women and coronary artery disease (cad) prof. roland kassab prof. roland kassab head of division of...
TRANSCRIPT
Women andWomen and Coronary Artery Coronary Artery
Disease (CAD)Disease (CAD) Prof. Roland KASSABProf. Roland KASSAB
Head of Division of Cardiology, HDFHead of Division of Cardiology, HDF
Metropolitan Palace Hotel, BeirutMetropolitan Palace Hotel, Beirut
1st May 20101st May 2010



Women and CADWomen and CAD EpidemiologyEpidemiology Cardiovascular risk factorsCardiovascular risk factors Risk stratificationRisk stratification DiagnosisDiagnosis Prognosis and treatment outcomePrognosis and treatment outcome JUPITER: meta-analysis of WomenJUPITER: meta-analysis of Women PCI and CABGPCI and CABG Hormone replacement therapyHormone replacement therapy ConcluionsConcluions

PROGNOSTIC VALUE : BNPPROGNOSTIC VALUE : BNP
EpidemiologyEpidemiology
Statistics on Women and Cardiovascular DiseaseStatistics on Women and Cardiovascular Disease Comparisons to MenComparisons to Men Age Differences Among WomenAge Differences Among Women Racial and Ethnic Group DifferencesRacial and Ethnic Group Differences

CVD and Other Major Causes of CVD and Other Major Causes of Death Death
for Women in the United States: for Women in the United States: 20042004
0
100,000
200,000
300,000
400,000
500,000
Total CVD CHD Cancer Stroke Asthma +COPD
Source: Adapted from American Heart Association 2008
Congestive Heart Failure: Congestive Heart Failure: Gender DifferencesGender Differences
Compared to men, women with heart Compared to men, women with heart failure are:failure are: OlderOlder More likely to have hypertensionMore likely to have hypertension More likely to have diabetesMore likely to have diabetes More likely to have diastolic dysfunctionMore likely to have diastolic dysfunction
Knowledge of diastolic dysfunction Knowledge of diastolic dysfunction prognosis and treatment is limited prognosis and treatment is limited
Trials of congestive heart failure Trials of congestive heart failure treatments have included mainly mentreatments have included mainly men
Source: Stromberg 2003
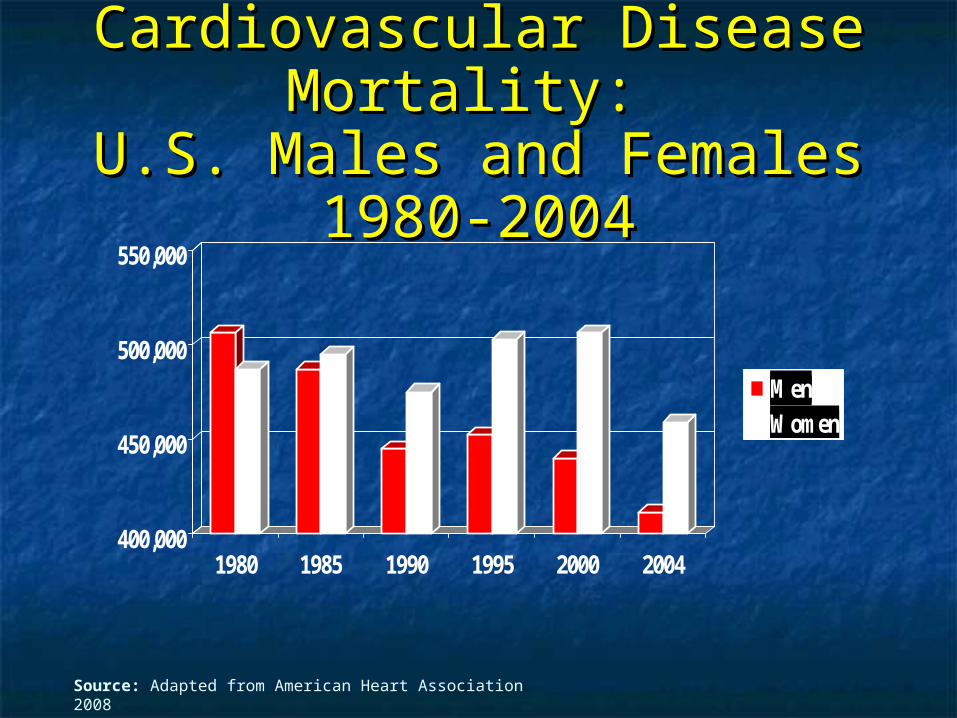
Cardiovascular Disease Cardiovascular Disease Mortality: Mortality:
U.S. Males and Females 1980-U.S. Males and Females 1980-20042004
400,000
450,000
500,000
550,000
1980 1985 1990 1995 2000 2004
MenWomen
Source: Adapted from American Heart Association 2008
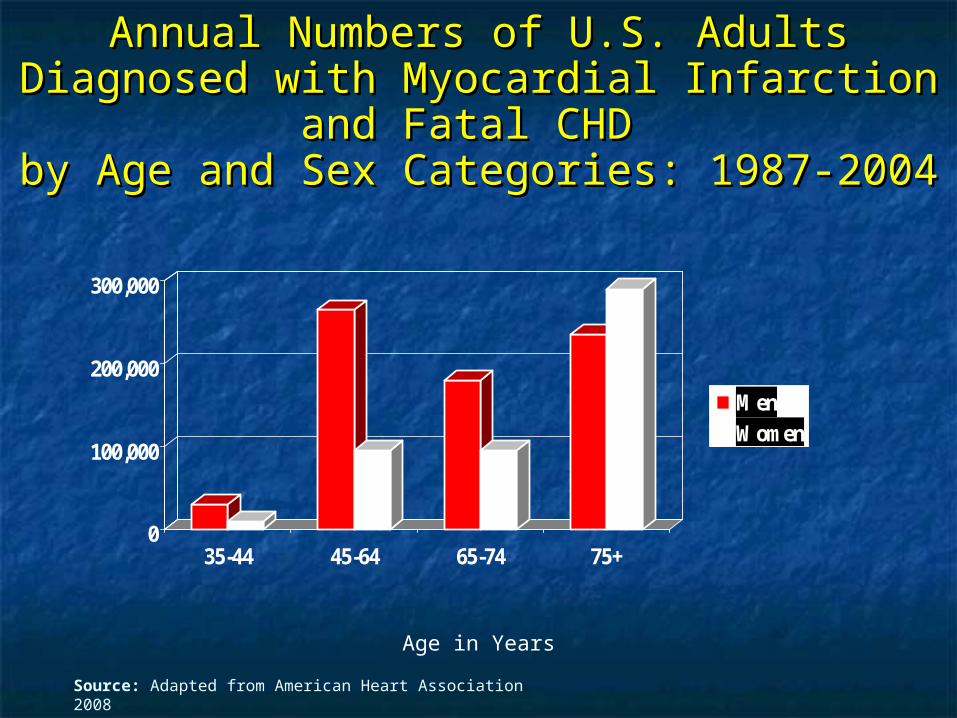
Annual Numbers of U.S. Adults Diagnosed Annual Numbers of U.S. Adults Diagnosed with Myocardial Infarction and Fatal CHD with Myocardial Infarction and Fatal CHD by Age and Sex Categories: 1987-2004by Age and Sex Categories: 1987-2004
0
100,000
200,000
300,000
35-44 45-64 65-74 75+
MenWomen
Source: Adapted from American Heart Association 2008
Age in Years
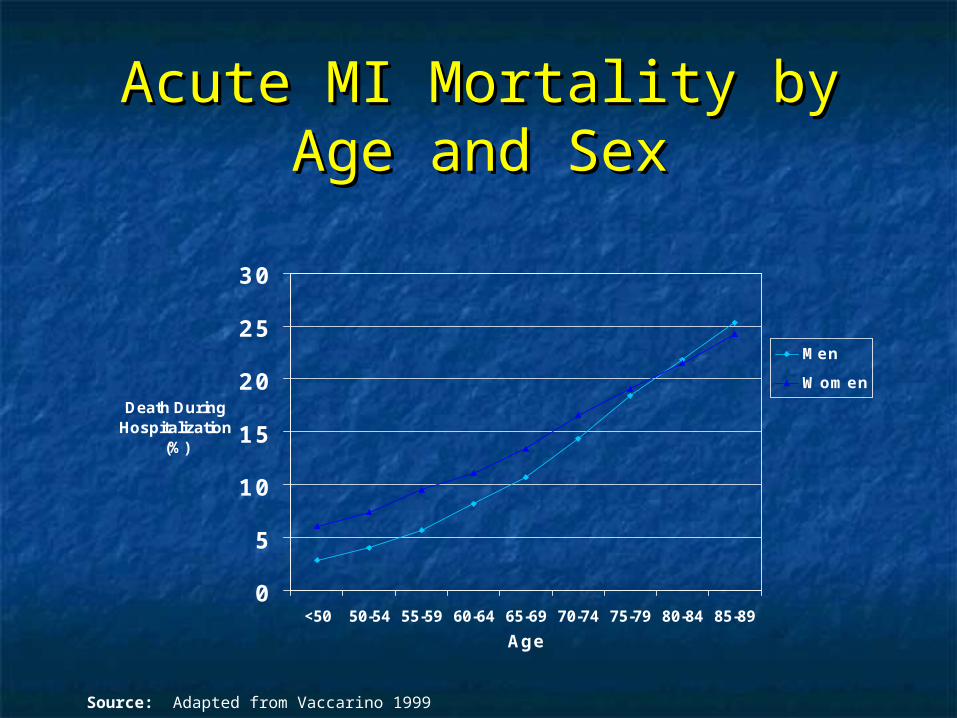
Acute MI Mortality by Age Acute MI Mortality by Age and Sexand Sex
0
5
10
15
20
25
30
<50 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89
Age
Death During Hospitalization
(%)
Men
Women
Source: Adapted from Vaccarino 1999
Racial and Ethnic GroupsRacial and Ethnic Groups
Cardiovascular disease is the leading Cardiovascular disease is the leading cause of death for African Americans, cause of death for African Americans, Latinos, Asian Americans, Pacific Latinos, Asian Americans, Pacific Islanders, and American IndiansIslanders, and American Indians
African American women are at the African American women are at the highest risk for death from heart disease highest risk for death from heart disease among all racial, ethnic, among all racial, ethnic, and gender groupsand gender groups
Source: American Heart Association 2004
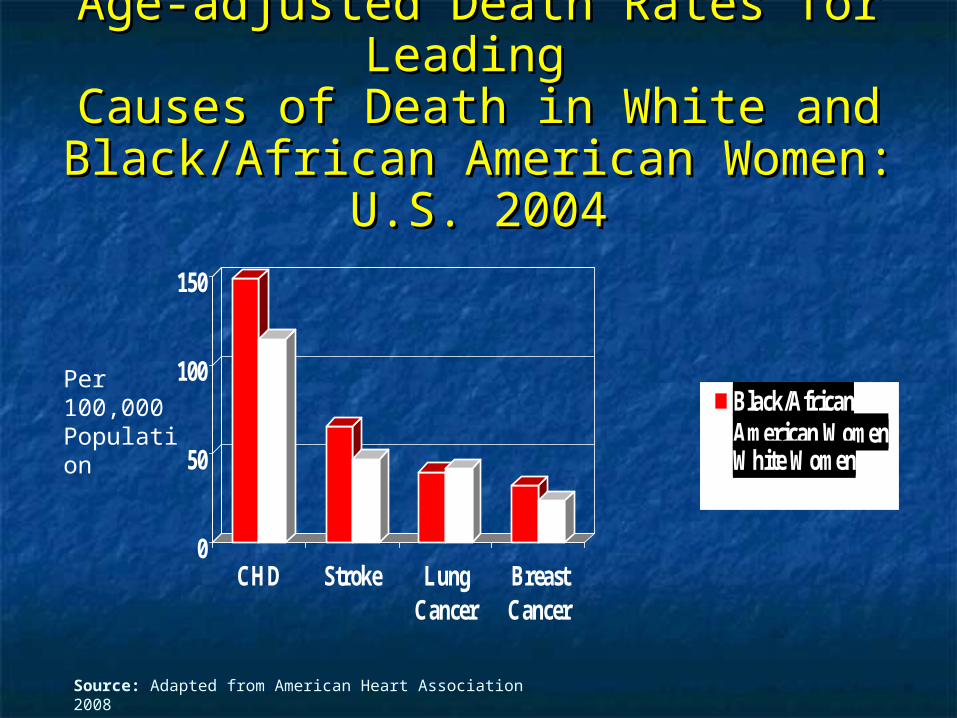
Age-adjusted Death Rates for Leading Age-adjusted Death Rates for Leading Causes of Death in White and Causes of Death in White and
Black/African American Women: U.S. Black/African American Women: U.S. 20042004
0
50
100
150
CHD Stroke LungCancer
BreastCancer
Black/AfricanAmerican WomenWhite Women
Source: Adapted from American Heart Association 2008
Per100,000Population
Summary 1Summary 1
Among U.S. women, cardiovascular Among U.S. women, cardiovascular disease is the leading cause of death disease is the leading cause of death
Among U.S. women, cardiovascular Among U.S. women, cardiovascular disease is the leading cause of death disease is the leading cause of death for whites, African Americans, Latinas, for whites, African Americans, Latinas, Asian Americans, Pacific Islanders, and Asian Americans, Pacific Islanders, and American IndiansAmerican Indians
Source: American Heart Association 2008

Summary 2Summary 2
Mortality from CVD has decreased more Mortality from CVD has decreased more for men in the past 20 years than for for men in the past 20 years than for womenwomen
Over 10,000 women under age 45 suffer Over 10,000 women under age 45 suffer an acute myocardial infarction every yearan acute myocardial infarction every year
Source: American Heart Association 2008

