accountable care organizations
DESCRIPTION
Accountable Care Organizations. Michael E. Speer, MD Vice Chair, TMA Committee on ACOs & Lee Spangler, JD TMA VP, Medical Economics. Motivations…. - PowerPoint PPT PresentationTRANSCRIPT

Accountable Care OrganizationsMichael E. Speer, MD
Vice Chair, TMA Committee on ACOs &
Lee Spangler, JDTMA VP, Medical Economics
“The health care delivery system is in the process of transformation from an emphasis on the freedom of individual physicians to practice as they see fit, to a systematic focus on assessment and accountability…. [P]roviders of medical care becoming accountable to patients and their employer/insurer representatives for the quality, effectiveness, and cost of care.”
-- James Lynn, Chairman of Aetna Life & CasualtyThe Promise of Managed Care: An Insurer’s Perspective Health Affairs, Winter 1991Health Affairs, Winter 1991
Motivations…

• This is the failed promise of managed care!• But it is the Holy Grail for employers and payors.
• Business has always moved to better quality for less cost – it is what consumers want and demand.• Better quality is achieved through minimizing variability
in processes.• Low cost is achieved through economies of scale.
• Reduce unit cost as the size increases.*Medicine is a handiwork industry –
custom treatment plans for patients
Motivations…

Motivations…
Motivations
• Mark McClellan, MD, PhD
• John Bertko
• Michael Chernew, PhD
• Stephen Shortell, PhD
• Joseph Antos, PhD
• Dana Goldman, PhD
• Elizabeth McGlynn, PhD
• Mark Pauly, PhD
• Leonard Schaeffer
• David Cutler, PhD
What People? Co-authors of Bending the Cost Curve

• Not just business – government desires more care and better care for less money.• Patient Protection and Affordable Care Act (PPACA);
Acute Care Episode (ACE) demonstration projects • United Kingdom National Health Service: “Liberating
the NHS” Whitepaper (July 2010).• Patients must be first and outcomes improved.
• Physicians must be accountable for results and gains in efficiency must occur.• Develop and implement quality standards.
• Risk adjusted assessment of physicians compared to peers.
Motivations…

• 18 months ago, few physicians were familiar with the ACO model. • Google search for “accountable care organization” =
300,000+ hits• ACOs pre-date PPACA:
2006: MedPac began writing and meeting about ACOs. 2009: Texas: proposed legislation to reform Medicaid and ERS
delivery/payment systems by relying on ACO concepts. Colorado, Vermont and Massachusetts legislatures are advancing
ACO model in Medicaid. MGMA & Dartmouth/Brookings: work with large systems to foster
model in private arena via direct contracting opportunities
Background/History
• Accountability movement not new — 40+ years
• Efforts to improve accountability began well before passage of ACA, but the new law accelerated interest
Background/History
• New wave of multipronged, complimentary efforts to revamp payment and delivery system: New CMS Center for Medicare and Medicaid
Innovation Test new payment and delivery models
Pilots test bundled payments, global capitation and other models within Medicare and Medicaid
Research and promotion of evidence-based medical treatments
Funding to support the medical home model and “community health teams”
Background/HistoryBackground/History

