1 pwr! retreat 2013 becky farley, phd, ms, pt founder/executive officer [email protected] sally...
TRANSCRIPT

1
PWR! Retreat2013
Becky Farley, PhD, MS, PTFounder/Executive [email protected]
Sally Michaels, PT, CCMChief Operations Officer
Parkinson
Wellness
Recovery
Empowerment, Education, Exercise, Enrichment
2
Sally Michaels, PT, CCMChief Operations Officer
EXERCISE REVOLUTIONISTS
Becky G. Farle
y, PhD, M
S, PT
Founder/CEO

3
Becky Farley, PhD, MS, PT Sally Michaels, PT, CCMFounder/Executive Officer Chief Operations [email protected] [email protected]
Parkinson Wellness Recovery
We believe people with PD can get BETTER and STAY BETTER with exercise!
501(c)(3) nonprofit organization
Vision
A community where individuals with Parkinson disease have access to “Exercise as Medicine.”

4
Real worldimplementation
Via thePWR! Project
Cutting-edgeresearch in exercise &
neuroplasticityExercise4BrainChange®
teaching principles
PWR! Gym
PWR! Clinicians & Fitness Professionals
The PWR! Model:
Model Community Neurofitness Center of Excellence
Specialty Exercise Events

PWR! AcademyPD-Exercise Experts
PWR!FitnessTraining
PWR!ClinicianTraining
PWR! MOVESPWR! Circuit
Introductory PWR! Events
PWR! RetreatMay 19-25
PWR! TrainMay 27-31
PWR! GymCommunity
Model NeuroFitnes
s Center of Exercise
Excellence Tucson, AZ
Individuals with PDCare Partners & CommunityEducate, Empower, Exercise,
Enrich
Components of the PWR! Project
Developing the networks and infrastructure for implementing exercise as medicine

6
www.pwr4life.org
Model Community NeuroFitness Center of Excellence
for Parkinson ExerciseTucson, AZ
Implementing “Exercise as Medicine”
7
PWR! RETREAT EXERCISE TEAM
Amanda Borneman – Wisconsin
Val Carter – Arizona
Amy Chan – Ohio
John Dean – Colorado
Josefa Domingos – Portugal
Stephanie Dunn – Colorado
Shana Gatschet – Kansas
Eleanor Hagan – New Jersey
Nancy Hillmer – Colorado
Amy Marriott – North Carolina
Claire McLean – California
Nancy Nelson – Oregon
Sarah Stahr – Ohio

8
PWR! RETREAT FACULTY
Margaret Anne Coles, OTR/L, MQI
Don Fiore
Catherine Genzler, E-RYT
Naomi Salins, MD
Holly Shill, MD
Tom Viviano

9
Exercise as Medicine for Parkinson disease
Exercise is a tool to optimize brain health, repair, and FUNction
Becky G. Farley, PhD, MS, [email protected]
WWW.PWR4LIFE.ORG

10
Exercise as Medicine Objectives
1. What does it mean?2. What is the evidence supporting new
paradigms for individuals with Parkinson disease?
3. What does it look like in action for individuals with Parkinson disease?
4. What can you do today?5. Exercise4BrainChange techniques LIVE
DEMO

Exercise as Medicine?What does it mean?
11
Exercise promotes• Brain health/protection• Brain repair• Brain adaptation• Behavioral recovery……..
from
the
INSID
E!

12
How does exercise change the brain?
At a structural level by making more & better…
Neuron
Synapses
Neurotransmitters
Blood Vessels

13
Molecular, Metabolic and Physiological brain changes also occur!
Improves glucose utilization Improves immune system Suppresses oxidative stress Stabilizes calcium homeostasis Reduces inflammation Improves mitochondrial function/ATP
production Increases growth/survival factors,
neurotransmitters
Cotman & Berchtold 2002; Kleim JA, Jones TA, & Schallert T. 2003
Bottom LINE:
Exercise promotes redundant, healthy, efficient brains:protect vulnerable neurons from stress & toxinsenhance recovery of damaged circuitshelp brains adapt to do more with less!!
Exercise targets multiple systems!!! Motor/Cognitive/Emotional/Autonomic

