agenda (revised) - welcome to lewisham ccg papers/prim… · agenda (revised) a meeting of the ......
TRANSCRIPT

AGENDA (revised)A meeting of the Primary Care Commissioning Committee in public
Date: Tuesday 25th April 2017 Time: 11.30 – 13:30 Venue: Rooms 1 & 2, Cantilever House, Eltham Road, London SE12 8RN Chair: Shelagh Kirkland, Governing Body Lay Member, Primary Care
Enquiries to: Hannah Reeves Telephone: 020 3049 3248 Email: [email protected]
Voting Members
Name Role Shelagh Kirkland Chair Vacancy Vice Chair: Lay Member – Patient Public Engagement Ray Warburton Lay Member - Chair of the Audit Committee and Conflicts of Interest Guardian Dr Marc Rowland LCCG Chair Dr Faruk Majid Clinical Director Dr Jacqueline McLeod Clinical Director Alison Browne Registered Nurse Member Martin Wilkinson LCCG Chief Officer Tony Read LCCG Chief Financial Officer Diana Braithwaite LCCG Director of Commissioning & Primary Care
a. 3 x Lay Memberso Chair: Lay Member for Primary Careo Vice Chair: Lay Member responsible for Patient Public Engagemento Lay Member: Chair of the Audit Committee and Conflicts of Interest Guardian
b. CCG Chairc. 2 Governing Body GP Membersd. Registered Nurse or Secondary Care Specialist (single member)e. CCG Chief Officerf. CCG Chief Financial Officerg. Director of Commissioning & Primary Care
Non-Voting Members
a. Local Medical Committee Representativeb. Healthwatch Representativec. Local Authority Representative of the Health and Wellbeing Board (Elected Member or Mandated
Officer)d. Officers as required to undertake business of the committeee. NHS England Representative
Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson 1
1 of 114
Quorum 1. The quorum shall be a minimum of 4 members, of which 2 must be Lay Members.
2. Where a quorum cannot be convened from the membership, owing to arrangements for themanagement of conflicts of interest or potential conflicts of interest; the Chair of the meeting willcomply with the conflicts of interest policy.
3. This may result in;
a. The meeting being deferredb. A discussion being undertaken but the decision deferred until the next meetingc. Discussion being undertaken being deferred to the Governing Body
Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson 2
2 of 114
Order of Business
No. Time Item Papers Presented by
1. 11:30 Welcome and introductions Chair
2. 11:35 Apologies for absence Chair
3. 11:40 Declarations of Interest Members should discuss any potential conflicts of interest with the Chair prior to the meeting.
There is a pecuniary interest on Agenda Item 4 and 8 for Dr Marc Rowland, Dr Jacky McLeod and Dr Faruk Majid.
Chair
4. 11:45 Minutes: Primary Care Joint Committee – 08/02/2017 Item removed - minutes will be published on the CCG website once agreed
Chair
5. 11:55 Matters arising 5.1 To note: Primary Care Joint Committee Urgent
Unplanned Decision 30.03.2017 – Belmont Hill Surgery merger with the Central Lewisham Care Partnership
Enc 2
Chair
Governance
6. 12:00 Level 3 – Delegated Commissioning 6.1 Primary Care Commissioning Committee Terms of
Reference (To note) 6.2 Memorandum of Understanding; (a) Southwark CCG
and Lewisham CCG (To note) 6.3 Supporting Structures (For discussion)
Enc 3a&b
Enc 3c
Victoria Medhurst
Diana Braithwaite
Decisions
7. 12:15 PMS Premium Commissioning Intentions: Update
Conflict of Interest – Mitigation: No financial information or specific detail on the proposed KPIs or service specifications associated with the PMS contract to be discussed
Enc 4 Ian Ross
8. 12:25 Membership Engagement in Clinical Commissioning – Local Improvement Scheme
Conflict of Interest – Mitigation: GP Members will not be permitted to vote on this item as it pertains to payments to individual GP Practices.
Enc 5 Charles Malcolm-Smith
Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson
3
3 of 114
9. 12:35 Care Quality Commission Inspections – Contractual Actions
9.1 Clifton Rise Family Practice 9.2 Sydenham Surgery 9.3 Torridon Road Medical Practice
Enc 6 a-c
Diana Braithwaite
To Note
10. 12:55 Special Allocation Scheme: Violent Patients Enc 7 Ian Ross
11. 13:10 GP Forward View (GPFV): Implementation Update Enc 8 Diana Braithwaite
12. 13:15 Primary Care Developments Enc 9 Diana Braithwaite
13. 13:25 AOB Chair
13. 13:30 Meeting Close Chair
Date of the next meeting: Tuesday 20th June 2017
Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson
4
4 of 114
Managing Conflicts of Interest: Governing Body, committees, sub-committees and working groups 1. The chair of the Governing Body and chairs of committees, subcommittees and working groups will ensure that
the relevant register of interest is reviewed at the beginning of every meeting, and updated as necessary.
2. The chair of the meeting has responsibility for deciding whether there is a conflict of interest and the appropriate course of corresponding action. In making such decisions, the chair may wish to consult the member of the governing body who has responsibility for issues relating to governance.
3. All decisions, and details of how any conflict of interest issue has been managed, should be recorded in the minutes of the meeting and published in the registers.
4. Where certain members of a decision-making body (be it the governing body, its committees or sub-committees, or a committee or sub-committee of the CCG) have a material interest, they should either be excluded from relevant parts of meetings, or join in the discussion but not participate in the decision-making itself (i.e., not have a vote).
5. In any meeting where an individual is aware of an interest, previously declared or otherwise, in relation to the scheduled or likely business of the meeting, the individual concerned will bring this to the attention of the chair, together with details of arrangements which have been confirmed by the governing body for the management of the conflict of interests or potential conflict of interests. Where no arrangements have been confirmed, the chair may require the individual to withdraw from the meeting or part of it. The new declaration should be made at the beginning of the meeting when the Register of Interests is reviewed and again at the beginning of the agenda item.
6. Where the chair of any meeting of the CCG, including committees, sub-committees, or the governing body, has a personal interest, previously declared or otherwise, in relation to the scheduled or likely business of the meeting, they must make a declaration and the deputy chair will act as chair for the relevant part of the meeting. Where arrangements have been confirmed with the governing body for the management of the conflict of interests or potential conflicts of interests in relation to the chair, the meeting must ensure these are followed. Where no arrangements have been confirmed, the deputy chair may require the chair to withdraw from the meeting or part of it. Where there is no deputy chair, the members of the meeting will select one.
7. Where significant numbers of members of the governing body, committees, sub committees and working groups are required to withdraw from a meeting or part of it, owing to the arrangements agreed by the Governing Body for the management of conflicts of interest or potential conflicts of interest, the remaining chair will determine whether or not the discussion can proceed.
8. In making this decision the chair will consider whether the meeting is quorate, in accordance with the number and balance of membership set out in the CCG’s standing orders or the relevant terms of reference. Where the meeting is not quorate, owing to the absence of certain members, the discussion will be deferred until such time as a quorum can be convened. Where a quorum cannot be convened from the membership of the governing body, committees, sub committees and working groups owing to the arrangements for managing conflicts of interest or potential conflicts of interest, the chair may invite on a temporary basis one or more of the following to make up the quorum so that the CCG can progress the item of business:
(a) an individual GP or a non-GP partner from a member practice who is not conflicted (b) a member of the Lewisham Health and Wellbeing Board; (c) If quorum cannot be achieved by (a) or (b) (above) a member of a governing body of another clinical
commissioning group.
9. These arrangements will be recorded in the minutes.
Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson
5
5 of 114
1
Lewisham Primary Care Joint Committee (PCJC) Meeting
URGENT PLANNED DECISION
DATE OF MEETING: 30th March 2017
Title: BUSINESS CASE FOR PROPOSED PARTNERSHIP MERGER IN LEWISHAM
AUTHOR: Debbie Power, Senior Commissioning Manager, NHS England (London) and Jill Webb, Head of Primary Care, SE London, NHS England (London)
E-Mail: [email protected]
SUMMARY:
The accompanying business case builds on the initial business case for the merger between Brockley Road Medical Centre, Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and St John’s Medical Centre (to form the Central Lewisham Care Partnership), which was agreed at the Lewisham Primary Care Joint Committee held on the 8th February 2017 (full papers at http://www.lewishamccg.nhs.uk/about-us/how-we-work/PCJC%20docs/SE%20London%20PCJCs%20meeting%2020170208.pdf)
This business case concerns the addition of the Belmont Hill Surgery to the Central Lewisham Care Partnership model and aligns to the original business case where the potential inclusion of Belmont Hill Surgery was referenced in section 1.
Appendix 6 of the original business case gives an overview of the post launch activities including key milestones and responsibilities. There has been a two month slippage against the original plan and as such the implementation date for the original scheme which was the 1st April 2017 has been deferred to the 1st June 2017. It is proposed that the inclusion of Belmont Hill Surgery in the super partnership takes place on the same date. An updated programme plan is enclosed as Appendix 2 to the business case.
As in the original business case approved on 8th February, the practices propose to work under a ‘super partnership model’, initially retaining each of the current PMS contracts held by the 6 existing practices, which the new entity will hold in trust; and at a later stage moving on to one PMS contract, or the partnership will consider the new voluntary Multispecialty Community Provider contract.
Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
6 of 114

2
This means that the 6 current PMS contracts will remain initially as separate contracts but benefiting from the integration of clinical and access services and systems. The date of the full merger into one contractual model has not yet been agreed although the current programme plan for post April 2017 has identified that an assessment of the contract merger is scheduled for January-March 2018. The practices propose that full merger will take place ‘when the health and care environment delivers the necessary stability to achieve this’. The approval of the original business case included a number of conditions. These conditions and the practice response are referenced at section 17 of the accompanying business case and summarised below. The business case identifies specific areas of performance variation for Belmont Hill Surgery including GP patient survey results, some QOF indicators and access issues. Plans to address these are included at section 5 of the business case as well as part of the updated programme plan. The business case fits strategically with the both local and national priorities and is supported by NHS Lewisham Clinical Commissioning Group (CCG). Lewisham LMC & the Healthier Communities Select Committee (HCSC) have not previously raised any concerns, although a follow up agenda item to discuss Belmont Hill’s addition to the merger has been added to the 26th April 2017 HCSC meeting. The following documentation is attached; a. completed criteria for considering a request for Practice Merger (Attachment A) b. business case for proposed Belmont Hill and Central Lewisham Care Partnership merger,
including Appendix 1 ‘Practice Profiles’ and Appendix 2 ‘updated programme plan’ (Attachment B)
KEY ISSUES: As described, this business case is supplementary to the initial business case for the merger between Brockley Road Medical Centre, Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and St John’s Medical Centre (to form the Central Lewisham Care Partnership). That business case was agreed at the Lewisham Primary Care Joint Committee held on the 8th February 2017 subject to a number of conditions.
7 of 114
3
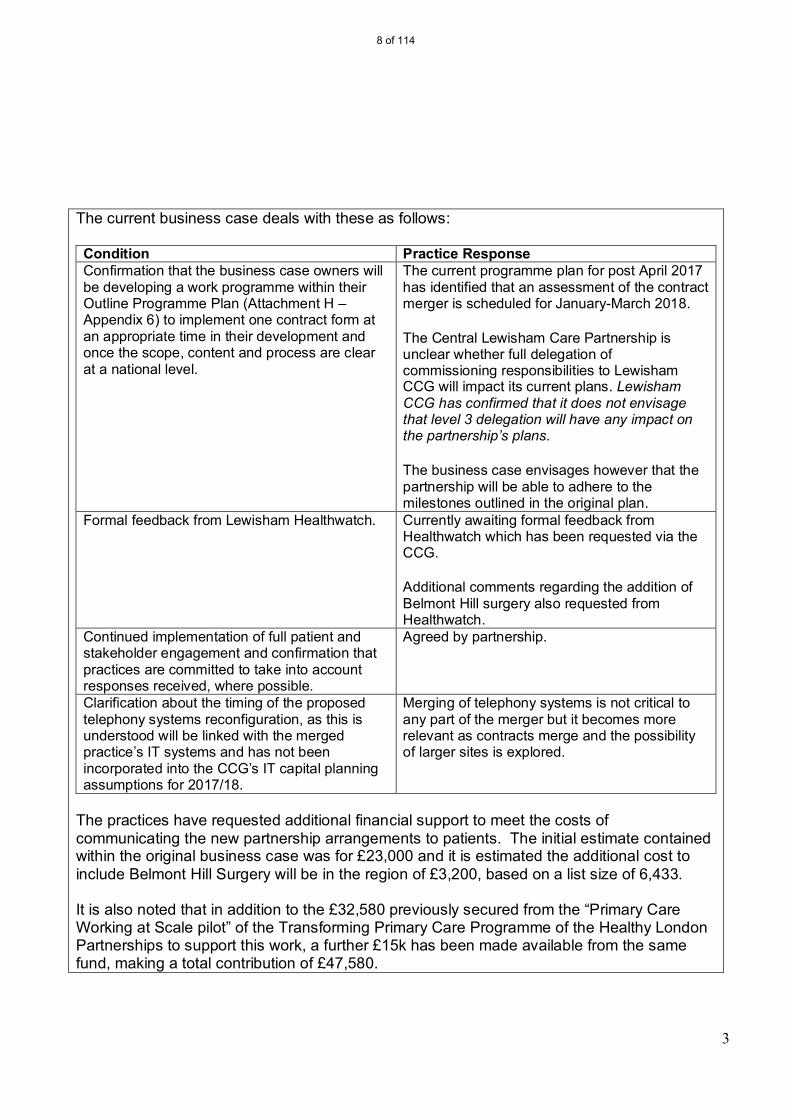
The current business case deals with these as follows: Condition Practice Response Confirmation that the business case owners will be developing a work programme within their Outline Programme Plan (Attachment H – Appendix 6) to implement one contract form at an appropriate time in their development and once the scope, content and process are clear at a national level.
The current programme plan for post April 2017 has identified that an assessment of the contract merger is scheduled for January-March 2018. The Central Lewisham Care Partnership is unclear whether full delegation of commissioning responsibilities to Lewisham CCG will impact its current plans. Lewisham CCG has confirmed that it does not envisage that level 3 delegation will have any impact on the partnership’s plans. The business case envisages however that the partnership will be able to adhere to the milestones outlined in the original plan.
Formal feedback from Lewisham Healthwatch. Currently awaiting formal feedback from Healthwatch which has been requested via the CCG. Additional comments regarding the addition of Belmont Hill surgery also requested from Healthwatch.
Continued implementation of full patient and stakeholder engagement and confirmation that practices are committed to take into account responses received, where possible.
Agreed by partnership.
Clarification about the timing of the proposed telephony systems reconfiguration, as this is understood will be linked with the merged practice’s IT systems and has not been incorporated into the CCG’s IT capital planning assumptions for 2017/18.
Merging of telephony systems is not critical to any part of the merger but it becomes more relevant as contracts merge and the possibility of larger sites is explored.
The practices have requested additional financial support to meet the costs of communicating the new partnership arrangements to patients. The initial estimate contained within the original business case was for £23,000 and it is estimated the additional cost to include Belmont Hill Surgery will be in the region of £3,200, based on a list size of 6,433. It is also noted that in addition to the £32,580 previously secured from the “Primary Care Working at Scale pilot” of the Transforming Primary Care Programme of the Healthy London Partnerships to support this work, a further £15k has been made available from the same fund, making a total contribution of £47,580.
8 of 114
4
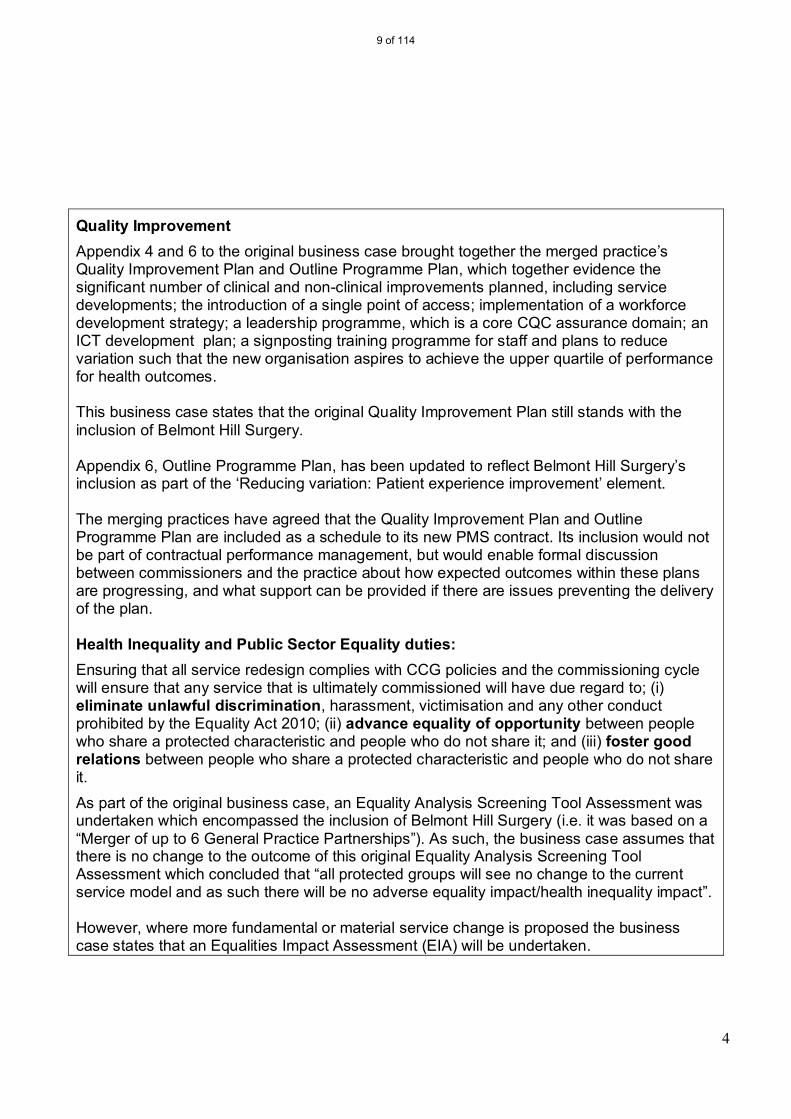
Quality Improvement Appendix 4 and 6 to the original business case brought together the merged practice’s Quality Improvement Plan and Outline Programme Plan, which together evidence the significant number of clinical and non-clinical improvements planned, including service developments; the introduction of a single point of access; implementation of a workforce development strategy; a leadership programme, which is a core CQC assurance domain; an ICT development plan; a signposting training programme for staff and plans to reduce variation such that the new organisation aspires to achieve the upper quartile of performance for health outcomes. This business case states that the original Quality Improvement Plan still stands with the inclusion of Belmont Hill Surgery. Appendix 6, Outline Programme Plan, has been updated to reflect Belmont Hill Surgery’s inclusion as part of the ‘Reducing variation: Patient experience improvement’ element. The merging practices have agreed that the Quality Improvement Plan and Outline Programme Plan are included as a schedule to its new PMS contract. Its inclusion would not be part of contractual performance management, but would enable formal discussion between commissioners and the practice about how expected outcomes within these plans are progressing, and what support can be provided if there are issues preventing the delivery of the plan. Health Inequality and Public Sector Equality duties: Ensuring that all service redesign complies with CCG policies and the commissioning cycle will ensure that any service that is ultimately commissioned will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
As part of the original business case, an Equality Analysis Screening Tool Assessment was undertaken which encompassed the inclusion of Belmont Hill Surgery (i.e. it was based on a “Merger of up to 6 General Practice Partnerships”). As such, the business case assumes that there is no change to the outcome of this original Equality Analysis Screening Tool Assessment which concluded that “all protected groups will see no change to the current service model and as such there will be no adverse equality impact/health inequality impact”. However, where more fundamental or material service change is proposed the business case states that an Equalities Impact Assessment (EIA) will be undertaken.
9 of 114

5
RECOMMENDATIONS: The Primary Care Joint Committee is asked to approve the addition of Belmont Hill Surgery to the original merger, including acceptance of the additional cost of writing to patients about the merger (estimated to be £3,200, which will be funded by NHS England) subject to formal feedback from Lewisham Healthwatch;
NHS England CONTACT: Name: Jill Webb; Head of Primary Care, SE London, NHS England (London) E-Mail: [email protected]
AUTHOR CONTACT: Name: Debbie Power, Senior Commissioning Manager - NHS England (London Region) E-Mail: [email protected]
10 of 114

Page 1 of 10
Mergers between practices London Region
Criteria for considering a request for a Proposed Partnership Merger in Lewisham
Practice Name & Address (1)
St John’s Medical Centre (G85038) 56 – 60 Loampit Hill, London, SE13 7SX
PMS Raw List Size: as at 1/01/17 14,239
CCG: Lewisham
Practice Name & Address (2)
Hilly Fields Medical Centre (G85055) 172 Adelaide Avenue, London, SE4 1JN
PMS Raw List Size: as at 1/01/17 12,369
CCG: Lewisham
Practice Name & Address (3)
Brockley Road Medical Centre (G85048) 467 Brockley Road, London, SE24 2PJ (operated by Hilly Fields partnership)
PMS Raw List Size: as at 1/01/17 5316
CCG: Lewisham
Practice Name & Address (4)
Morden Hill Surgery (G85035) 21 – 23 Morden Hill, London, SE13 7NN
PMS Raw List Size: as at 1/01/17 8934
CCG: Lewisham
Practice Name & Address (5)
Honor Oak Group Practice (G85089) 20 Turnham Road, Brockley, London, SE4 2LA
PMS Raw List Size: as at 1/01/17 9388
CCG: Lewisham
Practice Name & Address (6)
Belmont Hill Surgery (G85003) 6 Belmont Hill, Lewisham, London, SE13 5AY
PMS Raw List Size: as at 1/01/17 6430
CCG: Lewisham
Date Application made: March 2017 Region: London
Report template completed by Debbie Power Date completed 27th March 2017
Assessment Criteria Guidance Notes/Evidence that needs to be attached
Presentation of Case
Background in respect of each of the practices
Sections 1-8 of the attached business case detail the rationale and purpose of the proposed merger.
This appraisal is supplementary to the initial business case for the merger between Brockley Road Medical Centre, Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and St John’s Medical Centre (to form the Central Lewisham Care Partnership), which was agreed at the Lewisham Primary Care Joint Committee held on the 8th February 2017. This business case concerns the addition of the Belmont Hill Surgery to the Central Lewisham Care Partnership model and aligns to the original business case where the potential inclusion of Belmont Hill Surgery was referenced in section 1.
11 of 114
Page 2 of 10
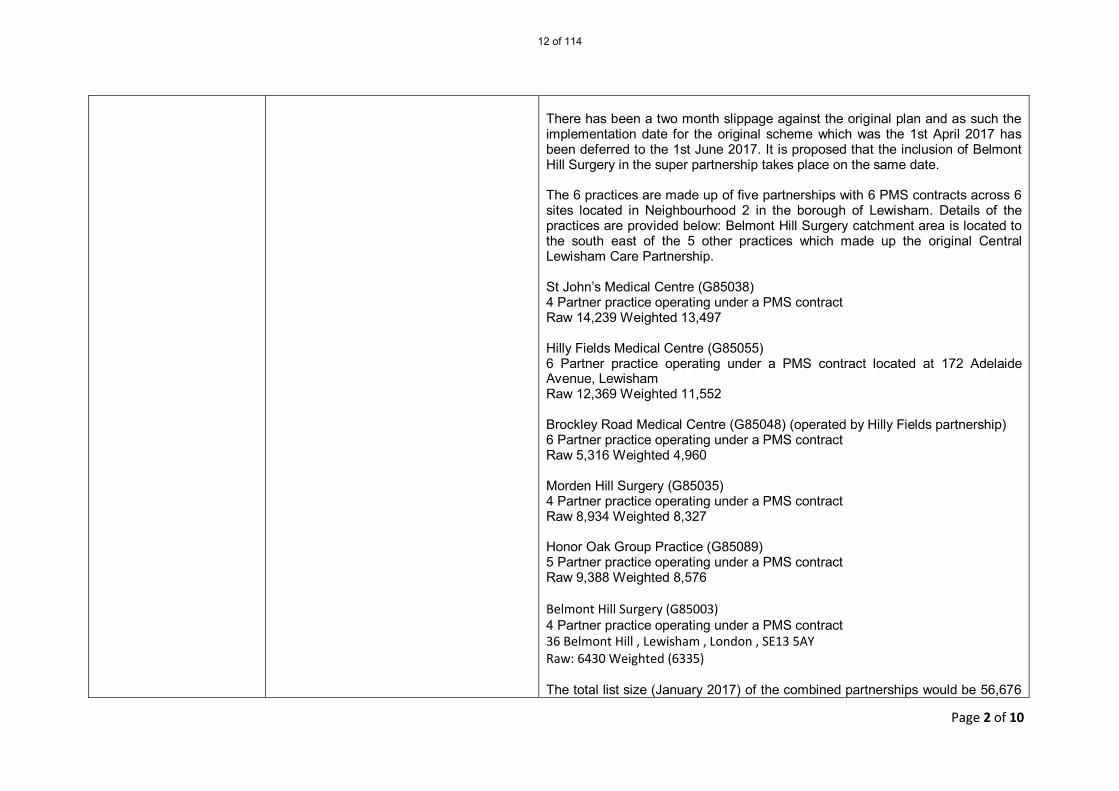
There has been a two month slippage against the original plan and as such the implementation date for the original scheme which was the 1st April 2017 has been deferred to the 1st June 2017. It is proposed that the inclusion of Belmont Hill Surgery in the super partnership takes place on the same date. The 6 practices are made up of five partnerships with 6 PMS contracts across 6 sites located in Neighbourhood 2 in the borough of Lewisham. Details of the practices are provided below: Belmont Hill Surgery catchment area is located to the south east of the 5 other practices which made up the original Central Lewisham Care Partnership. St John’s Medical Centre (G85038) 4 Partner practice operating under a PMS contract Raw 14,239 Weighted 13,497 Hilly Fields Medical Centre (G85055) 6 Partner practice operating under a PMS contract located at 172 Adelaide Avenue, Lewisham Raw 12,369 Weighted 11,552 Brockley Road Medical Centre (G85048) (operated by Hilly Fields partnership) 6 Partner practice operating under a PMS contract Raw 5,316 Weighted 4,960 Morden Hill Surgery (G85035) 4 Partner practice operating under a PMS contract Raw 8,934 Weighted 8,327 Honor Oak Group Practice (G85089) 5 Partner practice operating under a PMS contract Raw 9,388 Weighted 8,576 Belmont Hill Surgery (G85003) 4 Partner practice operating under a PMS contract 36 Belmont Hill , Lewisham , London , SE13 5AY Raw: 6430 Weighted (6335) The total list size (January 2017) of the combined partnerships would be 56,676
12 of 114
Page 3 of 10
(53,247 weighted list size). All practices provide both additional and essential services under their PMS contracts.
Information about local demography
Appendix 1 Practice Profiles provides details of the demography of the 6 practices. Further detail of the wider borough demography was provided in the original business case presented to the February 2017 PCJC.
The 6 practices are located within the London Borough of Lewisham which is an inner London borough.
The population of Lewisham is approximately 300,000 forming approximately 124,000 households
The age distribution in Lewisham is broadly similar to the inner London average with about 70% of working age, 20% under 16 and 10% over 65 years of age.
Around 30% of the population was born abroad as compared to 40% for inner London generally.
Both male and female life expectancy is similar to other inner London Boroughs.
The area of Central Lewisham which is very close to both St Johns Medical Centre and Morden Hill Surgery is projected to have population growth of 18,000 people by 2035 from 2015. Some of that growth has already happened with all the construction in and around the centre of Lewisham. With the rate of growth currently being seen in central Lewisham and the additional sites being developed this projected increase could be achieved sooner. This also includes the redevelopment of the Council’s own estates at Heathside and Lethbridge where an additional 1200 homes are being constructed. Lewisham CCG has commented that future plans for health will need to be able to accommodate this population growth. The CCG advises that the Local Authority would be open to discussions on a new health facility in central Lewisham and this has been identified in its Local Estate Strategy. In the future, consideration will need to be given as to whether the practices in this area can accommodate this growth within the existing estate. Any future discussion about the estate will need to take into account a) existing capacity b) its suitability c) affordability and d) the population changes in the area. With respect to the 6 practices:
The combined practices would have a total raw list size of approximately 57,000.
List sizes have been relatively stable with a small growth in list size
13 of 114
Page 4 of 10
since 2014 for all practices except Honor Oak which showed a 1% fall There is significant variation in deprivation scores between the practices. Morden Hill and Honor Oak show deprivation noticeably above the
national and CCG average. Hilly Fields and Brockley Road deprivation scores are noticeably below the averages with St John’s and Belmont close to the CCG norm.
What are the strategic benefits of agreeing a merger and do they meet the criteria set out above
Section 7 of the attached business case Section 7 of the attached business case confirms that the strategic fit of the new merged partnership to include Belmont Hill Surgery remains the same as that articulated in Section 7 of the original business case. The strategic benefits identified in the original business case included: Pro-active care working with local charities, community and voluntary
groups to make sure that services meet the needs of specific groups of people; maintaining a database of services and facilities that will help patients manage their own health and wellbeing and supporting hard to reach groups including the homeless.
Flexible access arrangements and a willingness to offer extended 8-8 opening, in line with commissioners’ strategic requirements. Implementation of 8-8 access is not planned until April 2018 and CCG commissioners will need to consider how this fits with its Lewisham wide Extended Access plans, particularly given the proximity of the practice’s premises to the Lewisham Hospital Hub.
Coordinated care and continuity of care developing a system that will be applied across all delivery sites that patients who most need a coordinated approach are identified, have a named professional, a care plan and are supported to manage their condition by MDTs
Enhanced use of digital technology to improve and develop systems such as telephone triage and Skype consultations and prescribing NHS approved health apps instead of or alongside medicines.
Working with others to further cement beneficial working arrangements with other key organisations in the health and care community and further afield including other local health and care organisations as well as those in the voluntary sector, charities and third sector organisations.
Improving consistency of care by establishing and maintaining consistently high standards across all practices sharing both clinical and non-clinical best practice thus reducing the variability and increasing the safety of care for all patients across the partnership. Implementation is planned for April 2018.
14 of 114

