antimicrobial effect of the endox endodontic system on...
TRANSCRIPT

FACULTEIT GENEESKUNDE EN
GEZONDHEIDSWETENSCHAPPEN
Academiejaar 2010 - 2011
Antimicrobial effect of the Endox Endodontic System® on planktonic and biofilm-grown
Enterococcus faecalis cells
Amir-Teymour MOINZADEH
Promotor: Prof. dr. Roeland De Moor Begeleider: Drs. Maarten Meire
Masterproef voorgedragen in de Master na Master Opleiding
Endodontologie


FACULTEIT GENEESKUNDE EN GEZONDHEIDSWETENSCHAPPEN
Academiejaar 2010 - 2011
Antimicrobial effect of the Endox Endodontic System® on planktonic and biofilm-grown
Enterococcus faecalis cells
Amir-Teymour MOINZADEH
Promotor: Prof. dr. Roeland De Moor Begeleider: Drs. Maarten Meire
Masterproef voorgedragen in de Master na Master Opleiding
Endodontologie

De auteur(s) en de promotor geven de toelating deze Masterproef voor consultatie
beschikbaar te stellen en delen ervan te kopiëren voor persoonlijk gebruik. Elk ander
gebruik valt onder de beperkingen van het auteursrecht, in het bijzonder met
betrekking tot de verplichting uitdrukkelijk de bron te vermelden bij het aanhalen van
resultaten uit deze Masterproef.
11 augustus 2011
Amir-Teymour MOINZADEH Prof. Dr. Roeland De Moor

Il est un certain nombre de personnes que je souhaiterais remercier pour leur contribution à
cette thèse.
Tout d‟abord le Professeur Roeland de Moor, qui m‟a offert l‟opportunité de mener cette
étude, qui m‟a fourni le cadre nécessaire à sa réalisation et m‟a amené à me poser certaines
questions pertinentes à son sujet.
Le Doctorant Maarten Meire, non seulement pour m‟avoir inculqué les notions de base
requises à mon travail de laboratoire, mais également pour sa guidance lors de l‟écriture de
cette thèse et pour tout son soutien depuis le début de cette étude.
Le Professeur Tom Coenye, pour sa constante disponibilité et la patience dont il a toujours
fait preuve pour répondre à toutes mes questions de profane en microbiologie. Je le remercie,
ainsi que le Professeur Hans Nelis, de m‟avoir accueilli au sein du laboratoire de leur
département dans le cadre de mes expériences.
Tous les membres du département de Microbiologie Pharmaceutique pour leur disponibilité et
leurs conseils.
Nathalie, pour son soutien, et sans qui la douce langue néerlandaise eut été massacrée dans ce
livre.
Table of contents
Abstract 1
Inleiding 2
Introduction 4
Materials & Methods 7
- Test device
- Test organism 10
- Determination of a sublethal concentration of NaOCl
on planktonic E. faecalis cells
- Effect of EES on planktonic E. faecalis cells
- Effect of EES on planktonic E. faecalis cells
in conjunction with a sublethal concentration of NaOCl
- Biofilm formation: inoculation
- Biofilm formation: effect of incubation time on biomass 11
- Effect of the EES on biofilm-grown E. faecalis cells 12
- Harvesting and quantification of the biofilms
- Plate count 13
Results 14
- Determination of a sublethal concentration
of NaOCl on planktonic E. faecalis cells
- Effect of EES on planktonic E. faecalis cells
with and without adjunction of NaOCl at a sublethal concentration
- Biofilm formation: effect of incubation time on biomass 15
- Effect of the EES on E. faecalis biofilms 16
Discussion 18
Conclusion 24
Samenvatting 25
References 32

1
Title
Antimicrobial effect of Endox Endodontic System® on planktonic and biofilm-grown
Enterococcus faecalis cells.
Abstract
Aim: To assess the antibacterial effect of the Endox Endodontic System®
(EES) on
Enterococcus faecalis cells in planktonic and sessile (biofilm-grown) state and to test whether
the electroporation ability attributed to the EES renders E. faecalis in planktonic state more
susceptible to sodium hypochlorite (NaOCl).
Methodology: One hundred µl of an E. faecalis suspension, containing approximately 106
cells, was subjected to EES treatment (3 fulgurations) or mixed with different concentrations
of sodium hypochlorite (NaOCl) with 1 min contact time. A sublethal NaOCl concentration
was used on the bacterial suspension after EES application. The number of surviving bacteria
after each treatment was determined by plate count.
E. faecalis biofilms were grown on hydroxyapatite blocks in a microtiter plate and incubated
for 24 hours. The biofilms were treated with EES (3 and 6 fulgurations) in a pipettor tip
containing physiological saline. Surviving bacteria were harvested and the number of CFU
per piece was determined by plate count.
Results: In the planktonic tests, there were no statistically significant differences in the
number of E. faecalis cells between control and treatment groups (P=0.12). In the biofilm
tests, there were no statistically significant differences in the number of E. faecalis cells
between control and treatment groups (P=0.19).
Conclusion: Within the limitations of this in vitro study, no antibacterial effect of EES on
planktonic or biofilm-grown E. faecalis cells could be demonstrated. The susceptibility of E.
faecalis to NaOCl was not affected by the use of the EES.
2
Het antibacteriële effect van het Endox Endodontic System®
op Enterococcus faecalis,
planktonisch en in biofilm
Inleiding
Endodontologie kan op basis van de definitie van de European Society of Endodontology als
volgt worden samengevat: „ Endodontologie is de studie van de vorm, functie en gezonde
toestand van de dentale pulpa en periradiculaire regio. Endodontologie bestudeert de
afwijkingen en traumata hiervan met het oog op preventie en behandeling; De meest
voorkomende endodontische ziekte is apicale peridontitis en wordt veroorzaakt door infectie
van het wortelkanaal.‟(European Society of Endodontology 2006)
Desinfectie van het wortelkanaal wordt dus beschouwd als een essentieel aspect van de
wortelkanaalbehandeling, aangezien micro-organismen een cruciale rol spelen in de
pathogenese van apicale peridontitis (AP) (Kakehashi et al. 1965) en hun eradicatie uit het
wortelkanaal van belang is voor de genezing van voorafbestaande AP (Fabricius et al. 2006).
Door middel van instrumentatie en lokale antimicrobiële therapie worden bacteriën uit het
wortelkanaal verwijderd, maar door de complexe anatomie van het wortelkanaal, zijn de
huidige technieken onvoldoende om het wortelkanaal te steriliseren (Sjögren et al. 1997). Als
een gevolg hiervan is apicale peridontitis een belangrijk gezondheidsprobleem in de
bevolking (Hommez et al. 2002, Ng et al. 2007, Peters et al. 2011).
Los van de complexe anatomie, speelt de vorming van een biofilm ter hoogte van het
wortelkanaaloppervlak een rol (Chavez de Paz 2007). Wanneer micro-organismen in contact
komen met oppervlaktes, produceren ze extracellulaire polymeren of glycocalyx, waardoor er
zich al het ware een enveloppe vormt rond de organismes en ze microkolonies onwikkelen
(Costerton et al. 1981). Deze biofilm-vorming bezorgt bacteriën een overlevingsvoordeel, niet
in het minst door verminderde gevoeligheid voor antibacteriële therapie en chemische agentia
(Bale et al. 1988, Chavez de Paz 2007).
Behandelde wortelkanalen van tanden met persisterende AP zijn voornamelijk
gekoloniseerd/geïnfecteerd met Gram-positieve bacteriën. Enterococcus faecalis, een
commensaal uit de gasto-intestinale tractus, mondholte en vagina, is hierbij de meest
frequente (Sundqvist et al. 1998) (Kayaoglu & Ørstavik 2004). Reinculturen van E. faecalis,
geïsoleerd uit wortelkanalen, werden beschreven (Portenier et al. 2003). E. faecalis heeft

3
verschillende overlevingsstrategieën, zoals resistentie ten opzichte van calciumhydroxide
(Distel et al. 2002) door middel van een protonpomp die de intracellulaire pH constant houdt
(Evans et al. 2002; Kobayashi et al. 1982) en de capaciteit om zich aan dentine te hechten
door collageen-bindende proteïnen (Hubble 2003). Dit alles bemoeilijkt eradicatie met de
conventionele endodontische agentia (Stuart et al. 2006).
In de hoop wortelkanaaldesinfectie te kunnen optimaliseren zijn er recent nieuwe technieken
ontwikkeld (Haapasalo et al. 2010). Eén ervan is gebaseerd op het principe van elektroporatie.
Hierbij wordt het celmembraan van bacteriën blootgesteld aan een korte hoogvoltage puls (>
1kV) om poriën te creëren, zodat micro-organismen meer gevoelig worden aan toegediende
chemische agentia (Haas & Aturaliye 1999).
In de endodontologie is het Endox Endodontic System® (EES) (Lysis, Nova Milanese, Italy)
ontwikkeld. Het werkingsmechanisme is gebaseerd op elektroporatie, met als doel micro-
organismen in het wortelkanaal vatbaarder te maken voor antibacteriële behandelingen zoals
natriumhypochloriet (NaOCl) (Cassanelli et al. 2008). Er wordt een actieve elektrode in het
wortelkanaal geplaatst en een neutrale elektrode wordt door de patiënt vastgehouden. De
geproduceerde elektromagnetische golven produceren een elektrisch veld dat de pulpa ableert
(Lendini et al. 2005) en micro-organismen in het wortelkanaal elimineert (Virtej et al. 2007).
In een studie van Lendini et al. verbeterde het gebruik van EES de reiniging van het
wortelkanaal en de eliminatie van organische residu‟s na mechanische instrumentatie (Lendini
et al. 2005). Virtej et al. onderzocht EES in een ex vivo model en stelde een antibacteriële
werking van EES vast, doch conventionele desinfectie met NaOCl was superieur (Virtej et al.
2007).
Het doel van deze studie is het antimicrobiële effect van het Endox Endodontic System®
te
onderzoeken, op E. faecalis, planktonisch en in biofilm en na te gaan of er verhoogde
gevoeligheid voor NaOCl ontstaat bij E. faecalis na het gebruik van EES.

