current update management of vap - jadeiisic2013 · current update management of vap george...
TRANSCRIPT

Current Update
Management of VAP
George Dimopoulos MD, PhD, FCCP
Professor, Critical Care Medicine
Chair of Infection Section ERS, Former Chair INFS ESICM, Consultant WHO
University Hospital ATTIKON, Medical School, University of Athens, Greece
JADE, Jakarta
12-14 April 2013

Conflict of interest disclosure
Prof Dimopoulos has no, real or perceived,
conflicts of interest that relate to this
presentation.

Ventilator Associated Pneumonia
1. Main nosocomial infection in patients receiving
Mechanical Ventilation
– Incidence : 8-15 cases per 1000 ventilator-days
– Mortality : 20 -50%
2. Is not “associated ” with the ventilators but with
artificial airways
3. Duration of MV, ICU and hospital LOS
4. Inappropriate antibiotic treatment : Mortality = 3,03
5. Economic impact : $41,294 charges per patient
Rotstein C. Can J Infect Dis Med Microbiol 2008, Kuti EL. J Critical Care 2008

VAP etiology- (SENTRY 2004–2008)
Etiology (%)
Pseudomonas aeruginosa 26,6
Acinetobacter baumannii 14,3
Klebsiella spp. 10,2
Enterobacter spp. 7
Serratia spp. 4,1
Staphylococcus aureus 19,5
N = 7496 cases
Jones R. Clin Infect Dis 2010; 51(S1):S81–S87
50%

Epidemiology of VAP Potentially Resistant Microorganisms
Group 1,: early-onset pneumonia without risk factors for PRM infection;
Group 2 : early-onset pneumonia with risk factors for PRM infection (who have received prior antibiotics or who have had prior
hospitalization within the past 90 days and immunosuppressive disease and/or therapy) or late-onset pneumonia
ATS Guidelines Am J Respir Crit Care Med
Group 1 (n=152) Group 2 (333) Overall (n=485) p value
Polymicrobial, n (%) 51 (23.5) 109(23.1) 160(23.2) 0.9
Pseudomonas aeruginosa 33(21.7) 82(24.6) 115(23.7) 0.5
Stenotrophomonas maltophilia 2(1.3) 14(4.2) 16(3.3) 0.1
MRSA 24(15.8) 58(17.4) 115(23.7) 0.5
Acinetobacter baumanii 24(15.8) 77(23.1) 101(20.8) 0.07
Martin-Loeches I , Deja M, Koulenti D, Dimopoulos G, Marsh B, Torres A, Niederman M, Jordi Rello and EU-VAP
Study Investigators. Intensive Care Med. 2013 Apr;39(4):672-81
The main message is
LOCAL EPIDEMIOLOGY !!!

Epidemiology of VAP Non-Potentially Resistant Microorganisms
Group 1 (n=152) Group 2 (333) Overall (n=485) p value
Polymicrobial, n (%) 51 (23.5) 109(23.1) 160(23.2) 0.9
MSSE 36(23.7) 41(12.3) 77(15.9) 0.002
Escherichia coli 20(13.2) 56(16.8) 76(15.7) 0.3
Klebsiella pneumoniae 17(11.2) 40(12.0) 57(11.8) 0.8
Streptococcus pneumoniae 11(7.2) 10(3.0) 21(4.3) 0.05
Serratia marcescens 7(4.6) 10(3.0) 17(3.5) 0.4
Haemophilus influenzae and
Moraxella catharrhalis 16(10.5) 16(4.8) 32(6.6) 0.002
Citrobacter spp 3(2.0) 4(1.2) 7(1.4) 0.6
Morganella spp 2(0.6) 2(0.4) 0.9
Enterobacter spp 11(7.2) 29(8.7) 40(8.2) 0.7
Proteus spp 5(3.3) 13(3.9) 18(3.7) 0.9
Martin-Loeches I , Deja M, Koulenti D, Dimopoulos G, Marsh B, Torres A, Niederman M, Jordi Rello and EU-VAP
Study Investigators. Intensive Care Med. 2013 Apr;39(4):672-81

Management of VAP
John Muscedere MDa, Peter
Dodek MD, MHScb, Sean
Keenan MD, MScb,
Rob Fowler MDCM, MSc,
Deborah Cook MD, MScd,
Daren Heyland MD, MSca,
for the VAP Guidelines
Committee and the Canadian
Critical Care Trials Group1
Journal of Critical Care 2008 23, 138–147

