capacitation-ivm culture of oocytes from small follicles in pcos...
TRANSCRIPT

Capacitation-IVM culture
of oocytes from small follicles
in PCOS patients
Johan Smitz & IVM Team
Follicle Biology Laboratory
Center for Reproductive Medicine
Vrije Universiteit Brussel (VUB)
Brussels , Belgium

Conflict of interest declaration
Speaker fees from :
BioMérieux,
Besins Female Healthcare,
Ferring Pharmaceuticals,
Merck

LEARNING OBJECTIVES
Acquire knowledge on :
- oocyte development in small human follicles
- oocyte Maturation in-vitro (IVM) :
recent developments
- improved method for clinical IVM :
CAPACITATION – IVM (“CAPA”)

IVM : what is it ?
DEFINITION
- is NOT a truncated IVF
- is NOT ‘rest’ material from IVF
DeVos et al. Human
Reproduction, 2016

SELECTION
PROCESS
Gougeon A. Human Reproduction 1986;2:81 - 87.
HUMAN FOLLICLE DEVELOPMENT
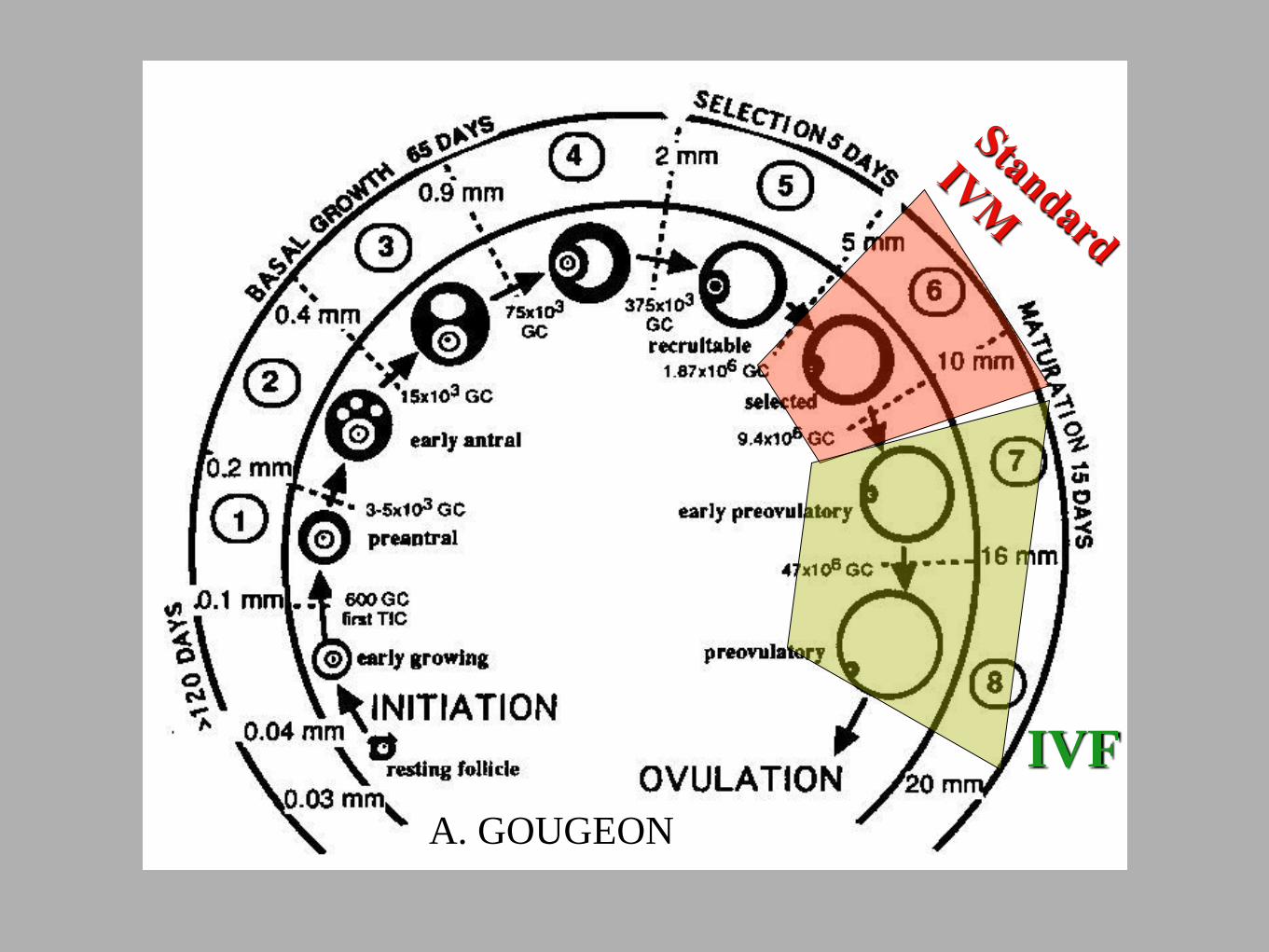
A. GOUGEON
IVF

