apoio à decisão em medicina intensiva usando ecbd pedro gago – i p leiria
TRANSCRIPT
Apoio à decisão em medicina intensiva usando
ECBD
Pedro Gago – I P Leiria

2
Intensive care
• About 250 variables are needed to describe an ICU patient
• Humans are unable to cope with more than seven variables at a time

3
Objectives
• Assist ICU doctors by providing accurate and timely predictions for:– the final outcome
– organ dysfunction or failure
• Must overcome natural physician resistance

4
Intensive Care Medicine
• Condition is severe to the point where it is very difficult for doctors to assess the patient’s state
• Objective is to stabilize in order to allow transfer to other units
• Highly invasive and very costly

5
Intensive Care Medicine
• Data from bed-side monitors may contain useful information
• Presently such data is not stored

6
Practical Issues
• Some variables values must be collected manually– Urine output
• Data Quality– Errors caused by human intervention
– Sensor malfunctions

7
Scores in use
• SAPS – indicative of the patient’s condition severity
• The worst values the first 24 hours of stay in the ICU are collected and the score is calculated

8
Scores in use (2)
• SOFA – measures organ dysfuntion/failure (worst daily values)
– Cardiovascular, hepatic, central nervous system, respiratory, renal, coagulation
• Worst daily values
• Indicative of patient’s condition evolution

9
INTCare
• Decision Support System to assist ICU doctors
• Uses available data in order to predict outcome and organ dysfunction/failure
• Not intended to replace doctors

10
INTCare (2)
• Semi-autonomous – updates its models as new data arrives
• Performance expected to improve with time
• Better results through the use of real time data

11
Architecture
PredictionAgent
Data MiningAgent
Heart RateO2 Sat.
Blood Pr.
ClinicalData
ModelInitialization
Agent
ClinicalData Entry
Agent
PerformanceData
InterfaceAgent
Dataacquisition
MonitoredData
Scenarios
ScenarioEvaluation
Agent
DataRetrieval
Agent
Bedside monitors
DATA ENTRY
KNOWLEDGE MANAGEMENT
INTERFACE
DataWarehouse
INFERENCE
SAPSSOFA
AdmissionDischarge
Physiologicaldata
Pre-processing
Agent
PerformanceAgent
KnowledgeBase
(PMML)

12
Architecture (2)
PredictionAgent
Data MiningAgent
Heart RateO2 Sat.
Blood Pr.
ClinicalData
ModelInitialization
Agent
ClinicalData Entry
Agent
PerformanceData
InterfaceAgent
Dataacquisition
MonitoredData
Scenarios
ScenarioEvaluation
Agent
DataRetrieval
Agent
Bedside monitors
DATA ENTRY
KNOWLEDGE MANAGEMENT
INTERFACE
DataWarehouse
INFERENCE
SAPSSOFA
AdmissionDischarge
Physiologicaldata
Pre-processing
Agent
EnsembleAgent
PerformanceAgent
KnowledgeBase
(PMML)

13
EURICOS II
• Data from 42 UCI from 9 countries
• 10 months (1998 and 1999)

14
EURICOS II (2)
• Data available includes:
– case mix (age, origin, etc)
– SAPS score
– daily SOFA scores
– intermediate outcomes
– final outcome
15
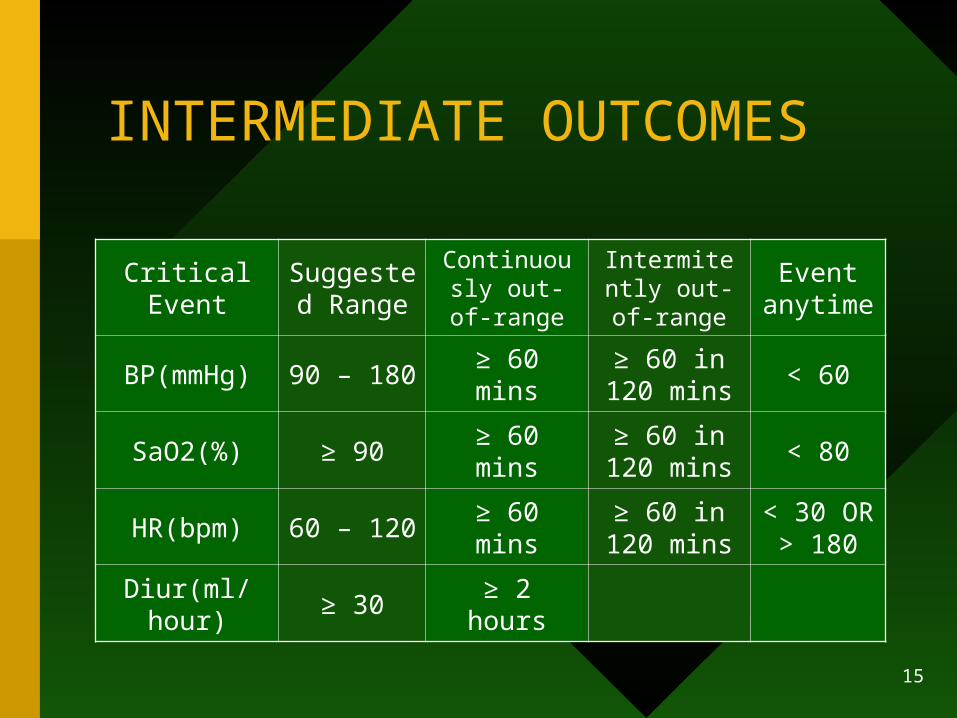
INTERMEDIATE OUTCOMES
Critical EventSuggested
RangeContinuously out-of-range
Intermitently out-of-range
Event anytime
BP(mmHg) 90 – 180 ≥ 60 mins≥ 60 in 120
mins< 60
SaO2(%) ≥ 90 ≥ 60 mins≥ 60 in 120
mins< 80
HR(bpm) 60 – 120 ≥ 60 mins≥ 60 in 120
mins< 30 OR
> 180
Diur(ml/hour) ≥ 30 ≥ 2 hours

16
Ensemble
• Training– Each model is trained on different subsets of the dataset
– Each variable has a 70% chance of being selected
– Starts with equal weights

17
Ensemble
• Evolution– Results from batches of records
– Weight adjustments according to individual model performance
– Worst performing models are deleted from the ensemble
– New models are trained using the most recent data and included in the ensemble

18
Ensemble
• Preliminary results (evolution doesn’t include new models)
– Ensemble trained with all cases still outperforms ensemble trained with less cases followed by weight adjustment
– Both outperform best individual model

19
Future Work
• Greater volume of data – deployment in other ICUs
• Reduce prediction window (next 6 hours instead of next day)
• Suggest course of action (must be delayed until physician resistance is lowered)