Empiric treatment
0 h. 48 h. 72 h.
Diagnosis of VAP Etiology Susceptibility
Microbiological diagnosis

Diagnosis of VAP
• Suspicion !!!!!! – Established Criteria
• Samples from the LRT – Invasive vs non-invasive techniques
– Quantitative vs qualitative cultures
• 335 episodes of clinically suspected VAP
– The introduction of antibiotics 72 h prior
to BAL did not affect the validity of the
test
Linssen CF et al, Intens Care Med 2008;26:20-30,
Fagon et al, Ann Intern Med 2000

Antimicrobial Treatment of VAP
American Thoracic Society Documents Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and
Healthcare-associated Pneumonia. Am J Respir Crit Care Med Vol 171. pp 388–416, 2005

Carbapenem-Resistance
P. aeruginosa (12, 21, 42%)
*A. baumannii (47, 26, 85%)
K. pneumoniae (1, 15, 49%)
http://www.ecdc.europa.eu

Antimicrobial Treatment of VAP
due to MDR / PDR pathogens
Antimicrobial
drugs
MDR or PDR
A. baumannii
ESBL-producing
Enterobacteriaceae
MRSA
Conventional
agents
Carbapenem
(Meropenem or
Imipenem / Cilastatin)
+
Sulbactam
Carbapenem
(Meropenem,1 g / 8 h
or Imipenem/ Cilastatin
500 mg / 6 h or 1 g /8 h;
or
Ertapenem 1 g qd)
Glycopeptide (esp.vancomycin,
after 25 -- 30 mg/kg loading, then
maintained with 15 mg/kg / 12 h)
Recommended
alternative
agent(s), or
regimen(s)
IV Colistin (2 MU / 8h)
+
IV Rifampicin(10 mg/kg/12 h)
Tigecycline
plus imipenem or colistin
Tigecycline
plus imipenem +amikacin
IV colistin (2 MU / 8 h) Linezolid
(600 mg loading, then 600 mg /12 h)
Vancomycin (standard dose)
+
Rifampicin (300 mg bid PO)
Quinupristin/dalfopristin
(7.5 mg/kg every 8 h)
Shio-Shin J & Po-Ren H Expert Opin Pharmacother. (2011) 12(14):2146-8

The role of Polymyxins
Polypeptide antibiotics
- 5 chemically different compounds polymyxin A, B, C, D, and E (by different species of Bacillus polymyxa)
Colistin sulfate (CS) - PO for bowel decontamination
- Locally as a powder for the treatment of bacterial skin infections
Colistimethate sodium (CMS) - also called colistin methanesulfate, pentasodium colisti-
methanesulfate, and colistin sulfonylmethate
- IV and by inhalation

Polymyxins - Mechanism of action
L-α-γ-diaminobutyric acid (Dab) molecules, contained in the
molecule of polymyxins, are positively charged
Lipopolysaccharide (LPS) molecules, which are present in
the cell wall of Gram-negative bacteria, are negatively charged
Polymyxins possess a higher affinity for LPS molecules than do
divalent cations such magnesium (Mg+2) and calcium (Ca+2) which
normally stabilize the LPS molecules
The result of this process causes an increase in the permeability
of the cell envelope, leakage of cell contents, and subsequently
bacterial cell death

Polymyxins - Are not active against……
Pseudomonas mallei
Burkholderia cepacia
Proteus spp.
Providencia spp.
Serattia spp.
Edwardsiella spp., and
Brucella spp.
Gram-negative and Gram-positive aerobic cocci
Gram-positive aerobic bacilli
All anaerobes, fungi, and parasites

Colistin Breakpoints of Resistance
Polymyxin P. aeruginosa A. baumannii Enterobacteriaceae
Committee (year)
S I R S I R S I R
Colistin
≤2 4 ≥8 ≤2 >2 CLSI
(2012)
≤4 >4 ≤2 >2 ≤2 >2 EUCAST (2012)
≤4 >4 ≤2 >2 ≤2 >2 BSAC
(2011)
S: ≤2; R: >2 (no specified species) CA-SFM (2003)
Polymyxin B ≤2 4 ≥8 ≤2 >2 CLSI
(2012)
CLSI = Clinical and Laboratory Standards Institute;, EUCAST = European Committee on Antimicrobial Susceptibility Testing; BSAC = British Society for Antimicrobial Chemotherapy;, CA-SFM = CA-Comité de l'Antibiogramme de la Société Française de Microbiologie, France.