Page 5 of 10
Signposting - Frontline staff will be trained further in signposting patients and carers to alternative sources of support and assistance including charities, local community groups and the voluntary sector. This will ensure that patients know that there are good alternatives to seeing a GP or nurse or attending A&E departments including using pharmacists and online, self-help resources. Signposting will be integrated with Social Services, information and advice. Implementation is planned for January 2018.
There may be concerns as to whether this planned merger will destabilise other local practices. The original business case identified this as a risk and included a Communications and Engagement Strategy 2016-17 (Appendix 3 to the original BC) which proposed a launch event to ‘seek to reassure practices in the area that they are not a threat but a positive development for the local health economy’.
The current business case states that neighbouring practices have been kept fully informed of the proposals for the original merger and the addition of Belmont Hill Surgery. One further neighbouring practice has entered into the first stage of talks regarding possible inclusion in the super partnership whilst the remaining 6 practices in the neighbourhood have been fully informed at the monthly neighbourhood meetings of the proposals.
Practice performance
Appendix 1 Practice Profiles
There are no contract sanctions on file for any of the 6 practices. Appendix 1 of the original business case detailed the profiles and performance of the original five practices which were intended to form Central Lewisham Care Partnership. Information was provided on NHS England Primary Care Web Tool general practice outcome standards, QOF, LNPCIS 2015/16, GP Patient Survey and Patient Online services. This appendix has been updated to include information associated with Belmont Hill Surgery. The current business case (section 5) identifies specific areas of performance variation for Belmont Hill Surgery including GP patient survey results, some QOF indicators and access issues and outlines immediate actions to address these. The practice is shown as ‘Approaching Review’ under GPOS (6 Level 1 Triggers). The GP Patient Survey results show that the practice rating is generally somewhat lower than CCG and National averages. Plans to address these variances are included in section 5 of the business case.
15 of 114
Page 6 of 10
The CQC report published in August 2016 rated the practice as ‘Good’ overall but ‘Requires Improvement’ for ‘Are Services Safe’. The practice has performed well when working in collaboration with others through the 2015/16 NHS Lewisham CCG Neighbourhood Primary Care Improvement Scheme (LNPCIS), particularly in regard to flu vaccinations. The Outline Programme Plan (Attachment H – Appendix 6 of original Business case) and Quality Improvement Plan (Attachment F –Appendix 4 of original Business case) outline a work programme to consistently improve clinical quality. The current business case states that many of the challenges articulated in the original business are generic across general practice and so equally apply to Belmont Hill Surgery. As such, the mitigating plans and actions proposed will also apply to Belmont Hill Surgery. The programme plan has also been updated to specifically include Belmont Hill as part of the ‘Reducing variation: Patient experience improvement’ element, which is an area where Belmont Hill showed the most significant variation.
Will the merger result in services being provided from premises that are fit for purpose in accordance with minimum standards set out in 2013 GMS Premises Costs Directions, or that have a Business Plan to achieve within no more than 12 months
Section 4 of Appendix 1 Practice Profiles Section 4 and Appendix 1 of the original business case discussed the premises issues associated with the merger. It referred to a proposed review of all premises within the new partnership in due course and that at this stage there would be no additional revenue costs. Equally there would be no property cost savings at this point. The original business case stated that the partners are working on an estates strategy which is due for completion in summer 2017 and will be the subject of full consultation with patients and statutory agencies. Belmont Hill Surgery is located in converted domestic premises and the current business case describes it as fit for purpose. The premises is freehold and has a current notional rent of £56,000 As a merged entity the larger partnership will be able to offer patients access to care at all of its sites which will enable improved utilisation of space and allow the development of new or extended services. There are no plans to close any of the existing premises at this time, pending the completion of the Estates strategy it has commissioned by Summer 17.
Has specified a clear plan Section 6, 7 and 8 of the business case The benefits specified in sections 5, 6, 7 and 8 of the original business case and
16 of 114

Page 7 of 10
of service improvements that will arise as a result of the merger
summarised below are not affected by the addition of Belmont Hill Surgery. Benefits for patients include: Improved accessibility to primary care in the community using different
options depending on need including Skype, longer face to face consultations, single point of access (call centre), enhanced signposting.
Easy access to a greater number of local specialised services based in practices and access to specialist support groups across the sites.
Better coordination and delivery of long term conditions’ services through refocused MDTs;
Clinicians who will be readily interchangeable between sites thus building capacity while still offering the same high quality of care and safety.
Access to more primary care services at longer and more convenient hours by utilising a hub and spoke approach;
Greater patient choice of GP such as access to female GPs. Patients will however, still be able to see their current GP.
Benefits for staff include: More flexible work patterns; Improved job satisfaction and less stress due to greater support available; Closer team working; More training and development opportunities shared across the sites; new
roles available; and more opportunities to specialise; Wider skill mix available enabling the development of new services and
ways of working; Development of a much more sustainable and viable organisation as a
whole rather than individually; Financial and efficiency savings; Reducing unnecessary duplication; Benefits for the health economy include: Reduced A&E attendance as the merged practice will provide improved
extended hours and more appointments as well as new ways of accessing healthcare;
Hard to reach groups across our area will have access to consistent, high quality approach with specialist care where needed;
Easy access to a greater number of practice based out of hospital specialised services available to a wider range of patients;
17 of 114
Page 8 of 10
Access to more primary care services in the community at longer and more convenient hours by utilising a hub and spoke approach.
Financial Support Request The business case states that the financial considerations detailed in the original
business case still remain relevant in relation to the inclusion of Belmont Hill Surgery. In terms of ‘organisational development and transformation support’ and ‘supporting service developments’ costs, the business case states that any increases in projected costs are expected to be only marginal when taking into account Belmont Hill Surgery as one additional practice as many of the associated supporting costs are fixed. The business case confirms that the financial commitments relative to the merger will be delivered via commercial arrangements with Bankers and the New Partnership. In addition to the £32,580 previously secured from the “Primary Care Working at Scale pilot” of the Transforming Primary Care Programme of the Healthy London Partnerships to support this work a further £15k has been made available from the same fund, making a total contribution of £47,580. The practices have requested that commissioners meet the costs of communicating the new partnership arrangements to patients (i.e. postage costs). The initial estimate contained within the original business case was for £23,000 and it is estimated the additional cost to include Belmont Hill Surgery will be in the region of £3,200, based on a list size of 6,433.
What is the CCG’s view of the proposed merger?
The merger still fits with the latest Lewisham CCG Primary Care Strategy (and also STP and Strategic Commissioning Framework for Primary Care Transformation in London) including: the delivery of proactive, accessible and coordinated care; practices working at scale; primary care working as an integral part of our local Neighbourhood Care
Networks; reducing variation and inequalities.
What is the LMC’s view of the proposed merger?
The LMC has been aware of ongoing work to develop this structure although it states it has not been directly involved. The LMC confirms it supports collaborative working and working at scale to improve GP resilience and specifically commented:
18 of 114
Page 9 of 10
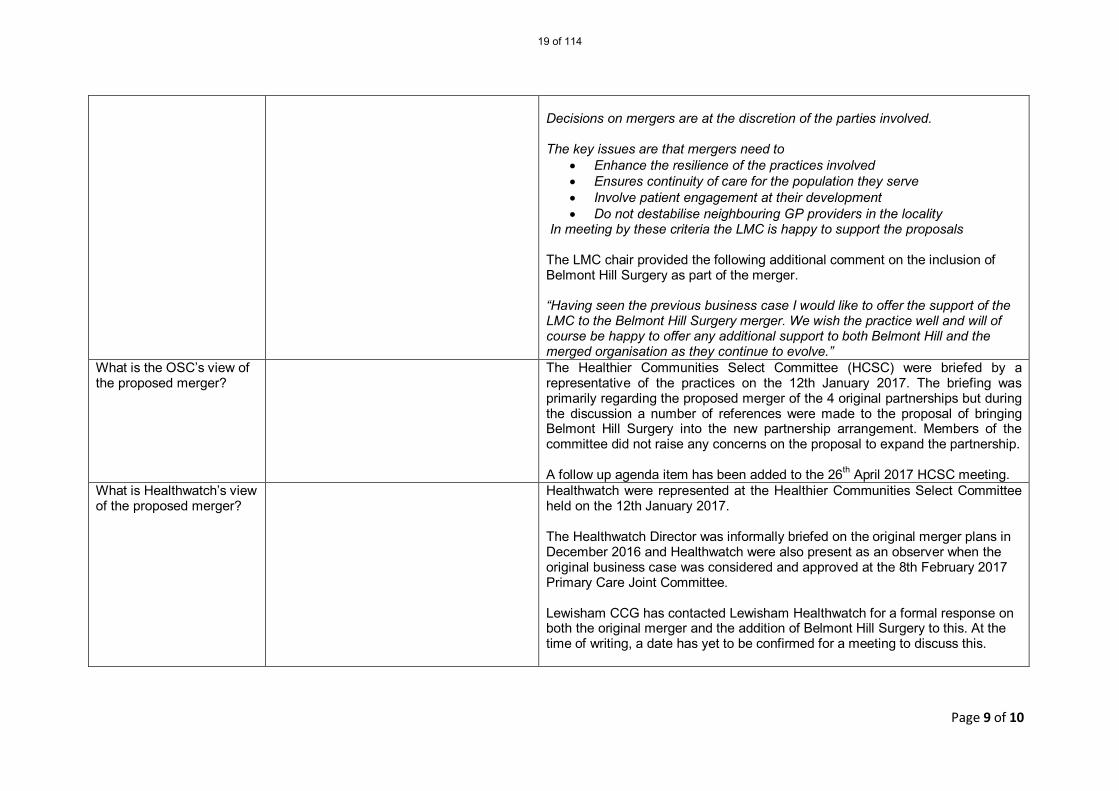
Decisions on mergers are at the discretion of the parties involved. The key issues are that mergers need to
Enhance the resilience of the practices involved Ensures continuity of care for the population they serve Involve patient engagement at their development Do not destabilise neighbouring GP providers in the locality
In meeting by these criteria the LMC is happy to support the proposals The LMC chair provided the following additional comment on the inclusion of Belmont Hill Surgery as part of the merger. “Having seen the previous business case I would like to offer the support of the LMC to the Belmont Hill Surgery merger. We wish the practice well and will of course be happy to offer any additional support to both Belmont Hill and the merged organisation as they continue to evolve.”
What is the OSC’s view of the proposed merger?
The Healthier Communities Select Committee (HCSC) were briefed by a representative of the practices on the 12th January 2017. The briefing was primarily regarding the proposed merger of the 4 original partnerships but during the discussion a number of references were made to the proposal of bringing Belmont Hill Surgery into the new partnership arrangement. Members of the committee did not raise any concerns on the proposal to expand the partnership. A follow up agenda item has been added to the 26th April 2017 HCSC meeting.
What is Healthwatch’s view of the proposed merger?
Healthwatch were represented at the Healthier Communities Select Committee held on the 12th January 2017. The Healthwatch Director was informally briefed on the original merger plans in December 2016 and Healthwatch were also present as an observer when the original business case was considered and approved at the 8th February 2017 Primary Care Joint Committee. Lewisham CCG has contacted Lewisham Healthwatch for a formal response on both the original merger and the addition of Belmont Hill Surgery to this. At the time of writing, a date has yet to be confirmed for a meeting to discuss this.
19 of 114

Page 10 of 10
Region recommendation to the Panel (will be subject to patient engagement)
The Primary Care Joint Committee is asked to approve the addition of Belmont Hill Surgery to the original merger, including acceptance of the additional cost of writing to patients about the merger (estimated to be £3200, which will be funded by NHS England) subject to formal feedback from Lewisham Healthwatch.
Date of Primary Care Joint Committee (PCJC) March 2017 Outcome: Please delete as appropriate
Approved / Approved with Conditions/ Rejected
Feedback from PCJC: Please insert Panel Members: Please insert
20 of 114

BUSINESS CASE FOR PROPOSED PARTNERSHIP MERGER IN
LEWISHAM
Belmont Hill Surgery
and the
Central Lewisham Care Partnership St John’s Medical Centre Hilly Fields Medical Centre
Brockley Road Medical Centre Morden Hill Surgery
Honor Oak Group Practice
27th March 2017
21 of 114

Page 2 of 15
Belmont Hill Surgery and the Central Lewisham Care Partnership (St John’s Medical Centre, Hilly Fields Medical Centre, Brockley Road Medical Centre,
Morden Hill Surgery, Honor Oak Group Practice)
Business Case for proposed partnership merger March 2017
Practice details summary:
Practice name and address (1)
St John’s Medical Centre 56 – 60 Loampit Hill London SE13 7SX
PMS Raw list size as at November 2016: 14,334
CCG: Lewisham
Practice name and address (2)
Hilly Fields Medical Centre 172 Adelaide Avenue, London, SE4 1JN
PMS Raw list size as at April 2016: 12,442
CCG: Lewisham
Practice name and Address (3)
Brockley Road Medical Centre 467 Brockley Road, London SE24 2PJ (operated by Hilly Fields partnership)
PMS Raw list size as at March 2016: 5,112
CCG: Lewisham
Practice name and address (4)
Morden Hill Surgery 21 – 23 Morden Hill London SE13 7NN
PMS Raw list size as at September 2016: 8,874
CCG: Lewisham
Practice name and address (5)
Honor Oak Group Practice 20 Turnham Road Brockley London SE4 2LA
PMS Raw list size as at July 2016: 9,312
CCG: Lewisham
Practice name and address (6)
Belmont Hill Surgery 36 Belmont Hill , Lewisham , London , SE13 5AY
PMS Raw list size as at January 2017: 6,433
CCG: Lewisham
22 of 114

Page 3 of 15
Table of Contents
Contents
1. Introduction and background................................................................................... 4
2. Our vision ................................................................................................................ 6
3. Practice profiles ....................................................................................................... 6
4. Strategic fit .............................................................................................................. 7
5. What issues do our practices currently face? ........................................................... 7
6. What benefits will a merger bring to our patients? .................................................. 8
7. What will be the benefits to our staff and organisations?......................................... 8
8. What will be the benefits for our local health economy?.......................................... 8
9. Stakeholder and patient engagement ...................................................................... 8
10. Structure of new partnership................................................................................. 11
11. Governance: Decision making ................................................................................ 12
12. Equalities Impact Assessment ................................................................................ 12
13. Risks ...................................................................................................................... 12
14. Key milestones....................................................................................................... 12
15. Finance.................................................................................................................. 13
16. Contractual models................................................................................................ 13
17. Conditions to which the original merger business case was approved .................... 14
23 of 114

Page 4 of 15
1. Introduction and background
This business case builds on the already approved business case for the merger between
Brockley Road Medical Centre, Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak
Group Practice and St John’s Medical Centre (under the Central Lewisham Care Partnership)
which was agreed at the Lewisham Primary Care Joint Committee held on the 8th February
2017 (full papers available at http://www.lewishamccg.nhs.uk/about-us/how-we-
work/PCJC%20docs/SE%20London%20PCJCs%20meeting%2020170208.pdf)
This business case, which concerns the addition of the Belmont Hill Surgery to this Partnership
model, aligns absolutely to the original business case where the potential inclusion of Belmont
Hill was actually referenced explicitly.
Additional considerations to the original business case as a result of Belmont Hill’s inclusion
will be articulated in this document.
Belmont Hill Surgery has been involved in discussions with Brockley Road Medical Centre,
Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and St John’s
Medical Centre about merging as part of the Central Lewisham Care Partnership for the past
9 months through the Steering Group structure as described in the original business case.
All the partnerships in the proposed merger hold PMS contracts, are located in
Neighbourhood 2 and are geographically adjacent. As members of both the providing and
commissioning entities for Neighbourhood 2 the five partnerships have a long track record
of working together on health and care initiatives.
The new partnership will hold the existing PMS contracts in trust in behalf of each practice
with the aim of merging these individual delivery contracts into one main contract subject
to Level 3 Clinical Commissioning Group requirements.
The partners of all the practices are committed to continuing the high quality care that is
presently delivered together with maintaining the viability and sustainability of general
practice, whilst also acknowledging that it must change in order in order to keep abreast of
capacity and demand issues. The partners have opted to implement a super partnership
24 of 114
Page 5 of 15
model whereby there will be one new partnership which will initially sign up to the
individual contract currently in place and will seek to bring them into one PMS contract
covering all the sites. In the short term this will enable us to merge vital back office services
thus making substantial financial and administrative efficiencies as well as enabling us to
move to a more integrated and flexible clinical team over time. As such, practices will be
seen as delivery sites supported by central services back office support.
The proposal is in line with both local and national strategy and will clearly deliver
significant benefits to our patients, partners, staff as well as the wider local health
community.
We are working closely with our patients to ensure a smooth transition into one
organisation. We have also initiated working groups on service development with patients
playing an active part at every stage. The initial effect on our patient population should not
be noticeable as unless patients express an interest in changing practices they will be seen in
the same way by the same team and will have no obligation to access any of the other
services available to them at other locations unless they. There will, however, be a range of
new services and methods of accessing services such as specialist diabetic clinics, key out-
patient services such as dermatology, cardiology, MSK together with potential exciting
developments in signposting, social services information and advice with a focus on health
and wellbeing in the broad community represented by the practice delivery centre base.
New technologies will include telephone single access, telephone triage and video
consultation all of which are being designed to improve the patient experience, particularly
for vulnerable and disadvantaged patient. We will work with patient representatives and
voluntary sector organisations to develop specifically targeted programmes for groups
deemed hard to reach and those who do not have English as a first language.
We continue to believe that our merger will act as a template for other practices in
both Lewisham and further afield enabling them to fast track progress from the learning
of others. We have had substantial interest in our model following various presentations
including at the recent Healthy London Partnership “21st Century Primary Care: Working at
Scale” conference held in March 2017.
25 of 114
Page 6 of 15
2. Our vision
The vision of the new merged partnership to include Belmont Hill remains the same as that
articulated in the original business case.
3. Practice profiles
Practice profiles have been updated to include details for Belmont Hill Surgery. This
can be found at Appendix 1.
The neighbourhood profile appended to the original business case still stands as all
practices are within the same neighbourhood.
Table 1: Practice contracts
Partnership Sites Contracts
St John’s Medical Centre 1. St John’s Medical Centre 1. Single PMS contract
Hilly Fields Medical Centre 1. Hill Fields Medical Centre
2. Brockley Road Medical
Centre
1. Single PMS contract
2. Single PMS contract
Morden Hill Surgery 1. Morden Hill Surgery 1. Single PMS contract
Honor Oak Group Practice 1. Honor Oak Group Practice 1. Single PMS contract
Belmont Hill Surgery 1. Belmont Hill Surgery 1. Single PMS contract
• The combined value of our PMS contracts is circa £7.4m;
• All five partnerships (six locations) have geographical coherence (see map in
Appendix 1);
• The total list size of the new partnership would be circa 57,000
• All practices are registered with CQC and St John’s Medical Centre, Hilly Fields
Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and Belmont Hill
Surgery have been rated as good. We are waiting for the Brockley Road Medical
Centre inspection result to be published.
26 of 114
Page 7 of 15
4. Strategic fit
The strategic fi t of the new merged partnership to include Belmont Hill Surgery remains
the same as that articulated in the original business case.
5. What issues do our practices currently face?
Many of the challenges articulated in the original business are generic across
general practice and so equally apply to Belmont Hill Surgery. As such, the
mitigating actions to be realised through working at scale that were described are
also relevant to Belmont Hill Surgery.
Specific areas of variation for Belmont Hill that are shown through the
comparative practice profiles in Appendix 1 are:
The following areas from GP patient survey:
o % saying overall experience of GP surgery
o % saying easy to get through to someone on phone
o % saying receptionists at GP surgery are helpful
o % saying they had a good experience of making an appointment
o % saying they had confidence and trust in the GP they saw or spoke
to
o % saying they are satisfied with the hours their GP surgery is open
o % saying in last 6 months, had enough support from local services or
organisations to help manage long-term health condition(s)
Online appointments offered
Diabetes and Mental health QOF indicators
These areas will be addressed through the new partnerships Quality Improvement
Plan and will be supported through sharing of best practice and the benefit of an
at scale organisation (i.e. more flexibility of workforce, less dependence on locum
staff, standardised call/recall systems and processes).
27 of 114
Page 8 of 15
Actions are also being undertaken in the immediate term to address these areas of
variation at Belmont Hill Surgery including:
A new 6 session a week salaried GP to start in May 2017, increasing GP
appointments by 31 per week
Increased reception hours
Receptionists have completed training via the Lewisham CEPN
Telephone queuing system introduced with no call drop facility
An increase in available online bookable appointments by 30%
6. What benefits will a merger bring to our patients?
The benefits the merger will bring to patients’ remains the same as that articulated in
the original business case.
7. What will be the benefits to our staff and organisations?
The benefits the merger will bring to our staff and organisations remains the same
as that articulated in the original business case.
8. What will be the benefits for our local health economy?
The benefits the merger will bring to the local health economy remains the same as
that articulated in the original business case.
9. Stakeholder and patient engagement
The Steering Group leading the practice merger are fully committed to engaging patients and all
stakeholders in the development and ultimate implementation of the proposed merger.
Discussions about the possible merger have been ongoing for the last two years and to date so
far we have undertaken the following:
• Held individual practice meetings with partners and staff to outline our proposed
28 of 114
Page 9 of 15
merger plans and to invite active participation in shaping and forming the new
organisation;
• Met with all the Practice Managers to ask them to be involved in the detail of the
proposed merger including leading on the TUPE process;
• Held discussions with representatives of the PPGs to outline our merger
proposals;
• Met with One Health Lewisham Ltd to discuss our merger plans;
• Met with LMC and actively engaged an LMC member in merger discussions;
• Met with NHS England and Lewisham CCG to gain support for our proposal;
• Met with other practices in the area that are considering the option of merging with
us at a later stage;
• Presented to the Lewisham Health Communities Select Committee.
The outline Communications and Engagement Strategy which was developed as part of the
original business case submission still stands and will be expanded to include all relevant
stakeholders of Belmont Hill Surgery.
Specific detail of engagement undertaken includes:
Stakeholder Detail / outcome of Engagement
Meeting held with key
representatives of
Belmont Hill Surgery
PPG on Friday 10th
March 2017
PPG members said they are cautiously optimistic, as long as it
doesn't affect the service they receive. They understand the
rationale for the change and can see the potential benefits
including improved access and reduced stress on staff members.
They were reassured to know that no staff will be losing their
jobs. They would like continuity of care from the same GP if
possible.
There will be a meeting of the individual sites PPGs in April 2017
to draw up a constitution and governance arrangements that will
continue to support specific delivery sites PPGs and there will
also be a Partnership wide PPG set up in order to deliver
consistency and a way of communicating the journey to deliver
the combined contract model in the future.
29 of 114

Page 10 of 15
Meeting with Belmont
Hill Surgery staff held
on 7th March 2017
Full staff meeting held, led by Colin Stears with Partners of
Belmont Hill Surgery. No real concerns expressed except that
some staff were anxious that they would be forced to move work
location. Staff were reassured that this would not be the case and
that all changes would be voluntary. There will be a further staff
wide meeting in April 2017 to discuss the establishment of an
employee’s council as the vehicle for ongoing employer and
employee dialogue.
Lewisham Healthier
Communities Select
Committee (HCSC)
The HCSC were briefed by Colin Stears on the 12th January 2017.
The briefing was primarily regarding the proposed merger of the
4 original partnerships but during the discussion Colin Stears
made a number of references to the proposal of bringing
Belmont Hill Surgery into the new partnership arrangement.
Members of the committee did not raise any concerns on the
proposal to expand the partnership.
Lewisham HealthWatch Lewisham HealthWatch has been contacted for a formal response
on both the original merger and the addition of Belmont Hill
Surgery to this. At the time of writing, the CCG are trying to
facilitate this.
The HealthWatch Director was informally briefed on the original
merger plans in December 2016 and Healthwatch were also
present as an observer when the original business case was
considered and approved at the 8th February 2017 Primary Care
Joint Committee.
Healthwatch were also present at the HCSC briefing given on the
12th January 2017 and did not raise any objections to the main
proposal or references to the wider expansion.
Neighbouring Practices Neighbouring Practices have been kept fully informed of the
proposals for the original merger and the addition of Belmont Hill
Surgery. One further neighbouring practice has entered into the
first stage of talks regarding possible inclusion in the super
partnership whilst the remaining 6 practices in the
Neighbourhood have been fully informed at the monthly
neighbourhood meetings of the proposals.
30 of 114
Page 11 of 15
Lewisham LMC Lewisham LMC chair provided the following comment on the
original merger business case:
“The LMC has been aware of on going work to develop this
structure. Although we have not been directly involved and as far
as I am aware the practices involved have not directly approached
either the local LMC or Londonwide for support. As you know the
LMC supports collaborative working and working at scale to
improve GP resilience. Decisions on mergers are at the discretion
of the parties involved. The key issues for me are that mergers
need to
Enhance the resilience of the practices involved
Ensures continuity of care for the population they serve
Involve patient engagement at their development
Do not destabilise neighbouring GP providers in the
locality.”
The chair of the local LMC, also attended the HCSC briefing given
on the 12th January 2017 and was present as an observer when
the original business case was considered and approved at the 8th
February 2017 Primary Care Joint Committee.
The LMC chair provided the following additional comment on the
inclusion of Belmont Hill Surgery as part of the merger.
“Having seen the previous business case I would like to offer the
support of the LMC to the Belmont Hill Surgery merger. We wish
the practice well and will of course be happy to offer any
additional support to both Belmont Hill and the merged
organisation as they continue to evolve.”
10. Structure of new partnership
The proposed organisational structure for the new partnership described in the original business
case would remain unchanged as a result of Belmont Hill Surgery joining the partnership.
31 of 114
Page 12 of 15
11. Governance: Decision making
The proposed Governance and Decision making arrangements for the new partnership
described in the original business case would remain unchanged as a result of Belmont Hill Surgery
joining the partnership.
12. Equalities Impact Assessment
As part of the original business case, an Equality Analysis Screening Tool Assessment was
undertaken which actually encompassed the inclusion of Belmont Hill Surgery (i.e. it was based
on a “Merger of up to 6 General Practice Partnerships”).
As such, the assumption is that there is no change to the outcome of this original Equality
Analysis Screening Tool Assessment which concluded that “all protected groups will see no
change to the current service model and as such there will be no adverse equality impact/health
inequality impact”.
Further, to restate the commitment made in the original Equality Analysis Screening Tool
Assessment, any proposed major changes to service delivery will always be assessed against
the Equality Analysis Screening Tool to determine if a full Equality Impact Assessment is
required.
13. Risks
Risks and mitigations detailed in the original business remain relevant in relation to the
inclusion of Belmont Hill Surgery.
14. Key milestones
The key milestones detailed in the original business case still remain relevant and unchanged
(in their content) in relation to the inclusion of Belmont Hill Surgery.
Appendix 6 of the original business case gives an overview of the post launch activities including
key milestones and major responsibilities. There has been a two month slippage against this
32 of 114