Are All Statins Born Alike ?Are All Statins Born Alike ?
Cardiovascular Risk Factors in Cardiovascular Risk Factors in WomenWomen
UnmodifiableUnmodifiable AgeAge Family HistoryFamily History
ModifiableModifiable Diabetes Diabetes DysplipidemiaDysplipidemia HypertensionHypertension ObesityObesity Poor DietPoor Diet Sedentary LifestyleSedentary Lifestyle Cigarette SmokingCigarette Smoking
Source: ATP III 2002, Mosca 2007
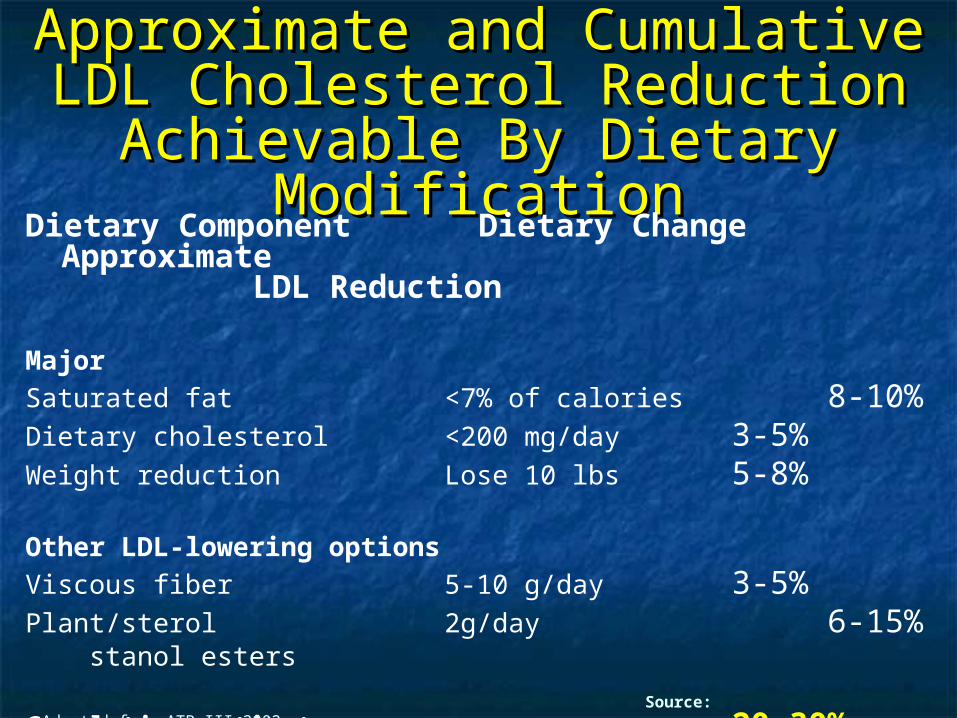
Approximate and Cumulative Approximate and Cumulative LDL Cholesterol Reduction LDL Cholesterol Reduction
Achievable By Dietary Achievable By Dietary ModificationModification
Dietary Component Dietary Change Approximate LDL Reduction
Major
Saturated fat <7% of calories 8-10%Dietary cholesterol <200 mg/day 3-5%Weight reduction Lose 10 lbs 5-8%
Other LDL-lowering options
Viscous fiber 5-10 g/day 3-5%Plant/sterol 2g/day 6-15% stanol esters
Cumulative estimate 20-30% Source: Adapted from ATP III 2002
Treatable Risk Factors: The Treatable Risk Factors: The Epidemiology of Cholesterol Levels Epidemiology of Cholesterol Levels
and Subfractionsand Subfractions Low HDL more important in women than menLow HDL more important in women than men
For every 1 mg/dL increase in HDL 3% decrease in For every 1 mg/dL increase in HDL 3% decrease in CHD risk for women and 2% decrease in CHD risk CHD risk for women and 2% decrease in CHD risk for menfor men
Total cholesterol/HDL ratio very predictive of CHD Total cholesterol/HDL ratio very predictive of CHD risk in womenrisk in women
Triglyceride elevation associated with greater Triglyceride elevation associated with greater atherogenic significance in women than in menatherogenic significance in women than in men
Source: Maron 2000
Treatable Risk Factors: Treatable Risk Factors: Cholesterol Level and Cholesterol Level and
SubfractionsSubfractions LDL>160 mg/dL associated with 3.3-fold LDL>160 mg/dL associated with 3.3-fold
elevation in risk for women less than 65 elevation in risk for women less than 65 years oldyears old
LDL pattern of small, dense particles LDL pattern of small, dense particles (more atherogenic) present in 25% of (more atherogenic) present in 25% of population, but less frequently seen in population, but less frequently seen in womenwomen
Menopausal transition associated with Menopausal transition associated with increasing proportion of this subfractionincreasing proportion of this subfractionSource: Keil 2000, Carr 2000, Hokanson 1996
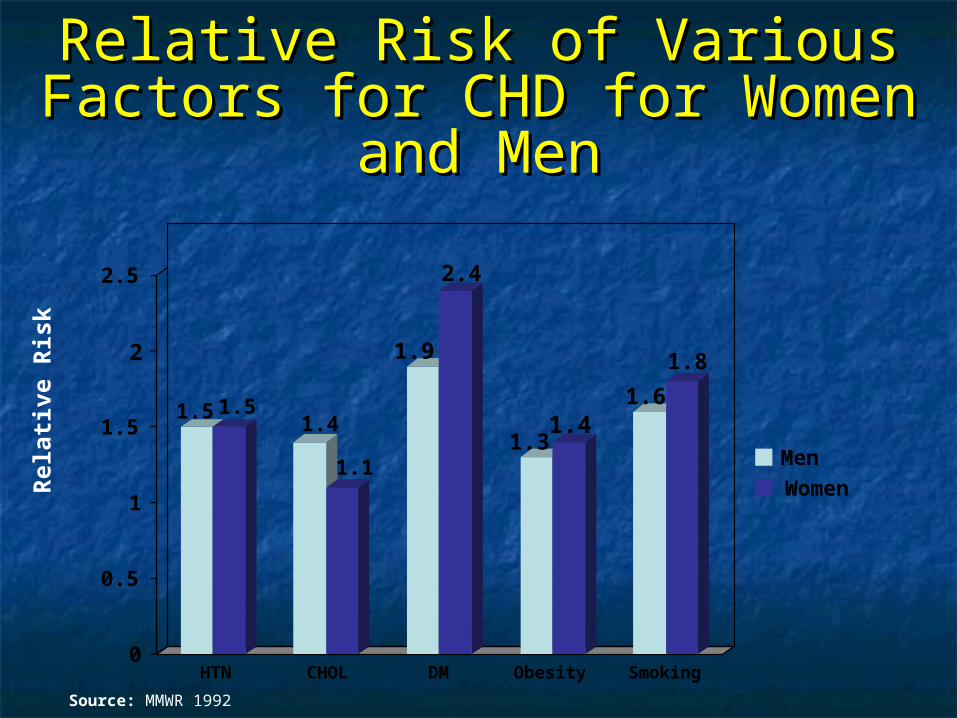
Source: MMWR 1992
Rel
ativ
e R
isk
1.5 1.51.4
1.1
1.9
2.4
1.31.4
1.6
1.8
0
0.5
1
1.5
2
2.5
HTN CHOL DM Obesity Smoking
Men
Women
Relative Risk of Various Factors Relative Risk of Various Factors for CHD for Women and Menfor CHD for Women and Men
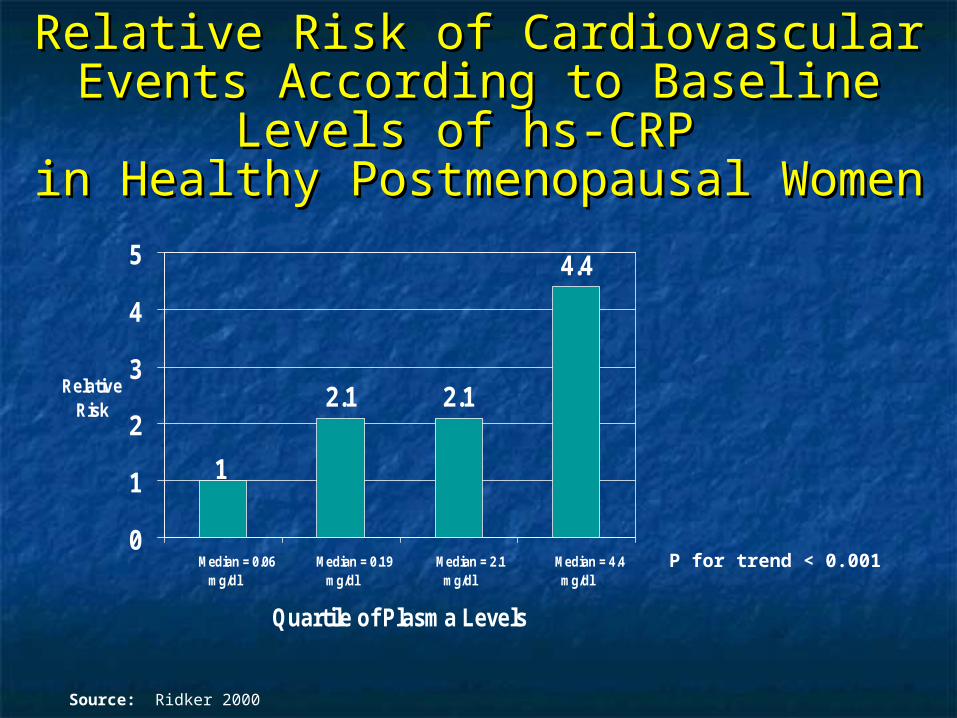
Relative Risk of Cardiovascular Events Relative Risk of Cardiovascular Events According to Baseline Levels of hs-CRP According to Baseline Levels of hs-CRP
in Healthy Postmenopausal Womenin Healthy Postmenopausal Women
2.1 2.1
4.4
1
0
1
2
3
4
5
Median = 0.06mg/dl
Median = 0.19mg/dl
Median = 2.1mg/dl
Median = 4.4mg/dl
Quartile of Plasma Levels
Relative Risk
P for trend < 0.001
Source: Ridker 2000
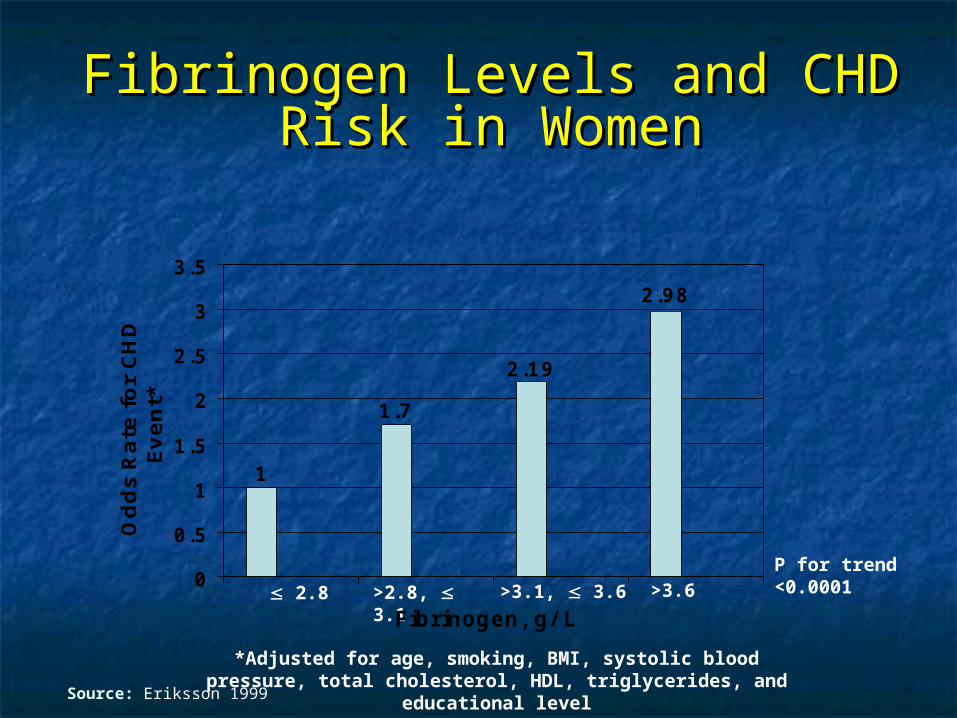
Fibrinogen Levels and CHD Risk Fibrinogen Levels and CHD Risk in Womenin Women
*Adjusted for age, smoking, BMI, systolic blood pressure, total cholesterol, HDL, triglycerides, and educational level
2.8 >2.8, 3.1 >3.1, 3.6 >3.6
Source: Eriksson 1999
2.19
1.7
1
2.98
0
0.5
1
1.5
2
2.5
3
3.5
Fibrinogen, g/ L
Od
ds
Rate
fo
r C
HD
Even
t*
P for trend <0.0001
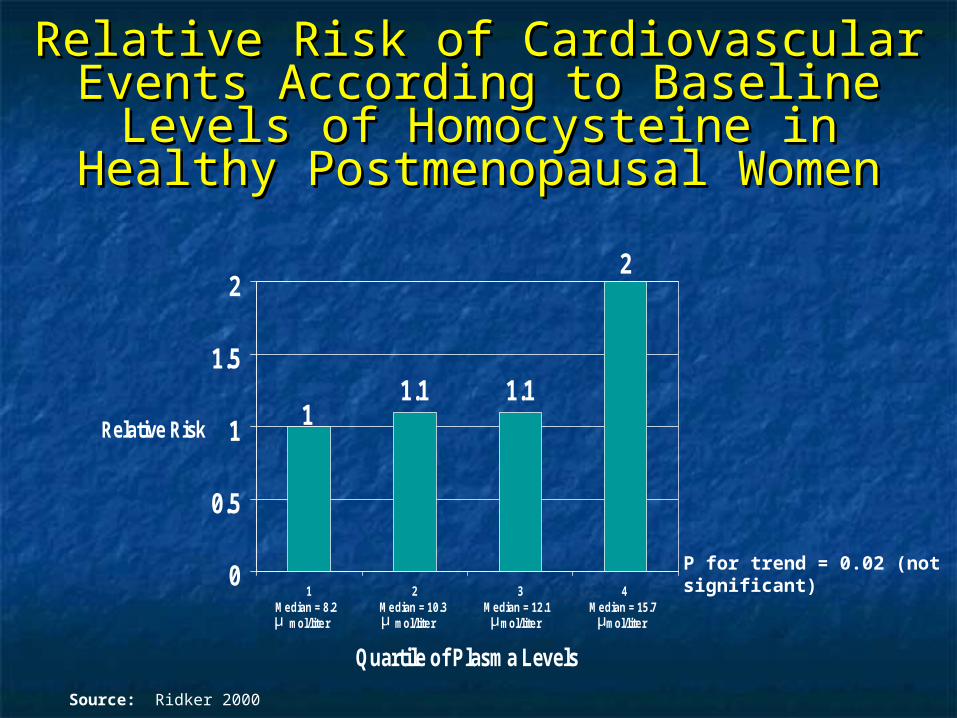
Relative Risk of Cardiovascular Events Relative Risk of Cardiovascular Events According to Baseline Levels of According to Baseline Levels of
Homocysteine in Healthy Homocysteine in Healthy Postmenopausal WomenPostmenopausal Women
1.1 1.1
2
1
0
0.5
1
1.5
2
1 Median = 8.2
mol/liter
2 Median = 10.3
mol/liter
3 Median = 12.1
mol/liter
4 Median = 15.7
mol/liter
Quartile of Plasma Levels
Relative Risk
P for trend = 0.02 (not significant)
μ μμμ
Source: Ridker 2000
Psychosocial Stressors in Psychosocial Stressors in Women with CHD: The Women with CHD: The
Stockholm Female Coronary Stockholm Female Coronary Risk StudyRisk Study
Among women who were married or Among women who were married or cohabitating with a male partner, marital cohabitating with a male partner, marital stress was associated with nearly 3-fold stress was associated with nearly 3-fold increased risk of recurrent CHD eventsincreased risk of recurrent CHD events
Living alone and work stress did not Living alone and work stress did not significantly increase recurrent CHD significantly increase recurrent CHD eventsevents
Source: Orth-Gomer 2000
Depression and CHD: Results Depression and CHD: Results from the Women’s Health from the Women’s Health
Initiative StudyInitiative Study
Depression is an independent predictor of CHD Depression is an independent predictor of CHD death among women with no history of CHDdeath among women with no history of CHD
Source: Wassertheil-Smoller 2004