Inhaled colistin for infections due to
MDR Gram-negative
Author year Setting Patients Dose/ duration Infection Pathogen Outcome
Hamer, 2000 Medical
wards
3 2-5 MU/day
12.6 days
VAP Pseudomonas aeruginosa
Clinical cure
100%
Michalopoulos 2005 ICU 8 1.5 to 6 MU/day
12.6 days
VAP A. baumanii P. aeruginosa
Clinical cure
87.5%
Kwa, 2005 ICU
Medical
wards
21 2-4 MU/day
14 days
VAP A. baumanii P. aeruginosa
Clinical cure
85.7%
Berlana, 2005 ICU 80 12 days VAP A. baumanii P. aeruginosa
Microbiological
cure 92%
Mataouakkil 2006 ICU 26 1 MU / 8h
15 days
VAP
bacteremia (3)
Acinetobacter baumanii
Clinical cure
100%
Michalopoulos 2008 ICU 60 1 MU / 8 h for 5 to
49 days +IV colistin
or meropenem
VAP A. baumanii P. aeruginosa K. pneumoniae
Clinical and
Microbiologic
cure 83.3%
Falagas 2009 Hospital
ICU
5 1MU/8 h or 0.5
MU/6 h for 6 to 11
days
VAP
HAP
A. baumanii P. aeruginosa K. pneumoniae
Clinical cure
80%

Inferior Clinical Efficacy of Colistin
• Suboptimal dosing
– lower total daily dosage of intravenous colistin
is associated with increased mortality
Falagas et al. Int J Antim Ag 2010; 35:194 – 199
• Delay in attaining an efficacious drug concentration
– Necessity to give a loading dose Plachouras et al. AAC 2009; 53:3430 –3436
• Optimal dosing regimen
– Once daily, twice daily or three times daily?

Which loading dose ?
0
1
2
3
0 12 24 36 48 60 72 84 96
Time after first dose (hours)
Co
listin
Co
ncen
tratio
n (
mg
/L)
3 MU x 39 MU + 4.5 MU x 212 MU + 4.5 MU x 29 MU (2h infusion) + 4.5 MU x 212 MU (2h infusion) + 4.5 MU x 2
The administration of a loading dose of 6 MU CMS resulted in colistin plasma concentrations above 1mg/L within 4 hours in the majority of the patients.
Mohamed AF, I.Karaiskos et al . AAC
2012;56:4241-9
Plachouras et al. AAC 2009; 53:3430 –3436

Couet W. CMI 2012:18:30-39.
Colistin clinical studies

Spread of colistin resistant isolates in parallel with the increased colistin consumption from pharmacy data
Among 30 patients colonized by ColRKP
27(90%) had received colistin (p < 0.001;
OR, 6.98; 95% CI, 2.0–24.3)
Among 94 patients exposed to colistin
27 (28.7%) were colonized by ColRKP.
These patients had received colistin for a
median of 20.0 days, compared with
14.5 days for patients not colonized by a
ColR strain (p 0.048)
Genotypic analysis of the isolates revealed
that the majority of the CRKP isolates
belonged to different clones. Clin Microbiol Infect 2011

Breakpoints of Tigecycline against
Enterobacteriacecae and Acinetobacter baumannii
MIC(μg/ml) Inhibition Zone (mm) Implementing
Organism or
proposing
authors S I R S I R
Enterobacteriaceae* ≤2 4 ≥8 ≥19 15-18 ≤14 US FDA
≤1 2 >2 - - - EUCAST
≤1 2 >2 ≥24 20-23 ≤19 BSAC
A.baumannii - - - - - - US FDA**
IE IE IE - - - EUCAST
≤1 2 >2 ≥24 20-23 ≤19 BSAC
≤2 4 ≥8 ≥16 13-15 ≤12 Jones RN et al
Giamarellou H and Poulakou G, Drugs, 2009

