women and brain injury biac conference 11 july 2008 carmela hutchison, president disabled...
TRANSCRIPT

Women and Brain InjuryWomen and Brain InjuryBIAC Conference BIAC Conference
11 July 200811 July 2008Carmela Hutchison, PresidentCarmela Hutchison, President
DisAbled Women's Network Canada-DisAbled Women's Network Canada-Réseau d‘action des femmes Réseau d‘action des femmes
handicapées du Canadahandicapées du Canada
LateLate Breaking NewsBreaking News Brain Injury Professional, published by the Brain Injury Professional, published by the North America Brain Injury SocietyNorth America Brain Injury Society (NABIS). (NABIS).
This issue is devoted to This issue is devoted to Women's Issues in Brain InjuryWomen's Issues in Brain Injury. .
This issue includes the following topics:This issue includes the following topics:
1. Women Care Givers: The Long-Term Effects on Health and Well Being1. Women Care Givers: The Long-Term Effects on Health and Well Being
2. The Effects of Chemotherapy on Cognition in Breast Cancer Survivors: Implications for 2. The Effects of Chemotherapy on Cognition in Breast Cancer Survivors: Implications for NeurorehabilitationNeurorehabilitation
3. My Life After the Injury: A Women's Story written by Marvel Vena3. My Life After the Injury: A Women's Story written by Marvel Vena
4. Women and Sexuality Post-TBI 4. Women and Sexuality Post-TBI
5. What Does Menopause Have To Do With Traumatic Brain Injury? A Case for 5. What Does Menopause Have To Do With Traumatic Brain Injury? A Case for ProgesteroneProgesterone
6. Health Concerns of Women with Brain Injury6. Health Concerns of Women with Brain Injury
7. Participatory Action Research in Women Living With the Consequences of Brain Injury 7. Participatory Action Research in Women Living With the Consequences of Brain Injury
Congratulations goes out to Elisabeth Sherwin, Ph.D. who served as this issue's guest Congratulations goes out to Elisabeth Sherwin, Ph.D. who served as this issue's guest editor. Hopefully Dr. Sherwin's goal of starting the ball rolling, that is, getting people to editor. Hopefully Dr. Sherwin's goal of starting the ball rolling, that is, getting people to speak about women's issues in traumatic brain injury will be fulfilled. Dr. Sherwin speak about women's issues in traumatic brain injury will be fulfilled. Dr. Sherwin certainly has got the ball rolling, and we all look forward to the forward to the success of certainly has got the ball rolling, and we all look forward to the forward to the success of this endeavor.this endeavor.
http://http://www.braininjurylawblog.com/brain-injury-news-womens-issues-in-brain-injury.htmlwww.braininjurylawblog.com/brain-injury-news-womens-issues-in-brain-injury.html

Do Women Fare Worse? A Metaanalysis of Gender Differences Do Women Fare Worse? A Metaanalysis of Gender Differences in Outcome After Traumatic Brain Injuryin Outcome After Traumatic Brain Injuryfrom from Neurosurgical FocusNeurosurgical Focus Elena Farace, Ph.D., Wayne M. Alves, Ph.D., Department of Neurosurgery, University Elena Farace, Ph.D., Wayne M. Alves, Ph.D., Department of Neurosurgery, University of Virginia; and INC Research, Charlottesville, Virginiaof Virginia; and INC Research, Charlottesville, Virginia
The purpose of this metaanalysis was to investigate possible gender The purpose of this metaanalysis was to investigate possible gender differences in TBI sequelae. A quantitative review of published studies of differences in TBI sequelae. A quantitative review of published studies of TBI outcome revealed eight studies (20 outcome variables) of TBI in which TBI outcome revealed eight studies (20 outcome variables) of TBI in which outcome was reported separately for men and women. outcome was reported separately for men and women.
Outcome was worse in women than in men for 85% of the measured Outcome was worse in women than in men for 85% of the measured variables, with an average effect size of -0.15. Although clinical opinion is variables, with an average effect size of -0.15. Although clinical opinion is often that women tend to experience better outcomes than do men after often that women tend to experience better outcomes than do men after TBI, the opposite pattern was suggested in the results of this metaanalysis. TBI, the opposite pattern was suggested in the results of this metaanalysis.
However, this conclusion is limited by the fact that in only a small However, this conclusion is limited by the fact that in only a small percentage of the total published reports on TBI outcome was outcome percentage of the total published reports on TBI outcome was outcome described separately for each sex. A careful, prospective study of sex described separately for each sex. A careful, prospective study of sex differences in TBI outcome is clearly needed.differences in TBI outcome is clearly needed.
Likely to underestimate total new TBI cases per year, because studies Likely to underestimate total new TBI cases per year, because studies under-samples the survivors who sustain milder TBI and who are never under-samples the survivors who sustain milder TBI and who are never hospitalized. Approximately 99,000 new survivors of TBI each year are hospitalized. Approximately 99,000 new survivors of TBI each year are classified as disabled.[26] Survivors of TBI tend to be young, which means classified as disabled.[26] Survivors of TBI tend to be young, which means that there is a high life-long cost of disability that there is a high life-long cost of disability

OverviewOverview What little research exists on gender differences in TBI What little research exists on gender differences in TBI
outcome suggests that outcome may be worse in women outcome suggests that outcome may be worse in women than in men. than in men.
Reports that case fatality rates were elevated in women Reports that case fatality rates were elevated in women as compared with men in two age groups. as compared with men in two age groups.
Findings from the UCLA Brain Injury Research Center, in Findings from the UCLA Brain Injury Research Center, in which case fatality rates at the Emergency Department which case fatality rates at the Emergency Department (while in the intensive care unit and after leaving it) were (while in the intensive care unit and after leaving it) were shown to be significantly higher for women compared shown to be significantly higher for women compared with men. with men.
In addition, the rate of poor outcomes (that is, death, In addition, the rate of poor outcomes (that is, death, persistent vegetative state, and severe disability) was persistent vegetative state, and severe disability) was significantly elevated for women compared with men at significantly elevated for women compared with men at 6, 12, 18 months post discharge. 6, 12, 18 months post discharge.

Why is Gender so Why is Gender so important?important?
Female gender was a significant predictor of the Female gender was a significant predictor of the development of post concussive symptoms at 1 development of post concussive symptoms at 1 month after suffering mild TBImonth after suffering mild TBI
In TBI research, gender is likely to interact with In TBI research, gender is likely to interact with many other outcome variables. If gender many other outcome variables. If gender interactions are not understood, they may end up interactions are not understood, they may end up obscuring true findings in TBI research. For obscuring true findings in TBI research. For example, sex differences in the metabolism of a example, sex differences in the metabolism of a pharmacological intervention may obscure true pharmacological intervention may obscure true treatment effects. The sex of the survivor may be treatment effects. The sex of the survivor may be a very important risk factor of TBI outcome. a very important risk factor of TBI outcome.
MethodologyMethodology
The procedures for performing a metaanalysis were followed. The procedures for performing a metaanalysis were followed. The published English-language literature on TBI outcome was The published English-language literature on TBI outcome was reviewed. Studies were included if they were published in a reviewed. Studies were included if they were published in a peer-reviewed journal or an edited book and were published peer-reviewed journal or an edited book and were published before January 1998. before January 1998.
While this study is older, it is still one of the only ones that had While this study is older, it is still one of the only ones that had the data I found relevant to our purpose, a common problem the data I found relevant to our purpose, a common problem pertaining to many women’s studies pertaining to many women’s studies
Even papers from our DAWN-RAFH Canada are still sought for Even papers from our DAWN-RAFH Canada are still sought for their value even though the research is 20 years old, it is often their value even though the research is 20 years old, it is often the only existing gender analysis. We need more research in the only existing gender analysis. We need more research in many areas of gender analysis and brain injury is no exception. many areas of gender analysis and brain injury is no exception. Journals should also be made free on line to survivors whose Journals should also be made free on line to survivors whose lives and decisions depend on the quality of information and lives and decisions depend on the quality of information and this dissemination strategy should be built in every grantthis dissemination strategy should be built in every grant

MethodologyMethodology Studies were required to include survivors who Studies were required to include survivors who
had suffered TBI and at least one outcome had suffered TBI and at least one outcome measure was reported separately for men and measure was reported separately for men and women. survivors were required to be 12 years of women. survivors were required to be 12 years of age or older. age or older.
An initial search on Medline resulted in 16,302 An initial search on Medline resulted in 16,302 references for "brain injuries," limited to 9822 for references for "brain injuries," limited to 9822 for English-language articles. Adding "sex or gender" English-language articles. Adding "sex or gender" reduced the number to 40 references, most of reduced the number to 40 references, most of which had been selected because the statement which had been selected because the statement "age and sex-matched controls" was included. "age and sex-matched controls" was included. These 40 studies were reviewed to determine if These 40 studies were reviewed to determine if they reported results separately for each sex. they reported results separately for each sex.

MethodologyMethodology In one study in which data were reported separately by sex there In one study in which data were reported separately by sex there
was considerable bias in its methodology, and it was excluded (the was considerable bias in its methodology, and it was excluded (the outcome measure was spouses' perceptions of change in the outcome measure was spouses' perceptions of change in the survivors' sexual behavior, in a sex-segregated Indian culture survivors' sexual behavior, in a sex-segregated Indian culture wherein only two wives spoke about their husbands, but all the wherein only two wives spoke about their husbands, but all the husbands spoke about their wives' behavior). The sample of husbands spoke about their wives' behavior). The sample of manuscripts was therefore limited to eight studies which, manuscripts was therefore limited to eight studies which, together, contained 20 variables for which outcome in men and together, contained 20 variables for which outcome in men and women was reported separately.women was reported separately.
Then the researchers made a selection of variables for analysis Then the researchers made a selection of variables for analysis and designed their statistical analysisand designed their statistical analysis
The first finding of interest in this metaanalysis was the small The first finding of interest in this metaanalysis was the small number of studies available for inclusion. The primary literature on number of studies available for inclusion. The primary literature on TBI outcomes is obviously much larger than that represented by TBI outcomes is obviously much larger than that represented by the studies included in this metaanalysis, but we included only in the studies included in this metaanalysis, but we included only in which results were reported separately for men and women.which results were reported separately for men and women.
EpidemiologyEpidemiology
Gender differences in the incidence of TBI are Gender differences in the incidence of TBI are well known.well known.
Survivors hospitalized in 1981 for mild head injury Survivors hospitalized in 1981 for mild head injury (Glasgow Coma Scale scores of 13--15) and found (Glasgow Coma Scale scores of 13--15) and found that the incidence was approximately twice as that the incidence was approximately twice as high in male as in female survivorshigh in male as in female survivors
In a different study the investigators found that in In a different study the investigators found that in men under age 65 years the rate of head injury men under age 65 years the rate of head injury was almost three times as high as in women in a was almost three times as high as in women in a Scottish sample of head-injured survivors.Scottish sample of head-injured survivors.
EpidemiologyEpidemiology Though men sustain a greater number of TBIs than women, Though men sustain a greater number of TBIs than women,
women still compromise a substantial portion of TBI survivors (one women still compromise a substantial portion of TBI survivors (one quarter to one third of the population according to these quarter to one third of the population according to these estimates).estimates).
The gender difference found in the incidence of TBI is only seen The gender difference found in the incidence of TBI is only seen from puberty until middle age, leaving a large part of the life span from puberty until middle age, leaving a large part of the life span with roughly equal rates of TBI between the sexes.with roughly equal rates of TBI between the sexes.
In several studies it has been shown that there are no gender In several studies it has been shown that there are no gender differences in the incidence of children sustaining TBI.differences in the incidence of children sustaining TBI.
In adults the incidence of TBI appears to be approximately the In adults the incidence of TBI appears to be approximately the same in men and women aged 45 to 75.same in men and women aged 45 to 75.
In older survivors (65 years of age or older) no gender shown In older survivors (65 years of age or older) no gender shown differences have been shown in the rate of TBI, with a sex ratio of differences have been shown in the rate of TBI, with a sex ratio of 49% men and 51% women. After age 75 years, there is a slightly 49% men and 51% women. After age 75 years, there is a slightly higher incidence of mild head injury in women, due mostly to falls.higher incidence of mild head injury in women, due mostly to falls.

EpidemiologyEpidemiology
Gender of the Survivor may in fact be a very Gender of the Survivor may in fact be a very important factor of TBI outcome. There appeared important factor of TBI outcome. There appeared to be only one published report specifically to be only one published report specifically designed to study the effect of sex on TBI designed to study the effect of sex on TBI outcome.outcome.
A thorough, metaanalytic review could help to A thorough, metaanalytic review could help to tease out possible gender differences in TBI tease out possible gender differences in TBI outcome and to identify important gaps in our outcome and to identify important gaps in our knowledge regarding recovery and outcome after knowledge regarding recovery and outcome after brain injury. brain injury.