Risk Stratification:Risk Stratification: High Risk High Risk
Diabetes mellitusDiabetes mellitus Documented atherosclerotic diseaseDocumented atherosclerotic disease
Established coronary heart diseaseEstablished coronary heart disease Peripheral arterial diseasePeripheral arterial disease Cerebrovascular diseaseCerebrovascular disease Abdominal aortic aneurysmAbdominal aortic aneurysm
Includes many patients with chronic kidney Includes many patients with chronic kidney disease, especially ESRDdisease, especially ESRD
10-year Framingham global risk > 20%, or high 10-year Framingham global risk > 20%, or high risk based on another population-adapted global risk based on another population-adapted global risk assessment toolrisk assessment tool
Source: Mosca 2007
Risk Stratification:Risk Stratification: At Risk:At Risk:
>> 1 major risk factors for CVD, including: 1 major risk factors for CVD, including: Cigarette smokingCigarette smoking HypertensionHypertension DyslipidemiaDyslipidemia Family history of premature CVD (CVD at < 55 years in a Family history of premature CVD (CVD at < 55 years in a
male relative, or < 65 years in a female relative)male relative, or < 65 years in a female relative) Obesity, especially central obesityObesity, especially central obesity Physical inactivityPhysical inactivity Poor dietPoor diet
Metabolic syndromeMetabolic syndrome Evidence of subclinical coronary artery disease (eg Evidence of subclinical coronary artery disease (eg
coronary calcification), or poor exercise capacity on coronary calcification), or poor exercise capacity on treadmill test or abnormal heart rate recovery after treadmill test or abnormal heart rate recovery after stopping exercisestopping exercise
Source: Mosca 2007
Definition of Metabolic Definition of Metabolic Syndrome in WomenSyndrome in Women
Abdominal obesity - waist Abdominal obesity - waist circumference circumference >> 35 in. 35 in.
High triglycerides ≥ 150mg/dLHigh triglycerides ≥ 150mg/dL Low HDL cholesterol < 50mg/dLLow HDL cholesterol < 50mg/dL Elevated BP ≥ 130/85mm HgElevated BP ≥ 130/85mm Hg Fasting glucose ≥ 100mg/dLFasting glucose ≥ 100mg/dL
Source: AHA/NHLBI 2005
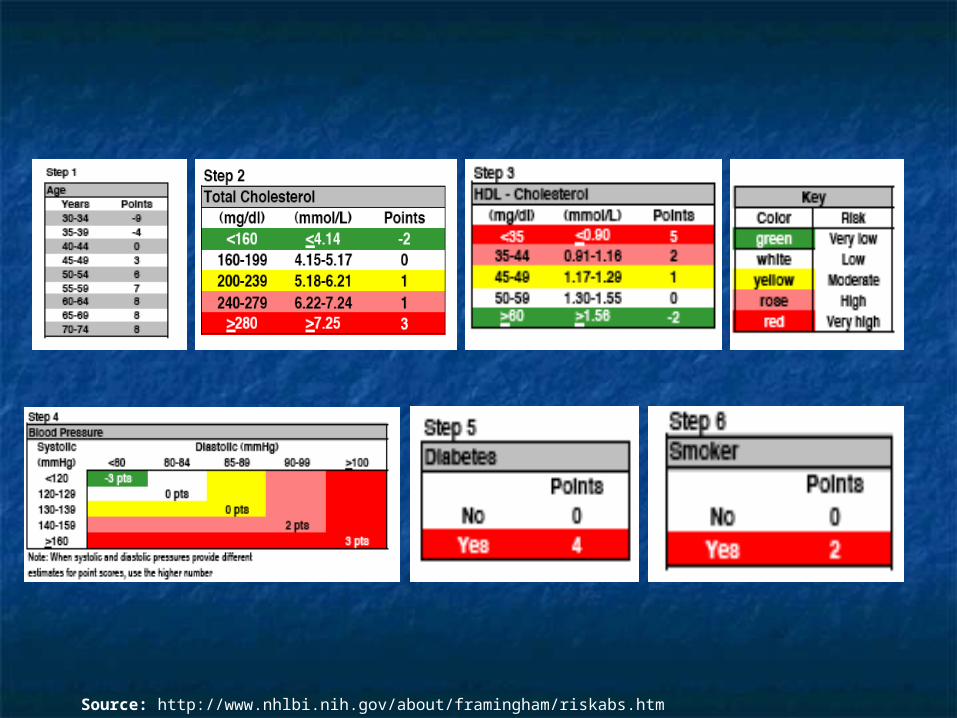
Source: http://www.nhlbi.nih.gov/about/framingham/riskabs.htm
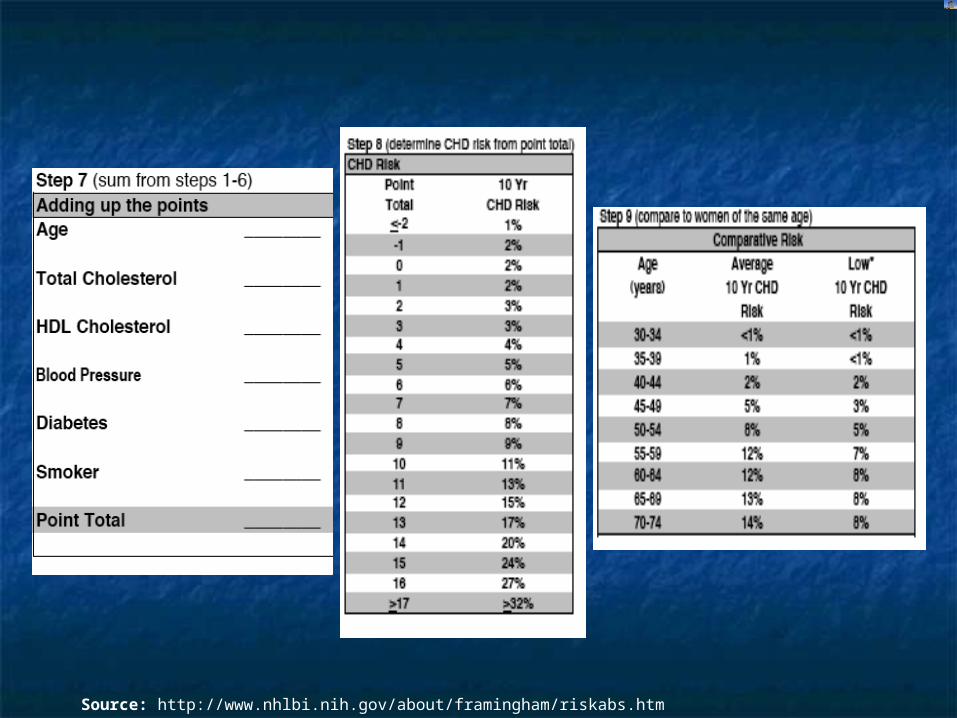
Source: http://www.nhlbi.nih.gov/about/framingham/riskabs.htm

Diagnosis of Coronary Artery Diagnosis of Coronary Artery Disease in WomenDisease in Women
Chest pain is experienced by most women with CHD, Chest pain is experienced by most women with CHD, but but non-chest painnon-chest pain presentations are more common presentations are more common in women than menin women than men
Other Presenting SymptomsOther Presenting Symptoms Upper abdominal pain, fullness, burning sensationUpper abdominal pain, fullness, burning sensation Shortness of breathShortness of breath NauseaNausea Neck, back, jaw painNeck, back, jaw pain
AssociationsAssociations Precipitated by exertionPrecipitated by exertion Precipitated by emotional distress Precipitated by emotional distress
Source: Charney 2002, Goldberg 1998
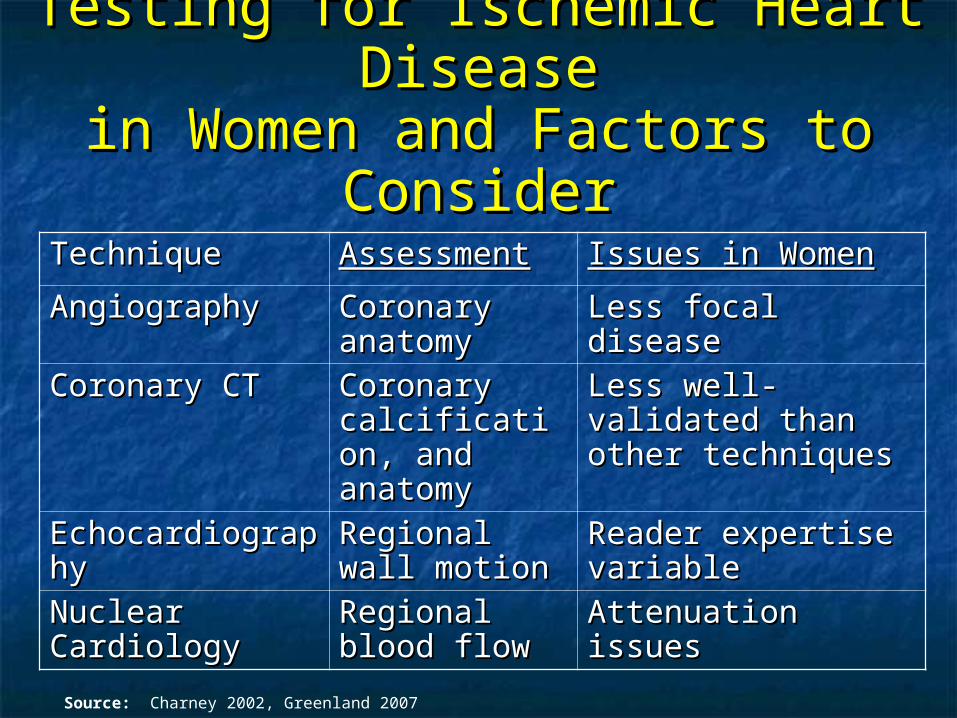
Testing for Ischemic Heart Testing for Ischemic Heart DiseaseDisease
in Women and Factors to in Women and Factors to ConsiderConsider
TechniqueTechnique AssessmentAssessment Issues in WomenIssues in Women
AngiographyAngiography Coronary Coronary anatomyanatomy
Less focal diseaseLess focal disease
Coronary CTCoronary CT Coronary Coronary calcification, calcification, and anatomyand anatomy
Less well-validated Less well-validated than other than other techniquestechniques
EchocardiographEchocardiographyy
Regional wall Regional wall motionmotion
Reader expertise Reader expertise variablevariable
Nuclear Nuclear CardiologyCardiology
Regional Regional blood flowblood flow
Attenuation issuesAttenuation issues
Source: Charney 2002, Greenland 2007
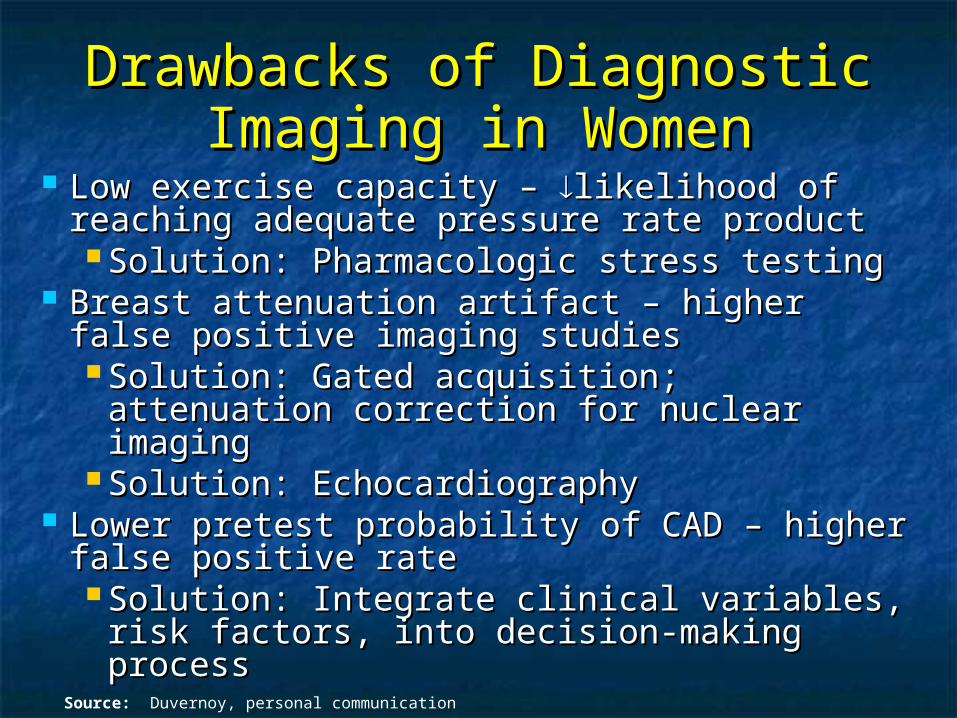
Drawbacks of Diagnostic Drawbacks of Diagnostic Imaging in WomenImaging in Women
Low exercise capacity – Low exercise capacity – likelihood of likelihood of reaching adequate pressure rate productreaching adequate pressure rate product Solution: Pharmacologic stress testingSolution: Pharmacologic stress testing
Breast attenuation artifact – higher false Breast attenuation artifact – higher false positive imaging studiespositive imaging studies Solution: Gated acquisition; attenuation Solution: Gated acquisition; attenuation
correction for nuclear imagingcorrection for nuclear imaging Solution: EchocardiographySolution: Echocardiography
Lower pretest probability of CAD – higher Lower pretest probability of CAD – higher false positive ratefalse positive rate Solution: Integrate clinical variables, risk Solution: Integrate clinical variables, risk
factors, into decision-making processfactors, into decision-making process
Source: Duvernoy, personal communication
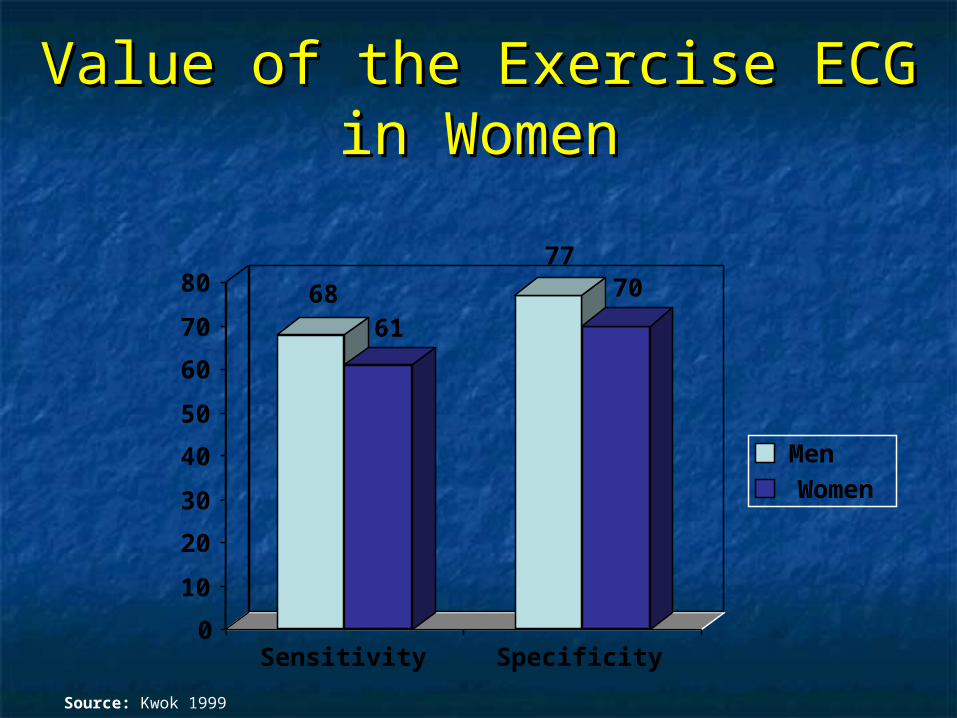
Value of the Exercise ECG in Value of the Exercise ECG in WomenWomen
6861
7770
0
10
20
30
40
50
60
70
80
Sensitivity Specificity
MenWomen
Source: Kwok 1999
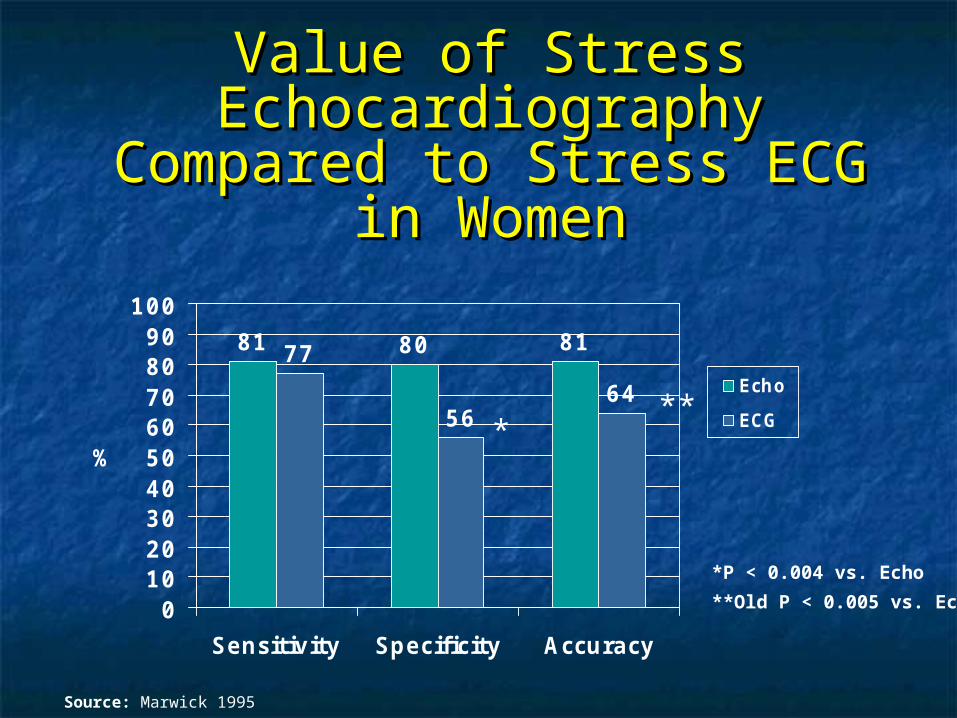
Value of Stress Value of Stress Echocardiography Compared Echocardiography Compared
to Stress ECG in Womento Stress ECG in Women
81 80 8177
5664
0102030405060708090
100
Sensitivity Specificity Accuracy
%
Echo
ECG
Source: Marwick 1995
*P < 0.004 vs. Echo
**Old P < 0.005 vs. Echo
***
CHD: Differences in CHD: Differences in Presentation and Findings in Presentation and Findings in Women Compared to MenWomen Compared to Men
Lower prevalence of MILower prevalence of MIMore severe CHFMore severe CHFMore severe anginaMore severe anginaLess angiographic CADLess angiographic CADMore ostial lesionsMore ostial lesionsMore microvascular More microvascular dysfunction?dysfunction?
Abnormal vasomotor tone?Abnormal vasomotor tone?More endothelial More endothelial dysfunction?dysfunction?
Source: Jacobs 2003
Women and CHD: Women and CHD: What Test to Order WhenWhat Test to Order When
For women at high or intermediate risk of coronary For women at high or intermediate risk of coronary artery disease, consider artery disease, consider treadmill echocardiogarphytreadmill echocardiogarphy or or nuclear perfusionnuclear perfusion imaging imaging
For women unable to exercise, consider For women unable to exercise, consider dobutaminedobutamine stress echocardiography or stress echocardiography or adenosine or adenosine or dipyridamoledipyridamole nuclear imaging nuclear imaging
In high risk women with typical symptoms of In high risk women with typical symptoms of coronary artery disease, consider coronary artery disease, consider coronary coronary angiographyangiography
For high risk women, consider For high risk women, consider cardiac cardiac catheterizationcatheterization if symptoms persist despite negative non-invasive if symptoms persist despite negative non-invasive imagingimaging
Source: Anderson 2007, Klocke 2003, Douglas 2008, Duvernoy 2005
Women and CHD: Women and CHD: What Test to Order WhenWhat Test to Order When
A stepwise approach beginning with conventional A stepwise approach beginning with conventional exercise testing may be considered for women exercise testing may be considered for women who:who: Are at low or intermediate risk for coronary Are at low or intermediate risk for coronary
artery diseaseartery disease Are able to exerciseAre able to exercise Have an electrocardiogram that can be Have an electrocardiogram that can be
interpreted during stress testinginterpreted during stress testing An An image-enhanced testimage-enhanced test may be more predictive may be more predictive
in women than conventional electrocardiogram in women than conventional electrocardiogram stress testing, and may also be more cost stress testing, and may also be more cost effective in women at intermediate risk for CHDeffective in women at intermediate risk for CHD
Source: Anderson 2007, Klocke 2003, Douglas 2008,Mieres 2005