Potential motor/nonmotor targets of exercise!
Prevention of cardiovascular complicationsArrest of osteoporosisImproved cognitive functionPrevention of depressionImproved sleepDecreased constipationDecreased fatigueImproved functional motor performanceImproved drug efficacyOptimization of the dopaminergic system
Speelman, AD et al. Nature Reviews Clinical Neurology 7, 528-534 (September 2011)

What about exercise in a neurodegenerative disease?
Parkinson disease is the only chronic neurodegenerative disease for which there are
highly effective symptomatic therapies.
MedicationDeep Brain Stimulation
Exercise

17
2
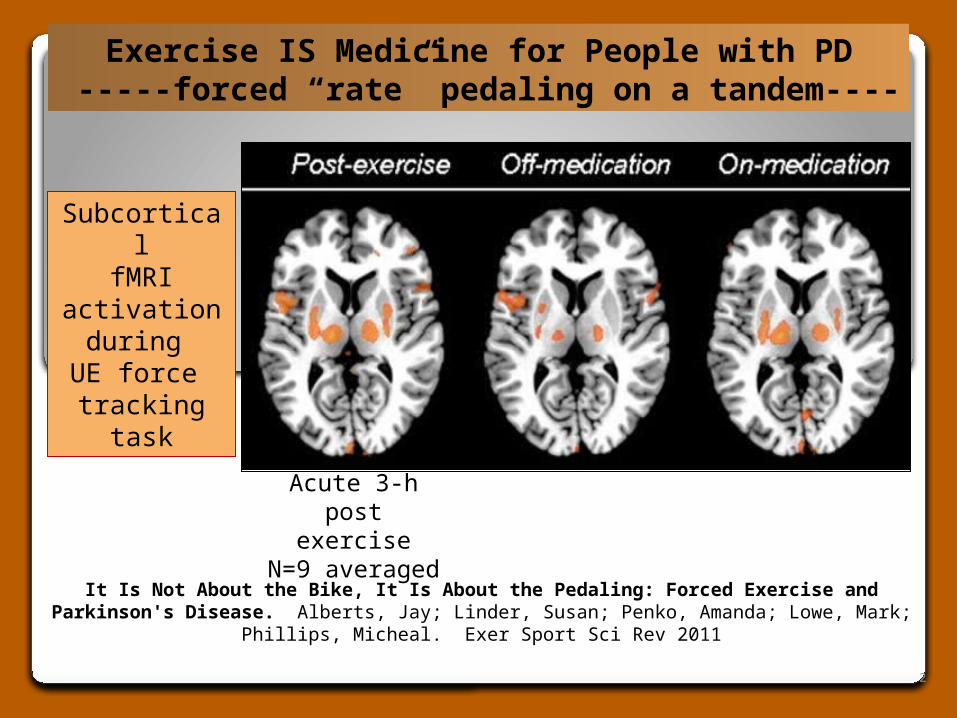
It Is Not About the Bike, It Is About the Pedaling: Forced Exercise and Parkinson's Disease. Alberts, Jay; Linder, Susan; Penko, Amanda; Lowe, Mark; Phillips, Micheal. Exer
Sport Sci Rev 2011
Exercise IS Medicine for People with PD -----forced “rate” pedaling on a tandem----
Acute 3-h post exercise
N=9 averaged
SubcorticalfMRI
activation during
UE force tracking task

19
Progressive Aerobic Training - Neural Priming Promotes
Brain/Muscle interactions
Turns on attentional/working memory systems
Increases motor output
Skill Acquisition Essentials - Learning
Promotes structural restoration, reorganization
Underlies long term behavioral changes
Automaticity
WHAT you do and HOW you do it MATTERS!Essential Components for Optimal Brain Change
“ready” to move & learn

20
Exercise4BrainChange in ACTIONProgressive Aerobic Training

21

22
Is vigorous exercise neuroprotective in people with PD?
Ahlskog1 Je. Neurology 2011;77:288-294
CONCLUSIONS - Progressive Aerobic Exercise Ongoing vigorous exercise and physical fitness should be highly encouraged. PD physical therapy programs should include
structured, graduated fitness instruction and guidance for deconditioned patients with PD. Levodopa and other forms of dopamine therapy
should be used to achieve maximum capability and motivation for patients to maintain fitness.