EpidemiologyEpidemiology
Based on the available evidence for TBI Outcome Based on the available evidence for TBI Outcome Predictors, the following questions were Predictors, the following questions were formulated:formulated:
1) Is there a gender difference in TBI outcome, and 1) Is there a gender difference in TBI outcome, and if so, what is the magnitude of that difference?if so, what is the magnitude of that difference?
2) Does a gender difference depend on the specific 2) Does a gender difference depend on the specific outcome measureoutcome measure
Worse Outcome in WomenWorse Outcome in Women
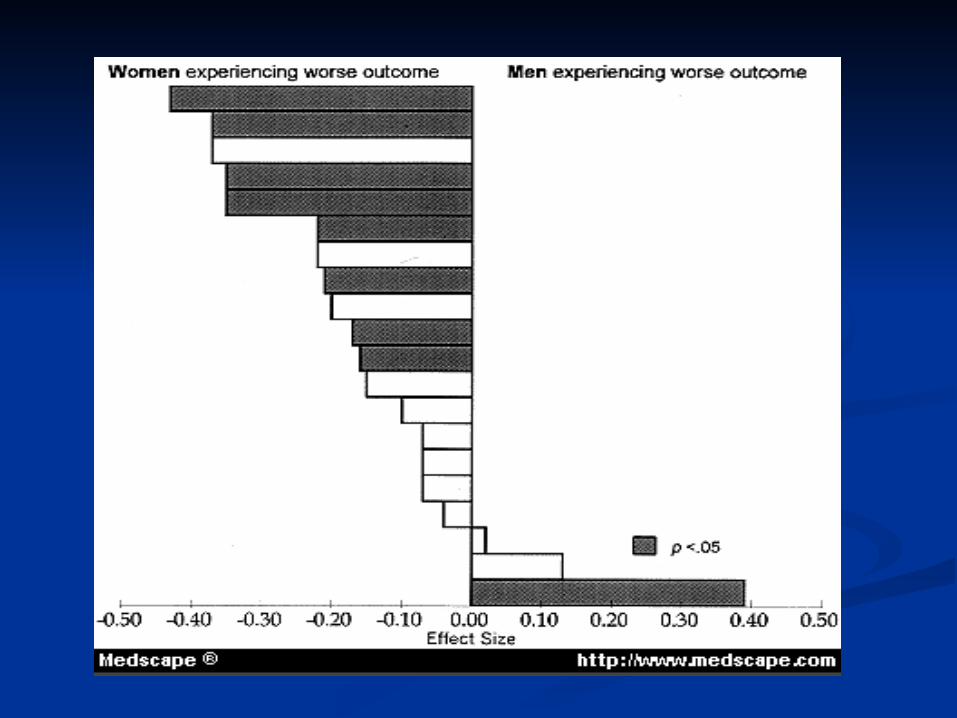
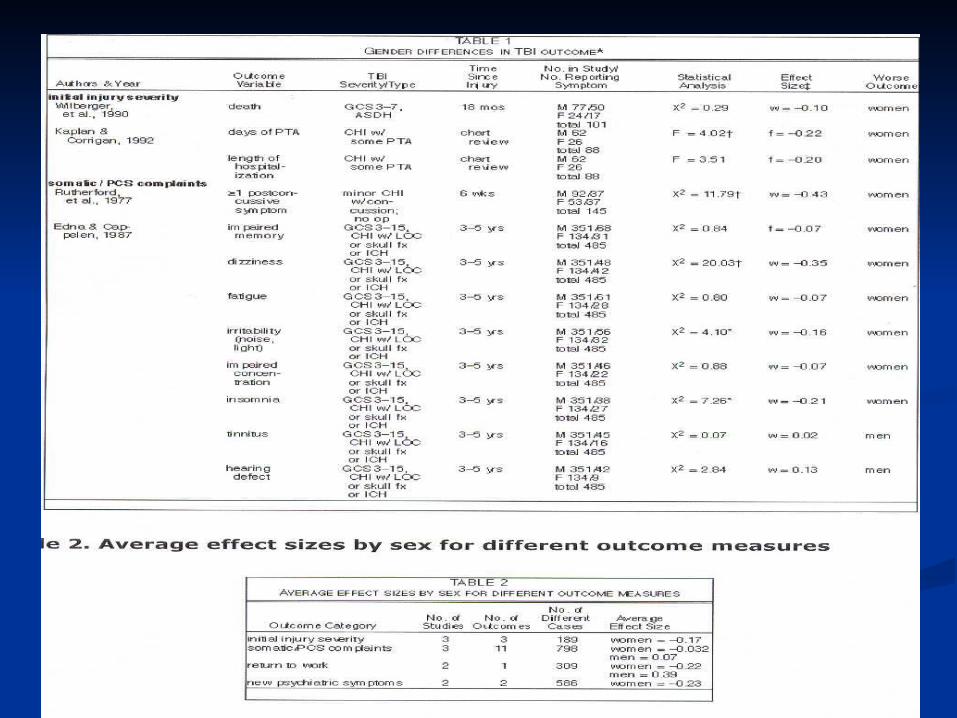
On average, outcome after TBI was found to be worse in On average, outcome after TBI was found to be worse in women than in men, regardless of the variable being women than in men, regardless of the variable being analyzed. in 17 (85%) of 20 outcome variables classified by analyzed. in 17 (85%) of 20 outcome variables classified by sex, outcome after TBI was worse in women across all sex, outcome after TBI was worse in women across all brain-injury types. Analysis of the results indicated that the brain-injury types. Analysis of the results indicated that the outcome gender ratios reported in the table on the next outcome gender ratios reported in the table on the next slide were very unlikely to happen by chanceslide were very unlikely to happen by chance
To understand the magnitude of these gender differences To understand the magnitude of these gender differences in TBI outcome, the table in the next slide includes the in TBI outcome, the table in the next slide includes the effect sizes of the gender differences at the study level. effect sizes of the gender differences at the study level. According to research practices, 0.1 can be considered a According to research practices, 0.1 can be considered a small effect size, 0.3 a medium effect size, and 0.5 a large small effect size, 0.3 a medium effect size, and 0.5 a large effect size. The mean effect size for this metaanalysis was -effect size. The mean effect size for this metaanalysis was -0.15 (the negative sign indicates women having worse 0.15 (the negative sign indicates women having worse outcome).outcome).

Worse Outcome in WomenWorse Outcome in Women
the largest effect size was found for having one or more post the largest effect size was found for having one or more post concussive symptoms at 6 weeks, with small to medium effect concussive symptoms at 6 weeks, with small to medium effect sizes shown for headache, dizziness insomnia, no return to work, sizes shown for headache, dizziness insomnia, no return to work, days of posttraumatic amnesia, and length of hospitalization. days of posttraumatic amnesia, and length of hospitalization. Outcomes were significantly worse in women (significance Outcomes were significantly worse in women (significance calculated within studies) than they were in men with regard to all calculated within studies) than they were in men with regard to all of these outcome variables except one: no return to work.of these outcome variables except one: no return to work.
The results of the study reported by one author (McMordie, et al.) The results of the study reported by one author (McMordie, et al.) are difficult to explain, considering the fact that in the same study are difficult to explain, considering the fact that in the same study women were found to have sustained more days of loss of women were found to have sustained more days of loss of consciousness (mean 42.83 days for men and 45.94 days for consciousness (mean 42.83 days for men and 45.94 days for women). It is interesting to note that this study also had the women). It is interesting to note that this study also had the longest length of time from injury to assessment (mean 6.7 years), longest length of time from injury to assessment (mean 6.7 years), perhaps suggesting an interaction of gender with outcome over perhaps suggesting an interaction of gender with outcome over time.time.

Worse Outcome in WomenWorse Outcome in Women
it may have been that only in studies with it may have been that only in studies with surprising differences between the sexes surprising differences between the sexes was data reported separately by sex. was data reported separately by sex. However, the rarity of studies reporting However, the rarity of studies reporting data separately for each sex, whether or data separately for each sex, whether or not the outcome differences were not the outcome differences were significant, suggests that gender has significant, suggests that gender has simply not been previously considered to simply not been previously considered to be an important risk factor in TBI outcome be an important risk factor in TBI outcome

Worse In WomenWorse In Women What might be the source of a sex difference in TBI outcome? Factors such What might be the source of a sex difference in TBI outcome? Factors such
as length of time from injury to the emergency room, age, premorbid as length of time from injury to the emergency room, age, premorbid functioning, location of damage within the brain, and type of lesion functioning, location of damage within the brain, and type of lesion produced, that influence TBI outcome are expected to vary randomly in a produced, that influence TBI outcome are expected to vary randomly in a population, and, therefore, are not expected to produce a sex difference in population, and, therefore, are not expected to produce a sex difference in TBI outcome. However, some of these factors potentially do correlate or TBI outcome. However, some of these factors potentially do correlate or interact with TBI survivor gender and may therefore relate to a difference interact with TBI survivor gender and may therefore relate to a difference in outcome. in outcome.
For example, men and women who sustain brain injuries may differ For example, men and women who sustain brain injuries may differ premorbidly. Traumatic brain injury sequelae may be reported differently. premorbidly. Traumatic brain injury sequelae may be reported differently.
Women may sustain different injuries, due to morphological differences in Women may sustain different injuries, due to morphological differences in our brains or to different causes of trauma. Established sex differences in our brains or to different causes of trauma. Established sex differences in cognitive ability and psychosocial factors may also play a role, as may cognitive ability and psychosocial factors may also play a role, as may differences in functional brain organization. differences in functional brain organization.
Sex hormones may affect outcome after TBI. Different treatments may Sex hormones may affect outcome after TBI. Different treatments may affect men and women differently. affect men and women differently.
A discussion of each of these possibilities follows A discussion of each of these possibilities follows
Premorbid FactorsPremorbid Factors Given that fewer women than men sustain TBI, perhaps the Given that fewer women than men sustain TBI, perhaps the
women who do suffer TBI differ systematically from the women who do suffer TBI differ systematically from the overall population. overall population.
For example, do men and women who sustain a TBI differ in For example, do men and women who sustain a TBI differ in premorbid IQ? Premorbid IQ is a significant predictor of TBI premorbid IQ? Premorbid IQ is a significant predictor of TBI outcome, given survival.outcome, given survival.
Sex differences may also exist in premorbid psychosocial Sex differences may also exist in premorbid psychosocial
factors such as family function, problem-solving skills, factors such as family function, problem-solving skills, education, employment, socioeconomic status, and medical education, employment, socioeconomic status, and medical insurance, all of which have been shown to be significant insurance, all of which have been shown to be significant predictors of outcome after TBI, although sex differences in predictors of outcome after TBI, although sex differences in these factors have not yet been tested in the TBI populationthese factors have not yet been tested in the TBI population
Symptom ReportingSymptom Reporting Sex differences in TBI outcome may result from the Sex differences in TBI outcome may result from the
different ways in which the two sexes report illness and different ways in which the two sexes report illness and symptoms. Indeed, more women report illnesses and make symptoms. Indeed, more women report illnesses and make more physician visits per person each year than men.more physician visits per person each year than men.
It may be easier for women to admit to having symptoms It may be easier for women to admit to having symptoms such as headaches, fatigue, anxiety, or depression than such as headaches, fatigue, anxiety, or depression than men. men.
When an outcome variable is subjective and/or nonspecific, When an outcome variable is subjective and/or nonspecific, such as fatigue, a difference in "outcome" between male such as fatigue, a difference in "outcome" between male and female survivors may simply be the result of the way in and female survivors may simply be the result of the way in which the sexes report behavior my editorial comment or which the sexes report behavior my editorial comment or the way researchers/caregivers interpret it. the way researchers/caregivers interpret it.
However, when the outcome variable is a more objective However, when the outcome variable is a more objective measure, such as a test score, or is an irrefutable measure, measure, such as a test score, or is an irrefutable measure, such as death, outcome is unlikely to be related to such as death, outcome is unlikely to be related to symptom-reporting behavior. symptom-reporting behavior.

Injury FactorsInjury Factors Outcome after TBI may differ in men and women because of Outcome after TBI may differ in men and women because of
gender-related behavioral patterns that cause the traumatic gender-related behavioral patterns that cause the traumatic accident. accident.
There is a great deal of evidence that men, especially young men, There is a great deal of evidence that men, especially young men, engage in risk-taking behavior far more frequently than women. engage in risk-taking behavior far more frequently than women.
According to the National Highway Traffic Safety Administration, According to the National Highway Traffic Safety Administration, men are more than twice as likely to be the driver in fatal car men are more than twice as likely to be the driver in fatal car crashes, and women are more likely to be the passenger in a car crashes, and women are more likely to be the passenger in a car crash. crash.
Men and women differ in safety-related activity such as using a Men and women differ in safety-related activity such as using a seatbelt or wearing a helmet. The National Highway Traffic Safety seatbelt or wearing a helmet. The National Highway Traffic Safety Administration study reported seatbelt use in 68% of women and Administration study reported seatbelt use in 68% of women and 56.8% of men in 1996. 56.8% of men in 1996.
Women may experience worse outcomes after TBI because they Women may experience worse outcomes after TBI because they are more likely to wear seatbelts and helmets and perhaps the use are more likely to wear seatbelts and helmets and perhaps the use of safety restraints changes the site of impact or increases the of safety restraints changes the site of impact or increases the severity needed to cause an injury. severity needed to cause an injury.
Cognition and Psychosocial Cognition and Psychosocial FactorsFactors
If women have worse outcomes than men after TBI, why is If women have worse outcomes than men after TBI, why is this effect not globally recognized? One possibility is that this effect not globally recognized? One possibility is that the worse outcomes reported in women may have been the worse outcomes reported in women may have been masked by women's relative strength in verbal fluency masked by women's relative strength in verbal fluency ability, which has been shown in a metaanalysis to have a ability, which has been shown in a metaanalysis to have a medium effect size.medium effect size.
When functional criteria for discharge requires that a When functional criteria for discharge requires that a survivor be able to ambulate and communicate, women's survivor be able to ambulate and communicate, women's superior verbal fluency, even after brain injury, may falsely superior verbal fluency, even after brain injury, may falsely cause their outcome to appear better than it actually is. In cause their outcome to appear better than it actually is. In these cases, women's strengths may be limited to speaking these cases, women's strengths may be limited to speaking ability, with significant performance and/or functional ability, with significant performance and/or functional deficits remaining undetected. This effect may cause an deficits remaining undetected. This effect may cause an overestimation of women's true level of function by their overestimation of women's true level of function by their caretakers and physicians, and it may result in women caretakers and physicians, and it may result in women being discharged before sufficient recovery, leading to being discharged before sufficient recovery, leading to worse outcome. worse outcome.