Page 13 of 15
original plan due to the timelines associated with the sign off of the original business case. As
such the implementation date for the original scheme which was the 1st April 2017 has been
changed to the 1st June 2017. The addition of Belmont Hill Surgery does not add any issues to
the plan for completion on this revised date. An updated programme plan is enclosed at
appendix 2.
15. Finance
The financial considerations detailed in the original business case still remain relevant in
relation to the inclusion of Belmont Hill Surgery. In terms of ‘Organisational development and
transformation support’ and ‘Supporting service developments’ costs, any increases in
projected costs are expected to be only marginal when taking into account Belmont Hill Surgery
as one additional practice as many of the associated supporting costs are fixed.
The financial commitments relative to this merger will be delivered via commercial
arrangements with Bankers and the New Partnership. £47,580 has also been allocated to
specifically support this work as part of the “Primary Care Working at Scale pilot” of the
Transforming Primary Care Programme of the Healthy London Partnerships.
As per usual practice, we would anticipate that commissioners will meet the costs of
communicating the new partnership arrangements to patients (i.e. postage costs). We estimate
this will be approximately £3,200 based on a list size of 6,433. In terms of process we have
recommended to commissioners that communication go out to patients across all 6 practices
simultaneously particularly due to the overlap in catchment areas so as to ensure a consistent
and coordinated approach.
16. Contractual models
The contractual model described in the original business would also apply to Belmont Hill
Surgery. Details of this are as follows:
• The new partnership will be seeking to retain each of the current PMS contracts held by
the existing practices. The new merged entity will hold these in trust;
• The new partnership will undertake to merge contracts when the health and care
environment delivers the necessary stability to achieve this;
33 of 114
Page 14 of 15
• Contracts could be merged into the new Multispeciality Community Provider style
contract. This will be reviewed when further details affecting PMS practices are
released and agreements are reached with commissioners on shape and form;
• Simple service level agreements will be exchanged between service delivery centres to
facilitate easy VAT efficient transfer of specialist partners and employees between
practices for services (e.g. GP’s, nurses HCA’s. Currently practices can incur VAT charges
on goods and services provided to other organisations with the exception of pre-
approved clinical services as described in NHS community contracts;
• A core central services SLA will be in place with each service delivery centre to
deliver partner agreed back office services;
• Further optional services will be developed and covered by a system of SLA annexes for
updating;
• Legally binding contracts will be negotiated between One Health Lewisham Ltd and the
new merged entity to task the GP owned provider to bid for certain contracts and
services on the new entity’s behalf;
• Contract and SLA arrangements will be reflected in an annex to the new partnership
deed.
17. Conditions to which the original merger business case was approved
An update against the conditions to which the original merger business case was approved is
given below.
Condition Update
Confirmation that the business
case owners will be developing a
work programme within their
Outline Programme Plan
(Attachment H – Appendix 6) to
implement one contract form at
an appropriate time in their
development and once the scope,
content and process are clear at a
national level.
As stated in Appendix 6 of the original Business Case,
the current programme plan for post April 2017 has
identified that an assessment of the contract merger is
scheduled for January-March 2018 with a number of
additional actions that will feed into that process
including an assessment of the impact on business
sustainability and direct patient care.
Central Lewisham Care Partnership are mindful that
there will be new commissioning arrangements on the
34 of 114
Page 15 of 15
1st April 2017, and that NHS Lewisham CCG will be a
fully delegated commissioner and at this stage we are
not sure, if at all, whether this will impact our current
plans as there will be a new governance structures
within the CCG, including a newly developed Primary
Care Commissioning Committee.
Having said this, there is nothing to suggest that we will
not be able to adhere to the milestones we outlined in
our original plan, which we believe offers the right level
of detail at this stage.
Formal feedback from Lewisham
HealthWatch.
This has been requested via the CCG. Please see
‘Stakeholder and patient engagement’ section for more
detail
Continued implementation of full
patient and stakeholder
engagement and confirmation
that practices are committed to
take into account responses
received, where possible.
Agreed by partnership. Please see ‘Stakeholder and
patient engagement’ section for more detail
Clarification about the timing of
the proposed telephony systems
reconfiguration, as this is
understood will be linked with the
merged practice’s IT systems and
has not been incorporated into
the CCG’s IT capital planning
assumptions for 2017/18.
Merging of telephony systems is not critical to any part
of the merger but it becomes more relevant as
contracts merge and the possibility of larger sites is
explored.
35 of 114

BUSINESS CASE FOR PROPOSED
PARTNERSHIP MERGER IN LEWISHAM
APPENDIX 1:
UPDATED PRACTICE PROFILES
To include Belmont Hill Surgery
St John’s Medical Centre Hilly Fields Medical Centre
Brockley Road Medical Centre Morden Hill Surgery
Honor Oak Group Practice
15th March 2017
36 of 114

Table of Contents
Contents
1. Location of all GP practices in Lewisham at 2015 .................................................................3
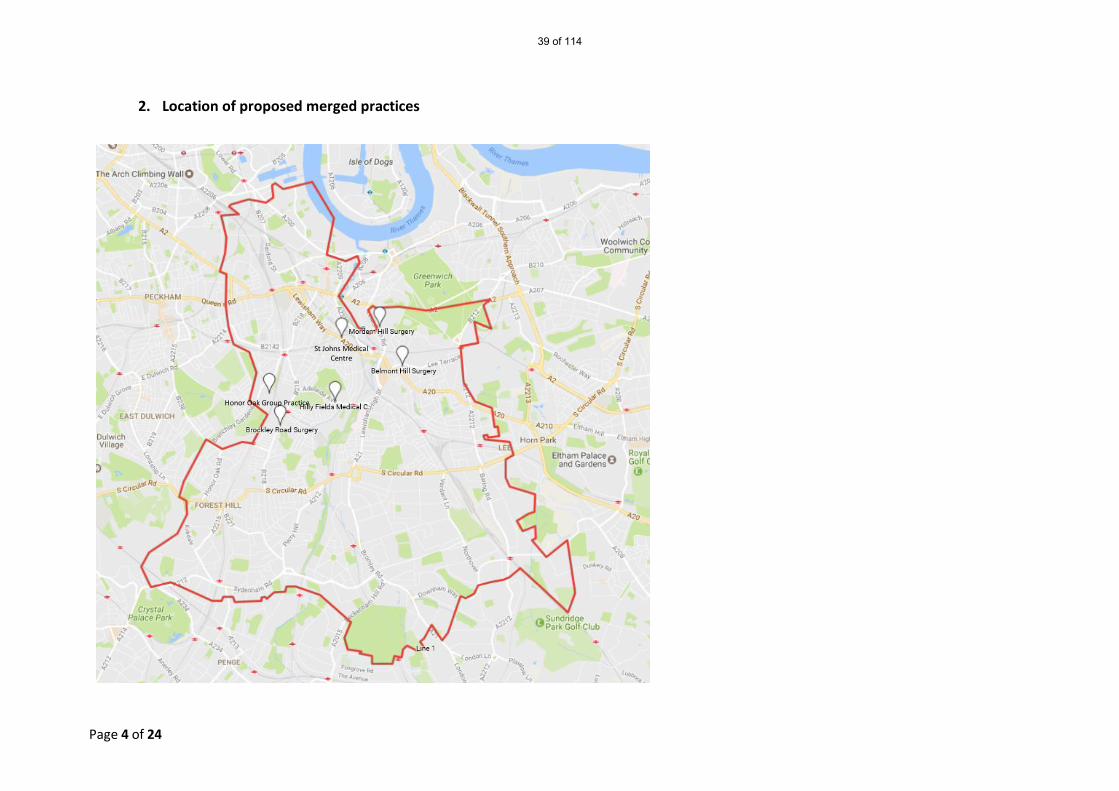
2. Location of proposed merged practices................................................................................4
3. Catchment area of proposed merging practices...................................................................5
4. Summary of practice property information ..........................................................................7
5. Distances in miles (by foot) between proposed merger sites...............................................8
6. Current partners in each partnership....................................................................................9
7. List size and age/sex breakdown.........................................................................................11
8. Deprivation and mortality ...................................................................................................13
9. Direct Enhanced Services/Local Commissioned Services 2016/17 .....................................14
10. Workforce............................................................................................................................16
11. Quality and Outcomes Framework 2015/16.......................................................................17
12. NHS England Primary Care Web Tool general practice outcome standards.......................18
13. Population Health Services Achievement ...........................................................................19
14. Patient Survey......................................................................................................................22
15. Patient online access – current baseline data on uptake (January 2017)...........................23
16. Membership of other bodies...............................................................................................24
37 of 114
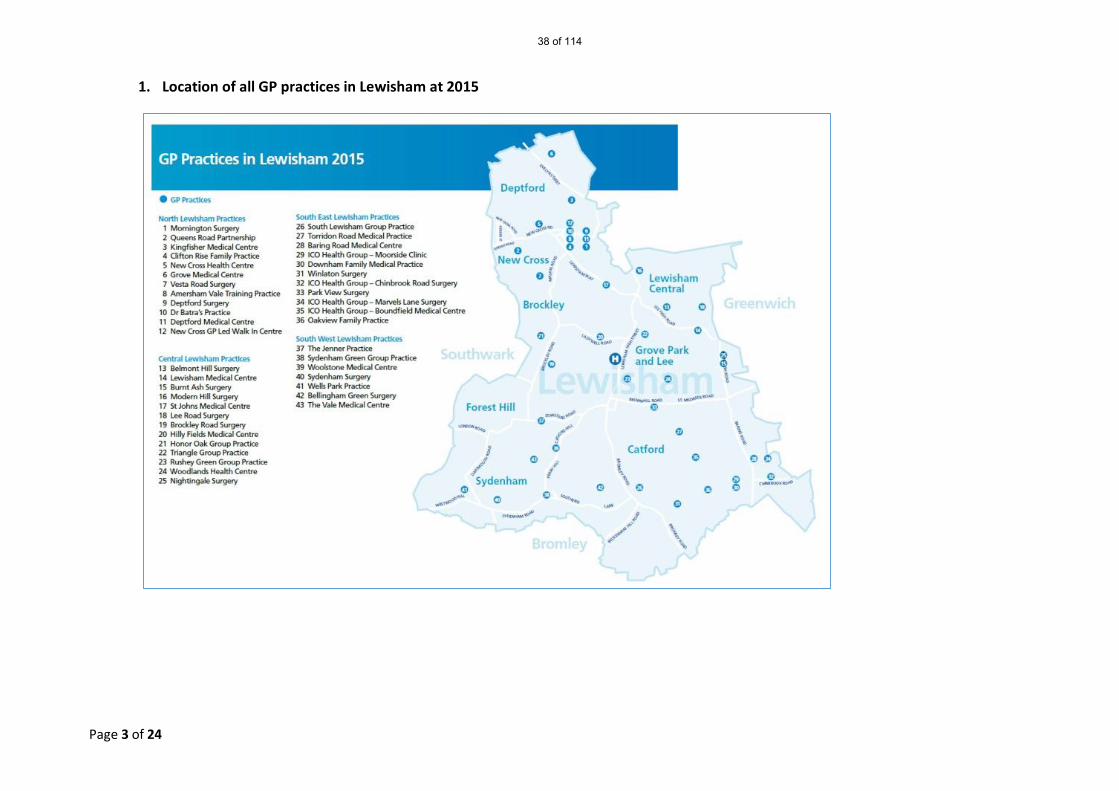
Page 3 of 24
1. Location of all GP practices in Lewisham at 2015
38 of 114
Page 4 of 24
2. Location of proposed merged practices
Honor Oak Group Practice
St Johns Medical Centre
39 of 114
Page 5 of 24
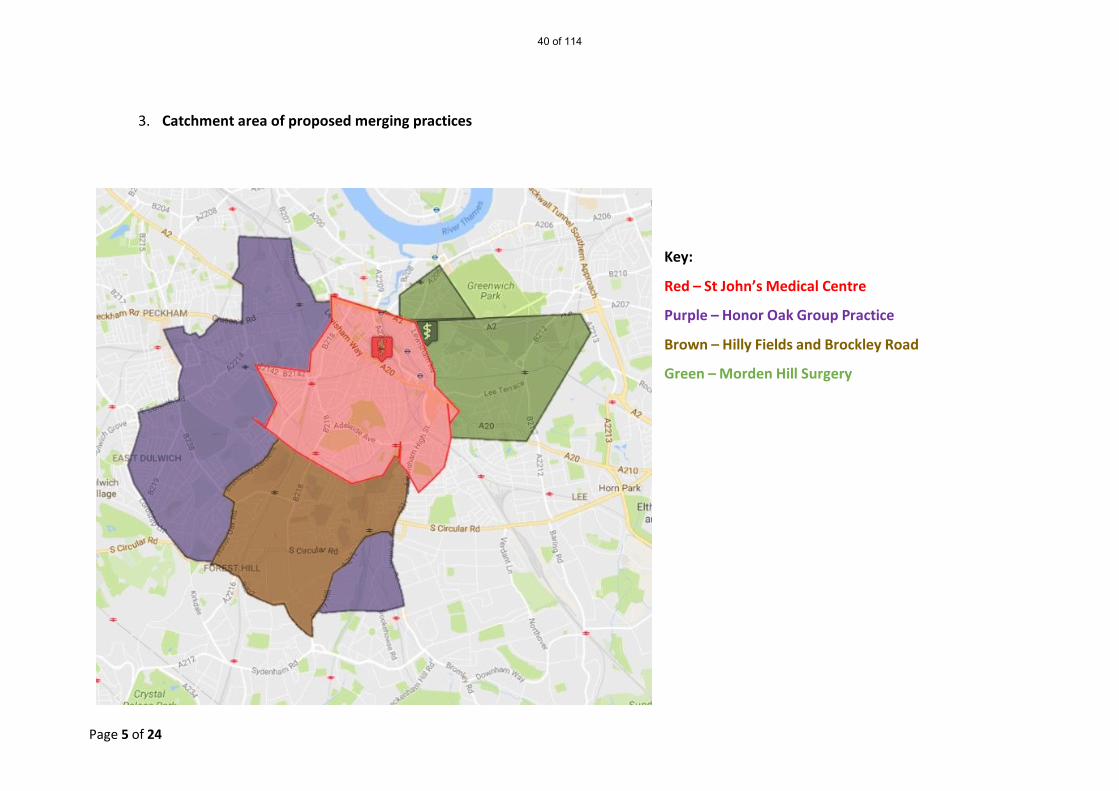
3. Catchment area of proposed merging practices
Key:
Red – St John’s Medical Centre
Purple – Honor Oak Group Practice
Brown – Hilly Fields and Brockley Road
Green – Morden Hill Surgery
40 of 114

Page 6 of 24
Belmont Hill catchment area
41 of 114

Page 7 of 24
4. Summary of practice property information
Property Name
Image Address Form of occupation £ Rent (budget) Net internal area (NIA) sqm Comments
Belmont Hill Surgery
36 Belmont Hill , Lewisham , London , SE13 5AY
Freehold £56,600 272 Although property not purpose built premises are fit for purpose.
42 of 114
Page 8 of 24
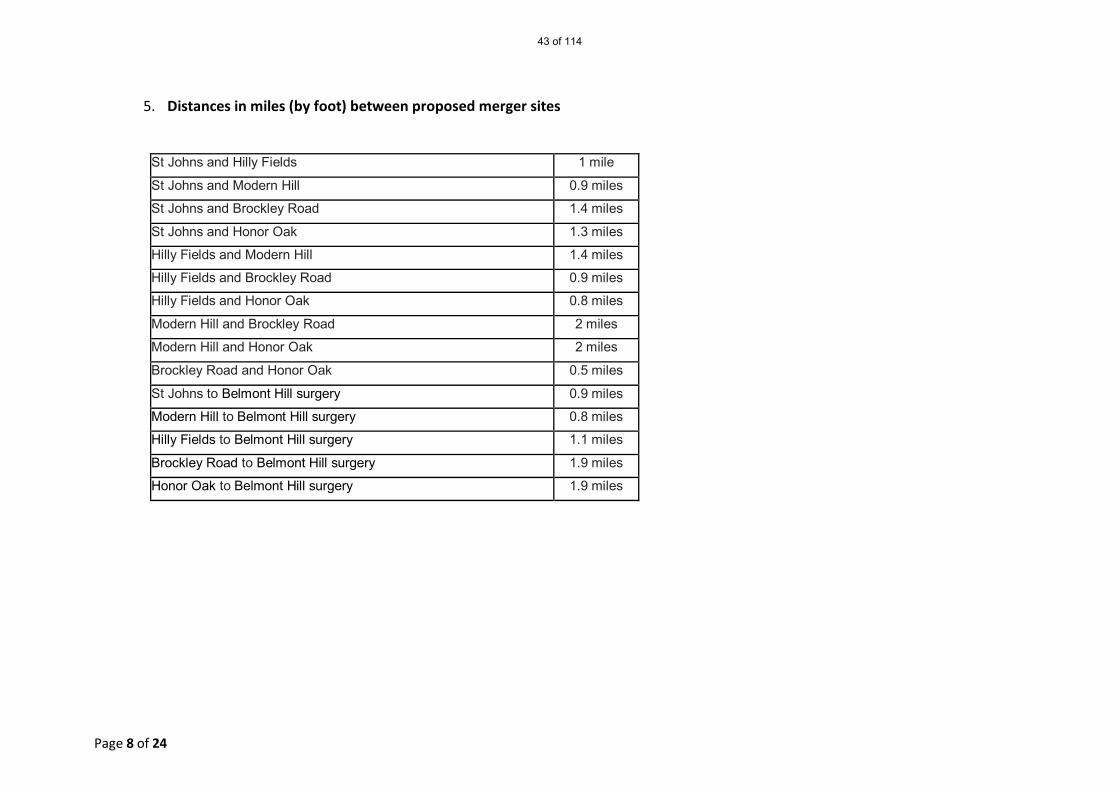
5. Distances in miles (by foot) between proposed merger sites
St Johns and Hilly Fields 1 mile
St Johns and Modern Hill 0.9 miles
St Johns and Brockley Road 1.4 miles
St Johns and Honor Oak 1.3 miles
Hilly Fields and Modern Hill 1.4 miles
Hilly Fields and Brockley Road 0.9 miles
Hilly Fields and Honor Oak 0.8 miles
Modern Hill and Brockley Road 2 miles
Modern Hill and Honor Oak 2 miles
Brockley Road and Honor Oak 0.5 miles
St Johns to Belmont Hill surgery 0.9 miles
Modern Hill to Belmont Hill surgery 0.8 miles
Hilly Fields to Belmont Hill surgery 1.1 miles
Brockley Road to Belmont Hill surgery 1.9 miles
Honor Oak to Belmont Hill surgery 1.9 miles
43 of 114
Page 9 of 24
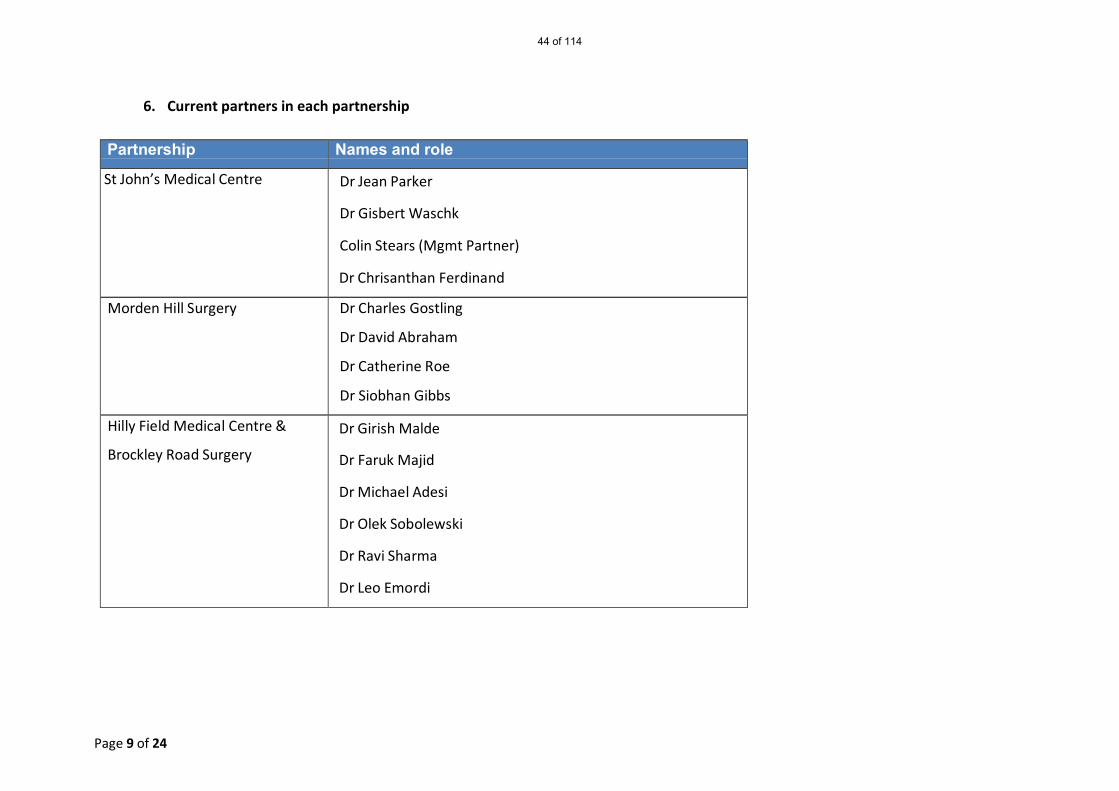
6. Current partners in each partnership
Partnership Names and role
St John’s Medical Centre Dr Jean Parker
Dr Gisbert Waschk
Colin Stears (Mgmt Partner)
Dr Chrisanthan Ferdinand
Morden Hill Surgery Dr Charles Gostling
Dr David Abraham
Dr Catherine Roe
Dr Siobhan Gibbs
Hilly Field Medical Centre &
Brockley Road Surgery
Dr Girish Malde
Dr Faruk Majid
Dr Michael Adesi
Dr Olek Sobolewski
Dr Ravi Sharma
Dr Leo Emordi
44 of 114
Page 10 of 24
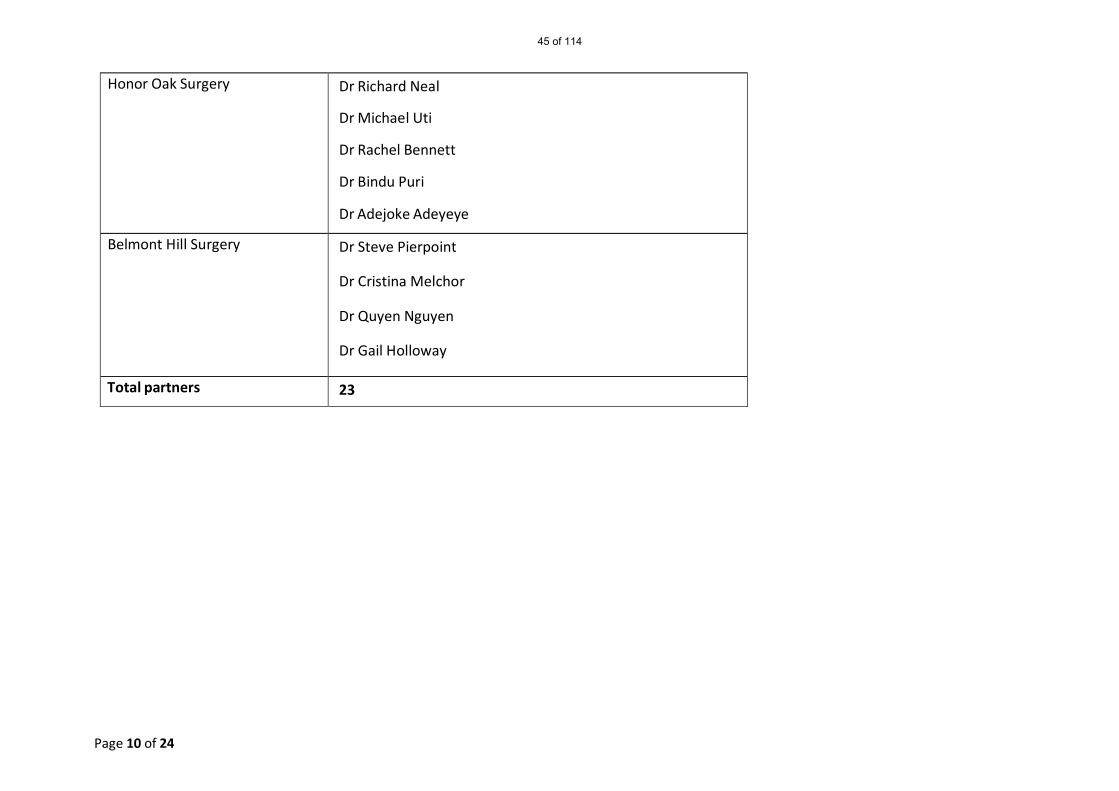
Honor Oak Surgery Dr Richard Neal
Dr Michael Uti
Dr Rachel Bennett
Dr Bindu Puri
Dr Adejoke Adeyeye
Belmont Hill Surgery Dr Steve Pierpoint
Dr Cristina Melchor
Dr Quyen Nguyen
Dr Gail Holloway
Total partners 23
45 of 114

Page 11 of 24
7. List size and age/sex breakdown Data from NHS Digital at 1/1/17
GP_PRACTICE_CODE TOTAL_ALL TOTAL_MALE TOTAL_FEMALE
Belmont Hill 6433 3191 3242
Modern Hill 8934 4380 4554
St Johns 14239 7059 7180
Brockley Road 5317 2621 2696
Hilly Fields 12367 5965 6402
Honor Oak 9406 4700 4706
GP_PRACTICE_CODE MALE_0-4
MALE_5-9
MALE_10-14
MALE_15-19
MALE_20-24
MALE_25-29
MALE_30-34
MALE_35-39
MALE_40-44
MALE_45-49
Belmont Hill 176 154 151 136 142 246 315 356 334 275
Modern Hill 279 259 250 216 238 414 539 481 356 309
St Johns 518 387 315 295 401 752 958 773 640 562
Brockley Road 218 156 84 88 120 272 340 328 230 183
Hilly Fields 420 390 323 281 283 418 586 632 623 505
Honor Oak 381 330 275 255 255 394 436 518 441 392
GP_PRACTICE_CODE MALE_50-54
MALE_55-59
MALE_60-64
MALE_65-69
MALE_70-74
MALE_75-79
MALE_80-84
MALE_85-89
MALE_90-94 MALE_95+
Belmont Hill 233 177 140 123 113 66 30 17 5 2
Modern Hill 289 225 150 127 91 67 53 24 11 2
St Johns 458 338 196 145 125 102 56 21 15 2
Brockley Road 159 125 92 68 50 46 36 19 6 1
Hilly Fields 443 323 204 169 140 93 82 37 10 3
Honor Oak 341 265 129 94 69 56 43 21 5 0
46 of 114