4
Introduction
“Endodontology is concerned with the study of the form, function and health of, injuries to
and diseases of dental pulp and periradicular region, their prevention and treatment; the
principal disease being apical periodontitis, caused by infection.” (European Society of
Endodontology, 2006). Micro-organisms and their by-products play a crucial role in the
pathogenesis of apical periodontitis (AP) (Kakehashi et al. 1965) and their eradication from
the root canal system is important to the healing process of pre-existing AP (Fabricius et al.
2006). As a consequence, disinfection of the root canal system has been recognized as an
essential aspect of endodontic therapy. The elimination of the micro-organisms from the root
canal system by means of instruments and antimicrobial agents is expected to provide the
favourable environment required for healing (Nair, 2004); Nevertheless, due to the complex
anatomy of the root canal system, current chemo-mechanical cleaning methods cannot render
this system bacteria-free (Sjögren et al. 1997) and as a result, apical periodontitis remains a
frequent pathology in the population (Hommez et al. 2002, Ng et al. 2007, Peters et al. 2011).
It is now accepted that in natural environments micro-organisms are commonly in close
association with surfaces (Costerton et al. 1987). Their growth on surfaces provokes the
production of important quantities of extracellular polymers, the glycocalyx, that will envelop
the attached cells and produce diffuse micro-colonies (Costerton et al. 1981). The ubiquitous
nature of sessile growth (biofilm) is recognized and extensively researched. In dilute and/or
hostile environments, growth and organization of microbial cells at surfaces confer them
many advantages upon the planktonic cells. The main hypothesis concerning the microbial
recalcitrance of microbial biofilms towards chemical and antibiotic treatments are the
following ones: (1) the produced glycocalyx prevents the penetration of antimicrobials agents
to the micro-organisms; (2) the surface of the glycocalyx and the outlying micro-organisms
have the capacity of reacting with and quenching some of the biocides; (3) the limitation of
the availability of nutrients within the biofilm diminishes the growth rate and can provoke
changes in the phenotype of the micro-organisms; (4) the attachment to surfaces causes the
genotype to shift towards one associated with sessile existence and this affects the
antimicrobial susceptibility. (Brown & Gilbert 1993) Furthermore there is also a possibility of
genetic exchange due to the close proximity of other cells. (Bale et al. 1988)

5
Increasing information is now available concerning the polymicrobial organization of micro-
organisms into biofilms on the root canal surfaces. The adaptative mechanisms provide the
biofilm community increased survival (Chavez de Paz 2007).
Enterococci are commensal of the gastrointestinal tract, the oral cavity and the vagina
(Kayaoglu & Ørstavik 2004). Enterococci are a major cause of nosocomial infections, and
within this group Enterococcus faecalis is the major cause of human enterococcal infections
(Murray 1998).
The microbial flora recovered from root filled teeth with persistent apical periodontitis is
mainly Gram-positive, Enterococcus faecalis being the most frequently recovered species
(Sundqvist et al. 1998). It is rarely present in the flora of untreated necrotic teeth (Sundqvist
1992), but is often present in previousely treated teeth (PTT) with AP (Molander et al. 1998).
According to Portenier et al., E. faecalis is even sometimes isolated in pure culture (Portenier
et al. 2003). Moreover E. faecalis possesses various survival strategies that enable its survival
in harsh conditions and make it therefore difficult to eradicate with the conventional
endodontic disinfectants (Stuart et al. 2006). Among those strategies there are: (1) its
resistance to calcium hydroxide (Distel et al. 2002) due to a proton pump which keeps the
cytoplasmic pH constant. (Evans et al. 2002, Kobayashi et al. 1982), (2) its widespread
genetic polymorphism (Lee et al., 2004), (3) its collagen-binding proteins which help it bind
dentin (Hubble et al. 2003), its small size which enables it to penetrate dentinal tubulis (Love
2001), (4) its tolerance to long starvation periods (Figdor et al. 2003) and its ability to
suppress the action of lymphocytes (Lee et al. 2004). Those specific features are enough
reasons to justify why it is an ideal species to be investigated.
In the strive for optimal root canal disinfection, the endodontic discipline has recently
witnessed the introduction of new methods and techniques promising better root canal
disinfection. (Haapasalo et al. 2010)
A promising path which has been investigated in some scientific fields is the increased
susceptibility of micro-organisms to chemicals after exposure to electric currents by means of
electroporation. Electroporation is defined as the application of a brief high voltage (>1 kV)
pulse with the aim of creating pores in the cell membranes of micro-organisms (Haas &
Aturaliye 1999). It has multiple applications for inserting material such as DNA, proteins,
viruses and other macromolecules inside cells. The created pores are caused by an increased

6
transmembrane voltage which has to reach a value of 0,5-1,5 V during at least a few
microseconds (the physiologic transmembrane voltage is 0,1 V). The applied impulses are
103- 10
4 V/m and last for micro- to milli-seconds. This causes reversible electrical breakdown
(REB) with an increase in molecular transport through the membrane. After few micro-
seconds there is a rapid membrane discharge which brings the elevated transmembrane
voltage back to the physiologic one. However the membrane recovery remains slow
especially with the influx and efflux of the chemicals provoking chemical imbalances which
will determine the faith of the cell, which is either survival or death (Weaver 1993).
The Endox Endodontic System® (EES) (Lysis, Nova Milanese, Italy) is a device that releases
high-frequency alternating current (HFAC) in form of electrical pulses of short duration. It
consists of an active electrode which can be placed into the root canal and a neutral electrode
held in the patient‟s hand. According to the manufacturer the electromagnetic wave produced
by this electrical discharge generates the passage of a considerable quantity of energy in the
field and is supposed to ablate pulp tissue (Lendini et al. 2005) and/or eliminate intra-canal
micro-organisms (Virtej et al. 2007).
Lendini and co-workers investigated the effect of EES on organic tissue in root canals and
concluded that these high frequency pulses improved the cleansing and elimination of organic
residues, though only after mechanical instrumentation (Lendini et al. 2005). Virtej et al.
tested various root canal disinfection methods in an ex vivo tooth model. They reported an
antibacterial effect of EES, but the conventional method of disinfection with NaOCl was
found to be superior (Virtej et al. 2007).
This electroporation phenomenon has been observed using the Endox device (Cassanelli et al.
2008). If this would be the case, the Endox may make the cells more susceptible to the effects
of antimicrobial agents such as sodium hypochlorite, the gold standard root canal irrigant
(Zehnder 2006).
The purpose of this study is to investigate the antimicrobial effect of the Endox Endodontic
System® on Enterococcus faecalis cells in planktonic and sessile (biofilm-grown) state and to
assess if E. faecalis would present an increased susceptibility to a sublethel NaOCl
concentration after use of the EES.

7
Materials and methods
Tested Device
The EES (Fig. 1) is composed of a positive electrode which is a stainless steel needle that is
placed inside the root canal (Fig. 3), and a neutral one which is held in the patient‟s hand. To
simulate this in vitro, the model used by Cassanelli et al. (Cassanelli et al. 2008) was
modified (Fig. 2). An orthodontic stainless-steel wire (TP orthodontics inc., USA) was linked
to the negative pole of the device. This 0.51mm diameter wire was chosen in order to fit
precisely in the narrowest opening of the 100µL pipettor tip simulating the root canal space
(Fig 4). The Endox Endodontic System (Fig 1) was set at incisor mode + boost .This
corresponds approximately to a 140 ms pulse at a frequency of 312.5 kHz and 1200 kV/m.
Fig. 1: The Endox Endodontic System

8
Figure 1: The EES device
Fig. 2: Schematic representation of the experimental setup
Positive electrode
elece Figure 4:
Fire flashes at the
negative electrode
during EES
application.
O+ +=r++
Neutral electrode electrode
Pipettor tip containing either bacterial suspension or HA block in NaCl 0.9%
EES

9
Figure 3: Positive electrodes of the EES
Figure 4: Pipettor tip containing bacterial suspension connected to the neutral electrode.