Gender Differences in Brain FunctionGender Differences in Brain Function Analysis of a growing body of evidence demonstrates that men's Analysis of a growing body of evidence demonstrates that men's
and women's brains differ in functional organization. In studies of and women's brains differ in functional organization. In studies of unilateral lesions in stroke survivors women have been shown to unilateral lesions in stroke survivors women have been shown to have more bilateral representation of Verbal and Performance IQ have more bilateral representation of Verbal and Performance IQ than men. than men.
This bilateral representation of verbal skills (spatial skills were not This bilateral representation of verbal skills (spatial skills were not tested) has also been supported by the results of a functional tested) has also been supported by the results of a functional magnetic resonance imaging study in which the authors found magnetic resonance imaging study in which the authors found that women possessed greater bilateral verbal-processing ability that women possessed greater bilateral verbal-processing ability in a lexical decision task than men.in a lexical decision task than men.
It is possible that a sex difference in brain organization relates to It is possible that a sex difference in brain organization relates to a sex difference in TBI outcome. Perhaps diffuse brain injury in TBI a sex difference in TBI outcome. Perhaps diffuse brain injury in TBI has a greater chance of affecting relevant function in women's has a greater chance of affecting relevant function in women's brains because there is a greater chance of the injury affecting a brains because there is a greater chance of the injury affecting a brain area, whereas men's more focally organized brains may be brain area, whereas men's more focally organized brains may be relatively spared. relatively spared.

Sex Hormones and TBI SequelaeSex Hormones and TBI Sequelae An interaction of TBI sequelae with sex hormones may relate to differences An interaction of TBI sequelae with sex hormones may relate to differences
in TBI outcome between men and women. Alkayed, et al. have found that in TBI outcome between men and women. Alkayed, et al. have found that estrogen had a protective effect against ischemia in female rats in which estrogen had a protective effect against ischemia in female rats in which they used an experimental stroke paradigm. they used an experimental stroke paradigm.
However, in an experimental brain trauma study, the authors found a However, in an experimental brain trauma study, the authors found a protective effect of estrogen (improvement in free magnesium protective effect of estrogen (improvement in free magnesium concentration, cytosolic phosphorylation potential, and motor function) concentration, cytosolic phosphorylation potential, and motor function) only in male rats. Lowered cytosolic phosphorylation potential after trauma only in male rats. Lowered cytosolic phosphorylation potential after trauma and higher mortality rates were demonstrated in all groups of female rats.and higher mortality rates were demonstrated in all groups of female rats.
Progesterone has also been shown to have a protective effect in reducing Progesterone has also been shown to have a protective effect in reducing brain edema in TBI sequelae in female rats.brain edema in TBI sequelae in female rats.
In progesterone-treated male and female rats a reduction in behavioral In progesterone-treated male and female rats a reduction in behavioral impairment and reduced neuronal degeneration 21 days after injury were impairment and reduced neuronal degeneration 21 days after injury were also demonstrated. A potential negative effect of sex hormones, especially also demonstrated. A potential negative effect of sex hormones, especially estrogen, may lead to a worse outcome in women after TBI. estrogen, may lead to a worse outcome in women after TBI.

Treatment EffectsTreatment Effects Differences in metabolism between the sexes also have potential Differences in metabolism between the sexes also have potential
effects on TBI brain sequelae and interactions with effects on TBI brain sequelae and interactions with pharmacological treatment. For example, there is a striking pharmacological treatment. For example, there is a striking gender-related difference reported in a study of the gender-related difference reported in a study of the pharmacokinetics of tirilazad, a neuroprotective agent recently pharmacokinetics of tirilazad, a neuroprotective agent recently investigated for prevention of ischemia-related neuronal damage investigated for prevention of ischemia-related neuronal damage after TBI.after TBI.
Tirilazad clearance was approximately 40% higher in young Tirilazad clearance was approximately 40% higher in young women than in young men. Therefore, if the agent did have a women than in young men. Therefore, if the agent did have a beneficial effect overall, due to increased metabolism in women beneficial effect overall, due to increased metabolism in women there may not have been a sufficient amount of the drug to have there may not have been a sufficient amount of the drug to have an effect. an effect.
Evidence for sex-related differences in brain metabolism can also Evidence for sex-related differences in brain metabolism can also be seen in a recent study of alpha 2--receptor by using positron be seen in a recent study of alpha 2--receptor by using positron emission tomography.[40] The authors found that global increases emission tomography.[40] The authors found that global increases in metabolism in response to norepinephrine treatment were in metabolism in response to norepinephrine treatment were revealed in women whereas none were demonstrated in men. revealed in women whereas none were demonstrated in men.
Importance of the Problem: Importance of the Problem: Clinical and ResearchClinical and Research
Either most TBI research has been performed only in men or the data have Either most TBI research has been performed only in men or the data have not been analyzed or reported separately by sex, clinicians have very little not been analyzed or reported separately by sex, clinicians have very little data to guide the management of women who sustain a TBI. The incidence data to guide the management of women who sustain a TBI. The incidence of TBI in women may be increasing, as women participate in more sports of TBI in women may be increasing, as women participate in more sports and other TBI-risky behaviors. Thus, a public health dilemma is potentially and other TBI-risky behaviors. Thus, a public health dilemma is potentially developing, in which practitioners may be faced with increasing numbers developing, in which practitioners may be faced with increasing numbers of women with TBI but will have scarce data to guide treatment. Endocrine of women with TBI but will have scarce data to guide treatment. Endocrine system and metabolic differences may interact with TBI treatment in ways system and metabolic differences may interact with TBI treatment in ways not understood. There may be a potential gender bias in referral and not understood. There may be a potential gender bias in referral and treatment, which means female TBI survivors may not be treated as treatment, which means female TBI survivors may not be treated as effectively as men. effectively as men.
Traumatic brain injury is a difficult area to study because it is a very Traumatic brain injury is a difficult area to study because it is a very heterogeneous phenomenon. Therefore, a great deal of "noise" will likely heterogeneous phenomenon. Therefore, a great deal of "noise" will likely persist in treatment-focused research. Interactions between TBI treatment persist in treatment-focused research. Interactions between TBI treatment and sex may obscure results, as may have partly been the case with and sex may obscure results, as may have partly been the case with tirilazad. Every reasonable effort should be undertaken to reduce this noise tirilazad. Every reasonable effort should be undertaken to reduce this noise so as to obtain a clearer picture of the true treatment effects and recovery so as to obtain a clearer picture of the true treatment effects and recovery mechanisms. Gender is one source of this noise that can be easily mechanisms. Gender is one source of this noise that can be easily identified and reported, which has been shown to have measurable effects. identified and reported, which has been shown to have measurable effects. In TBI studies, data should be reported separately by sex, and adjusted In TBI studies, data should be reported separately by sex, and adjusted analyses should be performed analyses should be performed

Importance of the Problem: Importance of the Problem: Clinical and ResearchClinical and Research
In only a small percentage of the total published literature on TBI In only a small percentage of the total published literature on TBI outcome are results separated by sex, but a quantitative review of outcome are results separated by sex, but a quantitative review of those studies reveals that worse outcomes are demonstrated in those studies reveals that worse outcomes are demonstrated in women after TBI overall. This sex difference may have women after TBI overall. This sex difference may have implications for TBI prevention and rehabilitation efforts. Further implications for TBI prevention and rehabilitation efforts. Further examination is clearly needed. examination is clearly needed.
If a sex-related difference in TBI outcome is found to be stable, If a sex-related difference in TBI outcome is found to be stable, future studies should endeavor to answer whether the difference future studies should endeavor to answer whether the difference in outcome stems from differences in mechanism (of the accident in outcome stems from differences in mechanism (of the accident or in the brain), from treatment variables, or from premorbid or in the brain), from treatment variables, or from premorbid gender differences. It is clear that a careful, prospective study of gender differences. It is clear that a careful, prospective study of the natural history of TBI mechanisms and sequelae is needed to the natural history of TBI mechanisms and sequelae is needed to determine the relation of gender differences to TBI outcome. determine the relation of gender differences to TBI outcome. Traumatic brain injury outcome data should be reported Traumatic brain injury outcome data should be reported separately by sex, and adjusted outcomes analyses should be separately by sex, and adjusted outcomes analyses should be conducted with gender as a covariate. The potentially worse conducted with gender as a covariate. The potentially worse outcomes in women after TBI should increase awareness of the outcomes in women after TBI should increase awareness of the fact that women not only do sustain TBI but may potentially be fact that women not only do sustain TBI but may potentially be more seriously affected than previously thought. more seriously affected than previously thought.

Source of DataSource of Data
http://www.medscape.com/viewarticle/405568_1http://www.medscape.com/viewarticle/405568_1Neurosurg Focus 8(1), 2000. © 2000 American Association of Do Neurosurg Focus 8(1), 2000. © 2000 American Association of Do Neurological Surgeons Do Women Fare Worse? A Metaanalysis of Gender Neurological Surgeons Do Women Fare Worse? A Metaanalysis of Gender Differences in Outcome After Traumatic Brain InjuryDifferences in Outcome After Traumatic Brain Injuryfrom from Neurosurgical FocusNeurosurgical Focus Elana Farace, Ph.D., Wayne M. Alves, Ph.D., Elana Farace, Ph.D., Wayne M. Alves, Ph.D., Department of Neurosurgery, University of Virginia; and INC Research, Department of Neurosurgery, University of Virginia; and INC Research, Charlottesville, VirginiaCharlottesville, Virginia
Manuscript received November 23, 1999. Manuscript received November 23, 1999. Accepted in final form December 22, 1999. Accepted in final form December 22, 1999. Abbreviations used in this paper:Abbreviations used in this paper: IQ = intelligence quotient, SS = sums IQ = intelligence quotient, SS = sums
of squares, TBI = traumatic brain injury of squares, TBI = traumatic brain injury Reprint:Reprint:
Address reprint requests to: Elana Farace, Ph.D.Address reprint requests to: Elana Farace, Ph.D., Department of , Department of Neurosurgery, University of Virginia, Charlottesville, Virginia 22908. email: Neurosurgery, University of Virginia, Charlottesville, Virginia 22908. email: [email protected]@virginia.edu

Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
Brain injury in battered women. Brain injury in battered women. Valera, Eve M.; Berenbaum, Howard; Valera, Eve M.; Berenbaum, Howard; Journal of Consulting and Clinical Psychology. 2003 Aug Vol 71(4) 797-804Journal of Consulting and Clinical Psychology. 2003 Aug Vol 71(4) 797-804 (PsycINFO Database Record (c) 2007 APA, all rights reserved)(PsycINFO Database Record (c) 2007 APA, all rights reserved) Digital Object Identifier: Digital Object Identifier: 10.1037/0022-006X.71.4.797 10.1037/0022-006X.71.4.797
Purpose of the study was to examine Purpose of the study was to examine
(a)(a) whether battered women in a sample of both shelter and non-shelter whether battered women in a sample of both shelter and non-shelter women are sustaining brain injuries from their partners, andwomen are sustaining brain injuries from their partners, and
(b)(b) if so, whether such brain injuries are associated with partner abuse if so, whether such brain injuries are associated with partner abuse severity, cognitive functioning, or psychopathology. Ninety nine battered severity, cognitive functioning, or psychopathology. Ninety nine battered women were assessed using neuropsychological, psychopathology, and women were assessed using neuropsychological, psychopathology, and abuse history measures. abuse history measures.
Almost three quarters of the sample sustained at least 1 partner-related Almost three quarters of the sample sustained at least 1 partner-related brain injury and half sustained multiple partner-related brain injuries. brain injury and half sustained multiple partner-related brain injuries. Further, in a subset of women (n = 57), brain injury severity was negatively Further, in a subset of women (n = 57), brain injury severity was negatively associated with measures of memory, learning, and cognitive flexibility and associated with measures of memory, learning, and cognitive flexibility and was positively associated with partner abuse severity, general distress, was positively associated with partner abuse severity, general distress, anhedonic depression, worry, anxious arousal, and posttraumatic stress anhedonic depression, worry, anxious arousal, and posttraumatic stress disorder symptoms. disorder symptoms.
Enhancing Independence in Women Experiencing Domestic ViolenceEnhancing Independence in Women Experiencing Domestic Violenceand Possible Brain Injury: An Assessment of an Occupational Therapy Intervention Page Range: 49 - 79DOI: 10.1300/J004v20n01_03 and Possible Brain Injury: An Assessment of an Occupational Therapy Intervention Page Range: 49 - 79DOI: 10.1300/J004v20n01_03 Copyright Year: 2004: Guttman, Diamond, Holness, Throgs,Brandofino, Pocheca, Eduardo, CharlesCopyright Year: 2004: Guttman, Diamond, Holness, Throgs,Brandofino, Pocheca, Eduardo, Charles
Women experiencing domestic violence and/or homelessness may have undiagnosed brain damage Women experiencing domestic violence and/or homelessness may have undiagnosed brain damage as a result of abuse over time. Traditionally, women experiencing domestic violence have been as a result of abuse over time. Traditionally, women experiencing domestic violence have been diagnosed and treated within a psychiatric paradigm in which the women's personality deficits were diagnosed and treated within a psychiatric paradigm in which the women's personality deficits were thought to contribute to repeated patterns of abuse. (and may also have gotten them cut off thought to contribute to repeated patterns of abuse. (and may also have gotten them cut off insurance benefits)insurance benefits)
This paradigm is increasingly challenged as researchers find that brain damage frequently occurs in This paradigm is increasingly challenged as researchers find that brain damage frequently occurs in women experiencing domestic violence. Such cognitive impairment may prevent women from using women experiencing domestic violence. Such cognitive impairment may prevent women from using higher executive skills to follow the many steps needed to leave the abusive environment: make an higher executive skills to follow the many steps needed to leave the abusive environment: make an exit plan (my addition), a safety plan (my addition), obtain a residence (my addition), obtain exit plan (my addition), a safety plan (my addition), obtain a residence (my addition), obtain employment needed for economic independence or relevant income supports (my addition), and employment needed for economic independence or relevant income supports (my addition), and live independently in the community. There may be physical accessibility and transportation issues live independently in the community. There may be physical accessibility and transportation issues to overcome that require negotiations and following rules of multiple agencies with some of the to overcome that require negotiations and following rules of multiple agencies with some of the rules conflicting (my addition).rules conflicting (my addition).
The study is an assessment of an intervention designed to address the cognitive deficits that may The study is an assessment of an intervention designed to address the cognitive deficits that may contribute to a woman's inability to leave the abusive environment. The intervention addressed (a) contribute to a woman's inability to leave the abusive environment. The intervention addressed (a) safety planning, (b) drug and alcohol awareness, (c) safe sex practices, (d) assertiveness and safety planning, (b) drug and alcohol awareness, (c) safe sex practices, (d) assertiveness and advocacy skill training, (e) anger management, (f) stress management, (g) boundary establishment advocacy skill training, (e) anger management, (f) stress management, (g) boundary establishment and limit setting, (h) vocational and educational skill training, (i) money management, (j) housing and limit setting, (h) vocational and educational skill training, (i) money management, (j) housing application, (k) leisure exploration, and (l) hygiene, medication routine, and nutrition.application, (k) leisure exploration, and (l) hygiene, medication routine, and nutrition.
Eighty-one percent of the participants attained scores indicating that they achieved their most Eighty-one percent of the participants attained scores indicating that they achieved their most favorable outcome. Nineteen percent of the participants attained scores indicating that they favorable outcome. Nineteen percent of the participants attained scores indicating that they achieved their expected outcome. All participants achieved their expected outcome or greater. achieved their expected outcome. All participants achieved their expected outcome or greater.
From personal experience in working with an OT, they were a vital part of my health care team in From personal experience in working with an OT, they were a vital part of my health care team in any recovery I have been able to achieveany recovery I have been able to achieve
http://braininjury.org.au/portal/fact-sheets/violence-and-acquired-brain-injury---fact-sheet.htmlhttp://braininjury.org.au/portal/fact-sheets/violence-and-acquired-brain-injury---fact-sheet.html
When we consider these impairments, it is not When we consider these impairments, it is not hard to see why a relationship can change when hard to see why a relationship can change when a partner experiences a brain injury. In fact, it has a partner experiences a brain injury. In fact, it has been noted that “marital separation, divorce and been noted that “marital separation, divorce and family discord are higher among family members family discord are higher among family members of individuals with traumatic brain injury, when of individuals with traumatic brain injury, when compared to the general population”. compared to the general population”.
Personality changes, particularly those tending Personality changes, particularly those tending towards anger and aggressiveness, place the towards anger and aggressiveness, place the greatest pressure on relationships. Another greatest pressure on relationships. Another significant strain on relationships is where the significant strain on relationships is where the brain-injured partner under-estimates or has no brain-injured partner under-estimates or has no insight into the extent of their disability.insight into the extent of their disability.

Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
So, what is it like for a woman who has experienced a brain injury So, what is it like for a woman who has experienced a brain injury and is in a relationship with a man? There can be no one answer and is in a relationship with a man? There can be no one answer to this question. Some women report a loss of self-esteem, to this question. Some women report a loss of self-esteem, confidence and self-identity. They may question their value as a confidence and self-identity. They may question their value as a mother and wife. As time goes on, frustration can build and mother and wife. As time goes on, frustration can build and psychological abuse may be inflicted on the wife and mother by psychological abuse may be inflicted on the wife and mother by family members. family members.
On the other hand, a woman who has sustained a brain injury may On the other hand, a woman who has sustained a brain injury may begin to manifest impulsive outbursts of anger and aggression begin to manifest impulsive outbursts of anger and aggression towards family members. Because of the brain injury, she may towards family members. Because of the brain injury, she may also be unable to perceive the effect this has on her partner and also be unable to perceive the effect this has on her partner and children. Responses to this behavior may evoke similar aggression children. Responses to this behavior may evoke similar aggression in them towards her. in them towards her.
Of course, some women experience tremendous ongoing support Of course, some women experience tremendous ongoing support from their partners, families, caregivers and friends. Let’s take a from their partners, families, caregivers and friends. Let’s take a moment and acknowledge those family members, partners, moment and acknowledge those family members, partners, caregivers and friends who help us fight back.caregivers and friends who help us fight back.

Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
Women with acquired brain injury with transient lifestyles, and Women with acquired brain injury with transient lifestyles, and who habitually use alcohol and other drugs, are perhaps who habitually use alcohol and other drugs, are perhaps particularly vulnerable to abuse by their male partners. Workers in particularly vulnerable to abuse by their male partners. Workers in homeless services report that they have found some of the homeless services report that they have found some of the women to be confused and frightened. women to be confused and frightened.
Their memory is affected to the point that they cannot remember Their memory is affected to the point that they cannot remember where they are and where they should be going next. For some, where they are and where they should be going next. For some, being raped is common. being raped is common.
They may not even remember the rape, but if they do, they may They may not even remember the rape, but if they do, they may be unable to judge that rape and sexual assault are unacceptable. be unable to judge that rape and sexual assault are unacceptable.
OK - as we are looking at violence in the lives of women and girls OK - as we are looking at violence in the lives of women and girls across the lifespan, I want to now focus on the important area of across the lifespan, I want to now focus on the important area of child abuse and acquired brain injury.child abuse and acquired brain injury.
Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
Unfortunately, for many of the children who survive, their brain injuries will Unfortunately, for many of the children who survive, their brain injuries will not have been diagnosed. Two of the reasons for this are that there is not have been diagnosed. Two of the reasons for this are that there is usually little to no external evidence of trauma and parents do not usually little to no external evidence of trauma and parents do not voluntarily report a history of abusing their child. voluntarily report a history of abusing their child.
Up to the age of 5, the incidence of head injury between girls and boys Up to the age of 5, the incidence of head injury between girls and boys from this type of family violence is equal. The problem with non-detection from this type of family violence is equal. The problem with non-detection and non-disclosure of such incidents is that children grow up never and non-disclosure of such incidents is that children grow up never knowing that they have a brain injury, and, of course, never receive the knowing that they have a brain injury, and, of course, never receive the support, understanding and treatment they need. support, understanding and treatment they need.
So, for a proportion of girls in our society, this early introduction to violence So, for a proportion of girls in our society, this early introduction to violence will be part of their life story, and many of them will permanently carry its will be part of their life story, and many of them will permanently carry its effects. Of course, this also holds for boys. effects. Of course, this also holds for boys.
Research has established a substantial link between frontal lobe damage Research has established a substantial link between frontal lobe damage and aggression in males. What the specific link is, is still unclear as frontal and aggression in males. What the specific link is, is still unclear as frontal lobe impairment does not always lead to violence or aggression. However, lobe impairment does not always lead to violence or aggression. However, how old a person is at the time of the injury has been identified as a factor how old a person is at the time of the injury has been identified as a factor in severity of injuryin severity of injury
Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
However, how old a person is at the time of the injury has However, how old a person is at the time of the injury has been identified as a significant factor. been identified as a significant factor.
Young males with chronic brain injury are more likely to Young males with chronic brain injury are more likely to continue to be violent as they grow up and to be more continue to be violent as they grow up and to be more susceptible to alcohol and other drugs, adding to the susceptible to alcohol and other drugs, adding to the likelihood of involvement with the criminal justice system.likelihood of involvement with the criminal justice system.
many of these young males do not know that they have an many of these young males do not know that they have an acquired brain injury as they have never been diagnosed. It acquired brain injury as they have never been diagnosed. It is not too far a leap to suggest that some of these young is not too far a leap to suggest that some of these young males received their initial brain injuries from violence in the males received their initial brain injuries from violence in the home that was never revealed or identified. Indeed, research home that was never revealed or identified. Indeed, research has shown that violent adult male offenders tend to have has shown that violent adult male offenders tend to have neuropsychological indicators of brain damage and have had neuropsychological indicators of brain damage and have had histories of severe head trauma. histories of severe head trauma.

Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
There is a correlation between acquired brain There is a correlation between acquired brain injury and men who batter their partners. injury and men who batter their partners. However, it is unclear whether a brain injury has However, it is unclear whether a brain injury has a unique role in domestic violence or whether it is a unique role in domestic violence or whether it is one of several factors, including an anti-social one of several factors, including an anti-social personality. personality.
Research has suggested though, that men with Research has suggested though, that men with acquired brain injury “are at risk of subsequently acquired brain injury “are at risk of subsequently becoming aggressive in their relationships with becoming aggressive in their relationships with women”. women”.
My comment is that it also begs the same My comment is that it also begs the same question in discussing female partner aggressionquestion in discussing female partner aggression
Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
A woman who has suffered a brain injury may not have the A woman who has suffered a brain injury may not have the ability to make an informed, consistent choice of whether to ability to make an informed, consistent choice of whether to leave or return to her abusive partner leave or return to her abusive partner
She may have a lessened ability to plan for her and her She may have a lessened ability to plan for her and her children’s safety children’s safety
She may be unable to abide by the refuge’s rules She may be unable to abide by the refuge’s rules
Her ability to take steps to obtain training or employment Her ability to take steps to obtain training or employment may be compromised may be compromised
She may also receive inappropriate referrals from well-She may also receive inappropriate referrals from well-meaningmeaning refuge workers which may actually compound her refuge workers which may actually compound her problems. problems.

Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
important to realize that subtle brain injury can be harder important to realize that subtle brain injury can be harder to assess immediately after a violent incident because the to assess immediately after a violent incident because the symptoms may appear weeks or months later. A particular symptoms may appear weeks or months later. A particular difficulty for women who habitually use alcohol and other difficulty for women who habitually use alcohol and other drugs is that their brain injuries may remain undiagnosed drugs is that their brain injuries may remain undiagnosed as certain behaviors are often assumed to be related to as certain behaviors are often assumed to be related to substance use.substance use.
This is all the more reason to ensure that workers in This is all the more reason to ensure that workers in
relevant areas receive sufficient training in acquired brain relevant areas receive sufficient training in acquired brain injury. To date it would seem that any major discussion injury. To date it would seem that any major discussion about women with disability and their access to women’s about women with disability and their access to women’s refuges has been about ensuring physical access. Now, for refuges has been about ensuring physical access. Now, for obvious reasons, this needs to extend to women with obvious reasons, this needs to extend to women with acquired brain injury. acquired brain injury.
Brain Injury and Abuse In Brain Injury and Abuse In WomenWomen
This article has been adapted with permission from a paper called This article has been adapted with permission from a paper called at the Partnerships Against Domestic Violence Forum at the at the Partnerships Against Domestic Violence Forum at the Sheraton Hotel, Perth in December 2001 by Fay Rice, Executive Sheraton Hotel, Perth in December 2001 by Fay Rice, Executive Director of Brain Injury Australia. Director of Brain Injury Australia.
Important to realize that subtle brain injury can be harder to Important to realize that subtle brain injury can be harder to assess immediately after a violent incident because the symptoms assess immediately after a violent incident because the symptoms may appear weeks or months later. A particular difficulty for may appear weeks or months later. A particular difficulty for women who habitually use alcohol and other drugs is that their women who habitually use alcohol and other drugs is that their brain injuries may remain undiagnosed as certain behaviors are brain injuries may remain undiagnosed as certain behaviors are often assumed to be related to substance use. often assumed to be related to substance use.
This is all the more reason to ensure that workers in relevant This is all the more reason to ensure that workers in relevant areas receive sufficient training in acquired brain injury. To date it areas receive sufficient training in acquired brain injury. To date it would seem that any major discussion about women with disability would seem that any major discussion about women with disability and their access to women’s refuges has been about ensuring and their access to women’s refuges has been about ensuring physical access. Now, for obvious reasons, this needs to extend to physical access. Now, for obvious reasons, this needs to extend to women with acquired brain injury. women with acquired brain injury.
This article has been adapted from a paper called at the This article has been adapted from a paper called at the Partnerships Against Domestic Violence Forum at the Sheraton Partnerships Against Domestic Violence Forum at the Sheraton Hotel, Perth in December 2001 by Fay Rice, Executive Hotel, Perth in December 2001 by Fay Rice, Executive

Traumatic Brain Injury in Prisons and Jails:Traumatic Brain Injury in Prisons and Jails:
An Unrecognized ProblemAn Unrecognized Problem Many people in prisons and jails are living with traumatic brain injury (TBI)-Many people in prisons and jails are living with traumatic brain injury (TBI)-
related problems that complicate their management and treatment while related problems that complicate their management and treatment while they are incarcerated. Because most prisoners will be released, these they are incarcerated. Because most prisoners will be released, these problems will also pose challenges when they return to the community. The problems will also pose challenges when they return to the community. The Centers for Disease Control and Prevention (CDC) recognizes TBI in prisons Centers for Disease Control and Prevention (CDC) recognizes TBI in prisons and jails as an important public health problem.and jails as an important public health problem.
What is known about TBI and related problems in prisons and jails?What is known about TBI and related problems in prisons and jails?
General:General:
More than two million people currently reside in U.S. prisons and jails.More than two million people currently reside in U.S. prisons and jails.
According to jail and prison studies, 25-87% of inmates report having According to jail and prison studies, 25-87% of inmates report having experienced a head injury or TBI 2-4 as compared to 8.5% in a general experienced a head injury or TBI 2-4 as compared to 8.5% in a general population reporting a history of TBI.5population reporting a history of TBI.5
Prisoners who have had head injuries may also experience mental health Prisoners who have had head injuries may also experience mental health problems such as severe depression and anxiety,3 substance use problems such as severe depression and anxiety,3 substance use disorders,6-8 difficulty controlling anger, or suicidal thoughts and/or disorders,6-8 difficulty controlling anger, or suicidal thoughts and/or attempts.attempts.