PROGNOSTIC VALUE : pro-PROGNOSTIC VALUE : pro-BNPBNP
Cardiovascular Disease in Cardiovascular Disease in Women : Prognosis and Women : Prognosis and
Treatment OutcomesTreatment Outcomes
Women Received Less Women Received Less Interventions Interventions
to Prevent and Treat Heart to Prevent and Treat Heart DiseaseDisease
Less cholesterol screeningLess cholesterol screening Less lipid-lowering therapiesLess lipid-lowering therapies Less use of heparin, beta-blockers and aspirin Less use of heparin, beta-blockers and aspirin
during myocardial infarctionduring myocardial infarction Less antiplatelet therapy for secondary Less antiplatelet therapy for secondary
preventionprevention Fewer referrals to cardiac rehabilitationFewer referrals to cardiac rehabilitation Fewer implantable cardioverter-defibrillators Fewer implantable cardioverter-defibrillators
compared to men with the same recognized compared to men with the same recognized indicationsindications
Sources: Chandra 1998, Nohria 1998, Scott 2004, O’Meara 2004, Hendrix 2005, Chou 2007, Hernandez 2007, Cho 2008
Prognosis After MIPrognosis After MI
38% of women die within first year Compared to 25% of men
35% of women will have second MI within 6 years Compared to 18% of men
Source: Wenger 2004
PrognosisPrognosis
Women < 65 yrs have Women < 65 yrs have 2 X mortality2 X mortality rate after MI rate after MI compared to men of same agecompared to men of same age
After MI, women have significantly higher rates of:After MI, women have significantly higher rates of: DepressionDepression Physical disabilityPhysical disability
After CABG, women have significantly higher rates of:After CABG, women have significantly higher rates of: Hospital readmissionHospital readmission Reduced mental health and physical functioningReduced mental health and physical functioning
Source: Vaccarino 1999, Ades 2002, Lauzon 2003, Vaccarino 2003
Undertreatment of MI in Undertreatment of MI in WomenWomen
Compared with men:Compared with men: Less emergent thrombolysisLess emergent thrombolysis Less acute catheterization and Less acute catheterization and
angioplastyangioplasty Less acute surgical revascularizationLess acute surgical revascularization Less use of heparin, beta-blockers, and Less use of heparin, beta-blockers, and
aspirinaspirin
Source: Chandra 1998, Nohria 1998
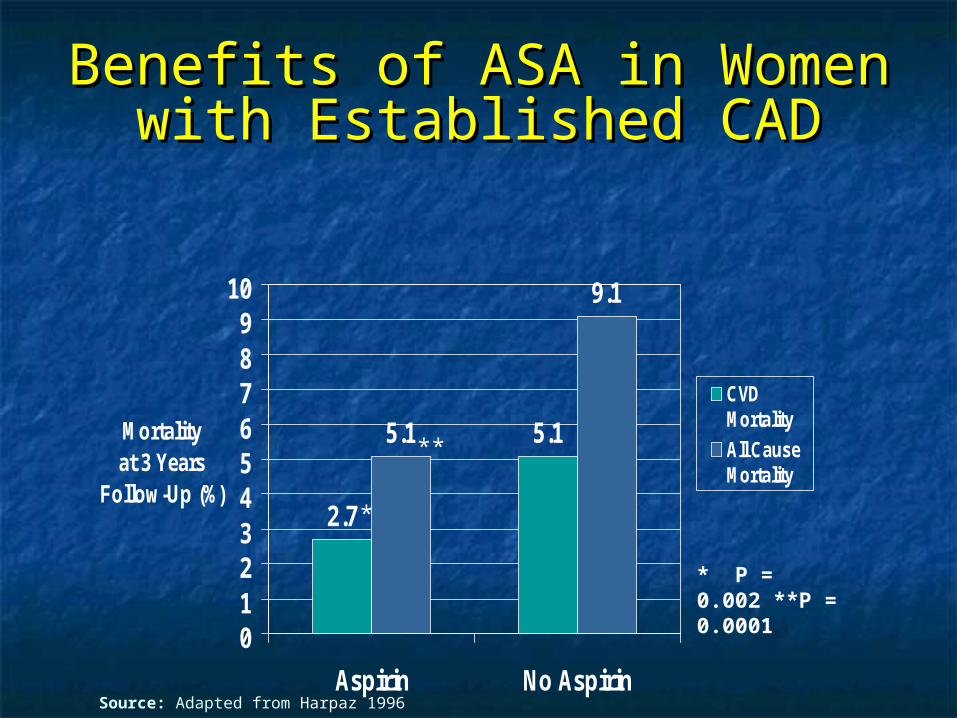
Benefits of ASA in Women with Benefits of ASA in Women with Established CADEstablished CAD
2.7
5.15.1
9.1
0123456789
10
Aspirin No Aspirin
Mortality at 3 Years
Follow-Up (%)
CVDMortality
All CauseMortality
* P = 0.002 **P = 0.0001
*
**
Source: Adapted from Harpaz 1996
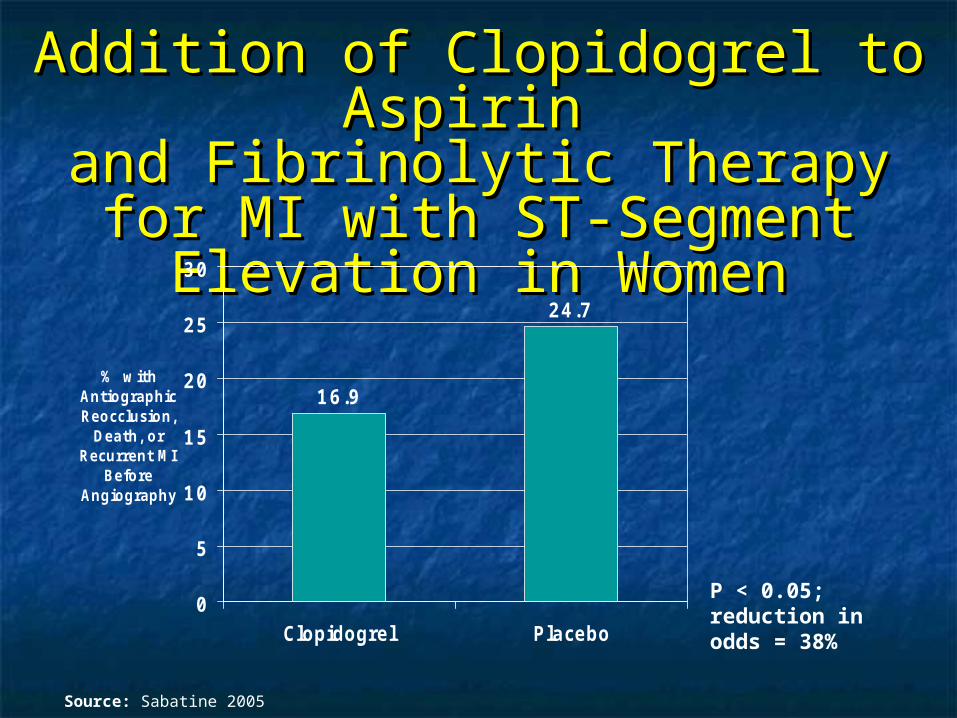
Addition of Clopidogrel to Addition of Clopidogrel to Aspirin Aspirin
and Fibrinolytic Therapy for MI and Fibrinolytic Therapy for MI with ST-Segment Elevation in with ST-Segment Elevation in
WomenWomen
16.9
24.7
0
5
10
15
20
25
30
Clopidogrel Placebo
% with Antiographic Reocclusion,
Death, or Recurrent MI
Before Angiography
P < 0.05; reduction in odds = 38%
Source: Sabatine 2005
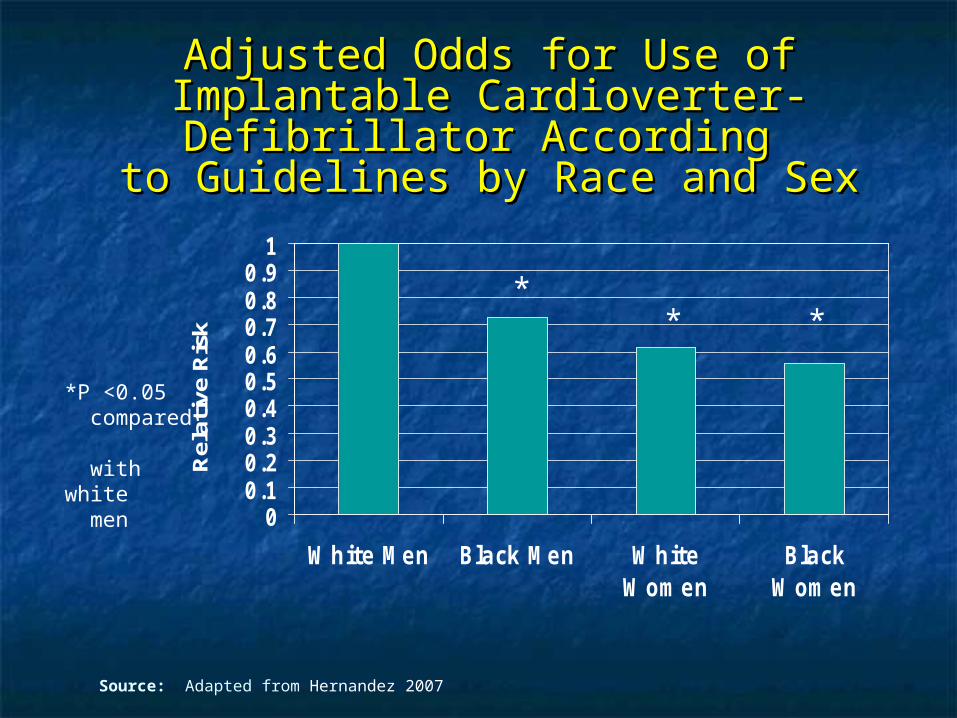
Adjusted Odds for Use of Implantable Adjusted Odds for Use of Implantable Cardioverter-Defibrillator According Cardioverter-Defibrillator According
to Guidelines by Race and Sexto Guidelines by Race and Sex
00.10.20.30.40.50.60.70.80.9
1
White Men Black Men WhiteWomen
BlackWomen
Rel
ativ
e R
isk
*P <0.05 compared with white men
Source: Adapted from Hernandez 2007
** *

