achieving socially significant reductions in problem
TRANSCRIPT

ACHIEVING SOCIALLY SIGNIFICANT REDUCTIONS IN PROBLEMBEHAVIOR FOLLOWING THE INTERVIEW-INFORMED
SYNTHESIZED CONTINGENCY ANALYSIS: A SUMMARY OF25 OUTPATIENT APPLICATIONS
JOSHUA JESSELQUEENS COLLEGE AND UNIVERSITY OF NORTH TEXAS
EINAR T. INGVARSSON AND RACHEL METRAS
UNIVERSITY OF NORTH TEXAS AND CHILD STUDY CENTER
HILLARY KIRK AND RUTH WHIPPLE
CHILD STUDY CENTER
Jessel, Hanley, and Ghaemmaghami (2016) reported the results of 30 interview-informed, syn-thesized contingency analyses (IISCAs) and found the IISCAs to be an effective tool for identify-ing the functions of problem behavior across a variety of topographies, participants, andsettings. Jessel et al. did not, however, include data on the effectiveness of the correspondingtreatments. In the current study, we collected and summarized 25 additional applications, fromanalysis to treatment, in which the IISCA was applied in an outpatient clinic. The IISCA identi-fied various social functions of problem behavior, which informed personalized treatments offunctional communication training with contingency-based reinforcement thinning. A 90% orgreater reduction in problem behavior was obtained for every participant by the end of the treat-ment evaluation. The assessment and treatment process was socially validated by caregivers whorated the procedures highly acceptable and helpful, and the improvement in their child’s behav-ior highly satisfactory.Key words: autism, functional analysis, problem behavior, functional communication train-
ing, reinforcement schedule thinning
Functional analysis of problem behaviorinvolves systematic manipulation of antecedentor consequent events that might influence theoccurrence of the behavior (Hanley, Iwata, &McCord, 2003). Functional analyses are con-ducted prior to treatment evaluations in anattempt to (a) identify the environmentalcauses of the problem behavior before it is
treated, (b) establish a baseline from which toevaluate treatment effects, and (c) create a suffi-ciently motivating context to teach sociallyappropriate alternative behavior (Hanley,2012). Functional analysis has become a staplein research on the assessment and treatment ofproblem behavior, because it has allowed forbehavior change to be understood at the levelof process. Functional analysis is likely to resultin more efficacious treatment outcomes com-pared to when function is merely inferred fromnonanalytic assessments or when behavior func-tion is not considered prior to treatment(Campbell, 2003; Heyvaert, Saenen, Campbell,Maes, & Onghena, 2014; Kahng, Iwata, &Lewin, 2002). The efficacy of treatments based
This research was supported in part by a grant fromMasonic Home and School of Texas. We thank GregoryHanley for his helpful comments on earlier versions ofthis manuscript. Einar T. Ingvarsson is now at the Vir-ginia Institute of Autism.
Address correspondence to: Joshua Jessel, Queens Col-lege, 65-30 Kissena Boulevard, Queens, NY 11367.Email: [email protected]
doi: 10.1002/jaba.436
JOURNAL OF APPLIED BEHAVIOR ANALYSIS 2018, 51, 130–157 NUMBER 1 (WINTER)
© 2018 Society for the Experimental Analysis of Behavior
130

on functional analyses has been summarized inmultiple outcome studies, which describe anumber of clinical cases within single-subjectdesigns. These studies have aggregated resultsof clinical cases treated in an outpatient setting(Kurtz et al., 2003), cases involving functionalcommunication training (FCT) and supple-mentary treatment components (Hagopian,Fisher, Sullivan, Acquisto, & LeBlanc, 1998;Rooker, Jessel, Kurtz, & Hagopian, 2013), andcases specific to reinforcement thinning proce-dures following FCT (Greer, Fisher, Saini,Owen, & Jones, 2016).Greer et al. (2016) described 25 clinical
applications of FCT based on functional ana-lyses indicating socially mediated problembehavior. FCT involves reinforcing a communi-cation response that specifies the reinforcer thatmaintains problem behavior, while placingproblem behavior on extinction (Carr & Dur-and, 1985). Following reductions in problembehavior during FCT for 22 cases, reinforce-ment was thinned by introducing signaledperiods in which reinforcement was not avail-able (e.g., multiple schedule, response restric-tion). Ninety-one percent (20 of 22) of thecases reached 4- to 5-min delays to reinforce-ment while maintaining at least an 80% reduc-tion in problem behavior. The authors reportedreplicating the standard functional analysis pro-cedures described by Iwata, Dorsey, Slifer, Bau-man, and Richman (1982/1994), as did theother outcome studies cited above (Hagopianet al., 1998; Kurtz et al., 2003; Rooker et al.,2013). However, social validity assessmentswere not included in any of these outcomestudies. Therefore, the acceptability of theassessment process, treatments, or outcomeswas not determined. Furthermore, multiple for-mats exist for conducting standard analysesprior to treatment, such as the brief (Northupet al., 1991), trial-based (Austin, Groves, Reyn-ish, & Francis, 2015; Sigafoos & Saggers,1995), or latency-based (Lambert et al., 2017;Thomason-Sassi, Iwata, Neidert, & Roscoe,
2011) formats. The treatment utility of theseslight variations to the standard functional anal-ysis format (Iwata et al.1982/1994) has yet tobe evaluated in similar large-scale outcomestudies.Hanley, Jin, Vanselow, and Hanratty (2014)
recently designed and evaluated a fundamen-tally different functional analysis format, namedthe interview-informed, synthesized contin-gency analysis (IISCA). The IISCA is informedby an interview with caregivers, and sometimesa brief observation, to determine evocative con-texts, putative reinforcers, and specific materialsto be included in an analysis. A single test con-dition is individualized for each patient fromthe assessment results and control conditionsare then designed from the test condition to bethe same except that the reinforcement contin-gency is absent in the control condition. IIS-CAs can involve multiple levels ofindividualization. First, the analysis materialsand interactions can be individualized to matchthose that are reported by caregivers as evoking(e.g., specific tasks or instructions) or reinfor-cing (e.g., specific toy or a certain song) prob-lem behavior. It is possible for a standardfunctional analysis to include this level of indi-vidualization; however, it is unclear how oftenthis occurs, because many multiple-participantstudies include a near-identical description ofthe initial functional analysis conditions withno apparent individualization (e.g., Fisher,Greer, Romani, Zangrillo, & Owen, 2016;Kurtz et al., 2003; Rooker et al., 2013; Wal-lace & Iwata, 1999). Second, the conditions/contingencies can be individualized in anIISCA to emulate the problematic context.Third, if a parent reports that the contingenciesco-occur, they can be synthesized to moreclosely approximate the typical conditions inthe client’s home. If a parent implicates onlypositive reinforcement, a negative reinforce-ment contingency will not be included in anindividualized analysis. This is a significantdeparture from the standard functional analysis
131ASSESSMENT AND TREATMENT

in which positive and negative reinforcementare always tested in isolated conditions andmultiple test conditions are included in all ana-lyses. Thus, the procedures of the standardfunctional analysis can be individualized, but itappears that researchers rarely do so.Hanley et al. (2014) conducted the IISCA
with three children diagnosed with autism, andimplemented treatment for each child based onthe results. The treatments consisted of teach-ing increasingly complex forms of communica-tion during FCT. Reinforcement was thenthinned by increasing the number of tasks orthe duration of isolate play with nonpreferredmaterials that the participant was required tocomplete to earn the reinforcers. Hanleyet al. effectively eliminated problem behaviorwhile simultaneously teaching communication,toleration, and compliance. Caregivers alsoreported high satisfaction with the assessmentprocess, treatment procedures, and treatmentoutcomes.The general utility of the IISCA was recently
described by Jessel et al. (2016), who summa-rized the results of 30 applications. The general-ity of the procedures was evident; the IISCAwas conducted with children and adults (1.8 to30 years old), with and without diagnoses(e.g., generalized anxiety disorder, attention def-icit hyperactivity disorder), across a variety ofproblem behavior (i.e., aggression, disruption,self-injurious behavior [SIB], loud vocaliza-tions), and in various settings (e.g., outpatientclinic, home, public school, day habilitationcenter). However, this study was limited to asummary of the assessment, without reports ofsubsequent treatment evaluations.To date, there have been 15 published single-
subject demonstrations of strong treatmenteffects when treatment was based on functionsidentified via the IISCA (e.g., Ghaemmaghami,Hanley, & Jessel, 2016; Ghaemmaghami, Han-ley, Jin, & Vanselow, 2015; Hanley et al.,2014; Santiago, Hanley, Moore, & Jin, 2016;Slaton, Hanley, & Raftery, 2017; Strand &
Eldevik, 2017). However, a large-scale evalua-tion of treatment effectiveness across consecu-tive clinical cases has not yet appeared in theliterature.We conducted the current study to deter-
mine the effectiveness of FCT and reinforce-ment schedule thinning following the IISCAfunctional analysis format. This research is adirect extension of Jessel et al. (2016), with theinclusion of treatment outcomes for a collec-tion of clinical cases over a span of almost twoyears. We used FCT as a form of treatment forall participants, because it is the most com-monly used function-based treatment (Tiger,Hanley, & Bruzek, 2008) and is empiricallyvalidated as treatment for the problem behaviorof individuals diagnosed with intellectual dis-abilities and autism (Kurtz, Boelter, Jarmolo-wicz, Chin, & Hagopian, 2011). In Study1, we summarized the results of 25 IISCAs forchildren with autism spectrum disorder (ASD)who had been admitted to an outpatient behav-ior disorders clinic due to problem behavior. InStudy 2, we summarized the results of the FCTand reinforcement thinning procedures, as wellas the results of a social validity assessment con-ducted with caregivers at the conclusion oftheir child’s participation.
STUDY 1: SUMMARY OFINTERVIEW-INFORMED SYNTHESIZED
CONTINGENCY ANALYSES
MethodParticipants and settings. Twenty-five chil-
dren from an outpatient clinic participated inthis study. All patients were referred to theclinic due to severe behavior problems requiringoutpatient services. The first 25 patients whoseproblem behavior was suspected to be main-tained by socially mediated reinforcement wereselected to participate. A total of 32 patientswere screened at the outpatient clinic. Fourpatients were excluded because they did notexhibit problem behavior during any visits to
JOSHUA JESSEL et al.132

