what’s up with cdu - wcmics.org · • patients complaining about long waiting times in cdu •...
TRANSCRIPT
What’s up with CDU ? Danielle Murray Manager Building Better Care Program Peter MacCallum Cancer Centre VCSRP Program Manager


In the beginning (2011 @ the old PeterMac)
• Patients complaining about long waiting times in CDU • Doctors complaining about not being able to get new
patients into CDU • Clerks complaining about constant interruptions from
unhappy patients wanting to know when there chemo would be ready
• Nurses complaining about needing to greet each new patient with an apology
• Pharmacy staff complaining that they are often blamed for the chemo being late… even when they hadn’t yet got a signed order!

Were we running a good service?
Hmmm…it was difficult to tell!!! We had data…. but had almost no information

WCMICS & Roche co-funded our initial CDU redesign project
The aims were: • Improve the patient’s experience by reducing
wait times on the day
• Improve access to first treatment
• Develop an accurate set of performance measures to inform future improvements
• Develop a clinically meaningful mechanism for prioritising access to first appointment


What did our patient’s tell us?
• 75% preferred morning appointments
• 75% wanted their medical review on the same day as treatment
• > 50% were happy to have bloods done day prior if that reduced the wait on the day
• ~30% did not think waiting more than 20 mins was acceptable!

What did our initial project achieve? Baseline: Time from appointment to treatment start= 32 mins Post Intervention: Median patient wait =19 mins
Baseline: Chemo manufactured within 10 mins of the appointment time = 47% Post Intervention = 75% Baseline: % chemo orders made in advance that get cancelled, disposed of or reworked= 52% Post Intervention: 8% Baseline: Time from request for Treatment to first treatment for Chemo/ RT patients =25 days Post Intervention: = 18 days

We were pretty happy with our results but….
• We still didn’t know if we were running a good service because we had no benchmarks???
Lingaratnum S, Murray D, Carle A, Kirsa SW, Paterson R, Rischin D. Developing a performance data suite to facilitate lean improvement in a chemotherapy day unit. JOP, April 9, 2013, doi: 10.1200/JOP. 2012.000755 JOP July 2013 vol.
Our recommendations included; • The need to create common measures
using consistent
• The need for a CDU COP to aid with benchmarking and shared learning
• The need for evidence based guidelines about how to prioritise patients for treatment/ “time to treat” https://www2.health.vic.gov.au/about/publications/policiesandguidelines/chemotheraphy-guidelines

DH commissioned the VCSRP (Victorian Chemotherapy Services Redesign Project)
4 key objectives
• Increase capability of Victorian CDUs to employ lean business improvement techniques to support locally lead service improvement
• Develop a CDU measures for improvement toolkit with a suite of performance measures to be made available to all CDUs
• To improve the efficiency of participating CDUs
• Spread the leanings using a Community of Practice

VCSRP Participants Round 1: 2013-14
– Austin Health – Ballarat – Barwon – Bendigo – Eastern Health (3 sites) – Peninsula Health – Southwest Health – Western Health
Round 2: 2015-16 – Albury Wodonga – Goulburn Valley – Mildura Base – Northern Hospital – Wangaratta – RCH – Wimmera
For every CDU the starting point was the same… they couldn’t see the woods through the trees
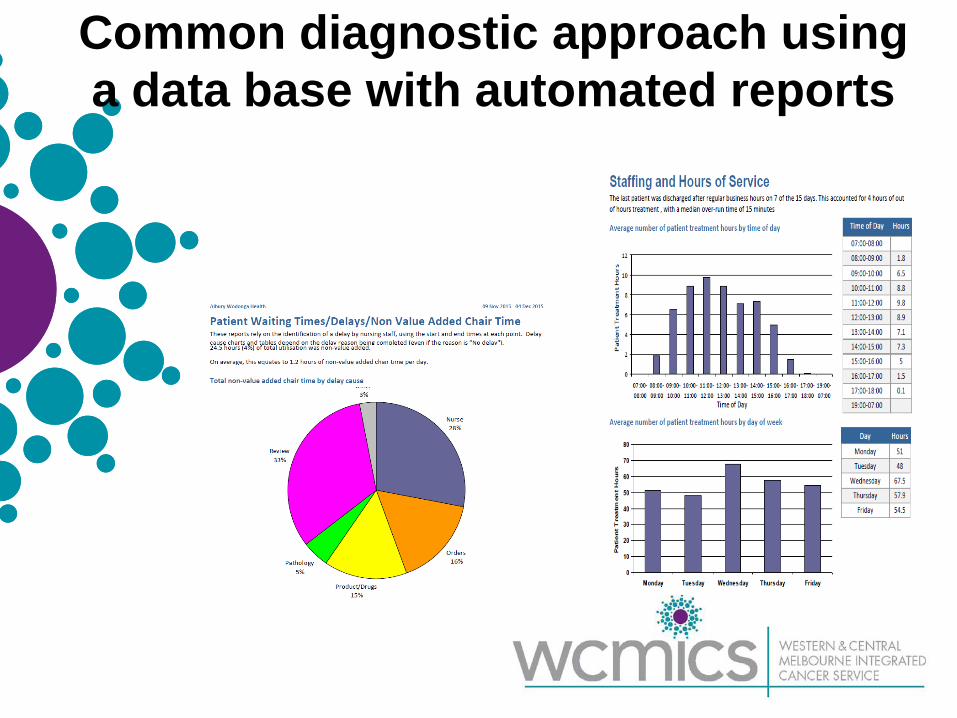
Common diagnostic approach using a data base with automated reports

What was the baseline like for VCSRP sites?
• 4/17 sites reported CDU data to exec (activity data only)
• No site had ever calculated chair utilisation
• 1/17 sites had measured their waiting times on the day
• 8/17 sites has a multi-D CDU management meeting in place

A tool kit to help CDUs learn how and why to measure performance was published
file:///C:/Users/Murray%20Danielle/Downloads/1401027_ChemotherapyGuide_web%20-%20PDF%20(1).pdf

Did we manage to replicate the improvements?
10% of chair utilisation still
wasted by idle time

Sincere thanks to…. • Jenny Byrne and the team from WCMICS who supported
the initial project at PeterMac which led us on this long and never ending journey
• To Cancer Strategy Branch and the ICS who supported the VCSRP and the COP and who will soon be uploading the full VCSRP report to the DH website!!
• and to our patients for being so patient!

Chemotherapy Day Unit Novel Nutrition Support
Program Belinda Steer
Clinical Lead Dietitian Peter MacCallum Cancer Centre
Acknowledgements Original project team (2010): • Amber Kelaart • Jacqueline Black • Jenelle Loeliger • Amanda Hill • Vicki Barrington Ongoing contributions: • Peter Mac Nutrition Department • Peter Mac Chemotherapy Day Unit • Peter Mac Food Services Dietitian

Overview of project • Aim to pilot and evaluate the feasibility and
acceptability of a novel nutrition support program for all patients attending the chemotherapy unit
• Focus on: – Timely identification, treatment and assessment of
patients at risk of malnutrition – Effective workforce planning – Fortified food model
• New model of care
Malnutrition screening tool (MST) completed on all patients by
nursing staff and triaged
Patients receiving high risk chemotherapy regimens (per
current screening criteria)
MST 0-1
(not at risk)
MST 2-3
(low risk)
MST 4-5
(high risk)
Provision of nourishing foods whilst on CDU, but
no formal nutrition intervention; for rescreen
at next CDU visit
Nutrition assistant intervention/ education and nourishing foods whilst on
CDU; rescreened at next CDU visit
Dietitian intervention/education (min fortnightly contact for at least 6wks) and provision of nourishing
foods while on CDU (including option of hot meal + nutritional
supplements)
Planned for nutrition follow-up and/or rescreened at next visit
Nutrition assistant coordinates all referrals to dietitian and food service

2012 and beyond • Interim model of care developed
– Maximising use of current resources • Project emphasised the importance of nutrition in the
chemotherapy setting = Increased engagement with the unit = Project outcomes sustainable
• No additional nutrition assistant EFT obtained to continue project model of care – Seen as a priority incorporated into their
existing role
Malnutrition screening tool (MST) completed on all patients by
nursing staff and triaged
Patients receiving high risk chemotherapy regimens (per
current screening criteria)
MST 0-1
(not at risk)
MST 2-3
(low risk)
MST 4-5
(high risk)
Provision of nourishing foods whilst on CDU, but
no formal nutrition intervention; for rescreen
at next CDU visit
Nursing staff to provide written nutrition education material to
patients. Provision of nourishing foods whilst on CDU; rescreened
at next CDU visit
Dietitian intervention/education (min fortnightly contact for at least
6wks). Inpatient nutrition assistants to provide hot meal +
nutritional supplements
Planned for nutrition follow-up and/or rescreened at next visit
Nursing staff refer high risk patients to unit dietitian. Unit dietitian notifies inpatient nutrition assistant to organise hot meals + nutritional supplements. service provision