Tigecycline per type of infection
and treatment group
M group PAM group M group+ PAM group Total
N=22 N =23 VAP
N =21
BSI
N =10
SI
N=14
N =45
Clinical outcome (%) 81.8 78.3 90.5 80 64.3 80
Microbiological
outcome (%)
63.6 56.5 57.1 80 50 60
14 day mortality %
attributable
crude
9.1
9.1
4.3
21.7
4.8
19
10
10
7.1
14.3
6.7
15.6
Hospital mortality %
attributable
crude
27.3
36.4
13
43.5
19
42.9
20
30
21.4
42.9
20
40
Poulakou et al, J of Infection 2009;58:273-84

Tigecycline vs imipenem/cilastatin
for the treatment of HAP
• A phase 3, multicenter, randomized, double-blind, study
– tigecycline vs imipenem/cilastatin regimen in 945 HAP patients
• Cure rates
– 67.9% for tigecycline and 78.2% for imipenem
– absolute difference -10.4 [-17.8 to -3.0]; p= 0.120
– non-inferiority criteria NOT MET
• In VAP
– Tigecycline 47.9% versus 70.1% for imipenem/cilastatin
– Tigecycline was noninferior to imipenem
Freire A et al, Diagn Microbiol Infect Dis 2010; 18 140-151

Tigecycline - Issues to be considered
• No adequate activity in bacteremias
• No licensed for VAP
• Possibility of breakthrough bacteremias with Proteus spp
inherently resistant to tigecycline, particularly in patients
pretreated with colistin
• Probably higher doses of tigecycline (i.e 100-150mg/12hrs)
are needed in order to achieve adequate levels for borderline
MICs (4-8μg/ml) or difficult body compartments

Antimicrobial susceptibilities of KPC-Kp Microbiological data from 18 infections, “ATTIKON” Hospital
MIC range
mg/L
MIC50
mg/L
MIC90 mg/L %
susceptible
Meropenem 4->256 64 >256 2
Minocycline 1->16 4 >16 55.2
Tigecycline 0.5-8 2 8 15.4*
Colistin 0.125-48 0.5 8 86
Gentamicin 2->256 4 16 70
Amikacin <8->32 32 >32 14
Fosfomycin 8->256 32 256 55
Souli M et al, CID 2010
*Susceptibility breakpoint: ≤1mg/L according to EUCAST 65.4% of isolates had an MIC ≤2mg/L
The main message is
LOCAL EPIDEMIOLOGY !!!

Aminoglycosides - Spectrum and Activity
Aminoglycosides are active
o against Gram (-) and some Gram (+)
o against Mycobacteria
Aminoglycosides + b-lactams = Synergy (?)
o β-lactam affects the cell wall of the bacteria providing the
increased penetration of aminoglycoside
o the increased entrance of aminoglycoside increases the
inhibition of proteino-synthesis of bacteria
In vitro : the greatest likelihood of synergy
o aminoglycoside + antipseudomonal penicillin (~ 90%)
o aminoglycoside + cephalosporin (~ 80%)
o aminoglycoside + carbapenem (~ 50%)
Hsin-Yun Sun et al, Chest 2011; 139(5):1172–1185

Aminoglycosides in clinical practice (I)
Aminoglycosides + broad-spectrum β-lactams
- should not be added to achieve synergism in treating Gram (-)
infections as combination
does not improve efficacy and adds side effects
The evidence from RTCTs in humans
- does not support the use of aminoglycosides in staphylococcal
or streptococcal endocarditis and is lacking for endocarditis
caused by enterococci
Leibovici et al, JAC;63(2)246-251

Proposed RCTs for answers about aminoglycosides
in clinical practice…………
Treatment Comparator Patients with
Anti-pseudomonal
β-lactam drug
Same
anti-pseudomonal β-lactam
+ an aminoglycoside
Infections caused
by P. aeruginosa
β-lactam drug β-lactam
+ an aminoglycoside
Bacterial endocarditis caused
by S. aureus, streptococci or
enterococci
Aminoglycoside Colistin or tigecycline Infections caused
by Gram (-) susceptible only to
these agents
Aminoglycoside
drug
a β-lactam drug Infections caused
by Gram-negative pathogens

A randomly selected sample of o 30 Klebsiella pneumoniae,
o 30 Pseudomonas aeruginosa, and
o 30 Acinetobacter baumannii
The MIC of fosfomycin for each isolate was
determined by the agar dilution method
Provisional breakpoint of susceptibility ≤ 64 μg/ml
according to CLSI criteria
What about fosfomycin ?