the clinic during a span of two weeks. One par-ticipant displayed a single topography of prob-lem behavior (i.e., elopement) that promptedthe use of a trial-based IISCA and treatmentprocess relying on a latency measure. Weexcluded these data from the current paper dueto these procedural differences. Another patientwas excluded because we obtained an insuffi-cient amount of interobserver agreement (IOA)data. Another patient’s services were discontin-ued prior to the completion of the functionalassessment period. The remaining 25 of thefirst 32 patients admitted to the outpatientclinic were included as participants. Three ofthe patients’ (Anson, Robin, and Kat) func-tional analyses were also included in the publi-cation by Jessel et al. (2016).The demographic information of each partic-
ipant is presented in Table 1. The majority ofthe participants were male (21 of 25) and themedian age was 5 years (range, 2 to 15 yearsold). All but one participant had a diagnosis ofASD; Sarah was typically developing but had adiagnosis of Tourette syndrome. The partici-pants’ language ability upon intake ranged fromnonvocal communication to vocal communica-tion using full, fluent sentences. Based onparental reports and observation of the partici-pants, we grouped most problem behavior intofour possible categories: problem behaviordirected toward others (aggression), problembehavior directed toward objects (disruption),problem behavior directed toward themselves(self-injurious behavior; SIB), and tantrums.The majority of participants had some combi-nation of these topographical classes of problembehavior. Some participants also had less com-mon forms of problem behavior such as loudvocalizations or spitting, and one participantdisplayed only inappropriate sexual behav-ior (ISB).Patients admitted to the clinic were provided
behavioral services 7 hr a day, 5 days a week,for 2 consecutive weeks. Assessment and treat-ment took place during the first week and
parent training was conducted during the sec-ond week. Sessions were conducted in 3-m x 6-m and 3-m x 4-m treatment rooms, with atleast one caregiver present to observe sessionsthroughout the entire assessment and treatmentprocess. One therapist conducted sessions (pri-mary implementer) while a second therapistcollected data (primary data collector). The pri-mary data collector also assisted during timesbetween sessions. The therapists had under-graduate degrees in psychology or related fields,but did not have any graduate training inbehavior analysis. The therapists were trainedand supervised by the first author, a Board Cer-tified Behavior Analyst-Doctoral (BCBA-D).Measurement and interobserver agreement. We
measured occurrences of multiple topographiesof problem behavior. Aggression was defined ashitting, kicking, scratching, or biting others.Disruption was defined as tearing, throwing,and hitting items. SIB was defined as hitting,scratching, or biting self. A tantrum wasdefined as dropping to the floor and crying orwhining for more than 30 s. Loud vocalizationswere defined as yelling, screaming, or swearing.In addition, ISB was recorded for one partici-pant who would attempt to touch other peo-ple’s genital areas. The rate of problembehavior was calculated by dividing the sessionduration in minutes by the total number ofresponses within each session.Some of the IISCAs included instructions to
complete tasks. The instructions were providedto the participant in three steps: verbal prompt,model prompt, and physical prompt. Compli-ance was scored if the participant completedthe task within 10 s of the first or secondprompt.Sessions were video recorded, and a second
observer independently scored a portion of thevideos to obtain interobserver agreement(IOA). IOA was calculated as total agreementby dividing the smaller number of responseswithin a session by the larger number. Totalagreement was used in place of more
133ASSESSMENT AND TREATMENT

conservative IOA calculations due to clinicalconstraints on training therapists in othermethods. We obtained IOA for 67% of ses-sions on average across participants (range,40%-100%). The mean IOA across partici-pants was 94% (range, 82%-100%). A sum-mary of IOA for each participant is available asSupporting Information.Experimental design. Two conditions, test
and control, were included in every IISCA andcompared in a multielement design. Sessionswere conducted in a fixed sequence: control-test-control-test-test, with additional sessions ofeither condition conducted when necessary.Control conditions were always conducted firstto build rapport with the participant in a con-text of rich reinforcement. The last two test ses-sions were conducted consecutively, without
the interspersed control session, to ensure thatrate of problem behavior was not a function ofthe patterned alternation of conditions.Procedure. All IISCAs were preceded by a
15- to 30-min open-ended interview with care-givers and a 10- to 40-min semistructuredobservation of the child. The interview wasconducted by a BCBA-D (the first author) andincluded questions pertaining to (a) the topog-raphy of problem behavior, (b) antecedents toproblem behavior, (c) consequences followingproblem behavior, and (d) any other contextu-ally relevant stimuli. The questionnaire usedduring the interview can be found in theappendix of Hanley (2012). During the obser-vation, the clinician unsystematically arrangedthe contexts described as likely to evoke prob-lem behavior. For example, a parent reported
Table 1Participant Characteristics
Participant Age Sex Diagnosis Language Abilitya Problem Behavior
Joe 5 M ASD 1 Agg, Dis, TantrumsAnson 7 M ASD, ID 1 Agg, Dis, SIBRobin 6 F ASD, ADHD 3 Agg, Dis, SIBKat 4 F ASD 1 Agg, Tantrums, SIBAri 15 M ASD, ID, ADHD 4 ISB
Lance 4 M ASD, ID 2 Agg, Dis, Loud vocAaron 7 M ASD, ADHD, ID 2 Agg, SIBStan 5 M ASD, ADHD 2 Agg, Dis, TantrumsMatt 11 M ASD, GAD 3 Agg, Dis, Tantrums, Loud vocKen 5 M ASD, ADHD, ID 1 Agg, Dis, TantrumsTim 4 M ASD, ID 1 Agg, Dis, TantrumsZane 3 M ASD, ID 1 Dis, SIB, TantrumsKane 5 M ASD, ADHD, ID 2 Agg, Dis, TantrumsMike 8 M ASD 2 Agg, Dis, TantrumsJohn 4 M ASD 2 Agg, Tantrums, Loud vocSteve 4 M ASD, ID 1 Agg, TantrumsMax 4 M ASD, ID 3 Agg, Dis, TantrumsAlex 2 M ASD, ID 1 Agg, Dis, SIB, SpittingSarah 7 F Tourette syndrome 4 Agg, Dis, SIB, TantrumsAnnie 5 F ASD, ADHD, ID 3 TantrumsDan 6 M ASD, ADHD 4 Agg, Tantrums, Loud vocGreg 6 M ASD, ADHD 2 Agg, SIB, Tantrums, Loud vocDace 11 M ASD, ID 2 Agg, Dis, SIB, TantrumsLarry 5 M ASD, ADHD, ID 3 Agg, Dis, SIB, Tantrums, Loud vocAce 2 M ASD, ID 1 Aggression, SIB, Loud voc
a 1 = non-vocal; 2 = 1-word utterances; 3 = short diffluent sentences; 4 = full fluencyNote. ASD is autism spectrum disorder. ID is intellectual disability. ADHD is attention deficit/hyperactivity disorder.GAD is generalized anxiety disorder. Agg is aggression. Dis is disruption. ISB is inappropriate sexual behavior. SIB isself-injurious behavior. Loud voc is loud vocalizations.
JOSHUA JESSEL et al.134

that problem behavior was likely to occur whentheir child’s independent play with a train setwas interrupted with parent-directed play. Inthis instance, the therapist gave the child accessto the train and observed what problem behav-iors occurred when the therapist instructed thechild to play with the train differently. Ari’scase was unique due to the topography of hisproblem behavior (i.e., ISB). His parentsreported that he would touch his sister or othergirls inappropriately if they were playing withhis iPad. As reported, his sister would then “feeluncomfortable” and either run away to tell theparents or simply go to a different area of thehouse, leaving Ari with the iPad. We thereforearranged for female therapists to remove Ari’siPad and return access only following ISBattempts.Problem behaviors reported by parents, as
well as any problem behavior that occurredduring the observation but was not reported bycaregivers during the interview, was included inthe definition and measurement of targetbehavior. The information obtained from boththe interview and observation was then used tocreate a single test condition and a matchedcontrol condition for the IISCA.IISCA sessions were 3 to 10 min and
involved delivery of the putative reinforcer(s)contingent on problem behavior in the testcondition, and continuous noncontingentaccess to reinforcement in the control condi-tion. The BCBA-D determined the initial ses-sion duration based on the problem behaviorduring the observation. If the evocative situa-tion resulted in immediate problem behavior,the sessions were shorter (3 to 5 min). Iflengthier exposure to the evocative situationwas needed to evoke problem behavior, the ses-sions were extended to 10 min.Relevant establishing operations were
arranged at the beginning of each test conditionsession. The establishing operations were ante-cedent stimuli or events that were implicatedby the interview and observation to evoke
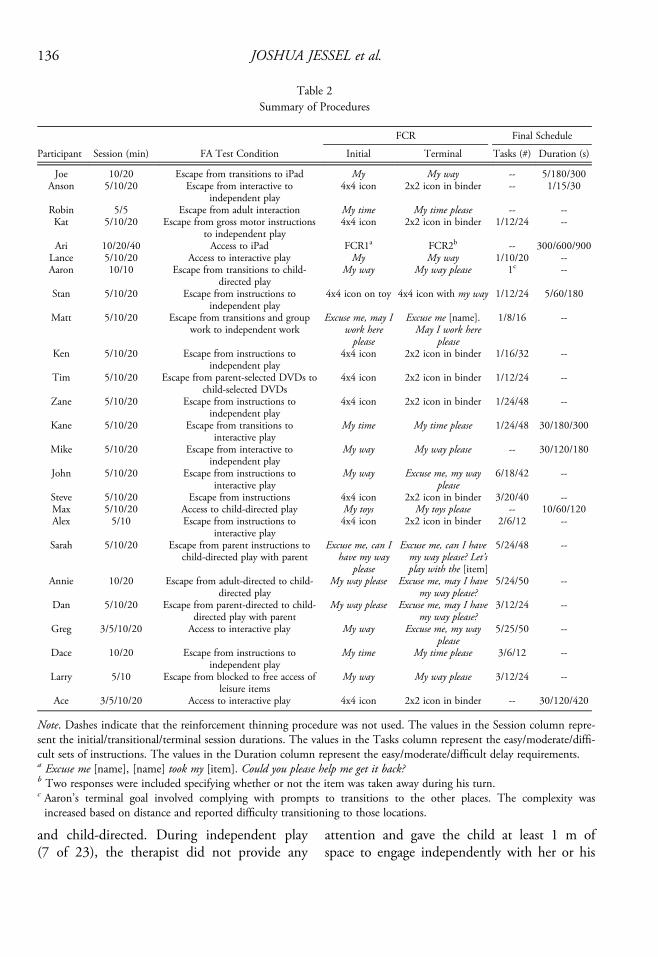
problem behavior related to the putative rein-forcers (e.g., removing preferred items, present-ing demands, directing the child’s play). Anyproblem behavior that occurred during the pre-sentation of the establishing operation resultedin the presentation of the putative reinforcer(s)for 30 s. If multiple reinforcers were synthe-sized, they were provided simultaneously. Anyproblem behavior during the 30-s presentationof the reinforcer resulted in no programmedchanges. At the beginning of each control con-dition session, the abolishing operations werearranged. The abolishing operations were ante-cedent stimuli or events that were implicatedby the interview and observation to eliminateproblem behavior related to the putative rein-forcers from the test condition (e.g., access topreferred items, no demands, unstructuredplay). Any problem behavior that occurred dur-ing the control condition resulted in no envi-ronmental changes. Thus, the test and controlconditions were matched and included all ofthe same stimuli. The only difference betweenthe conditions was the motivating operations(i.e., establishing vs. abolishing) and themethod of reinforcer delivery (i.e., contingenton problem behavior vs. noncontingent).Table 2 provides a brief summary of the pro-
cedures for each participant. For 20 of 25 par-ticipants, we included some form of negativereinforcement in the test condition. The nega-tive reinforcement contingency took the formof escape from transitions (4 of 20), escapefrom interactive or adult-directed play (4 of20), or escape from some form of instruction(9 of 20). The negative reinforcement contin-gencies for some participants were more indi-vidualized, and included escape from adultattention (Robin), specific gross-motor instruc-tions (Kat), working with others present(Matt), and parent-selected DVDs (Tim).The IISCA for 23 of the 25 participants
included some form of positive reinforcement.Many of these conditions included one of threepossible forms of play: independent, interactive,
135ASSESSMENT AND TREATMENT
and child-directed. During independent play(7 of 23), the therapist did not provide any
attention and gave the child at least 1 m ofspace to engage independently with her or his
Table 2Summary of Procedures
FCR Final Schedule
Participant Session (min) FA Test Condition Initial Terminal Tasks (#) Duration (s)
Joe 10/20 Escape from transitions to iPad My My way -- 5/180/300Anson 5/10/20 Escape from interactive to
independent play4x4 icon 2x2 icon in binder -- 1/15/30
Robin 5/5 Escape from adult interaction My time My time please -- --Kat 5/10/20 Escape from gross motor instructions
to independent play4x4 icon 2x2 icon in binder 1/12/24 --
Ari 10/20/40 Access to iPad FCR1a FCR2b -- 300/600/900Lance 5/10/20 Access to interactive play My My way 1/10/20 --Aaron 10/10 Escape from transitions to child-
directed playMy way My way please 1c --
Stan 5/10/20 Escape from instructions toindependent play
4x4 icon on toy 4x4 icon with my way 1/12/24 5/60/180
Matt 5/10/20 Escape from transitions and groupwork to independent work
Excuse me, may Iwork hereplease
Excuse me [name].May I work here
please
1/8/16 --
Ken 5/10/20 Escape from instructions toindependent play
4x4 icon 2x2 icon in binder 1/16/32 --
Tim 5/10/20 Escape from parent-selected DVDs tochild-selected DVDs
4x4 icon 2x2 icon in binder 1/12/24 --
Zane 5/10/20 Escape from instructions toindependent play
4x4 icon 2x2 icon in binder 1/24/48 --
Kane 5/10/20 Escape from transitions tointeractive play
My time My time please 1/24/48 30/180/300
Mike 5/10/20 Escape from interactive toindependent play
My way My way please -- 30/120/180
John 5/10/20 Escape from instructions tointeractive play
My way Excuse me, my wayplease
6/18/42 --
Steve 5/10/20 Escape from instructions 4x4 icon 2x2 icon in binder 3/20/40 --Max 5/10/20 Access to child-directed play My toys My toys please -- 10/60/120Alex 5/10 Escape from instructions to
interactive play4x4 icon 2x2 icon in binder 2/6/12 --
Sarah 5/10/20 Escape from parent instructions tochild-directed play with parent
Excuse me, can Ihave my way
please
Excuse me, can I havemy way please? Let’splay with the [item]
5/24/48 --
Annie 10/20 Escape from adult-directed to child-directed play
My way please Excuse me, may I havemy way please?
5/24/50 --
Dan 5/10/20 Escape from parent-directed to child-directed play with parent
My way please Excuse me, may I havemy way please?
3/12/24 --
Greg 3/5/10/20 Access to interactive play My way Excuse me, my wayplease
5/25/50 --
Dace 10/20 Escape from instructions toindependent play
My time My time please 3/6/12 --
Larry 5/10 Escape from blocked to free access ofleisure items
My way My way please 3/12/24 --
Ace 3/5/10/20 Access to interactive play 4x4 icon 2x2 icon in binder -- 30/120/420
Note. Dashes indicate that the reinforcement thinning procedure was not used. The values in the Session column repre-sent the initial/transitional/terminal session durations. The values in the Tasks column represent the easy/moderate/diffi-cult sets of instructions. The values in the Duration column represent the easy/moderate/difficult delay requirements.a Excuse me [name], [name] took my [item]. Could you please help me get it back?b Two responses were included specifying whether or not the item was taken away during his turn.c Aaron’s terminal goal involved complying with prompts to transitions to the other places. The complexity wasincreased based on distance and reported difficulty transitioning to those locations.
JOSHUA JESSEL et al.136