10
Test organism
A pure culture of E. faecalis ATCC 10541 was grown in Tryptic Soy Broth (TSB) and
incubated overnight at 37 °C. A ten-fold serial dilution was then prepared in physiological
saline (PS, 0.9% (w/v) NaCl), to obtain working concentrations of 106 to 10
7 CFU/mL.
Determination of a sublethal concentration of NaOCl on planktonic E. faecalis cells
The tested NaOCl concentrations were: 0.025% (w/v), 0.0025%, 0.00025% and 0.000025%.
To this end, freshly prepared NaOCl 2.5% w/v (University Hospital Pharmacy, Ghent,
Belgium) was diluted into different concentrations. 100 µL of the working suspension was
added to 10 mL of the different NaOCl concentrations and vortexed. After 1 min exposure,
1mL of the solution was added to 9 mL Na2S2O3 (2.5%) for neutralization of NaOCl. Serial
tenfold dilutions in TSB were made (10-1
to 10-5
).
Effect of EES on planktonic E. faecalis cells
100 µl of the working suspension was taken with a sterile pipettor tip. The tip was then placed
on a stainless-steel wire connected to the neutral pole of the Endox device. The black needle
(positive electrode) was introduced into the pipettor tip until the mid-level of the solution and
3 fulgurations were given at incisive mode + boost. The pipettor tip was then removed from
the wire and its content emptied in 10 mL saline. Serial tenfold dilutions in TSB were made
(10-1
to 10-5
).
Effect of EES on planktonic E. faecalis cells in conjunction with a sublethal
concentration of NaOCl
100 µl of the working suspension was subjected to 3 EES fulgurations as described above.
The pipettor tip was then removed from the wire and its content emptied in 10 mL of NaOCl
(2.5x10-5
%), and 1 min contact time was allowed. Then 1 mL was added to 9 mL Na2S2O3
(2.5%) for neutralization of the NaOCl activity. Serial ten-fold dilutions in TSB were made
(10-1
to 10-5
).
Biofilm formation: inoculation
Enterococcus faecalis was inoculated into Tryptic Soy Broth (TSB) and grown overnight at
37°C. Cells were collected by centrifugation (4000 rpm, 4 min) and the pellets were
resuspended in fresh TSB. 12 hydroxyapatite disks (5 x 2 mm, Clarkson Chromatography
Products, South Williamsport, PA, USA) (Fig. 5) were sterilized and placed in different

11
compartments of flat-bottomed 24-well polystyrene microtitre plates (TPP, Trasadingen,
Switzerland). The wells were inoculated with 2 mL of the E. faecalis cell suspension. The
microtiter plate was incubated at 37°C for 4 hours to allow the adhesion process to take place.
Then the inoculum suspension was removed, the wells were rinsed twice with 1 mL TSB to
remove nonadherent cells. Two mL of fresh TSB was added to each compartment, and the
plates were incubated at 37°C.
Fig 5: Standardized HA block.
Biofilm formation: effect of incubation time on biomass
Before choosing the incubation time of the biofilms in the subsequent series of experiment,
the effect of the incubation time on the biomass was investigated in order to check if any
significant difference would be found between a 1-day old and a 3-days old biofilm. Biofilms
were grown for 24 and 72 hours (n=6 per group). Based on the comparison of the number of
recovered bacteria under these conditions, 24 hour incubation time was chosen for subsequent
experiments. After inoculation and incubation, the discs were randomly allocated to the
experimental or control groups. The different treatments were carried out in triplicate on at
least three discs (n ≥ 9).

12
Effect of the EES on biofilm-grown E. faecalis cells
An overnight culture of E. faecalis was freshly prepared. Hydroxyapatite disks were
segmented into blocks of equal sizes which could fit in a 100 µL pipettor tip. Those blocks
were then sterilized and placed in different compartments of a microtiter plate. They were
then inoculated as mentioned before and incubated for 24h.
0.1 mL saline was preleved with a sterile pipettor tip. The tip was then placed on a stainless-
steel wire connected to the neutral pole of the Endox device. A HA block was introduced in
the pipettor tip by means of sterile pliers (Fig. 6). The Endox tip (positive electrode) was
introduced into the pipettor tip in the vicinity of the HA block and proceeded to 0, 3 or 6
fulgurations at incisive + boost mode according to the tested group.
Fig 6: HA block inside the pipettor tip.
Harvesting and quantification of the biofilms
To harvest surviving adherent cells, each HA disc or block was transferred to a test tube
containing 10 ml of TSB and subjected three times to the combination of 30 seconds vortex
mixing and 30 seconds sonication (Branson 3510, 42 kHz, 100 W, Branson Ultrasonics
Corp.). Serial tenfold dilutions in TSB were made (10-1
to 10-7
).

13
Plate count
Aliquots (1ml) of each (diluted) bacterial suspension were transferred to Petri dishes and
mixed with molten (45°C) TSA. After solidification of the agar, the plates were incubated
aerobically at 37°C for at least 48 h. Finally, the number of colony forming units (CFUs) in
the undiluted suspensions were calculated and expressed as CFU/10ml for the suspension
tests and CFU/piece for the biofilm tests. Cell counts were logarithmically transformed to
normalize the data prior to statistical comparison (one-way ANOVA, post hoc Scheffe test
and t-test. Level of significance set at 5%) (PASW Statistics 18, SPSS Inc, Chicago, IL). The
mean and standard deviation of each group were calculated.