In vitro antimicrobial susceptibility of fosfomycin
K. pneumoniae P. aeruginosa A. baumannii
All isolates were ESBL and MBL (blaVIM-1) producers
All isolates were ESBL
producers
MIC range: 8-64 μg/ml
MIC range: 4 to >512 μg/ml
MIC range: 64 to >512
μg/ml
MIC range: 8-64 μg/ml MIC50 16 μg/ml MIC90 32 μg/ml
MIC50 32 μg/ml
and
MIC90 128 μg/ml
MIC50 256 μg/ml and
MIC90 >512 μg/ml
None of the isolates was
resistant
20% of the isolates were
resistant to fosfomycin
A randomly selected sample of 30 Klebs. pneumoniae, 30 P. aeruginosa, and 30 A. baumannii
The MIC of fosfomycin for each isolate was determined by the agar dilution method
Provisional breakpoint of susceptibility ≤ 64 μg/ml
Dimopoulos et al Eur J Clin Micr Infect Dis 2008

Fosfomycin in Critically-ill Patients
with KPC-Klebsiella infections
Michalopoulos A et. al Clin Microbiol Infect 2010; 16: 184-6
Characteristic
Mean age, years 67.5
APACHE II score 23.4
No. of organ dysfunction,
median 3
VAP
Primary bacteremia
Other
5
2
4
All cause hospital mortality 18.2%


Efficacy of Fosfomycin (F) in XDR and PDR
Gram-negative infections in ICU patients
In vivo efficacy of fosfomycin ?
Microbiologically documented infections by Gram (-)
S : Fosfom, R : Ceph, Quinolones, beta-lactamase inhibitors
- 45 pts / 12 ICUs, Mean (age 55.6 years, APACHE II 19.8, SOFA 8.6)
- Primary/ secondary bacteremia (16 /6), CVCBSIs (8), VAP (14), IAIs(7)
- Sepsis, severe sepsis and septic shock 21.4%, 7.1%, 21.4%
- K. pneumoniae KPC(+) 83.7%, P. aeruginosa 35.7%, PDR 15, XDR 30
K. Pontikis, I. Karaiskos, Ch. Paskalis, A. Koutsoukou, E. Roilides, G. Dimopoulos, G. Nakos, N. Maggina, S. Bastani, A.
Prekates, G. Poulakou, H. Giamarellou on behalf of the Hellenic Study Group of "ICU Infections“
ECCMID 2013: Abstract received - Abst. Nr. 2653

Fosfomycin IV, 6gr x 4 per day, for a mean of 12 days
+
Colistin (28 pts) and Tigecycline (17 pts)
Clinical Outcome o Successful by day 14 in 55.8% including 10 pts with PDR strains
o Failure in 27.9%
o Relapse in 4.7%
o Superinfection in 4.7%.
Microbiological Outcome o Bacterial eradication was observed in 54.8%
o Resistance development to F in 4 cases.
Main adverse event
o reversible hypokalemia (6 pts)
K. Pontikis, I. Karaiskos*, Ch. Paskalis, A. Koutsoukou, E. Roilides, G. Dimopoulos, G. Nakos, N. Maggina, S. Bastani, A. Prekates, G.
Poulakou, H. Giamarellou on behalf of the Hellenic Study Group of "ICU Infections ECCMID 2013: Abstract received - Abst. Nr. 2653

Vancomycin and the Lung
Vancomycin penetration into lung tissue
was evaluated in 30 pts following 1g vancomycin.
Ratios of lung tissue to serum concentration ranged 0.24 to 0.41 at
1 and 12h, respectively.
1 of 6 pts at 6h, and 3 of 7 pts at 12h
had NO detectable levels of vancomycin
in lung tissue.
A 1h iv infusion of a 1g dose of vancomycin
does not achieve sustained lung concentrations above the MIC.
Cruciani et al J Antimicrob Chemother 1996;38:865-9

Boselli et al Crit Care Med 2005:33;1529-33

ZEPHyR Trial - Clinical Success Rates
PP at EOS MITT at EOS PP at EOT MITT at EOT 0
20
40
60
80
100
Clin
ical success r
ate
Linezolid Vancomycin
P = 0.042 P = 0.049
P = 0.002 P = 0.004
57.6% 95/165
54.8% 102/186
83.3% 150/180 80.1%
161/201
46.6% 81/174
44.9% 92/205
69.9% 130/186
67.8% 145/214
Wunderink RG et al Clin Infect Dis 2012; 54:621–9.

