complications of laparoscopic surgery for diverticulitis bradley r. davis, md, facs, fascrs...
TRANSCRIPT

Complications of Laparoscopic Surgery for
DiverticulitisBradley R. Davis, MD, FACS, FASCRS
Associate Professor of Surgery
University of Cincinnati

Disclosures
• Paid Consultant for Ethicon Endo Inc.

Diverticulosis
Prevalence USA• < 40 years old - 5%• >50 years old - 35%• >85 years old - 65%

Laparoscopic Resection for Diverticulitis
Diverticulitis
• benign disease
• relatively common
• technically challenging
• numerous studies

Diverticulitis
• Changing paradigms on when to offer elective resection– 4 episodes of uncomplicated disease– Fistula– Stricture– Persistent symptoms/phlegmon
• The days of a “chip shot” sigmoid colectomy are ending/over

Laparoscopy for Diverticulitis
• More than 100 studies published• Most single institution noncomparative• All comparative studies demonstrate:
– Longer operative times - 30-60 minutes– Quicker return of bowel function - 1-2 days– Shorter hospital stay - 2-7 days

Laparoscopy for Diverticulitis
• Large National US Database– 1998-2000 Nationwide Inpatient Samples– 709 (3.8%) laparoscopic sigmoid resections– 17735 (96%) open sigmoid resections
• Shorter mean LOS - 7.5 vs. 9.4 days• Fewer complications - 20% vs. 29%• More pts d/c to home - 91% vs. 71%
Guller, Arch Surg 2003;138:1179

Diverticulitis
Noel, JK et al. J Am Coll Surg. 2007 Feb;204(2):291-307

Colorectal Residents% Laparoscopic Resections
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 20050
5
10
15
20
25
30
35
40
45
50
Diverticulitis
Colon Cancer
LAR
IC Crohn's
IPAA
Schoetz, JACS, September 2006

Laparoscopy vs. Open
Gervaz et al. Ann Surg 2010
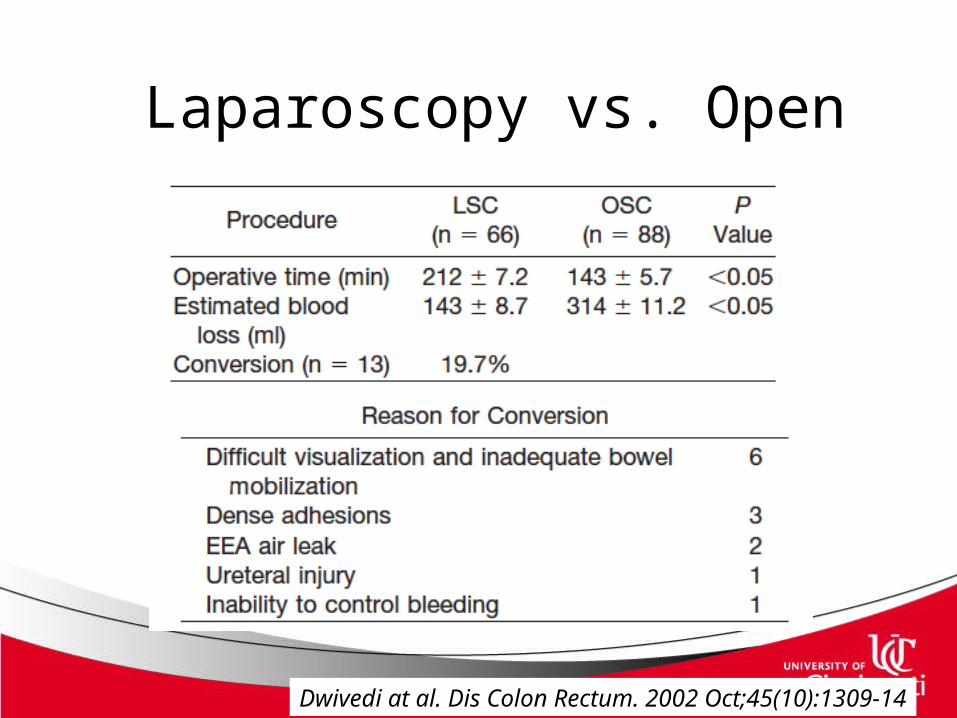
Laparoscopy vs. Open
Dwivedi at al. Dis Colon Rectum. 2002 Oct;45(10):1309-14

Laparoscopy vs. Open
Dwivedi at al. Dis Colon Rectum. 2002 Oct;45(10):1309-14

Factors Effecting Outcomes
• Complicated vs Uncomplicated– Fistula– Stenosis– Diverticulitis vs diverticulosis
• Experience – high volume vs low volume

Conversions
LeMoine et al. Br J Surg. 2003


Experience
Scheidbach et al. Dis Col Rect 2004

Experience
Jones et al. Ann Surg. 2008
Diverticulitis
• Increasing experience with the acute management of perforated diverticulitis– Laparoscopic washout and drainage– Laparoscopic Hartmann’s Procedure– Laparoscopic resection with anastomosis

Acute Diverticulitis
• 68 Patients– Hinchey I: 27– HincheyII: 29– Hinchey III: 7
• 16 Concurrent fistula• 8 Phlegmons
Titu at al. Colorectal Dis. 2009

Acute Diverticulitis
• Median OR time: 110mins (45-195)
• One Conversion
• Postoperative Mortality: 3.3%
• LOS: 5 days
Titu at al. Colorectal Dis. 2009

Laparoscopic Colectomy:Mastering the Complex Case• Set it up right• Start from known – work both sides of
the phlegmon• Put in right ports• Alternate
– Go open– Change extraction site– The approach – medial vs. lateral

Alternate Approach –Perf Tic
• Medial• Good technique
– Traction– Set it up– Help your partner– Set the clock

Alternate Approach –Perf Tic
• Lateral• Good technique
– Traction– Set it up– Stay in the plane– Watch the smoke– Stay oriented– Set the clock

Alternate Approach –Perf Tic
• Lateral• Good technique
– Traction– Set it up– Stay in the plane– Watch the smoke– Stay oriented– Set the clock

Laparoscopic Colectomy:Mastering the Complex Case
• Alternate– Go open– Change extraction site– The approach – medial vs. lateral– The technique – put in a hand

Alternate - Extraction Site
• Midline– Easier to convert– Easier to perform
– Limited open exposure
• Pfannenstiel– Difficult to convert– Good access for HAL– Good exposure to
pelvis
– Difficult to perform especially small incision


Optimize Chances
• Ureteral catheters +/-• Hand Assisted through pfannestiel
– dissection and anastomosis “open” – deal with air leak, phlegmon
• Mobilize flexure• Resect to normal feeling colon to rectum

Ureteral Catheters
Wexner et al. Tech Coloproctol. 2008 Mar;12(1):45-50

Complicated Diverticulitis:Alternatives to Conversion
• Pfannenstiel incision after:– mobilization of splenic flexure– division of vascular pedicle
• Hand-assisted laparoscopy– allows tactile sensation– blunt separation

Conclusion
• Complex case• Experience counts• Maximize chances
– Approach– Extraction– HAL– +/- Ureteral catheters
• Alternate approach early