Page 12 of 24
GP_PRACTICE_CODE FEMALE_0-4 FEMALE_5-9 FEMALE_10-14
FEMALE_15-19
FEMALE_20-24
FEMALE_25-29
FEMALE_30-34
FEMALE_35-39
FEMALE_40-44
Belmont Hill 161 177 146 140 183 306 326 315 240
Modern Hill 274 245 198 220 285 505 586 442 337
St Johns 489 413 336 284 509 854 978 717 530
Brockley Road 189 138 111 102 160 338 371 292 192
Hilly Fields 417 395 353 285 342 529 588 652 567
Honor Oak 349 362 272 224 292 439 501 521 366
GP_PRACTICE_CODE FEMALE 45-49
FEMALE 50-54
FEMALE 55-59
FEMALE 60-64
FEMALE 65-69
FEMALE 70-74
FEMALE 75-79
FEMALE 80-84
FEMALE 85-89
FEMALE 90-94 FEMALE 95+
Belmont Hill 235 202 177 132 149 108 117 59 43 18 8
Modern Hill 308 312 231 164 110 100 92 67 51 20 7
St Johns 520 436 310 223 176 153 113 65 55 12 7
Brockley Road 140 145 119 85 78 74 69 43 27 19 4
Hilly Fields 540 433 347 248 207 174 115 115 57 28 10
Honor Oak 350 316 229 160 93 80 65 46 28 11 2
47 of 114

Page 13 of 24
8. Deprivation and mortality
Data from NHS England Primary care web tool (Including Data up to Quarter 1 2016)
Index of Multiple
Deprivation (Q 1 2016)
Income Deprivation Affecting Children (Q 1 2016)
Income deprivation affecting Older People (Q 1 2016)
Standard mortality rates (July 2015)
St Johns MC 27.43 0.3 0.29 130.67
Modern Hill Surgery 39.47 0.54 0.54 119.22
Hilly Fields MC 19.25 0.19 0.24 116.18
Brockley Road Surgery 17.65 0.13 0.2 109.43
Honor Oak 39.93 0.42 0.47 128.46
Belmont Hill 29.47 0.12 0.15 93.31
CCG Mean (2010) 30.82 0.35 0.31 - National Mean (2010) 23.85 0.23 0.23 -
48 of 114
Page 14 of 24
sc h e m e
9. Direct Enhanced Services/Local Commissioned Services 2016/17
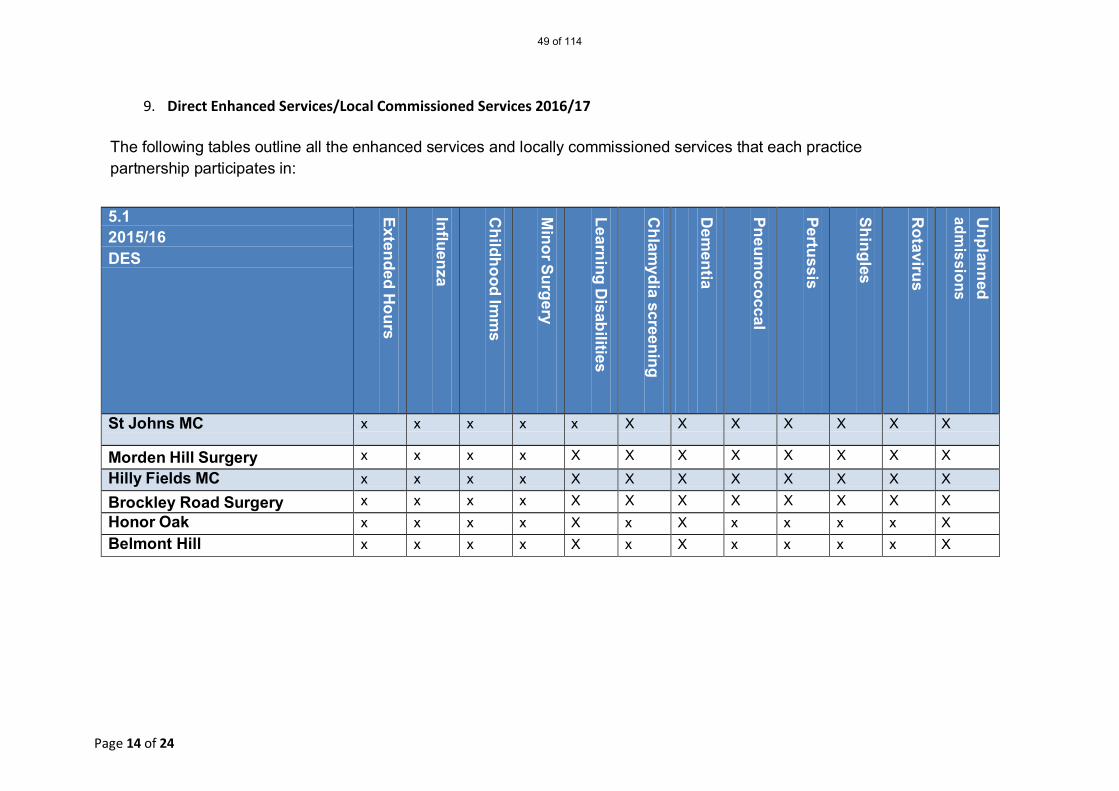
The following tables outline all the enhanced services and locally commissioned services that each practice partnership participates in:
5.1 2015/16 DES
Extended Hours
Influenza
Childhood Im
ms
Minor Surgery
Learning Disabilities
Chlam
ydia screening
Dem
entia Pneum
ococcal
Pertussis
Shingles
Rotavirus
Unplanned
admissions
St Johns MC x x x x x X X X X X X X
Morden Hill Surgery x x x x X X X X X X X X
Hilly Fields MC x x x x X X X X X X X X
Brockley Road Surgery x x x x X X X X X X X X Honor Oak x x x x X x X x x x x X Belmont Hill x x x x X x X x x x x X
49 of 114
Page 15 of 24
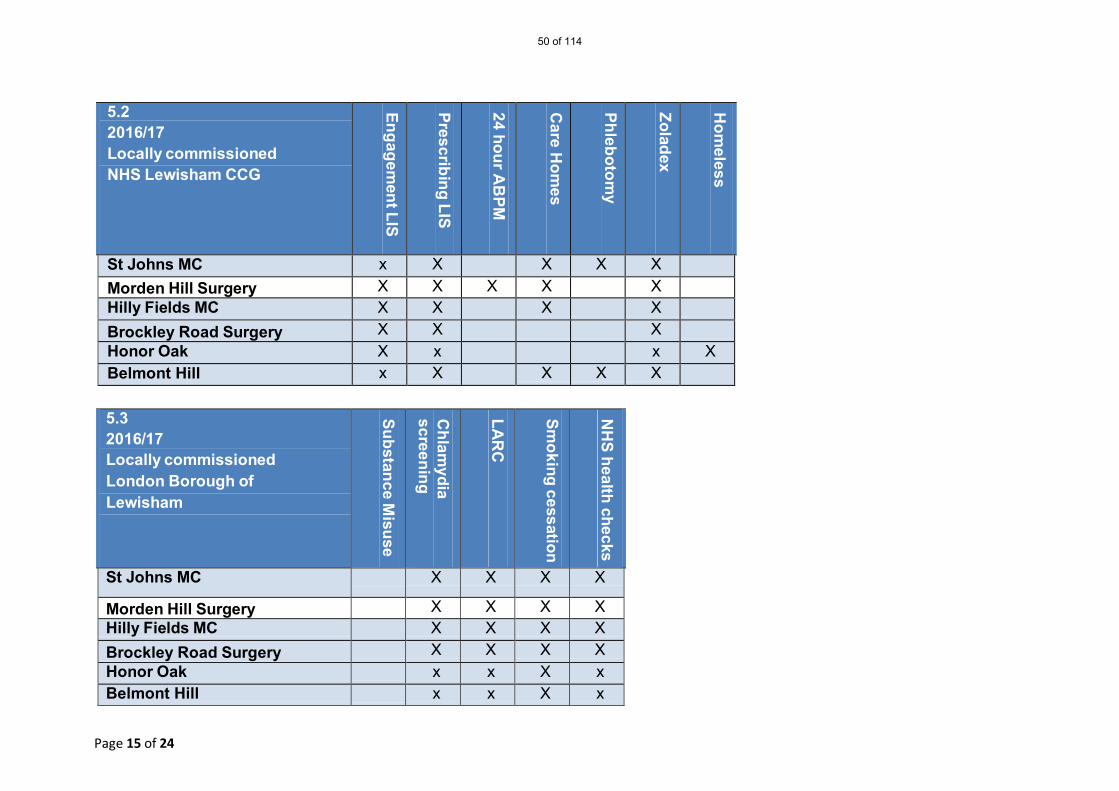
5.2 2016/17 Locally commissioned NHS Lewisham CCG
Engagement LIS
Prescribing LIS
24 hour AB
PM
Care H
omes
Phlebotomy
Zoladex
Hom
eless
St Johns MC x X X X X
Morden Hill Surgery X X X X X
Hilly Fields MC X X X X
Brockley Road Surgery X X X
Honor Oak X x x X Belmont Hill x X X X X
5.3 2016/17 Locally commissioned London Borough of Lewisham
Substance Misuse
Chlam
ydia screening
LAR
C
Smoking cessation
NH
S health checks
St Johns MC X X X X
Morden Hill Surgery X X X X Hilly Fields MC X X X X Brockley Road Surgery X X X X Honor Oak x x X x Belmont Hill x x X x
50 of 114

Page 16 of 24
10. Workforce
The following table lists number of WTE staff in each staff category which includes any unfilled vacancies. Note: GPs are defined by number of sessions and includes GP partner clinical sessions, all other staff groups WTE is defined as 37½ hours.
Workgroups including current unfilled vacancies
GPs Practice Nurses & HCAs
ANPs Managers Admin Reception Data
St Johns MC 3 7 6 5 18
Modern Hill Surgery 4 2 4 1 10
Hilly Fields MC/ Brockley Road Surgery
6 5 5 2 17
Honor Oak 5 1 4 1 9
Belmont Hill 3.75 1 0.25 1 6.48
Note: WTE GPS = 9 sessions All other staff WTE = 37½ hours
51 of 114

Page 17 of 24
11. Quality and Outcomes Framework 2015/16
Practice Total QOF points
Clinical domain
Public Health Domain
Outlining areas of delivery
St John’s Medical Centre
540.23 416.32 96.91 CHD, COPD, diabetes
Morden Hill Surgery 531.64 408.35 91.18 CHD, diabetes
Hilly Fields Medical Centre
511.96 389.49 95.50 CHD, diabetes
Brockley Road Medical Centre
506.95 383.17 97.00 CHD, diabetes, dementia, hypertension, mental health
Honor Oak Group Practice
538.49 417.64 95.97 Diabetes
Belmont Hill 527.18 406.60 96.15 Diabetes, Mental health
52 of 114

Page 18 of 24
12. NHS England Primary Care Web Tool general practice outcome standards
The following are identified areas that have Level 1 triggers in the current practices. These are outcomes where the practice performance is below the national average. No practice has any Level 2 triggers.8
General Practice Outcome Standards
6a) AF Est D
iag R
ate
12) CH
D Est D
iag Rate
13a) Dem
entia D
iagnosis Rate (A
dj)
27d) SMI Physical
Health (d1+d2)
9) CO
PD Est D
iag Rate
14a) %N
aproxen and Ibuprofen
21) Satisfaction (A
ccess) a-c
27d) SMI Physical
Health (d1+d2)
4b) Smoking Status
(LTC)
10) Asthm
a Est Diag
Rate
17) Satisfaction (Q
uality) a-g
20) Patient Experience
27c) SMI Physical
Health (B
P)
5a) Smoking
Cessation A
dvice
26c) Depression
Assessm
ent
St Johns MC x x x x x x x x x
Modern Hill Surgery x x x x
Hilly Fields MC x x x x x x x x x
Brockley Road Surgery x x x x x x x x x
Honor Oak x x x x x x
Belmont Hill x x x x x
Total 6 4 1 3 5 1 4 3 2 2 2 3 3 2 1
3 Level One Trigger – The practice is in the mid-range 60-95% when compared to the absolute variance from 1. Level Two Trigger – The practice is in the bottom
5% when compared to the absolute variance from 1
53 of 114
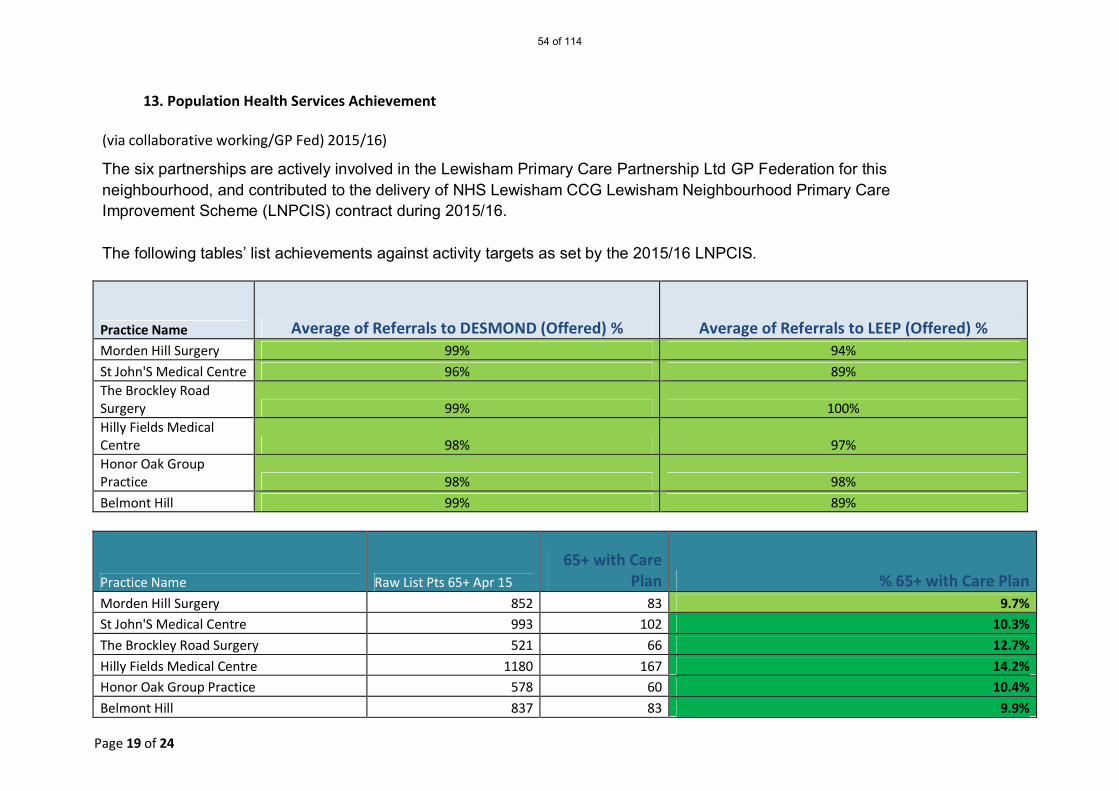
Page 19 of 24
13. Population Health Services Achievement
(via collaborative working/GP Fed) 2015/16)
The six partnerships are actively involved in the Lewisham Primary Care Partnership Ltd GP Federation for this neighbourhood, and contributed to the delivery of NHS Lewisham CCG Lewisham Neighbourhood Primary Care Improvement Scheme (LNPCIS) contract during 2015/16.
The following tables’ list achievements against activity targets as set by the 2015/16 LNPCIS.
Practice Name Average of Referrals to DESMOND (Offered) % Average of Referrals to LEEP (Offered) % Morden Hill Surgery 99% 94%
St John'S Medical Centre 96% 89% The Brockley Road Surgery 99% 100% Hilly Fields Medical Centre 98% 97% Honor Oak Group Practice 98% 98%
Belmont Hill 99% 89%
Practice Name Raw List Pts 65+ Apr 15
65+ with Care Plan % 65+ with Care Plan
Morden Hill Surgery 852 83 9.7% St John'S Medical Centre 993 102 10.3%
The Brockley Road Surgery 521 66 12.7%
Hilly Fields Medical Centre 1180 167 14.2% Honor Oak Group Practice 578 60 10.4%
Belmont Hill 837 83 9.9%
54 of 114
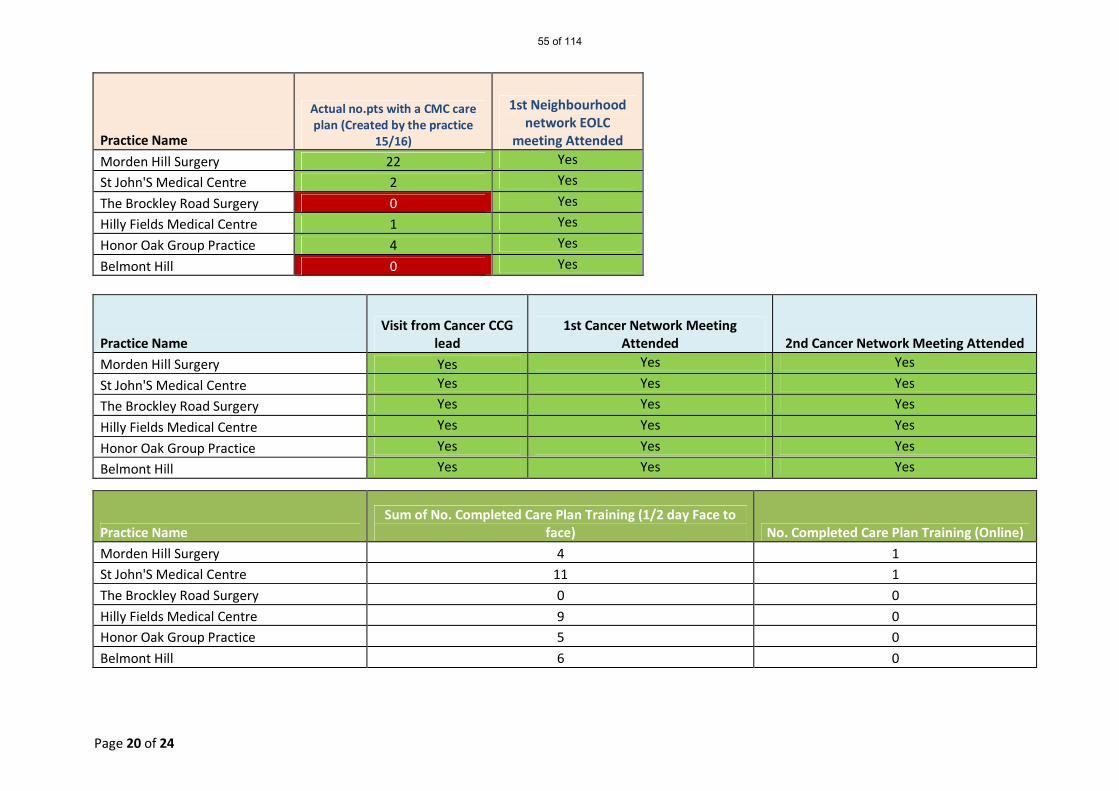
Page 20 of 24
Practice Name
Actual no.pts with a CMC care plan (Created by the practice
15/16)
1st Neighbourhood network EOLC
meeting Attended
Morden Hill Surgery 22 Yes
St John'S Medical Centre 2 Yes
The Brockley Road Surgery 0 Yes
Hilly Fields Medical Centre 1 Yes
Honor Oak Group Practice 4 Yes
Belmont Hill 0 Yes
Practice Name Visit from Cancer CCG
lead 1st Cancer Network Meeting
Attended 2nd Cancer Network Meeting Attended
Morden Hill Surgery Yes Yes Yes
St John'S Medical Centre Yes Yes Yes
The Brockley Road Surgery Yes Yes Yes
Hilly Fields Medical Centre Yes Yes Yes
Honor Oak Group Practice Yes Yes Yes
Belmont Hill Yes Yes Yes
Practice Name Sum of No. Completed Care Plan Training (1/2 day Face to
face) No. Completed Care Plan Training (Online)
Morden Hill Surgery 4 1 St John'S Medical Centre 11 1
The Brockley Road Surgery 0 0
Hilly Fields Medical Centre 9 0 Honor Oak Group Practice 5 0
Belmont Hill 6 0
55 of 114
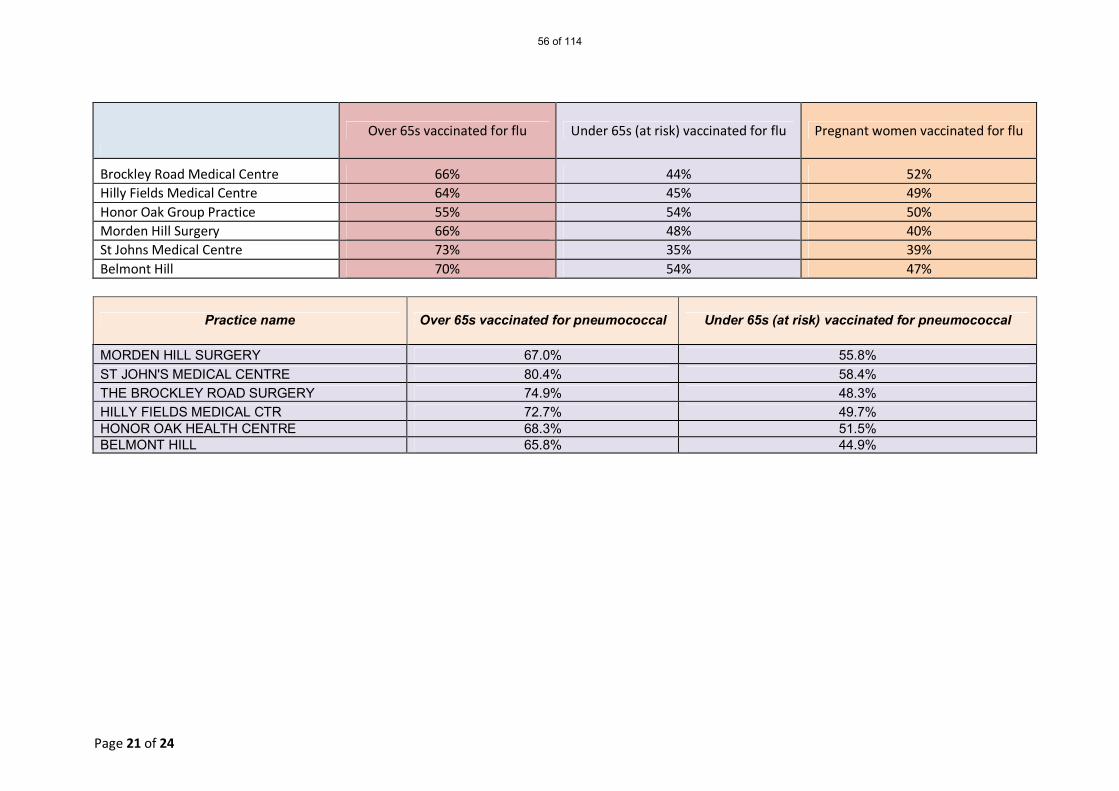
Page 21 of 24
Over 65s vaccinated for flu Under 65s (at risk) vaccinated for flu Pregnant women vaccinated for flu
Brockley Road Medical Centre 66% 44% 52% Hilly Fields Medical Centre 64% 45% 49% Honor Oak Group Practice 55% 54% 50% Morden Hill Surgery 66% 48% 40% St Johns Medical Centre 73% 35% 39% Belmont Hill 70% 54% 47%
Practice name Over 65s vaccinated for pneumococcal Under 65s (at risk) vaccinated for pneumococcal
MORDEN HILL SURGERY 67.0% 55.8% ST JOHN'S MEDICAL CENTRE 80.4% 58.4% THE BROCKLEY ROAD SURGERY 74.9% 48.3% HILLY FIELDS MEDICAL CTR 72.7% 49.7% HONOR OAK HEALTH CENTRE 68.3% 51.5% BELMONT HILL 65.8% 44.9%
56 of 114
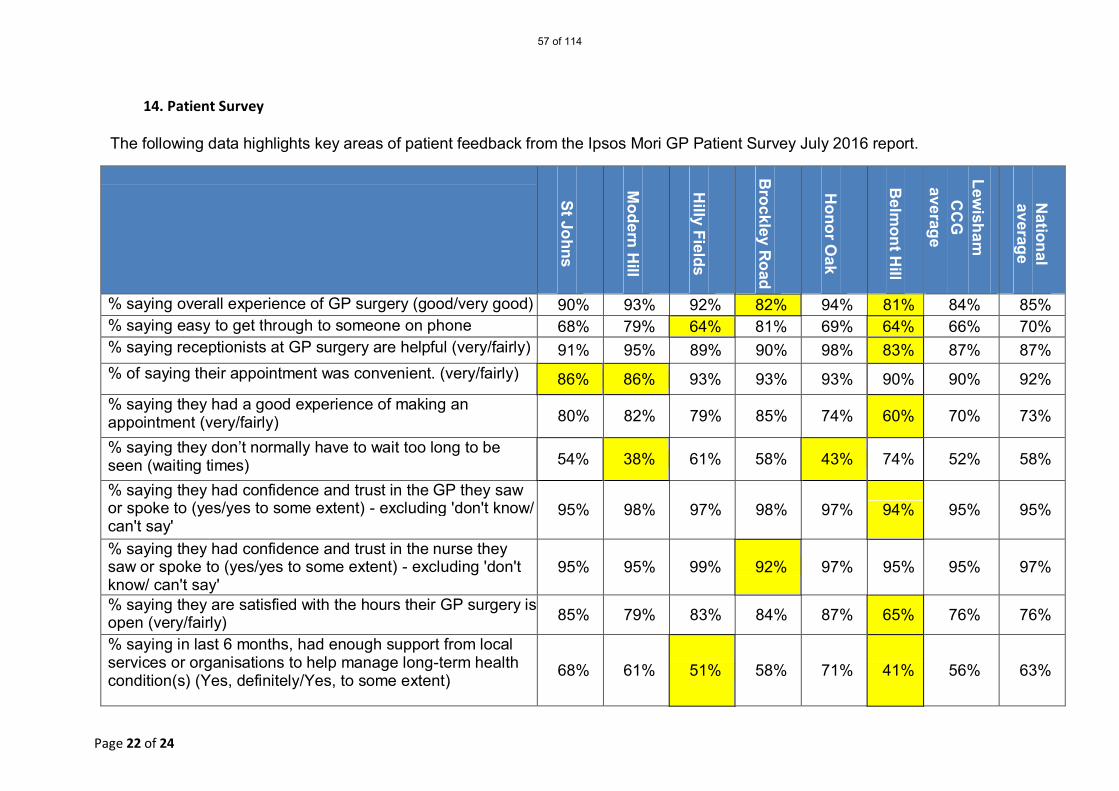
Page 22 of 24
14. Patient Survey
The following data highlights key areas of patient feedback from the Ipsos Mori GP Patient Survey July 2016 report.
St Johns
Modern H
ill
Hilly Fields
B
rockley Road
H
onor Oak
Belm
ont Hill
Lew
isham
CC
G
average
National
average
% saying overall experience of GP surgery (good/very good) 90% 93% 92% 82% 94% 81% 84% 85% % saying easy to get through to someone on phone (very/fairly)
68% 79% 64% 81% 69% 64% 66% 70% % saying receptionists at GP surgery are helpful (very/fairly) 91% 95% 89% 90% 98% 83% 87% 87% % of saying their appointment was convenient. (very/fairly) 86% 86% 93% 93% 93% 90% 90% 92% % saying they had a good experience of making an appointment (very/fairly) 80% 82% 79% 85% 74% 60% 70% 73%
% saying they don’t normally have to wait too long to be seen (waiting times) 54% 38% 61% 58% 43% 74% 52% 58%
% saying they had confidence and trust in the GP they saw or spoke to (yes/yes to some extent) - excluding 'don't know/ can't say'
95% 98% 97% 98% 97% 94% 95% 95%
% saying they had confidence and trust in the nurse they saw or spoke to (yes/yes to some extent) - excluding 'don't know/ can't say'
95% 95% 99% 92% 97% 95% 95% 97%
% saying they are satisfied with the hours their GP surgery is open (very/fairly) 85% 79% 83% 84% 87% 65% 76% 76%
% saying in last 6 months, had enough support from local services or organisations to help manage long-term health condition(s) (Yes, definitely/Yes, to some extent) 68% 61% 51% 58% 71% 41% 56% 63%
57 of 114
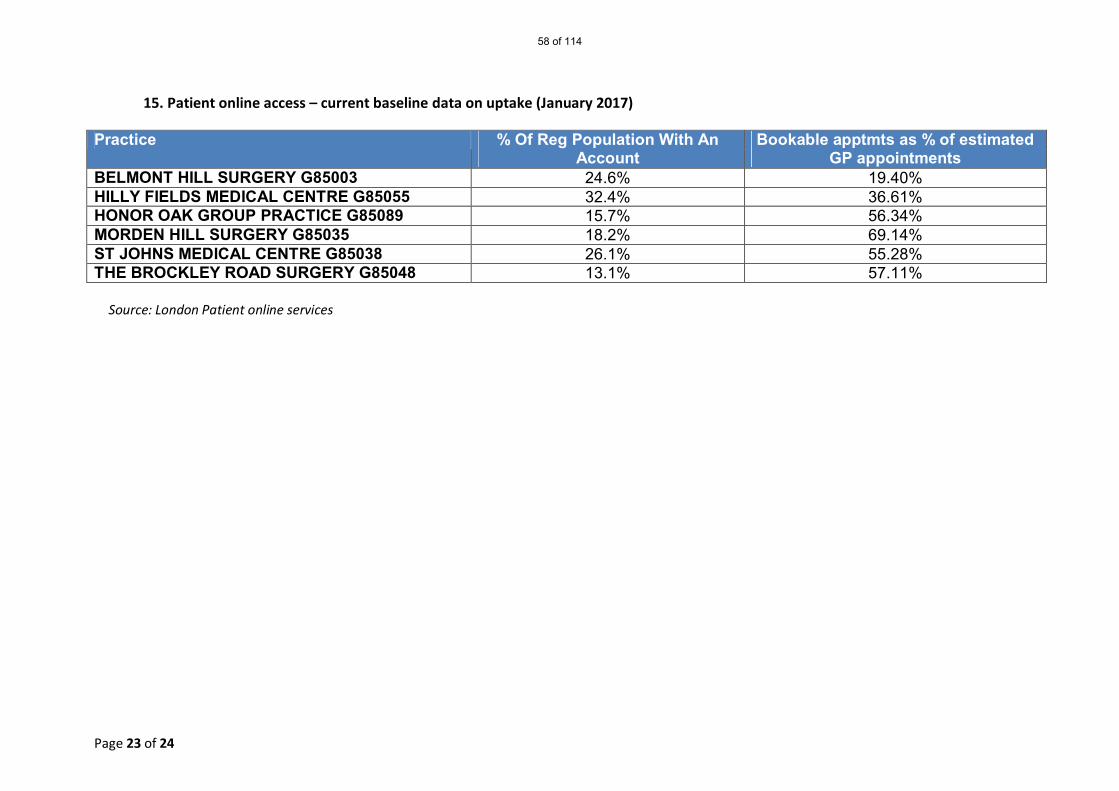
Page 23 of 24
15. Patient online access – current baseline data on uptake (January 2017) Practice % Of Reg Population With An
Account Bookable apptmts as % of estimated
GP appointments BELMONT HILL SURGERY G85003 24.6% 19.40% HILLY FIELDS MEDICAL CENTRE G85055 32.4% 36.61% HONOR OAK GROUP PRACTICE G85089 15.7% 56.34% MORDEN HILL SURGERY G85035 18.2% 69.14% ST JOHNS MEDICAL CENTRE G85038 26.1% 55.28% THE BROCKLEY ROAD SURGERY G85048 13.1% 57.11%
Source: London Patient online services
58 of 114
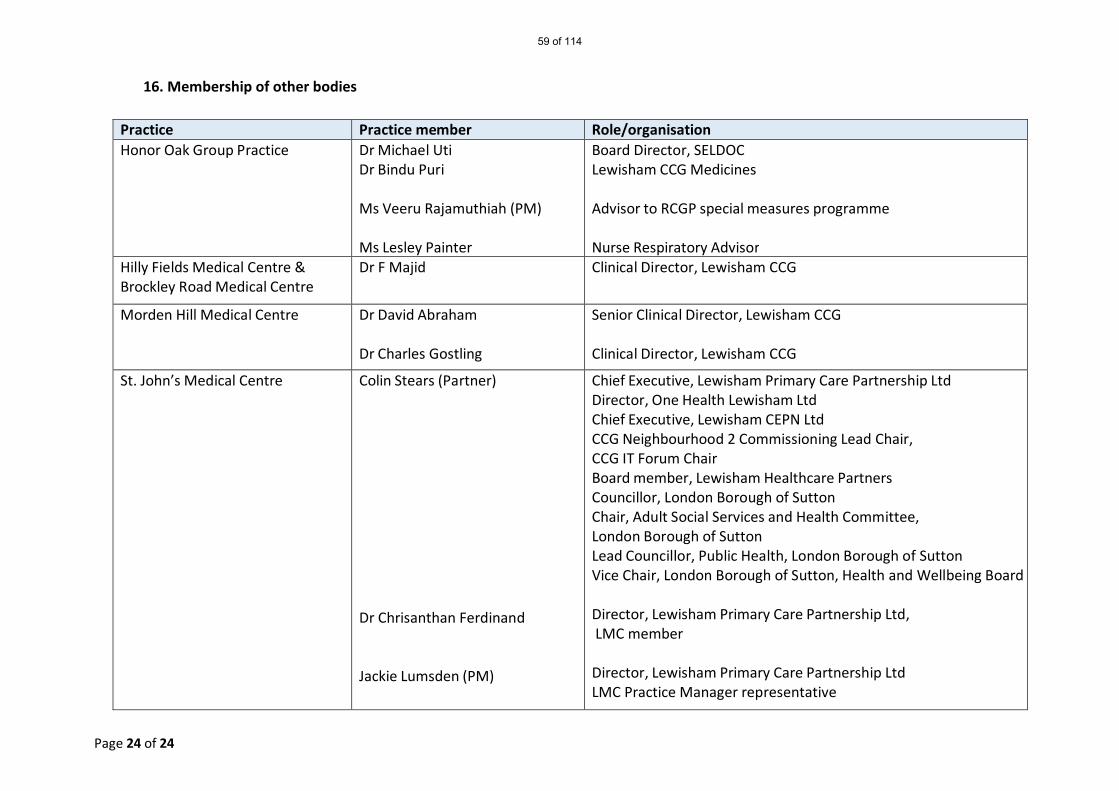
Page 24 of 24
16. Membership of other bodies
Practice Practice member Role/organisation Honor Oak Group Practice Dr Michael Uti
Dr Bindu Puri Ms Veeru Rajamuthiah (PM)
Ms Lesley Painter
Board Director, SELDOC Lewisham CCG Medicines Advisor to RCGP special measures programme Nurse Respiratory Advisor
Hilly Fields Medical Centre & Brockley Road Medical Centre
Dr F Majid Clinical Director, Lewisham CCG
Morden Hill Medical Centre Dr David Abraham Dr Charles Gostling
Senior Clinical Director, Lewisham CCG Clinical Director, Lewisham CCG
St. John’s Medical Centre Colin Stears (Partner)
Dr Chrisanthan Ferdinand Jackie Lumsden (PM)
Chief Executive, Lewisham Primary Care Partnership Ltd Director, One Health Lewisham Ltd Chief Executive, Lewisham CEPN Ltd CCG Neighbourhood 2 Commissioning Lead Chair, CCG IT Forum Chair Board member, Lewisham Healthcare Partners Councillor, London Borough of Sutton Chair, Adult Social Services and Health Committee, London Borough of Sutton Lead Councillor, Public Health, London Borough of Sutton Vice Chair, London Borough of Sutton, Health and Wellbeing Board Director, Lewisham Primary Care Partnership Ltd, LMC member Director, Lewisham Primary Care Partnership Ltd LMC Practice Manager representative
59 of 114
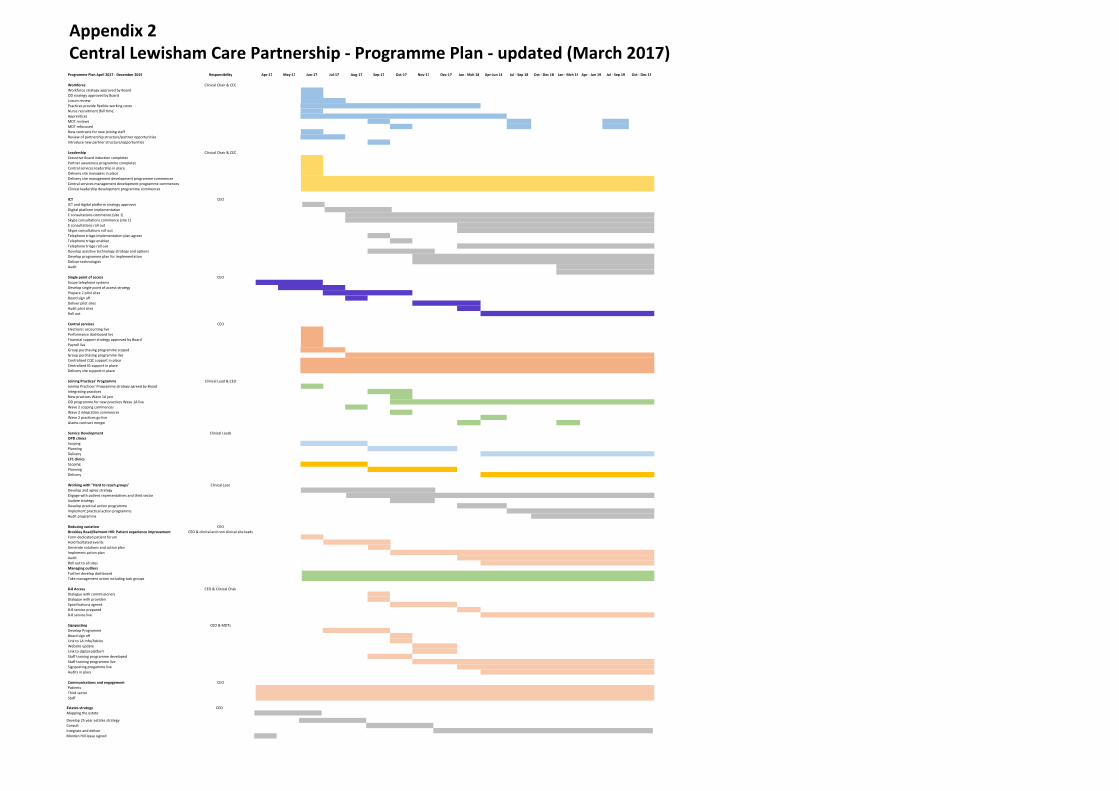
Programme Plan April 2017 ‐ December 2019 Responsibility Apr‐17 May‐17 Jun‐17 Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17 Jan ‐ Mch 18 Apr‐Jun 18 Jul ‐ Sep 18 Oct ‐ Dec 18 Jan ‐ Mch 19 Apr ‐ Jun 19 Jul ‐ Sep 19 Oct ‐ Dec 19
Workforce Clinical Chair & CEO
Workforce strategy approved by Board
OD strategy approved by Board
Locum review
Practices provide flexible working cover
Nurse recruitment (full time)
Apprentices
MDT reviews
MDT refocused
New contracts for new joining staff
Review of partnership structure/partner opportunities
Introduce new partner structure/opportunities
Leadership Clinical Chair & CEO
Executive Board induction completed
Partner awareness programme completed
Central services leadership in place
Delivery site managers in place
Delivery site management development programme commences
Central services management development programme commences
Clinical leadership development programme commences
ICT CEO
ICT and digital platform strategy approved
Digital platform implementation
E consultations commence (site 1)
Skype consultations commence (site 1)
E consultations roll out
Skype consultations roll out
Telephone triage implementation plan agreed
Telephone triage enabled
Telephone triage roll out
Develop assistive technology strategy and options
Develop programme plan for implementation
Deliver technologies
Audit
Single point of access CEO
Scope telephone systems
Develop single point of access strategy
Prepare 2 pilot sites
Board sign off
Deliver pilot sites
Audit pilot sites
Roll out
Central services CEO
Electronic accounting live
Performance dashboard live
Financial support strategy approved by Board
Payroll live
Group purchasing programme scoped
Group purchasing programme live
Centralised CQC support in place
Centralised IG support in place
Delivery site support in place
Joining Practices' Programme Clinical Lead & CEO
Joining Practices' Programme strategy agreed by Board
Integrating practices
New practices Wave 1A join
OD programme for new practices Wave 1A live
Wave 2 scoping commences
Wave 2 integration commences
Wave 2 practices go live
Assess contract merger
Service Development Clinical Leads
OPD clinics
Scoping
Planning
Delivery
LTC clinics
Scoping
Planning
Delivery
Working with "Hard to reach groups" Clinical Lead
Develop and agree strategy
Engage with patient representatives and third sector
Update strategy
Develop practical action programme
Implement practical action programme
Audit programme
CEO
CEO & clinical and non clinical site leads
Reducing variation
Brockley Road/Belmont HIll: Patient experience improvement Form dedicated patient forum
Hold faciltated events
Generate solutions and action plan
Implement action plan
Audit
Roll out to all sites
Managing outliers
Further develop dashboard
Take management action including task groups
8‐8 Access CEO & Clinical Chair
Dialogue with commissioners
Dialogue with providers
Specifications agreed
8‐8 service prepared
8‐8 service live
Signposting CEO & MDTs
Develop Programme
Board sign off
Link to LA Info/Advice
Website update
Link to digital platform
Staff training programme developed
Staff training programme live
Signposting progamme live
Audits in place
Communications and engagement CEO
Patients
Third sector
Staff
Appendix 2Central Lewisham Care Partnership - Programme Plan - updated (March 2017)
Develop 25 year estates strategy
Consult
Integrate and deliver
Morden Hill lease signed
Estates strategy CEO
Mapping the estate