Gender Gap in Dyslipidemia Gender Gap in Dyslipidemia TreatmentTreatment
Significantly more men than women have Significantly more men than women have annual cholesterol measurementsannual cholesterol measurements
Significantly more men than women Significantly more men than women receive effective lipid-lowering therapyreceive effective lipid-lowering therapy
African Americans receive less lipid-African Americans receive less lipid-lowering treatment compared to whiteslowering treatment compared to whites
Source: O’Meara 2004, Hendrix 2005, Chou 2007, Cho 2008
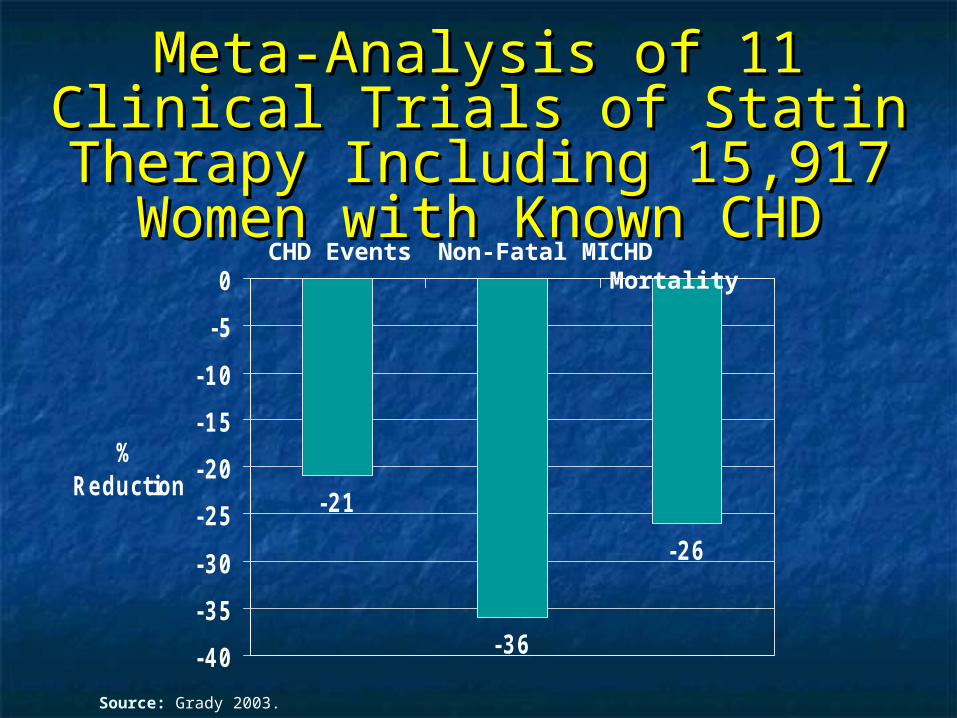
Meta-Analysis of 11 Clinical Meta-Analysis of 11 Clinical Trials of Statin Therapy Trials of Statin Therapy
Including 15,917 Women with Including 15,917 Women with Known CHDKnown CHD
-21
-36
-26
-40
-35
-30
-25
-20
-15
-10
-5
0
% Reduction
CHD Events Non-Fatal MI CHD Mortality
Source: Grady 2003.
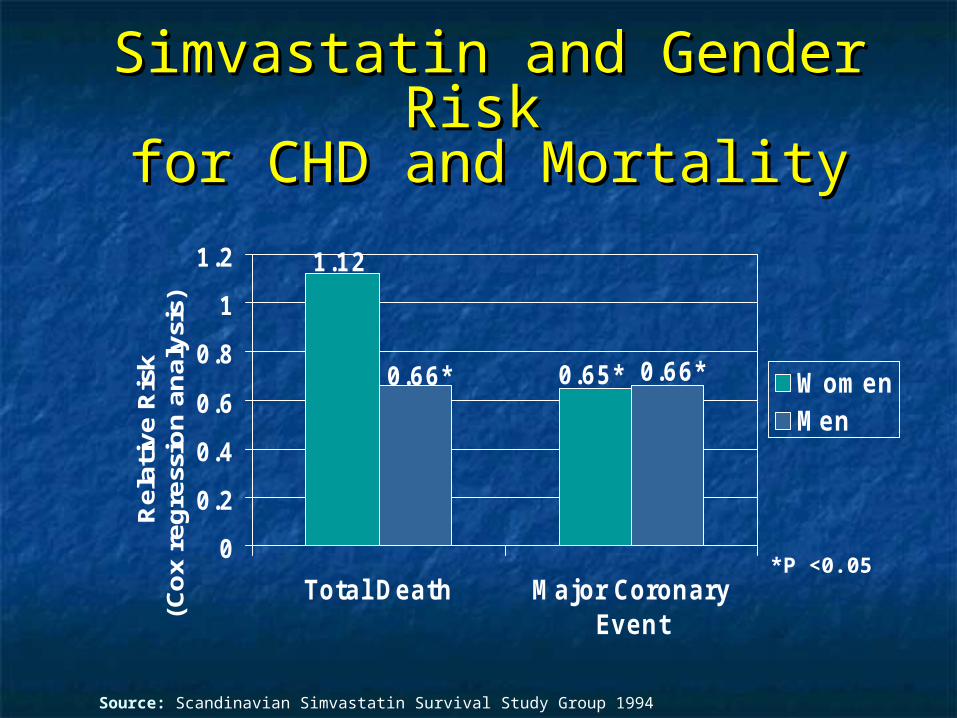
Simvastatin and Gender Risk Simvastatin and Gender Risk for CHD and Mortalityfor CHD and Mortality
0.65*
1.12
0.66* 0.66*
0
0.2
0.4
0.6
0.8
1
1.2
Total Death Major CoronaryEvent
Rel
ativ
e R
isk
(Co
x re
gre
ssio
n a
nal
ysis
)
WomenMen
*P <0.05
Source: Scandinavian Simvastatin Survival Study Group 1994
Heart Protection Study: Major Heart Protection Study: Major FindingsFindings
Randomized, placebo-controlled trial of over Randomized, placebo-controlled trial of over 20,000 patients at risk for CVD20,000 patients at risk for CVD
Statin treatment reduced the risk of heart Statin treatment reduced the risk of heart attacks and strokes by at least one third, as attacks and strokes by at least one third, as well as reducing the need for arterial well as reducing the need for arterial surgery, angioplasty and amputations.surgery, angioplasty and amputations.
Major CV events were reduced in women Major CV events were reduced in women (5082 enrolled) as well as men, and in all (5082 enrolled) as well as men, and in all age groups, across all cholesterol levels.age groups, across all cholesterol levels.
Source: HPS Writing Group, Lancet 2002

Primary Prevention of CHD Events Primary Prevention of CHD Events with Statin Treatment: with Statin Treatment:
AFCAPS/TexCAPSAFCAPS/TexCAPS
-46
-37
-50-45-40-35-30-25-20-15-10
-50
% MenWomen
Relative Risk of First Major Coronary Events
P < 0.001 compared to placebo
Source: Downs 1998