preferred leisure items. During interactive play(6 of 23), the therapist provided verbal andphysical attention while the participant engagedwith the preferred items. During child-directedplay (5 of 23), the therapist honored anyrequests made by the participants and onlyinteracted with them following bids for atten-tion. For two participants (Joe and Ari), thepositive reinforcement contingency involvedthe delivery of only one item, an iPad. For oneparticipant (Tim), the positive reinforcementwas specific to DVDs that he selected. Thepositive reinforcement for Matt was access toindependent academic work.We included a synthesized contingency of
both positive and negative reinforcement forthe majority of participants (19 of 25). Weimplemented isolated positive reinforcementwith four participants (Ari, Lance, Max, andGreg) and attempted to isolate negative rein-forcement with two participants (i.e., no posi-tive reinforcement was programmed during theescape interval for Robin and Steve). The con-tingencies were tested in isolation when theresults of the interview and observation sug-gested that they did not co-occur with otherputative contingencies.
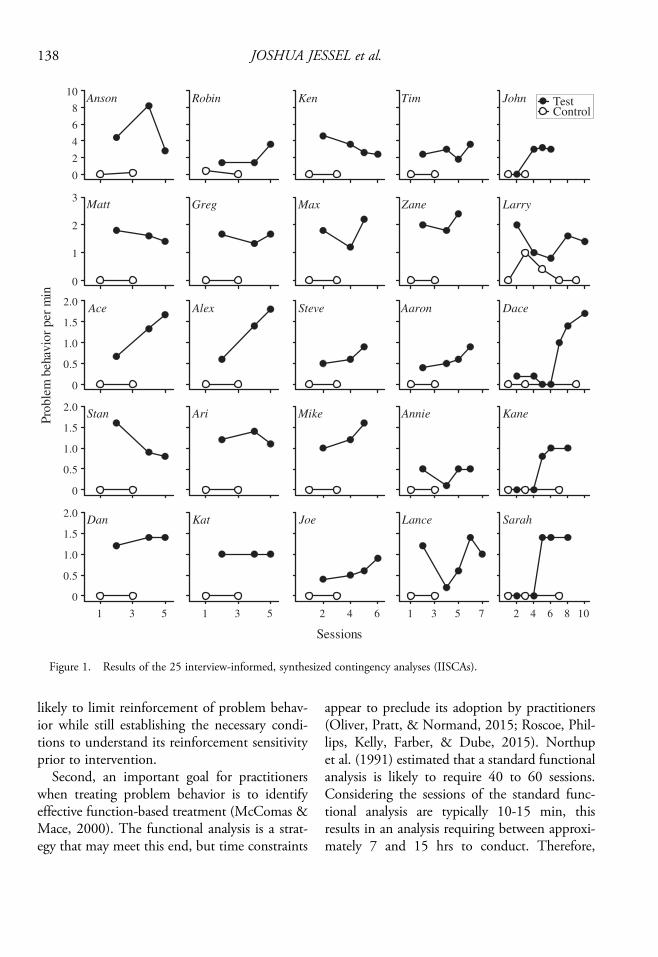
Results and DiscussionThe results of the 25 IISCA applications are
presented in Figure 1. Higher rates of problembehavior were observed across participants dur-ing the test condition (M = 1.5 RPM; SD =1.04) relative to the control condition (M = 0.02RPM; SD = 0.07). For 20 out of 25 participants,there was no overlap between the test and con-trol conditions. In four cases in which overlapoccurred, it was due to problem behavior occur-ring at low or zero rates at the beginning of theanalysis. No problem behavior was observed dur-ing the control condition for 22 out of 25 partici-pants. For most of the IISCAs, the minimumnumber of sessions (i.e., five) was sufficientbecause of the limited overlap and near
elimination of problem behavior during the con-trol condition. Fourteen participants requiredfive sessions total, six participants required sixsessions, and the remaining five participantsrequired seven or more sessions. Based on thenumber of sessions and the duration of each ses-sion, the mean duration of the analysis was35.6 min and the median was 25 min.We replicated the results of previous research
(Jessel et al., 2016), and the results support theIISCA as an efficient tool for determiningsocially mediated functions of problem behav-ior. The brevity of functional analysis is animportant parameter to consider for practicalreasons, as suggested by the multiple functionalanalysis formats designed for that purpose(e.g., Northup et al., 1991; Thomason-Sassiet al., 2011). There are at least two clinicallyguided purposes for using formats that requireless time to conduct. First, identification ofbehavioral function requires the target responseto occur and be reinforced. Because the targetresponse during a functional analysis is problembehavior, it is best to (a) obtain only anamount of problem behavior necessary todetect a difference between the test and controlconditions (i.e., there is no benefit and onlygreater risk when problem behavior occurs at arate exceeding that expected by the reinforce-ment period duration—e.g., 2 per min with30 s reinforcement intervals), and (b) minimizeits exposure to reinforcement. Extended expo-sure to reinforcement could lead to initial resis-tance to treatment (see Nevin & Shahan, 2011for a review of behavioral momentum in appli-cation). On the other hand, avoiding functionalanalysis altogether leads behavior analysts torely on highly inferential indirect or descriptiveassessment tools (Iwata, DeLeon, & Roscoe,2013; Lerman & Iwata, 1993) that yield onlyinformation about the prevalence of antecedentand consequences without any means to under-stand the relevance of those events to problembehavior (Hanley, 2012; Iwata & Dozier,2008). An efficient functional analysis format is
137ASSESSMENT AND TREATMENT
likely to limit reinforcement of problem behav-ior while still establishing the necessary condi-tions to understand its reinforcement sensitivityprior to intervention.Second, an important goal for practitioners
when treating problem behavior is to identifyeffective function-based treatment (McComas &Mace, 2000). The functional analysis is a strat-egy that may meet this end, but time constraints
appear to preclude its adoption by practitioners(Oliver, Pratt, & Normand, 2015; Roscoe, Phil-lips, Kelly, Farber, & Dube, 2015). Northupet al. (1991) estimated that a standard functionalanalysis is likely to require 40 to 60 sessions.Considering the sessions of the standard func-tional analysis are typically 10-15 min, thisresults in an analysis requiring between approxi-mately 7 and 15 hrs to conduct. Therefore,
Robin Ken Tim John TestControl
ZaneMaxGreg Larry
2 4 6 8 10
Sarah
Annie
5
Dace
KaneMike
SteveAlex
2 4 6
Joe
1 3 5
Kat
Ari
1 3 5 7
Lance
Aaron
Pro
ble
m b
ehavio
r per
min
Sessions
2
4
6
8
10
0
Anson
1
2
3
0
Matt
1 3
0.5
1.0
1.5
2.0
0
Dan
0.5
1.0
1.5
2.0
0
Stan
0.5
1.0
1.5
2.0
0
Ace
Figure 1. Results of the 25 interview-informed, synthesized contingency analyses (IISCAs).
JOSHUA JESSEL et al.138