Page 1 of 3
Lewisham Primary Care Joint Committee (PCJC) meeting
30th March 2017
Part 1 meeting
Meeting held via teleconference
DRAFT Minutes
Meeting Chair: Ray Warburton
Lewisham Primary Care Joint Committee Attendees: Ray Warburton (RW) Member CCG Lay Member Dr Marc Rowland (MR) Member CCG Chair Dr Jacky McLeod (JM) Member CCG Governing Body GP Liz Wise (LW) Member NHS England – London (Director of Primary Care) Other attendees:
Tony Read (TR) CCG Chief Financial Officer Jill Webb (JW) NHS England – London (Head of Primary Care) Ashley O'Shaughnessy (AOS) CCG Deputy Director Primary Care Ian Ross (IR) CCG Associate Director of Primary Care Transformation Apologies:
Martin Wilkinson CCG Chief Officer Gary Beard NHS England – London (Assistant Head of Primary Care)
61 of 114
Page 2 of 3
Item Action 1. Introduction and apologies
RW welcomed all to the meeting of the Primary Care Joint Committee of NHS Lewisham CCG and NHS England (held via teleconference) to consider the urgent planned decision of the proposed merger between Belmont Hill Surgery and the Central Lewisham Care Partnership. The outcome of this meeting will be reported publically at the first meeting of the new Lewisham Primary Care Commissioning Committee scheduled for April 2017 under fully delegated Primary Care Commissioning arrangements. Apologies were received from Martin Wilkinson, CCG Chief Officer and Gary Beard, NHS England – London (Assistant Head of Primary Care).
2. Declaration of Interests RW declared that he is patient at Belmont Hill Surgery. No other new Declarations of Interest were made.
3. Matters Arising None.
For Decision 4.
Proposed merger of Belmont Hill Surgery and the Central Lewisham Care Partnership
JW introduced the circulated papers which requested that the Joint Committee approve the addition of Belmont Hill Surgery to the previously approved merger of the Central Lewisham Care Partnership, subject to formal feedback from Lewisham Healthwatch. The circulated business case and supporting papers build on the initial business case for the merger between Brockley Road Medical Centre, Hilly Fields Medical Centre, Morden Hill Surgery, Honor Oak Group Practice and St John’s Medical Centre (to form the Central Lewisham Care Partnership), which was agreed at the Lewisham Primary Care Joint Committee meeting held on the 8th February 2017. Key points to note were:
• That the Central Lewisham Care Partnership had accepted/responded to all the original conditions to which their original merger business case was subject to
• That go-live of the merger had been delayed to the 1st July 2017 but that this will allow Belmont Hill Surgery to go-live at the same time as the other practices
• That an additional £15,000 had been secured to support the merger from the “Primary Care Working at Scale pilot” of the Transforming Primary Care Programme of the Healthy London Partnerships
62 of 114

Page 3 of 3
• That formal feedback from HealthWatch on both the original merger and the addition of Belmont Hill Surgery was still outstanding
• That the practices have requested additional financial support to meet the
costs of communicating the new partnership arrangements to patients, estimated to be in the region of £3,200, based on a list size of 6,433 for Belmont Hill Surgery
Members were asked to confirm their support/provide comment:
• MR gave his approval to the business case.
• JM gave her approval to the business case.
• LW gave her approval to the business case but queried if there were any key risks to be considered. It was commented that some of the major risks of a merger of this scale have actually been mitigated by the corporate partnership model of merger that had been adopted, where contracts and clinical systems are not fully merged from the outset.
• RW gave his approval to the business case, emphasizing the condition for
formal feedback from HealthWatch.
He did query at what stage a primary care provider might become ‘too’ big. It was commented that each merger business case would be considered on its own merits, that there are already some practice groups of over 100,000 patients and that the addition of Belmont Hill Surgery would not create the need to consider this situation in Lewisham at this stage. RW also queried at what stage patients at Belmont Hill Surgery would see improvements in service quality and satisfaction in the areas that were highlighted as currently varying from CCG and/or National averages. It was commented that there were both immediate short term actions as well as more medium to long term actions articulated in the business case and supporting programme plan to address this.
TR gave his support to the business case subject to the key points raised by JW. Based on the above discussions, the Lewisham Joint Committee gave its approval to the addition of Belmont Hill Surgery to the previously approved merger of the Central Lewisham Care Partnership, including acceptance of the additional cost of writing to patients about the merger, subject to formal feedback from Lewisham Healthwatch.
Any other business 5. None.
63 of 114
NHS Lewisham CCG Primary Care Commissioning Committee Terms of Reference
March 2017 Version 4.1
64 of 114
Terms of Reference
March 2017
Author/s: NHS England and Lewisham CCG (localised)
Effective Date: 1st April 2017
Review Date: 31st March 2018
Document owner/CCG Contact/s: Victoria Medhurst, Associate Director Integrated Governance
Diana Braithwaite, Director of Commissioning & Primary Care
Lewisham CCG Consultation:
Lewisham CCG Primary Care Programme Board Workshop – 15th February 2017
Ray Warburton OBE, Lay Member, Audit Chair and CoI Champion – 22nd February 2017
Ratified: Governing Body (Chairs action as per Governing Body on 09.03.2017)
Version Control Version Date Amendment By 0.1 09/03/2017 Draft to Governing Body Victoria Medhurst 0.2 27/03/2017 Amendments sent to GB members
following discussion at GB Victoria Medhurst
0.3 30/03/2017 Addition of 3rd Lay Member title following comments from R Warburton
Victoria Medhurst
65 of 114

Terms of reference – NHS Lewisham CCG Primary Care Commissioning Committee Introduction 1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that
NHS England was inviting CCGs to expand their role in primary care commissioning and to submit expressions of interest setting out the CCG’s preference for how it would like to exercise expanded primary medical care commissioning functions. One option available was that NHS England would delegate the exercise of certain specified primary care commissioning functions to a CCG.
2. In accordance with its statutory powers under section 13Z of the National Health Service
Act 2006 (as amended), NHS England has delegated the exercise of the functions specified in Schedule 2 to these Terms of Reference to NHS Lewisham CCG. The delegation is set out in Schedule 1.
3. The CCG has established the NHS Lewisham CCG Primary Care Commissioning
Committee (“Committee”). The Committee will function as a corporate decision-making body for the management of the delegated functions and the exercise of the delegated powers as set out in NHS Lewisham CCG’s Constitution and Scheme of Delegation.
4. It is a committee comprising representatives of the following organisations:
• NHS Lewisham CCG; • In attendance:
o Lewisham Council representative of the Health and Wellbeing Board; o Lewisham Local Medical Committee; o Lewisham Healthwatch; o Officers as required to undertake business of the committee, including South
east London CCGs Primary Care Contracts Team.
Statutory Framework 5. NHS England has delegated to the CCG authority to exercise the primary care
commissioning functions set out in Schedule 2 in accordance with section 13Z of the NHS Act.
66 of 114
6. Arrangements made under section 13Z may be on such terms and conditions (including terms as to payment) as may be agreed between the NHS England Board and the CCG.
7. Arrangements made under section 13Z do not affect the liability of NHS England for the
exercise of any of its functions. However, the CCG acknowledges that in exercising its functions (including those delegated to it), it must comply with the statutory duties set out in Chapter A2 of the NHS Act and including: a) Management of conflicts of interest (section 14O); b) Duty to promote the NHS Constitution (section 14P); c) Duty to exercise its functions effectively, efficiently and economically (section 14Q); d) Duty as to improvement in quality of services (section 14R); e) Duty in relation to quality of primary medical services (section 14S); f) Duties as to reducing inequalities (section 14T); g) Duty to promote the involvement of each patient (section 14U); h) Duty as to patient choice (section 14V); i) Duty as to promoting integration (section 14Z1); j) Public involvement and consultation (section 14Z2).
8. The CCG will also need to specifically, in respect of the delegated functions from NHS England, exercise those in accordance with the relevant provisions of section 13 of the NHS Act; a. Duty to have regard to impact on services in certain areas (section 13O); b. Duty as respects variation in provision of health services (section 13P).
9. The Committee is established as a committee of the CCG Governing Body in accordance with Schedule 1A of the “NHS Act”.
10. The members acknowledge that the Committee is subject to any directions made by
NHS England or by the Secretary of State. Role of the Committee 11. The Committee has been established in accordance with the above statutory provisions
to enable the membership of the committee to make collective decisions on the review, planning and procurement of primary care services in Lewisham, under delegated authority from NHS England.
67 of 114
12. In performing its role the Committee will exercise its management of the functions in
accordance with the agreement entered into between NHS England and NHS Lewisham CCG, which will sit alongside the delegation and terms of reference.
13. The functions of the Committee are undertaken in the context of a desire to promote
primary care co-commissioning to increase quality, efficiency, productivity and value for money and to remove administrative barriers.
14. The role of the Committee shall be to carry out the functions relating to the
commissioning of primary medical services under section 83 of the NHS Act. 15. The Committee has an operational remit under the strategic direction approved by the
Governing Body in relation to primary care, which includes; a. GMS, PMS and APMS contracts (including the design of PMS and APMS contracts,
monitoring of contracts, taking contractual action such as issuing breech/remedial notices and removing a contract);
b. Newly designed enhanced services; c. Design of local incentives schemes as an alternative to Quality Outcomes Framework
(QOF); d. decisions in relation to the establishment of new GP practices (including branch
surgeries) and closure of GP practices; e. Approving practice mergers; f. Making decisions on ‘discretionary’ payments (e.g. returner/retainer schemes); g. Decisions about commissioning urgent care (including home visits as required) for out
of area registered patients; h. Planning primary medical care services in the Lewisham including carrying out needs
assessments; i. Undertaking reviews of primary medical care services in the Lewisham; j. Decisions in relation to the management of GP practice performance and including
(and without limitation); decisions and liaison with the Clinical Quality Commission (CQC), where there is reported non-compliance with standards (excluding any decisions in relation to the performers list);
k. Management of the delegated funds in the Lewisham; l. Premises Costs Directions functions; m. Co-ordinating a common approach to the commissioning of primary care services with
other commissioners in the area where appropriate; and
68 of 114

n. Such other ancillary activities as are necessary in order to exercise the Delegated Functions.
16. The CCG will also carry out other activities as detailed in Schedule 1 of the Delegation Agreement between NHS Lewisham CCG and NHS England.
17. In particular the Committee will support the Governing Body in fulfilling the following functions and duties to:
a. Meet the public sector equality duty;
b. Act effectively, efficiently and economically;
c. Act with a view to securing continuous improvement to the quality of services;
d. Have regard to the need to reduce inequalities;
e. Promote the involvement of patients, their carers and representatives in decisions
about their healthcare;
f. Act with a view to enabling patients to make choices;
g. Promote innovation; and
h. Act with a view to promoting integration of both health services with other health
services and health services with health-related and social care services where
the CCG considers that this would improve the quality of services or reduce
inequalities.
Geographical Coverage 18. The Committee will make decisions in respect of primary care in the London Borough of
Lewisham population including GP registered population. Membership 19. The Committee shall consist of: 19.1Members with voting rights
a. 3 x Lay Members o Chair: Lay Member for Primary Care o Vice Chair: Lay Member responsible for Patient Public Engagement o Lay Member: Chair of the Audit Committee and Conflicts of Interest Guardian
b. CCG Chair c. 2 Governing Body GP Members
69 of 114
d. Registered Nurse or Secondary Care Specialist (single member) e. CCG Chief Officer f. CCG Chief Financial Officer g. Director of Commissioning & Primary Care 19.2 Non-Voting Members a. Local Medical Committee Representative b. Healthwatch Representative c. Local Authority Representative of the Health and Wellbeing Board (Elected Member or
Mandated Officer) d. Officers as required to undertake business of the committee e. NHS England Representative 20. The Chair of the Committee shall be a Lay Member of NHS Lewisham CCG. This will not
be the Lay Member responsible for Audit. 21. The Vice Chair of the Committee shall be a Lay Member of NHS Lewisham CCG. This
will not be the Lay Member responsible for Audit. Meetings and Voting 22. As a committee of the Governing Body, the Committee will operate in accordance with
the CCG’s Standing Orders (in line with NHS England Standard Operating Procedures). This includes the capacity to manage urgent matters outside the normal arrangements.
23. The aim of the Committee will be to achieve consensus decision-making wherever possible. In the event that a vote is required, each member of the Committee shall have one vote. The Committee shall reach decisions by a simple majority of members present, but with the Chair having a second and deciding vote, if necessary.
Quorum 24. The quorum shall be a minimum of 4 members, of which 2 must be Lay Members.
25. Where a quorum cannot be convened from the membership, owing to arrangements for
the management of conflicts of interest or potential conflicts of interest; the Chair of the meeting will comply with the conflicts of interest policy.
70 of 114

26. This may result in; a. The meeting being deferred b. A discussion being undertaken but the decision deferred until the next meeting c. Discussion being undertaken being deferred to the Governing Body Frequency of meetings 27. The Committee will meet regularly 6 times per year. After 12 months the frequency will
be reviewed.
28. Meetings of the Committee shall: a. be held in public, subject to the application of 25(b); b. the Committee may resolve to exclude the public from a meeting that is open to the
public (whether during the whole or part of the proceedings) whenever publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted or for other special reasons stated in the resolution and arising from the nature of that business or of the proceedings or for any other reason permitted by the Public Bodies (Admission to Meetings) Act 1960 as amended or succeeded from time to time;
c. the closed confidential part of the meeting (as provided for at 25(b) above) shall be referred to as Part 2 of the meeting and shall have a separate agenda and minutes;
d. the Committee may invite the representatives of the local authority (Health and Wellbeing Board), Local Medical Committees and Healthwatch to Part 2 of any meeting where it considers it is appropriate for such representatives to attend all or part of Part 2 of the meeting.
29. The committee may meet in common with other CCGs in south east London (NHS CCG
Bexley, NHS CCG Bromley, NHS CCG Greenwich, NHS CCG Lewisham and NHS CCG Southwark – or any combination of these CCGs) when there is common business to transact.
30. Members of the Committee have a collective responsibility for the operation of the Committee. They will participate in discussion, review evidence and provide objective expert input to the best of their knowledge and ability, and endeavour to reach a collective view.
71 of 114

31. The Committee may delegate tasks to such individuals, sub-committees or individual members as it shall see fit, provided that any such delegations are consistent with the parties’ relevant governance arrangements, are recorded in a scheme of delegation, are governed by terms of reference as appropriate and reflect appropriate arrangements for the management of conflicts of interest.
32. The Committee may call additional experts to attend meetings on an ad hoc basis to
inform discussions. 33. Members of the Committee shall respect confidentiality in attending and undertaking the
business of the committee. 34. The Committee will present an executive summary report and its minutes to the
governing body of NHS Lewisham CCG and the London area team of NHS England following each meeting for information, including the minutes of any sub-committees to which responsibilities are delegated under paragraph 28 above.
35. The CCG will also comply with any reporting requirements set out in its Constitution. 36. Terms of Reference will be reviewed on an annual basis.
Accountability of the Committee 37. The Committee will be accountable for the expenditure of the primary care budget
delegated from NHS England to the Governing Body of Lewisham CCG. Responsibility for authorising expenditure against this budget may be further delegated only as set out in the Scheme of Reservation and Delegation ratified by the Governing Body.
38. For the avoidance of doubt, in the event of any conflict between the terms of the CCG’s Operational Scheme of Delegation, the Committee’s Terms of Reference and the CCG’s Prime Financial Policies, the Operational Scheme of Delegation will prevail.
39. The Committee may be required where appropriate to provide reports and information to other Committees of the CCG.
Decisions 40. The Committee will make decisions within the bounds of its remit as set out in clause 22.
72 of 114