Statins for the Primary Prevention of CVD in Women with Elevated hsCRP or Dyslipidemia:
Results from JUPITER and Meta-Analysis of Women from Primary Prevention Statin Trials
Samia Mora, Robert J Glynn, Judith Hsia, Jean G MacFadyen,Jacques Genest, and Paul M Ridker
Brigham and Women’s HospitalHarvard Medical School
Boston, MA
on behalf of the JUPITER Trial Study Group
Circulation 2010; 121:1069-1077
Background
Statins for patients with CVD is established• Similar benefit in women, men• Relative risk reduction ~20-30%
Statins for women with no CVD is controversial• Prior meta-analyses: non-significant • RR CHD events 0.87 (0.22-1.68), P=0.17
N = 11, 435 women
Walsh and Pignone, JAMA 2004;2243
Objectives
1. Pre-specified analysis in JUPITER for efficacy and safety of rosuvastatin in women and men with elevated hsCRP and non-elevated LDL cholesterol
2. Updated meta-analysis of statin therapy for primary prevention of CVD in women
JUPITER : Trial Objective
To investigate whether rosuvastatin 20 mg vs placebo decreases major CVD eventsin apparently healthy men and women with LDL < 130 mg/dL (3.36 mmol/L) who are at increased vascular risk due to enhanced inflammatory response, with hsCRP > 2 mg/L
Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin
Ridker PM et al NEJM 2008;2195
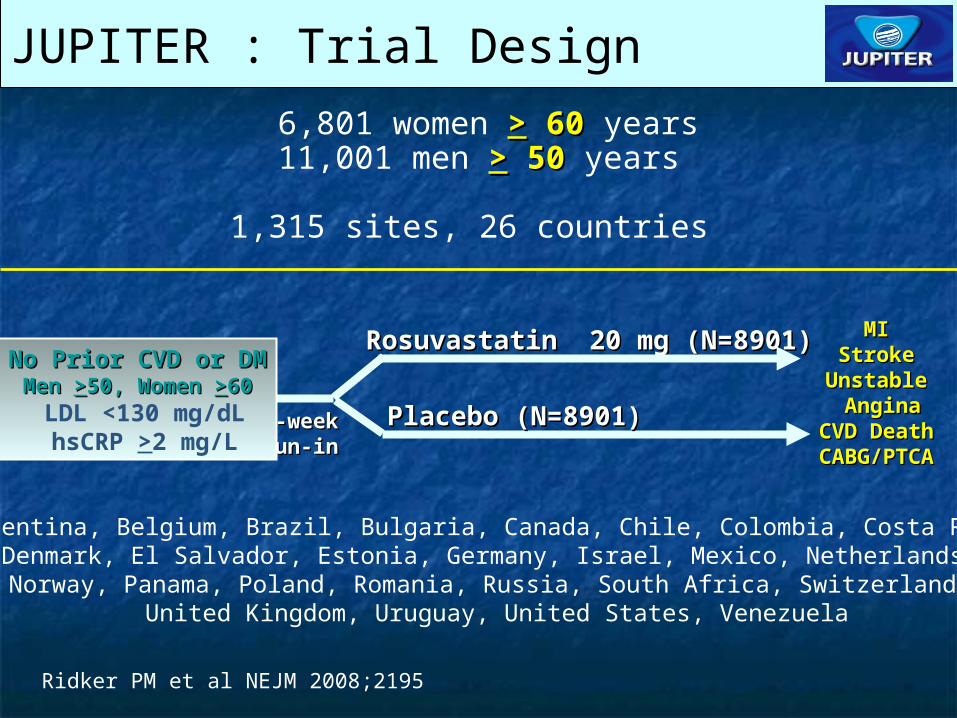
Rosuvastatin 20 mg (N=8901)Rosuvastatin 20 mg (N=8901) MIMIStrokeStroke
UnstableUnstable AnginaAngina
CVD DeathCVD DeathCABG/PTCACABG/PTCA
6,801 women >> 60 60 years11,001 men >> 50 50 years
1,315 sites, 26 countries
4-week 4-week run-inrun-in
No Prior CVD or DMNo Prior CVD or DMMen Men >>50, Women 50, Women >>6060
LDL <130 mg/dL hsCRP >2 mg/L
JUPITER : Trial Design
Placebo (N=8901)Placebo (N=8901)
Argentina, Belgium, Brazil, Bulgaria, Canada, Chile, Colombia, Costa Rica, Denmark, El Salvador, Estonia, Germany, Israel, Mexico, Netherlands, Norway, Panama, Poland, Romania, Russia, South Africa, Switzerland,
United Kingdom, Uruguay, United States, Venezuela
Ridker PM et al NEJM 2008;2195
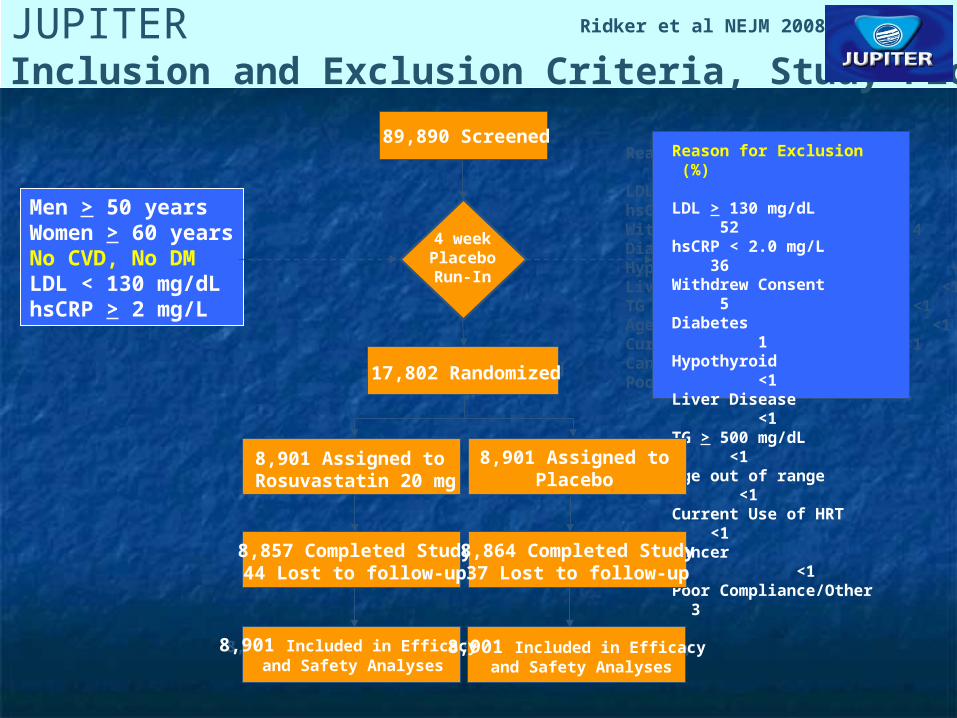
JUPITERInclusion and Exclusion Criteria, Study Flow
89,863 Screened
17,802 Randomized
8,901 Assigned to Rosuvastatin 20 mg
8,901 Assigned toPlacebo
Reason for Exclusion (%)
LDL-C > 130 mg/dL 53hsCRP < 2.0 mg/L 37Withdrew Consent 4Diabetes 1Hypothyroid <1Liver Disease <1TG > 500 mg/dL <1Age out of range <1Current Use of HRT <1Cancer <1Poor Compliance/Other 3
8,600 Completed Study120 Lost to follow-up
8,600 Completed Study120 Lost to follow-up
8,901 Included in Efficacy and Safety Analyses
8,901 Included in Efficacy and Safety Analyses
89,890 Screened
Men > 50 yearsWomen > 60 yearsNo CVD, No DMLDL < 130 mg/dLhsCRP > 2 mg/L
17,802 Randomized
Reason for Exclusion (%)
LDL > 130 mg/dL 52hsCRP < 2.0 mg/L 36Withdrew Consent 5Diabetes 1Hypothyroid <1Liver Disease <1TG > 500 mg/dL <1Age out of range <1Current Use of HRT <1Cancer <1Poor Compliance/Other 3
4 weekPlaceboRun-In
8,857 Completed Study44 Lost to follow-up
8,901 Assigned to Rosuvastatin 20 mg
8,901 Assigned toPlacebo
8,864 Completed Study37 Lost to follow-up
8,901 Included in Efficacy and Safety Analyses
8,901 Included in Efficacy and Safety Analyses
Ridker et al NEJM 2008
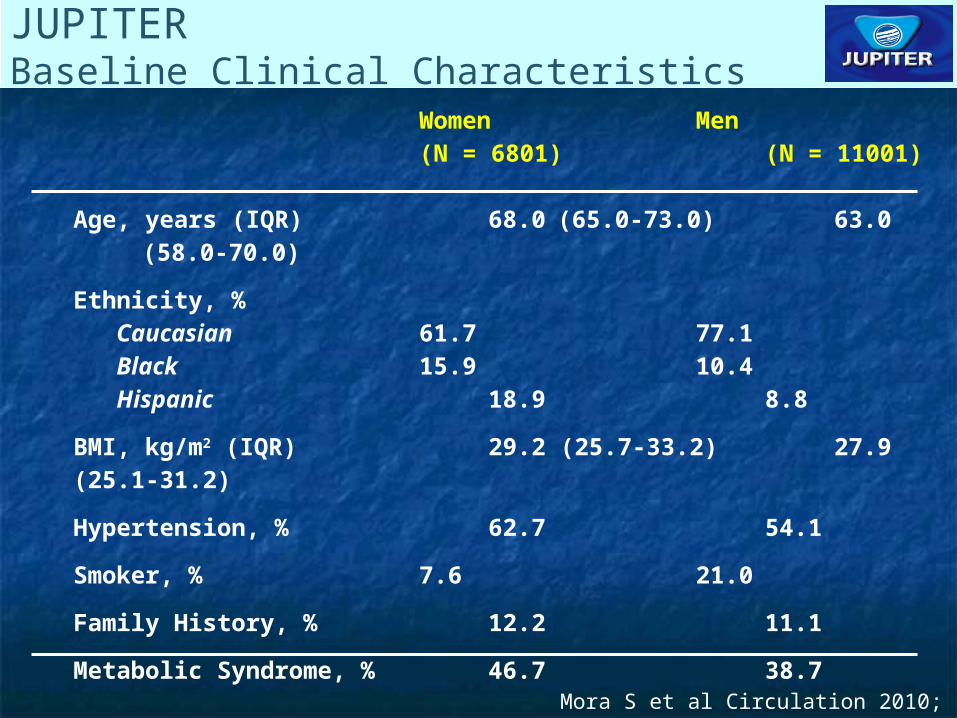
JUPITERBaseline Clinical Characteristics
Women Men(N = 6801) (N = 11001)
Age, years (IQR) 68.0 (65.0-73.0) 63.0 (58.0-70.0)
Ethnicity, % Caucasian 61.7 77.1 Black 15.9 10.4 Hispanic 18.9 8.8
BMI, kg/m2 (IQR) 29.2 (25.7-33.2) 27.9 (25.1-31.2)
Hypertension, % 62.7 54.1
Smoker, % 7.6 21.0
Family History, % 12.2 11.1
Metabolic Syndrome, % 46.7 38.7
All values are median (interquartile range) or %Mora S et al Circulation 2010; 1069
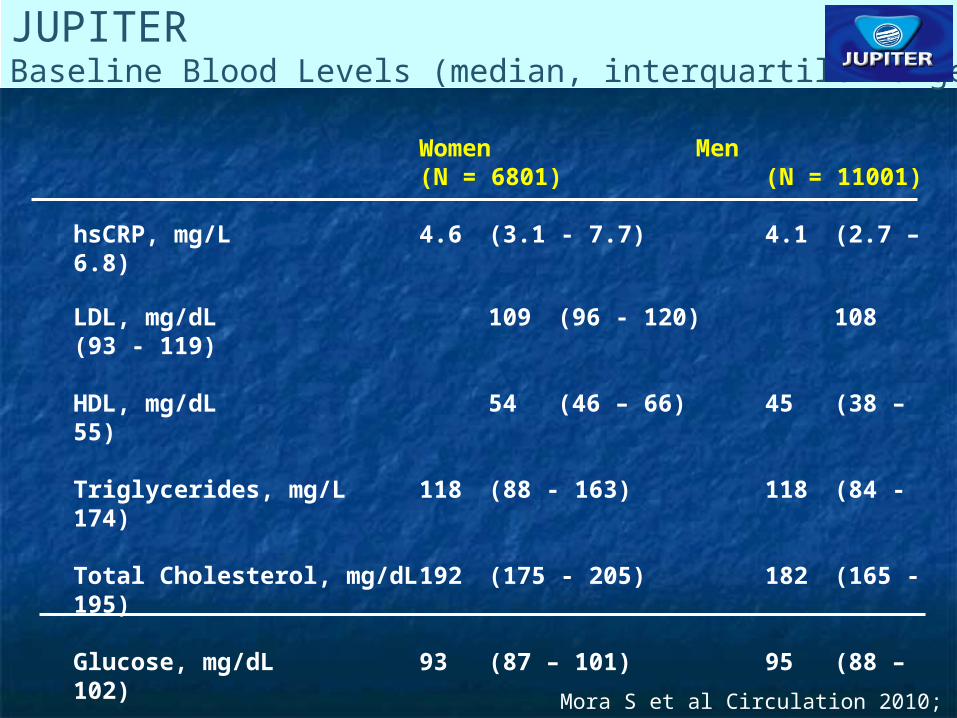
JUPITERBaseline Blood Levels (median, interquartile range)
Women Men(N = 6801) (N = 11001)
hsCRP, mg/L 4.6 (3.1 - 7.7) 4.1 (2.7 – 6.8) LDL, mg/dL 109 (96 - 120) 108 (93 - 119)
HDL, mg/dL 54 (46 – 66) 45 (38 – 55)
Triglycerides, mg/L 118 (88 - 163) 118 (84 - 174)
Total Cholesterol, mg/dL 192 (175 - 205) 182 (165 - 195)
Glucose, mg/dL 93 (87 – 101) 95 (88 – 102)
HbA1c, % 5.8 (5.5 – 6.0) 5.6 (5.4 – 5.9)
All values are median (interquartile range).
Mora S et al Circulation 2010; 1069
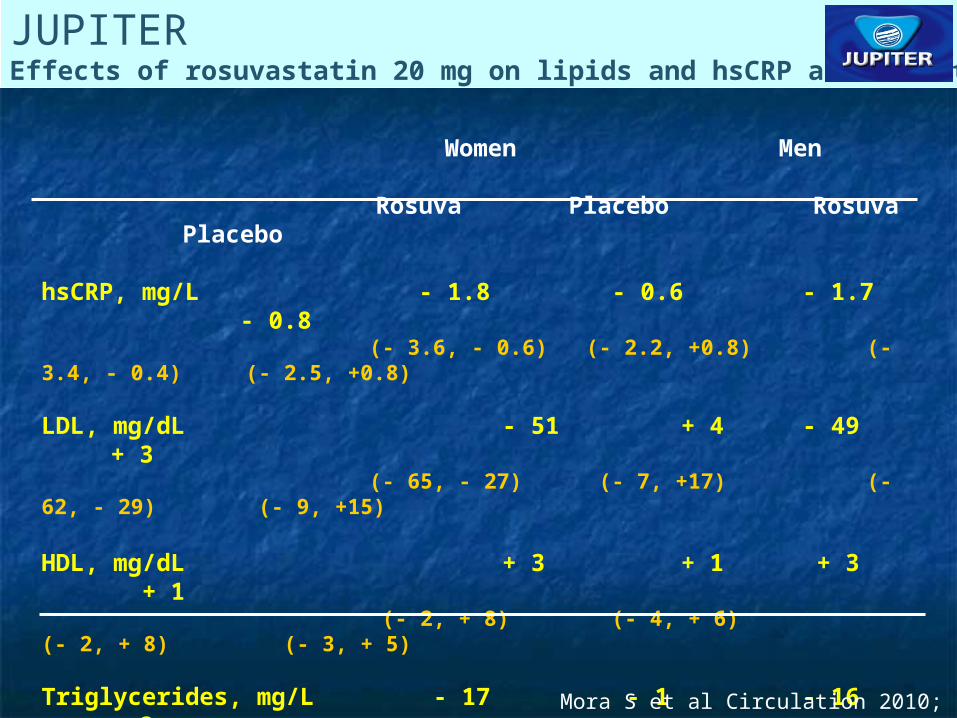
JUPITEREffects of rosuvastatin 20 mg on lipids and hsCRP at 12 months
Women Men Rosuva Placebo Rosuva Placebo
hsCRP, mg/L - 1.8 - 0.6 - 1.7 - 0.8 (- 3.6, - 0.6) (- 2.2, +0.8) (- 3.4, - 0.4) (- 2.5, +0.8)
LDL, mg/dL - 51 + 4 - 49 + 3 (- 65, - 27) (- 7, +17) (- 62, - 29) (- 9, +15)
HDL, mg/dL + 3 + 1 + 3 + 1 (- 2, + 8) (- 4, + 6) (- 2, + 8) (- 3, + 5)
Triglycerides, mg/L - 17 - 1 - 16 + 2 (- 44, + 3) (- 23, +21) (- 50, +7) (- 26, +27)
Total Cholesterol, mg/dL - 51 + 4 - 50 + 3 (- 68, - 27) (- 9, +19) (- 66, - 28) (- 9, +17)
All values are median (interquartile range) change from baseline to 12 months
Mora S et al Circulation 2010; 1069
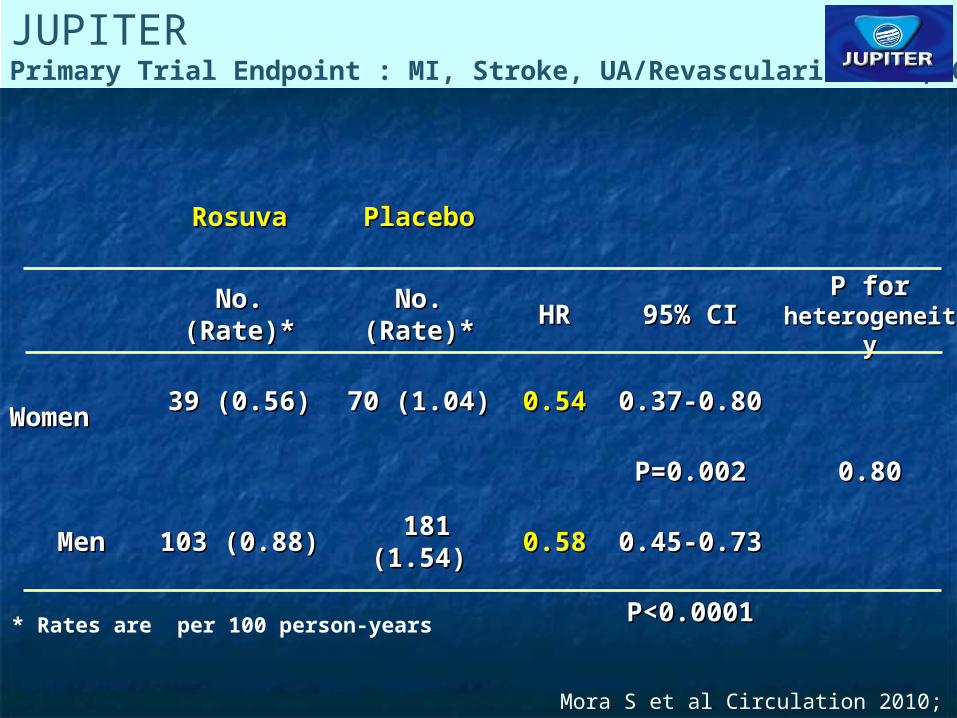
JUPITERPrimary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death
RosuvaRosuva PlaceboPlacebo
No. (Rate)*No. (Rate)* No. (Rate)*No. (Rate)* HRHR 95% CI95% CI P for P for heterogeneityheterogeneity
WomenWomen 39 (0.56)39 (0.56) 70 (1.04)70 (1.04) 0.540.54 0.37-0.800.37-0.80
P=0.002P=0.002 0.800.80
MenMen 103 (0.88)103 (0.88) 181 (1.54)181 (1.54) 0.580.58 0.45-0.730.45-0.73
P<0.0001P<0.0001
* Rates are per 100 person-years
Mora S et al Circulation 2010; 1069
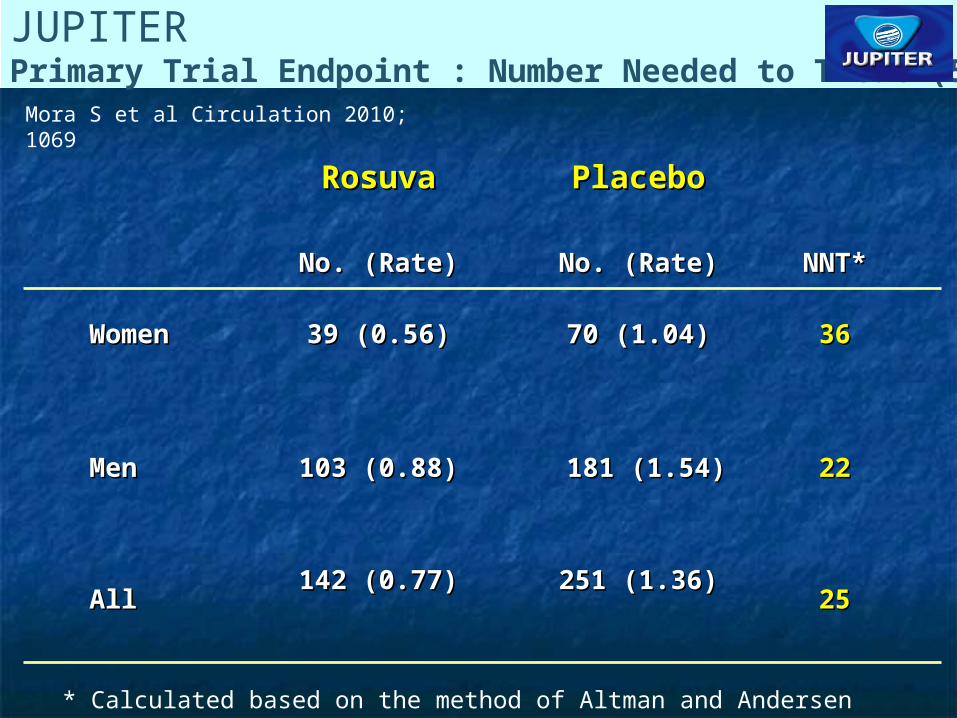
JUPITERPrimary Trial Endpoint : Number Needed to Treat (5-years)
RosuvaRosuva PlaceboPlacebo
No. (Rate)No. (Rate) No. (Rate)No. (Rate) NNT*NNT*
WomenWomen 39 (0.56)39 (0.56) 70 (1.04)70 (1.04) 3636
MenMen 103 (0.88)103 (0.88) 181 (1.54)181 (1.54) 2222
AllAll142 (0.77)142 (0.77) 251 (1.36)251 (1.36)
2525
* Calculated based on the method of Altman and Andersen
Mora S et al Circulation 2010; 1069
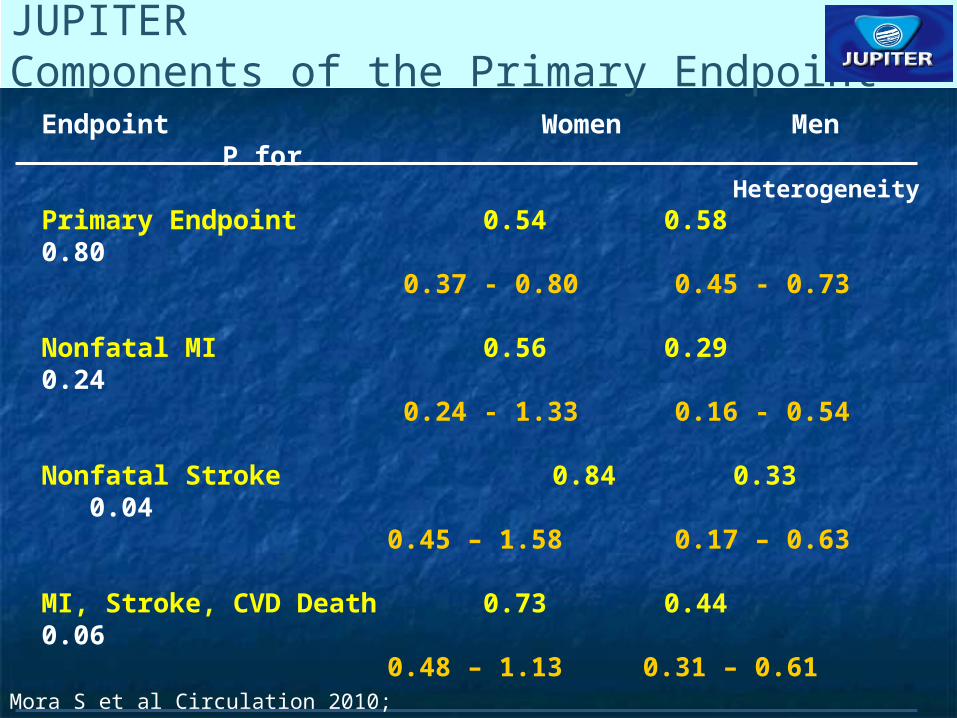
JUPITERComponents of the Primary Endpoint
Endpoint Women Men P for Heterogeneity
Primary Endpoint 0.54 0.58 0.80 0.37 - 0.80 0.45 - 0.73
Nonfatal MI 0.56 0.29 0.24 0.24 - 1.33 0.16 - 0.54
Nonfatal Stroke 0.84 0.33 0.040.45 – 1.58 0.17 – 0.63
MI, Stroke, CVD Death 0.73 0.44 0.060.48 – 1.13 0.31 – 0.61
Revasc/Unstable Angina 0.24 0.63 0.010.11 – 0.51 0.46 – 0.85
All-cause Death 0.77 0.82 0.740.55 – 1.06 0.66 – 1.03Mora S et al Circulation 2010; 1069
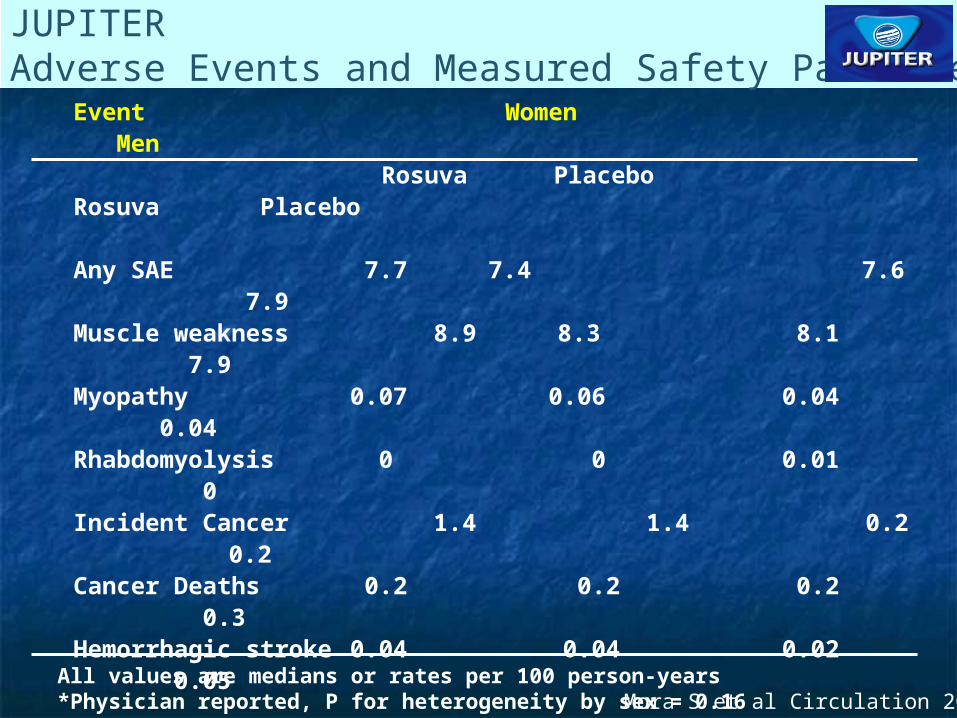
JUPITERAdverse Events and Measured Safety Parameters
Event Women Men Rosuva Placebo Rosuva Placebo
Any SAE 7.7 7.4 7.6 7.9Muscle weakness 8.9 8.3 8.1 7.9Myopathy 0.07 0.06 0.04 0.04Rhabdomyolysis 0 0 0.01 0Incident Cancer 1.4 1.4 0.2 0.2Cancer Deaths 0.2 0.2 0.2 0.3Hemorrhagic stroke 0.04 0.04 0.02 0.05
GFR (ml/min/1.73m2 at 12 mth) 64.1 64.2 71.0 70.5ALT > 3xULN 0.04 0.07 0.16 0.10
Fasting glucose (24 mth) 96 95 99 99HbA1c (% at 24 mth) 5.9 5.9 5.9 5.8Incident Diabetes* 1.5 1.0 1.4 1.2
All values are medians or rates per 100 person-years*Physician reported, P for heterogeneity by sex = 0.16 Mora S et al Circulation 2010; 1069
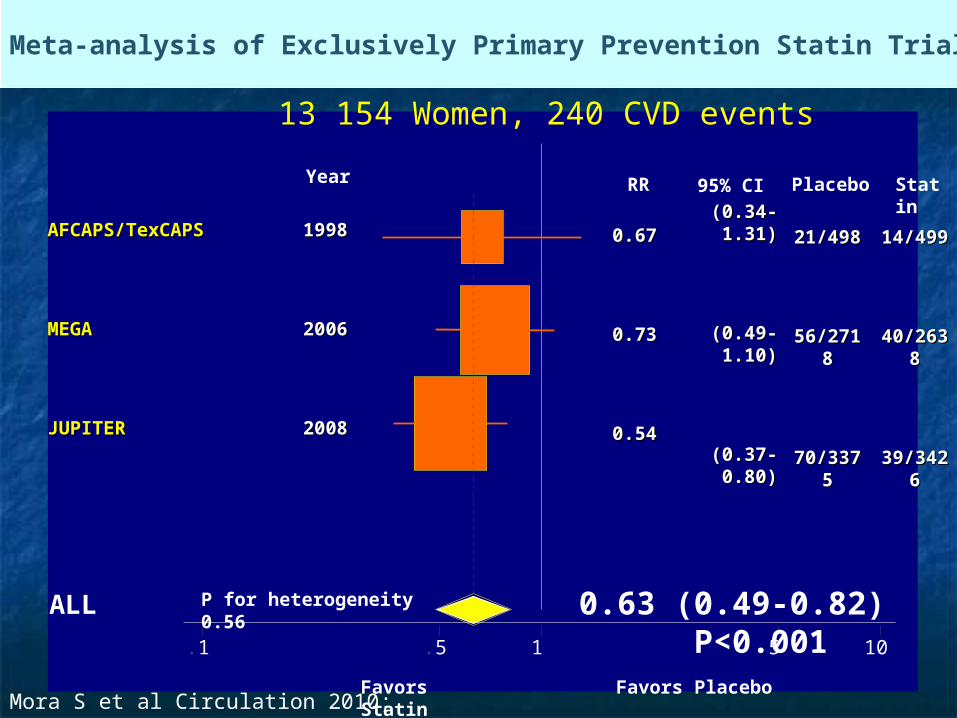
Meta-analysis of Exclusively Primary Prevention Statin Trials in Women
.1 .5 1 5 10
AFCAPS/TexCAPSAFCAPS/TexCAPS 19981998
MEGAMEGA 20062006
JUPITERJUPITER 20082008
0.63 (0.49-0.82) P<0.001P for heterogeneity 0.56ALL
Favors Statin Favors Placebo
(0.34-1.31)(0.34-1.31)
(0.49-1.10)(0.49-1.10)
(0.37-0.80)(0.37-0.80)
21/49821/498
56/271856/2718
70/337570/3375
14/49914/499
40/263840/2638
39/342639/3426
RR 95% CI Placebo Statin
0.670.67
0.730.73
0.540.54
Year
13 154 Women, 240 CVD events
Mora S et al Circulation 2010; 1069
Study Limitations
JUPITER median follow-up 1.9 years (max 5)
Limited long-term safety data for rosuvastatin
Low absolute event rates in women <65 years
Meta-analysis: degree of LDL cholesterol lowering differed
Mora S et al Circulation 2010; 1069
Conclusions – JUPITER sex-specific analysis
Among apparently healthy women with elevated hsCRP and non-elevated LDL cholesterol, rosuvastatin resulted in similar and significant relative risk reduction in CVD compared with men
Women had lower absolute event rates, especially <65 years old
Women had more benefit for revascularization / unstable angina, men had more benefit for stroke
Subgroup analysis suggested women with family history of premature CHD benefit more than those without family history
Higher physician-reported diabetes in women compared with men,but test for heterogeneity by sex non-significant
Overall safety in women similar to men Mora S et al Circulation 2010; 1069
JUPITERConclusions – Meta-Analysis
For primary prevention of CVD in women, statin allocation yielded significant relative risk reduction by one third
This relative risk reduction is similar to prior results in men for primary prevention and men or women for secondary prevention
These findings may have guideline implications for statin therapy in apparently healthy women meeting JUPITER entry criteria, even without high risk Framingham scores
Mora S et al Circulation 2010; 1069