What is an ACO

• Keep in mind … the ACO doesn’t happen unless physicians are involved. A facility (i.e., hospital) can’t do it alone.
• As you evaluate the agreement and the structure of the offers made to you or that you will develop – HAVE AN EXIT STRATEGY.• How do I terminate or dissolve if the prospects are
poor or the measurements are inappropriate/adverse?• What are my duties if the ACO dissolves?
• Who owns the patient lists and medical records?
• Non-Compete clauses
What is an ACO
• Race to the bottom??• Quality measures along with the economic incentives
prevent the cheapest, worst, care.
• Quality measures must be met before a bonus is paid.
• If quality measures aren’t met – anticipate penalties.
• Goal: achieve the best value for the dollar.
What is an ACO
• Race to the bottom??• Difficulty measuring value – quality measures offers a tool.
• Business favors this concept.
• Business won’t pay for a “widget” that fails to meet specifications.
• Attempt to apply specifications to practice of medicine.
• Physician ranking systems already in place have weaknesses.
What is an ACOWhat is an ACO
What is an ACO
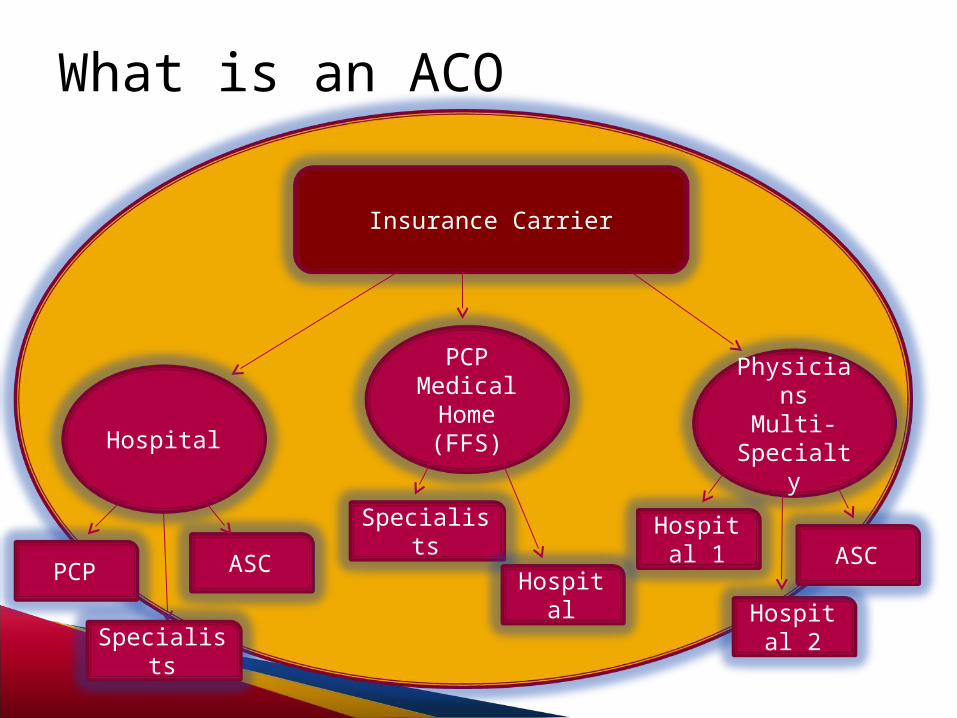
Insurance Carrier
PCPMedical Home(FFS)
Specialists
Hospital
Hospital
PCP
Specialists
ASC
Physicians Multi-
Specialty
Hospital 1
Hospital 2
ASC
• Federal PPACA• Pediatric ACO demonstration project (Sec. 2706).
• A state medicaid project for which the Secretary shall establish guidelines to ensure that the quality of is not less than the quality of care that would have otherwise been provided. Also a participating State, in consultation with the Secretary, shall establish an annual minimal level of savings that must be reached by an ACO in order for the incentive to be paid. 2012-2016.
• The State must apply to be part of this project. ACO participation is dependant on the State Medicaid Program’s decision to participate.
• Texas Health and Human Services Commission indicated it will pursue the pilot.
What is an ACO

• Federal PPACA• “A state option under Medicaid to provide a health home for
individuals with chronic conditions” is part of the latest rulemaking.
• “The term ‘health home’ is …a designated provider … or a health team selected by an eligible individual with chronic conditions to provide health home services.”
• “States pay the designated provider … for the provision of health home services.” • A state specifies in the State plan amendments to Medicaid the
methodology it will use to determine payment.• Payments may be tiered to reflect the severity of the patient’s
condition or the “provider’s” capability.
What is an ACO

• Federal PPACA• The Pediatric ACO must “allow qualified pediatric medical
providers to be recognized as an ACO… in the same manner as an ACO under the Medicare…” Shared Savings Program.
• Medicare Shared Savings Program (Sec. 3022).• Promote accountability for a patient population
• Coordinate items and services under parts A and B; and
• Encourage “high quality and efficient service delivery” and investment• Infrastructure; and
• Redesigned care processes.
What is an ACO
• Medicare Shared Savings Program (Sec. 3022).• This section defines ACOs – Who may form ACOs?
• Professionals in group practice arrangements.
• Networks of individual practices of ACO professionals.
• Partnerships or joint venture arrangements between hospitals and ACO professionals.
• Hospitals employing ACO professionals.
• Such other groups of providers of services and suppliers as the Secretary determines appropriate.
What is an ACO

• Medicare Shared Savings Program (Sec. 3022).• What does PPACA believe an ACO should look like?
• Be accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to it.
• Enter into a 3-year contract with the government.
• Have a formal legal structure permits it to receive and distribute payments.
• Sufficient primary care “professionals” sufficient for the number of beneficiaries in the ACO which is at least 5,000 beneficiaries.
What is an ACO

• Medicare Shared Savings Program (Sec. 3022).• What does PPACA believe an ACO should look like?
• Have a leadership structure that includes clinical and administrative systems.
• Have defined processes to promote evidence-based medicine and patient engagement, report on quality and cost measures, and coordinate care.
• Be patient-centered using patient or the use of individualized care plans.
What is an ACOWhat is an ACO

• Medicare Shared Savings Program (Sec. 3022).• How does CMS believe an ACO should look?
• Shared Governance Structure
• ACO Participants must have “at least 75% control” of the governing body.
• Medicare Beneficiaries must be on the governing body.
• The use of a beneficiary advisory panel is acceptable.
• Governing body MUST BE SEPARATE and UNIQUE to the ACO where the ACO is comprised of multiple independent entities.
What is an ACO

• Medicare Shared Savings Program• Operations Requirements (CMS Proposed Reg. §425.5)
• The ACO: an executive director (ED) or general partner.• Must report to the governing board.
• The ED’s leadership team must have “the ability to influence or direct clinical practice to improve efficiency processes and outcomes.”
• Clinical management “must be managed by a full-time senior level medical director…physically present on a regular basis in an established ACO location, AND …
• Must be a board-certified physician, AND • Licensed in the State in which the ACO operates.
What is an ACO