Short- vs
long- duration
antibiotic
regimens for
VAP: a
systematic
review and
meta-analysis
Mortality between the two arms.
Antibiotic-free days between the two arms.
Relapses between the two arms
Dimopoulos et al , Chest 2013 (in press)

Salvage Therapy for Pan-Drug Resistant
Enterobacteriaceae: The Available Antibiotics
1. Chloramphenicol, Co-trimoxazole, Nitrofurantoin
for Klebsiella pneumoniae carbapenemase(+)
2. Temocillin: active against ESBL(+) and AmpC(+)
Enterobacteriaceae. Available only in Belgium and the UK
3. High dose Amikacin (50mg/kg) plus hemofiltration
4. Combination of 2 carbapenems: Ertapenem + Doripenem?

In vitro chemostat model (doripenem MIC, 4 g/ml).
Control
Erta alone
Dori alone
Dori+erta
In vivo murine thigh infection model (doripenem MIC, 4 g/ml)
Antimicrobial agents and chemotherapy 2011; 55(6): 3002–3004
Exploiting increased in vitro affinity of KPC enzymes for ertapenem “a suicide substrate”

Prevention of VAP
• Pharmacological and non-pharmacological measures
• Airway care methods major development
– Efficacy, feasibility and low cost
Passive humidifiers (heat and moisture exchangers)
Open vs closed tracheal suction system
Continuous or intermittent subglottic secretion systems
New materials for the endotracheal tube cuff
Polyurethane vs polyvinyl cuff (avoids the leakage of secretions)
Coated endotracheal tube with silver (antibacterial properties)
• Bundles (group of measures) • Semi-recumbent position, hand hygiene, staff education, adequate
nurse/patient staffing ratios, microbiological surveillance,
antibiotic control policies, no change of ventilator circuits, standarized protocols
for sedation and weaning
Siempos I et al, Crit Care Med 2007; 35;2843-51, Polaert J et al, J Thorac Cardiovasc Surg 2008;135:771-8,
Kollef M et al, JAMA 2008;300;805-813, Kuti El et al, Crit Care 2008;2391-100

Impact of patient position on the
incidence of VAP
Incidence of clinically diagnosed VAP
semirecumbent (treatment) to supine position (control) and prone
(treatment) to supine position (control).
Death incidence comparing semirecumbent
(treatment) to supine position (control) and prone (treatment) to
supine position (control).
Patients positioned semirecumbently 45° have significantly lower incidence of clinically diagnosed VAP compared to patients
positioned supinely. On the other hand, the incidence of clinically diagnosed VAP among patients positioned pronely does not
differ significantly from the incidence of clinically diagnosed VAP among patients positioned supinely.
Alexiou V, Ierodiakonou V and Dimopoulos G. J Crit Care 2009