Incarcerated WomenIncarcerated Women: : Although women are outnumbered by men in U.S. prisons Although women are outnumbered by men in U.S. prisons
and jails, their numbers more than doubled from 1990 to and jails, their numbers more than doubled from 1990 to 2000.1,10 As of June 2005, more than 200,000 women were 2000.1,10 As of June 2005, more than 200,000 women were incarcerated.1 Women now represent 7% of the total U.S. incarcerated.1 Women now represent 7% of the total U.S. prison population and 12% of the total U.S. jail population.prison population and 12% of the total U.S. jail population.
Women inmates who are convicted of a violent crime are Women inmates who are convicted of a violent crime are more likely to have sustained a pre-crime TBI and/or some more likely to have sustained a pre-crime TBI and/or some other form of physical abuse.11men with substance use other form of physical abuse.11men with substance use disorders have an increased risk for TBI compared with disorders have an increased risk for TBI compared with other women in the general U.S. population.other women in the general U.S. population.
Preliminary results from one studyPreliminary results from one study suggest that TBI among suggest that TBI among women in prison is very common.women in prison is very common.
Substance abuse, violence, and Substance abuse, violence, and homelessnesshomelessness::
Studies of prisoners’ self-reported health indicate that those with Studies of prisoners’ self-reported health indicate that those with one or more head injuries have significantly higher levels of alcohol one or more head injuries have significantly higher levels of alcohol and/or drug use during the year preceding their current and/or drug use during the year preceding their current incarceration.incarceration.
The U.S. Department of Justice has reported that 52% of female The U.S. Department of Justice has reported that 52% of female
offenders and 41% of male offenders are under the influence of offenders and 41% of male offenders are under the influence of drugs, alcohol, or both at the time of their arrest,14 and that 64% of drugs, alcohol, or both at the time of their arrest,14 and that 64% of male arrestees tested positive for at least one of five illicit drugs male arrestees tested positive for at least one of five illicit drugs [cocaine, opioids, marijuana, methamphetamines, or PCP]. [cocaine, opioids, marijuana, methamphetamines, or PCP].
Among male prisoners, a history of TBI is strongly associated with Among male prisoners, a history of TBI is strongly associated with perpetration of domestic and other kinds of violence.perpetration of domestic and other kinds of violence.
Children and teenagers who have been convicted of a crime are Children and teenagers who have been convicted of a crime are more likely to have had a pre-crime and/or some other kind of more likely to have had a pre-crime and/or some other kind of physical abuse.physical abuse.
Homelessness has been found to be related to both head injury and Homelessness has been found to be related to both head injury and
prior imprisonment. prior imprisonment.
How do TBI-related problems affect prisoners with TBI How do TBI-related problems affect prisoners with TBI and others during their incarcerationand others during their incarceration??
Attention deficits may make it difficult for the prisoner with TBI to Attention deficits may make it difficult for the prisoner with TBI to focus on a required task or respond to directions given by a focus on a required task or respond to directions given by a correctional officer. Either situation may be misinterpreted, thus correctional officer. Either situation may be misinterpreted, thus leading to an impression of deliberate defiance on the part of the leading to an impression of deliberate defiance on the part of the prisoner. prisoner.
Memory deficits can make it difficult to understand or remember Memory deficits can make it difficult to understand or remember rules or directions, which can lead to disciplinary actions by jail or rules or directions, which can lead to disciplinary actions by jail or prison staff.prison staff.
Irritability or anger might be difficult to control and can lead to an Irritability or anger might be difficult to control and can lead to an incident with another prisoner or correctional officer and to further incident with another prisoner or correctional officer and to further injury for the person and others.injury for the person and others.
Slowed verbal and physical responses may be interpreted by Slowed verbal and physical responses may be interpreted by correctional officers as uncooperative behavior.correctional officers as uncooperative behavior.
Uninhibited or impulsive behavior, including problems controlling Uninhibited or impulsive behavior, including problems controlling anger6 andanger6 and unacceptable sexual behavior, may provoke other unacceptable sexual behavior, may provoke other prisoners or result in disciplinary action by jail or prison staff.prisoners or result in disciplinary action by jail or prison staff.
What is needed to address the problem of TBI ?What is needed to address the problem of TBI ? A recent report from the Commission on Safety and Abuse in A recent report from the Commission on Safety and Abuse in
America’s Prisons recommends increased health screenings, America’s Prisons recommends increased health screenings, evaluations, and treatment for inmates.evaluations, and treatment for inmates.
In addition, TBI experts and some prison officials have suggested:In addition, TBI experts and some prison officials have suggested:
Routine screening of jail and prison inmates to identify a history ofRoutine screening of jail and prison inmates to identify a history ofTBI.TBI.
Screening inmates with TBI for possible alcohol and/or substance Screening inmates with TBI for possible alcohol and/or substance abuse and appropriate treatment for these co-occurring abuse and appropriate treatment for these co-occurring conditions. conditions.
Additional evaluations to identify specific TBI-related problems and Additional evaluations to identify specific TBI-related problems and determine how they should be managed. Special attentiondetermine how they should be managed. Special attention should should be given to impulsive behavior, including violence, sexual be given to impulsive behavior, including violence, sexual behavior and suicide risk if the inmate is depressed. behavior and suicide risk if the inmate is depressed.

What is needed to address TBI-related problems after release What is needed to address TBI-related problems after release from jails and prisons?from jails and prisons?
Lack of treatment and rehabilitation for persons with mental health and Lack of treatment and rehabilitation for persons with mental health and substance abuse problems while incarcerated increases the probability that substance abuse problems while incarcerated increases the probability that they will again abuse alcohol and/or drugs when released.they will again abuse alcohol and/or drugs when released.
Persistent substance problems can lead to homelessness, return to illegal Persistent substance problems can lead to homelessness, return to illegal drug activities, re-arrest, and increased risk of death after release. As a result, drug activities, re-arrest, and increased risk of death after release. As a result, criminal justice professionals and TBI experts have suggested the following:criminal justice professionals and TBI experts have suggested the following:
- Community re-entry staff should be trained to identify a history of TBI and have- Community re-entry staff should be trained to identify a history of TBI and haveaccess to appropriate consultation with other professionals with expertise in TBI. access to appropriate consultation with other professionals with expertise in TBI.
- Transition services for released persons returning to communities should - Transition services for released persons returning to communities should accommodate the problems resulting from a TBI. accommodate the problems resulting from a TBI.
- Released persons with mental health and/or substance abuse problems should- Released persons with mental health and/or substance abuse problems shouldreceive case management services and assistance with placement into receive case management services and assistance with placement into
communitycommunitytreatment programs.treatment programs.
-CDC supports new research to develop better methods for identifying inmates -CDC supports new research to develop better methods for identifying inmates withwith
a history of TBI and related problems and for determining how many of them are a history of TBI and related problems and for determining how many of them are livingliving with TBIwith TBI

Further information is available from these Further information is available from these websites:websites:
Traumatic Brain Injury (TBI):Traumatic Brain Injury (TBI):CDC, National Center for Injury Prevention and Control CDC, National Center for Injury Prevention and Control www.cdc.gov/ncipc/tbi/TBI.htmwww.cdc.gov/ncipc/tbi/TBI.htm This site provides information for professionals and the general This site provides information for professionals and the general public regarding TBI. Topics include prevention, causes, outcomes, and research. Data reports public regarding TBI. Topics include prevention, causes, outcomes, and research. Data reports regarding TBI in the United States and many free publications and fact sheets can be downloaded. regarding TBI in the United States and many free publications and fact sheets can be downloaded. Materials are available in English and Spanish. Materials are available in English and Spanish.
Health Issues in Correctional Settings: Health Issues in Correctional Settings: CDC, National Center for HIV, STD, and TB Prevention CDC, National Center for HIV, STD, and TB Prevention www.cdc.gov/nchstp/od/cccwg/default.htmwww.cdc.gov/nchstp/od/cccwg/default.htm This site provides information for public health and This site provides information for public health and criminal justice professionals about health topics with an emphasis on infectious diseases in the criminal justice professionals about health topics with an emphasis on infectious diseases in the correctional setting. It also has materials for the general public with links to related organizations. correctional setting. It also has materials for the general public with links to related organizations.
Intimate Partner Violence (IPV):Intimate Partner Violence (IPV):CDC, National Center for Injury Prevention and Control CDC, National Center for Injury Prevention and Control www.cdc.gov/ncipc/factsheets/ipvfacts.htmwww.cdc.gov/ncipc/factsheets/ipvfacts.htm The site provides information for professionals and the The site provides information for professionals and the general public regarding IPV. The site contains an overview and fact sheet about IPV, prevention general public regarding IPV. The site contains an overview and fact sheet about IPV, prevention strategies, links to other IPV prevention organizations, and a list of current CDC publications. strategies, links to other IPV prevention organizations, and a list of current CDC publications.
Legal Issues of Persons with TBI within Correctional Settings: Legal Issues of Persons with TBI within Correctional Settings: National Disability Rights National Disability Rights Network Network www.ndrn.org/aboutus/consumer.htmwww.ndrn.org/aboutus/consumer.htm This site provides information about the laws This site provides information about the laws protecting the civil and human rights of persons with disabilities, including TBI. Incarcerated persons protecting the civil and human rights of persons with disabilities, including TBI. Incarcerated persons with disabilities, or their families, can receive help from the Network regarding prisoners’ legal with disabilities, or their families, can receive help from the Network regarding prisoners’ legal rights, access to mental health services and/or medication, and restoration of benefits upon release. rights, access to mental health services and/or medication, and restoration of benefits upon release.
Substance Abuse: SubstanceSubstance Abuse: Substance Abuse & Mental Health Services Administration Abuse & Mental Health Services Administration www.samhsa.govwww.samhsa.gov This site provides information about treatment resources for persons with, or at This site provides information about treatment resources for persons with, or at
risk for, mental and/or substance abuse problems. Also, the site provides information for risk for, mental and/or substance abuse problems. Also, the site provides information for professionals regarding alcohol and other drug-related disorders. The site has materials for specific professionals regarding alcohol and other drug-related disorders. The site has materials for specific populations and age groups and hotline numbers for support organizations.populations and age groups and hotline numbers for support organizations.
Substance UseSubstance Use Although there is general agreement that chronic ingestion of alcohol poses great risks for normal Although there is general agreement that chronic ingestion of alcohol poses great risks for normal
cardiovascular functions and peripheral-vascular homeostasis, a direct cause and effect between the cardiovascular functions and peripheral-vascular homeostasis, a direct cause and effect between the real phenomena of alcohol-induced headache and risk of brain injury and stroke is not appreciated. real phenomena of alcohol-induced headache and risk of brain injury and stroke is not appreciated.
Binge drinking of alcohol is associated with an ever-growing number of strokes and sudden death. It is Binge drinking of alcohol is associated with an ever-growing number of strokes and sudden death. It is becoming clear that alcohol ingestion can result in profoundly different actions on the cerebral becoming clear that alcohol ingestion can result in profoundly different actions on the cerebral circulation alcohol ingestion can result in profoundly different actions on the cerebral circulation circulation alcohol ingestion can result in profoundly different actions on the cerebral circulation (e.g., vasodilatation, vasoconstriction-spasm, vessel rupture), depending upon dose and physiologic (e.g., vasodilatation, vasoconstriction-spasm, vessel rupture), depending upon dose and physiologic state of host.state of host.
Such animals became susceptible to stroke from nonlethal doses of ethanol. Human subjects with Such animals became susceptible to stroke from nonlethal doses of ethanol. Human subjects with mild head injury have been found to exhibit early deficits in serum ionized Mg (IMg2+); the greater mild head injury have been found to exhibit early deficits in serum ionized Mg (IMg2+); the greater the degree of early head injury (30 min-8 h), the greater and more profound the deficit in serum the degree of early head injury (30 min-8 h), the greater and more profound the deficit in serum IMg2+ and the greater the ionized Ca (ICa2+) to IMg2+ ratio. survivors with histories of alcohol abuse IMg2+ and the greater the ionized Ca (ICa2+) to IMg2+ ratio. survivors with histories of alcohol abuse or ingestion of alcohol prior to head injury exhibited greater deficits in IMg2+ (and higher or ingestion of alcohol prior to head injury exhibited greater deficits in IMg2+ (and higher ICa2+/IMg2+ ratios) and, unlike the subjects without alcohol, did not leave the hospital for at least ICa2+/IMg2+ ratios) and, unlike the subjects without alcohol, did not leave the hospital for at least several days. several days.
Women, for some unknown reason, exhibit a much higher incidence of morbidity and mortality from Women, for some unknown reason, exhibit a much higher incidence of morbidity and mortality from subarachnoid hemorrhage (SAH) than men. Data on 105 men and women with different types of subarachnoid hemorrhage (SAH) than men. Data on 105 men and women with different types of stroke indicate that, on the average, a 20% deficit in serum IMg2+ is seen; total Mg (TMg) or blood pH stroke indicate that, on the average, a 20% deficit in serum IMg2+ is seen; total Mg (TMg) or blood pH is usually near normal. is usually near normal.
Women with SAH, however, exhibit much lower IMg2+ and higher ICa2+/IMg2+ ratios; the presence Women with SAH, however, exhibit much lower IMg2+ and higher ICa2+/IMg2+ ratios; the presence of ethanol in the blood is associated with even more depression in IMg2+ in SAH in women. It is of ethanol in the blood is associated with even more depression in IMg2+ in SAH in women. It is possible that prior alcohol ingestion is, in large measure, responsible for a great deal of this possible that prior alcohol ingestion is, in large measure, responsible for a great deal of this unexplained higher incidence of SAH in women. It has recently been reported that the cyclical unexplained higher incidence of SAH in women. It has recently been reported that the cyclical changes in estrogenic hormones appear to control the serum IMg2+ level in young women. A surge in changes in estrogenic hormones appear to control the serum IMg2+ level in young women. A surge in estrogenic levels prior to SAH could thus precipitate, in part, the SAH.estrogenic levels prior to SAH could thus precipitate, in part, the SAH.
www.http://cat.inist.fr/?aModele=afficheN&cpsidt=1192809www.http://cat.inist.fr/?aModele=afficheN&cpsidt=1192809
Substance UseSubstance Use
Avoid alcohol & other drugs if possible Avoid alcohol & other drugs if possible
Alcohol and other drugs Affect the central Alcohol and other drugs Affect the central nervous system and in varying degrees, impair a nervous system and in varying degrees, impair a person’s ability to think clearly and control person’s ability to think clearly and control emotions and behavior. These abilities are often emotions and behavior. These abilities are often impaired by an acquired brain injury and impaired by an acquired brain injury and therefore when people use drugs and alcohol they therefore when people use drugs and alcohol they are likely to experience even greater problems are likely to experience even greater problems with alertness, memory, problem-solving and with alertness, memory, problem-solving and controlling their behavior and emotions. controlling their behavior and emotions.
War & TBIWar & TBI They find that even when there are no outward signs of injury from the blast, cells deep within the brain They find that even when there are no outward signs of injury from the blast, cells deep within the brain
can be altered, their metabolism changed, causing them to die, says Geoff Ling, an advance-research can be altered, their metabolism changed, causing them to die, says Geoff Ling, an advance-research scientist with the Pentagon.scientist with the Pentagon.
They find that even when there are no outward signs of injury from the blast, cells deep within the brain They find that even when there are no outward signs of injury from the blast, cells deep within the brain can be altered, their metabolism changed, causing them to die, says Geoff Ling, an advance-research can be altered, their metabolism changed, causing them to die, says Geoff Ling, an advance-research scientist with the Pentagon. scientist with the Pentagon.
The newly discovered brain damage at the cellular level can be permanent — especially after repeated The newly discovered brain damage at the cellular level can be permanent — especially after repeated exposures to blasts — and lead to lasting neurological deterioration, Ling and Cernak sayexposures to blasts — and lead to lasting neurological deterioration, Ling and Cernak say
When the war in Iraq began, clinicians treating the wounded began noticing similar symptoms. Some When the war in Iraq began, clinicians treating the wounded began noticing similar symptoms. Some screenings at military bases showed that 10% to 20% of returning troops may have suffered such head screenings at military bases showed that 10% to 20% of returning troops may have suffered such head wounds. wounds.
Substance Use To make matters worse, whatever damage occurred was so microscopic that it could not Substance Use To make matters worse, whatever damage occurred was so microscopic that it could not be found with imaging tests. be found with imaging tests.
Roadside bombs, also called improvised explosive devices (IEDs), are the cause of most cases of brain Roadside bombs, also called improvised explosive devices (IEDs), are the cause of most cases of brain injury and account for almost 80% of all wounds to U.S. troops. Many troops caught near these injury and account for almost 80% of all wounds to U.S. troops. Many troops caught near these explosions can suffer symptoms such as perforated eardrums, ringing in the ears, blurred vision, explosions can suffer symptoms such as perforated eardrums, ringing in the ears, blurred vision, memory lapses and headachesmemory lapses and headaches
Soldiers often shake off the effects and return to combat.Soldiers often shake off the effects and return to combat.
Iraq and Afghanistan veterans treated by the Department of Veterans Affairs say they have been Iraq and Afghanistan veterans treated by the Department of Veterans Affairs say they have been exposed to anywhere from six to 25 bomb blasts during their combat experiences, says Barbara exposed to anywhere from six to 25 bomb blasts during their combat experiences, says Barbara Sigford, VA director of physical medicine. Ling and other scientists say repeated blast exposure can Sigford, VA director of physical medicine. Ling and other scientists say repeated blast exposure can aggravate any brain damageaggravate any brain damage
"That would be very, very difficult to do. You don't know (how many blast exposures are too many). Half "That would be very, very difficult to do. You don't know (how many blast exposures are too many). Half a dozen? One? I mean, what's the tipping point?“a dozen? One? I mean, what's the tipping point?“
http://www.usatoday.com/news/world/iraq/2007-09-23-traumatic-brain-injuries_N.htmhttp://www.usatoday.com/news/world/iraq/2007-09-23-traumatic-brain-injuries_N.htm

Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary InjuriesInjuries
http://www.sciencedaily.com/releases/2005/07/05http://www.sciencedaily.com/releases/2005/07/050727063759.htm0727063759.htm
June 1, 2008 June 1, 2008 Psychiatric Times. Vol. 25 No. 7 Psychiatric Times. Vol. 25 No. 7
Mood and Anxiety Disorders Following Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Traumatic Brain Injury Differences Between Military and Nonmilitary InjuriesMilitary and Nonmilitary Injuries
Ricardo E. Jorge, MDRicardo E. Jorge, MD
Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
TBI has been described as the "signature wound" TBI has been described as the "signature wound" of Operation Iraqi Freedom and Operation of Operation Iraqi Freedom and Operation Enduring Freedom in Afghanistan. Enduring Freedom in Afghanistan.
Modern body armor has greatly reduced the Modern body armor has greatly reduced the frequency of severe injuries to the thoracic and frequency of severe injuries to the thoracic and abdominal regions. abdominal regions.
Consequently, injuries to the head and the Consequently, injuries to the head and the extremities are the predominant wounds extremities are the predominant wounds encountered in contemporary battlefields. encountered in contemporary battlefields.
The use of Kevlar helmets has significantly The use of Kevlar helmets has significantly reduced the frequency of penetrating head reduced the frequency of penetrating head injuries, making closed head injury (eg, from injuries, making closed head injury (eg, from blasts, motor vehicle accidents, or falls) the most blasts, motor vehicle accidents, or falls) the most frequent form of TBI observed in current military frequent form of TBI observed in current military operations.operations.
Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
According to military records, blast injuries constitute the According to military records, blast injuries constitute the most frequent type of injury observed, accounting for most frequent type of injury observed, accounting for approximately two-thirds of war-zone evacuations.approximately two-thirds of war-zone evacuations.
A recent study reported that 88% of soldiers treated at a A recent study reported that 88% of soldiers treated at a medical unit in Iraq were injured by improvised explosive medical unit in Iraq were injured by improvised explosive devices or mortar fire. devices or mortar fire.
The vast majority of injuries (97%) observed among the The vast majority of injuries (97%) observed among the troops of a Marine unit in Iraq were produced by improvised troops of a Marine unit in Iraq were produced by improvised explosive devices or mines.explosive devices or mines.
In addition, it has been estimated that 59% of soldiers with In addition, it has been estimated that 59% of soldiers with blast injuries have sustained a TBI. As of March 2006, 28% blast injuries have sustained a TBI. As of March 2006, 28% of all injured troops in these conflicts had a TBI, with blast of all injured troops in these conflicts had a TBI, with blast being the cause in most cases (88%).being the cause in most cases (88%).
Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
The troops in Iraq and Afghanistan are different from other military The troops in Iraq and Afghanistan are different from other military groups and from civilian populations at risk for a TBI. groups and from civilian populations at risk for a TBI.
In contrast to other conflicts (eg, the Vietnam War), deployed military In contrast to other conflicts (eg, the Vietnam War), deployed military forces in Iraq are all-volunteer, professional troops. forces in Iraq are all-volunteer, professional troops.
A recent study reported on the demographic characteristics of a large A recent study reported on the demographic characteristics of a large cohort of soldiers in Iraq. About 90% of the troops were men in their cohort of soldiers in Iraq. About 90% of the troops were men in their 20s; 56.4% were white, 16.2% were black, 14.7% were Hispanic 20s; 56.4% were white, 16.2% were black, 14.7% were Hispanic American, 2.6% were Asian American, and 10.1% were other. About American, 2.6% were Asian American, and 10.1% were other. About half (45.4%) were married and most had a high school education half (45.4%) were married and most had a high school education
Overall, military samples were found to have better psychosocial Overall, military samples were found to have better psychosocial adjustment than civilians with a TBI.adjustment than civilians with a TBI.
Within the military cohort, 6% reported past psychiatric disorders, Within the military cohort, 6% reported past psychiatric disorders, and 4.2% reported past alcohol use disorders. The rates for alcohol and 4.2% reported past alcohol use disorders. The rates for alcohol abuse were significantly lower than the ones observed in civilian abuse were significantly lower than the ones observed in civilian samples.samples.

Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
Although psychiatric disturbance will certainly have a negative impact on Although psychiatric disturbance will certainly have a negative impact on the clinical recovery and quality of life of injured veterans, the frequency, the clinical recovery and quality of life of injured veterans, the frequency, phenomenological characteristics, and clinical correlates of mood and phenomenological characteristics, and clinical correlates of mood and anxiety disorders that occur after a TBI have not been thoroughly anxiety disorders that occur after a TBI have not been thoroughly described among veterans returning from Iraq and Afghanistan. described among veterans returning from Iraq and Afghanistan.
Researchers reported on 2 cases of veterans with mild head injuries who, Researchers reported on 2 cases of veterans with mild head injuries who, although they were initially judged fit to return to light duty, experienced although they were initially judged fit to return to light duty, experienced dramatic personality changes 3 to 5 months after the TBI. dramatic personality changes 3 to 5 months after the TBI.
A comprehensive battery of neuropsychological tests and A comprehensive battery of neuropsychological tests and electrophysiological measures revealed significant impairments on tasks electrophysiological measures revealed significant impairments on tasks probing complex attentional functions, speed of information processing, probing complex attentional functions, speed of information processing, and problem-solving ability.and problem-solving ability.
Unfortunately, the impact of mood and anxiety disorders on Unfortunately, the impact of mood and anxiety disorders on neuropsychological performance was not assessed. The investigators neuropsychological performance was not assessed. The investigators concluded that these 2 cases are paradigmatic of a growing number of concluded that these 2 cases are paradigmatic of a growing number of veterans referred to their rehabilitation center.veterans referred to their rehabilitation center.
Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
Previous epidemiological studies suggest that there is a high prevalence of Previous epidemiological studies suggest that there is a high prevalence of mental health disorders among military personnel in Iraq and Afghanistan.mental health disorders among military personnel in Iraq and Afghanistan.
A recent study of 103,788 veterans first seen at the Veterans Affairs Health A recent study of 103,788 veterans first seen at the Veterans Affairs Health Care System (VA) following active duty in Iraq and Afghanistan reported Care System (VA) following active duty in Iraq and Afghanistan reported that about 25% of all veterans received a mental health diagnosis.that about 25% of all veterans received a mental health diagnosis.
The median time from service separation to the first VA clinic visit (mostly The median time from service separation to the first VA clinic visit (mostly in primary care settings) was 2.9 months after separation, and the most in primary care settings) was 2.9 months after separation, and the most frequent diagnoses were PTSD (13%) and mood disorders (11%). frequent diagnoses were PTSD (13%) and mood disorders (11%).
In another recent study, the frequency of mood and anxiety disorders In another recent study, the frequency of mood and anxiety disorders following a mild TBI in 2525 US soldiers returning from Iraq was examined.following a mild TBI in 2525 US soldiers returning from Iraq was examined.
PTSD was strongly associated with the occurrence of a mild TBI. Soldiers PTSD was strongly associated with the occurrence of a mild TBI. Soldiers with a mild TBI were more likely to have poorer medical outcomes. More with a mild TBI were more likely to have poorer medical outcomes. More important, PTSD and depression were most frequently linked to poor important, PTSD and depression were most frequently linked to poor outcomes.outcomes.

Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
It must be noted that assessment of a mild TBI in the It must be noted that assessment of a mild TBI in the context of military operations is difficult for multiple context of military operations is difficult for multiple reasons, including retrospective bias and the fact that reasons, including retrospective bias and the fact that alterations of consciousness (a decisive criterion in the alterations of consciousness (a decisive criterion in the traditional definition of a mild TBI) may be part of an acute traditional definition of a mild TBI) may be part of an acute stress reaction rather than the consequence of a traumatic stress reaction rather than the consequence of a traumatic injury. injury.
This may result not only in an overestimation of the number This may result not only in an overestimation of the number of TBI cases but also in a biased estimate of the strength of of TBI cases but also in a biased estimate of the strength of the association between a TBI and PTSD, given that acute the association between a TBI and PTSD, given that acute stress reactions are a significant predictor of later PTSD. stress reactions are a significant predictor of later PTSD.
However, the stronger relationship of psychiatric illness However, the stronger relationship of psychiatric illness with a history of loss of consciousness suggests that subtle with a history of loss of consciousness suggests that subtle forms of brain damage may contribute to the genesis of forms of brain damage may contribute to the genesis of these disorders. these disorders.

Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
Assessment of the type, location, and extent of these brain alterations Assessment of the type, location, and extent of these brain alterations requires the use of more sensitive neuroimaging techniques such as requires the use of more sensitive neuroimaging techniques such as diffusion tensor imagingdiffusion tensor imaging, functional MRI, or magnetic resonance , functional MRI, or magnetic resonance spectroscopy. spectroscopy.
Cognitive dysfunction is a major contributor to disability following a TBI. Cognitive dysfunction is a major contributor to disability following a TBI.
Neuropsychological changes following active duty in Iraq and Afghanistan Neuropsychological changes following active duty in Iraq and Afghanistan were examined by the Neurocognition Deployment Health Study. were examined by the Neurocognition Deployment Health Study.
The investigators concluded that deployment to Iraq was associated with The investigators concluded that deployment to Iraq was associated with increased risk of neuropsychological deficits.increased risk of neuropsychological deficits.
However, the relationship of these cognitive changes to the presence of However, the relationship of these cognitive changes to the presence of mood and anxiety disorders has not been adequately studied and mood and anxiety disorders has not been adequately studied and constitutes one of the priorities of research in this field. constitutes one of the priorities of research in this field.
Is a TBI a significant risk factor for mental health problems following active Is a TBI a significant risk factor for mental health problems following active duty in Iraq or Afghanistan? Are the phenomenological presentation and duty in Iraq or Afghanistan? Are the phenomenological presentation and clinical course of psychiatric disorders that occur after a TBI different from clinical course of psychiatric disorders that occur after a TBI different from those observed in survivors without brain damage? those observed in survivors without brain damage?

Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
These important clinical questions require more extensive These important clinical questions require more extensive investigation. Furthermore, the physiopathology of blast investigation. Furthermore, the physiopathology of blast injuries, particularly in the case of recurrent exposure to injuries, particularly in the case of recurrent exposure to blasts, has not been fully elucidated and might be blasts, has not been fully elucidated and might be substantially different from the mechanisms described in substantially different from the mechanisms described in other forms of TBI. other forms of TBI.
This pathophysiology may be contributing to differences in This pathophysiology may be contributing to differences in the clinical presentation of these TBI survivors. For the clinical presentation of these TBI survivors. For example, preliminary studies that compare blast versus example, preliminary studies that compare blast versus nonblast closed head injuries among veterans admitted to nonblast closed head injuries among veterans admitted to the Walter Reed Army Medical Center suggest that the Walter Reed Army Medical Center suggest that survivors injured in a blast are more likely than those with a survivors injured in a blast are more likely than those with a nonblast TBI to present with acute stress reaction and nonblast TBI to present with acute stress reaction and PTSD.PTSD.
Mood and Anxiety Disorders Following Traumatic Brain Mood and Anxiety Disorders Following Traumatic Brain Injury Differences Between Military and Nonmilitary Injury Differences Between Military and Nonmilitary
InjuriesInjuries
TBI has been associated with an increased frequency of TBI has been associated with an increased frequency of psychopathological disorders in both civilian and military psychopathological disorders in both civilian and military populations. populations.
Disruption of prefrontal circuits regulating mood and emotional Disruption of prefrontal circuits regulating mood and emotional processing is an important causative factor in the genesis of these processing is an important causative factor in the genesis of these syndromes. syndromes.
In addition, mood and anxiety disorders account for a significant In addition, mood and anxiety disorders account for a significant part of disability resulting from TBI of varying severity.part of disability resulting from TBI of varying severity.
Thus, there is an urgent need to study clinical characteristics, Thus, there is an urgent need to study clinical characteristics,
mechanisms, and treatment alternatives for these conditions. In mechanisms, and treatment alternatives for these conditions. In turn, the information obtained from survivors with brain injuries turn, the information obtained from survivors with brain injuries may provide further insight into the pathophysiology of these may provide further insight into the pathophysiology of these disorders in the population as a whole. In addition, gender analysis disorders in the population as a whole. In addition, gender analysis needs to be an important component of the research.needs to be an important component of the research.

Brain Injury, Gender & Brain Injury, Gender & Age Age
http://www.medicinenet.com/script/main/art.asp?articlekey=9053http://www.medicinenet.com/script/main/art.asp?articlekey=905300
TBIs accounted for 50 percent of all unintentional fall deaths and 8 TBIs accounted for 50 percent of all unintentional fall deaths and 8 percent of nonfatal fall-related hospitalizations among older percent of nonfatal fall-related hospitalizations among older adults.adults.
As people age, their risk of falling increases due to a number of As people age, their risk of falling increases due to a number of factors such as mobility problems due to muscle weakness or poor factors such as mobility problems due to muscle weakness or poor balance, loss of sensation in feet, chronic health problems, vision balance, loss of sensation in feet, chronic health problems, vision changes or loss, medication side effects or drug interactions, and changes or loss, medication side effects or drug interactions, and domestic hazards such as clutter and poor lighting, according to domestic hazards such as clutter and poor lighting, according to background information in the study.background information in the study.
"Most people think older adults may only break their hip when "Most people think older adults may only break their hip when they fall, but our research shows that traumatic brain injuries can they fall, but our research shows that traumatic brain injuries can also be a serious consequence. These injuries can cause long-term also be a serious consequence. These injuries can cause long-term problems and affect how someone thinks or functions. They can problems and affect how someone thinks or functions. They can also impact a person's emotional well-being," Dr. Ileana Arias, also impact a person's emotional well-being," Dr. Ileana Arias, director of the CDC's National Center for Injury Prevention and director of the CDC's National Center for Injury Prevention and Control, said in a prepared statement.Control, said in a prepared statement.
TBIs, caused by a blow or bump to the head, may be missed or TBIs, caused by a blow or bump to the head, may be missed or misdiagnosed among older adults.misdiagnosed among older adults.

Brain Injury, Gender & Brain Injury, Gender & AgeAge
In this study, researchers analyzed data from the National Center for In this study, researchers analyzed data from the National Center for Health Statistics' National Vital Statistics System and the Agency for Health Statistics' National Vital Statistics System and the Agency for Healthcare Research and Quality's Nationwide Inpatient Sample.Healthcare Research and Quality's Nationwide Inpatient Sample.
Among the findings:Among the findings: Men had higher fall-related TBI death rates than women — 26.9 per Men had higher fall-related TBI death rates than women — 26.9 per
100,000 vs. 17.8 per 100,000. 100,000 vs. 17.8 per 100,000. The rate of fall-related TBI hospitalization for men was 146.3 per 100,000, The rate of fall-related TBI hospitalization for men was 146.3 per 100,000,
compared to 158.3 per 100,000 for women. compared to 158.3 per 100,000 for women. Death and hospitalization rates for fall-related TBIs generally increased Death and hospitalization rates for fall-related TBIs generally increased
with age. with age. Most men (54.9 percent) and women (61.5 percent) hospitalized with a fall-Most men (54.9 percent) and women (61.5 percent) hospitalized with a fall-
related TBI spent two to six days in hospital. related TBI spent two to six days in hospital. The median charges for these hospitalizations were $19,191 for men and The median charges for these hospitalizations were $19,191 for men and
$16,006 for women.$16,006 for women. The study was published in the June issue of the The study was published in the June issue of the Journal of Safety Journal of Safety
ResearchResearch.. As more baby boomers reach retirement age, the increasing number of As more baby boomers reach retirement age, the increasing number of
fall-related TBIs will become more of a burden on the health care system fall-related TBIs will become more of a burden on the health care system unless action is taken to prevent such injuries, Arias said.unless action is taken to prevent such injuries, Arias said.
SOURCE: U.S. Centers for Disease Control and Prevention, news release, SOURCE: U.S. Centers for Disease Control and Prevention, news release, June 23, 2008 June 23, 2008
Brain Injury, Gender & Age: Child/YouthBrain Injury, Gender & Age: Child/Youth
http://www.springerlink.com/content/v143u14082xl2556http://www.springerlink.com/content/v143u14082xl2556 Foundations of Sport-Related Brain Injuries10.1007/0-387-Foundations of Sport-Related Brain Injuries10.1007/0-387-
32565-4_13Semyon Slobounov and Wayne Sebastianelli32565-4_13Semyon Slobounov and Wayne Sebastianelli Rimma Danov2 Rimma Danov2 (2) NHL Concussion Program, UPMC (2) NHL Concussion Program, UPMC
Center for Sports Medicine Hospital for Joint Diseases, New Center for Sports Medicine Hospital for Joint Diseases, New York University Medical Center, Adelphi University, Private York University Medical Center, Adelphi University, Private Practice, New York AbstractPractice, New York Abstract
With the rapid development of neuroimaging and With the rapid development of neuroimaging and neuroscience in the past several years, the body of neuroscience in the past several years, the body of research and clinical knowledge about concussion research and clinical knowledge about concussion processes in adults continues to rapidly increase. processes in adults continues to rapidly increase. Nevertheless, many questions involving the functioning of a Nevertheless, many questions involving the functioning of a human brain post-head injury and its recover remain human brain post-head injury and its recover remain unanswered. unanswered.

Brain Injury, Gender & Age: Brain Injury, Gender & Age: Child/YouthChild/Youth
There is even less known about neurodynamics of There is even less known about neurodynamics of concussive processes and recovery in children, concussive processes and recovery in children, whose young brain remains in a state of constant whose young brain remains in a state of constant developmental change. developmental change.
There is enormous amount of variations, which There is enormous amount of variations, which are introduced in to the picture of pediatric are introduced in to the picture of pediatric concussion, that have to do with the child’s brain concussion, that have to do with the child’s brain developmental phase at the time of the injury, its developmental phase at the time of the injury, its capacity for plasticity and adaptation to TBI, and capacity for plasticity and adaptation to TBI, and other factors. This chapter attempts to provide an other factors. This chapter attempts to provide an overview of research and clinical data relevant to overview of research and clinical data relevant to the complex interplay of a child’s developing the complex interplay of a child’s developing brain and the effects of a mild head injury. brain and the effects of a mild head injury.

Brain Injury, Gender & Age: Brain Injury, Gender & Age: Child/YouthChild/Youth
There is a growing body of research suggesting that even mild There is a growing body of research suggesting that even mild head injuries produce significant neurocognitive and head injuries produce significant neurocognitive and neurobehavioral deficits in children and adolescents. As elucidated neurobehavioral deficits in children and adolescents. As elucidated below, there is some uncertainty and controversy in regards to the below, there is some uncertainty and controversy in regards to the definition, sequelae of, and recovery from pediatric concussions. definition, sequelae of, and recovery from pediatric concussions.
The review of literature supports the idea that concussive The review of literature supports the idea that concussive processes produce a unique profile of neurocognitive and processes produce a unique profile of neurocognitive and neurobehavioral deficits that is different for each child, given his neurobehavioral deficits that is different for each child, given his developmental phase at the onset of injury and pre- and post-developmental phase at the onset of injury and pre- and post-injury characteristics. injury characteristics.
The role of a comprehensive neuropsychological examination in The role of a comprehensive neuropsychological examination in detection of these deficits is substantial, as it delineates child’s detection of these deficits is substantial, as it delineates child’s unique profile of strengths and weaknesses that are essential for unique profile of strengths and weaknesses that are essential for effective treatment planning and adequate academic placement. effective treatment planning and adequate academic placement.

Coping skillsCoping skills
USING COMPUTERS FOR REHABILITATION USING COMPUTERS FOR REHABILITATION Individuals, family members and professionals are painfully aware that the most disabling Individuals, family members and professionals are painfully aware that the most disabling
consequences of brain injury are usually Cognitive and behavioural deficits. There are many consequences of brain injury are usually Cognitive and behavioural deficits. There are many rehabilitation facilities using computers in their programmes, as they are cheap, provide repeated trials, rehabilitation facilities using computers in their programmes, as they are cheap, provide repeated trials, help prepare for employment, provide leisure activity and require little supervision. help prepare for employment, provide leisure activity and require little supervision.
There are some issues for the person with a brain injury that need evaluation such as visual acuity and There are some issues for the person with a brain injury that need evaluation such as visual acuity and coordination. There is a range of adaptive hardware such as alternative input devices, decelerator coordination. There is a range of adaptive hardware such as alternative input devices, decelerator cards, voice synthesisers and screen enlargers which can assist. cards, voice synthesisers and screen enlargers which can assist.
Computers can increase self-esteem after an injury. For many it may provide their first opportunity to Computers can increase self-esteem after an injury. For many it may provide their first opportunity to work independently since their injuries. Others feel the computer is not critical of poor performance on work independently since their injuries. Others feel the computer is not critical of poor performance on a task. a task.
Computers cannot help with all deficits following brain injury but they can help develop skills related to Computers cannot help with all deficits following brain injury but they can help develop skills related to the following: the following:
-Attention/concentration -Attention/concentration -Impulsivity -Impulsivity -Distractibility -Distractibility -Learning/memory -Learning/memory -Visual tracking/scanning -Visual tracking/scanning -Planning/organization -Planning/organization -Eye-hand coordination -Eye-hand coordination -Problem solving -Problem solving -Spatial analysis/synthesis -Spatial analysis/synthesis -Cognitive endurance. -Cognitive endurance.

OrganizationOrganization The frontal lobe of the brain is responsible for the act of organising The frontal lobe of the brain is responsible for the act of organising
our lives. Unfortunately it is very susceptible to injury and some our lives. Unfortunately it is very susceptible to injury and some find great difficulty with prioritising, sequencing, organising, find great difficulty with prioritising, sequencing, organising, initiating and completing tasks. initiating and completing tasks.
Improve your Lifestyle Improve your Lifestyle Factors such as anxiety, stress, multiple demands and fatigue can Factors such as anxiety, stress, multiple demands and fatigue can
have serious effects on your ability to organize. Therefore, the have serious effects on your ability to organize. Therefore, the improvement of a person’s emotional and physical well-being will improvement of a person’s emotional and physical well-being will most likely have benefits for their mental alertness and ability to most likely have benefits for their mental alertness and ability to plan and priorities. Important considerations for improving general plan and priorities. Important considerations for improving general well-being include: well-being include:
A balanced diet and appropriate supplements i.e. vitamins A balanced diet and appropriate supplements i.e. vitamins Sufficient restful sleep Sufficient restful sleep Regular exercise Regular exercise Relaxation and stress-reduction strategies Relaxation and stress-reduction strategies Following prescribed medication guidelines and medical advice Following prescribed medication guidelines and medical advice Avoiding alcohol, cigarettes and drugs. Avoiding alcohol, cigarettes and drugs.