Why IVM systems stay under-utilised
1- FOLLICLE HETEROGENEITY
the HCG injection on 6-12 mm follicles
causes asynchronous maturation of oocytes
2 - INAPPROPRIATE SIGNALLING is
induced “spontaneous” vs “induced” meiosis
re-initiation

Effect of hCG triggering in IVM
( Son et al., RBM Online 2008 )
compact cumulus
expanded
cumulus
GV
GV
MI
MII
PR 23,3%
PR 40%
Post HCG = In vivo + in vitro
maturation
Type of cumulus-oocytes obtained and OUTCOME
NOTE :
What the data show on “+hCG” - IVM
Generally low implantation rates
Increased early pregnancy loss
Need for multiple ET(2-4 Embryos)
Results: hesitant adoption by clinics

IVM and assessment of
oocyte/embryo quality
Property In vivo maturation In vitro maturation
Transcriptional
silencing Complete Leaky
Maternal RNA
processed Complete Partial
Metabolic loading Maximal Partial
Gap junctional comm. Maintained Retracted
Ca stores Maximal Partial
Pace of progression Slow Fast
Meiotic progression Complete Incomplete
D. Albertini, 2nd Biogenesi Conference, 2010
SMALL Follicle LARGE Follicle

How to IMPROVE
1- FOLLICLE HETEROGENEITY
the HCG injection on 6-12 mm follicles
causes asynchronous maturation of oocytes
2 - INAPPROPRIATE SIGNALLING is
induced “spontaneous” vs “induced” meiosis
re-initiation
Positive stimulus

HOW TO IMPROVE ?
Use a system inspired from animal production
Better exploit the small (2-8 mm) follicles ? Learn about
Gamete competences
Receptors expression
Signalling cascades

FIVE KEY STEPS TO IMPROVE IVM
ABANDON HCG INJECTION
GIVE FSH or HP-hMG PRIMING: 2-3 DAYS
USE DEFINED CULTURE MEDIA, NO SERUM
APPLY POSITIVE IN-VITRO MATURATION STIMULUS
PRE – MATURATION ( “CAPACITATION“ ) CULTURE

AVOID HCG to FOSTER CUMULUS- OOCYTE COMMUNICATION

POTENTIAL of CAPACITATION-IVM versus Standard of Care
Sanchez et al.,2017 HR
100
79
62
50
32
25
100
70
53
43
23
18
100
48
31
23
14
8
COCs MII 2PN GQED3 ED3 Q1-top quality
Blastocysts D5-D6
ICSI (PCOS, n=97)
CAPA (n=15)
Standard IVM (n=15)
TRANSFERABLE BLASTOCYSTS OBTAINED
PER 100 COC ( sibling oocytes )
‘stimulated ICSI’ CAPA-IVM“NEW” STANDARD IVM

OOCYTE PHYSIOLOGY : ‘flash’ REVIEW
1- In the small antral follicle (2-8 mm) the
oocyte is actively kept under meiotic arrest
what are the main mechanisms ?
2- By LH rise: meiosis reinitiation and
cumulus expansion ?
what are the prerequisite conditions ?