conducting a standard functional analysis maybe outside the reach of practitioners who do notwork in inpatient settings. The IISCA provides aviable solution, because it typically requires aslittle as 25 min to complete. However, the dura-tion of the interviews and observations thatinform the IISCA are not reported in the currentstudy, and it is unknown how much these preas-sessments precisely influence the brevity of theanalysis. A comparison of efficiency that includespreassessment duration cannot be achieved,because the precise duration of preassessmentsare not typically reported for either the IISCA orthe standard functional analysis formats. Fur-thermore, this comparison may be unnecessaryconsidering that the maximum duration of theIISCA interview and observation (70 min)added to the median analysis duration (25 min),is still less than the time it takes to conduct astandard functional analysis.Efficiency is, in part, achieved during an
IISCA by conducting a single test condition inwhich the suspected contingencies are emulatedand synthesized, rather than multiple test condi-tions in which typical contingencies are evalu-ated in isolation. Synthesis reduces experimentalprecision, because the effects of individual con-tingencies (e.g., escape vs. tangible) are not iso-lated (Fisher et al., 2016; Hanley et al., 2014).Although ecological precision is clearlyimproved by more closely approximating thenatural environment, it is unclear whether ananalysis that capitalizes on possible interactiveeffects of multiple naturally occurring conse-quences improves or reduces treatment effec-tiveness. A recent study by Slaton et al. (2017)suggests that improvement in treatment out-come may be more likely with synthesized con-tingencies (which favor ecological overexperimental precision). The within-subjectcomparative analyses showed that function-based treatments designed from IISCAs wereefficacious in four of four applications whereasfunction-based treatments designed from differ-entiated standard analyses for the same four
participants were efficacious in only two of fourapplications.The results of Slaton et al. (2017) and other
studies that have shown treatment efficacy(Ghaemmaghami et al., 2015; Ghaemmaghamiet al., 2016) or treatment effectiveness andsocial validation of the treatment effects(Hanley et al., 2014; Santiago et al., 2016;Strand & Eldevik, 2017) provides strong evi-dence of the utility of the IISCA in designingtreatments for severe problem behavior. Thesestudies show what is possible from an IISCA. Itis still not at all obvious whether it is probablethat an effective outcome will result from anIISCA. By effective, we mean outcomes show-ing zero or near-zero rates of problem behavior,the maintenance of newly acquired and impor-tant social skills, and high satisfaction with theoutcomes by relevant caregivers. The purposeof Study 2 was to describe the probability ofthese outcomes with all participants from Study1 and then to compare these outcomes to thoseobtained in other outcome studies in whichstandard analyses were used as the basis fortreatment.
STUDY 2: SUMMARY OF TREATMENTOUTCOMES FROM THE IISCA
MethodParticipants and settings. Sessions were con-
ducted in the same settings and with the sameparticipants as in Study 1.Measurement and interobserver agreement.
The measurement of problem behavior andcompliance was identical to Study 1. In addi-tion, different forms of communication and theduration of time without reinforcement wererecorded. To record the duration of time with-out reinforcement, a timer was started whenreinforcers were removed and stopped everytime reinforcers were re-presented. This mea-sure was included to determine tolerance fordelays to reinforcement during reinforcementthinning. Participants were taught a minimum
139ASSESSMENT AND TREATMENT

of three different topographies of functionalcommunication responses (FCRs), differing incomplexity. The complexity of the FCR wasdependent on the participants’ initial verbalabilities (Table 1) and was gradually increasedto a more socially appropriate level throughoutthe treatment.The definition of each participant’s FCRs is
presented in Table 2. Nine participants werenonvocal and their simple FCR involved hand-ing the therapist a 10.2 cm x 10.2 cm picturecard that was placed directly in front of them.The larger picture cards were used as a simpleFCR for all nonvocal participants to ensure thatthe initial treatment included a low effort andnovel response. The complexity of theseresponses was increased to a terminal goal ofhanding over a 5.1 cm x 5.1 cm card locatedinside a binder. The simple FCRs for partici-pants who had vocal verbal behavior varied;however, the majority were two word phrases(e.g., “My way”). Phrases such as “my way”were used because they (a) can be expanded tomore complex phrases (e.g., “May I have myway please”), (b) properly identified the generalclass of multiple different reinforcers, and(c) were unlikely to have historical relation toproblem behavior due to their novelty(Winborn, Wacker, Richman, Asmus, & Geier,2002). The terminal complexity of the vocalFCRs included an interaction with the therapistin which the participant first requested his orher attention (i.e., “Excuse me?”). Following aresponse from the therapist, the participantcompleted the phrase (e.g., “May I have myway please?). The complex FCR was scoredonly if the participant emitted both the requestfor attention and request for reinforcement.The participants were also taught a tolerance
response to denials of reinforcement. Denialsoccurred when the experimenter said “Nope,”“Not right now,” or a similar phrase in responseto participant requests. For the nonvocal partici-pants, the tolerance response involved placingtheir hands together or handing over an
additional picture card with the printed phrase“No problem.” The tolerance response for thevocal participants included some variation ofthe phrase, “Okay, no problem” while placingtheir hands together. Observers scored the num-ber of occurrences for all of the different formsof communication. For each response, the countwas converted to a rate by dividing the sum bythe duration of the session in minutes.Observers also scored duration of reinforcementaccess. Onset of reinforcement access occurredwhen the experimenter delivered the reinforcer,and offset occurred when the experimenterremoved the reinforcer.The IOA for the frequency measures was
calculated as a total agreement. The IOA forduration of time without reinforcement was cal-culated by dividing the shorter duration by thelonger duration for each session. The IOA foreach participant is presented in the SupportingInformation. A second observer independentlycollected data for IOA purposes during a meanof 27% of sessions (range, 17%-38%). Themean IOA across participants for problembehavior, FCRs, tolerance response, reinforce-ment, and compliance was 94% (range, 82%-100%), 98% (range, 86%-100%), 97% (range,87%-100%), 90% (range, 87%-94%), and 97%(range, 85%-100%), respectively.Experimental design. Following a baseline
condition, the treatment for each participantwas evaluated using the logic of a changing cri-terion design (Kazdin, 1982). The effects of thecontingency were evaluated across a minimumof three possible criteria (i.e., simple FCR,complex FCR, tolerance response), graduallyincreasing the complexity of a participant’sresponse for the identified reinforcers. In somecases, a fourth response criterion was includedwith the addition of a second complex FCR.Functional control was demonstrated when therate of each level of communication changed ina predictable direction with the change in thereinforcement contingency. A reversal back tothe baseline condition was not conducted
JOSHUA JESSEL et al.140

because it was counter-therapeutic and a dem-onstration of functional control during achanging-criterion design does not requirewithdrawing the treatment (Kazdin, 1982).Procedure. The test conditions from the
IISCA served as the baseline for the treatmentevaluation. The results of the IISCA were alsoused to inform the results of the subsequentskill-based treatment. The participants were firsttaught a novel response that produced the iden-tified reinforcers. In addition, those reinforcerswere withheld following any instances of prob-lem behavior. For example, if we found a par-ticipant’s problem behavior to be maintainedby escape from adult-directed play and access tochild-directed play, the participant would haveaccess to child-directed play only followinginstances of the target response, “My way.” Ifproblem behavior occurred, the therapist wouldcontinue to direct the participant’s play.The participants were first taught to emit the
FCR during FCT. To teach vocal FCRresponses, the therapists used a progressiveprompt-delay procedure (Charlop, Schreib-man, & Thibodeau, 1985). The prompt-delayprocedure began with an immediate verbalmodel of the target FCR. The prompt was thenprogressively delayed to 2 s, 5 s, and 10 sdepending on the participants’ independentcommunication. To teach responses thatinvolved exchange of a picture card, the thera-pists used most-to-least prompting. Trialsbegan with an immediate full physical promptto hand the therapist the picture card. The fullphysical prompt was then faded to partial-physical and gestural prompts as the partici-pants began to independently hand the thera-pist the picture card. Problem behavior wasplaced on extinction during the FCT trainingtrials; if any problem behavior occurred, thetherapists withheld the reinforcers that hadbeen identified in the IISCA. Each session was10 trials, and mastery criteria were set at twosessions with a minimum of 70% independentcorrect responding and fewer than three
instances of problem behavior. FCT trainingtrials were conducted in a minimum of threephases, each phase for the different form ofcommunication. The FCT treatment evalua-tion began following mastery of each commu-nication response.The FCT treatment evaluation involved pre-
senting the reinforcer(s) contingent on eachinstance of the target communication responsewhile problem behavior was placed on extinc-tion. Although prompts for the FCRs wereremoved, every 30 s the participants were pro-vided with a reminder of the target response(e.g., “Remember, you can always say ‘my way’if you want to play your way”). The reminderwas only delivered if the participant had notengaged in the FCR and if problem behaviorwas not occurring at the moment. As statedabove, the treatment was evaluated across aminimum of three forms of communication.Each new communication-training phase wasinitiated following three consecutive sessionswith fewer than three instances of problembehavior. During the FCT treatment evalua-tion, sessions were either 5 or 10 min. Theduration of the session was identical to the ses-sion duration during each participant’s IISCA.The treatment evaluation began after the
participant acquired the simple FCR during theFCT training trials. During the first phase ofthe treatment evaluation, the simple FCR pro-duced the reinforcer(s). When the mastery cri-teria were met, FCT training trials began forthe complex FCR. Following mastery of thecomplex FCR, the second phase of the treat-ment evaluation was implemented, duringwhich the complex FCR produced thereinforcer(s) while both the simple FCR andproblem behavior were placed on extinction. Insome cases, this process was repeated a thirdtime to teach the participant another complexFCR. For example, a participant could haveoriginally been taught the FCR, “My way.”Following mastery, “My way” would be placedon extinction and a new FCR of “My way,
141ASSESSMENT AND TREATMENT

please” would be reinforced. At this point, allof the previously targeted FCR forms would nolonger be reinforced and the terminal complex-ity, “May I have my way please” would betaught. After three sessions with near zero ratesof problem behavior during the final FCTtreatment evaluation phase, training began forthe tolerance response. When the participanthad mastered the tolerance response, anothertreatment evaluation phase was implemented.In this phase, 50% of trials were identical tothe last phase of FCR treatment evaluation,while the other 50% were “tolerance” trials. Inthe latter trial type, the FCR response was notreinforced; instead, the therapist said, “Notnow.” If the participant emitted the toleranceresponse, reinforcement was delivered. Toler-ance trials and FCR trials were randomly inter-spersed, and the simple FCR and problembehavior were placed on extinction. Reinforce-ment thinning began following three sessionswith little to no problem behavior during thetolerance response evaluation.We conducted reinforcement thinning using
the procedures described by Ghaemmaghamiet al. (2016) for 24 of the 25 participants.Robin did not participate in the reinforcement-thinning phase because following the FCTtreatment evaluation, her FCRs were on adecreasing trend and problem behaviorremained low throughout the day. Robin wastherefore deemed no longer to need intensiveservices specifically targeting problem behavior,and began to receive different clinical services.For the other participants, duration of rein-forcer access was gradually reduced by intro-ducing delay-to-reinforcement trials. Thesetrials were randomly interspersed with trials inwhich immediate reinforcement was pro-grammed for the complex FCR and toleranceresponse (see Figure 2).For some participants, the duration of the
delay depended on compliance to a set numberof task demands (Figure 2, top panel). Thisreinforcement thinning procedure can be
conceptualized as a chained schedule using dif-ferential reinforcement of alternative behavior(DRA). During a delay-to-reinforcement trial,when the participant emitted the complexFCR, the therapist said, “Not now,” which setthe occasion to emit the tolerance response.Following the tolerance response, the partici-pant was provided a set number of demands tocomplete before the reinforcer was re-presented.The instructions were identical to those usedduring the IISCA and were participant-specific,based on the reports by the caregivers from theinterview. For example, if adult-directed playwas a problematic context, the therapist wouldprovide the participants with instructions suchas, “Put this puzzle piece in next” or “Makethis car go up the tracks.” If problem behavioroccurred during the delay, the number of tasksthe participant was required to complete wasreset. This DRA-based reinforcement thinningapproach was used when parents reportedproblem behavior or noncompliance duringinstructions.For other participants, the duration of the
delay depended only on whether or not prob-lem behavior occurred (Figure 2, bottompanel). This reinforcement thinning procedurecan be conceptualized as a chained scheduleusing differential reinforcement of other behav-ior (DRO). Instead of demands being pre-sented, the participant had to engage in anyform of appropriate behavior without problembehavior. This could include engaging withother items (nonpreferred) or completingsupervised transitions to other locations. Thenonpreferred items were those the participantsdid not select during preference assessmentsthat were conducted multiple times per day(see Ghaemmaghami et al., 2016). The non-preferred items were included if caregiversreported having difficulty completing house-hold tasks because the extent of the partici-pants’ problem behavior required constantsupervision. When the delay was introduced,the participant was provided an instruction
JOSHUA JESSEL et al.142