14
Results
Determination of a sublethal concentration of NaOCl on planktonic E. faecalis cells
Table 1 shows the effect of the different NaOCl concentrations on planktonic E. faecalis cells.
After 1 min contact with 2.5x10-3
% NaOCl, no cells were recovered. Contact with 2.5x10-4
%
NaOCl resulted in a mean reduction in viable counts of 5.8 log units which is statistically
significant (P<0.001). Contact with 2.5x10-5
% NaOCl did not result in a statistical significant
reduction in viable counts (P=0.99). So only NaOCl 2.5x10-4
% and NaOCl 2.5x10-5
% were
sublethal to the tested organism after 1 minute exposure, so that 2.5x10-3
% NaOCl was lethal.
Due to better reproducibility (less standard deviation) of the results, the latest concentration
(NaOCl 2.5x10-5
%) was chosen for the subsequent experiment.
Table 1: Effect of different NaOCl concentrations on planktonic E. faecalis cells (1 min
contact time).
Treatment n Mean log CFU +/- SD
Control 20 7.48 +/- 0.16
NaOCl 2.5x10-3
% 9 0 +/- 0
NaOCl 2.5x10-4
% 9 1.68 +/- 2.15
NaOCl 2.5x10-5
% 9 7.30 +/- 0.24
The results represent mean values with their standard deviations.
Effect of EES on planktonic E. faecalis cells with and without adjunction of NaOCl at a
sublethal concentration
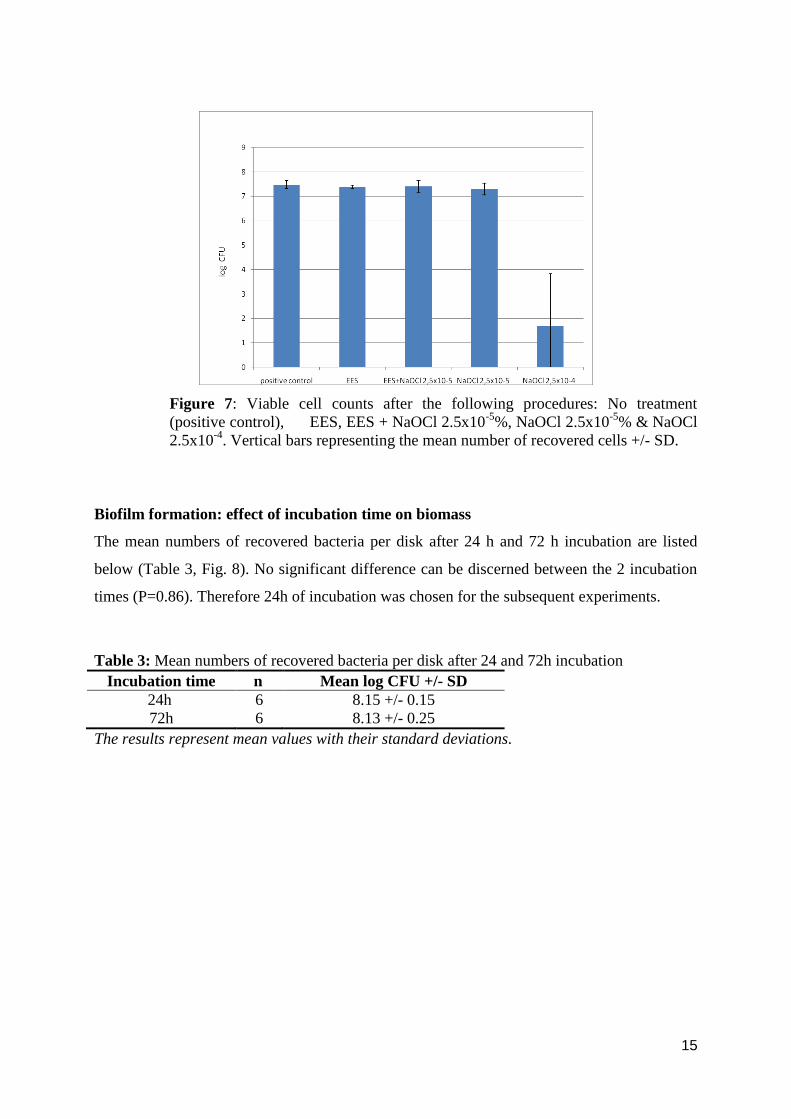
Table 2 contains the logarithmic counts of the following groups: positive control/ EES with
and without use of NaOCl at the chosen sublethal concentration and sodium hypochlorite at
the chosen sublethal concentration alone. No significant difference was found between the 4
groups (P=0.12). During fulguration, flashes were frequently noticed at the end of the pipettor
tip (Fig. 10).
Table 2: Effect of EES on planktonic E. faecalis cells with and without adjunction of NaOCl
at a sublethal concentration
Treatment n Mean log CFU +/- SD
Control 20 7.48 +/- 0.16
Endox 9 7.38 +/- 0.08
Endox + NaOCl 2.5x10-5
% 9 7.40 +/- 0.26
NaOCl 2.5x10-5
% 9 7.30 +/-0.24
The results represent mean values with their standard deviations.
15
Figure 7: Viable cell counts after the following procedures: No treatment
(positive control), EES, EES + NaOCl 2.5x10-5
%, NaOCl 2.5x10-5
% & NaOCl
2.5x10-4
. Vertical bars representing the mean number of recovered cells +/- SD.
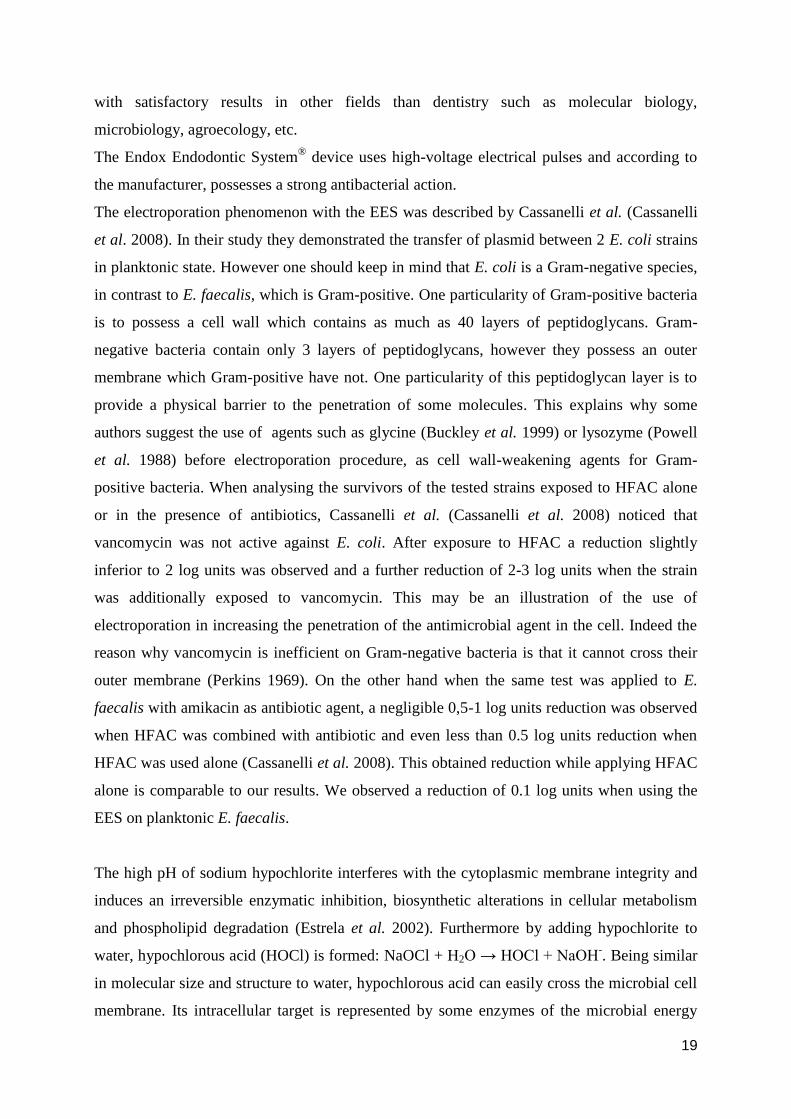
Biofilm formation: effect of incubation time on biomass
The mean numbers of recovered bacteria per disk after 24 h and 72 h incubation are listed
below (Table 3, Fig. 8). No significant difference can be discerned between the 2 incubation
times (P=0.86). Therefore 24h of incubation was chosen for the subsequent experiments.
Table 3: Mean numbers of recovered bacteria per disk after 24 and 72h incubation
Incubation time n Mean log CFU +/- SD
24h 6 8.15 +/- 0.15
72h 6 8.13 +/- 0.25
The results represent mean values with their standard deviations.

16
Figure 8: Biomass of an E. faecalis biofilm after 24h and 72h incubation.
Vertical bars representing the mean number of recovered cells +/- SD.
Effect of the EES on E. faecalis biofilms
The mean numbers of culturable E. faecalis cells after EES application (3 and 6 fulgurations)
are presented in Table 4 and Figure 9. No significant differences were found between the
control group and the treatment groups (P = 0.19).
Table 4: Effect of the EES (3 and 6 applications) on E. faecalis biofilms.
Group n Mean log CFU+/- SD
Control 12 6.73 +/- 0.41
EES (3 fulgurations) 9 6.51 +/- 0.35
EES (6 fulgurations) 9 6.81 +/- 0.26
The results represent mean values with their standard deviations.

17
Figure 9: Viable cell counts from an E. faecalis biofilm after the following
procedures: no treatment (positive control), EES (3fulgurations and 6
fulgurations). Vertical bars represent the mean number of recovered cells +/-
SD.
Figure 10: Flash at the negative electrode during EES application.