MEIOTIC ARREST
Regulation
cAMP
ATP
AC
5’AMP
ATP
AC
5’AMP
cAMP

LH ACTIVATES THE EGF- LIKE SYSTEM ESSENTIAL TO OOCYTE MATURATION
Theca
cells
Mural granulosa
cells BM
Cumulus
cells
Oocyte
LH PDE3A
cAMP
Gs
LHR GPR3 / GPR12
PDE4D
PDE4D
BM: basal membrane; hCG: human chorionic gonadotropin; LH: luteinising hormone; EGF: epidermal growth factor; EGFR: epidermal growth factor receptor; LHCGR: lutropin-
choriogonadotropic hormone receptor; PDE4E, Phosphodiesterase 4E; PDE3A, Phosphodiesterase 3A; AC, adenylyl cyclase.
Conti et al. Mol Endocrinol 2006;20:715–723
EGFR
LHCGR
AC3/9
Epi
AR
BTC
EGF-LIKE
FACTORS
OOCYTE SECRETED
FACTORS (OSF)
CUM GDF-9 FGF2 BMP15
GONADOTROPHINS

A. GOUGEON
Is Nuclear
Maturation
completed ?
FSH-R
POSITIVE
Stimulus
PRIMARY IMPRINTS
EGF-Like ?
EGF-R ?
PCO OVARY

PICK-UP of SMALL ( 2-8 mm) Follicles
from PCOS
When COC are detached from the follicle wall
1- essential receptor systems and growth factors are not yet fully functional
2- meiosis inhibition is missing in simple media

NON-hCG IVM : Characterising GV stage oocyte from 2 to 6 mm follicles ( = 70% of harvest )
96 98 100
102
104
106
108
110
112
114
116
118
120
122
124
0
4
8
12
16
20
24
28
Diameter (µm)
Nu
mb
er o
f o
oc
yte
s
ControlA Meiotically incompetent
94 96 98 100
102
104
106
108
110
112
114
116
118
120
0
10
20
30
40
50
60
70
Diameter (µm)
Nu
mb
er o
f o
oc
yte
s
N = 293
B
C D<105µm' ≥105'and'<110µm' ≥110µm'
4" 19" 84"
3,7%" 17,8%" 78,5%"
<105µm' ≥105'and'<110µm' ≥110µm'
32# 98# 163#
10,9%# 33,4%# 55,6%#
Dispersed(%)
Intermediate(%)
Condensed(%)
Controlsmall <105µm 3(75) 0 1(25)
medium ≥105<110µm 3(27.3) 3(27.3) 5(45.5)large ≥110µm 20(31.3) 10(15.6) 34(53.1)
Total(N=79) 26(32.9) 13(16.5) 40(50.6)
Meioicallyincompetent
small <105µm 17(65.4) 6(23.1) 3(11.5)medium ≥105<110µm 46(59.7) 21(27.3) 10(13.0)
large ≥110µm 49(38.0) 51(39.5) 29(22.5)
Total(N=232) 112(48.3) 78(33.6) 42(18.1)
Chromatinconfiguration
Mean (n=107) 112,6 ± 5,1 µm
Diameter of immature
oocytes before IVM
Chromatin configuration in
immature oocytes before
IVM
Dispersed Intermediate CondensedDispersed Intermediate CondensedDispersed Intermediate Condensed
96 98 100
102
104
106
108
110
112
114
116
118
120
122
124
0
4
8
12
16
20
24
28
Diameter (µm)
Nu
mb
er o
f o
oc
yte
sControlA Meiotically incompetent
94 96 98 100
102
104
106
108
110
112
114
116
118
120
0
10
20
30
40
50
60
70
Diameter (µm)
Nu
mb
er o
f o
oc
yte
s
N = 293
B
C D<105µm' ≥105'and'<110µm' ≥110µm'
4" 19" 84"
3,7%" 17,8%" 78,5%"
<105µm' ≥105'and'<110µm' ≥110µm'
32# 98# 163#
10,9%# 33,4%# 55,6%#SANCHEZ et al. Human
Reproduction, 2015 TRANSCRIPTIONAL
SILENCING Variable Stage

STANDARD IVM
CAPACITATION + IVM
•Works for COCs from follicle Ø
diameter ≥ 8 mm
•STANDARD IVM METHODS are
not focused on increasing
oocyte competence
•COC from 2-6 mm follicles
require capacitation before
IVM
•Tailor capacitation time to
follicle size (24–48 hours)
•HYPOTHESIS :
“CAPACITATION CULTURE”
o ENHANCES MATURATION
POTENTIAL
o INCREASES THE BLASTOCYST
YIELD
Ø : Average
CAPACITATION (CAPA) culture
Can IMPROVE IVM from smaller follicles