such as, “[preferred items] are not available butyou can play with the [nonpreferred items] ifyou would like.” Access to the items was pre-sented as a choice and the participant was notrequired to play with the items in order for thereinforcers to be delivered at the end of theDRO interval. The supervised transitions wereincluded if caregivers reported not being able totake the participant to any locations away fromtheir preferred items. If problem behavioroccurred during the DRO interval, the dura-tion requirement was reset.The number of demands and duration
requirements were progressively increased con-tingent on two consecutive sessions of little tono problem behavior. In addition, three levelsof delays were randomly interspersed withineach session during each step of the thinningprocedure. The levels differed in difficultybased on the number of demands or the dura-tion of the delay. Therefore, there were five
different types of trials a participant could expe-rience, and a different response was scheduledfor reinforcement on each trial. Each sessionconsisted of an equal proportion (i.e., .20) oftrials including a complex FCR, toleranceresponse, easy level demands/delay, moderatelevel demands/delay, or difficult level ofdemands/delay. The sequence of trials wasdetermined by a random number generator;however, all five trial-types had to occur beforeany of them could be repeated. Session dura-tion during reinforcement thinning wasincreased to 20 min for most participants. Ses-sions were extended to accommodate the delayinterval when the programmed delay was longerthan the session duration. The entire treatmentpackage involved the intermittent and unpre-dictable reinforcement of communication, tol-eration, and compliance chains.Social validity evaluation. Caregivers com-
pleted two questionnaires as a part of the intake
DRA-Based Reinforcement Thinning
DRO-Based Reinforcement Thinning
Access toSR blocked
Emission of FCR
No Delay (1:5)"Sure"
Tolerance (1:5)"Wait/not yet"
Emission oftolerance response
SR deliveryand
next trial
Delay (3:5)"Wait/not yet"
Emission oftolerance response
"First do x"x completed
Access toSR blocked
Emission of FCR
No Delay (1:5)"Sure"
Tolerance (1:5)"Wait/not yet"
Emission oftolerance response
SR deliveryand
next trial
Delay (3:5)"Wait/not yet"
Emission oftolerance response"Do x if you want"
No problembehavior fort seconds
Figure 2. A schematic of the procedures used during DRA-based reinforcement thinning (top panel) and DRO-based reinforcement thinning (bottom panel). Numbers in the parentheses refer to the ratio of those trials occurring in asession.
143ASSESSMENT AND TREATMENT

and discharge process in the outpatient clinic.The first questionnaire (see Supporting Informa-tion) was provided during an intake meetingand again during the discharge meeting, andincluded two sets of 40 questions related to dailysituations (e.g., school, peer interactions, mealtime) and problem behavior (e.g., aggression,self-injury, general problem behavior). The care-givers were asked to rate whether or not each sit-uation or behavior mentioned was a problem ona scale from “Almost never presents a problem”to “Presents a serious problem.” The number ofsituations and behaviors the caregivers rated asbeing a serious problem was then comparedbefore and after the child’s 2-week participationin the assessment and treatment process.The second questionnaire was administered
during the discharge meeting, and involved aset of questions concerning caregivers’ satisfac-tion with the improvements observed and howacceptable they found the recommended treat-ment. Caregivers were asked to rate all theitems on a 7-point Likert-type scale rangingfrom not acceptable/satisfied/helpful to highlyacceptable/satisfied/helpful.
Results and DiscussionThe reductions in problem behavior across
phases for each participant are presented inTable 3. Elevated rates of problem behaviorwere observed across participants during base-line (M = 1.65 RPM, SD = 0.98). During theinitial phase of the treatment evaluation, prob-lem behavior was eliminated for 18 out of25 participants. Overall, a 95% reduction inproblem behavior was observed across all par-ticipants (M = 0.04 RPM, SD = 0.09). Whenthe complex FCR was taught in the final phaseof the treatment evaluation, problem behaviorremained low (M = 0.06, SD = 0.1), with com-plete elimination observed for 60% (15 of 25)of the participants. For 48% of the participants(12 of 25), complete elimination of problembehavior was achieved during the entire FCT
treatment evaluation prior to reinforcementthinning. The rate of problem behaviorremained low during reinforcement thinning,with complete elimination observed with threeparticipants, at least 90% reduction observedwith 16 participants, and at least 80% reduc-tion across all participants.The means presented above were calculated
from complete phases. However, in previousoutcome studies, results have typically beenevaluated by calculating means using only thefinal portions of baseline and treatment phases(e.g., Greer et al., 2016; Hagopian et al., 1998;Rooker et al., 2013; Wacker et al., 1998). Forexample, the percentage reduction in problembehavior could be calculated using only the lastthree or five sessions of baseline and the lastthree or five sessions of treatment. To allow forcomparison with previous studies, we con-ducted an additional data analysis of problembehavior reduction comparing the last three ses-sions of baseline and the last three sessions oftreatment. We included the last three sessionsbecause the baseline phase for the majority ofour participants only required three points. Thetreatment outcome for each participant is pre-sented in Table 3 and summarized in Figure 3.Overall, problem behavior was largely elimi-nated for 15 participants, with the rate of prob-lem behavior for all participants reduced by atleast 90%. In addition, we used a Wilcoxonsigned-rank test to compare the rates of prob-lem behavior before and after the introductionof the treatment. The Wilcoxon signed-ranktest is a nonparametric statistical analysisdesigned to analyze two dependent sets of data(Wilcoxon, 1945). We found the results to bestatistically significant (Z = -4.37, p < .001).The terminal schedules for each participant
during reinforcement thinning are presented inTable 2. The DRA-based reinforcement thin-ning procedure was used with 15 of the 25 par-ticipants. The terminal task requirement rangedfrom 16 to 50 instructions. An example ofthe treatment process, using a DRA-based
JOSHUA JESSEL et al.144

reinforcement thinning procedure with oneparticipant, is presented in Figure 4. Johnexhibited high rates of problem behavior duringthe baseline phase (M = 3.07 RPM, SD =0.12). When the reinforcers identified duringthe functional analysis were presented contin-gent on the simple FCR, problem behavior waseliminated and elevated rates of the simpleFCR were observed (M = 1.67 RPM, SD =0.12). The reinforcers were then presented con-tingent on the complex FCR1. The problembehavior remained at zero, elevated rates of thecomplex FCR1 were observed (M = 1.4 RPM,SD = 0), but the rates of the simple FCR1dropped to zero. During the final phase ofFCT, the contingency was switched to the
complex FCR2. Stable rates of the complexFCR2 were subsequently observed (M = 1.4RPM, SD = 0), and rates of the complex FCR1were reduced to zero while problem behaviorand the simple FCR remained at zero. Thus,when and only when the reinforcement contin-gency supported a response did we observe ele-vated rates of the target response, whileresponses that were reinforced only in the pre-ceding phase decreased, and responses that werenot reinforced in the current or precedingphase remained at zero. When reinforcementthinning was introduced, John began emittingthe tolerance response (M = 1 RPM, SD =0.35) along with the complex FCR2 (M = 1.2RPM, SD = 0.2). As instructions were
Table 3Problem Behavior per Min and Percentage Reduction across Assessment and Treatment Phases for 25 Consecutive
Participants
Treatment
Treatment Evaluation
Participant Baseline (Final 3) Initial Terminal Reinforcement Thinning Outcome (Final 3)
Joe 0.6 0 (100%) 0 (100%) 0.04 (93%) 0 (100%)Anson 5.13 0.4 (92%) 0.16 (97%) 0.14 (97%) 0.03 (99%)Robin 2.13 0 (100%) 0 (100%) -- 0 (100%)Kat 1 0 (100%) 0.05 (95%) 0.13 (87%) 0 (100%)Ari 1.23 0.07 (94%) 0.01 (99%) 0.01 (99%) 0.02 (98%)
Lance 0.88 0 (100%) 0 (100%) 0.01 (99%) 0 (100%)Aaron 1.6 0 (100%) 0.3 (81%) 0.14 (91%) 0.1 (94%)Stan 1.1 0.03 (97%) 0.3 (73%) 0.15 (86%) 0 (100%)Matt 1.6 0.04 (97%) 0 (100%) 0.07 (96%) 0 (100%)Ken 3.3 0 (100%) 0 (100%) 0.14 (96%) 0.02 (99%)Tim 2.8 0 (100%) 0 (100%) 0.05 (98%) 0 (100%)Zane 2.07 0.16 (92%) 0 (100%) 0.07 (97%) 0 (100%)Kane 0.93 0 (100%) 0 (100%) 0.13 (86%) 0.02 (98%)Mike 1.27 0 (100%) 0.2 (84%) 0 (100%) 0 (100%)John 3.07 0 (100%) 0 (100%) 0.08 (97%) 0 (100%)Steve 0.67 0 (100%) 0 (100%) 0 (100%) 0 (100%)Max 1.73 0.18 (90%) 0.24 (86%) 0.08 (95%) 0.02 (99%)Alex 1.27 0 (100%) 0.12 (91%) 0.24 (81%) 0.13 (90%)Sarah 1.4 0 (100%) 0 (100%) 0 (100%) 0 (100%)Annie 0.4 0 (100%) 0.05 (88%) 0.06 (86%) 0 (100%)Dan 1.33 0 (100%) 0 (100%) 0.16 (88%) 0.08 (94%)Greg 1.56 0.13 (91%) 0 (100%) 0.18 (88%) 0.07 (96%)Dace 1.37 0 (100%) 0 (100%) 0.03 (97.8%) 0 (100%)Larry 1.27 0 (100%) 0.07 (95%) 0.23 (82%) 0.1 (92%)Ace 1.22 0 (100%) 0 (100%) 0.04 (97%) 0 (100%)Mean 1.65 0.08 (95%) 0.06 (96%) 0.1 (94%) 0.02 (99%)
Note. The number in the parentheses represents the percentage reduction from the functional analysis test condition.Outcome refers to the mean of the final three sessions from the treatment. All other means include entire data sets fromeach treatment phase.
145ASSESSMENT AND TREATMENT