Beyond the project - now • Our new home = ↑ number of treatment chairs = ↑
demand for services • Modifications to existing model of care • Significant benefits of having an established integrated,
sustained model of care: – Minimising change in a time of lots of change – Minimal changes to model of care required – Engagement high – Benefits have been realised

HOW DO I DO THAT AGAIN?
Vodcasts for patients with feeding tubes and swallowing difficulties
Rhys Hughes, Hannah Ray, Belinda Steer, Lauren Muir, Nicole Kiss & Jenelle Loeliger Nutrition & Speech Pathology Department Peter MacCallum Cancer Centre

Project Background • Patients receive an abundance of information from
many different health professionals during treatment (often overwhelming)
• Retention of skills and information becomes difficult
• Patients often have multiple carers, all whom may not be able to attend the education sessions
• Development of vodcasts that demonstrate step by
step instructions on aspects of nutrition and speech pathology management
Project Aims • Maximise understanding of information / education
provided
• Improve accuracy and confidence in management and self-care of treatment related complications
• Reduce potential problems arising when patients return home
• Provide practical strategies to help patients meet their nutritional and speech pathology requirements and achieve optimal outcomes
• Promote consistency of practice
• Be freely / easily accessible

Methods

Vodcast topics deemed most beneficial by consumers:
Module 1 How to administer a syringe bolus feed via a gastrostomy tube (PEG)
Module 2 How to administer a gravity bolus feed via a nasogastric tube (NGT)
Module 3 How to administer medications via a feeding tube
Module 4 Laryngectomy care
Module 5 How to thicken fluids (Mildly Thick)
Module 6 How to thicken fluids (Moderately Thick)
Module 7 How to thicken fluids (Extremely Thick)

Evaluation Ease of use Accuracy of content Relevance of content Acceptance of content Technology suitability Accessibility of content Increased knowledge gained from the content Increased confidence in completing skill Usefulness in clinical practice

Results Patient feedback was positive with the majority reporting the vodcasts were useful and significantly improved both their skills and confidence.
“Beneficial in addition to the clinical education provided.”
“A fantastic tool especially to assist all members of the family who were not there for education session(s).”
“Very impressed by the idea…it would help put my mind at ease [when returning home] that I won’t make any mistakes.”
Results • Majority rated their skills, confidence, management of
complications and ability to share information with others prior to watching the vodcasts as low (~85%)
• After watching the vodcasts this increased to high (~90%)
• 100% increase in overall confidence ratings
• 100% of participants felt they would watch the vodcasts again
• Clinician feedback was positive, most reporting they provided a useful adjunct to face-to-face education
• No resistance shown to watching vodcasts

Results • Promotional materials and information have been
disseminated to aid implementation of vodcasts into clinical practice
• Presented at multiple conferences including MASCC, COSA and ANZHNCS
• Further evaluation in 2017

Conclusions Assists in providing clear and consistent clinical information that can enhance patient safety and improve outcomes.
Current and future plans… • Ongoing review of the webpage content • Implementation of iPads to use vodcasts in the
clinical setting / bedside systems • Further vodcast modules / additions • Vodcasts in other languages (narration and text) • PMCC Head and Neck Pharmacist

Vodcasts Access • The completed vodcasts are freely accessible
via eviQ Cancer Education Online • Not required to create a log-in to access the
vodcasts • Accessing the website
https://education.eviq.org.au • Developed screen shots about access to go
with the vodcast handout

The SMART Clinic
A SMART partnership approach to managing palliative care patients – breaking down
institutional barriers
Presenter: Dr A Dabscheck Palliative Medicine Consultant, Western Health


Needs Analysis
Source: The Macedon Ranges and North Western Melbourne Medical Local, 2014. Comprehensive Needs Assessment.
• Limited access to GPs and psychological services in the western region

Our patients are “doubly vulnerable”
• By this I mean that the socio economic environment has conspired to give our patient an increased vulnerability to chronic disease and cancers, hence an increased mortality compared to the state, plus decreased access to Health services. We know from our feasibility study and the Macedon Ranges and Western Medicare Local Needs Analysis 2014 that our patients have decreased access to Primary Health and Allied Health services.

Structural Vulnerability
" Structural Vulnerability" is a concept which captures our patients. Structural and social forces are intersecting to constrain decision making, frame choices and limit life options to make people vulnerable to risk and harm. Advances in Nursing Science Issue: Volume 39(4), October/December 2016, p 293–307
Lack of Service Coordination
• The May 2014 Comprehensive Needs Assessment from the Macedon Ranges and North Western Melbourne Medicare Local identified lack of effective service coordination between health services as a barrier to care across the geographic catchment area of Western Health

Institutional Support
• Both Mercy Palliative Care and Western Health recognised the need to improve Palliative Care services to our many mutual patients and took advantage of WCMICS as a funding body to set up the SMART Clinics.
• Both Mercy and Western showed flexibility to allow this to happen.

Background
• Western Health (WH) provides an in patient hospital based Palliative Care Consultation Service which is managed by Cancer Services and a separate In Patient Palliative Care Unit, which is managed by Sub Acute Services.
• Mercy Palliative Care offers a community based palliative care service which is multidisciplinary in approach, including nursing, counseling and bereavement services.

Aims
• Both services aim to provide a physical and emotional “safe haven” to improve the quality of life and symptoms of patients (and their families) when they are suffering from life limiting or life threatening illnesses.
• In this instance the illness is cancer. • The place of care may be hospital, the palliative
care unit or home, which may include aged care facility

Identifying the need • Both Western Health and Mercy Palliative Care had recognised that
a group of patients were ‘slipping’ through the gaps. • Oncology patients seen exclusively as outpatients often had
symptom issues that could potentially benefit from palliative care input – either consult service or community palliative care.
• These patients are often not referred to palliative care until admitted as an inpatient when disease or symptoms become more severe or approaching end of life.
• Late referral to community palliative care, or not referred at all and family missing out on bereavement and counselling support.
• Avoidable presentations to Emergency or multiple hospital admissions.

SMART CLINIC
• The SMART (Symptom Management Assessment & Referral Team) Clinic evolved from the Out Reach Program.
• Project officer (Kathy Hendry) employed through a WCMICS grant to implement clinic.
• We have further broken down institutional barriers between the hospital and community by seeing patients at a hospital Out Patient Clinic which is staffed by a Mercy Nurse, Hospital Pharmacist and Palliative Care Consultant.

Survey of Oncology Consultants and Registrars
• Supported anecdotal evidence of need • Survey served as an awareness raising exercise • All tumour groups supportive of clinic • “How soon can you start!”
• All layers of hospital management were very
supportive.

Commencement • Project committee and working groups established
• Clinical committee which included a consumer representative who has had personal experience of involvement with Mercy Palliative Care and is a WH volunteer in Out Patients
• Evaluation = sustainability • Pharmacy



Consultations 62 patients 1/06/12-31/12/13.
36 reviews
Referral source Colorectal Unit -8 Onc. Ward – 4 MPC-4 GP - 4 Priv Cons Rooms - 2 Day Oncology-5
Lung unit - 6 General Oncology – 18 Emergency -1 Renal Unit -1 Breast -4 Haematology -1 Research – 2 Ward Sunshine -1
Reason for referral (Often a combination)
52 Pain Management 27 other symptoms 18 link to community palliative care
14 medication advice
Pharmacy input All Pharmacy Care Plan commenced
15 provided with injectable medications
All medication education
2 community pharmacy contact
Pain scores reduced By next assessment in 83% cases – Not all have pain
Not all able to be followed up – 70% follow up rate
Referrals to community palliative care
27 25 to Mercy 2 to other Community services
21 patients already known to Mercy when seen in SMART
Deaths 23 deaths 10 at home 9 PCU 4 In acute hospital beds
Emergency Presentations
• Patients in the palliative phase commonly require frequent ED presentations for symptom management, particularly associated with disease progression.
• Our data indicates that the presence of the SMART clinic has reduced ED presentations by more than 43%.
Survey Feedback (22) • The SMART clinic has been well received by both patients
and carers with overwhelmingly positive feedback. Major achievements are;
• Early linking to community palliative care with palliative care being seen as part of the treating team rather than End of Life Care.
• The team approach of doctors, nurse and pharmacist working together was well received by patients and carers.
• Better understanding of medications and disease process. • Improved symptom control. • Empowerment and inclusion of carers. • Car parking (or lack of it) is the main area of
concern expressed by both patients and carers