41. The Committee will ensure that any conflicts of interest are dealt with in accordance with
the CCG’s Constitution and Standards of Business Conduct Policies which for the avoidance of doubt may include members (voting or otherwise) being excluded from a decision and/or the discussions leading thereto.
42. The decisions of the Committee shall be binding on NHS Lewisham CCG and NHS England.
43. All attendees are required to declare their interests as a standing agenda item for every committee before the item is discussed, in line with the Lewisham CCG policy on Conflicts of Interest (http://www.lewishamccg.nhs.uk/news-publications/Policies/Documents/Lewisham%20CCG%20Conflicts%20of%20Interest%20Policy%20November%202016.pdf).
44. The chair of the meeting of has ultimate responsibility for deciding whether there is a
conflict of interest and for taking the appropriate course of action in order to manage the conflict of interest.
45. In the event that the chair of a meeting has a conflict of interest, the vice chair is
responsible for deciding the appropriate course of action in order to manage the conflict of interest. If the vice chair is also conflicted then the remaining non- conflicted voting members of the meeting should agree between themselves how to manage the conflict(s).
46. In making such decisions, the chair (or vice chair or remaining non-conflicted members
as above) may wish to consult with the Conflicts of Interest Guardian or another member of the governing body.
47. The chair should ask at the beginning of each meeting if anyone has any conflicts of
interest to declare in relation to the business to be transacted at the meeting. Each member of the group should declare any interests which are relevant to the business of the meeting whether or not those interests have previously been declared. Any new interests which are declared at a meeting must be included on the CCG’s relevant register of interests to ensure it is up- to-date.
73 of 114
Reporting 48. The CCG will ensure a person shall act as Secretary to the Committee and will:
a. Circulate the minutes and actions to all members of the Committee within 7 working days of any meeting of the Committee;
b. Report the proceedings of each meeting of the Committee to the next Governing Body;
c. Produce an executive summary report which sets out any decisions made by the Committee to be presented at the next meeting of the Governing Body;
d. The Chair shall draw to the attention of the Governing Body any issues that require disclosure to the full Governing Body or require executive action.
[Signature provisions]
Signatures will be applied upon delegation
Schedule 1 – Delegation (will be included on submission to NHS England)
74 of 114
CCG Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson
CHAIR’S ACTION
The NHS Lewisham Clinical Commissioning Group’s Constitution states: it is recognised that there will be times when urgent decisions are required. The Chair has the discretion to define urgent decisions. To ensure transparency, any urgent decisions will be recorded and notified in the minutes of the next meeting in public of the CCG Governing Body. Title: Approval of the Terms of Reference for the Primary Care Commissioning Committee Recommendation proposed: The recommendation is to approve the Terms of Reference for the Primary Care Commissioning Committee further to clarification from NHS England with regards to what is being delegated to the CCG and some minor amendments to the Terms of Reference. Rationale for Chair’s action: At the Governing Body meeting on 09 March 2017, the Terms of Reference for the Primary Care Commissioning Committee were submitted for approval. Minor amendments to the Terms of Reference were requested at the meeting. However, the Governing Body were not willing to approve the Terms of Reference as concerns were expressed with regards to clarity for what delegated functions the CCG would be taking on.
Subsequently, advice has been sought from NHS England National Team. The response to the question posed was:
• Decisions in relation to the commissioning, procurement and management of Primary Medical Services Contracts, including but not limited to the following activities:
o decisions in relation to Enhanced Services; o decisions in relation to Local Incentive Schemes (including the design of
such schemes); o decisions in relation to the establishment of new GP practices (including
branch surgeries) and closure of GP practices; o decisions about ‘discretionary’ payments; o decisions about commissioning urgent care (including home visits as
required) for out of area registered patients; • The approval of practice mergers; • Planning primary medical care services in the Area, including carrying out needs
assessments; • Undertaking reviews of primary medical care services in the Area; • Decisions in relation to the management of poorly performing GP practices and
including, without limitation, decisions and liaison with the CQC where the CQC has reported non-compliance with standards (but excluding any decisions in relation to the performers list);
• Management of the Delegated Funds in the Area; • Premises Costs Directions Functions; • Co-ordinating a common approach to the commissioning of primary care services
with other commissioners in the Area where appropriate; and
75 of 114

CCG Chair: Dr Marc Rowland Chief Officer: Martin Wilkinson
• Such other ancillary activities that are necessary in order to exercise the Delegated Functions. Further action required: None. Approving Lay Member: Ray Warburton I, Marc Rowland(Chair), support and agree the action: Signature: Date: 19.04.17 I, Martin Wilkinson (Chief Officer), support and agree the action: Signature: Date: 06.04.17 Date of Governing Body meeting:
76 of 114

1
Memorandum of Understanding between South East London Clinical Commissioning Groups for primary care commissioning arrangements from 1st April 2017
1. Introduction to the MOU
This Memorandum of Understanding (MOU) sets out how the Clinical Commissioning Groups (CCGs) in South East London will work together to support the successful implementation of new primary care commissioning arrangements. It confirms mutual commitments and responsibilities.
NHS Southwark CCG (the “lead CCG”) will host NHS England primary care commissioning staff on behalf of the other CCGs in South East London.
The agreement is intended to cover the period between 1 April 2017 and 31 March 2019. The agreement may be varied or terminated by mutual agreement between the six parties, following a minimum of six months’ notice.
NHS England (London) NHSE(L) has, since April 2013, organised its primary care commissioning capability around Strategic Planning Group footprints, which have now been superseded by Sustainability and Transformation Plan (STP) footprints. The STP Footprint London wide model is proposing a broadly consistent way of executing delivery both in terms of monitoring quality and undertaking quality improvement initiatives. It also establishes better reporting of the assurance responsibilities (which cover contract and performance monitoring) of NHSE(L). NHSE(L) staff will be geographically assigned (locally known as ‘embedded’) into South East London.
This MoU should be read alongside two documents (Appendices 1 and 2): Appendix 1 - the Delegation Agreement between the CCGs in South East London, which sets out governance arrangements Appendix 2 - the Memorandum of Understanding between the employer, NHSE(L), and the lead CCG, Southwark CCG. The MOU includes:
• Which areas of primary care commissioning are delegated to CCGs and which are
retained at a London level • The responsibilities of the STP areas and of NHS England • The size of the NHS England team which will be transferred across
2. Key objectives of the MOU
The key objectives of this MOU are to: • Set out the common purpose between Southwark CCG who will host NHS England
primary care commissioning staff on behalf of the other CCGs in South East London • Set out the duration of the relationship • Describe the key principles between the lead CCG, Southwark, and the other CCGs
in South East London • Set out the relationship between the parties • Set out the roles and expectations of the lead CCG and the other CCGs in South
East London • Outline the funding arrangements • Outline how disputes and failures to perform shall be addressed
77 of 114
2
3. Common Purpose The common purpose between Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs is to enable successful implementation of new primary care commissioning arrangements in South East London. This will facilitate better decisions around commissioning of services and the transaction of those decisions, enabling an holistic approach to patient care delivery, with services being commissioned to support the local needs of patients residing in each CCG. A total of 15 staff from NHSE(L) will move into the STP footprint of South East London and deliver the delegated functions in alignment with the six CCGs. This approach: • Supports place-based commissioning • Allows a balance of perspectives and demands between CCGs and NHSE(L) to
focus on delegated functions • Encourages flexibility, alignment and joint learning • Enables the development of closer and more integrated working • Allows improved collaboration across functions • Provides skills development across functions • Promotes better understanding and achievement of STP plans • Reduces bureaucracy through direct contact between CCGs and NHSE(L) NHSE(L) staff assigned to South East London CCGs will be based at Skipton House in Elephant and Castle.
4. Key Principles
Primary care commissioning: NHS England is responsible for the direct commissioning of services outside the remit of clinical commissioning groups, namely retained medical primary care functions (as set out in Schedule 3 of the 2017/18 Delegation Agreement), non-medical primary care, public health, offender health, military and veteran health and specialised services.
Geographically Assigned Organisational Model: Employment contracts for NHSE(L) employees and CCG employees will not change and mixed management and delivery teams will be utilised as appropriate. Employees will be on different terms and conditions, depending on their respective employers. Formal processes will be managed by the employing organisation, whilst day to day reporting of staff and operational line management will be the responsibility of the lead CCG. This has been noted in Schedule 7 of Delegation Agreements.
Assigned Team: The NHSE(L) team will be hosted for day to day purposes within South East London and deliver the delegated functions in alignment with the CCGs. This will avoid duplication of work and enable effective use of Primary Care commissioning staff, which is recognised as a constrained resource.
5. Relationship between parties The lead CCG commits to: • Ensuring there is appropriate and equitable resource and management capacity for
each CCG South East London CCGs recognise the importance of making a success of the new primary care commissioning arrangements. They therefore commit to:
78 of 114
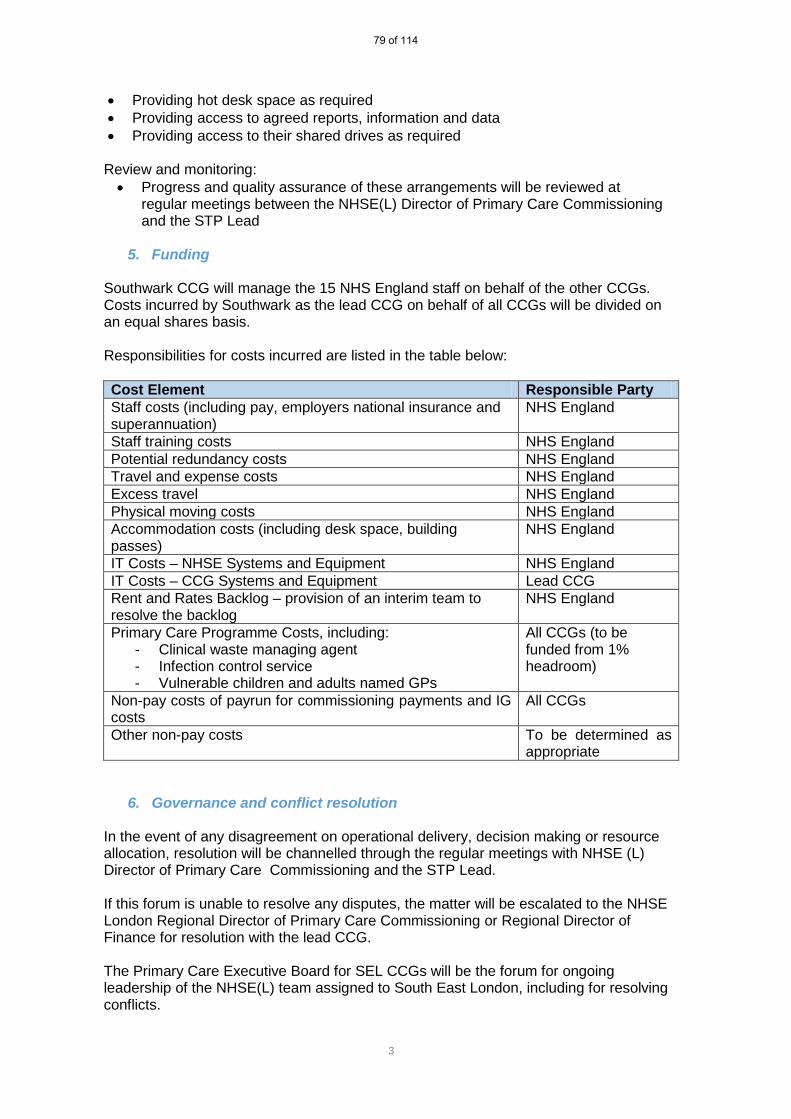
3
• Providing hot desk space as required • Providing access to agreed reports, information and data • Providing access to their shared drives as required
Review and monitoring: • Progress and quality assurance of these arrangements will be reviewed at
regular meetings between the NHSE(L) Director of Primary Care Commissioning and the STP Lead
5. Funding
Southwark CCG will manage the 15 NHS England staff on behalf of the other CCGs. Costs incurred by Southwark as the lead CCG on behalf of all CCGs will be divided on an equal shares basis. Responsibilities for costs incurred are listed in the table below: Cost Element Responsible Party Staff costs (including pay, employers national insurance and superannuation)
NHS England
Staff training costs NHS England Potential redundancy costs NHS England Travel and expense costs NHS England Excess travel NHS England Physical moving costs NHS England Accommodation costs (including desk space, building passes)
NHS England
IT Costs – NHSE Systems and Equipment NHS England IT Costs – CCG Systems and Equipment Lead CCG Rent and Rates Backlog – provision of an interim team to resolve the backlog
NHS England
Primary Care Programme Costs, including: - Clinical waste managing agent - Infection control service - Vulnerable children and adults named GPs
All CCGs (to be funded from 1% headroom)
Non-pay costs of payrun for commissioning payments and IG costs
All CCGs
Other non-pay costs To be determined as appropriate
6. Governance and conflict resolution In the event of any disagreement on operational delivery, decision making or resource allocation, resolution will be channelled through the regular meetings with NHSE (L) Director of Primary Care Commissioning and the STP Lead. If this forum is unable to resolve any disputes, the matter will be escalated to the NHSE London Regional Director of Primary Care Commissioning or Regional Director of Finance for resolution with the lead CCG.
The Primary Care Executive Board for SEL CCGs will be the forum for ongoing leadership of the NHSE(L) team assigned to South East London, including for resolving conflicts.
79 of 114
4
If a conflict between CCGs cannot be resolved within the Primary Care Executive Board, the dispute will be escalated and resolved by the Chief Officers of the relevant CCGs.
Signed: Chief Officer, CCG 12 April 2017
80 of 114

1 | P a g e P C C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 4 Personal Medical Services (PMS) contract review
MANAGERIAL LEAD: Ashley O’Shaughnessy, Deputy Director Primary Care
AUTHOR: Ian Ross, Associate Director Primary Care
RECOMMENDATIONS: The Primary Care Commissioning Committee (PCCC) is asked to agree that, following the conclusion of negotiations with the local LMC, an extraordinary meeting of the PCCC be convened to consider an urgent planned decision regarding the approval of the NHS England (London) PMS review assurance template. This template will include details of the agreed PMS Commissioning Intentions and final offer to practices. It is expected that this meeting will take place in early May 2017. SUMMARY: Further to the PMS contract review update paper and supporting PMS Commissioning Intentions for Lewisham that were approved by the Lewisham Primary Care Joint Committee on the 11th February 2017 (http://www.lewishamccg.nhs.uk/about-us/how-we-work/PCJC%20docs/SEL%20PCJC%20Meeting%2011%20Feb%202016_Enc%20J%20PMS%20CIs2.pdf), discussions are still ongoing regarding the implementation of the PMS contract review in Lewisham. Further to negotiations at a London level between NHSE and the Londonwide LMC, the review was paused across London in April 2016. The pause was lifted in November 2016, with negotiations to be undertaken locally by CCGs, in partnership with NHS England (London) and local LMCs. Before the pause, a ‘London Offer’ had been proposed for all practices, with some mandatory KPIs in addition to a local component. Post pause, the London Offer was no longer mandatory, with each CCG able to agree local use of PMS Premium funding. For the past few months, the CCG has been engaging with the local LMC, with support from NHSE, in negotiating the detailed KPIS and specifications underpinning the locally agreed Commissioning Intentions. At time of writing, these negotiations are still ongoing. The CCG is required to submit a PMS review assurance template to NHS England (London) which will include details of the agreed PMS Commissioning Intentions and final offer to practices – this is expected to be submitted by the end of April 2017/early May 2017, hence the need for an urgent planned decision.
81 of 114
2 | P a g e P C C A P R 2 0 1 7
KEY ISSUES: • The PMS review process was paused across London between April 2016 and November 2016.
• Negotiations are now to be lead at a local level and there is no mandatory ‘London offer’.
• NHS Lewisham CCG is still in negotiation with the local LMC.
• It is planned for the revised PMS contracts to go live on the 1st October 2017.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Contract Management: To manage effectively the CCG’s contract portfolio to ensure that the
CCG’s Operating Plan‘s commitments are met in 2017/18. This includes ensuring our financial targets are met and value for money is achieved.
CONFLICT OF INTEREST (CoI): It is recognised that Clinical Directors in their role as General Practitioners have a direct CoI as this item relates to GP practice contracts. Therefore, in order to mitigate potential CoI and/or any undue influence; 1. This paper includes no financial information on the proposed PMS contract 2. This paper includes no specific detail on the proposed KPIs or service specifications associated
with the PMS contract
CONSULTATION HISTORY: • Primary Care Joint Committee • Primary Care Programme Board • Membership Forum / Neighbourhood meetings • Local LMC/Londonwide LMC • NHS England • Lewisham council / Lewisham Public Health
PUBLIC ENGAGEMENT: PMS commissioning Intentions discussed at neighbourhood PPG meetings in March 2016
HEALTH INEQUALITY DUTY & PUBLIC SECTOR EQUALITY DUTY: Ensuring that all service redesign complies with CCG policies and the commissioning cycle will ensure that any service that is ultimately commissioned will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD CONTACT: Name: Ashley O’Shaughnessy; Email: [email protected]
AUTHOR CONTACT: Name: Ian Ross ; Email: [email protected]
82 of 114
3 | P a g e P C C A P R 2 0 1 7
83 of 114
1 | P a g e P C C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 5 Supporting Practice Engagement in Clinical Commissioning: Local Improvement Scheme for 2017/18 MANAGERIAL LEAD: Charles Malcolm-Smith, Deputy Director (Strategy & Organisational Development
AUTHOR: Ashley O’Shaughnessy, Deputy Director Primary Care
RECOMMENDATIONS: The Primary Care Commissioning Committee are asked to approve;
1. The Supporting Practice Engagement in Clinical Commissioning Local Improvement Scheme for 2017/18.
2. The recommendation that a full review of the Scheme is conducted by September 2017 to support decisions on Membership Engagement (GP practices) in Clinical Commissioning.
SUMMARY: The purpose of this 2017/18 Local Improvement Scheme is to support Lewisham GP Practices and their neighbourhoods to actively engage in high quality, cost effective clinically-led commissioning and service redesign by financially compensating Practices for the input required to achieve measurable, quality and cost effective engagement.
Continuing the success of previous years, this year’s Local Improvement Scheme is again specifically seeking to support collaborative working and engagement between practices within neighbourhoods and also collectively across the borough.
KEY ISSUES:
• The Local Improvement Scheme specification is enclosed which details the requirements, funding and reporting arrangements.
• The value of this Local Improvement Scheme is aligned to previous years with overall funding part of an already agreed membership engagement budget.
• It is recommended that the Local Improvement Scheme is reviewed by September 2017 to inform arrangements for 2018/19 – with regard to how best to support Practice Engagement in Clinical Commissioning.
CORPORATE AND STRATEGIC OBJECTIVES: Contract Management: To manage effectively the CCG’s contract portfolio to ensure that the CCG’s Operating Plan‘s commitments are met in 2017/18. This includes ensuring our financial targets are met and value for money is achieved.
CONFLICT OF INTEREST (CoI): The Primary Care Commissioning Committee is asked to approve the Supporting Practice Engagement in Clinical Commissioning Local Improvement Scheme 2017/18. However, it is
84 of 114
2 | P a g e P C C C A P R 2 0 1 7
recognised that Clinical Directors in their role as General Practitioners will financially benefit from the Local Improvement Scheme. Therefore, in order to mitigate perceived/potential CoI and/or any undue influence;
1. The Local Improvement Scheme builds on previous years arrangements with only minor amendments the requirements
2. The Local Improvement Scheme has been reviewed against an adapted NHSE Local Improvement Scheme assessment template that has previously been used under joint commissioning arrangements (attached);
3. In regard to Requirement 2, “The design/redesign of locally commissioned services”, the following wording has been included in the Local Improvement Scheme;
“Neighbourhoods, and their constituent practices, when developing their plans must do so in their capacity as commissioners and not providers so as to manage any perceived or real conflict of interest.”
CONSULTATION HISTORY:
• The scheme builds on Engagement Local Improvement Schemes from previous years • The Local Improvement Scheme was discussed at the Membership Forum held in March 2017 • The Local Medical Committee have endorsed the Local Improvement Scheme
PUBLIC ENGAGEMENT: N/A
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: Overall the Local Improvement Scheme will support the involvement of clinicians to ensure that their insight and understanding of the needs of their patients are reflected in commissioning decisions, such as where there are existing health inequalities.
Requirement 2 in particular will support the improvement of commissioned services to meet the specific health needs and experience of local populations in Lewisham at a neighbourhood level.
RESPONSIBLE MANAGERIAL LEAD CONTACT: Name: Charles Malcolm-Smith; E-mail: [email protected]
AUTHOR CONTACT: Name: Ashley O’Shaughnessy; E-mail: [email protected]
85 of 114
1 | E n g a g e m e n t L I S 1 7 / 1 8
Version 1.0 Local Improvement Scheme (LIS) 2017/18 Supporting Practice Engagement in Clinical Commissioning 1. Purpose: The purpose of this 2017/18 Local Improvement Scheme (LIS) is to support Lewisham GP Practices and their neighbourhoods to actively engage in high quality, cost effective clinically-led commissioning and service redesign by financially compensating Practices for the input required to achieve measurable, quality and cost effective engagement. Continuing the success of previous years, this year’s LIS is again specifically seeking to support collaborative working and engagement between practices within neighbourhoods and also collectively across the borough. 2. Background: This LIS will support the clinical leadership of the NHS in Lewisham working in partnership with the Lewisham Clinical Commissioning Group (LCCG). To be successful, the Clinical Commissioning Group will need to work with constituent Practices via neighbourhoods, including other key partners such as London Borough of Lewisham (and service providers) to make clinical commissioning work and deliver improved outcomes for local people. Funding will be made available to each Practice to support engagement in clinical commissioning. Learning from previous LISs have been used in constructing this LIS. 3. Eligibility Criteria: All NHS GP practices within Lewisham Clinical Commissioning Group. 4. Duration: The LIS covers the 12 month period 1st April 2017 to 31st March 2018. 5. Requirements: The LIS sets out the requirements which must be met in Sections A (engagement requirements) and B (commissioning requirements).
86 of 114
2 | E n g a g e m e n t L I S 1 7 / 1 8
6. REQUIREMENTS:
SECTION A Requirement 1: Engagement with LCCG activities through attendance at neighbourhood commissioning meetings and membership events, validation of practice staff contact details and completion of quarterly membership surveys. a) Over the period 1st April 2017 – 31st March 2018, Practices are required to have GP
representation at a minimum of 8 neighbourhood commissioning meetings • Additional Practice members (GPs, Practice managers, nurses) can attend meetings,
but no additional funding will be available
• Neighbourhood commissioning meetings will be a minimum of 2 hours in duration
• Practice representatives at neighbourhood commissioning meetings will be required to provide effective and regular intra-practice communication of clinical commissioning matters with both clinical and non-clinical members of the practice team
b) Practices are required to have GP representation at the two scheduled CCG membership events over the course of the year. Any additional qualifying events will be agreed through the Membership Forum. • Additional Practice members (GPs, Practice managers, nurses, administrative staff)
can attend these membership events and are encouraged to do so – this will be supported through the provision of SELDOC cover for all events
c) Practices are required to validate a staff contact list on a quarterly basis to support
effective communications between the CCG and its members
d) Practices are to respond to a minimum of four CCG membership surveys which will be shared electronically. A minimum of one response is to be returned by each practice for each survey
87 of 114

3 | E n g a g e m e n t L I S 1 7 / 1 8
SECTION B Requirement 2: The design/redesign of locally commissioned services This requirement is seeking to engage practices working within their neighbourhoods in the design/redesign of locally commissioned services. The aim is to promote real engagement with the CCG at a practice and neighbourhood level and demonstrate the impact and influence that CCG members can exert over service design/redesign and also ensure the delivery of “true clinical commissioning” by the CCG. Practices must work collaboratively in their neighbourhoods to achieve this indicator and submit their ideas as a neighbourhood and/or borough. Evidence of intra practice engagement/discussions will need to be demonstrated. Proposed timetable: Time Period
16/17 Action
Q2 Confirm service design/redesign area and whether plans will be developed by the neighbourhood itself or jointly with other neighbourhoods
Q3 To have drafted service design/redesign documentation (template to be available and distributed by the CCG)
Q4 To share proposals with partners (including patients) and update plans in light of feedback
Neighbourhoods, and their constituent practices, when developing their plans must do so in their capacity as commissioners and not providers so as to manage any perceived or real conflict of interest. 7. Funding: The total available for each Practice is £3,600. Section A – Total available funding per practice is £1800. For a practice to receive the full £1800 they will have to achieve ALL the requirements in Section A. Partial achievement does not earn any funding. Section B - Total available funding per practice is £1800. For a practice to receive the full £1800 they will have to achieve ALL the requirements in Section B. Partial achievement does not earn any funding. The payment for Section A (Requirement 1) will be made in November 2017 (with the expectation that all items within that requirement will be achieved). This payment will be reclaimed in full for non-delivery of any of the necessary requirements. The remaining payment for Section B (Requirement 2) will be payable in March 2018.
88 of 114

4 | E n g a g e m e n t L I S 1 7 / 1 8
8. Reporting: Section A - Requirement 1 • Practice attendance record at Neighbourhood meetings (CCG to collate and validate). • Practice attendance record at membership events (CCG to collate and validate). • Quarterly return of validated practice staff contact list • Return of membership surveys (minimum of 1 per practice per questionnaire) • One set of practice meeting minutes for 2017/18 documenting intra-practice
communication of clinical commissioning matters discussed at a neighbourhood commissioning meeting
Section B – Requirement 2 • Submission of service design/redesign documentation • Demonstration of intra practice engagement
9. Support offered to the Practices: GP Practices will be supported through the work of Neighbourhoods, Neighbourhood leads and the CCG in addition to information made available through GP Interactive (http://www.gpinteractivelewisham.nhs.uk/). 10. Participation: Practices are required to formally sign up to the LIS to confirm their commitment to active participation under this scheme and fulfil the detailed requirements. Practices should sign up to the LIS via a confirmation email to [email protected] by Friday 19th May 2017 which will be taken as acceptance of the requirements and reporting arrangements as detailed in this LIS.
89 of 114
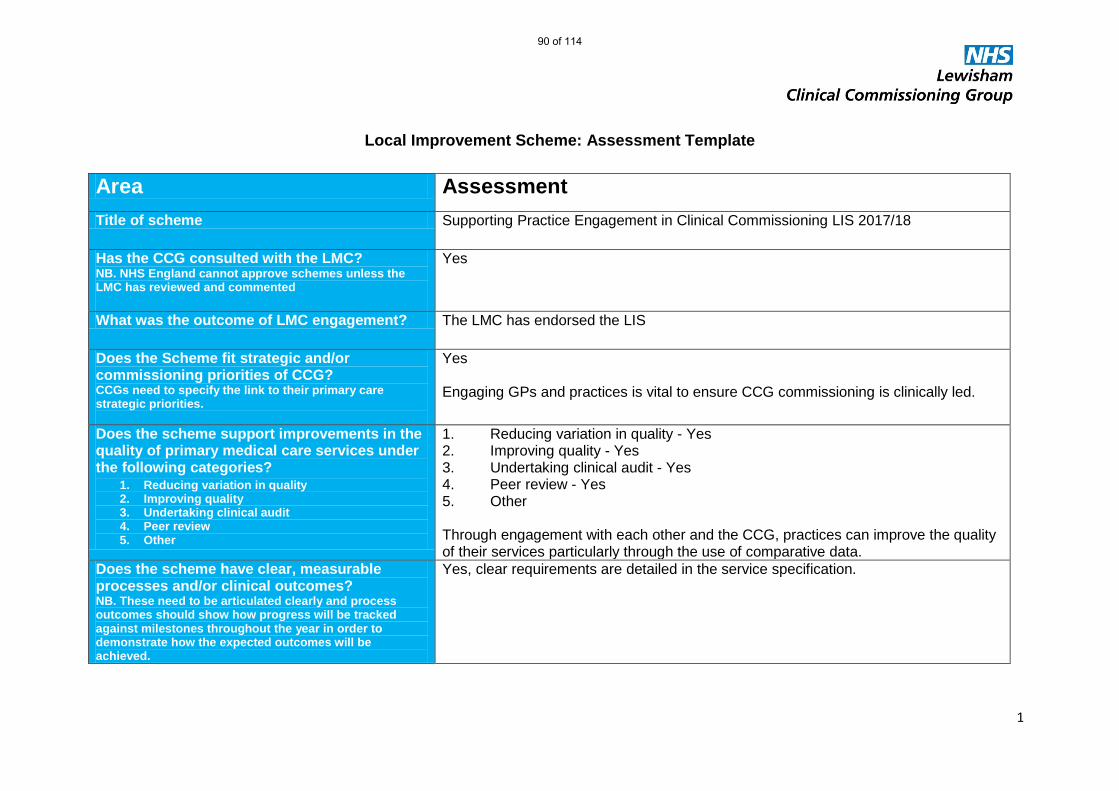
1
Local Improvement Scheme: Assessment Template
Area Assessment Title of scheme Supporting Practice Engagement in Clinical Commissioning LIS 2017/18
Has the CCG consulted with the LMC? NB. NHS England cannot approve schemes unless the LMC has reviewed and commented
Yes
What was the outcome of LMC engagement? The LMC has endorsed the LIS
Does the Scheme fit strategic and/or commissioning priorities of CCG? CCGs need to specify the link to their primary care strategic priorities.
Yes Engaging GPs and practices is vital to ensure CCG commissioning is clinically led.
Does the scheme support improvements in the quality of primary medical care services under the following categories?
1. Reducing variation in quality 2. Improving quality 3. Undertaking clinical audit 4. Peer review 5. Other
1. Reducing variation in quality - Yes 2. Improving quality - Yes 3. Undertaking clinical audit - Yes 4. Peer review - Yes 5. Other Through engagement with each other and the CCG, practices can improve the quality of their services particularly through the use of comparative data.
Does the scheme have clear, measurable processes and/or clinical outcomes? NB. These need to be articulated clearly and process outcomes should show how progress will be tracked against milestones throughout the year in order to demonstrate how the expected outcomes will be achieved.
Yes, clear requirements are detailed in the service specification.
90 of 114