presented, the variability of his problem behav-ior increased, but the mean rate remained low(M = 0.08 RPM, SD = 0.15) and compliancewas high (M = 98.4%, SD = 1.87).Six participants experienced the DRO-based
reinforcement thinning procedures, and the ter-minal requirement ranged from 30 s to 900 sfor these participants. Figure 5 shows an exam-ple of a participant who experienced the DRO-based reinforcement thinning procedures. Joe’sproblem behavior was on an increasing trendduring the baseline phase (M = 0.6 RPM, SD =0.22). When FCT was initiated, his problembehavior was eliminated, and the simple FCRincreased (M = 1.53 RPM, SD = 0.21). Ele-vated rates of the complex FCR were observed(M = 1.77 RPM, SD = 0.06) during the finalphase of FCT while problem behaviorremained at zero and the simple FCR was nolonger emitted. Following the baseline condi-tion, we observed increased rates of the FCRsonly when the reinforcers were presented con-tingent on each. In addition, the complexity ofthe FCRs increased with the increase in the setcriteria. When reinforcement thinning began,
the reinforcers were presented 50% of the timecontingent on the complex FCR and toleranceresponses. This resulted in elevated rates of thetolerance response (M = 0.93 RPM, SD =0.23), and low and stable rates of complexFCRs (M = 0.77 RPM, SD = 0.15). Delayswere introduced after Joe acquired the toleranceresponse. The duration of reinforcer access wasgradually decreased, and time without access toreinforcement was gradually increased as prob-lem behavior remained low (M = 0.05 RPM,SD = 0.08). By the final thinning level, timewithout reinforcement was 16.75 min out of a20 min session.The remaining participants experienced a
combination of DRA- and DRO-based rein-forcement thinning procedures. Figure 6 repre-sents the treatment process for Kane. Anincreasing trend in problem behavior wasobserved during the baseline phase (M = 0.56RPM, SD = 0.46). However, Kane’s problembehavior was eliminated during FCT when hewas taught the simple FCR (M = 1.4 RPM, SD= 0.2). The rate of the simple FCRs dropped tozero when the contingency was shifted to thecomplex FCR (M = 1.53 RPM, SD = 0.12). Therate of problem behavior remained at zero. Thecomplex FCR continued to occur at elevatedrates (M = 1.27 RPM, SD = 0.12) after the toler-ance response (M = 0.8 RPM, SD = 0) wasadded to the contingency, rates of problembehavior remained at zero, while simple FCRsoccurred infrequently (M = 0.13 RPM, SD =12). Throughout FCT, Kane’s problem behav-ior was reduced in comparison to the baselinecondition, and increasingly complex FCRs wereobserved when reinforcement was contingent onthem. DRA-based reinforcement thinning wasfirst introduced to increase Kane’s compliancewith simple instructions and transition-baseddemands (e.g., “stand up,” “hold hands,” “walkto [area],” “sit in chair”) because his problembehavior was sensitive to escape from transitionswhich involved losing access to preferred items.As the number of instructions was progressively
Baseline Treatment
0
2
4
6
N = 25
p < .001
Pro
ble
m b
ehav
ior
per
min
Figure 3. Mean rate of problem behavior (horizontalline) before (final three baseline) and after (final threetreatment) the introduction of treatment. Each symbolrepresents one of the 25 consecutive participants. Statisti-cal significance determined by the two-tailed Wilcoxonsigned-rank test (Z = -4.37, p < .001).
JOSHUA JESSEL et al.146

0
1
2
3
4
John
BL
FCT
Reinforcement Thinning
Sim
ple
FC
R
Co
mp
lex
FC
R1
Co
mp
lex
FC
R2
Pro
ble
m b
ehav
ior
per
min
0.5
1.0
1.5
2.0
0
Sim
ple
FC
R
per
min
5 10 15 20 25 30 35
0.5
1.0
1.5
2.0
0
20
40
60
80
100
Thinning Levels
1. Tolerance 4. 3/9/18
2. 1/1/1 5. 6/18/42
3. 1/2/3
0 1 2 3 4 5
Sessions
To
lera
nce r
esp
onse
per
min
Co
mplian
ce (%
)
0.5
1.0
1.5
2.0
0
Co
mple
x F
CR
1
per
min
0.5
1.0
1.5
2.0
0
Co
mple
x F
CR
2
per
min
Figure 4. Treatment evaluation for John who experienced the DRA-based reinforcement thinning procedures. Thevalues in the thinning levels refer to the easy/moderate/difficult set of instructions. For example, in level 5 schedule thinning,John was asked to complete 6 instructions, 18 instructions, or 42 instructions with equal probability during a session.
147ASSESSMENT AND TREATMENT

increased, Kane’s rates of problem behaviorremained low, with the exception of a burst dur-ing the first session in which he was presentedwith instructions. When Kane reached24 instructions in the trial with the highest diffi-culty, the DRO-based reinforcement thinningprocedure was added to his treatment package.Instructions to transition away from his toys todifferent areas of the building were introduced.Kane had to walk with the therapist for theentirety of the interval without problem behav-ior to avoid resetting the required time interval.By the final thinning level, Kane’s rates of prob-lem behavior remained low (M = 0.02, SD =0.02), percentage of compliance remained high(M = 98.7%, SD = 0.47), and he was experienc-ing an 11.93-min mean delay without reinforce-ment in a 20-min session.The mean percentage of session time with-
out reinforcement during the final reinforce-ment thinning level across all the participants ispresented in Figure 7. Although no durationrequirement was in place for participants whoexperienced the DRA-based reinforcementthinning procedures, an average of 51% of thesession was spent without reinforcement. Thiswas more than three times the duration duringthe initial level of FCT.The results of the pre- and post-ratings of
caregiver concerns are presented in Figure 8.Caregivers rated many situations and behaviorsas major concerns prior to the onset of theassessment and treatment process (M = 12.9,SD = 6.4). When the same measure wasobtained following the assessment and treat-ment process, there was a 76% decrease in thenumber of major concerns (M = 3.1, SD =3.4). Inversely, a 74% increase was observed inthe number of situations or behaviors that werenot considered a concern before (M = 13.0, SD= 6.1) and after (M = 22.7, SD = 8.7) the clini-cal services.Caregivers’ acceptance of the treatment and
satisfaction with the improvement observed intheir child’s behavior is presented in Figure 9.
The majority of caregivers found the treatmenthighly acceptable (M = 6.8, SD = 0.5), withonly two caregivers scoring the treatment lowerthan 7 out of 7. In addition, most of the care-givers were satisfied with the overall amount ofimprovement seen in their child’s problembehavior (M = 6.5, SD = 0.7) and communica-tion skills (M = 6.3, SD = 0.8). Lastly, parentsalso found the treatment to be very helpfulwith improving behavior in the home (M =6.9, SD = 0.3).
We found FCT with contingency-basedreinforcement thinning informed by an IISCAto be an effective treatment across 25 clinicalcases. At least a 90% reduction in problembehavior was obtained across all participantswithin a 1-week period. These treatment proce-dures and improvements in problem behaviorand appropriate communication were ratedhighly acceptable, satisfactory, and helpful bycaregivers. These results show that function-based treatments informed by the IISCA areeffective for treating severe problem behavior.The positive results of the assessment and treat-ment process were replicated with children andadolescents, with and without multiple diagno-ses, and with a range of language abilities.Therefore, the current study extends the gener-ality of the assessment and treatment processesbased on the IISCA.It is difficult to determine at what point dur-
ing the reinforcement thinning process theschedule of reinforcement reaches a level that issustainable in the classroom or home environ-ment. Although most of the participantsreached a terminal goal likely to be acceptablefollowing their participation, some were able toreach a treatment schedule of only modestdelay. For example, Anton’s terminal delayinterval was 30 s. In the current model, partici-pation was restricted to a fixed duration of2 weeks, and some participants may haverequired more time to reach larger delay inter-vals. In such cases, we provided information tothe parents during parent training on (a) the
JOSHUA JESSEL et al.148

0.0
0.5
1.0
1.5
Joe
Reinforcement ThinningBL
FCT
Sim
ple
FC
R
Co
mp
lex
FC
R
Pro
ble
m b
ehav
ior
per
min
0.0
0.5
1.0
1.5
2.0
Sim
ple
FC
R p
er
min
10 20 30 40 50
0.0
0.5
1.0
1.5
2.0
0
500
1000
1500
1 24
5
Thinning Levels
1. Tolerance 4. 5/30/60 s
2. 1/3/5 s 5. 5/60/180 s
3. 1/15/30 s 6. 5/180/300 s
6
3
Sessions
To
lera
nce r
esp
onse
per
min
Experie
nced D
elay
(s)
0.0
0.5
1.0
1.5
2.0
Co
mple
x F
CR
per
min
Figure 5. Treatment evaluation for Joe who experienced the DRO-based reinforcement thinning procedures. Thevalues in the thinning levels represent the easy/moderate/difficult delay intervals. For example, in level 6 schedule thin-ning, Joe was told to wait for 5 s, 180 s, or 300 s with equal probability during a session.
149ASSESSMENT AND TREATMENT

rationale and goals of reinforcement thinning,(b) the procedures and criteria we used to thinreinforcement, and (c) indicators of when it issafe to thin the schedule of reinforcement orwhen to return to an earlier schedule require-ment. Nevertheless, future research should beconducted on evaluating procedures for trans-ferring these treatments to caregivers and tohomes and classrooms.Although the brief time required to achieve
these socially validated effects may be consid-ered a strength of the study, it may not be fea-sible for practitioners to devote 7 hr per day,5 days per week to one patient. Hanleyet al. (2014) achieved similar outcomes withthree participants diagnosed with ASD in 22 to32 (M = 27) 1-hr outpatient and home consul-tations, which lasted a total of 8 to 14 (M =11.3) weeks. Thus, the results obtained aremore likely to be due to the effectiveness of theIISCA and treatment processes than the partic-ular distribution of the intervention process.Practitioners may be able to choose the sched-ule that best fits their situation, knowing thatbetween 20 and 35 hours of therapy will proba-bly be needed for an effective outcome.To better understand how the current results
relate to other function-based treatment out-come studies, we compared the results and theprocesses to achieve them in the current studyto three other outcome studies (see Figure 10).No supplemental procedures (i.e., punishment,alternative reinforcement) were required toachieve satisfactory outcomes for the 25 partici-pants in the current study. Most of the applica-tions (22 of 25) in Greer et al. (2016) also didnot require supplemental procedures. By con-trast, approximately 50% of the applications inHagopian et al. (1998) and Rookeret al. (2013) that involved FCT and reinforce-ment thinning required the addition of supple-mental procedures. We then compared thepercentage of cases resulting in at least 80-, 90-, or 95% reductions in problem behavior acrossthe four studies (Figure 10; reductions were
assessed prior to schedule thinning [top panel],and following schedule thinning [bottompanel]). The current study had the highest per-centage of applications with ≥ 80% reductionsin problem behavior, followed by Greeret al. (2016), Rooker et al. (2013), and Hago-pian et al. (1998). The same pattern wasobserved when considering the reductions fol-lowing reinforcement thinning (bottom panel),with the exception that Hagopian et al. hadslightly more applications with ≥ 95% reduc-tions in problem behavior compared to Roo-ker et al.The current study differed from the previous
outcome studies in multiple ways; therefore, itis difficult to determine what contributed tothe comparatively better outcomes from thisstudy. Improved treatment outcomes could beaccounted for by considering evaluation cri-teria. Many studies have used a more conserva-tive measure (e.g., final five sessions instead offinal three) when calculating the percentagereduction in problem behavior from baseline totreatment. There is precedence for includingthree sessions (Wacker et al., 1998), and in thecurrent study, this measure was chosen forpractical reasons, because the IISCA often onlyincluded three sessions in the test condition.Nevertheless, these differing criteria may affectdifferences across outcome studies. It is possiblethat the participant samples differed in funda-mental ways, and that these differences mayaccount for the differences in outcomes. It isalso possible and just as plausible that the dif-ferences in the assessment and treatment proce-dures were responsible for the observeddifferences.Regarding assessment, the functional analysis
procedures for all of the previous outcomestudies were identical and cited the standardformat from Iwata et al. (1982/1994). We con-ducted a particular type of functional analysis,and IISCA, that differed from the standardfunctional analysis format, and this changecould have resulted in improved treatment
JOSHUA JESSEL et al.150