What do GPs say? • 84 surveys faxed to GPs – 18 returned • 22% return rate – this is a difficult group for response. • All 18 happy with clinic – high level of satisfaction: • Comments re information from the clinic – • “Very thorough” • “Succinct and to the point” • “Helped with (his) ongoing management of
medications”

Advantages:
• Patient and family do not feel deserted by the treating team
• Referral to Mercy takes place in the hospital providing Mercy nurses to access all relevant information
• Referrals earlier in the disease process allowing a trusting relationship to develop
• Emergency medications arranged at the time of referral – GPs can have difficulty prescribing these
• Pharmacy presence allows planning and education to take place at time of referral
• Faxing of the BOSSNet notes directly to GP allows timely communication – GPs are feeling more supported with provision of ongoing care
• Trend towards a reduction in Emergency presentations


Curative Intent Patients • We are seeing an increasing number of
patients being managed with curative intent but suffer from symptoms related to their treatment as well as their cancer e.g., anal cancer
• Our unique relationship with Mercy allows these patients to be admitted to our joint service to manage their symptoms and then discharged back.

The Future Need-Psycho Oncology for the West.
• In the Footscray and St Albans area, according to the Macedon Ranges and Western Medicare Local Needs Analysis 2014;
• Virtually no access to public and private psychiatry • Limited access and long wait times for public psychology (limited • private psychology) • Low private health insurance coverage inhibits access to private • mental health services because of high costs • Increasing prevalence for mental health issues amongst the refugee • population • Concern in relation to the impact on the mental health of carers • From University of Newcastle research we know that WH has a higher
percentage of psychological distress amongst Oncology patients than the national average (28% vs 21%).
• •

Acknowledgements • Fran Gore and Mercy Health • WH Divisional Director – Ms Jenny Walsh • WH Director of Cancer Services– Prof Michael Green • WH Cancer Services Manager – Ms Adele Mollo /Tim
Chui • WH Director Palliative Care – Dr Maria Coperchini • Palliative Care Consult Team Nurses Mercy Health • WCMICS as project funding body • Project Officer- Kath Hendry • Dr Philip Tran and Dr Gail Ryan • Doctors, Nurses and Admin Staff at WH & SHRTC

WCMICS – 10 Years! Brian Le
Palliative Care
Royal Melbourne Hospital Peter MacCallum Cancer Centre

Projects • Early Integration of Palliative Care in
Oncology (2011)
• Bereavement support in a Cancer Centre (2009) • Improving GP Integration in Cancer Supportive Care (2014)
– Outline – Outcomes – Benefits – Sustainability

Early Integration of Palliative Care in Oncology (EIPCO)
• Collaboration between Royal Melbourne, Peter Mac and St Vincent’s
• Project team including consumer representative (Shirley Carvosso)
• Co-lead project team: – Linda Mileshkin – Jennifer Philip

EIPCO
• 3 phases: – Clinician interviews about
perceptions of barriers and aids to palliative care involvement in lung cancer treatment
– Retrospective audit of outcomes – Implementation across 3 hospitals of
model of early palliative care

EIPCO
• Outcomes: – Widely welcomed – Issues around:
• Timing • Site of care (particularly for regional
patients) • Responsibility of care and information
sharing

EIPCO • Outcomes:
– N=329 over 1 year (2011-2012)
Advance care planning (%) EOL care plan documented
66
Palliative Care referrals (%) Referral made Referral within 90 days of diagnosis
Timing of referral, median (days) Days from diagnosis to referral Days from referral to death
100 100 10 (3-35) 71 (28-156)
ICU admission within 30 days of death (median) 3 ED admission within 30 days of death (median) 0 Acute hospital admission within 30 days of death (median) 1 Treatment within 14 days of death (%)
Chemotherapy Radiotherapy
6 9
Treatment within 30 days of death Chemotherapy New chemotherapy regimen
11 9

EIPCO
• Benefits: – Identification of ideal model of care
• Informed by stakeholders • Standardised care, delivered in a
model fitting each institution – Evidence based – Evidence generating – Promote good patient outcomes

EIPCO
• Enhanced cross institutional
collaboration – Reduced variations in care
• Critical role of consumer input

EIPCO
• Sustainability
– Early routine palliative care remains somewhat controversial
– Implications for both palliative care and oncology

EIPCO
• Small beginnings big things can grow! – PEARL (Palliative care Early in
Advanced Lung Cancers) – Cancer Australia Grant 2016
• Lead investigator Linda Mileshkin • National study in collaboration with
ALTG / PaCCSC
EIPCO
– STEP care (Standardised Early
Palliative Care) • Victorian Cancer Agency 2015
– Lead investigator Jenny Philip – Multisite study

Final thoughts • Projects are hard work
– Application process – Building the case – Getting sign off (!) – And then it gets harder…

Final thoughts
• Wonderful opportunity to examine practice
• Collaboration with partners • Standardise and optimise care • Generate evidence • Continuous improvement

Safe handling guidelines for "new" anti-cancer molecules
Marliese Alexander on behalf of the project steering committee
led by Prof Michael Green

Background • Operator exposure risks with traditional cytotoxics are well
established
• Extension of same practices for MABs – Presumed similar risks – Variation across health services
• Impact on patient waiting times and costs • Available guidelines conflicting and/or exclusive of MABs

Project Overview
4. Consultation with Government and Professional Associations MOGA – HSANZ – CNSA – SHPA – COSA – ISOPP
Safe Work Australia – Work Safe Victoria – Victorian Department of Health (Cancer Strategy and Development)
Commonwealth Department of Health and Ageing
Project Team / Project Oversight
1. National Clinical Practice Survey
2. Synthesis of Evidence
Multidisciplinary Writing Group
3. Consensus Meetings
Governance and Process Guideline Writing Group: • Multidisciplinary (17 members with National representation including
medical, pharmacy, nursing and a consumer) – While the guidelines are designed to protect healthcare personnel,
consumers are directly impacted by decisions relating to drug preparation and administration
– Consumer involvement was essential to ensure consumer values were maintained and reflected in recommendations
– Jane was involved from day 1 to project completion – THANK YOU!
• Involvement from public and private sectors (in metropolitan and regional centres)
• Develop guidelines based on robust and reproducible methodology
outlined by NHMRC
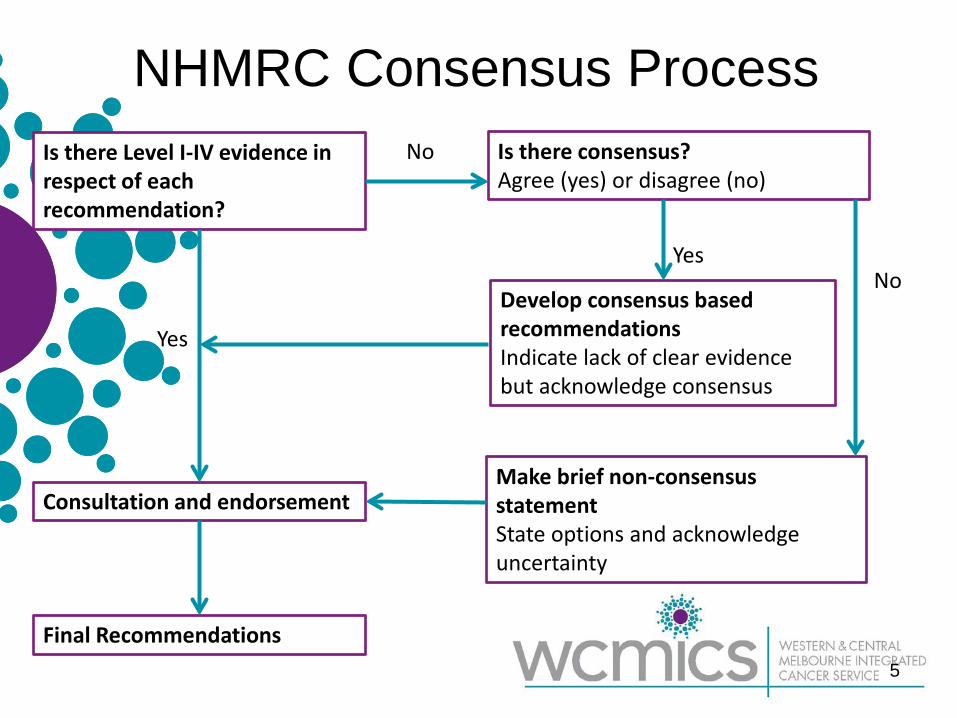
NHMRC Consensus Process
5
Is there Level I-IV evidence in respect of each recommendation?
Is there consensus? Agree (yes) or disagree (no)
Develop consensus based recommendations Indicate lack of clear evidence but acknowledge consensus
Make brief non-consensus statement State options and acknowledge uncertainty
Consultation and endorsement
Final Recommendations
Yes No
No
Yes

