blister aneurysms- evolution of endovascular management
TRANSCRIPT

Vipul GuptaNeurointerventional SurgeryArtemis Agrim Institute of Neurosciences

Blister aneurysms …
Classical ICA blister aneurysms Dissecting aneurysm with a bleb Very small berry aneurysms

Small Blister/dissecting…
“Very small, friable, symptomatic” Blister aneurysms (BA) are rare lesions characterized by a
hemispherical shape and fragile walls Non-branching sites from the dorsomedial wall of the
internal carotid artery (ICA), anterior communicating (AComA) and basilar artery …
Small size & atypical location- RA & 3D needed Blister/disecting- rapid change in size and morphology in
follow-up angiograms
Owaga A et al , Neurosurgery 2000;47:578
Meling TR et al J Neurosurg 2008;108:662
Sim SY et al J Neurosurg 2006;105:400

Management…
Pathology - focal wall defects covered by a thin layer of fibrous tissue and adventitia and lack of usual collagenous layerSurgical Options - Direct clipping, clipping plus wrapping, wrapping alone, clipping with Sundt encircling graft clips, encircling silicone clip application, primary suturing of ICA, vascular staple clip closure of ICA and trapping with or without extracranial-intracranial bypass
High risk of premature rupture during surgery, large lacerationsEndovascular- difficult to coil, friable, continued growth, stent needed (issues in SAH)Shikawa T, Neurosurgery 1997;40:403Lee BH et al J Neurosurg 2008

Issue- blister; control- protamine, coils

Stents
Flow modification Intimal growth and healing Change of angles
Issues Persistent fillingAnti-platelet therapy in SAHSingle/double/flow divertor

Classical blister aneurysm
34-year M, SAH


Stent …

Further evolution – flow diverters (stents)
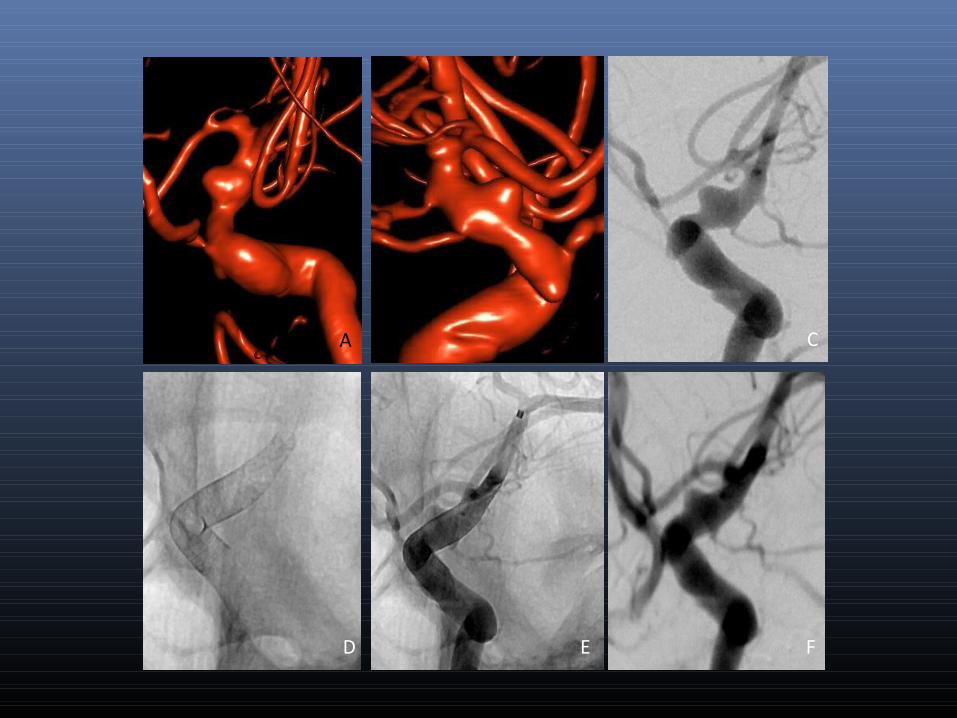
D E F
B CA B