2
Is the scheme rewarding outcomes? NB. NHS England cannot approve schemes that do not reward outcomes.
Yes, clear requirements are detailed in the service specification.
Is there any overlap with what is paid for under the Primary Medical Care Contract, DES, QOF? NB NHS England cannot approve duplicate payments but there will be situations where a LIS scheme is paying for work in excess of existing arrangements
No
What are the proposed Contractual arrangements? e.g. SLA, Letters of Intent, National Contract (not mandated)
Signed letter of intent
What is the total financial value of the scheme? £144,000 - £3600 x 40 practices What is the payment structure? NB. It is expected that there will be a payment that is only realised on achievement of key deliverables. i.e. not all of the payment will be made ‘up front’
50% (£1,800) of this payment will be made in Nov 2017 against the engagement activities listed under Requirement 1. The remaining 50% (£1800) will be paid in March 2018 against the delivery of Requirement 2.
What are the arrangements if outcomes are not achieved? e.g. Clawbacks or no achievement payment released
Practices will not receive payments for non-delivery of Requirement 2. A claw back clause has been included in the specification for non delivery of Requirement 1 as this is associated with an interim payment based on expected delivery.
Is participation in the scheme optional or mandatory for CCG member practices? If other scenarios apply, please specify
Optional, but it is anticipated that all practices will partake as in previous years.
Assessment undertaken by: Ashley O’Shaughnessy – Deputy Director Primary Care
Date: 18th April 2017
91 of 114
1 | P a g e P C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 6(a) Clifton Rise Family Practice G85026 Lewisham CCG Review of Need for Contractual Action Following Inspection by the CQC CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director, Primary Care Lead MANAGERIALLEAD: Jill Webb, Head of Primary Care and Diana Braithwaite, Director of Commissioning & Primary Care
AUTHOR: Debbie Power, Senior Commissioning Manager
RECOMMENDATIONS: The members of the Primary Care Commissioning Committee are asked to; 1. Approve that the contractor be formally required to provide assurance that all actions necessary to
achieve CQC compliance have been completed and to submit evidence, as may be required by NHS England.
2. Endorse the proposal to offer any necessary support to the practice in continuing to meet their required CQC and contractual obligations.
SUMMARY: The Care Quality Commission (CQC) carried out a comprehensive inspection of Clifton Rise Family Practice on 20 April 2016. The report was published on 16th November 2016 and is available at: http://www.cqc.org.uk/location/1-569709197
The practice was rated as ‘Requires Improvement’ in the following areas: - ‘Are services safe?’ - ‘Are services well-led?’ It was rated ‘Good’ for: - Are services effective?’ - ‘Are services caring?’ - ‘Are services responsive to people’s needs?’
The practice received an overall rating of ‘Requires improvement’ for the quality of care provided by the practice.
The Primary Care Joint Committee previously approved the London region Standard Operating Procedure for Primary Medical contracts: A consistent approach to responding to Care Quality Commission ‘Requires Improvement’ ratings. The considerations within this have been used to determine what formal contractual actions, if any, may be recommended to the PCJC, as a result of Clifton Rise Family Practice receiving a Requires Improvement notice.
The considerations have included: 1. Should contractual action be considered?
When a practice is in receipt of a CQC report indicating that they ‘Require Improvement’, they have immediately breached their contract. ‘The Contractor shall comply with all relevant legislation and have regard to all relevant guidance issued by the Board or the Secretary of State
92 of 114
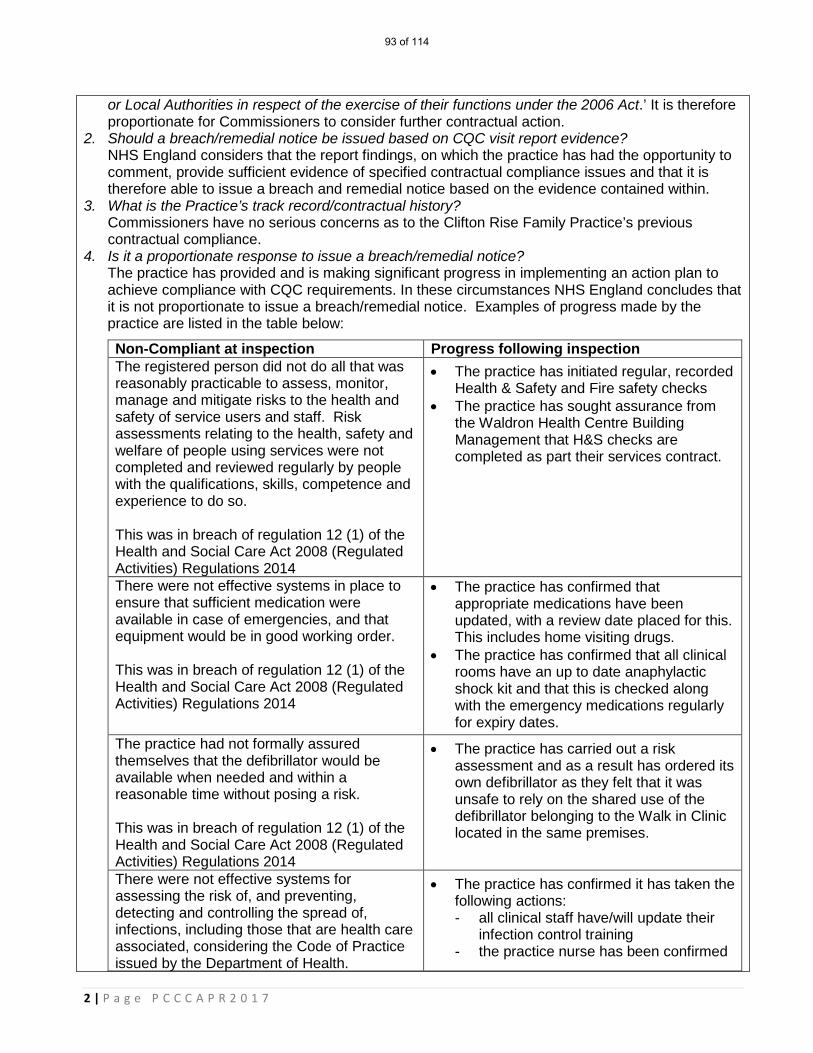
2 | P a g e P C C C A P R 2 0 1 7
or Local Authorities in respect of the exercise of their functions under the 2006 Act.’ It is therefore proportionate for Commissioners to consider further contractual action.
2. Should a breach/remedial notice be issued based on CQC visit report evidence? NHS England considers that the report findings, on which the practice has had the opportunity to comment, provide sufficient evidence of specified contractual compliance issues and that it is therefore able to issue a breach and remedial notice based on the evidence contained within.
3. What is the Practice’s track record/contractual history? Commissioners have no serious concerns as to the Clifton Rise Family Practice’s previous contractual compliance.
4. Is it a proportionate response to issue a breach/remedial notice? The practice has provided and is making significant progress in implementing an action plan to achieve compliance with CQC requirements. In these circumstances NHS England concludes that it is not proportionate to issue a breach/remedial notice. Examples of progress made by the practice are listed in the table below:
Non-Compliant at inspection Progress following inspection The registered person did not do all that was reasonably practicable to assess, monitor, manage and mitigate risks to the health and safety of service users and staff. Risk assessments relating to the health, safety and welfare of people using services were not completed and reviewed regularly by people with the qualifications, skills, competence and experience to do so. This was in breach of regulation 12 (1) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014
• The practice has initiated regular, recorded Health & Safety and Fire safety checks
• The practice has sought assurance from the Waldron Health Centre Building Management that H&S checks are completed as part their services contract.
There were not effective systems in place to ensure that sufficient medication were available in case of emergencies, and that equipment would be in good working order. This was in breach of regulation 12 (1) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014
• The practice has confirmed that appropriate medications have been updated, with a review date placed for this. This includes home visiting drugs.
• The practice has confirmed that all clinical rooms have an up to date anaphylactic shock kit and that this is checked along with the emergency medications regularly for expiry dates.
The practice had not formally assured themselves that the defibrillator would be available when needed and within a reasonable time without posing a risk. This was in breach of regulation 12 (1) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014
• The practice has carried out a risk assessment and as a result has ordered its own defibrillator as they felt that it was unsafe to rely on the shared use of the defibrillator belonging to the Walk in Clinic located in the same premises.
There were not effective systems for assessing the risk of, and preventing, detecting and controlling the spread of, infections, including those that are health care associated, considering the Code of Practice issued by the Department of Health.
• The practice has confirmed it has taken the following actions: - all clinical staff have/will update their
infection control training - the practice nurse has been confirmed
93 of 114
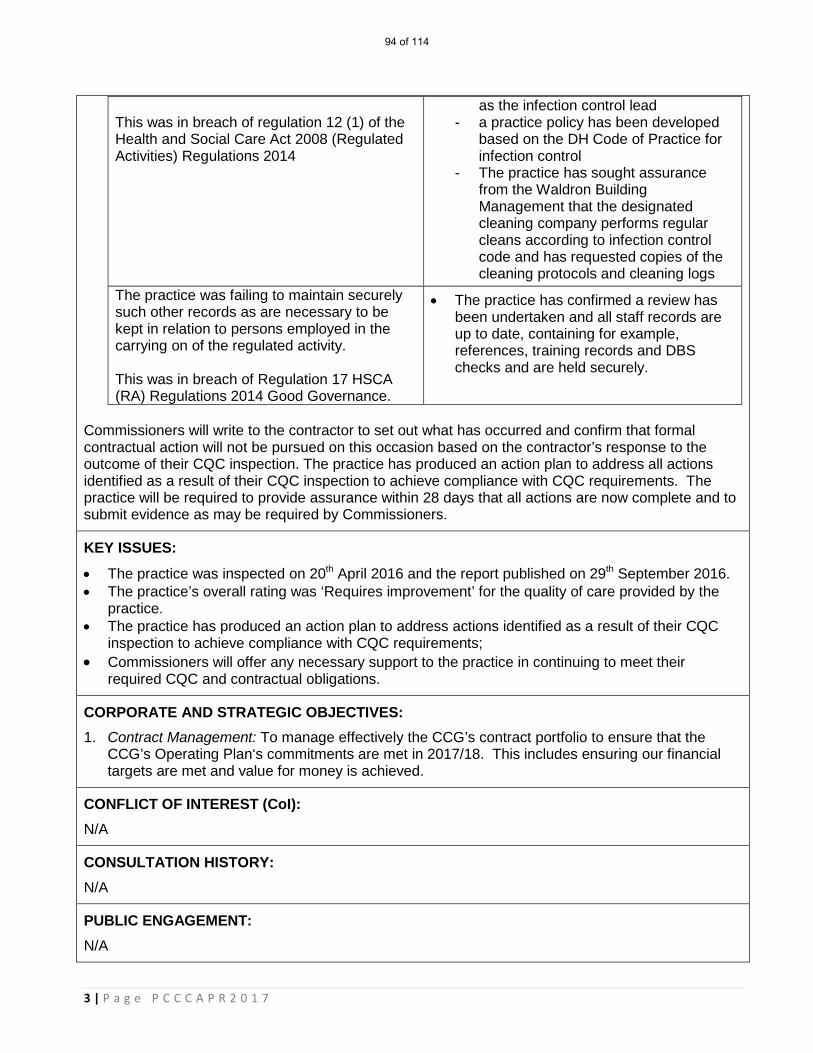
3 | P a g e P C C C A P R 2 0 1 7
This was in breach of regulation 12 (1) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014
as the infection control lead - a practice policy has been developed
based on the DH Code of Practice for infection control
- The practice has sought assurance from the Waldron Building Management that the designated cleaning company performs regular cleans according to infection control code and has requested copies of the cleaning protocols and cleaning logs
The practice was failing to maintain securely such other records as are necessary to be kept in relation to persons employed in the carrying on of the regulated activity. This was in breach of Regulation 17 HSCA (RA) Regulations 2014 Good Governance.
• The practice has confirmed a review has been undertaken and all staff records are up to date, containing for example, references, training records and DBS checks and are held securely.
Commissioners will write to the contractor to set out what has occurred and confirm that formal contractual action will not be pursued on this occasion based on the contractor’s response to the outcome of their CQC inspection. The practice has produced an action plan to address all actions identified as a result of their CQC inspection to achieve compliance with CQC requirements. The practice will be required to provide assurance within 28 days that all actions are now complete and to submit evidence as may be required by Commissioners.
KEY ISSUES:
• The practice was inspected on 20th April 2016 and the report published on 29th September 2016. • The practice’s overall rating was ‘Requires improvement’ for the quality of care provided by the
practice. • The practice has produced an action plan to address actions identified as a result of their CQC
inspection to achieve compliance with CQC requirements; • Commissioners will offer any necessary support to the practice in continuing to meet their
required CQC and contractual obligations.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Contract Management: To manage effectively the CCG’s contract portfolio to ensure that the
CCG’s Operating Plan‘s commitments are met in 2017/18. This includes ensuring our financial targets are met and value for money is achieved.
CONFLICT OF INTEREST (CoI): N/A
CONSULTATION HISTORY: N/A
PUBLIC ENGAGEMENT: N/A
94 of 114
4 | P a g e P C C C A P R 2 0 1 7
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: All commissioned services will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD/S CONTACT: Jill Webb, Head of Primary Care; E-Mail: [email protected]
95 of 114

1 | P a g e P C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 6(b) Sydenham Surgery G85081 Review of Need for Contractual Action Following Inspection by the CQC CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director, Primary Care Lead MANAGERIALLEAD: Jill Webb, Head of Primary Care and Diana Braithwaite, Director of Commissioning & Primary Care
AUTHOR: Debbie Power, Senior Commissioning Manager
RECOMMENDATIONS: The members of the Primary Care Commissioning Committee are asked to; 1. Approve that the contractor be formally required to provide assurance that all actions necessary to
achieve CQC compliance have been completed and to submit evidence, as may be required by NHS England.
2. Endorse the proposal to offer any necessary support to the practice in continuing to meet their required CQC and contractual obligations.
SUMMARY:
The Care Quality Commission (CQC) carried out a comprehensive inspection of Sydenham Surgery on 17th August 2016. The report was published on 28th October 2016 and is available at: http://www.cqc.org.uk/location/1-521446680 The practice was rated as ‘Requires Improvement’ in the following areas: - ‘Are services safe?’ - ‘Are services well-led?’ It was rated ‘Good’ for: - Are services effective?’ - ‘Are services caring?’ - ‘Are services responsive to people’s needs?’
The practice received an overall rating of ‘Requires improvement’ for the quality of care provided by the practice.
The Primary Care Joint Committee previously approved the London region Standard Operating Procedure for Primary Medical contracts: A consistent approach to responding to Care Quality Commission ‘Requires Improvement’ ratings. The considerations within this have been used to determine what formal contractual actions, if any, may be recommended to the PCJC, as a result Sydenham Surgery receiving a Requires Improvement notice.
The considerations have included: 1. Should contractual action be considered?
When a practice is in receipt of a CQC report indicating that they ‘Require Improvement’, they have immediately breached their contract. ‘The Contractor shall comply with all relevant
96 of 114
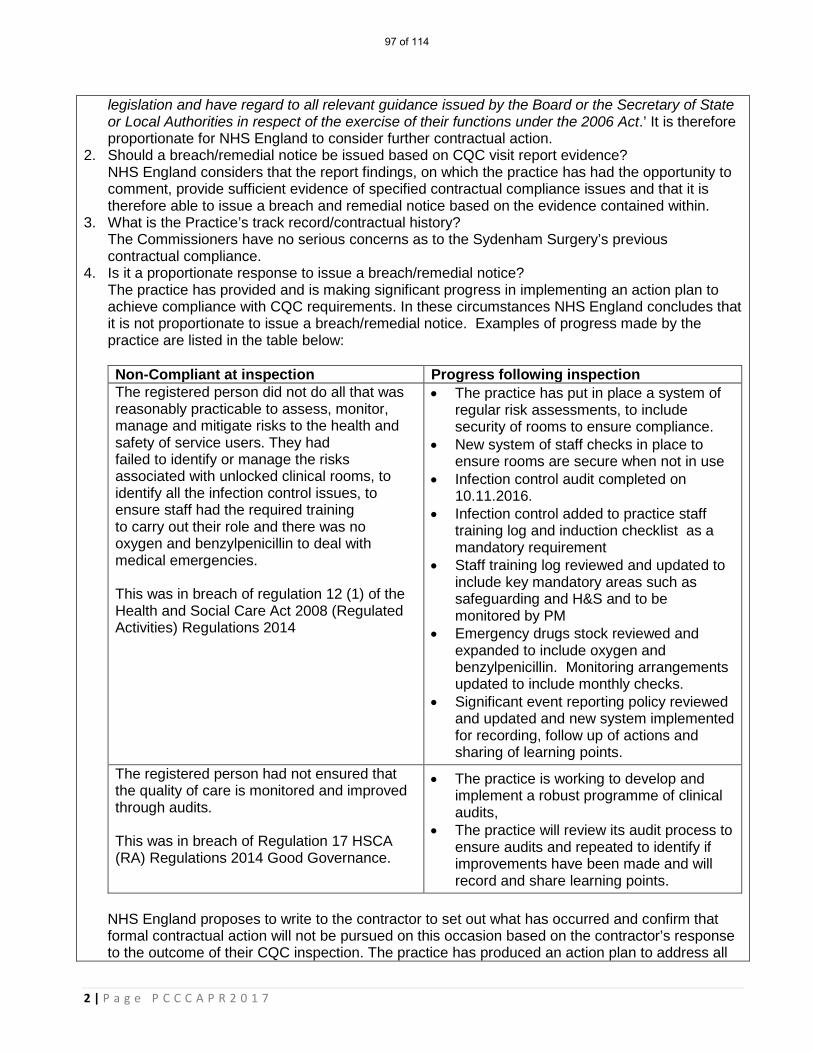
2 | P a g e P C C C A P R 2 0 1 7
legislation and have regard to all relevant guidance issued by the Board or the Secretary of State or Local Authorities in respect of the exercise of their functions under the 2006 Act.’ It is therefore proportionate for NHS England to consider further contractual action.
2. Should a breach/remedial notice be issued based on CQC visit report evidence? NHS England considers that the report findings, on which the practice has had the opportunity to comment, provide sufficient evidence of specified contractual compliance issues and that it is therefore able to issue a breach and remedial notice based on the evidence contained within.
3. What is the Practice’s track record/contractual history? The Commissioners have no serious concerns as to the Sydenham Surgery’s previous contractual compliance.
4. Is it a proportionate response to issue a breach/remedial notice? The practice has provided and is making significant progress in implementing an action plan to achieve compliance with CQC requirements. In these circumstances NHS England concludes that it is not proportionate to issue a breach/remedial notice. Examples of progress made by the practice are listed in the table below:
Non-Compliant at inspection Progress following inspection The registered person did not do all that was reasonably practicable to assess, monitor, manage and mitigate risks to the health and safety of service users. They had failed to identify or manage the risks associated with unlocked clinical rooms, to identify all the infection control issues, to ensure staff had the required training to carry out their role and there was no oxygen and benzylpenicillin to deal with medical emergencies. This was in breach of regulation 12 (1) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014
• The practice has put in place a system of regular risk assessments, to include security of rooms to ensure compliance.
• New system of staff checks in place to ensure rooms are secure when not in use
• Infection control audit completed on 10.11.2016.
• Infection control added to practice staff training log and induction checklist as a mandatory requirement
• Staff training log reviewed and updated to include key mandatory areas such as safeguarding and H&S and to be monitored by PM
• Emergency drugs stock reviewed and expanded to include oxygen and benzylpenicillin. Monitoring arrangements updated to include monthly checks.
• Significant event reporting policy reviewed and updated and new system implemented for recording, follow up of actions and sharing of learning points.
The registered person had not ensured that the quality of care is monitored and improved through audits. This was in breach of Regulation 17 HSCA (RA) Regulations 2014 Good Governance.
• The practice is working to develop and implement a robust programme of clinical audits,
• The practice will review its audit process to ensure audits and repeated to identify if improvements have been made and will record and share learning points.
NHS England proposes to write to the contractor to set out what has occurred and confirm that formal contractual action will not be pursued on this occasion based on the contractor’s response to the outcome of their CQC inspection. The practice has produced an action plan to address all
97 of 114
3 | P a g e P C C C A P R 2 0 1 7
actions identified as a result of their CQC inspection to achieve compliance with CQC requirements. The practice will be required to provide assurance within 28 days that all actions are now complete and to submit evidence as may be required by NHS England.
KEY ISSUES:
• The practice was inspected on 17th August 2016 and the report was published on 28th October 2016.
• The practice’s overall rating was ‘Requires improvement’ for the quality of care provided by the practice.
• The practice has produced an action plan to address actions identified as a result of their CQC inspection to achieve compliance with CQC requirements;
• Commissioners will offer any necessary support to the practice in continuing to meet their required CQC and contractual obligations.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Contract Management: To manage effectively the CCG’s contract portfolio to ensure that the
CCG’s Operating Plan‘s commitments are met in 2017/18. This includes ensuring our financial targets are met and value for money is achieved.
CONFLICT OF INTEREST (CoI): N/A
CONSULTATION HISTORY: N/A
PUBLIC ENGAGEMENT: N/A
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: All services commissioned will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD/S CONTACT: Jill Webb, Head of Primary Care; E-Mail: [email protected]
98 of 114

1 | P a g e P C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 6(c) Torridon Road Medical Practice G85032 Review of Need for Contractual Action Following Inspection by the CQC CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director, Primary Care Lead MANAGERIALLEAD: Jill Webb, Head of Primary Care and Diana Braithwaite, Director of Commissioning & Primary Care
AUTHOR: Debbie Power, Senior Commissioning Manager
RECOMMENDATIONS: The members of the Primary Care Commissioning Committee are asked to; 1. Approve that the contractor be formally required to provide assurance that all actions necessary to
achieve CQC compliance have been completed and to submit evidence, as may be required by NHS England.
2. Endorse the proposal to offer any necessary support to the practice in continuing to meet their required CQC and contractual obligations.
SUMMARY: The Care Quality Commission (CQC) carried out a comprehensive inspection of Torridon Road Surgery on 11 February 2016 and the practice received an overall rating of ‘Requires Improvement’ for the quality of care provided by the practice.
The practice was rated as ‘Requires Improvement’ in the following areas: - ‘Are services safe?’ - ‘Are services caring?’ - ‘Are services responsive to people’s needs?’ - ‘Are services well-led?’ It was rated ‘Good’ for: - ‘Are services effective?’
The CQC undertook a focussed follow up inspection on 8 November 2016 to check that the practice had followed their plan to meet all requirements. The practice received an overall rating of ‘Good’ but ‘Requires Improvement’ for caring services. The report was published on 6 January 2017 and both reports are available at: http://www.cqc.org.uk/location/1-559571507
The Primary Care Joint Committee previously approved the London region Standard Operating Procedure for Primary Medical contracts: A consistent approach to responding to Care Quality Commission ‘Requires Improvement’ ratings. The considerations within this have been used to determine what formal contractual actions, if any, may be recommended to the PCCC, as a result Torridon Road Surgery receiving a Requires Improvement notice.
The considerations have included: 1. Should contractual action be considered?
99 of 114
2 | P a g e P C C C A P R 2 0 1 7
When a practice is in receipt of a CQC report indicating that they ‘Require Improvement’, they have immediately breached their contract. ‘The Contractor shall comply with all relevant legislation and have regard to all relevant guidance issued by the Board or the Secretary of State or Local Authorities in respect of the exercise of their functions under the 2006 Act.’ It is therefore proportionate for NHS England to consider further contractual action.
2. Should a breach/remedial notice be issued based on CQC visit report evidence? NHS England considers that the comprehensive report findings, on which the practice has had the opportunity to comment, provide sufficient evidence of specified contractual compliance issues and that it is therefore able to issue a breach and remedial notice based on the evidence contained within.
3. What is the Practice’s track record/contractual history? The Commissioners have no serious concerns as to Torridon Road Surgery’s previous contractual compliance.
4. Is it a proportionate response to issue a breach/remedial notice? The practice has made significant progress in implementing an action plan to achieve compliance with CQC requirements. At the focussed follow up inspection visit carried out by the CQC on 8 November 2016 the practice was found to be ‘Good’ overall. In these circumstances NHS England concludes that it is not proportionate to issue a breach/remedial notice.
At the follow up visit the practice was found to be ‘requires improvement’ for caring services and it was identified by the CQC that the practice must make improvements as follows: The practice had received feedback from patients that they were not providing person centred care but had not taken sufficient action to address this. This was in breach of regulation 9 (1) (3)(a)(c)(d) of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014.
NHS England proposes to write to the contractor to set out what has occurred and confirm that formal contractual action will not be pursued on this occasion based on the contractor’s response to the outcome of their comprehensive CQC inspection and overall rating of ‘Good’ achieved at their subsequent focussed inspection. The practice will be required provide written assurance that they have completed all outstanding actions identified as a result of their follow up inspection on 8th November 2016 and to submit evidence, as may be required by NHS England.
KEY ISSUES:
• The practice received a comprehensive inspection on 11th February 2016 and was re-inspected on 8th November 2016. The second visit report was published on 6th January 2017;
• At the comprehensive inspection the practice’s overall rating was ‘Requires improvement’ for the quality of care provided by the practice;
• The practice has made significant progress in implementing an action plan to achieve compliance with CQC requirements;
• At the focussed follow up inspection the practice was found to be ‘Good’ overall but requires improvement for caring services;
• Commissioners will offer any necessary support to the practice in continuing to meet their required CQC and contractual obligations.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Contract Management: To manage effectively the CCG’s contract portfolio to ensure that the
CCG’s Operating Plan‘s commitments are met in 2017/18. This includes ensuring our financial targets are met and value for money is achieved.
CONFLICT OF INTEREST (CoI):
100 of 114
3 | P a g e P C C C A P R 2 0 1 7
N/A
CONSULTATION HISTORY: N/A
PUBLIC ENGAGEMENT: N/A
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: Commissioned services will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD/S CONTACT: Jill Webb, Head of Primary Care; E-Mail: [email protected]
101 of 114