National Survey • National survey distributed to 222 medical, nursing and pharmacy
personal via relevant professional body membership • National representation (majority Vic), rural and regional, public and
private
• Less than half of respondents had access to MAB handling guidelines. • Majority of MABs are prepared in pharmacy cytotoxic cabinets. • Attitudes and opinions vary by profession.
– Toxicity profile rated as strongest reason to determine manufacturing procedures
– Internalisation potential comparatively inconsequential – Perceived differences between safety requirements for different
MABS (i.e. denosumab and rituximab)

Risk Assessment Questions • What are the independent risk factors that determine level of
occupational exposure risk to MABs?
• Is the framework/mechanism for risk-classification the same for each class of agent or for individual agents?
• What are the exposure risks by staff role/discipline and personal circumstances?
• What interventions/safeguards can be utilised to mitigate exposure risk?
• What other factors, not related to occupational exposure risk, may
influence how MABs are prepared?

Occupational Exposure Risk Toxicity: Rated strongest determinant of practice
• No data that MABs are cytotoxic (via direct cytotoxic action)
• No data that MABs are genotoxic or mutagenic
• Limited data that some MABs may have an association with increased risk of lymphoma and other malignancies during therapeutic use.
• No data that MABs are teratogenic or have developmental toxicity during occupational use
• No data that MABs have organ toxicity at low doses
• No evidence of immunogenicity associated with occupational exposure to MABs at low doses
Internalisation Potential: Not identified as a strong determinant of practice • Little or no potential for internal exposure (oral, mucosal, inhalation,
dermal) during occupational handling
Other Factors • Current funding arrangements for hospitals: additional payments for
intravenous therapy • In Victoria, funding is payable for chemotherapy administered
intravenously
• Costs associated with use of personal protective equipment (PPE) • Greater risk of exposure with manufacturing will require greater level
of PPE
• Impact of manufacturing procedures on patient wait time and throughput
• Level of training of manufacturing operators: • Drugs in powder form or where incorrect reconstitution of liquid drug
may result in drug becoming aerosolised increases risk of internal exposure by inhalation
• Complexity of manufacturing. Occupational exposure risk increases with: • Increasing number of preparation steps • Use of part vials
Risk Assessment Answers • Assessment of independent risk factors that determine level of
occupational exposure risk to MABs (low internalisation potential, no known toxicity at occupational exp levels)
• Determine a framework/mechanism for risk-classification by class of agent or individual agent (denosumab versus rituximab / humanized versus chimeric versus murine / by molecular size all equal when considering occupation exposure risk)
• Identify exposure risk by staff role/discipline and personal circumstances (manufacture > administration > waste disposal)
• Use of interventions/safeguards to mitigate against exposure risk (personal protective equipment likely sufficient)
• Other factors not related to occupational exposure risk that influence how MABs are prepared (timely access to drug / financial implications / medication safety…)

The Guidelines
12 months, 17 committee members, 222 surveyed clinicians, one literature review, >50 participants across two consensus meetings, endorsement from 7 professional organisations 3 simple steps

Step 1

Step 2

Step 3
Where to now… • Are institutions aware of the guidelines?
– Google scholar tells me the guidelines have been cited on 7 occasions, the evidence review paper on 5 occasions, and national practice survey on 3 occasions
• Have institutions reviewed their practices against recommendations?
• Have institutions implemented practice changes as a result of
recommendations?
• Are staff agreeable that the level of intervention recommended in these guidelines appropriately mitigates potential occupational exposure risk?
• Have practice changes had any impact on safety, productivity, medication error, drug wastage or other financial costs?


Early Endometrial Cancer Survivorship Project
Danielle Carpenter Clinical Nurse Consultant Gynaeoncology Service
Endometrial Cancer Survivorship Project: the team
• Nurses: Anna Dingle, Amy Cooper, Tarnya Hotchkin, Danielle Carpenter, Katy Weare, Jess Jude
• Drs Sally Dooley, Ines Rio, Orla McNally • Dietician: Ingrid Currington, • Physiotherapist: Sarah Cleaver • Consumer: Kathryn Marshall • Project officer: Sita Vij, Jo Werda, • Data Management: Shauna McEgan • BreaCan: Lee Kennedy • WCMICS: Michael Barton • University of Melbourne: Lynette Joubert • North West local: Samantha Smorgon, Angela Ouroumis

Why Endometrial Cancer
• Most common gynaecological cancer
• Often diagnosed at Stage 1
• Highly curable
Stage 5 year survival 1A 91 1B 88 1C 81 11A 77 11B 67 111A 60 111B 41 111C 32 1VA 20 1VB 5

Improved 5 year relative survival rate for uterine cancer:
– From 1982 - 1987 to 2006 – 2010, survival rates increased from 75% to 82%.
From 1982 – 2008, incidence rate of: – Uterine cancer increased by 22% (13.8
to 16.8 per 100,000) – Ovarian cancer decreased by 15% – Cervical cancer decreased by 51%
Source: ‘Gynaecological cancers in Australia: An overview’ (1)

Obesity as a risk factor for endometrial cancer
Systematic literature review (2013) involving 159 articles (2): Convincing evidence that body fatness increases the risk of endometrial cancer. In 2012, 60% of adults were overweight or obese. Of these, more than 25% classified as obese (4)
Obesity trend projected to continue and as obesity increases so does the risk of developing endometrial cancer which equals more patients
How does obesity influence the development of endometrial cancer?
Type 1 – Endometrioid, early stage, oestrogen dependent.
Type 2 – Non-endometrioid, serous, clear cell, high grade, high stage, non-oestrogen dependent.

Mechanisms: how does obesity increase risk of type 1 endometrial cancers?
Obesity: a toxic state of high circulating levels of oestrogen, insulin resistance and inflammation (5)
1. OESTROGEN (2,5)
• Excess levels of oestrogen in obese women caused by increased conversion of androgens to oestrogen in adipose tissue / fat
• Hyperinsulinaemia → lower levels of SHBG which increases bioavailability of free oestrogens.
• Oestrogens bind to endometrial cell DNA to increase transcription & interact with growth factor signalling pathways, promoting proliferation and tumour growth.
2. INCREASED INSULIN AND INSULIN RESISTANCE (2,5) • ↑ bioavailability of IGF-1 (growth factor that drives cellular proliferation) 3. CHRONIC INFLAMMATORY STATE (2,5) • ↑ levels of proinflammatory cytokines & hormones → effects on immune
system & • ↑ oxidative stress → implicated in tumour growth

Survival: are there differences between morbidly obese and non-obese patients?
von Gruenigen et al, 2006 (n=380) (13)
Of those BMI >40 who died, 67% of deaths due to causes other than endometrial cancer, whereas in those BMI <40, only 43% deaths were unrelated to cancer.
Relative Risk (RR) for death from uterine cancer is 6.25 for women with BMI >40 v healthy BMI (18.5 – 25) (3)

Impact of BMI on survival & quality of life in cancer survivors
• Rising incidence of EC & ↑ survival rates = more survivors in total
• Poorer QOL in obese endometrial cancer survivors(14).
– 60% of EC survivors had a new diagnosis with medication or hospitalisation related to obesity within the first year (15)
• Obesity: not a negative prognostic factor for cancer recurrence, except in very obese (due to more favourable histopathological profile) but likely higher morbidity & mortality rates from causes unrelated to cancer

Low risk endometrial cancer: current model of care for follow-up
• WCMICS project – 2009
Endometrial Year1 Year2 Year3 Year4 Year5 Year 6-10
Low-medium risk 4-6/12 4-6/12 12/12 12/12 Discharge
Recommended Abdomino-pelvic examination ……………………
High risk 3/12 3/12 6/12 6/12 6/12 12/12

Endometrial Cancer Survivorship Project: Pre-program cohort audit
• N=67 (would have been eligible for NLC if it existed)
• Histories on-site:off-site – 29:38 • 20 on-site eligible for analysis • Number of appointments 5 to 20/patient • No documentation on discharge from clinic
with regards to re-referral if concerned. • 80% with weight >80kg (min BMI records) 2 were still in follow up 3 referrals was made
Referrals from clinic
Dietician 0
Physiotherapy 1
Psychosexual 0
Menopause after cancer clinic
2
Incontinence 0

Endometrial cancer:recurrence
• Women in routine follow-up delay seeking advice early about symptoms
• Not always picked up with abdominopelvic exam or pap/vault smears
• Local recurrences mostly present with bleeding • Distant recurrence unlikely to be found unless the
woman is symptomatic and at this point treatment options are limited

So….Then what?
• The development, implementation and evaluation of a survivorship model of care for women with early endometrial cancer.
• Social model of health which was focused on overall wellness
• Collaboration with all health care providers • In the most appropriate setting for the woman.