B
C D
A


21/12/15
24/12/15

17 patients: SS, ODS, SS+Coil 1 rebleed (died)Good outcome on f/u – 82%Mortality – 18%
Blister Aneurysm
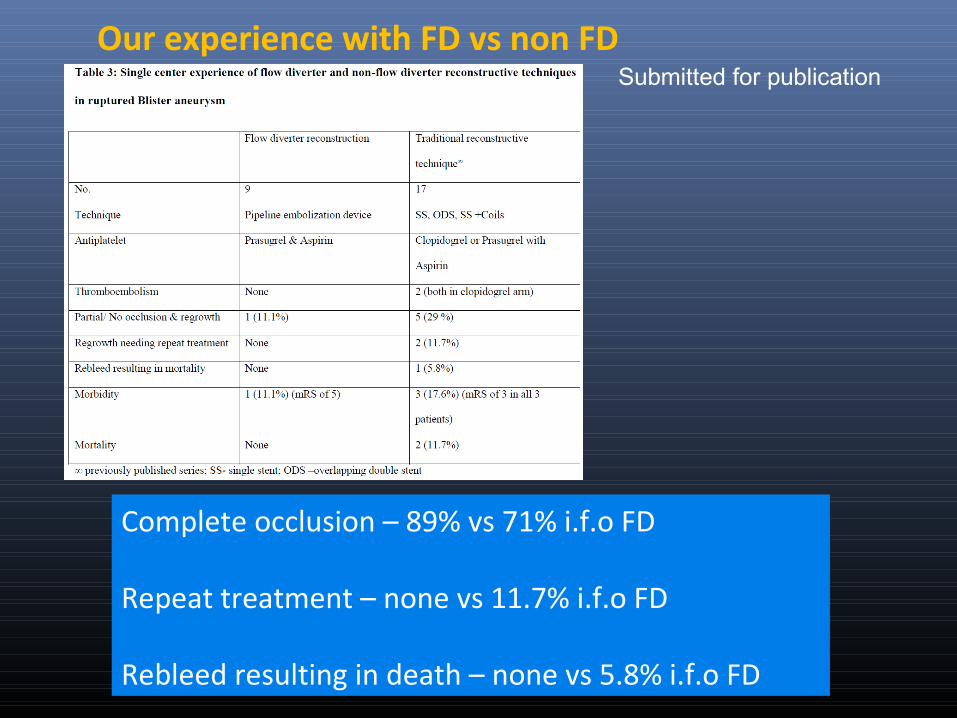
Our experience with FD vs non FD
Complete occlusion – 89% vs 71% i.f.o FD
Repeat treatment – none vs 11.7% i.f.o FD
Rebleed resulting in death – none vs 5.8% i.f.o FD
Submitted for publication

Learning points
• FD was safe and effective in these aneurysms and compared favorably with our previously reported results with stent(single/overlapping) and coiling
• In our series loading with Pasugrel and ecospirin was safe and effective for flow diverter placement in acutely ruptured blister aneurysms
Antiplatelet protocol: 2 hrs prior to stent deploymentEcosprin 150 mg & Prasugrel 50 mg
Heparin 3000 IU at start of procedure1000 IU to 2000 IU prior to stent deploymentACT 300 (x 2 upper limit of normal)

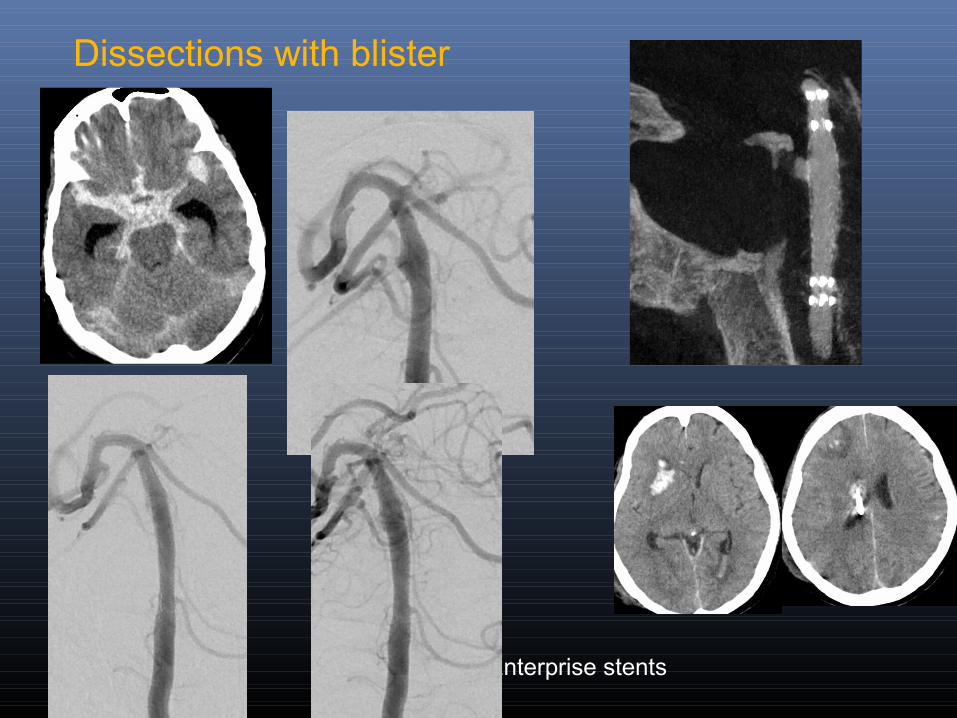
Dissections with blister EVD
2-overlapping Enterprise stents

A B C
D E F



Very small aneurysms …

Dissecting blister aneurysm – poor gradeEVD
2-overlapping Enterprise stents
Blister/dissecting aneurysms


Small blister/dissecting
Small blister/dissecting- important to detect and recognize
Difficult cases for surgery or endovascular Previous Options- single stent, overlapping
stents, stent and coil Current TOC in ICA – FD Careful anti-platelet protocol Distinguish between blister vs dissecting vs
very small berry

For more information on:STROKE & NEUROVASCULAR INTERVENTIONS:
URL:www.sanif.co.in
Facebook:https://www.facebook.com/strokeawarenessindiahttps://www.facebook.com/vipul.gupta.35175
Twitterhttps://twitter.com/drvipulgupta25
LinkedINhttps://in.linkedin.com/pub/dr-vipul-gupta/51/8a1/25a
YouTubeChannel: Stroke & Neurovascular Interventionswww.youtube.com/c/StrokeNeurovascularInterventionsfoundation
Dr Vipul Gupta

Thank you ….