Skill Acquisition Essentials Applied to PD
High Physical Effort – Forced Use◦Push beyond self selected effort!◦ACTIVATE for FUNCTIONHigh Attentional Focus ◦Train awareness of movement/actionsHigh Cognitive Engagement◦Progressively challenge difficultyHigh Emotional Engagement◦Novel/reward-based/meaningful practice
23
Target PD-Specific deficits – Integrate exercise programs or techniques that are
research-based and neuroplasticity-principled
Practice high effort whole body BIG movements and action sequences
Foundation for function, all practice Spinal flexibility Agility (coordination/balance training) Augment proprioceptive feedback Kinesthetic awareness training High effort rate or strength training Dual Task Training Dance, Tai Chi, Boxing, Qigong, Yoga
Use it or lo
se it!
Use it and Im
prove it!
PWR!
MOVES

25
Exercise4BrainChange in ACTIONACTIVATION for FUNction.

26
Social Support/Stress Reduction/Optimism/Empowerment

27
Unmet needsForced Use Training That Targets Multifactorial Deficits
Bradykinesia, rigidity, sensory, environmental, attentional, cognitive, emotional, and medication
Postural Instability Inadequate anticipatory and reactive postural responses
◦ Delayed stepping responses/abnormal righting
Freezing “glued to floor” feeling Early indicators: hesitation, anxiety, dual task interference,
incoordination, hastening, marked shuffling, fear of falling

How you practice matters!
Forced TurningUse it and Improve it
Anti-Freezing

29
Postural Control Progressive Difficulty with success and no fear.

Recent advances in basic neuroscience:
Animal models with PD show response to exercise varies with phase of disease
30
1. Preclinical phase — Neuroprotection
2. Early/Moderate phase — Neurorepair
3. Late phase — Adaptation

Brain Change in Parkinson disease – animal models
100
0
Dia
gn
osi
s
Refe
rral
to
thera
pyNeuroprotectio
n
Adaptation
Time (years)
Moto
r S
ymp
tom
s 1
st
Ap
pear
Neurorepair
% D
op
am
i ne n
eu
ron
s
Preclinical Early/Moderate Advanced
DA level threshold
Window of disease reversibility

32
Indirect Evidence for Neuroprotection in People With Parkinson’s Disease.
Epidemiological, Anecdotal & Experimental
Direct evidence in healthy seniors for improved brain health with aerobic exercise
Regular, moderate to vigorous exercise in midlife–lowers risk for developing PD.
Exercise may increase survival rate. Higher cognitive scores associated with greater
physical fitness Regular exercise reduces the severity of
motor/nonmotor symptoms and improves function with 3-6 month retention.
Chen et al. 2005; Hale et al. 2008; Gray et al. 2009; Bilowit 1956; Sasco et al.1992; Palmer et al. 1986; Archer et al. 2011;
Reuter et al. 2011