Low risk endometrial cancer
• Low risk refers to low risk of cancer recurrence – FIGO Stage 1A /1B (G1 and 2) endometrioid
– 1A G3 and High risk cell types excluded
• Both newly diagnosed women and those already in
the hospital follow-up.

The development of a survivorship model of care for women with early endometrial cancer
WCMICS funded: Purpose
• Obtain evidence about the model of care in terms of: – Acceptability (for women, general practice and
hospital staff) – Effectiveness – Impact – Sustainability
• Contribute to the evidence-base in terms of models of survivorship care and supporting people with cancer to live well.

Overview Presents to
gynae-onc for care
MDM identified for
NLC
Consultant review in clinic to confirm
eligibility
•TARGET 75 NLC
information given
• Multiple domains covered. • Health care plan
NLC face to face or
telephone
GP contact • GP follow-up
Early Hospital review if
concerned
Potential for other sources

Endometrial Cancer Survivorship Project: Follow up Care plan
• Diagnosis & History summary • Treatment summary • Co-morbidities • Investigations (MRI, Histology) • Medications • Physical assessment (weight, height, BP) • Health and Wellbeing management
– Nutrition, physical activity, heart health, psychosocial (inc. mental health), sexuality, menopause, fertility, incontinence, FCC, bone health and any other symptoms or concerns
• Recommended Schedule for Follow-up • Follow-up guidelines for GP • Access details for re-referral

Endometrial Cancer Survivorship Project

Endometrial Cancer Survivorship Project: Results
Nurse-led Clinic Offered 73 Face to face 59 Telephone 5 Declined 3 Did not attend 5

Endometrial Cancer Survivorship Project: Results
Care Plans and Surveys Sent to women and GPs 64 Awaiting specialist sign-off 0 GP surveys returned 22 Patient surveys returned -Pre NLC -Post NLC
64 25
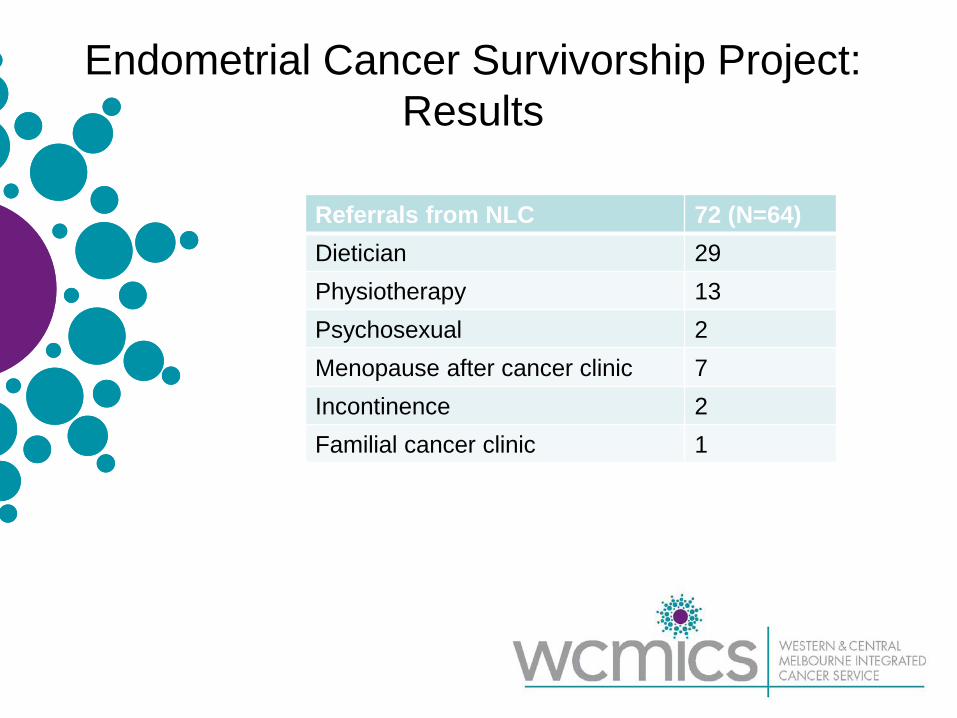
Endometrial Cancer Survivorship Project: Results
Referrals from NLC 72 (N=64) Dietician 29 Physiotherapy 13 Psychosexual 2 Menopause after cancer clinic 7 Incontinence 2 Familial cancer clinic 1

• ECSP Survey – consumer post-NLC

Q1: How useful did you find your appointment with the hospital nurse?
• Answered: 25 • Skipped: 0

Q3: As a result of your appointment with the nurse, have you made any lifestyle
changes? • Answered: 24 • Skipped: 1

Q4: Did the hospital nurse refer you to another health professional e.g. dietician,
physiotherapist, counsellor?
• Answered: 25 • Skipped: 0

Q5: Do you find the Follow-Up Care Plan sent to you by the hospital useful?
• Answered: 23 • Skipped: 2

Q7: Did you discuss your Follow-Up Care Plan or any ongoing issues you have with
your GP? • Answered: 24 • Skipped: 1

Q9: How useful was the appointment with your GP?
• Answered: 22 • Skipped: 3

Q10: As a result of your appointment with your GP, have you made any lifestyle
changes? • Answered: 21 • Skipped: 4

Q11: Do you feel like you still have issues or concerns about your health and well-being
that you need to discuss or need more information about?
• Answered: 24 • Skipped: 1
ECSP Survey – GP Survey
• 22 Responses

Q1: Have you seen your patient since her follow-up appointment with the hospital
nurse?
• Answered: 22 • Skipped: 0

Q2: Did any issues arise during this appointment that you were unsure how to
manage? (e.g. patient did not attend, a specific patient request, investigations etc.)
• Answered: 21 • Skipped: 1

Q4: How useful did you find the Follow-Up Care Plan?
• Answered: 22 • Skipped: 0

Q5: Have you used the information in the Follow-Up Care Plan to guide a discussion with your patient about their ongoing issues
/ concerns?
• Answered: 21 • Skipped: 1

Q6: Have you used the Follow-Up Care Plan to develop your own management plans / care
plans?
• Answered: 19 • Skipped: 3

Q8: Do you feel confident in providing follow-up cancer care for your patient?
• Answered: 21 • Skipped: 1
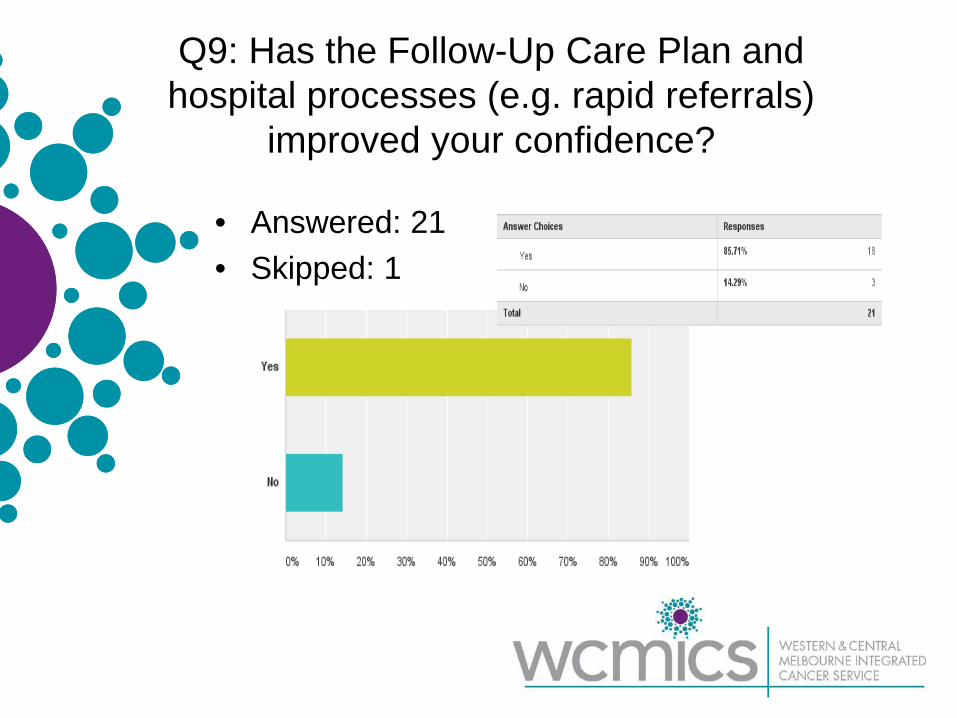
Q9: Has the Follow-Up Care Plan and hospital processes (e.g. rapid referrals)
improved your confidence?
• Answered: 21 • Skipped: 1