1 | P a g e P C C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 7 Special Allocation Scheme (SAS): Violent Patients
CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director lead for Primary Care MANAGERIAL LEAD: Ian Ross, Associate Director – Primary Care Transformation
AUTHOR: Ian Ross, Associate Director – Primary Care Transformation
RECOMMENDATIONS: The Primary Care Commissioning Committee are asked to note;
1. That an interim Special Allocation Scheme, also known as the ‘Violent Patients’, service has been commissioned from Rushey Green Group Practice, under a directed enhanced service, initially for a 12 month period with a service start date of 1st April 2017.
SUMMARY: The purpose of a directed enhanced service for patients who have been subject to immediate removal from a practice’s patient list is to provide a stable environment for the patient to receive continuing health care, addressing any underlying causes of aggressive behaviour and providing a safe environment for the individuals involved in delivering that treatment. This is a nationally commissioned service and when a practice in Lewisham requests the immediate removal of a patient because of an act or threat of violence the police must be informed in accordance with relevant regulations and NHS Lewisham CCG should be notified.
NHS Lewisham CCG should ensure that these potentially violent patients know about the new arrangements and register with the provider of the directed enhanced service and that appropriate security facilities are available to protect the provider and other patients. Such provision could occur in general practices, in hospitals, in police stations or in other suitable secure locations. Consideration should be given to minimising the possibility of home visits by providing patient transport services with police or security support. Such support should also be available if any home visits are undertaken because of clinical necessity, after a full telephone assessment of the patient’s medical condition.
The directed enhanced service should provide for a thorough assessment of the patient’s clinical, psychological and social needs, especially those which may result in unrealistic expectations and which may have led to physically or verbally aggressive behaviour in the past.
The directed enhanced service should provide time to educate the patient and his or her family or carers on the best way to obtain good quality and continuing services from primary care in particular and the NHS in general. NHS Lewisham CCG input into this should be considered to demonstrate to the patient that it is NHS Lewisham CCG which has decided to include the patient in this particular pattern of care.
Patients will need to be clearly informed that they were having care provided within the directed enhanced service specifically because of their previous violent behaviour. It should be made clear to patients that they are not being excluded from receiving primary care medical services but that their behaviour compromises their right to have access to normal arrangements and locations for receiving
102 of 114
2 | P a g e P C C C A P R 2 0 1 7
those services.
The provision of care to a patient within a directed enhanced service for violent patients should be subject to a twelve-monthly review. This would be initiated by the provider and would give an opportunity to consider whether or not the patient should continue within the directed enhanced service. It would be supplemented by a more wide-ranging three-yearly review where NHS Lewisham CCG might seek more substantive justification for a continuance - for example, that the patient could not learn new behaviour because of an underlying personality disorder.
The service currently has 27 registered patients with approximately 7 active, i.e. frequent users of the service but this could of course change at any time.
The previous provider of this service, the New Cross HC, gave notice on their contract in January 2017. This service was openly offered out to all practices in Lewisham, on a number of occasions, with limited interest.
KEY ISSUES:
• NHS Lewisham CCG, under Level 3 commissioning, has the responsibility for ensuring that every person in the borough has access to primary care services and is able to register with a local GP practice.
• The cost of delivering this service is much more expensive than standard primary care access • However, if this patient group did not have access to primary care services they may access other
parts of the system, such as A&E, which could potentially introduce additional pressures and costs into the system plus patients would not be receiving their treatment at the appropriate setting.
• The long term vision for this service is that it may be commissioned under a single service specification across the 6 CCGs in South East London. These discussions are still evolving and will be bought to the PCCC when ready for consideration.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Planned Care: To support people with long term conditions better with proactive, holistic care
which improves the quality of their lives, is provided ‘out of hospital’ and reduces the requirement for hospital based outpatient attendances and inpatient admissions.
2. Urgent & Emergency Care: To commission Urgent Care and Emergency service which aligns the adult and children's physical and mental health services and addresses urgent care as early as possible ‘upstream’ – ‘right care, right time, right place’. This is the first phase of working towards commissioning an integrated Primary and Urgent care system.
CONFLICT OF INTEREST (CoI): N/A
CONSULTATION HISTORY: N/A
PUBLIC ENGAGEMENT: N/A
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: This service will enable all patients to have access to primary care from a GP – irrespective of the
103 of 114
3 | P a g e P C C C A P R 2 0 1 7
reasons for removal from a GPs register All commissioned services will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD CONTACT: Name: Ian Ross ; Email: [email protected]
AUTHOR CONTACT: Name: Ian Ross ; Email: [email protected]
104 of 114

1 | P a g e P C C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 8 GP Forward View – Implementation Update
CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director lead for Primary Care MANAGERIAL LEAD: Ashley O'Shaughnessy, Deputy Director Primary Care
AUTHOR: Ashley O'Shaughnessy, Deputy Director Primary Care
RECOMMENDATIONS: The Primary Care Commissioning Committee is asked to note the update on the implementation of the GP Forward View.
SUMMARY: NHS England set out its ambitions for the transformation of general practice services in the GP Forward View (GPFV), published in April 2016 (https://www.england.nhs.uk/wp-content/uploads/2016/04/gpfv.pdf) This paper provides a high level update on the local implementation of the GP FV in Lewisham and also indicates the value of funding that has been made available through the GP FV to Lewisham.
GP FV area Update Associated funding
Dedicated Implementation resource
Recruitment of joint post (two year fixed term) with Bromley CCG is now complete. In Lewisham, this resource will initially be supporting the implementation of extended access.
Joint 8b resource with Bromley CCG for 2 years
Practice resilience
A high level plan for the next three years has been developed jointly with One Health Lewisham Ltd (Gp Federation) and LMC to utilise the available funding.
Areas already delivered/being delivered:
• An all practice diagnostic (led by One Health Lewisham Ltd) to fully assess the level of local resilience support needed has been completed
• Immediate support for practices with high need (i.e. finance/business planning/interim resource) is in progress
£144k in 16/17, £44K in 17/18 and £44k 18/19
105 of 114

2 | P a g e P C C C A P R 2 0 1 7
• Practice working at scale workshop held in December 2016
• Support for GP Federation leadership to effectively deliver this programme in progress
Areas in development:
• Creation of a local GP Resilience Task Force
• Development of a local Locum Bank of GPs, Practice Nurses, HCAs and other practice support staff
• Further support for practices in relation to working at scale
Intention for 17/18 is to continue work commenced in 16/17, particularly practice level support as informed by the diagnostic exercise.
Admin and clerical training
Programme commissioned through Lewisham Community Education Provider Network (CEPN) for 16/17 to build capability and capacity in core management skills to increase practice efficiency.
Plans for 17/18 are under discussion with CEPN and Lewisham practice managers forum leads to complement other already planned training initiatives.
£27k available for 16/17. £55k available for 17/18 and £55k for 18/19.
Extended access (8-8, 7 days a week)
Standalone hub (8-8, 7 days per week) on Lewisham Hospital site went live as planned on 3rd April 2017 – service provided by One Health Lewisham Ltd.
Commercial in confidence as service has been subject to procurement
General practice development programme
EoI submitted for Time for Care programme to commence in 17/18 – initial meeting held on 24.2.17 with CCG, One Health Lewisham Ltd, LMC and NHSE. Programme consists of the following key elements:
• Time for Care learning in action programme –
using a collaborative approach to learning and improvement
• General Practice Improvement Leader programme – building capability for improvement leaders
• Quick Start modules taken from the Productive General Practice series – providing hands on support to practices.
Although direct funding is not available to support the Time for Care programme, specialist support and training is provided
106 of 114

3 | P a g e P C C C A P R 2 0 1 7
eConsultations – CCG currently assessing options for implementation in 17/18.
For eConsultations, £83k available for 17/18 and £111k for 18/19.
Estates Technology and Transformation Fund (ETTF)
Central Lewisham estates bid (£612k) and Population Health Management technology bid (£400k) have been successful and moved into the next phase. London wide ETTF bid to support an accelerated implementation of Patient Online Services in Q4 2016/17 successfully delivered in Lewisham (£50k).
As stated
Clinical Pharmacist in General Practice
One Health Lewisham Ltd have submitted a bid for this scheme (including strong links to LIMOS) which has been successful. The CCG are now working with One Health Lewisham Ltd to assess how the funding gap might be met and how the scheme will be implemented in practices.
60% funded in 1st
year 40% funded in 2
nd
year 20% funded in 3
rd
year
KEY ISSUES:
• None
CORPORATE AND STRATEGIC OBJECTIVES: 1. Planned Care: To support people with long term conditions better with proactive, holistic care
which improves the quality of their lives, is provided ‘out of hospital’ and reduces the requirement for hospital based outpatient attendances and inpatient admissions.
CONFLICT OF INTEREST (CoI): N/A
CONSULTATION HISTORY: N/A
PUBLIC ENGAGEMENT: N/A
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: All commissioned services will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD CONTACT: Name: Ashley O’Shaughnessy, [email protected]
AUTHOR CONTACT:
107 of 114
1 | P a g e P C C A P R 2 0 1 7
PCCC Primary Care Commissioning Committee Tuesday 25th April 2017
ENCLOSURE 9 Primary Care Developments
CLINICAL LEAD/S: Dr Jacky McLeod, Clinical Director, Primary Care Lead MANAGERIALLEAD: Diana Braithwaite, Director of Commissioning & Primary Care
AUTHOR: Sonia Ennals, Interim Estates Lead, Ian Ross, Associate Director – Primary Care Performance and Diana Braithwaite
RECOMMENDATIONS: 1. The members of the Primary Care Commissioning Committee are asked to note the update on
the following proposed changes to core primary care services, which will be subject to business cases and approval by the Committee;
a. The consolidation of the ICO Health Group primary care services in Grove Park and the intention to develop a new purpose built Health Centre.
b. The proposed relocation of New Cross Health Centre to the Waldron Health Centre. c. The early discussions that are underway concerning the potential merger between the
Winlaton Surgery and South Lewisham Group Practice.
SUMMARY: The purpose of this briefing is to provide the Primary Care Commissioning Committee with an overview of GP Practice mergers and developments, which strategically fits with local priorities as set out in the CCG’s Primary Care Strategy for General Practice, Our Healthier South East London – Community Based Care, Sustainability & Transformation Plan; delivering core general practice ‘at scale’. This is also supported nationally, as articulated in the General Practice Forward View, specifically with regard to the sustainability of General Practice.
The four core components of the CCGs commissioning approach for General Practice – as per the CCGs Refreshed Primary Care Strategy approved by the Governing Body in November 2016;
1. Supporting GP practices to work together and provide care and services at scale; 2. GP practices delivering primary care are an integral part of Neighbourhood Care Networks; 3. Shifting resources from secondary care to primary care to support care in the community; 4. Supporting outlier GP practices to reduce variation and the improve quality of services
provided.
The CCGs aim is to support development of the provider landscape to provide primary and community based care via appropriate population based services. The table below lists the providers and new models of care, which will be delivering services and the characteristics;
109 of 114
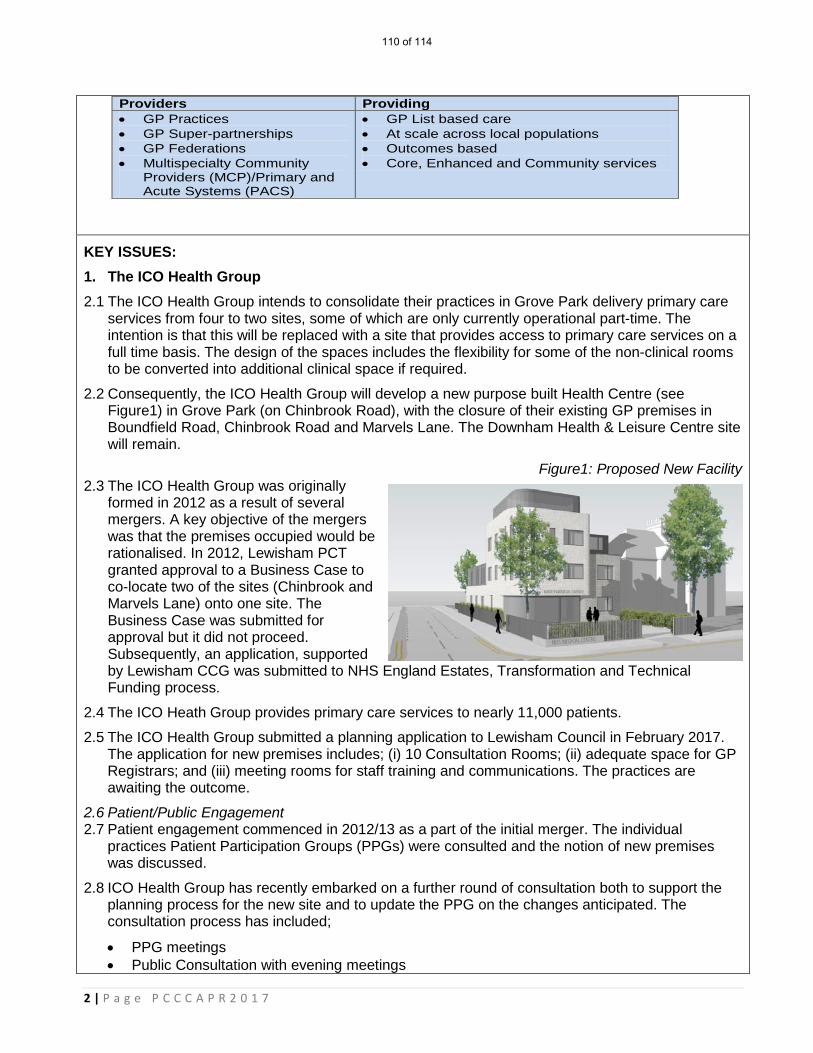
2 | P a g e P C C C A P R 2 0 1 7
KEY ISSUES: 1. The ICO Health Group 2.1 The ICO Health Group intends to consolidate their practices in Grove Park delivery primary care
services from four to two sites, some of which are only currently operational part-time. The intention is that this will be replaced with a site that provides access to primary care services on a full time basis. The design of the spaces includes the flexibility for some of the non-clinical rooms to be converted into additional clinical space if required.
2.2 Consequently, the ICO Health Group will develop a new purpose built Health Centre (see Figure1) in Grove Park (on Chinbrook Road), with the closure of their existing GP premises in Boundfield Road, Chinbrook Road and Marvels Lane. The Downham Health & Leisure Centre site will remain.
Figure1: Proposed New Facility 2.3 The ICO Health Group was originally
formed in 2012 as a result of several mergers. A key objective of the mergers was that the premises occupied would be rationalised. In 2012, Lewisham PCT granted approval to a Business Case to co-locate two of the sites (Chinbrook and Marvels Lane) onto one site. The Business Case was submitted for approval but it did not proceed. Subsequently, an application, supported by Lewisham CCG was submitted to NHS England Estates, Transformation and Technical Funding process.
2.4 The ICO Heath Group provides primary care services to nearly 11,000 patients.
2.5 The ICO Health Group submitted a planning application to Lewisham Council in February 2017. The application for new premises includes; (i) 10 Consultation Rooms; (ii) adequate space for GP Registrars; and (iii) meeting rooms for staff training and communications. The practices are awaiting the outcome.
2.6 Patient/Public Engagement 2.7 Patient engagement commenced in 2012/13 as a part of the initial merger. The individual
practices Patient Participation Groups (PPGs) were consulted and the notion of new premises was discussed.
2.8 ICO Health Group has recently embarked on a further round of consultation both to support the planning process for the new site and to update the PPG on the changes anticipated. The consultation process has included;
• PPG meetings • Public Consultation with evening meetings
Providers Providing • GP Practices • GP Super-partnerships • GP Federations • Multispecialty Community
Providers (MCP)/Primary and Acute Systems (PACS)
• GP List based care • At scale across local populations • Outcomes based • Core, Enhanced and Community services
110 of 114
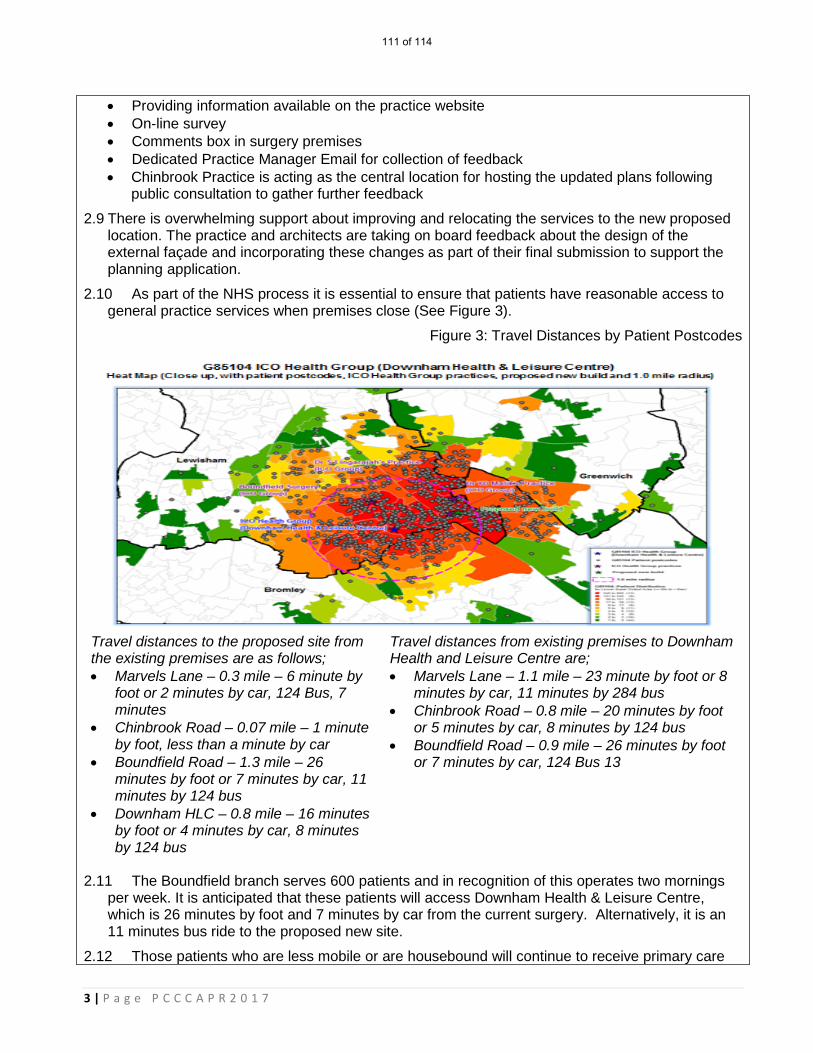
3 | P a g e P C C C A P R 2 0 1 7
• Providing information available on the practice website • On-line survey • Comments box in surgery premises • Dedicated Practice Manager Email for collection of feedback • Chinbrook Practice is acting as the central location for hosting the updated plans following
public consultation to gather further feedback
2.9 There is overwhelming support about improving and relocating the services to the new proposed location. The practice and architects are taking on board feedback about the design of the external façade and incorporating these changes as part of their final submission to support the planning application.
2.10 As part of the NHS process it is essential to ensure that patients have reasonable access to general practice services when premises close (See Figure 3).
Figure 3: Travel Distances by Patient Postcodes
Travel distances to the proposed site from the existing premises are as follows; • Marvels Lane – 0.3 mile – 6 minute by
foot or 2 minutes by car, 124 Bus, 7 minutes
• Chinbrook Road – 0.07 mile – 1 minute by foot, less than a minute by car
• Boundfield Road – 1.3 mile – 26 minutes by foot or 7 minutes by car, 11 minutes by 124 bus
• Downham HLC – 0.8 mile – 16 minutes by foot or 4 minutes by car, 8 minutes by 124 bus
Travel distances from existing premises to Downham Health and Leisure Centre are; • Marvels Lane – 1.1 mile – 23 minute by foot or 8
minutes by car, 11 minutes by 284 bus • Chinbrook Road – 0.8 mile – 20 minutes by foot
or 5 minutes by car, 8 minutes by 124 bus • Boundfield Road – 0.9 mile – 26 minutes by foot
or 7 minutes by car, 124 Bus 13
2.11 The Boundfield branch serves 600 patients and in recognition of this operates two mornings
per week. It is anticipated that these patients will access Downham Health & Leisure Centre, which is 26 minutes by foot and 7 minutes by car from the current surgery. Alternatively, it is an 11 minutes bus ride to the proposed new site.
2.12 Those patients who are less mobile or are housebound will continue to receive primary care
111 of 114
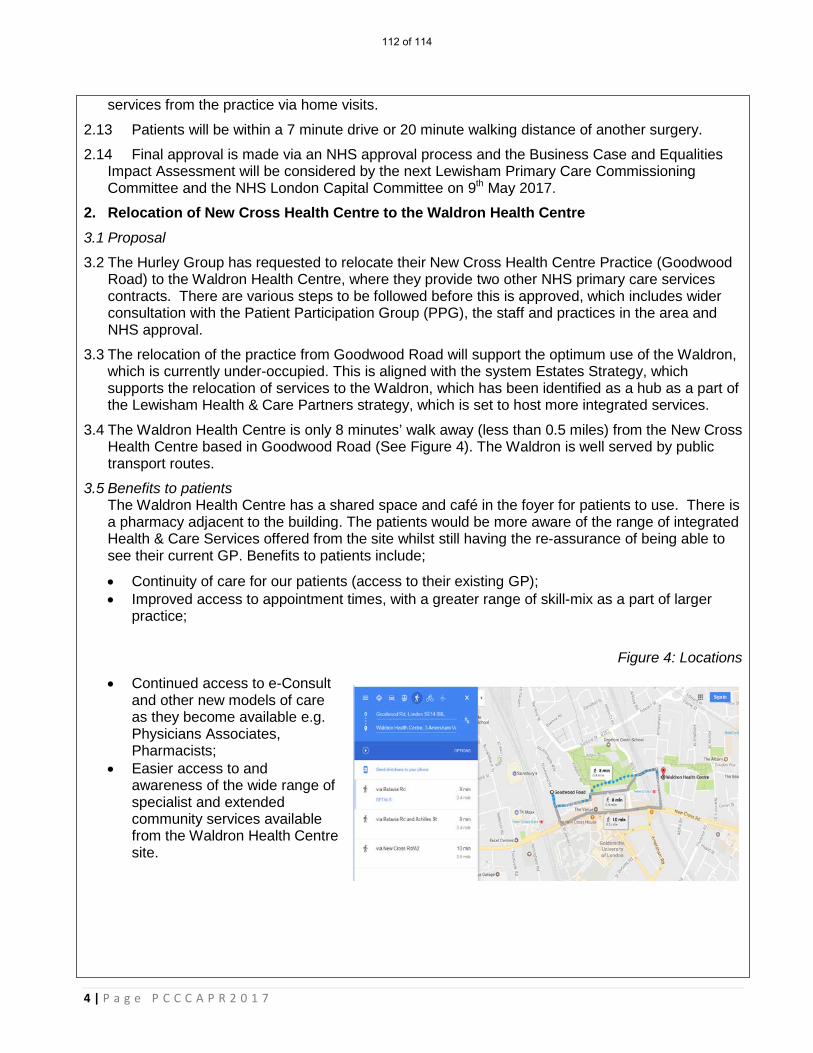
4 | P a g e P C C C A P R 2 0 1 7
services from the practice via home visits.
2.13 Patients will be within a 7 minute drive or 20 minute walking distance of another surgery.
2.14 Final approval is made via an NHS approval process and the Business Case and Equalities Impact Assessment will be considered by the next Lewisham Primary Care Commissioning Committee and the NHS London Capital Committee on 9th May 2017.
2. Relocation of New Cross Health Centre to the Waldron Health Centre 3.1 Proposal
3.2 The Hurley Group has requested to relocate their New Cross Health Centre Practice (Goodwood Road) to the Waldron Health Centre, where they provide two other NHS primary care services contracts. There are various steps to be followed before this is approved, which includes wider consultation with the Patient Participation Group (PPG), the staff and practices in the area and NHS approval.
3.3 The relocation of the practice from Goodwood Road will support the optimum use of the Waldron, which is currently under-occupied. This is aligned with the system Estates Strategy, which supports the relocation of services to the Waldron, which has been identified as a hub as a part of the Lewisham Health & Care Partners strategy, which is set to host more integrated services.
3.4 The Waldron Health Centre is only 8 minutes’ walk away (less than 0.5 miles) from the New Cross Health Centre based in Goodwood Road (See Figure 4). The Waldron is well served by public transport routes.
3.5 Benefits to patients The Waldron Health Centre has a shared space and café in the foyer for patients to use. There is a pharmacy adjacent to the building. The patients would be more aware of the range of integrated Health & Care Services offered from the site whilst still having the re-assurance of being able to see their current GP. Benefits to patients include;
• Continuity of care for our patients (access to their existing GP); • Improved access to appointment times, with a greater range of skill-mix as a part of larger
practice;
Figure 4: Locations
• Continued access to e-Consult and other new models of care as they become available e.g. Physicians Associates, Pharmacists;
• Easier access to and awareness of the wide range of specialist and extended community services available from the Waldron Health Centre site.
112 of 114
5 | P a g e P C C C A P R 2 0 1 7
4. Potential merger between Winlaton Surgery and South Lewisham Group Practice 4.1 Proposal
4.2 There are discussions about a potential merger between Winlaton Surgery and South Lewisham Group Practice (SLGP). The merger will enable SLGP to provide greater choice of appointment times, improved physical access and a wider pool of clinicians. Patients would still be able to see their usual GP and Nurse. Overall, it will enable SLGP to respond flexibly to any future changes that happen locally and in the NHS generally.
4.3 The Winlaton Surgery serves approximately 2000 patients.
4.4 In addition, Dr S Sivagnanasundaram will be retiring from Winlaton Surgery and this will support legacy planning. If the Winlaton Surgery re-locates to South Lewisham Group Practice there would be advantages for the patients; (i) it is a purpose built building, which is easily accessible for patients with mobility issues; (ii) car parking; and (iii) good transport links.
4.5 Such a merger would essentially; help to secure the sustainability of two practices that once merged will cover in the region of 17,000 patients.
4.6 The Council has supported the redevelopment of the South Lewisham Group Practice site via s106, which will support the merger.
4.7 The business case is in development and will be submitted to the Primary Care Commissioning Committee in May/June 2017.
CORPORATE AND STRATEGIC OBJECTIVES: 1. Planned Care: To support people with long term conditions better with proactive, holistic care
which improves the quality of their lives, is provided ‘out of hospital’ and reduces the requirement for hospital based outpatient attendances and inpatient admissions.
2. Urgent & Emergency Care: To commission Urgent Care and Emergency service which aligns the adult and children's physical and mental health services and addresses urgent care as early as possible ‘upstream’ – ‘right care, right time, right place’. This is the first phase of working towards commissioning an integrated Primary and Urgent care system.
CONFLICT OF INTEREST (CoI): N/A
CONSULTATION HISTORY: Consultation with key stakeholders will take place as a part of the business case process. Engagement with the Healthier Communities Select Committee is scheduled for 25th April 2017.
PUBLIC ENGAGEMENT: Public Engagement is a requirement with mergers or material changes to services – each of the proposed changes, have or will include engagement with practice Patient Participation Groups (PPG) and Healthwatch as a part of the business case process.
HEALTH INEQUALITY & PUBLIC SECTOR EQUALITY DUTIES: Equalities Impact Assessments (EIA) will be conducted as a part of the Business Case process.
Ensuring that all service redesign complies with CCG policies and the commissioning cycle will ensure that any service that is ultimately commissioned will have due regard to; (i) eliminate unlawful discrimination, harassment, victimisation and any other conduct prohibited by the Equality
113 of 114
6 | P a g e P C C C A P R 2 0 1 7
Act 2010; (ii) advance equality of opportunity between people who share a protected characteristic and people who do not share it; and (iii) foster good relations between people who share a protected characteristic and people who do not share it.
RESPONSIBLE MANAGERIAL LEAD CONTACT: Name: Diana Braithwaite; Email: [email protected]
114 of 114