Improve maturation
by a 2-STEP CULTURE
STEP 1 : actively inhibit the immediate GVBD STEP 2 : administer the positive maturation trigger
By keeping up cAMP in COC :
persistent communication between cumulus -
oocyte leading to a slower GVBD : this results in
an increased oocyte developmental capacity.
TRANSLATIONAL RESEARCH
- Luciano (2002) - bovine
- Rebecca Thomas & Rob Gilchrist (2003)- bovine
- Kawashima (2008) - pig
- Daniela Nogueira (2004)- mouse – human

OPTIONS TO CONTROL MEIOTIC ARREST
CAPA SPOM
CNP
(Pre-IVM)
ZHANG M LUCIANO AM (2011)
Gilchrist RB and Thompson J, 20062
CNP
OSF
1. Gilchrist RB et al. Reproduction 2016;152:R143–R157; 2. Gilchrist RB and Thompson JG. Theriogen 2006; 67:6–15; 3.
2. Zhang M et al. Endo 2010;152:4377-4385
C-TYPE NATRIURETIC PEPTIDE PDE- INHIBITORS

CAPA- IVM TREATMENT SCHEME
shortened CLINICAL PART reduced monitoring and drugs cost
OPU

IN VITRO STUDY :
Capacitation and Maturation Culture
Meiosis
Stimulators
EGF-LIKE
Natural Meiotic inhibitors
•C-type Natriuretic Peptide
GV GV
CAPACITATION culture
24 or 48 hrs
AT RETRIEVAL AFTER PRE-MATURATION
Physiological level of essential components
growth factors – anti-oxydants – GSH …
PB
IVM
AFTER IVM
After EXPANSION
ICSI
2-8 mm Follicles

CAPACITATION-IVM compared to STANDARD IVM
LABORATORY PART
CAPA
system
OPU Pre-IVM IVM
Standard
IVM
IVM
30h
OPU
IVM Patients (sibling oocyte study):
women with PCOS; personalized
stimulation 3/4x225-150-75IU hMG,
OPU 42h after last hMG
At retrieval Post CAPA Post CAPA-IVM
ICSI
Embryo
culture till D3
or blastocyst
stage (D5 or
6)
Embryo culture
till blastocyst
stage (D5 or 6) Vitrification
Vitrification
and / or ET
NGS:
SAFETY DATA
Ploidy
methylation
30h (24-46h)
CONTROL :

Cooperation with Prof Gavin Kelsey
The Babraham Institute, Cambridge
12 conventional ICSI
20 CAPA-IVM / ICSI
• Day 5 or 6 Day 6
• Good quality blastocysts (BL3, BL4; AA, AB, BA, BB)
DNA methylation analysis by PBAT (post-bisulfite adaptor tagging) in single
blastocysts
Methylation data were compared to Okae et al, 2014 : (deeply
sequenced pool of 80 human blastocysts)
Whole genome methylation analysis in human blastocysts derived from CAPA-IVM

Global methylation variation in human
blastocysts was NOT affected by
• Type of ART: CAPA-IVM vs ICSI
• Culture medium
• Sex of the embryo
• Day 5 or Day 6 culture
• Blastocyst expansion grade (BL3/BL4)

CLINICAL DEVELOPMENT OF IVM
RESULTS CAPACITATION-IVM
by 2018
5 Pilot Studies
169 PCOS Patients
Brussels @ UZbrussel (Profs Devos M & Anckaert E ) : Safety DATA
Hoshiminh@ MyDuc ( Profs Lan Vuong & Manh Tuong ) : RCT
Osaka @ IVF Japan (Profs Morimoto & Fukuda ) : Application

Total Patients Patients COC MII% Total Available
N with ET Day 3 Embryon Transferred
Embryos
Implantations
(number of sacs)%
Ongoing
Pregnancy% Deliveries
Total
Babies
STD-IVM 40 33 653 48 141 67 19 28% * 12 9 11
2,0 ** 36%
Per patient data 16,3 7,8 3,5
CAPA-IVM 40 37 723 63 176 78 31 40% * 19 16 22
2,1 ** 51%
Per patient data 18,1 11,4 4,4
* Per Transferred Embryos (Total embryos transferred)
** Per Embryo Transfer (All patients with embryo transfer)
UPDATED TILL 07-09-18First ET cycle
CLINICAL OUTCOME
RCT CAPA-IVM vs. STANDARD IVM combined with
FREEZE ALL and ET D3
Only DATA of FIRST frozen DAY-3 EMBRYO TRANSFER
G. Griesinger 2015
Calculation of IMPLANTATION rate
CONFIDENTIAL PRELIMINARY DATA VUB and MyDuc
Unpublished data confidential