Q10: Are you aware of the rapid outpatient referral process back to the
Gynae-Oncology Service?
• Answered: 22 • Skipped: 0

Q11: Are you confident that you can access timely guidance and support from the
Gynae-Oncology Service?
• Answered: 20 • Skipped: 2

Thank you.
Any questions?

Development of an online
education resource to improve nursing care of older people with
cancer Mei Krishnasamy
Chair in Cancer Nursing University of Melbourne
VCCC: Research and Education Lead - Nursing

The GO Resource
Project Team Consumer Member • Heather Watson QUT • Kylie Ash RMH • Joanne Martin Western Health • Oanh Nguyen • Shannon Uren UoM • Mei Krishnasamy (PI)
PeterMac • Rose Kamateros • Cathie Pigott • Sarah Blashke RWH • Jason Dakin • Jess Jude EviQ • Shelley Rushton • Annie Zheng WCMICS • Di Saward
Background and Rationale
2015 Intergenerational Report • Number of Australians aged 65 years
and over - projected to more than double by 2054-55 compared with 2015
• By 2054-55: 4.9 per cent of the population(~ 2 million Australians) will be aged 85 and over
2015 Intergenerational Report. Australia in 2055: http://www.treasury.gov.au

https://canceraustralia.gov.au/affected-cancer/cancer-statistics

The imperative • Older people (> 65 years) are less likely to
undergo screening, receive surgery, radiotherapy or chemotherapy than younger people (Berger et al, Trans Am Clin Climatol Assoc. 2006; Uyar et al, Gynecol Oncol. 2005; Koroukian, Health Serv Res. 2005)
• Physical suitability for treatment or patient
preference seem unlikely to fully explain disparity in treatments (NCIN, 2013)
• Older people less likely to report suboptimal
experiences of care (NHS, CPES, 2014; VCCC, CPES, 2014)

The gap • No dedicated geriatric oncology nursing
learning resource
• Integration of geriatric oncology into the training programs of healthcare professionals – recognised by SIOG* as an urgent priority
* SIOG: International Society of Geriatric Oncology. http://www.siog.org/content/siog-10-priorities-initiative (2012)

Project objectives
• To develop the first Australian geriatric oncology nursing online education resource to support knowledge development of nurses caring for older people with cancer
• To carry out end user pilot testing of the resource to assess functionality and relevance of content to practice

Project governance
Project Team
Consumer Advisors
Nurses
Expert Review Panel
Inform & feedback: teaching and learning expertise and content, module structure and storyboarding, language, images, screening tools, cultural diversity, ethical concepts, quizzes, interactive learning activities, relevance to practice

The process
Revised to include
consumers
Literature reviews,
searches , video
development
CNSA members

Deliverable: The Resource


Evaluation • 21st of March - 30th of May 2016 • Nurses from PeterMac, RWH, RMH
and, the Cancer Nurses Society of Australia (CNSA)
• Following ethics, nurses approached via NUMS/CNSA
• Study information and link to resources emailed to potential participants
• Link provided to resources and unique ID allocated

Participants ( n= 92) Victoria 40
QLD 21
NSW 15
WA 8
SA 4
Tasmania 3
NT 1

Evaluation: Function, Relevance to Practice and Self-Reported Impact on
Knowledge Function:
• Format for how videos displayed • Streamlining of slides (removal of
unnecessary pop-ups) • Correction of typographical errors • Navigation streamlining • Review of response categories
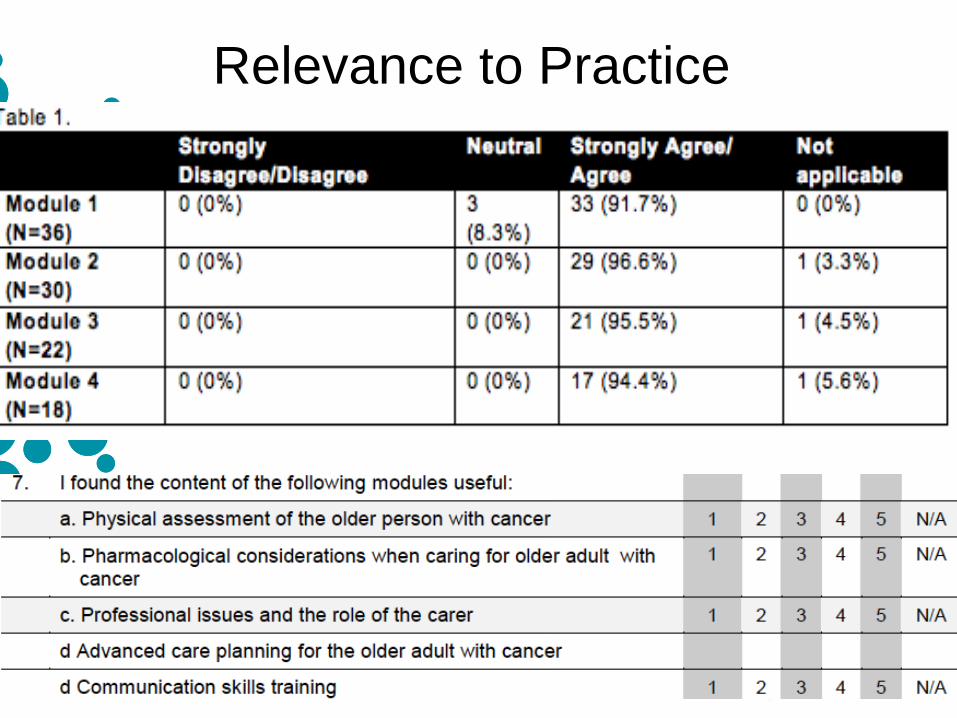
Relevance to Practice

Self-Reported Impact on Knowledge

Implementation and sustainability
• National launch at the Clinical Oncology Society of Australia- Annual Scientific Meeting (November 2016)
• Resource is housed on the eviQ website: https://education.eviq.org.au/courses/geriatric-oncology
• Dissemination via CNSA and COSA newsletters and flyers
• Project and resource presented at the CNSA, COSA conferences in 2015 and 2016
• Publication in preparation

Sustainability
• EviQ education team will monitor use – in line with all education resources hosted on their site: Google analytics
• Checklist/document produced by project team and retained by eviQ - with of slides were statistics may change and framework for review of new policies/evidence - coordinated by eviQ/CNSA

Next steps • Resource will be integrated into UoM
cancer and palliative care Grad Cert. programs
• Discussion underway to incorporate resource into the EdCan Cancer Nursing Competency Framework resources (Cancer Australia)
• More $s: to undertake formal evaluation of competence and competency
• To consider potential for role innovation and advancement

Thank you https://education.eviq.org.au/co
urses/geriatric-oncology
Diabetes Management - developing consensus
guidelines Kathleen Steele
Manager, Diabetes Education St Vincent’s Public Hospital Melbourne
Increasing numbers of patients with cancer expressed confusion and anxiety to our Credentialled Diabetes Nurse Educators (CDE) about:
• their diabetes management
• inconsistent advice titrating insulin doses
• no standardised approach
Background

• Reviewed the literature • Different prioritories by different specialist teams
• Needing a patient centered approach
How can we improve this experience ?
• Co-diagnosis of diabetes and cancer presents many challenges
• Hyperglycemia is associated with poor outcomes
• Lack of data on patients with cancer and diabetes
• Gap in clinical management resources for this group
• Corticosteroid guidelines exist, but are not specific for patients with cancer
• Patients are receiving differing recommendations for diabetes management.
Background Summary