0.5
1.0
1.5BL
FCT
Reinforcement Thinning
Sim
ple
FC
R
Co
mp
lex
FC
R
Kane
0
Pro
ble
m b
ehav
ior
per
min
0.5
1.0
1.5
2.0
0
Sim
ple
FC
R
per
min
0.5
1.0
1.5
2.0Thinning Levels
1. Tolerance 4. 1/3/6 7. 1/12/24+30/60/90 s
2. 1/1/1 5. 1/6/12 8. 1/12/24+30/90/180 s
3. 1/2/3 6. 1/12/24 9. 1/12/24+30/180/300 s
0 1 2 3 4 5 6 7 8 9To
lera
nce r
esp
onse
per
min
0.5
1.0
1.5
2.0
0
Co
mple
x F
CR
per
min
5 10 15 20 25 30 35 40
20
40
60
80
100
0
200
400
600
800
0
Sessions
Co
mpli
ance (
%)
Experie
nced D
elay
(s)
Figure 6. Treatment evaluation for Kane who experienced both the DRA- and DRO-based reinforcement thinningprocedures. The values in the thinning levels represent the easy/moderate/difficult set of instructions and the easy/mod-erate/difficult delay intervals. For example, in level 9 schedule thinning, Kane was asked to complete 1 instruction,12 instructions, or 24 instructions and asked to wait for 30 s, 180 s, and 300 s with equal probability during a session.
151ASSESSMENT AND TREATMENT

effects. Some support for this comes from Sla-ton et al. (2017) who observed better treatmentoutcomes from the IISCA than from a standardanalysis for participants who experienced both.The critical differences are probably thosetacted in the name of the analysis—the inclu-sion of personalized reinforcement contingen-cies that are informed from an interview andthe synthesis of those contingencies into a sin-gle context that is used as the basis for teachingskills. Regarding treatment, all participants wereexposed to contingency-based reinforcementthinning procedures in the current study. Incontrast, previous studies often included time-based thinning (e.g., Hagopian et al., 1998) ormultiple schedules during reinforcement thin-ning (e.g., Greer et al., 2016). In a within-subject comparison of variations in time-baseddelays and contingency-based reinforcementthinning, Ghaemmaghami et al. (2016) foundcontingency-based procedures to result ingreater reductions in problem behavior,reduced likelihood of collateral responding(e.g., excessive manding), and increases in expe-rienced delays to reinforcement with four par-ticipants. In the context of treatingautomatically reinforced stereotypy, Slaton andHanley (2016) recently showed that strongstimulus control over appropriate and problembehavior was not achieved with multiple sched-ules but was achieved with chained schedulesfor the same participants (participants also pre-ferred the chained schedule over the multipleschedule). Of course, the functional analysisprocedures and the contingency-based thinningmay have interacted to produce improvedoutcomes.There were other procedural differences
between the current and previous studies thatmay have enhanced treatment outcomes. Forexample, the participants were taught multipleforms of communication of increasing com-plexity in the current study. Besides the socialand developmental appropriateness of teachingchildren multiple ways of communicating,
0
20
40
60
80
Pre-
ThinningPost-
Thinning
N = 25
Perc
enta
ge o
f se
ssio
n
wit
ho
ut
rein
forc
em
ent
Figure 7. Mean percentage of session without rein-forcement before and after the introduction of reinforce-ment thinning. Pre-thinning refers to the mean of theFCT sessions before tolerance was introduced. Post-thinning refers to the mean of the sessions of the finalreinforcement thinning level.
0
5
10
15
20N = 25
Num
ber
of
Are
as
Rat
ed a
s a
Maj
or
Co
ncern
Intake Discharge
0
10
20
30
40
Num
ber
of
Are
as
Rat
ed a
s N
ot
a C
oncern
Figure 8. The mean number of settings and behaviorsrated as major concerns (top panel) and not a concern(bottom panel) before and after the patients’ participation.Error bars represent standard error measurement (SEM).
JOSHUA JESSEL et al.152

teaching multiple and more complex FCRsmay have therapeutic value as well. In a transla-tional evaluation, Lambert, Bloom, Samaha,
Dayton, and Rodewald (2015) taught threeadults with developmental disabilities to emitarbitrary responses using traditional DRA orwith serial alternative response training. Theserial alternative response training involvedsequentially reinforcing and extinguishing threedifferent alternative responses. When all behav-ior was placed on extinction, Lambertet al. (2015) found that the target response wasmore likely to resurge in the traditional DRAcondition in which only one response wastaught. Our arrangement was similar in that wesequentially taught different mands of increas-ing complexity while placing the previousforms on extinction.
GENERAL DISCUSSION
We found that the IISCA enabled us toaddress the core objectives of a functional anal-ysis (Hanley, 2012). The IISCA established anunderstanding of problem behavior by identify-ing socially mediated variables maintainingproblem behavior with 25 patients. The IISCAtest condition served as an appropriate baselinefor subsequent treatment evaluations, and thereinforcement contingencies from the IISCAprovided a highly motivating instructional con-text, as shown by the successful replacement of
1 2 3 4 5 6 7
You found the recommended treatment acceptable
You are satisfied with the amount ofimprovement seen in problem behavior
You are satisfied with the amountof improvement seen in
communication skills
You found the assessment andtreatment helpful to your home situation
Notacceptable/satisfied/helpful
Highlyacceptable/satisfied/helpfulCaregiver Rating
Figure 9. Each symbol represents an individual rating by a caregiver. The mean caregiver ratings (vertical line) oftreatment acceptability, performance improvement, and helpfulness.
>80% >90% >95%
Current Study
Greer et al.
(2016)
Rooker et al.
(2013)
Hagopian et al.
(1998) Pre Sr Thinning
Reduction in Problem Behavior:
n = 25
n = 25
n = 58
n = 25
0 20 40 60 80 100
Current Study
Greer et al.
(2016)
Rooker et al.
(2013)
Hagopian et al.
(1998) Post Sr Thinning
n = 22
n = 25
n = 29
n = 12
Percentage of applications
Publi
cat
ions
Figure 10. Percentage of applications in each outcomestudy with greater than 80% (white), 90% (gray), and95% (black) reductions in problem behavior before (toppanel) and after reinforcement thinning (bottom panel).Only applications that involved FCT with extinction andno supplemental procedures were included in thiscomparison.
153ASSESSMENT AND TREATMENT

problem behavior with multiple forms ofsocially appropriate communication responsesof increasing complexity. Perhaps most impor-tant was that we observed large reductions inproblem behavior across all participants by theend of reinforcement thinning. In other words,this study illustrates both what is possible aswell as what is probable when an IISCA is usedto develop FCT and contingency-based sched-ule thinning procedures to treat severe problembehavior.The results of Study 1 directly replicate the
IISCAs from Jessel et al. (2016) and Slatonet al. (2017) in that all were efficient, with themajority being conducted in 30 min or less. Ina recent survey of 700 practicing behavior ana-lysts, Oliver et al. (2015) found that 63%reported never or almost never using a func-tional analysis. The views of 205 practitionersin Massachusetts mirrored this sentiment, whena majority of them reported choosing descrip-tive assessment over functional analyses (Roscoeet al., 2015). Thus, practitioners are choosingefficient assessments in the absence of analysiseven though they are known to be unreliable(Iwata et al., 2013) and of uncertain treatmentutility (Hanley, 2012). Follow-up surveys in5 to 10 years will help to determine if prefer-ences for assessments change with the introduc-tion of more efficient and valid functionalanalysis formats, like the IISCA.Despite the experimental imprecision of the
IISCA, we found in Study 2 that the IISCAallowed for effective and socially valid treat-ment outcomes. In fact, IISCA-informed treat-ments seemed to result in improved treatmenteffects in comparison to other formats. In theoutcome study by Greer et al. (2016), supple-mental procedures using arbitrary reinforce-ment were required in 20% of the applicationsof FCT during reinforcement thinning. Rookeret al. (2013) found similar results, with 23% ofapplications requiring supplemental reinforce-ment or punishment procedures when FCTalone failed to reduce problem behavior. None
of the patients in the current study requiredsupplemental treatment procedures, and thereductions in problem behavior were achievedusing only the reinforcers identified via theIISCA. However, more single-subject compari-sons of treatments informed by each functionalanalysis format, like that modeled by Slatonet al. (2017) are needed. As of now, the IISCAhas sufficient evidence to support its utility indeveloping an effective function-based treat-ment in the same time it would take to con-duct a typical 30-60 min indirect assessment.The IISCA provides an empirical demonstra-tion of functional control over problem behav-ior, a baseline from which to evaluatetreatment, and a motivating context to shapeappropriate behavior, whereas an indirectassessment of equal duration provides none ofthese. Thus, we argue that the concern that afunctional analysis requires too much time isno longer relevant. An IISCA is time-efficientand has demonstrated utility for designingtreatments. Practitioners can therefore remaincommitted to an empirical and analytic under-standing of problem behavior prior to itstreatment.It should also be recognized that ecological
validity was strong throughout the assessmentand treatment process, because caregivers pro-vided the qualitatively rich information guidinganalysis and treatment decisions. A specificproblematic context occasioning problembehavior in the home or school was arranged inthe test condition of the functional analysis. Inaddition, the participants were taught to com-ply with tasks or engage in alternative activitiesnominated by caregivers as areas of concernwhen functional reinforcers were not available.Structuring the assessment and treatment con-text to fit the environment specified by thecaregivers may reduce the effort of treatmentimplementation in other contexts. For example,there are no additional reinforcers, punishers,or materials needed (e.g., red/green boards sig-naling when reinforcement is available) given
JOSHUA JESSEL et al.154