18
Discussion
E. faecalis is found in root canals associated with endodontic treatment failure (Molander et
al. 1998) and appears to possess the ability to resist inhospitable conditions such as an
alkaline environment (Flahaut et al. 1997) and long-period starvation(Hartke et al. 2002). So
when other species surrender, this one still survives. This makes E. faecalis an interesting
species for evaluating the effect of different antimicrobial strategies (Kayaoglu & Orstavik
2004). Its susceptibility to disinfection procedures, both in planktonic and sessile state, has
already been extensively investigated (Stuart et al. 2006). Even though E. faecalis possesses
subtle defence mechanisms, it has been demonstrated that it cannot stand the action of NaOCl
at the highest concentrations used during endodontic treatment (Retamozo et al. 2010).
However E. faecalis is frequently identified in cases with post-treatment disease (Molander et
al. 1998, Portenier et al. 2003). This leads us to the question whether the capacity of the
endodontic flora to locate itself in fins and ramifications, and escape chemo-mechanical
preparation, would explain the difficulty to render a root canal bacteria-free (Lin et al. 2008).
The complexity of the root canal system offers indeed an excellent ecological refuge to the
micro-organisms (Vertucci 1984, Fabricius 2006). Therefore new approaches are and should
be looked after in order to provide better disinfection of those unreachable areas of the root
canal system (Meire et al. 2009).
In a dilute or hostile environment, growth and organization of microbial cells at surfaces
confer them many advantages (such as increased protection, increased growth prospects,
environmental modulation and the possibility of exchanging genetic material), which are not
apparent in nutritionally-rich environments. Such associations between micro-organisms and
between micro-organisms and their environment are called biofilm (Costerton et al. 1987).
The theory about the capacity of micro-organisms to be in close association with surfaces and
form a biofilm is now widely accepted.
One of the strategies which have gained interest in eradication against biofilms is the use of
electric current in conjunction with chemicals. This is one of the applications of the
electroporation principle. Electroporation can be defined as the application of a brief high
voltage (>1 kV) pulse with the aim of creating pores in the cell membranes of a suspension of
micro-organisms (Haas & Aturaliye 1999). This results in a significant increase of
the electrical conductivity and permeability of the cell plasma membrane caused by the
externally applied electrical field (Neumann et al. 1982). This method is already being used
19
with satisfactory results in other fields than dentistry such as molecular biology,
microbiology, agroecology, etc.
The Endox Endodontic System® device uses high-voltage electrical pulses and according to
the manufacturer, possesses a strong antibacterial action.
The electroporation phenomenon with the EES was described by Cassanelli et al. (Cassanelli
et al. 2008). In their study they demonstrated the transfer of plasmid between 2 E. coli strains
in planktonic state. However one should keep in mind that E. coli is a Gram-negative species,
in contrast to E. faecalis, which is Gram-positive. One particularity of Gram-positive bacteria
is to possess a cell wall which contains as much as 40 layers of peptidoglycans. Gram-
negative bacteria contain only 3 layers of peptidoglycans, however they possess an outer
membrane which Gram-positive have not. One particularity of this peptidoglycan layer is to
provide a physical barrier to the penetration of some molecules. This explains why some
authors suggest the use of agents such as glycine (Buckley et al. 1999) or lysozyme (Powell
et al. 1988) before electroporation procedure, as cell wall-weakening agents for Gram-
positive bacteria. When analysing the survivors of the tested strains exposed to HFAC alone
or in the presence of antibiotics, Cassanelli et al. (Cassanelli et al. 2008) noticed that
vancomycin was not active against E. coli. After exposure to HFAC a reduction slightly
inferior to 2 log units was observed and a further reduction of 2-3 log units when the strain
was additionally exposed to vancomycin. This may be an illustration of the use of
electroporation in increasing the penetration of the antimicrobial agent in the cell. Indeed the
reason why vancomycin is inefficient on Gram-negative bacteria is that it cannot cross their
outer membrane (Perkins 1969). On the other hand when the same test was applied to E.
faecalis with amikacin as antibiotic agent, a negligible 0,5-1 log units reduction was observed
when HFAC was combined with antibiotic and even less than 0.5 log units reduction when
HFAC was used alone (Cassanelli et al. 2008). This obtained reduction while applying HFAC
alone is comparable to our results. We observed a reduction of 0.1 log units when using the
EES on planktonic E. faecalis.
The high pH of sodium hypochlorite interferes with the cytoplasmic membrane integrity and
induces an irreversible enzymatic inhibition, biosynthetic alterations in cellular metabolism
and phospholipid degradation (Estrela et al. 2002). Furthermore by adding hypochlorite to
water, hypochlorous acid (HOCl) is formed: NaOCl + H2O → HOCl + NaOH-. Being similar
in molecular size and structure to water, hypochlorous acid can easily cross the microbial cell
membrane. Its intracellular target is represented by some enzymes of the microbial energy
20
metabolism. This results in a powerful lethal action of chlorine on bacteria without possibility
of microbial resistance. In addition to exerting its antimicrobial activity inside the cytoplasmic
compartment, NaOCl also possesses a degrading effect on the cellular membrane.
A concentration is lethal to the micro-organisms present in a suspension when it is high
enough to eradicate all the cells contained in this suspension. Sublethal concentrations are all
the concentrations which are not high enough to eradicate all the cells present in the
suspension. After a sublethal chemical treatment we can distinguish different proportions of
dead cells (lethally or irreversibly injured), uninjured cells (normal cells) and injured cells
(stressed, reversibly injured) (Wu 2008).
Apart from investigating the direct antimicrobial effect of the EES on planktonic cells, we
also wished to evaluate if the application of electric current by the EES would be an aid to the
chemical disinfection by a sublethal concentration of NaOCl which would be innocuous
otherwise. To investigate this we first looked for a sublethal concentration of sodium
hypochlorite to which we could expose the bacteria for 1 minute after having them
electrostimulated. Starting from a 2.5% NaOCl solution, ten-fold serial dilutions allowed us to
test concentrations ranging between 2.5 x 10-2
% to 2.5 x 10-5
%. The only identified sublethal
concentrations were 2.5 x 10-4
% and 2.5 x 10-5
%. Of those two the latest was chosen because
of more reproducibility in number of surviving cells. Indeed 2.5 x 10-4
% was most of the time
lethal to our suspension. When comparing 2.5 x 10-5
% NaOCl to saline, a decrease of 0.18
log CFU could be observed with NaOCl after 1 minute exposure. This reduction is not
statistically significant. 2.5 x 10-4
% even though sublethal was mainly lethally or irreversibly
injuring the microorganisms so that 2.5 x 10-5
% was mainly stressing or reversibly injuring
them but was unable to kill them after 1 minute exposure. Therefore the latter was chosen. E.
faecalis was electrostimulated 3 times and then either exposed for a whole minute to sodium
hypochlorite at 2.5 x 10-5
% or to physiologic saline. No difference was observed among those
2 groups and the control group (no treatment). From this we can conclude that EES alone or
in combination with NaOCl at a sublethal concentration has no effect on planktonic E.
faecalis cells under the conditions of the present study.
The following fold of our study was the investigation of the effect of the EES on E. faecalis
biofilms. We first started with a quantitative comparison between 24 and 72 hours-old E.
faecalis biofilms by means of plate counting. Even if some authors (Chavez de Paz et al.
2010, Jiang et al. 2011) are now using a 24h biofilm, we first wanted to confirm if
quantitatively a difference existed between a 24h biofilm and an older one such as a 72h one.

21
The present results showed no difference in terms of CFU count between biofilms grown for
24 or 72 hours. Even though a difference certainly exists in terms of biofilm maturity and
complexity when using longer (e.g. several weeks) incubation times, this can in no way be
compared to the degree of maturation of the biofilms met in infected root canals in vivo,
which have already been contaminated for months or even years.
The next experiment evaluated the effect of the EES on a 24h E. faecalis biofilm grown on
hydroxyapatite (HA) blocks. HA blocks were chosen as surface to grow the biofilms for 2
main reasons reasons. First dentin is composed of HA for 70%. Second, the HA blocks
provided a good way to standardize the surface area and homogeneity to which the biofilm
would attach. Due to the fact that no antibacterial activity could be determined in the
planktonic experiment and that biofilms are considered more resistant, a subgroup with 6
impulses was added. Nevertheless, 3 as well as 6 impulses didn‟t exhibit any antibacterial
action. The EES failed to show any antibacterial activity on a 24h E. faecalis biofilm. The fact
that it could not affect this relatively young single-species biofilm suggests its probable
inefficiency when dealing with more complex biofilms such as those present in an infected
root canal in vivo.
Concerning the antimicrobial activity of the EES, Virtej et al. in their clinical study found that
the EES was less effective than other disinfection methods, but they still noticed a reduction
from approximately 10 000 to 4000 CFU in bacterial counts after EES application (Virtej et
al. 2007). When converted into logarithmic count this corresponds to a reduction from 4 log
to 3,6 log units. Furthermore in their study, teeth were infected by an oral flora issued from
human saliva, which is known to be composed of a “melting-pot” of species and not of a
specific strain as we did in our study (Brito et al. 2007). This may be one of the explanations
to the antimicrobial activity observed since different strains are unequally resistant to electric
current because of the differences in their cell membranes composition (Lojewska et al.
1989). In addition they used the paper point technique for sampling, which is considered to be
unable to provide a trustful representation of the degree of infection of the root canal system
(Möller 1966) especially when one is willing to sample biofilms. In their study they used 6
electric impulses so that we only used 3 in our planktonic experiments. This may also
contribute to the observed difference. Lastly there is no information about the used medium in
their setup to conduct the electrical flow inside the root canal and yet it is known that
properties such as the chemical composition of the conducting solution, have an effect on the
efficiency of electroporation (Lee et al. 2008).

22
One of the advantages of this in vitro model was that it offered a direct visualisation of the
medium during the testing. For instance, adjustments of the neutral electrode were sometimes
necessary during the testing due to the formation of bubbles (gas) which could disrupt the
electric conductivity within the medium. In the narrowest extremity of the pipettor tip, which
would correspond to the apex in a tooth model, “flashes” were frequently observed. This
might be some sort of arc flashing. An arc flash is the ball of fire that explodes from an
electrical short circuit. A short circuit in an electrical circuit allows a current to travel along a
path where essentially no (or a very low) electrical impedance is encountered. In a circuit
which has both capacitors and resistors, such as a root canal, the total amount of opposition to
an alternating current is called impedance (Nekoofar et al. 2006). According to Ushiyama,
this value presents a sharp variation at the root canal constriction (the narrowest point at the
apical foramen), where the voltage gradient and current density are the highest (Ushiyama
1983). Passed the constriction, there is a sharp decline of the voltage value due to the sudden
opening, and this may be the point where a short circuit would take place.
The explosive nature of those flashes raises safety concerns to periradicular tissues, especially
when one considers that larger cells such as nerve cells for instance are more vulnerable to
electrical breakdown than smaller such as bacteria are (Lee & Kolodney 1987).
Different experimental settings with various current settings and a multitude of tested micro-
organisms can be found in the literature (Haas & Aturaliye 1999, Szuminsky et al. 1994).
Factors such as electrical field strength, treatment time, cell size, membrane surface charge,
cytoplasm, and suspending medium also seem to play a role on the susceptibility of species to
electrical pulses (Lojewska et al. 1989).
These could explain the heterogeneity of the results obtained by the use of high frequency
current on micro-organisms. This is well-illustrated by the study of Lee et al. In which 1
electric impulse in brine was enough to totally inactivate L. monocytogenes whereas 10 were
necessary when the test was conducted in saline (Lee et al. 2008).
According to Weaver et al., the 2 possible causes of cell death after electroporation are
membrane rupture and chemical imbalance between the intra and extra-cellular compartments
(Weaver et al. 1993).
In this study we tested E. faecalis which, as a Gram-positive organism, possesses a thick
peptidoglycan layer which can prevent bursting induced by high cytoplasmic osmotic
pressure.