Encouraged by Oncology Services Manager to: • Develop consensus guidelines
• apply for funding from WCMICS
• partner with another Health Service
Solution

Success

Approached previous successful WCMICS recipient for advice on
consensus guideline development
Ask for Advice

1. Planning Phase
• Recruited project manager 0.4EFT • Identified and appointed Steering Committee:
Consumer representative WCMICS representative Pharmacy representative Cancer Centre representative Endocrinologists from St V’s & RMH Oncologists from St V’s & RMH Credentialled Diabetes Nurse Educators-St V’s, RMH
• Comprehensive Lit review
• Ethics submission
Project Methodology

2. Review Phase 6 Month Retrospective Audit: to assess the diabetes management of patients undergoing chemotherapy in the cancer day centre. Data Analysis: 104 patients with diabetes identified:
– 71 (68%) no documented HbA1c – 25 (24%) no BGLs recorded
HbA1c not recorded, 71
HbA1c recorded, 33
HbA1c not recorded
HbA1c recorded

Snapshot audit of current patients in cancer centre short patient questionnaire 38 patient surveys collected 9 (24%) diagnosed with diabetes
• 7 had T2DM • 1 had steroid-induced diabetes • 1 had pre-diabetes
14 (37%) patients positive family history of diabetes

Healthcare Professional Survey Aim: to guide development of guidelines Method: Case Studies via survey monkey 41 Respondents included:
– 8 Medical Oncologists – 8 Dietitians – 6 Diabetes Nurse Educators – 5 Haematologists – 5 Pharmacists – 3 GPs – 2 Endo Reg – 2 Oncology Nurses – 2 Endocrinologists
Endo, 2
CDNE, 6
RN, 2
GP, 3
Oncologist, 8 Haematologist,
5
Pharmacist, 5
Endo Reg, 2
Dietitian, 8

• Respondents without background in diabetes were not confident in managing diabetes
33 requested information on managing diabetes in cancer patients -
81%
12 of 13 oncologists /Haematologists requested guidance-
92%
Results Health Care Professional Survey
• Inpatient cancer patients are (generally) managed appropriately • Many ambulatory pts are receiving therapy plus Dexamethasone
• I don’t remember how to treat diabetes and I’m not interested re-learning
• I don’t even think about sugar levels in my patients • A “high” but asymptomatic sugar is the least of my patients
problems • Someone needs to tell me:
• What to test and when • What might be an important result • What I can do • When I should refer to a Diabetic service
• It needs to be one page and in large font • It needs to be in the context of the:
• Cancer illness • Treatment intent (cure vs palliation)
The oncologists view …..
3. Development Phase Guidelines written as flow charts
Workshopped by project committee
Presented at the 2015 ADS/ADEA National Conference for
consensus approval
Voting poll - both online and written, to provide feedback
presented at the NADC Meeting in Sydney October 2015
3 month Pilot of Guidelines
Post pilot Audit completed
Project Methodology Cont’d
Implementing the guideline St Vincent’s RMH
The Greyhound Paradigm “You leave the driving to us”
The Hertz Paradigm “We’ll put you in the drivers seat

RMHResults • Data collected on 53 patients during pilot period • 14/53 (26%) had pre-existing diabetes • 2 referred with new diabetes
• HbA1c ordered in 28 patients • 4 had HbA1c >6.5% (without previously known diabetes)
• 38/53 (73%) received steroids
• 12 had glucose levels out of the target range. • 8 referred to the Diabetes Team

St Vincent’s Results • Data collected on177 patients attending Oncology
Day centre during the pilot phase • 11% - diagnosed diabetes • 31% had documented HbA1c measurement 11% had HbA1c >6.5%
• 80% received steroids during treatment • 52% had documented treatment changes • compared to 21% pre pilot

GC-glucocorticoid, HbA1c-glycated haemoglobin, FBG–fasting blood glucose, CDE–Credentialed Diabetes Educator, SBGM–Self Blood Glucose Monitoring, BG-Blood Glucose, BGL–blood glucose level, PP-post prandial, SU-Sulphonylurea, QID-4 times a day, HCP-healthcare professional.
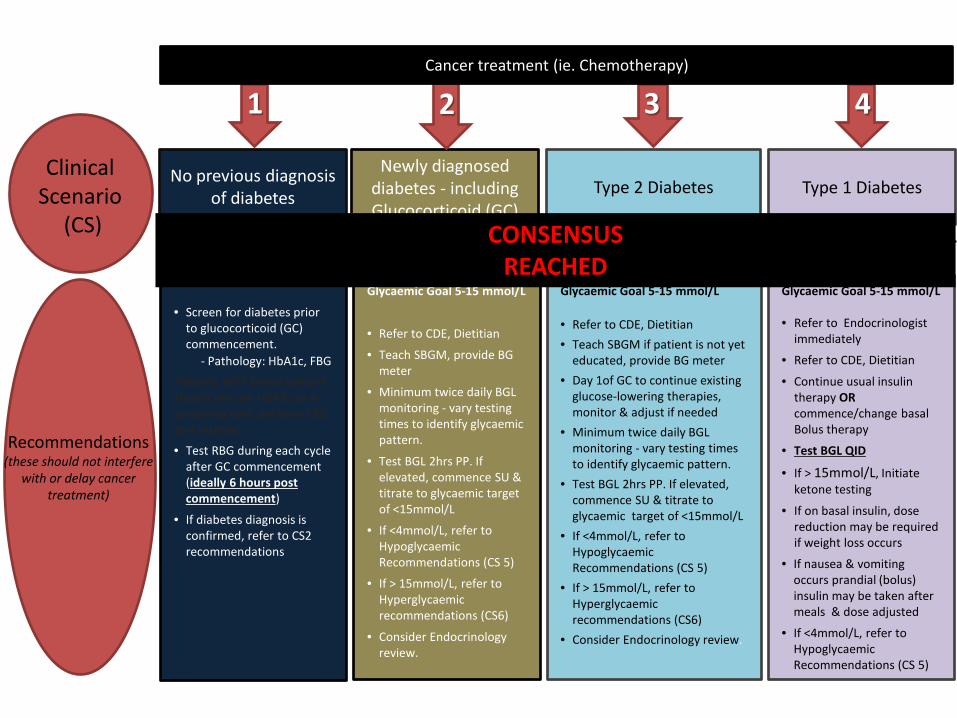
Glycaemic Goal 5-15 mmol/L
• Refer to CDE, Dietitian
• Teach SBGM, provide BG meter
• Minimum twice daily BGL monitoring - vary testing times to identify glycaemic pattern.
• Test BGL 2hrs PP. If elevated, commence SU & titrate to glycaemic target of <15mmol/L
• If <4mmol/L, refer to Hypoglycaemic Recommendations (CS 5)
• If > 15mmol/L, refer to Hyperglycaemic recommendations (CS6)
• Consider Endocrinology review.
Newly diagnosed diabetes - including Glucocorticoid (GC)
Induced
2
Glycaemic Goal 5-15 mmol/L • Refer to Endocrinologist
immediately
• Refer to CDE, Dietitian
• Continue usual insulin therapy OR commence/change basal Bolus therapy
• Test BGL QID
• If > 15mmol/L, Initiate ketone testing
• If on basal insulin, dose reduction may be required if weight loss occurs
• If nausea & vomiting occurs prandial (bolus) insulin may be taken after meals & dose adjusted
• If <4mmol/L, refer to Hypoglycaemic Recommendations (CS 5)
Type 1 Diabetes
4
• Screen for diabetes prior to glucocorticoid (GC) commencement.
- Pathology: HbA1c, FBG Patients with blood cancers should not use HbA1c as a screening tool, perform FBG test instead.
• Test RBG during each cycle after GC commencement (ideally 6 hours post commencement)
• If diabetes diagnosis is confirmed, refer to CS2 recommendations
1
No previous diagnosis of diabetes
Recommendations (these should not interfere
with or delay cancer treatment)
Clinical Scenario
(CS)
These guidelines aim to provide a standardised line of care for cancer patients who are 1) at high-risk of developing diabetes, 2) already diagnosed with diabetes or 3) those on high doses of Glucocorticoids (GC). The aim is for early detection of diabetes in these patients, improving management of resulting co-morbidities and enhancing patient’s QOL.
Glycaemic Goal 5-15 mmol/L • Refer to CDE, Dietitian • Teach SBGM if patient is not yet
educated, provide BG meter • Day 1of GC to continue existing
glucose-lowering therapies, monitor & adjust if needed
• Minimum twice daily BGL monitoring - vary testing times to identify glycaemic pattern.
• Test BGL 2hrs PP. If elevated, commence SU & titrate to glycaemic target of <15mmol/L
• If <4mmol/L, refer to Hypoglycaemic Recommendations (CS 5)
• If > 15mmol/L, refer to Hyperglycaemic recommendations (CS6)
• Consider Endocrinology review.
Type 2 Diabetes
3 Cancer treatment (ie. Chemotherapy)
CONSENSUS REACHED