33
The Dopamine system is more efficient with exercise in human PD too!!!
• Noisy circuits are silenced• DA receptors are upregulated• Medications are more effective
or optimized!
Direct Evidence forNeurorepair in Human PD
Fisher et al. 2004; 2008; Petzinger et al. 2007; Vuckovic et al. 2010; Fisher et al., submitted!!!
34
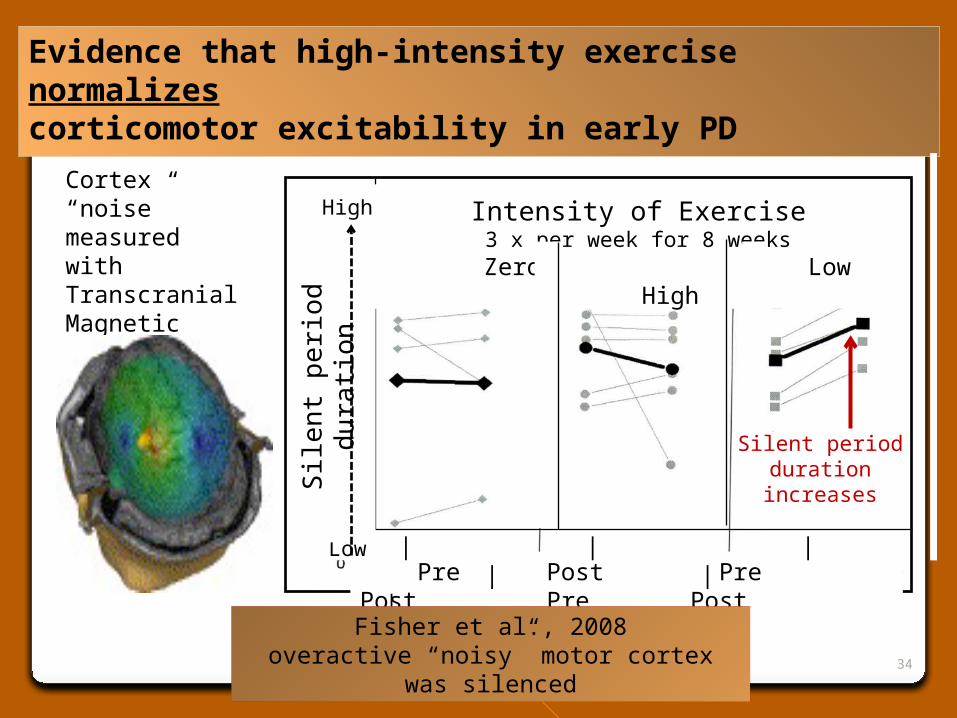
Evidence that high-intensity exercise normalizes corticomotor excitability in early PD
Cortex “noise” measured with Transcranial Magnetic Stimulation (TMS)
Pre Post Pre Post Pre Post
Intensity of Exercise3 x per week for 8 weeks
Zero Low High
High
Low
Sile
nt p
erio
d d
ura
tion
| | | | | |
Silent perioddurationincreases
Fisher et al., 2008overactive “noisy” motor cortex was silenced
35
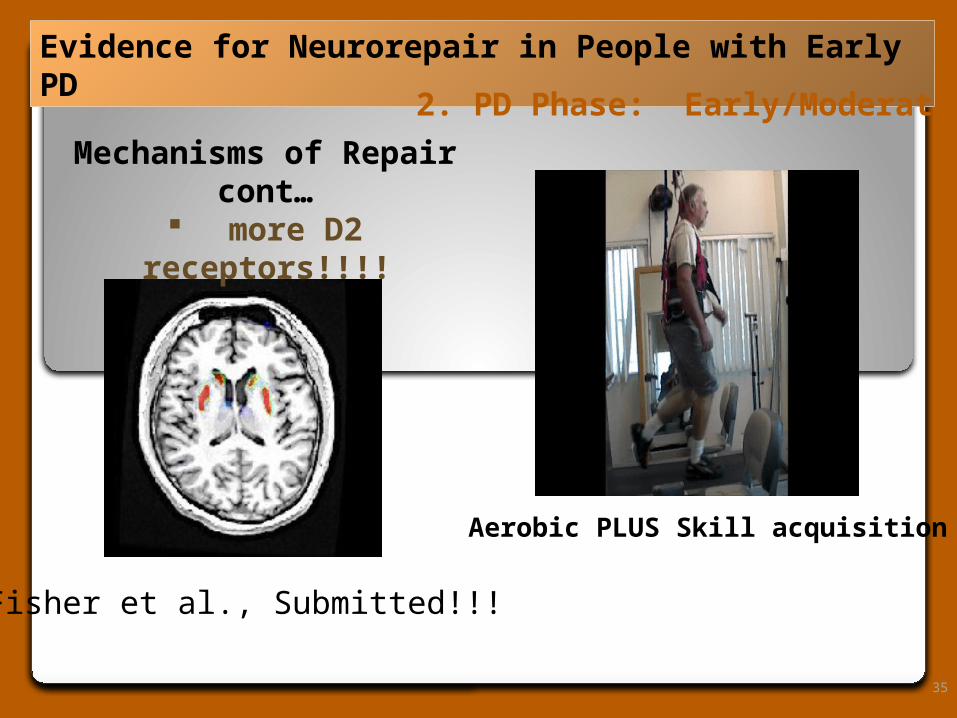
Evidence for Neurorepair in People with Early PD
Mechanisms of Repair cont…
more D2 receptors!!!!
Fisher et al., Submitted!!!
2. PD Phase: Early/Moderate
Aerobic PLUS Skill acquisition

36
Effectiveness of Intensive Inpatient Rehabilitation Treatment on Disease Progression in Parkinsonian Patients: A Randomized Controlled Trial With 1-Year Follow-up.
Giuseppe Frazzitta, MD et al. Neurorehabi Neural Repair, Aug 15, 2011
Evidence that annual intensive bouts of exercise augment the effects of medication in human PD
start After 4 weeks IRT
end of year
After 4 weeks IRT
start end of year
0
5
10
15
20
25
30
IRT (n = 25) CONTROL (n = 25)
Un
ifie
d P
D R
atin
g S
cale
III
Differences statistically different (p < 0.0001)dashed lines = not significant
50*mg/d less
30*mg/d more
* Time X Group P = 0.004