Interventional Procedures Interventional Procedures and Surgeryand Surgery
Higher complication and death ratesHigher complication and death rates Smaller artery sizeSmaller artery size More co-existing illnesses (older at More co-existing illnesses (older at
presentation)presentation) Higher rates of diabetesHigher rates of diabetes More urgent and emergent presentationsMore urgent and emergent presentations Higher incidence of congestive heart failure in Higher incidence of congestive heart failure in
women from diastolic dysfunctionwomen from diastolic dysfunction
Source: Jacobs 2003
Coronary Coronary Revascularization Revascularization
in Women Compared to in Women Compared to MenMen Increased use of PTCA compared to stents, Increased use of PTCA compared to stents,
because of smaller vessel sizebecause of smaller vessel size Decreased rates of glycoprotein IIb/IIIa Decreased rates of glycoprotein IIb/IIIa
inhibitor use, possibly because of increased inhibitor use, possibly because of increased bleeding complications in womenbleeding complications in women
Higher in-hospital mortality for CABG and PCIHigher in-hospital mortality for CABG and PCI Higher rates of vascular complicationsHigher rates of vascular complications Higher transfusion ratesHigher transfusion rates
Source: Jacobs 2003
Revascularization Outcomes Revascularization Outcomes in Women: Improvements in in Women: Improvements in
Recent YearsRecent Years
NHLBI registry data shows improved clinical NHLBI registry data shows improved clinical success rates and lower major complication success rates and lower major complication rates for women undergoing PTCArates for women undergoing PTCA
Retrospective data suggest that women Retrospective data suggest that women have lower mortality rates when undergoing have lower mortality rates when undergoing off-pump CABG, compared to standard off-pump CABG, compared to standard CABGCABG
Source: Jacobs 1997, Petro 2000
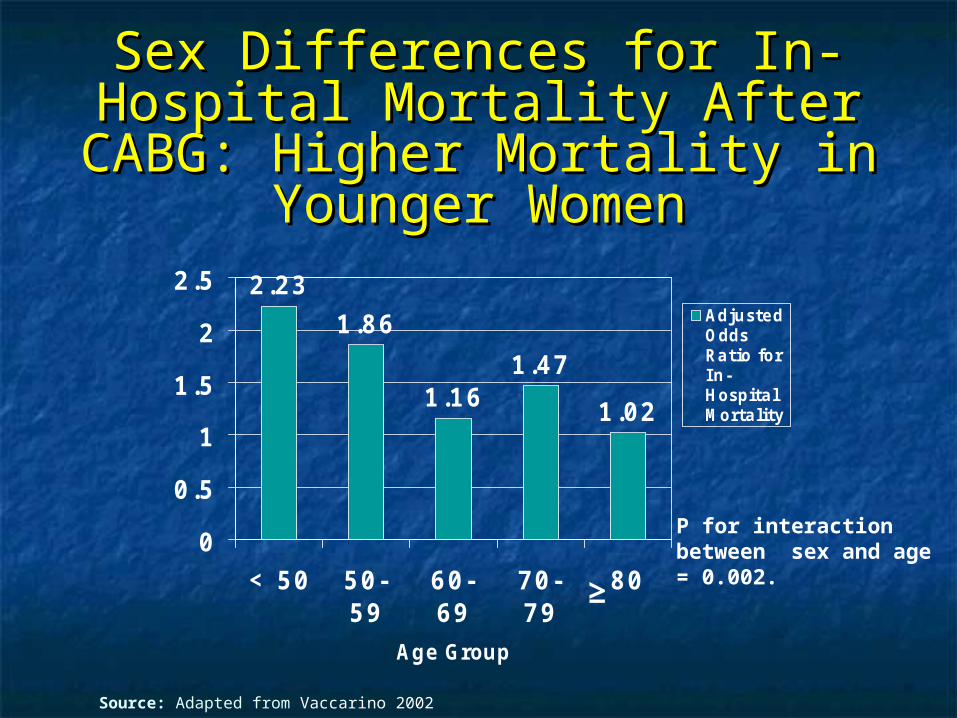
Sex Differences for In-Hospital Sex Differences for In-Hospital Mortality After CABG: Higher Mortality After CABG: Higher Mortality in Younger WomenMortality in Younger Women
2.23
1.86
1.161.47
1.02
0
0.5
1
1.5
2
2.5
< 50 50-59
60-69
70-79
80
Age Group
AdjustedOddsRatio forIn-HospitalMortality
P for interaction between sex and age = 0.002.
≥
Source: Adapted from Vaccarino 2002
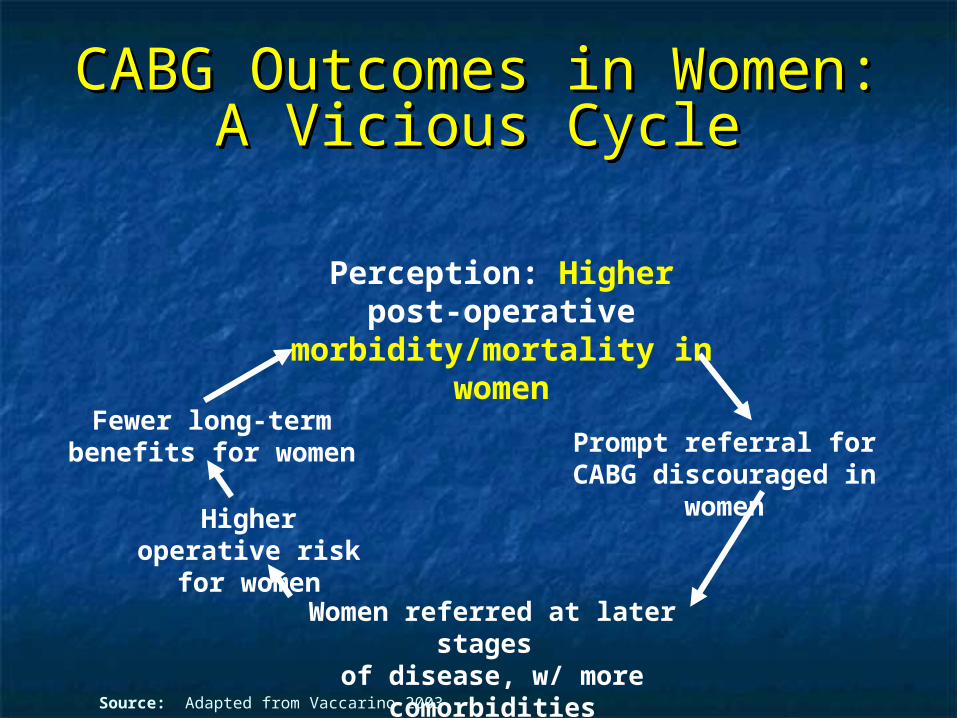
CABG Outcomes in Women: CABG Outcomes in Women: A Vicious CycleA Vicious Cycle
Perception: Higher post-operative morbidity/mortality
in women
Prompt referral for CABG discouraged in women
Women referred at later stages of disease, w/ more comorbidities
Higher operative risk for women
Fewer long-term benefits for women
Source: Adapted from Vaccarino 2003