SUMMARY IMPLANTATION RATE from Fresh vs VITRIFIED DAY 3 EMBRYOS
RCT´s – Vietnam NO HCG
Lan et al 2018 + HCG
Cohen et al 2018 +HCG
TRANSFER TYPE
STD IVM Vitrif N=33
CAPA-IVM Vitrif N=37
FRESH N=823
Vitrified N=50
FRESH N=263
Vitrified N=51
IR (%) 28% 40% 25% 21% 14% 4%
Unpublished data confidential

Infertility treatment in PCOS :
conventional approach
CURRENT TREATMENT
• Lifestyle intervention
• First line therapy: - clomiphene or letrozole
• Second line therapy:
- gonadotrophins
- laparoscopic surgery (drilling)
• If additional infertility factors: IVF/ICSI
- GnRH antagonist / Agonist stimulus in
hyperandrogenic anovulatory PCOS
RESULTS / COMPLICATIONS
• Ovulation in 80%
• Pregnancy in 35 %
• Multiples : 10%
• Pregnancy in 20% per cycle
• Cancelled for Risk : 10-30%
• Multiples : 15-25%
• OHSS developed : 5-10%
• cum birth rate 58% ( 3 cy )
• OHSS : few (GnRHa trigger)
• Discomfort : high
• Multiples : 11-30 %
(Balen et al., HRU 2016 ; Molenaer et al , 2016)

NEW APPROACH PCOS
•Lifestyle intervention
•First line therapy: - clomiphene or letrozole
• Second line therapy:
CAPA – IVM : no HCG Single eFET
RESULTS versus
COMPLICATIONS
Ovulation in 80%
Pregnancy in 35 %
Multiples : 10%
Short treatment
Zero multiples
short time to pregnancy
Treatment of PCOS in 2018 : CAPA-IVM

CONCLUSIONS
• IVM is the only ART that totally excludes OHSS
• IVM reduces burden and cost for the patient
• GV oocytes from 2-6 mm follicles from PCOS patients can reach full
developmental capacity after capacitation culture (“CAPA”)
• CAPA-IVM increases the number of embryos per oocyte pick–up (4-5)
• CAPA- IVM embryos are chromosomally and epigenetically normal
• High implantation rates (40%) from vitrified/warmed Capa-IVM embryos
• Healthy children born (N=30) from CAPA-IVM in JAPAN and VIETNAM

ACKNOWLEDGEMENTS
Funding
- Fund For Research Flanders (FWO)
- Fund for Innovation in Technology (IWT)
- Free University Brussels (VUB)
Vrije Universiteit
Brussel (VUB)
Michel De Vos
Ellen Anckaert
Flor Sanchez
Sergio Romero
Heidi Van Ranst
Francesca Lolicato
Nurses, embryologists
&medical staff of CRG
at UZBRUSSEL
Jeremy Thompson
David Mottershead
SPRH, Robinson
Institute, University of
Adelaide
NSWU ( Sidney )
Rob Gilchrist
National University
Vietnam
MyDuc Hospital (
Hochiminh City )
Vuong Thi Ngoc Lan
Ho Manh Tuong
Le Hoang Anh
Ma Pham Que Mai
Nurses, embryologists
IVF JAPAN GROUP
IVF OSAKA
Yoshiharu Morimoto
Isaku Fukuda
Nurses, embryologists
And medical staff at IVF
Japan

3.9 2.2
RESULTS: EMBRYOLOGY
STD
CAPA
60%
51%
At oocyte Retrieval
Post CAPA 24h
Post IVM 32h
CAPA-IVM System

CNP – ARREST :
ADVANTAGES of CAPA for
the embryology laboratory
PHYSIOLOGICAL ARREST BY NATURAL PEPTIDE
• NO CHEMICAL SUBSTANCES NEEDED
AFTER CAPA CULTURE
POSITIVE MEIOTIC TRIGGER • Gives max MII at 30 hrs • Allows SINGLE SPERM
INJECTION TIME
COC CAPACITATION TIME WINDOW
• SHIFTS e-LAB ACTIVITIES
WITHIN NORMAL WORK HOURS