23
However due to the extreme diversity of the endodontic microbiota in clinical situation (Brito
et al. 2007), it is expected from a disinfecting method to be targeting at the widest range of
species as possible.

24
Conclusion
Within the limitations of this in vitro study, no antibacterial effect of Endox Endodontic
System on planktonic or biofilm-grown E. faecalis cells could be demonstrated. The
susceptibility of planktonic E. faecalis to NaOCl was not modified by application of the EES.
The results also highlight the importance of testing the efficiency of new devices before
clinical use.

25
Samenvatting
Doelstelling:
Deze studie onderzocht enerzijds het antibacteriële effect van het Endox Endodontic System®
(EES) op Enterococcus faecalis, in planktonische vorm en in biofilm. Anderzijds werd er
onderzocht of de gevoeligheid van E. faecalis voor natriumhypochloriet (NaOCl) toeneemt na
behandeling met EES.
Achtergrond:
Bij de wortelkanaalbehandeling is desinfectie van het wortelkanaal van cruciaal belang in de
preventie en genezing van apicale peridontitis. E. faecalis is het meest voorkomende micro-
organisme in reeds behandelde wortelkanalen en heeft enkele eigenschappen die eliminatie
met conventionele therapie bemoeilijken. Recent werden nieuwe technieken ontwikkeld, zoals
EES, gebaseerd op elektroporatie, om desinfectie van het wortelkanaal te optimaliseren.
Methodologie:
Het Endox Endodontic System®
(EES) (Lysis, Nova Milanese, Italy) wordt in een in vitro
opstelling, een aanpassing van het model van Cassanelli et al. (Cassanelli et al. 2008), getest.
Een 0.51mm orthodontische roestvrij staaldraad (TP orthodontics inc., USA) wordt aan de
negatieve pool van het toestel gekoppeld en past in een 100 µl pipettip, wat het wortelkanaal
nabootst. Het EES wordt in incisor mode + boost stand gezet, wat overeenkomt met een 140
ms pulse met een frequentie van 312.5 kHz en 1200 kV/m.
Als bacteriële cultuur werd een reincultuur van E. faecalis ATCC 10541 gebruikt met groei in
Tryptic Soy Broth (TSB) en overnachtincubatie op 37 °C. Vervolgens werd dit verdund in
fysiologische oplossing (NaCl 0.9%) tot werkoplossingen met een concentratie van 106- 10
7
CFU/ml.
Voor de experimenten met E. faecalis in planktonische vorm, werd eerst de sublethale dosis
van NaOCl bepaald: NaOCl 2.5% w/v (University Hospital Pharmacy, Ghent, Belgium) werd
verdund tot concentraties van 0.025% (w/v), 0.0025%, 0.00025% en 0.000025%. Vervolgens
werd 100µl van de bacteriële werkoplossing toegevoegd aan 10 ml van iedere bereide
concentratie NaOCl. Na één minuut contacttijd werd 1 ml van deze oplossing toegevoegd aan
9 ml Na2S2O3 (2.5%) voor de neutralisatie van NaOCl. Vervolgens werden verdunningen van
10-1
tot 10-5
geënt in TSB. Als tweede experiment werd het effect van EES op E.faecalis in
planktonische vorm onderzocht door 100µl bacteriële werkoplossing in een steriele pipettip te

26
pipetteren en te verbinden via de staaldraad met het Endoxtoestel. De positieve elektrode
werd in de oplossing gebracht en er werden 3 pulsen toegediend. Nadien werd de
werkoplossing uit de pipettip opgelost in 10 ml fysiologische oplossing en verdunningen van
10-1
tot 10-5
werden geënt in TSB. Als laatste experiment met E. faecalis in planktonische
vorm werd het effect van EES in combinatie met een subletale dosis van NaOCl onderzocht.
Hierbij werd 100µl werkoplossing in de pipettip gepipetteerd en zoals hierboven beschreven
werden 3 pulsen toegediend na aansluiting op het toestel. De inhoud van de pipettip werd
vervolgens toegevoegd aan 10 ml NaOCl (2.5x10-5
%) met een contacttijd van 1 min. Eén ml
van deze oplossing werd geneutraliseerd met 9 ml Na2S2O3 (2.5%). Vervolgens werden
verdunningen van 10-1
tot 10-5
geënt in TSB.
Voor de experimenten met E. faecalis in biofilm werd E. faecalis, geïnoculeerd in TSB en
overnacht geïncubeerd op 37°C. Na centrifugatie (4000 rpm, 4 min) werd de pellet opnieuw
in suspensie gebracht in verse TSB. Twaalf hydroxyapatietschijfjes (HA) (5 x 2 mm, Clarkson
Chromatography Products, South Williamsport, PA, USA) werden gesteriliseerd en in een 24-
well polystyrene microtitre plaat (TPP, Trasadingen, Switzerland) geplaatst. Iedere well werd
geïnoculeerd met 2 ml E. faecalis suspensie. Na 4u incubatie op 37 °C, werd de
inoculumvloeistof verwijderd en werd iedere well gespoeld met 1 ml TSB om non-adherente
cellen te verwijderen. Na toevoeging van 2 ml vers TSB in elke well, werd de plaat
geïncubeerd op 37°C. Om het effect van de incubatietijd op de biomassa te bepalen werd een
incubatietijd van 24u en 72u met elkaar vergeleken en werd 24u incubatietijd gekozen voor de
verdere experimenten. De HA-schijfjes werden willekeurig verdeeld over controle en
interventiegroep (n ≥ 9). Om het effect van EES op E. faecalis in biofilm te onderzoeken
werden HA-schijfjes in gelijke blokjes gesneden zodat ze in een pipettip pasten. Honderd
microliter fysiologische oplossing werd in de pipettip gepipetteerd waaraan een, zoals
hierboven beschreven, met biofilm bereid HA-plaatje werd toegevoegd. Dit werd verbonden
met het Endox toestel (cfr hierboven) en 3 of 6 pulses werden toegediend. De overlevende
adherente cellen werden nadien gecollecteerd door het HA-plaatje in 10ml TSB op te vangen
en nadien driemaal gedurende 30 seconden te vortexen in combinatie met 30 sec sonicatie
(Branson 3510, 42 kHz, 100 W, Branson Ultrasonics Corp.). Vervolgens werden seriële
verdunningen gemaakt (10-1
to 10-7
).
Eén ml van elke bacteriële verdunning werd uitgeplaat in een petrischaal met Tryptic Soy
Agar (TSA) en geïncubeerd op 37 °C gedurende minstens 48u. Het aantal CFU in de
onverdunde oplossing werd berekend en uitgedrukt als CFU/10ml voor de experimenten met
planktonische oplossing en CFU/plaat voor de biofilm experimenten. Gemiddelden en

27
standaarddeviaties werden berekend en na logaritmische transformatie werden de data
statistisch geanalyseerd met one-way ANOVA en t-test (PASW Statistics 18, SPSS Inc,
Chicago, IL).
Resultaten:
De subletale dosis van NaOCl voor E.faecalis was NaOCl 2.5x10-4
% en NaOCl 2.5x10-5
%
terwijl NaOCl 2.5x10-3
% letaal was. Omwille van een betere reproduceerbaarheid werd de
concentratie van NaOCl 2.5x10-5
% gekozen voor de verdere experimenten.
Het aantal CFU/ml van E. faecalis, in de experimenten met E.faecalis in planktonische vorm,
was niet significant verschillend tussen de 4 onderzochte groepen: namelijk, controlegroep,
groep behandeld met EES, groep behandeld met EES + NaOCl 2.5x10-5
% en groep
behandeld met NaOCl 2.5x10-5
% alleen (P = 0.12).
Biofilmexperimenten: Er was geen significant verschil in aantal bacteriën per disk tussen een
incubatietijd van 24u of 72 u (P = 0.86). Een incubatietijd van 24u werd in de verdere
experimenten gebruikt. Het effect van een behandeling met EES, zowel 3 als 6 pulses, op E.
faecalis in een biofilm was niet significant verschillend in vergelijking met de controlegroep
(P = 0.19).

