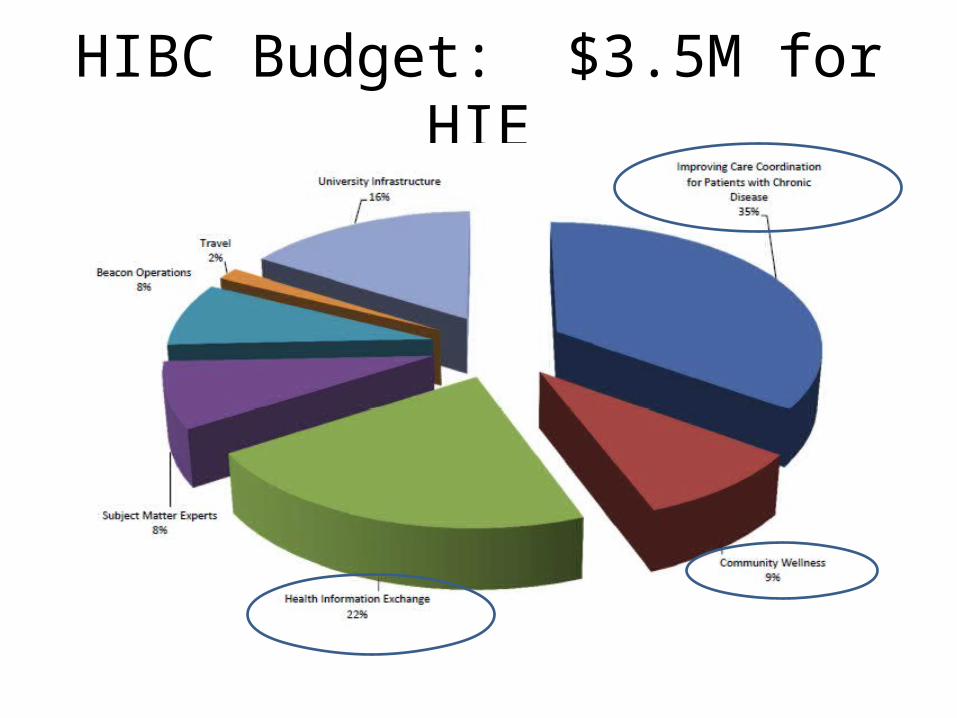
HIBC Budget: $3.5M for HIE
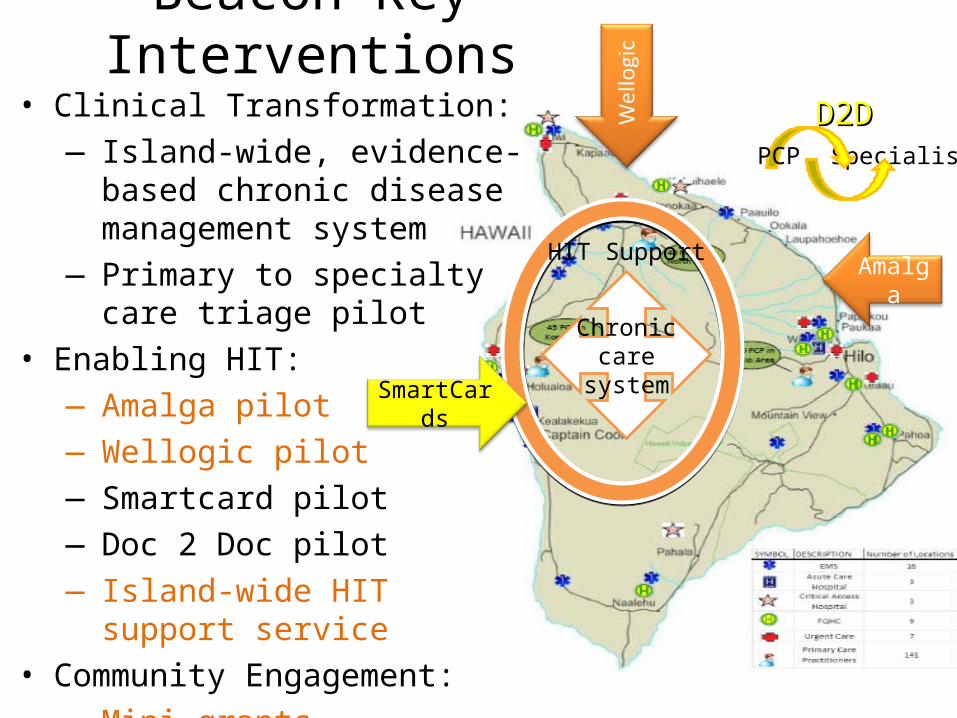
Beacon Key Interventions
Chronic care system
AmalgaHIT Support
SmartCards
SpecialistPCP
D2DD2D• Clinical Transformation:― Island-wide, evidence-based
chronic disease management system
― Primary to specialty care triage pilot
• Enabling HIT:― Amalga pilot― Wellogic pilot― Smartcard pilot― Doc 2 Doc pilot― Island-wide HIT support service
• Community Engagement:― Mini-grants
Beacon Progress
• Meaningful use of Electronic medical records• Clinical Transformation• Mini-grants• www.hibeacon.org web site• Wellogic HIE• Amalga HIE
Health Information Exchange (HIE)Policy
• HIE “Harmonization bill”– Why– Benefits
Growing Effective Use of “Mid-level” Providers- Progress
• Why: – Extends capacity of physician providers
• Where:– Puna Community Health Center
• Impact: – High patient & employee satisfaction– Lower ER visits
• Addressing Barriers:
Hawaii IslandHospital Collaboration