SEEK MEDICAL ADVICE IF: • Blood glucose does not improve despite 2 supplemental insulin doses or remains > 20.0 mmol/L or those unable to administer supplementary insulin • Ketones are moderate to heavy (urine) / >1.5 mmol/L (blood) or present & not decreasing with supplemental insulin • Signs of DKA /HHS are present such as vomiting, drowsiness, confusion, disorientation, hyperventilation, dehydration or severe abdominal pain • Vomiting is persistent especially if frequent for more than 2-4 hours or becomes blood- or bile- stained • Hypoglycaemia is severe or blood glucose cannot be maintained above 4.0 mmol/L • Severe dehydration • Patient unable to fulfil recommendations or safely self-manage insulin/monitoring
Nausea & vomiting
7
For hypoglycaemia prevention (< 4mmol/L) • Reduce insulin (up to 20-50%) of total daily dose • Consider reducing SU
For persistent hyperglycaemia > 20mmol/L • Administer up to 10%- 20% of total daily
dose supplemental insulin
• Patients with Type 1 diabetes should check for ketonaemia
• PATIENTS WITH TYPE 1 DIABETES MUST NOT CEASE INSULIN • Symptoms need to be differentiated from hyperglycaemia, hypoglycaemia or ketoacidosis. • Intercurrent illness needs to be diagnosed & treated • Test BGL QID, initiate more frequent monitoring of BGL levels • Prandial insulin may be taken after meals & dose adjusted if nausea or vomiting occurs
If unable to consume food administer: • Carbohydrate containing fluids if blood glucose < 15.0 mmol/L • Carbohydrate free fluids if blood glucose > 15.0 mmol/L
GC-glucocorticoid, HbA1c-glycated haemoglobin, FBG–fasting blood glucose, CDE–Credentialed Diabetes Educator, SBGM–Self Blood Glucose Monitoring, BG-Blood Glucose, BGL–blood glucose level, PP-post prandial, SU-Sulphonylurea, QID-4 times a day, HCP-healthcare professional.
Clinical Scenario
(CS)
Recommendations (these should not interfere
with or delay cancer treatment)
Cancer treatment (ie. Chemotherapy)
These guidelines aim to provide a standardised line of care for cancer patients who are 1) at high-risk of developing diabetes, 2) already diagnosed with diabetes or 3) those on high doses of Glucocorticoids (GC). The aim is for early detection of diabetes in these patients, improving management of resulting co-morbidities and enhancing patient’s QOL.
CONSENSUS REACHED
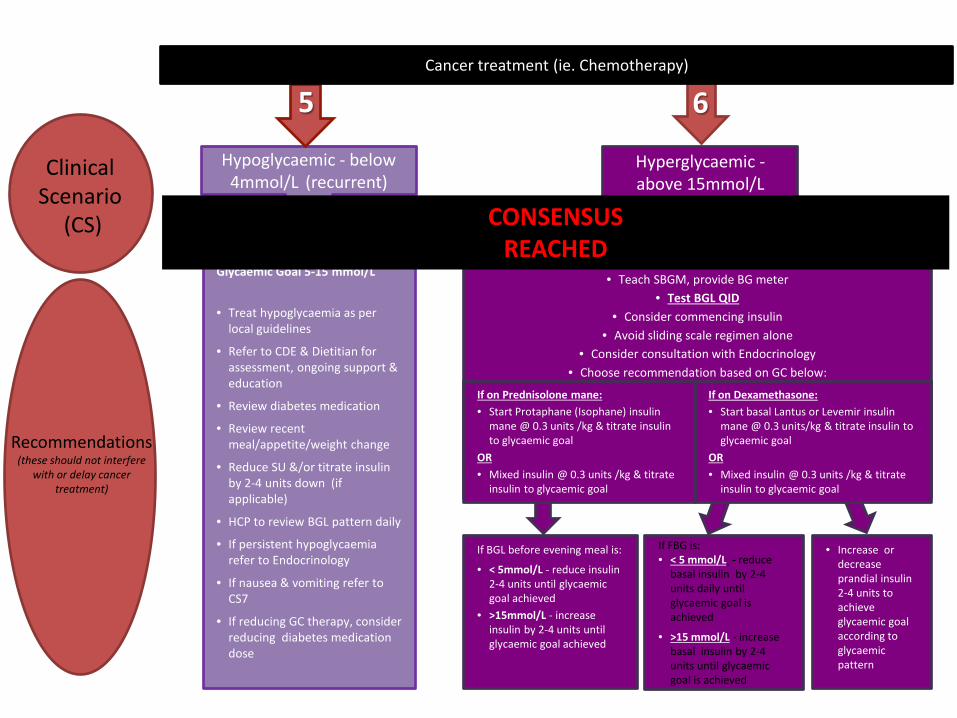
Glycaemic Goal 5-15 mmol/L
• Treat hypoglycaemia as per local guidelines
• Refer to CDE & Dietitian for assessment, ongoing support & education
• Review diabetes medication
• Review recent meal/appetite/weight change
• Reduce SU &/or titrate insulin by 2-4 units down (if applicable)
• HCP to review BGL pattern daily
• If persistent hypoglycaemia refer to Endocrinology
• If nausea & vomiting refer to CS7
• If reducing GC therapy, consider reducing diabetes medication dose
Hypoglycaemic - below 4mmol/L (recurrent)
5
Clinical Scenario
(CS)
If FBG is: • < 5 mmol/L - reduce
basal insulin by 2-4 units daily until glycaemic goal is achieved
• >15 mmol/L - increase basal insulin by 2-4 units until glycaemic goal is achieved
If BGL before evening meal is:
• < 5mmol/L - reduce insulin 2-4 units until glycaemic goal achieved
• >15mmol/L - increase insulin by 2-4 units until glycaemic goal achieved
• Increase or decrease prandial insulin 2-4 units to achieve glycaemic goal according to glycaemic pattern
Glycaemic Goal 5-15 mmol/L • Teach SBGM, provide BG meter
• Test BGL QID • Consider commencing insulin
• Avoid sliding scale regimen alone • Consider consultation with Endocrinology
• Choose recommendation based on GC below: If on Prednisolone mane:
• Start Protaphane (Isophane) insulin mane @ 0.3 units /kg & titrate insulin to glycaemic goal
OR • Mixed insulin @ 0.3 units /kg & titrate
insulin to glycaemic goal
If on Dexamethasone: • Start basal Lantus or Levemir insulin
mane @ 0.3 units/kg & titrate insulin to glycaemic goal
OR • Mixed insulin @ 0.3 units /kg & titrate
insulin to glycaemic goal
Hyperglycaemic - above 15mmol/L
6
GC-glucocorticoid, HbA1c-glycated haemoglobin, FBG–fasting blood glucose, CDE–Credentialed Diabetes Educator, SBGM–Self Blood Glucose Monitoring, BG-Blood Glucose, BGL–blood glucose level, PP-post prandial, SU-Sulphonylurea, QID-4 times a day, HCP-healthcare professional.
Recommendations (these should not interfere
with or delay cancer treatment)
Cancer treatment (ie. Chemotherapy)
These guidelines aim to provide a standardised line of care for cancer patients who are 1) at high-risk of developing diabetes, 2) already diagnosed with diabetes or 3) those on high doses of Glucocorticoids (GC). The aim is for early detection of diabetes in these patients, improving management of resulting co-morbidities and enhancing patient’s QOL.
CONSENSUS REACHED

What Next
Recommendations not rigid protocols Writing guidelines for publication Develop optimal method of promoting guidelines for GPs & those working in cancer centres

WCMICS Steering Committee
• Professor Richard MacIsaac • Laita Bokhari • Kathleen Steele • Professor Glenn Ward • Elizabeth Mulrooney • Andrew Cording • Lesa Stewart • Dr. Sue Ann McLachlan
• Professor Peter Colman • Carmel Parlapiano • Katie Marley • Professor Mark Rosenthal
• Graham Giles
• Sue Kirsa