28
Nabeschouwing
In deze studie werd het effect van het Endox Endodontic System®
(EES) onderzocht op E.
faecalis in planktonische vorm en in een biofilm. Daarbij werd eveneens nagekeken of EES
de gevoeligheid van planktonische E. faecalis voor NaOCl toeneemt. Als micro-organisme
werd E. faecalis onderzocht omdat dit micro-organisme enerzijds wordt teruggevonden in
wortelkanalen, geassocieerd met therapiefalen (Molander et al. 1998) en anderzijds
verschillende overlevingsstrategieën bezit om in ongunstige omstandigheden te overleven,
zoals resistentie tov een alkalische omgeving (Flahaut et al. 1997) en verminderde
voedingsstoffen (Hartke et al. 2002). Omwille van die reden werd het effect van verschillende
antibacteriële strategieën tegenover E. faecalis reeds meermaals onderzocht (Stuart et al.
2006). Echter, ondanks deze verschillende verdedigingsmechanismen, blijkt E. faecalis niet
weerstandig tegenover NaOCl, in concentraties zoals ze gebruikt worden in de
endodontologie (Retamozo et al. 2010). En toch wordt E. faecalis teruggevonden in
wortelkanalen, geassocieerd met therapiefalen (Molander et al. 1998, Portenier et al. 2003).
De complexe morfologie van het wortelkanaalsysteem biedt hiervoor een mogelijke
verklaring (Vertucci 1984, Fabricius 2006). Daarenboven vormen bacteriën een biofilm
wanneer ze in contact komen met een oppervlak, waardoor hun overlevingsmogelijkheden
toenemen (Costerton et al. 1987). Nieuwe behandelingsmethodes worden onderzocht om de
desinfectie van deze complexe structuur te optimaliseren (Meire et al. 2009).
Eén van deze nieuwe strategieën in de behandeling van de biofilm is het gebruik van
methodes gebaseerd op het principe van elektroporatie, zoals het Endox Endodontic System®
(EES). Hierbij wordt een kortdurende hoogvoltage puls (> 1kV) toegediend om poriën te
creëren in het celmembraan en zo de gevoeligheid voor chemische agentia te verhogen (Haas
& Aturaliye 1999). Cassanelli et al. (Cassanelli et al. 2008) onderzocht dit
elektroporatieprincipe met EES op planktonische E. coli en kon plasmide-transfer tussen 2 E.
coli stammen aantonen.
In deze studie vonden we geen significant effect wanneer E. faecalis in planktonische vorm,
werd behandeld met EES tov controle, noch wanneer EES werd gecombineerd met een
subletale dosis van NaOCl. Dit is in overeenstemming met een studie van Cassanelli et al.
(Cassanelli et al. 2008) waarbij E. faecalis werd behandeld met een high frequency alternating
current (HFAC) alleen of in combinatie met amikacine waarbij slechts beperkte reductie in
CFU/ml werd waargenomen. Dit in tegenstelling tot een ander deel van dezelfde studie

29
waarbij E. coli werd behandeld met HFAC alleen, HFAC in combinatie met vancomycine of
vancomycine alleen. Hierbij had vancomycine alleen geen effect en trad er na alleen HFAC
slechts een beperkte reductie van minder dan 2 log CFU/ml op. Er werd wel een additionele
reductie van 2-3 log CFU/ml waargenomen wanneer de stam naast HFAC ook werd
behandeld met vancomycine. (Cassanelli et al. 2008). Dit kan verklaard worden door
verschillende karakteristieken tussen Gram- positieve en Gram-negatieve bacteriën. Gram-
positieve bacteriën zoals bv. E. faecalis bezitten een dikke peptidoglycaanwand, die als een
fysische barrière fungeert.
In deze studie werd een subletale dosis NaOCl gebruikt, omdat we wilden nagaan of de
toediening van een elektrische stroom een toegevoegde waarde heeft aan chemische
desinfectie. Het werkingsmechanisme van NaOCl is tweeërlei: enerzijds verstoort de hoge pH
van NaOCl de membraanintegriteit, anderzijds wordt er hypochloorzuur (HOCl) gevormd
wanneer in contact met water. HOCl diffundeert vrij over het celmembraan en interfereert met
enzymatische processen van het energiemetabolisme en degradeert eveneens het
celmembraan. Er was geen significant verschil in reductie CFU/ml planktonisch E. faecalis
tussen controlegroep, de groep behandeld met een subletale dosis NaOCl alleen en deze die
behandeld werd met EES in combinatie met een subletale dosis NaOCl.
In het tweede deel van de studie werd het effect van EES op E. faecalis in biofilm in vitro
onderzocht. Deze biofilm werd gevormd op hydroxyapatiet (HA), waaruit dentine voor 70%
is opgebouwd. Aangezien er geen effect van EES werd vastgesteld op E. faecalis in suspensie
werden 3 en 6 pulsen met een controle vergeleken. Tussen de drie verschillende groepen was
er geen statistisch significante reductie in CFU/plaat E. faecalis. Hieruit kunnen we
vermoeden dat er in vivo evenmin onder de hier onderzochte omstandigheden een effect op
meer complexe biofilms zal zijn, zoals aanwezig in een geïnfecteerd wortelkanaal.
Het antibacteriële effect van EES werd in een klinische studie van Virtej et al. onderzocht. Ze
observeerden een reductie van ongeveer 10.000 tot 40.000 CFU na behandeling met EES. Dit
was echter inferieur aan andere desinfectiemethoden (Virtej et al. 2007).
In vitro kon in onze studie geen significante reductie in CFU/ml van E. faecalis in suspensie
worden aangetoond. Er zijn meerdere mogelijke verklaringen voor deze verschillende
bevindingen, enkele daarvan zijn: wij onderzochten een reincultuur en dienden slechts 3
pulsen toe. In de studie van Virtej et al. (Virtej et al. 2007) werd EES onderzocht op de totale

30
mondflora wat een „melting-pot‟ van micro-organismen en derhalve met verschillende
gevoeligheden. Er werden 6 ipv 3 pulsen toegediend.
Een voordeel van onze in vitro opstelling was dat onmiddellijke visualisatie van het medium
mogelijk was. Herpositionering van de elektrode was mogelijk indien nodig. Er werden
eveneens af en toe „flashes‟ (vuurflitsen) waargenomen. Het mechanisme hierachter is niet
helemaal duidelijk en mogelijks worden deze veroorzaakt door verschillen in geleiding en
impedantie in het wortelkanaal. Of dit verschijnsel veilig is voor het periradiculaire weefsel
en grotere cellen zoals bijvoorbeeld zenuwcellen is niet duidelijk (Lee & Kolodney 1987).
De heterogeniciteit aan resultaten die in de literatuur terug te vinden is in verband met de
werking en effecten van EES kan verklaard worden door de verschillende experimentele
designs en de variëteit aan onderzochte micro-organismen. (Haas & Aturaliye 1999;
Szuminsky et al. 1994, Lee et al. 2008). In deze studie werd het effect van EES op E. faecalis
onderzocht, een Gram-positieve bacterie met een dikke peptidoglycaanwand die weerstand
biedt aan hoge cytoplasmatische osmotische druk en barsten voorkomt.
Hoe dan ook wordt van een desinfectie-methode in de endodontologische setting verwacht dat
een zo breed mogelijk spectrum van micro-organismen wordt behandeld.

31
Conclusie
Binnen de beperkingen van deze in vitro studie kon geen antibacterieel effect aangetoond
worden van het Endox Endodontic System® op E. faecalis, in planktonische vorm of in
biofilm. De gevoeligheid van in suspensie voorkomende E. faecalis werd niet gemodificeerd
door behandeling met EES. De resultaten benadrukken het belang van het onderzoeken van
nieuwe behandelingsmethoden vóór het gebruik in de klinische praktijk.

32
Reference list
Bale MJ, Fry JC, Day MJ (1988) Transfer and occurrence of large mercury resistance
plasmids in river epilithon. Applied and Environmental Microbiology 54, 972-8.
Brito LC, Teles FR, Teles RP, França EC, Ribeiro-Sobrinho AP, Haffajee AD, Socransky SS
(2007) Use of multiple-displacement amplification and checkerboard DNA-DNA
hybridization to examine the microbiota of endodontic infections. Journal of Clinical
Microbiology 45, 3039-49.
Brown MR, Gilbert P (1993) Sensitivity of biofilms to antimicrobial agents. Journal of
Applied Microbiology 74, 87S-97S.
Buckley ND, Vadeboncoeur C, LeBlanc DJ, Lee LN, Frenette M (1999) An effective
strategy, applicable to Streptococcus salivarius and related bacteria, to enhance or
confer electroporation competence. Applied and Environmental Microbiology 65, 3800-4.
Cassanelli C, Marchese A, Cagnacci S, Debbia EA (2008) Alteration of Membrane
Permeability of Bacteria and Yeast by High Frequency Alternating Current (HFAC). The
Open Microbiology Journal 2, 32-7.
Chavez de Paz LE (2007) Redefining the persistent infection in root canals: possible role
of biofilm communities. Journal of Endodontics 33, 652-62.
Chávez de Paz LE, Bergenholtz G, Svensäter G (2010) The effects of antimicrobials on
endodontic biofilm bacteria. Journal of Endodontics 36, 70-7.
Costerton JW, Irvin RT, Cheng KJ (1981). The bacterial glycocalyx in nature and disease.
Annual Review of Microbiology 35, 299-324.
Costerton JW, Cheng KJ, Geesey GG, Ladd TI, Nickel JC, Dasgupta M, Marrie TJ (1987)
Bacterial biofilms in nature and disease. Annual Review of Microbiology 41, 435-64.