Trauma care collaboration- “BITAC”Maternal/ Child collaboration- “CHI”Discharge planning-Beacon/ Long Term Care
Hui –Alliance Potentially Specialty Care coverage Potentially credentials verificationPotentially continuing education
Kona Community Hospital•Collaboration Initiatives -
– Level III Trauma Program– Big Island / Maui Collaborative / Cardiology
• Recruiting Challenges
– Primary Care– Cardiology– Obstetrics– Orthopedic Surgery– ENT– Urology– Hospitalists
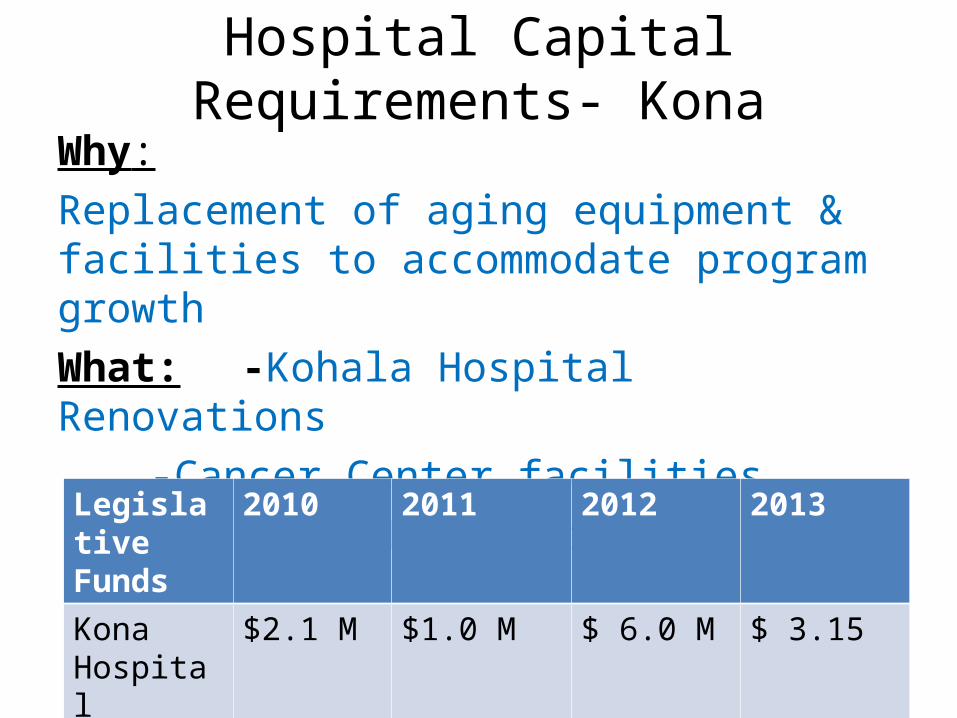
Hospital Capital Requirements- KonaWhy: Replacement of aging equipment & facilities to accommodate program growth
What: -Kohala Hospital Renovations
-Cancer Center facilities
-New hospital planningLegislative Funds
2010 2011 2012 2013
Kona Hospital
$2.1 M $1.0 M $ 6.0 M $ 3.15
Funded yes yes yes Needed
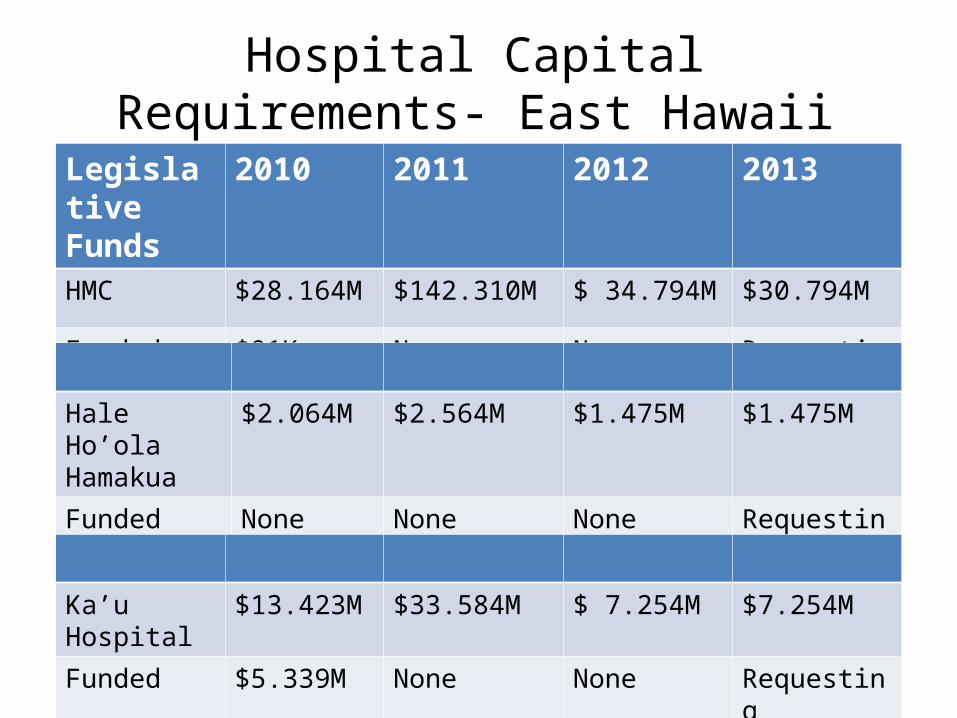
Hospital Capital Requirements- East Hawaii
Legislative Funds
2010 2011 2012 2013
HMC $28.164M $142.310M $ 34.794M $30.794M
Funded $91K Only None None Requesting
Hale Ho’ola Hamakua