37
High IntensityTreadmill Training in ADV PD

Timing matters: early is better than later Intensity matters – dosage (freq/dur/work)
Forced Use – Beyond self selected effort Intermittent bouts Vigorous aerobic training
Specificity matters – Make it PD-specific “use it or lose it” or “use it and improve it”
Continuous (threshold) of exercise to sustain Inactivity/Stress is pro-degenerative Exercise may optimize response to meds
Implications to Human
38
Response to exercise, dosage, specificity of training may be different across disease
severity.

Time for new Paradigms!!!
Exercise4BrainChange™
PWR! Project
Early
Intervention
Continuous
Access
PARKINSON EXERCISE REVOLUTION !!!
Forced use
Intermitten
t intensive
bouts for
LIFE!
Optimal M
eds
Neuroplastic
ity-principled

What you can do Today!• Find a PWR! PD-exercise expert.
• Start exercise at diagnosis and go regularly. Just like medicine, get your dosages checked.
• Get annual INTENSIVE bouts of 1:1 PD-specific rehabilitation training every year at a minimum.
• Ask for a reassessment/tune-up every 3-6 months before you start to have problems. Don’t wait!
• Participate in community exercise and enrichment programs all the time!• Advocate for change!

41
PW
R!
Han
ds
PW
R!
Rea
ch
PW
R!
UP
PW
R!
Ro
ck
PW
R!
Twis
t
PW
R!
Ste
p
PW
R!
Vo
ice
PWR! MOVES™
NOT JUST EXERCISE. PD-specific skill training for FUNction.

42
Bui
ld C
ompl
exity
Ret
rain
Aut
omat
icity

Skill Acquisition Essentials Applied to PWR! MOVES
◦High Physical Effort – Forced Use Push beyond self selected effort! Train bigger/faster whole body movements and action sequences
◦High Attentional Focus Train awareness of movement/actions
◦High Cognitive Engagement Progressively challenge difficulty
◦High Emotional Engagement Novel/reward-based/meaningful practice
43
PWR!
MOVES

44
What are PWR! MOVES
Level 1 – Get ready to move; slow, guided movement and imagery; sustained active stretch; increase confidence; focus attention
Level 2 – increase effort across the entire motor system/ACTIVATE; 7+ effort
Level 3 – Challenge complexity, postural control, challenge attention
Level 4 – decrease predictability, increase cognitive load, reduce reliance of vision

45
PD-specific exercise that targets the motor/sensory/cognitive/emotional symptoms. ◦ Relearning! Use it or lose it. Use it and improve it.
Foundation skills in PD target the primary DA dependent symptoms of bradykinesia and rigidity.◦ Rhythmical, whole body, high effort large amplitude
movements for maximal activation and re-calibration of normal movement awareness.
Add Difficulty/Complexity to address other symptoms related to the cognitive aspects of movement (agility/anticipatory & reactive postural responses; environmental adaptation; divided attention for multi-tasking).◦ Integrate into everyday living - recreation, sports, chores,
work, functionFUNction - Motivate/Reward-based/Empower/Educate
Exercise4BrainChange!

46
Progressive Multidirectional Stepping – PD-specific Skill acquisition training
8 sets of 1 rep each direction
Right Forward x1Right SidewardRight Backward
Left ForwardLeft SidewardLeft Backward
Model; Mental Imagery; Add Auditory Cues; Add/change secondary tasks; Increase complexity of motor sequence
1 set of 8 reps each direction
Right Forward x8Right SidewardRight Backward
Left ForwardLeft SidewardLeft Backward

47
Progressive Multidirectional Stepping – Skill acquisition training
8 sets of 1 rep each direction
Right Forward x1Left ForwardRight SidewardLeft BackwardRight BackwardLeft Backward
Model; Mental Imagery; Add Auditory Cues; Add/change secondary tasks; Increase complexity of motor sequence.
8 sets of 1 rep each direction
Right Forward x1Left SidewardLeft BackwardRight SidewardLeft ForwardRight Backward

48
www.pwr4life.org