33
Distel JW, Hatton JF, Gillespie MJ (2008) Biofilm formation in medicated root canals.
Journal of Endodontics 28, 689-93.
Estrela C, Estrela CR, Barbin EL, Spanó JC, Marchesan MA, Pécora JD (2002) Mechanism of
action of sodium hypochlorite. Brazilian Dental Journal 13, 113-7.
European Society of Endodontology (2006) Quality guidelines for endodontic treatment:
consensus report of the European Society of Endodontology. International Endodontic
Journal 39, 921-30.
Evans M, Davies JK, Sundqvist G, Figdor D (2002) Mechanisms involved in the resistance of
Enterococcus faecalis to calcium hydroxide. International Endodontic Journal 35, 221-8.
Fabricius L, Dahlén G, Sundqvist G, Happonen RP, Möller AJ (2006) Influence of residual
bacteria on periapical tissue healing after chemomechanical treatment and root filling of
experimentally infected monkey teeth. European Journal of Oral Sciences 114, 278-85.
Perkins HR (1969) Composition of bacterial cell walls in relation to antibiotic action.
Advances in Pharmacology 7, 283-307.
Figdor D, Davis JK, Sundqvist G (2003) Starvation survival, growth and recovery of
Enterococcus faecalis in human serum. Oral Microbiology and Immunology 18, 234-9.
Flahaut S, Hartke A, Giard JC, Auffray Y (1997) Alkaline stress response in Enterococcus
faecalis: adaptation, cross-protection and changes in protein synthesis. Applied and
Environmental Microbiology 63, 812-4.
Haapasalo M, Shen Y, Qian W, Gao Y (2010) Irrigation in endodontics. Dental Clinics of
North America 54, 291-312.
Haas CN, Aturaliye D (1999) Semi-quantitative characterization of electroporation-
assisted disinfection processes for inactivation of Giardia and Cryptosporidium. Journal
of Applied Microbiology 86, 899-905.

34
Hartke A, Lemarinier S, Pichereau V, Auffray Y (2002) Survival of Enterococcus faecalis in
seawater microcosms is limited in the presence of bacterivorous zooflagellates. Current
Microbiology 44, 329-35.
Holo H, Nes IF. High-Frequency Transformation, by Electroporation, of Lactococcus lactis
subsp. cremoris Grown with Glycine in Osmotically Stabilized Media (1989) Applied and
Environmental Microbiology 55, 3119-23.
Hommez GM, Coppens CR, De Moor RJ (2005) Periapical health related to the quality of
coronal restorations and root fillings. International Endodontic Journal 35, 680-9.
Hubble TS, Hatton JF, Nallapareddy SR, Murray BE, Gillespie MJ (2003) Influence of
Enterococcus faecalis proteases and the collagen-binding protein, Ace, on adhesion to dentin.
Oral Microbiology and Immunology 18, 121-6.
Jiang LM, Hoogenkamp MA, van der Sluis LW, Wesselink PR , Crielaard W, Deng DM
(2011) Resazurin metabolism assay for root canal disinfectant evaluation on dual-species
biofilms. Journal of Endodontics 37, 31-5.
Kakehashi S, Stanley HR, Fitzgerald RJ (1965) The effects of surgical exposures of dental
pulps in germfree and conventional laboratory rats. Oral Surgery, Oral Medicine, Oral
Pathology 20, 340-9.
Kayaoglu G, Ørstavik D (2004) Virulence factors of Enterococcus faecalis: relationship to
endodontic disease. Critical Reviews in Oral Biology & Medicine 1, 308-20.
Kobayashi H, Murakami N, Unemoto T (1982) Regulation of the cytoplasmic pH in
Streptococcus faecalis. The Journal of Biological Chemistry 25, 13246-52.
Lee W, Lim S, Son HH, Bae KS (2004) Sonicated extract of Enterococcus faecalis induces
irreversible cell cycle arrest in phytohemagglutinin-activated human lymphocytes. Journal of
Endodontics 30, 209-12.

35
Lee MH, Han DW, Woo Yi, Uzawa M, Park JC (2008) Inactivation of Listeria
monocytogenes in brine and saline by alternating high-voltage pulsed current. Journal of
Microbiology and Biotechnology 18, 1274-7.
Lee RC, Kolodney MS (1987) Electrical injury mechanisms: electrical breakdown of cell
membranes. Plastic and Reconstructive Surgery 80, 672-9.
Lin S, Platner O, Metzger Z, Tsesis I (2008) Residual bacteria in root apices removed by a
diagonal root-end resection: a histopathological evaluation. International Endodontic Journal
41, 469-75.
Lendini M, Alemanno E, Migliaretti G, Berutti E (2005) The effect of high-frequency
electrical pulses on organic tissue in root canals. International Endodontic Journal 38, 531-8.
Lojewska Z, Farkas DL, Ehrenberg B, Loew LM (1989) Analysis of the effect of medium and
membrane conductance on the amplitude and kinetics of membrane potentials induced by
externally applied electric fields. Biophysical Journal 56, 121-8.
Love RM (2001) Enterococcus faecalis--a mechanism for its role in endodontic failure.
International Endodontic Journal 34, 399-405.
Meire MA, De Prijck K, Coenye T, Nelis HJ, De Moor RJ (2009) Effectiveness of different
laser systems to kill Enterococcus faecalis in aqueous suspension and in an infected tooth
model. International Endodontic Journal 42, 351-9.
Molander A, Reit C, Dahlén G, Kvist T (1998) Microbiological status of root-filled teeth with
apical periodontitis. International Endodontic Journal 31, 1-7.
Möller AJR (1966) Microbial examination of root canals and periapical tissues of human
teeth. Methodological Studies. PhD thesis, Göteborg. 151-3
Murray BE (1998) “Diversity among the multidrug-resistant enterococci” Emerging
Infectious Diseases 4, 46-65

36
Nair PN (2004) Pathogenesis of apical periodontitis and the causes of endodontic failures.
Critical Reviews in Oral Biology & Medicine 1, 348-81
Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PM (2006) The fundamental operating
principles of electronic root canal length measurement devices. International Endodontic
Journal 39, 595-609.
Neumann E, Schaefer-Ridder M, Wang Y, Hofschneider PH (1982) Gene transfer into mouse
lyoma cells by electroporation in high electric fields. European Molecular Biology
Organization Journal 1, 841-5.
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K (2007) Outcome of primary root canal
treatment: systematic review of the literature - part 1. Effects of study characteristics on
probability of success. International Endodontic Journal 40, 921-39
Perkins HR (1969) Composition of bacterial cell walls in relation to antibiotic action.
Advances in Pharmacology & Chemotherapy 7, 283-307.
Peters LB, Lindeboom JA, Elst ME, Wesselink PR (2011) Prevalence of apical periodontitis
relative to endodontic treatment in an adult Dutch population: a repeated cross-sectional
study. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology
111, 523-8.
Portenier I, Waltimo TMT, Haapasalo L (2003) Enterococcus faecalis – the root canal
survivor and „star‟ in post-treatment disease. Endodontic topics 6, 135-55.
Powell IB, Achen MG, Hillier AJ, Davidson BE (1988) A Simple and Rapid Method for
Genetic Transformation of Lactic Streptococci by Electroporation. Applied and
Environmental Microbiology 54, 655-660.
Retamozo B, Shabahang S, Johnson N, Aprecio RM, Torabinejad M (2010) Minimum contact
time and concentration of sodium hypochlorite required to eliminate Enterococcus faecalis.
Journal of Endodontics 36, 520-3.

37
Sjögren U, Figdor D, Persson S, Sundqvist G (1997) Influence of infection at the time of
rootfilling on the outcome of endodontic treatment of teeth with apical periodontitis.
International Endodontic Journal 30, 297-306
Stuart CH, Schwartz SA, Beeson TJ, Owatz CB (2006) Enterococcus faecalis: its role in root
canal treatment failure and current concepts in retreatment. Journal of Endodontics 32, 93-8.
Sundqvist G (1992) Associations between microbial species in dental root canal infections.
Oral Microbiology & Immunology 7, 257-62.
Sundqvist G, Figdor D, Persson S, Sjögren U (1998) Microbiologic analysis of teeth with
failed endodontic treatment and the outcome of conservative re-treatment. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology and Endodontology 85, 86-93.
Szuminsky NJ, Albers AC, Unger P, Eddy JG (1994) Effect of narrow, pulsed high voltages
on bacterial viability. Physical Therapy 74, 660-7.
Ushiyama J (1983) New principle and method for measuring the root canal length. Journal of
Endodontic 9, 97-104.
Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surgery, Oral
Medicine, Oral Pathology 58, 589-99.
Virtej A, MacKenzie CR, Raab WH, Pfeffer K, Barthel CR (2007) Determination of the
performance of various root canal disinfection methods after in situ carriage. Journal of
Endodontics 33, 926-9.
Weaver JC (1993) Electroporation: a general phenomenon for manipulating cells and tissues.
Journal of Cellular Biochemistry 51, 426-35.
Wu VC (2008) A review of microbial injury and recovery methods in food.
Food Microbiology 25, 735-44.

38
Zehnder M (2006) Root canal irrigants. Journal of Endodontics 32, 389-98.