$2.064M $2.564M $1.475M $1.475M
Funded None None None Requesting
Ka’u Hospital $13.423M $33.584M $ 7.254M $7.254M
Funded $5.339M None None Requesting
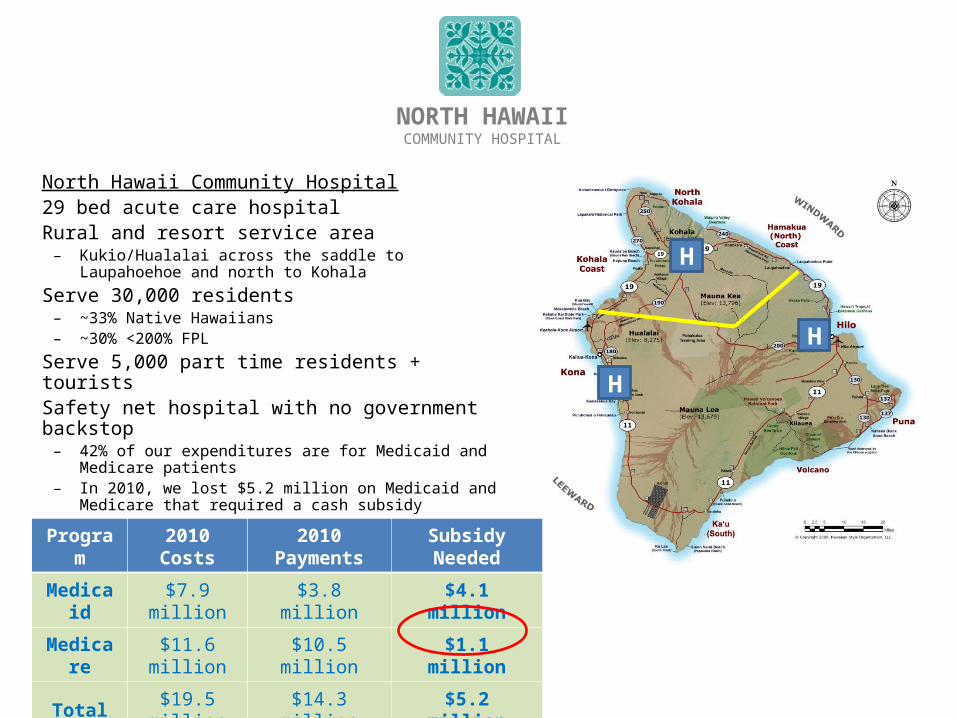
North Hawaii Community Hospital29 bed acute care hospitalRural and resort service area
– Kukio/Hualalai across the saddle to Laupahoehoe and north to Kohala
Serve 30,000 residents– ~33% Native Hawaiians– ~30% <200% FPL
Serve 5,000 part time residents + touristsSafety net hospital with no government backstop
– 42% of our expenditures are for Medicaid and Medicare patients
– In 2010, we lost $5.2 million on Medicaid and Medicare that required a cash subsidy
NORTH HAWAIICOMMUNITY HOSPITAL
H
Program 2010 Costs 2010 Payments Subsidy Needed
Medicaid $7.9 million $3.8 million $4.1 million
Medicare $11.6 million $10.5 million $1.1 million
Total $19.5 million $14.3 million $5.2 million
H
H
NORTH HAWAIICOMMUNITY HOSPITAL
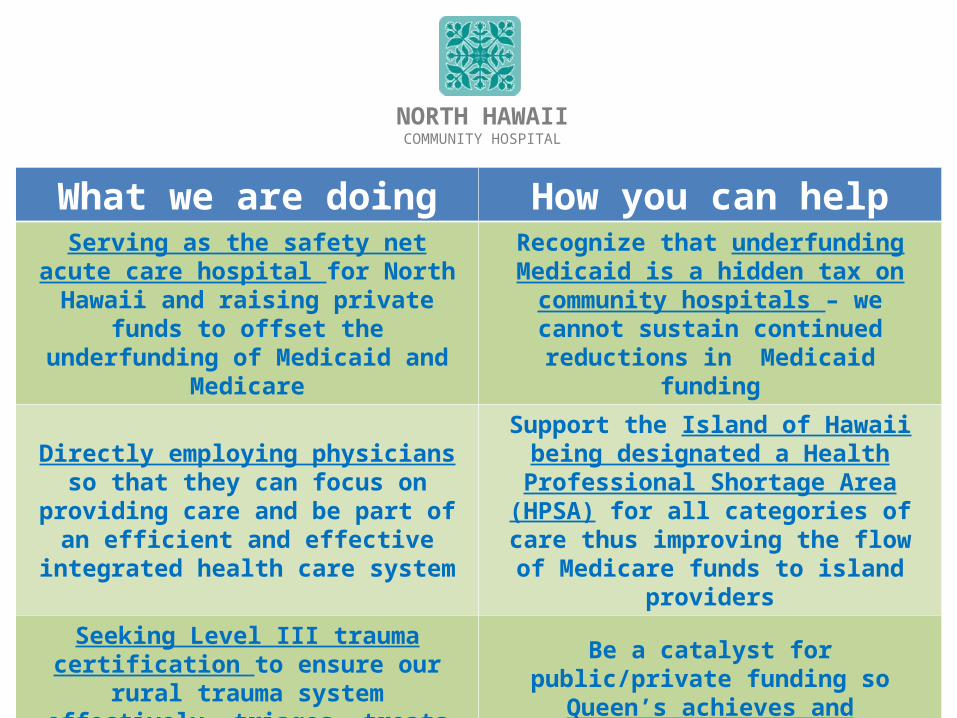
What we are doing How you can helpServing as the safety net acute care hospital for North Hawaii and raising private funds to
offset the underfunding of Medicaid and Medicare
Recognize that underfunding Medicaid is a hidden tax on community hospitals – we cannot sustain continued reductions in
Medicaid funding
Directly employing physicians so that they can focus on providing care and be part of an efficient and effective integrated health
care system
Support the Island of Hawaii being designated a Health Professional Shortage Area (HPSA) for all categories of care thus improving the flow of Medicare funds to
island providers
Seeking Level III trauma certification to ensure our rural trauma system effectively triages, treats and transports critical injured
or ill patients
Be a catalyst for public/private funding so Queen’s achieves and permanently
maintains Level I trauma status
Addressing the shortage of specialty care through telemedicine
Enable widespread adoption of telemedicine including medical providers in
other states
What Other Solutions?