that the interactions in treatment are similar tothose that were occurring on a daily basis withthe important exception being the timing ofthe delivery of the synthesized reinforcers. Nev-ertheless, measurement of caregiver treatmentfidelity during training and evaluations ofadherence to the procedures following dischargeare necessary in future work.In addition, social validity measures should
continue following discharge, and multipleglobal outcomes such as IQ, classroom perfor-mance, adaptive functioning, and quality of lifeshould be measured following discharge todetermine the broader effects treatment ofproblem behavior may have for the patient andhis or her family.
REFERENCES
Austin, J. L., Groves, E. A., Reynish, L. C. &Francis, L. L. (2015). Validating trial-based func-tional analyses in mainstream primary school class-rooms. Journal of Applied Behavior Analysis, 48, 274-288. https://doi.org/10.1002/jaba.208
Campbell, J. M. (2003). Efficacy of behavioral interven-tions for reducing problem behavior in persons withautism: A quantitative synthesis of single-subjectresearch. Research in Developmental Disabilities, 24,120-138. https://doi.org/10.1016/S0891-4222(03)00014-3
Carr, E. G., & Durand, V. M. (1985). Reducing behaviorproblems through functional communication train-ing. Journal of Applied Behavior Analysis, 18, 111-126. https://doi.org/10.1901/jaba.1985.18-111
Charlop, M. H., Schreibman, L., & Thibodeau, M. G.(1985). Increasing spontaneous verbal responding inautistic children using a time delay procedure. Journalof Applied Behavior Analysis, 18, 155-166. https://doi.org/10.1901/jaba.1985.18-155
Fisher, W. W., Greer, B. D., Romani, P. W.,Zangrillo, A. N., & Owen, T. M. (2016). Compari-sons of synthesized and individual reinforcement con-tingencies during functional analysis. Journal ofApplied Behavior Analysis, 49, 596-616. https://doi.org/10.1002/jaba.314
Ghaemmaghami, M., Hanley, G. P., & Jessel, J. (2016).Contingencies promote delay tolerance. Journal ofApplied Behavior Analysis, 49, 548-575. https://doi.org/10.1002/jaba.333
Ghaemmaghami, M., Hanley, G. P., Jin, S. C., &Vanselow, N. R. (2015). Affirming control by multi-ple reinforcers via progressive treatment analysis.
Behavioral Interventions, 31, 70-86. https://doi.org/10.1002/bin.1425
Greer, B. D., Fisher, W. W., Saini, V., Owen, T. M., &Jones, J. K. (2016). Functional communication train-ing during reinforcement schedule thinning: An anal-ysis of 25 applications. Journal of Applied BehaviorAnalysis, 49, 105-121. https://doi.org/10.1002/jaba.265
Hagopian, L. P., Fisher, W. W., Sullivan, M. T.,Acquisto, J., & LeBlanc, L. A. (1998). Effectivenessof functional communication training with and with-out extinction and punishment: A summary of21 inpatient cases. Journal of Applied BehaviorAnalysis, 31, 211-235. https://doi.org/10.1901/jaba.1998.31-211
Hanley, G. P. (2012). Functional assessment of problembehavior: Dispelling myths, overcoming implementa-tion obstacles, and developing new lore. BehaviorAnalysis in Practice, 5, 54-72.
Hanley, G. P., Iwata, B. A., & McCord, B. E. (2003).Functional analysis of problem behavior: A review.Journal of Applied Behavior Analysis, 36, 147-185.https://doi.org/10.1901/jaba.2003.36-147
Hanley, G. P., Jin, C. S., Vanselow, N. R., &Hanratty, L. A. (2014). Producing meaningfulimprovements in problem behavior of children withautism via synthesized analyses and treatments. Jour-nal of Applied Behavior Analysis, 47, 16-36. https://doi.org/10.1002/jaba.106
Heyvaert, M., Saenen, L., Campbell, J. M., Maes, B., &Onghena, P. (2014). Efficacy of behavioral interven-tions for reducing problem behavior in persons withautism: An updated quantitative synthesis of single-subject research. Research in DevelopmentalDisabilities, 35, 2463-2476. https://doi.org/10.1016/j.ridd.2014.06.017
Iwata, B. A., DeLeon, I. G., & Roscoe, E. M. (2013).Reliability and validity of the functional analysisscreening tool. Journal of Applied Behavior Analysis,46, 271-284. https://doi.org/10.1002/jaba.31
Iwata, B. A., Dorsey, M. F., Slifer, K. J.,Bauman, K. E., & Richman, G. S. (1994). Toward afunctional analysis of self-injury. Journal of AppliedBehavior Analysis, 27, 197-209. (Reprinted fromAnalysis and Intervention in Developmental Disabilities,2, 3-20, 1982) https://doi.org/10.1901/jaba.1994.27-197
Iwata, B. A., & Dozier, C. L. (2008). Clinical applicationof functional analysis methodology. Behavior Analysisin Practice, 1, 3-9. http://doi.org/10.1007/BF03391714
Jessel, J., Hanley, G. P., & Ghaemmaghami, M. (2016).Interview-informed synthesized contingency analyses:Thirty replications and reanalysis. Journal of AppliedBehavior Analysis, 49, 576-595. https://doi.org/10.1002/jaba.316
Kahng, S., Iwata, B. A., & Lewin, A. B. (2002). Behav-ioral treatment of self-injury, 1964-2000. American
155ASSESSMENT AND TREATMENT

Journal on Mental Retardation, 107, 212-221.https://doi.org/10.1352/0895-8017(2002)107<0212:BTOSIT>2.0.CO;2
Kazdin, A. E. (1982). Single-case research designs: Methodsfor clinical and applied settings. New York, NY:Oxford University Press.
Kurtz, P. F., Boelter, E. W., Jarmolowicz, D. P.,Chin, M. D., & Hagopian, L. P. (2011). An analysisof functional communication training as an empiri-cally supported treatment for problem behavior dis-played by individuals with intellectual disabilities.Research in Developmental Disabilities, 32, 2935-2942. https://doi.org/10.1016/j.ridd.2011.05.2009
Kurtz, P. F., Chin, M. D., Huete, J. M.,Tarbox, R. S. F., O’Connor, J. T.,Paclawskyj, T. R., & Rush, K. S. (2003). Functionalanalysis and treatment of self-injurious behavior inyoung children: A summary of 30 cases. Journal ofApplied Behavior Analysis, 36, 205-219. https://doi.org/10.1901/jaba.2003.36-205
Lambert, J. M., Bloom, S. E., Samaha, A. L.,Dayton, E., & Rodewald, A. M. (2015). Serial alterna-tive response training as intervention for target responseresurgence. Journal of Applied Behavior Analysis, 48,765-780. https://doi.org/10.1002/jaba.253
Lambert, J. M., Staubitz, J. E., Roane, J. T., Houchins-Juárez, N. J., Juárez, A. P., Sanders, K. B., &Warren, Z. E. (2017). Outcome summaries oflatency-based functional analyses conducted in hospi-tal inpatient units. Journal of Applied Behavior Analysis,50, 487-494. https://doi.org/10.1002/jaba.399
Lerman, D. C., & Iwata, B. A. (1993). Descriptive andexperimental analyses of variables maintaining self-injurious behavior. Journal of Applied Behavior Analysis,26, 293-319. http://doi.org/10.1901/jaba.1993.26-293
McComas, J. J., & Mace, F. C. (2000). Theory and prac-tice in conducting functional analysis. InE. S. Shapiro & T. R. Kratochwill (Eds.), Behavioralassessment in schools (pp. 78-103). New York, NY:The Guildford Press.
Nevin, J. A., & Shahan, T. A. (2011). Behavioralmomentum theory: Equations and applications. Jour-nal of Applied Behavior Analysis, 44, 877-895.https://doi.org/10.1901/jaba.2011.44-877
Northup, J., Wacker, D., Sasso, G., Steege, M.,Cigrand, K., Cook, J., & DeRaad, A. (1991). A brieffunctional analysis of aggressive and alternative behav-ior in an outclinic setting. Journal of Applied BehaviorAnalysis, 24, 509-522. https://doi.org/10.1901/jaba.1991.24-509.
Oliver, A. C., Pratt, L. A., & Normand, M. P. (2015). Asurvey of functional behavior assessment methodsused by behavior analysts in practice. Journal ofApplied Behavior Analysis, 48, 817-829. https://doi.org/10.1002/jaba.256
Rooker, G. W., Jessel, J., Kurtz, P. F., & Hagopian, L. P.(2013). Functional communication training with and
without alternative reinforcement and punishment:An analysis of 58 applications. Journal of AppliedBehavior Analysis, 46, 708-722. https://doi.org/10.1002/jaba.76
Roscoe, E. M., Phillips, K. M., Kelly, M. A.,Farber, R., & Dube, W. V. (2015). A statewide sur-vey assessing practitioners’ use and perceived utilityof functional assessment. Journal of Applied BehaviorAnalysis, 48, 830-844. https://doi.org/10.1002/jaba.259
Santiago, J. L., Hanley, G. P., Moore, K., & Jin, C. S.(2016). The generality of interview-informed func-tional analyses: Systematic replications in school andhome. Journal of Autism and Developmental Disorders,46, 797-811. https://doi.org/10.1007/s10803-015-2617-0
Sigafoos, J., & Saggers, E. (1995). A discrete-trialapproach to the functional analysis of aggressivebehaviour in two boys with autism. Australia &New Zealand Journal of Developmental Disabilities,20, 287-297. https://doi.org/10.1080/07263869500035621
Slaton, J. D., & Hanley, G. P. (2016). Effects of multipleversus chained schedules on stereotypy and itemengagement. Journal of Applied Behavior Analysis, 49,927-946. https://doi.org/10.1002/jaba.345
Slaton, J. D., Hanley, G. P., & Raftery, K. J. (2017).Interview-informed functional analyses: A comparisonof synthesized and isolated components. Journal ofApplied Behavior Analysis, 50, 252-277. https://doi.org/10.1002/jaba.384
Strand R. C. W., & Eldevik, S. (2017). Improvements inproblem behavior in a child with autism spectrumdiagnosis through synthesized analysis and treatment:A replication in an EIBI home program. BehavioralInterventions, 1-10. https://doi.org/10.1002/bin.1505
Thomason-Sassi, J. L., Iwata, B. A., Neidert, P. L., &Roscoe, E. M. (2011). Response latency as an index ofresponse strength during functional analyses of prob-lem behavior. Journal of Applied Behavior Analysis, 44,51-67. https://doi.org/10.1901/jaba.2011.44-51.
Tiger, J. H., Hanley, G. P., & Bruzek, J. (2008). Func-tional communication training: A review and practi-cal guide. Behavior Analysis in Practice, 1, 16-23.
Wallace, M. D., & Iwata, B. A. (1999). Effects of sessionduration on functional analysis outcomes. Journal ofApplied Behavior Analysis, 32, 175-183. https://doi.org/10.1901/jaba.1999.32-175
Wacker, D. P., Berg, W. K., Harding, J. W.,Derby, K. M., Asmus, J. M., & Healy, A. (1998).Evaluation and long-term treatment of aberrant behav-ior displayed by young children with disabilities.Developmental and Behavioral Pediatrics, 19, 260-266.
Wilcoxon, F. (1945). Individual comparisons by rankingmethods. Biometrics Bulletin, 1, 80-83.
Winborn, L., Wacker, D. P., Richman, D. M.,Asmus, J., & Geier, D. (2002). Assessment of mandselection for functional communication training
JOSHUA JESSEL et al.156

packages. Journal of Applied Behavior Analysis, 35,295-298. https://doi.org/10.1901/jaba.2002.35-295
Received September 29, 2016Final acceptance December 18, 2017Action Editor, John Borrero
SUPPORTING INFORMATION
Additional Supporting Information may befound in the online version of this article at thepublisher’s website.
157ASSESSMENT AND TREATMENT