• Commitment to ACO Clinical Activities (CMS Proposed Regulations §425.5)• ACO participants must have a “meaningful commitment”
to clinical integration.• Financial Investment OR• “Human investment” – time and effort.
• ACO should have a MD/DO-directed QA and PI committee(s).―Physician directed does not mean ONLY physicians!! • Oversees the establishment of internal performance standards
for quality of care and services and cost effectiveness.• Also it must “hold ACO providers/suppliers accountable” for
meeting standards.
What is an ACO

• What does it mean to “hold accountable?”• ACO participants must agree to comply with guidelines
and processes; AND • Be subject to performance evaluations and potential
remedial actions, including their expulsion from the ACO.
• The ACO must have policies and procedures for expulsion of ACO participants and ACO provider/suppliers from the ACO.• Can you expel a hospital or hospital system?
What is an ACO

• Medicare Shared Savings Program (Sec. 3022).• Payment?
• Payment shall continue to be made to providers of services and suppliers participating in an ACO under the original Medicare fee-for-service program under parts A and B in the same manner as they would otherwise be made.
• A participating ACO is eligible to receive payment for shared savings if: • ACO meets quality performance standards and actually achieves
savings.
• Payment is a percent of the difference between the estimated average per capita Medicare expenditures in a year (risk-adjusted) as compared to historical benchmark for the ACO. The remainder of such difference shall be retained by the government.
What is an ACO
• Medicare Shared Savings Program (Sec. 3022). • Two Tracks - (1) All Risk or (2) Risk in Year 3 Only.
• There shall be no administrative or judicial review of:• Assessment of the quality of care furnished by an ACO and the
establishment of performance standards;
• Assignment of Medicare fee-for-service beneficiaries to an ACO;
• The determination of whether an ACO is eligible for shared savings and the amount of such shared savings, including the determination of the estimated average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries assigned to the ACO and the average benchmark for the ACO.
Losses “Carry Forward.”
What is an ACO

• November 2010 – How can small practices participate in ACOs?• Funding• Antitrust Exemptions
• The rules are out! So will the Confusion end?• Unlike other PPACA regulations these are NOT interim
final rules --- there is a 60 day comment period.• There may be significant changes.
Continued Confusion
• Antitrust Enforcement & Exemptions: 2 Entities• “The latest standoff between the Justice Department and
Federal Trade Commission centers on a key piece of the Obama administration's health-care overhaul.”
• “At times, officials have resorted to coin flips and turn-taking games to settle which agency will get jurisdiction.”
• “In addition to the most recent coin toss—which several people familiar with the matter said the Justice Department won—the agencies have employed the "possession arrow" system borrowed from college basketball, in which they take turns.” *WSJ 4/12/11
Continued Confusion

• Improving Medicaid/Medicare accountability – and achieving meaningful savings – must have a robust physician network. • Physicians are necessary for ACOs to work. Medical Homes vs.
Health Homes.
• Texas: Only 42 percent of physicians report seeing all new Medicaid patients; in 2000, 67 percent reported same
• Medicaid payments average 73 percent of Medicare and 50 percent of commercial payments.
• Lack of competitive rates will discourage physicians from developing or participating in ACOs or other initiatives.
TMA Position
• ACO model is designed to be “physician centric” so it is a potential opportunity to increase physician prominence in the accountability discussion
• Continued evolution of ACO model gives physicians opportunities to influence the future, but no time to dawdle.
• Antitrust Exemptions: May contribute to increased alignment and collaboration among physicians, making it easier for patients and physicians to navigate a complicated system.
Potential Opportunities

• Increases focus on importance of primary care and prevention as well as use of evidence-based standards
• May bring practices new dollars to support investments in infrastructure, such as HIT.
• May allow direct contracting with employers, thereby removing insurers OR hospitals as an intermediary
Potential Opportunities
Potential Drawbacks

• Temptation to curtail necessary care if incentives are not carefully crafted.
• Is the Unicorn still an accurate description:• “They [ACOs] only work if the provider gets paid less for the same
patient population. Why would they be dumb enough to voluntarily accept that outcome?” Why would anyone “spend millions to develop an ACO so they can get less money? Only in the policy wonk netherland does that compute.”
• Bob Laszewski - Health Care Policy and Marketplace Review, April 7, 2011.
• “A new health care delivery model promises heavy scrutiny from the nation's top federal agencies, scores of clinical-measure requirements, downside risk and uncertainty for success. Any volunteers?”
• Accountability Arrives By Rich Daly and Jessica Zigmon
Potential Drawbacks

• ACOs are here – PPACA provides for them and commands HHS to aid in their development.
• This is the search by payors for the better cheaper medical service.• Patients have different expectations than
employers/payors. Employers are also patients.• How physicians approach the opportunity (leaders
or mere participant) will have a fundamental impact on structure and focus.
• Only the future will tell whether mistakes of the past are repeated or reformed.
Conclusion