StructureStructure Structure allows us to put most of our lives on automatic Structure allows us to put most of our lives on automatic
pilot and reserve creativity, memory, and novelty for more pilot and reserve creativity, memory, and novelty for more important areas. important areas.
After a brain injury many find that they lose this structure After a brain injury many find that they lose this structure to their day, particularly if they are not working. It is crucial to their day, particularly if they are not working. It is crucial to have well defined tasks for the day. to have well defined tasks for the day.
Set a timetable each day that will ensure the healthy Set a timetable each day that will ensure the healthy lifestyle above. For example, sleep can be properly lifestyle above. For example, sleep can be properly regulated by always going to sleep and waking at set times. regulated by always going to sleep and waking at set times. Meal times should be at set times and never skipped. Meal times should be at set times and never skipped.
Work with family members to arrange a weekly plan for Work with family members to arrange a weekly plan for visiting others, exercise and any rehabilitation tasks. visiting others, exercise and any rehabilitation tasks.
Organize your EnvironmentOrganize your Environment
Get a daily planner, diary or electronic organizer and write things Get a daily planner, diary or electronic organizer and write things down in the order you are going to do them. down in the order you are going to do them.
Get into the habit of checking your schedule at the beginning of Get into the habit of checking your schedule at the beginning of every day or the night before. The aim is to arrange surroundings every day or the night before. The aim is to arrange surroundings so that less reliance or demand is placed upon a person’s so that less reliance or demand is placed upon a person’s memory. memory.
Strategies for organizing the environment include the following: Strategies for organizing the environment include the following:
Using a note pad system beside the phone Using a note pad system beside the phone Using a large notice board and making plans Using a large notice board and making plans Having a special place to keep objects which tend to go missing Having a special place to keep objects which tend to go missing Labeling or color-coding cupboards as a reminder of where things Labeling or color-coding cupboards as a reminder of where things
are kept are kept Tying objects to places e.g. a pen to the phone or a key to a belt. Tying objects to places e.g. a pen to the phone or a key to a belt. Place your household address by every phone in the house in case Place your household address by every phone in the house in case
you need to call for help, and in your wallet or handbagyou need to call for help, and in your wallet or handbag
THE IMPORTANCE OF APPROPRIATE THE IMPORTANCE OF APPROPRIATE IDENTIFICATIONIDENTIFICATION
With each step toward independence, it With each step toward independence, it becomes more important to have proper becomes more important to have proper identification at all times. In the event of identification at all times. In the event of seizures, ensure that the individual has seizures, ensure that the individual has information in the form of a bracelet, information in the form of a bracelet, necklace and/or wallet card that accesses necklace and/or wallet card that accesses medical instructions. If the person could medical instructions. If the person could become lost then maps or a record of the become lost then maps or a record of the address should be carried at all times. address should be carried at all times.

LISTS, LISTS, LISTSLISTS, LISTS, LISTS A To-Do List is a handy tool. Get a whiteboard and A To-Do List is a handy tool. Get a whiteboard and
put it up somewhere in your house. Write on it put it up somewhere in your house. Write on it the things that you have to do and then erase the things that you have to do and then erase them as you complete them. them as you complete them.
Sometimes people will list 50 projects and none Sometimes people will list 50 projects and none of them will get done. If you have this problem, of them will get done. If you have this problem, create a list of five projects that you want to do create a list of five projects that you want to do and write them on the whiteboard. Don’t add and write them on the whiteboard. Don’t add another project to the list until you completed another project to the list until you completed one of the five items. one of the five items.
As you add one, you have to subtract one. You As you add one, you have to subtract one. You may want to limit it to only three projects if five is may want to limit it to only three projects if five is overwhelming. overwhelming.
Setting GoalsSetting Goals
We all have goals we have set out to achieve, often at a subconscious We all have goals we have set out to achieve, often at a subconscious level. Goals keep us focused on a purpose and help us through difficult level. Goals keep us focused on a purpose and help us through difficult times when many others less motivated would give up.times when many others less motivated would give up.
A person who wants to get the most out of life often has a number of goals A person who wants to get the most out of life often has a number of goals
simmering at the same time. By setting goals you can get out of negative simmering at the same time. By setting goals you can get out of negative mindsets and help you gain more control over your life. It pays to set these mindsets and help you gain more control over your life. It pays to set these out in writing and approach them step-by-step. out in writing and approach them step-by-step.
If your formal rehabilitation has finished, some goals may be to continue If your formal rehabilitation has finished, some goals may be to continue further work yourself. It is crucial to have an accurate idea of your further work yourself. It is crucial to have an accurate idea of your strengths and weaknesses. strengths and weaknesses.
After sustaining a brain injury, people often have unrealistic ideas here if After sustaining a brain injury, people often have unrealistic ideas here if their self-awareness has been affected, so the involvement of rehabilitation their self-awareness has been affected, so the involvement of rehabilitation professionals or family is a good idea. professionals or family is a good idea.
Goal Setting StepsGoal Setting Steps One way to plan and organize a goal involves designing a goal One way to plan and organize a goal involves designing a goal
schedule which may include some of the following sections: schedule which may include some of the following sections: Goal Goal Task/steps Task/steps Time frame Time frame Aim for completion Aim for completion Potential barriers Potential barriers How to overcome barriers How to overcome barriers Benefits of achieving the goal Benefits of achieving the goal Measures of success. Measures of success. It is important to realize the underlying emotions or needs behind It is important to realize the underlying emotions or needs behind
a goal. For example, you may want to return to work but find your a goal. For example, you may want to return to work but find your Cognitive deficits prevent this. Why do you want to return to Cognitive deficits prevent this. Why do you want to return to work? It may be the sense of being productive, of being part of a work? It may be the sense of being productive, of being part of a team and feeling esteemed by peers. In this case looking at team and feeling esteemed by peers. In this case looking at volunteer work for a community organization may achieve these volunteer work for a community organization may achieve these underlying underlying

GoalsGoals
Achieving goals is a step by step process. It may seem too Achieving goals is a step by step process. It may seem too daunting at first but families can provide support and daunting at first but families can provide support and assistance in a graduated way. The recovery process is assistance in a graduated way. The recovery process is more like a marathon than a sprint. Both you and your more like a marathon than a sprint. Both you and your family need patience, positive attitudes and plenty of loving family need patience, positive attitudes and plenty of loving support for each other. support for each other.
Goals should be adjusted to fit your learning style or Goals should be adjusted to fit your learning style or hobbies. If you hate reading or writing then your goals hobbies. If you hate reading or writing then your goals shouldn’t use written exercises or reading of books. If you shouldn’t use written exercises or reading of books. If you don’t mind writing then keeping a journal is an excellent don’t mind writing then keeping a journal is an excellent way to record your progress, especially when you feel you way to record your progress, especially when you feel you aren’t getting anywhere. A journal can keep track of the aren’t getting anywhere. A journal can keep track of the “three steps forward, two back” that can sometimes feature “three steps forward, two back” that can sometimes feature in recovery. in recovery.

Memory AidsMemory Aids
Memory is an important part of getting organized. Memory is an important part of getting organized. When effectively used to store information, When effectively used to store information, memory aids should enable a person to focus upon memory aids should enable a person to focus upon learning and recalling details for which a strategy learning and recalling details for which a strategy cannot be used. Types of external aids include: cannot be used. Types of external aids include:
A diary for storing and planning A diary for storing and planning Notebooks of all sizes for various places Notebooks of all sizes for various places Lists and checklists Lists and checklists Alarm clock, wristwatch alarm and timer Alarm clock, wristwatch alarm and timer Calendar Calendar Wall chart Wall chart Tape recorder. Tape recorder.
Bringing it all TogetherBringing it all Together
All of these suggestions are compensatory strategies—that is they All of these suggestions are compensatory strategies—that is they compensate for skills that your brain is not as good at any more. compensate for skills that your brain is not as good at any more. The good news is that the right strategies can go a long way to The good news is that the right strategies can go a long way to making up for a sluggish frontal lobe. All it takes is commitment to making up for a sluggish frontal lobe. All it takes is commitment to getting these strategies into place and being survivor with getting these strategies into place and being survivor with yourself! yourself!
Copyright Brain Injury Association of Queensland, Inc, Australia, Copyright Brain Injury Association of Queensland, Inc, Australia, 2007. This is one of a range of fact sheets made available by the 2007. This is one of a range of fact sheets made available by the Brain Injury Association of Queensland. While all care has been Brain Injury Association of Queensland. While all care has been taken to ensure information is accurate, these fact sheets are only taken to ensure information is accurate, these fact sheets are only intended as a guide and proper medical or professional advice and intended as a guide and proper medical or professional advice and information should be sought. The Association will not be held information should be sought. The Association will not be held responsible for any injuries or damages that arise from following responsible for any injuries or damages that arise from following the information provided in these fact sheets. You can visit the the information provided in these fact sheets. You can visit the Association’s website at Association’s website at www.braininjury.org.auwww.braininjury.org.au or send emails to or send emails to [email protected]@braininjury.org.au

SUPPORT GROUPSSUPPORT GROUPS
Support groups play a vital role in the lives of people with Support groups play a vital role in the lives of people with brain injuries and their families, and never more so than brain injuries and their families, and never more so than when the individual completes rehabilitation and finds that when the individual completes rehabilitation and finds that life is changed in ways that the individual and the family life is changed in ways that the individual and the family find puzzling or difficult to manage. find puzzling or difficult to manage.
Groups enable the individual to identify with others with Groups enable the individual to identify with others with similar problems, and together solutions are often found. similar problems, and together solutions are often found. Additionally, as a result of group interaction, the individual Additionally, as a result of group interaction, the individual feels less alone and a sense of “belonging” is very feels less alone and a sense of “belonging” is very important to those whose lives have been dramatically important to those whose lives have been dramatically changed. changed.
In the opinion of the presenter, the groups should allow for In the opinion of the presenter, the groups should allow for choice to attend. Mandatory participation tied to further choice to attend. Mandatory participation tied to further rehabilitation or insurance benefits is an oppressive rehabilitation or insurance benefits is an oppressive practice undermining free choice and empowerment.practice undermining free choice and empowerment.
In the opinion of the groups are best conducted in a barrier-In the opinion of the groups are best conducted in a barrier-free environment that is away from clinical settings.free environment that is away from clinical settings.
Women’s TBI Support Women’s TBI Support GroupsGroups
http://www.mssm.edu/tbicentral/resources/support_group.shtmlhttp://www.mssm.edu/tbicentral/resources/support_group.shtml Over 100 women attended and gave voice to issues they had held in silence. They Over 100 women attended and gave voice to issues they had held in silence. They
discussed the loss of personal and professional identity, disruption to the family discussed the loss of personal and professional identity, disruption to the family structure, lack of knowledge and understanding about brain injury and common structure, lack of knowledge and understanding about brain injury and common problems after a brain injury, such as fatigue, depression, isolation, and changes in problems after a brain injury, such as fatigue, depression, isolation, and changes in sexuality.sexuality.
This group continues 13 years later as the only one of its kind in New York City. It This group continues 13 years later as the only one of its kind in New York City. It provides a monthly gathering place for women to discuss their cognitive and provides a monthly gathering place for women to discuss their cognitive and emotional needs, grapple with challenges common to female survivors of brain injury emotional needs, grapple with challenges common to female survivors of brain injury and to learn from the experiences of their peers. Group members remark that when and to learn from the experiences of their peers. Group members remark that when they come to group, they feel understood, at ease and accepted, something often they come to group, they feel understood, at ease and accepted, something often lacking in their everyday relationships. lacking in their everyday relationships.
Over the years, many women have found support in the group as they adapted their Over the years, many women have found support in the group as they adapted their lives to accommodate new goals, given the changes thrust upon them by brain lives to accommodate new goals, given the changes thrust upon them by brain injury.injury.
For example, nine years ago Janet was taking courses to allow her to pursue a For example, nine years ago Janet was taking courses to allow her to pursue a position in veterinary care when she slipped on icy pavement and hit her head.position in veterinary care when she slipped on icy pavement and hit her head.
The author joined Mount Sinai as a research assistant in 1996 and later became co-The author joined Mount Sinai as a research assistant in 1996 and later became co-leader of the Women's Support Group (a postdoctoral fellow in neuropsychology, Dr. leader of the Women's Support Group (a postdoctoral fellow in neuropsychology, Dr. Doris Chun, is the second co-leader). She had been a financial executive when I Doris Chun, is the second co-leader). She had been a financial executive when I suffered an aneurysm in 1990. I now feel that brain injury survivors “her included” suffered an aneurysm in 1990. I now feel that brain injury survivors “her included” derive great hope from seeing others with brain injury functioning well and enjoying derive great hope from seeing others with brain injury functioning well and enjoying their jobs everyday. My TBI was a shock, then a challenge, which turned into a new their jobs everyday. My TBI was a shock, then a challenge, which turned into a new beginning. During the recovery process, I discovered that while one door had closed beginning. During the recovery process, I discovered that while one door had closed behind me, a window had been opened.behind me, a window had been opened.