• DOH• HMA• Others
Collaboration on Priorities
How can we work together to achieve these priorities?
What barriers must be reduced?
Next Steps
What additional info?Who else is essential to be
included in the discussions?Policy conference call?
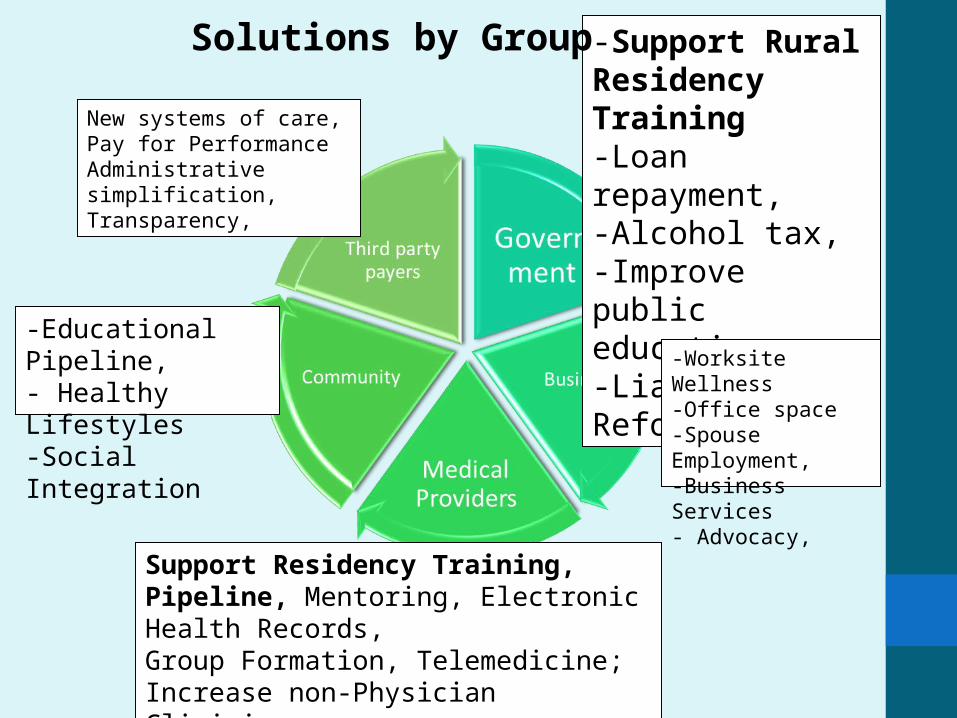
New systems of care,Pay for PerformanceAdministrative simplification,Transparency,
-Support Rural Residency Training -Loan repayment, -Alcohol tax,-Improve public education-Liability Reform
-Educational Pipeline,- Healthy Lifestyles -Social Integration
-Worksite Wellness-Office space-Spouse Employment,-Business Services - Advocacy,
Support Residency Training, Pipeline, Mentoring, Electronic Health Records, Group Formation, Telemedicine; Increase non-Physician Clinicians, Medical Home Model, Regionalization
Solutions by Group
Mahalo
• www.hawaiihealthcarealliance.org• Tools for policy makers