““Hormone Replacement Hormone Replacement Therapy” Therapy”
Risk-Benefit Balance: 1960’s- Risk-Benefit Balance: 1960’s-1990’s1990’s
Risks
BenefitsCHD Osteoporosis Vasomotor SymptomsGU SymptomsSkin Preservation
Source: Limacher 2002
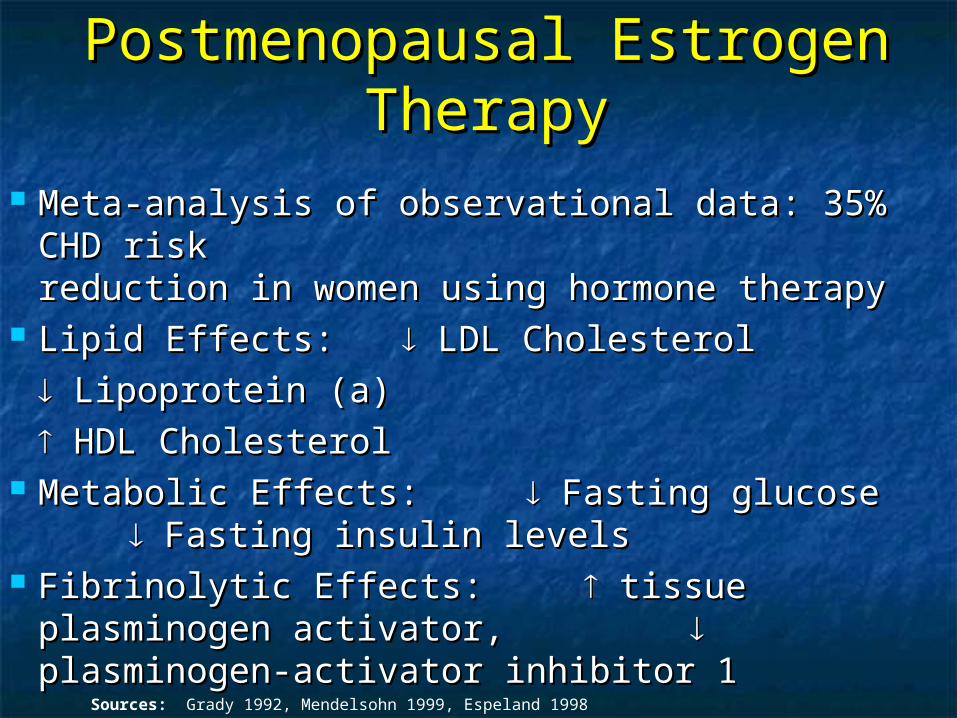
Postmenopausal Estrogen Postmenopausal Estrogen TherapyTherapy
Meta-analysis of observational data: 35% CHD Meta-analysis of observational data: 35% CHD risk risk reduction in women using hormone therapyreduction in women using hormone therapy
Lipid Effects:Lipid Effects: LDL Cholesterol LDL Cholesterol
Lipoprotein (a)Lipoprotein (a)
HDL CholesterolHDL Cholesterol Metabolic Effects: Metabolic Effects: Fasting glucose Fasting glucose
Fasting insulin levels Fasting insulin levels Fibrinolytic Effects: Fibrinolytic Effects: tissue plasminogen tissue plasminogen
activator, activator, plasminogen-activator plasminogen-activator inhibitor 1inhibitor 1 Sources: Grady 1992, Mendelsohn 1999, Espeland 1998
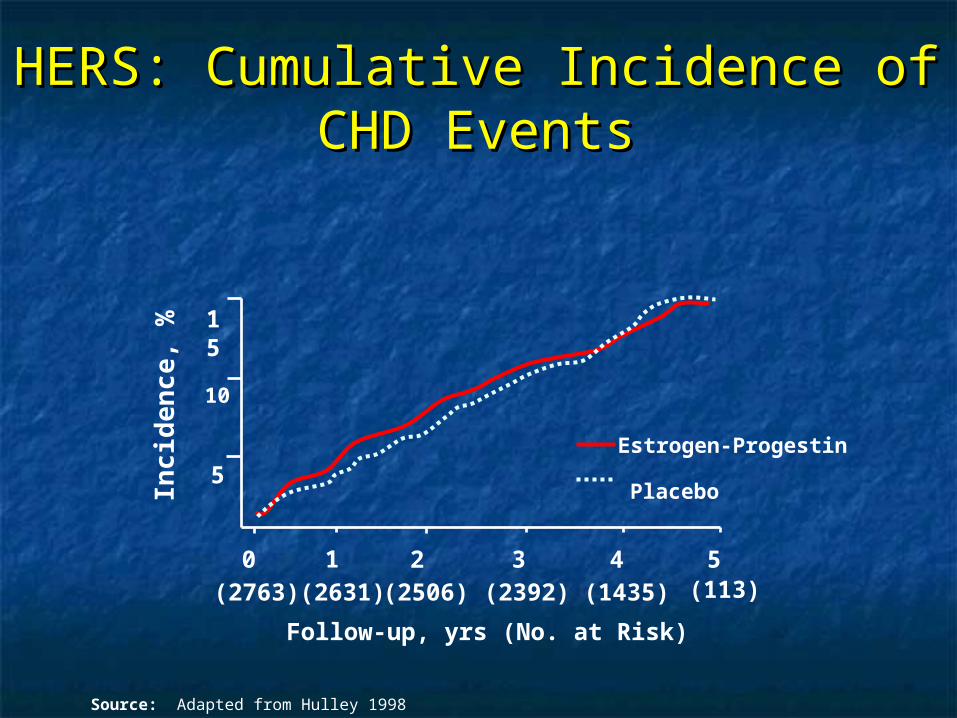
HERS: Cumulative Incidence of HERS: Cumulative Incidence of CHD EventsCHD Events
Follow-up, yrs (No. at Risk)
Inc i
den
ce
, %
0 2 3 4 51
10
5
15
(2763) (2631) (2506) (2392) (1435) (113)
Estrogen-Progestin
Placebo
Source: Adapted from Hulley 1998

Women’s Health Initiative Women’s Health Initiative Estrogen and Progestin Arm: Estrogen and Progestin Arm:
Absolute Excess RiskAbsolute Excess Risk
Excess CHD events: 7/10,000 woman-years
Excess stroke events : 8/10,000 woman-years
Excess pulmonary emboli: 8/10,000 woman-years
Excess invasive breast cancer: 8/10,000 woman-years
Source: Writing Group for the WHI Investigators 2002
Women’s Health Initiative Women’s Health Initiative Estrogen and Progestin Arm: Estrogen and Progestin Arm:
Absolute BenefitsAbsolute Benefits
Fewer colorectal cancers: 6/10,000 woman-years
Fewer hip fractures: 5/10,000 woman-years
Source: Writing Group for the WHI Investigators 2002
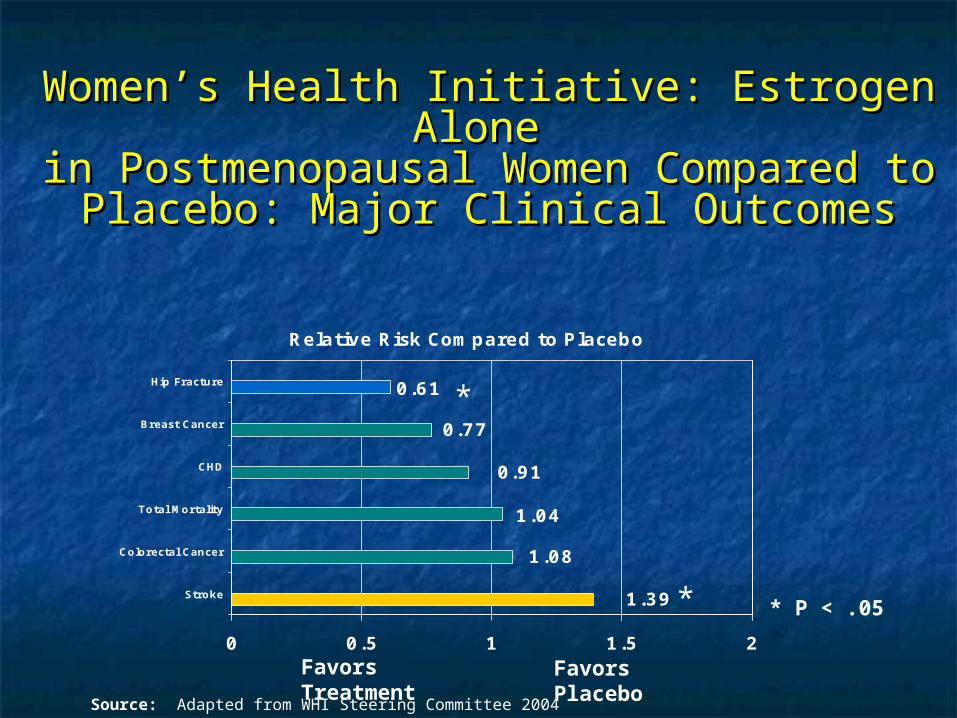
Women’s Health Initiative: Estrogen Alone Women’s Health Initiative: Estrogen Alone in Postmenopausal Women Compared to in Postmenopausal Women Compared to
Placebo: Major Clinical OutcomesPlacebo: Major Clinical Outcomes
0.61
0.77
0.91
1.04
1.08
1.39
0 0.5 1 1.5 2
Stroke
Colorectal Cancer
Total Mortality
CHD
Breast Cancer
Hip Fracture
Relative Risk Compared to Placebo
*
* P < .05*
Favors Treatment Favors Placebo
Source: Adapted from WHI Steering Committee 2004
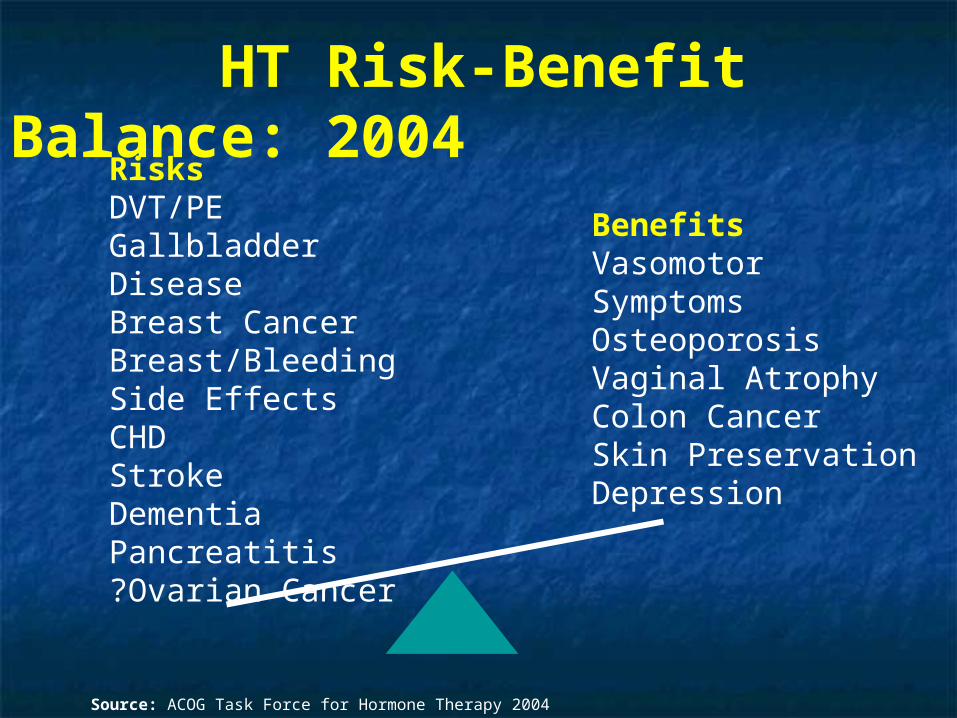
HT Risk-Benefit Balance: 2004
BenefitsVasomotor SymptomsOsteoporosisVaginal AtrophyColon CancerSkin PreservationDepression
RisksDVT/PEGallbladder DiseaseBreast CancerBreast/Bleeding Side EffectsCHDStrokeDementiaPancreatitis?Ovarian Cancer
Source: ACOG Task Force for Hormone Therapy 2004
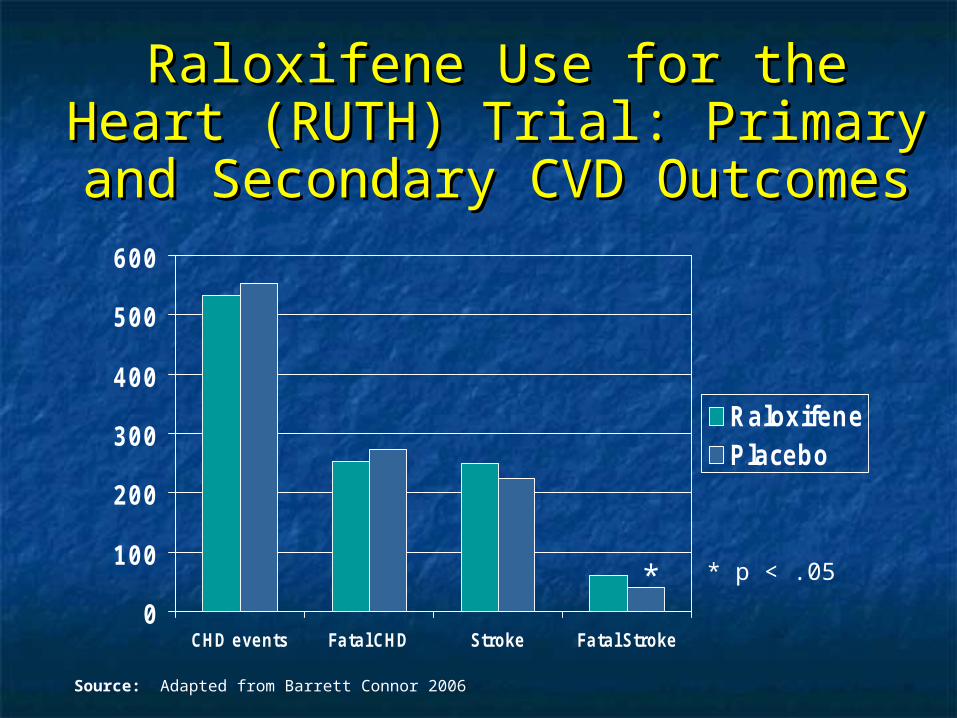
Raloxifene Use for the Heart Raloxifene Use for the Heart (RUTH) Trial: Primary and (RUTH) Trial: Primary and Secondary CVD OutcomesSecondary CVD Outcomes
0
100
200
300
400
500
600
CHD events Fatal CHD Stroke Fatal Stroke
RaloxifenePlacebo
Source: Adapted from Barrett Connor 2006
* * p < .05
Interventions that are not Interventions that are not useful/effective useful/effective
and may be harmful for the and may be harmful for the prevention prevention
of heart diseaseof heart disease Hormone therapy and selective Hormone therapy and selective
estrogen-receptor modulators estrogen-receptor modulators (SERMs) should not be used for the (SERMs) should not be used for the primary or secondary prevention of primary or secondary prevention of CVDCVD
Source: Mosca 2007
Menopausal Hormone Therapy, Menopausal Hormone Therapy, SERMs and CVD: Summary of Major SERMs and CVD: Summary of Major
Randomized TrialsRandomized Trials Use of estrogen plus progestin associated with a Use of estrogen plus progestin associated with a
small but significant risk of CHD and strokesmall but significant risk of CHD and stroke Use of estrogen without progestin associated with Use of estrogen without progestin associated with
a small but significant risk of strokea small but significant risk of stroke Use of all hormone preparations should be limited Use of all hormone preparations should be limited
to short term menopausal symptom reliefto short term menopausal symptom relief Use of a selective estrogen receptor modulator Use of a selective estrogen receptor modulator
(raloxifene) does not affect risk of CHD or stroke, (raloxifene) does not affect risk of CHD or stroke, but is associated with an increased risk of fatal but is associated with an increased risk of fatal strokestroke
Source: Hulley 1998, Rossouw 2002, Anderson 2004, Barrett-Connor 2006

ConclusionsConclusions
♥ Gender differences exist in diagnosis, treatment, and prognosis of CHD
♥ Knowledge of gender differences is essential for appropriate therapy
♥ Evidence-based guidelines provide a new framework for prevention and treatment of cardiovascular disease in women

THANK YOUTHANK YOU