Using a surveillance method… ..concordance between VAP and BSI pathogenic isolates and
prior respiratory tract (RT) or gastrointestinal tract (GT) colonization
Surveillance cultures Acinetobacter, Pseudomonas, Klebsiella - VAP (PPV 67–94%, NPV 73–100%)
- Bacteremia (PPV 43–54%, NPV 88-100%)
Surveillance-guided initial
antibiotic therapy - appropriate in 91% and 86% of
patients with VAP and bacteremia
respectively.
Papadomichelakis et al Intensive Care Med (2008) 34:2169–2175
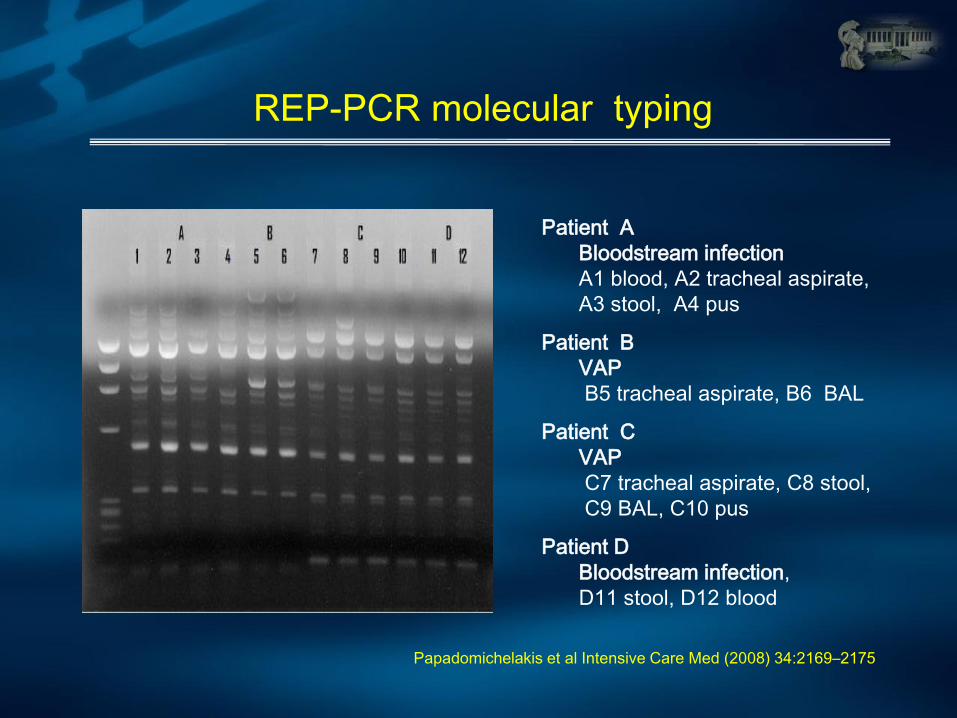
REP-PCR molecular typing
Patient A
Bloodstream infection
A1 blood, A2 tracheal aspirate,
A3 stool, A4 pus
Patient B
VAP
B5 tracheal aspirate, B6 BAL
Patient C
VAP
C7 tracheal aspirate, C8 stool,
C9 BAL, C10 pus
Patient D
Bloodstream infection,
D11 stool, D12 blood
Papadomichelakis et al Intensive Care Med (2008) 34:2169–2175

Hand Hygiene
• Handwashing – Washing hands with
plain soap and water
• Antiseptic handwash – Washing hands with
water and soap or other
detergents containing
an antiseptic agent
• Alcohol-based handrub – Rubbing hands with an
alcohol-containing
preparation
• Surgical hand hygiene
/antisepsis – Handwashing or using an
alcohol-based handrub
before operations by
surgical personnel
Guideline for Hand Hygiene in Health-care Settings. MMWR 2009;51:RR-16
X represents VRE culture positive sites
The hand
of a doctor
in the agar

Hand flora
“transient” flora
Εnterobacteriacae
E. coli, Klebsiella spp.,
Proteus spp., Serratia
spp., Enterobacter spp.
Pseudomonas spp
Acinetobacter spp
MRSA
VRE
“resident” flora
• CοNS
• Micrococci,
• Propionibacterium spp

Hand Hygiene - the right way
Hand Hygiene - avoiding the recontamination

Hand Hygiene - with the appropriate solution
Good Better Best
Plain Soap is good at reducing
bacterial counts
Antimicrobial
soap
is better
Alcohol-based handrub
are the best

Use of artificial nails by healthcare workers poses
risk to patients?
5
35
10
0
10
20
30
40
p<0.05
% R
eco
very
of
gra
m
neg
ati
ve b
acte
ria
Natural (n=31)
Artificial (n=27)
Polished (n=31)
ARTIFICIAL
POLISHED
NATURAL
Edel et. al, Nursing Research 1998: 47;54-59
Avoid wearing artificial nails, keep natural nails <1/4 inch
if caring for high risk patients (ICU, OR)

Compliance in ATTIKON hospital

What is different in critical illness ?
• Capillary leak*
- increased body fluid
• Organ dysfunctions elimination
accumulation of metabolites
• Administration of multiple drugs - drug interactions
- altered protein binding
* Capillary leak lead to ………..
…...important changes in concentrations
of antibiotics with low volumes of
distribution
(penicillins, cephalosporins, carbapenems and aminoglycosides

Concentration (
mg/L
)
Time (hours) 0
Cmin (Trough))
Cmax (Peak)
MIC
AUC
MIC
t>MIC Time dependent
Concentration dependent
AUC/MIC = AUIC
PK-PD Dose concentration effect

Volume of distribution (Vd)
500 mg 500 mg
Beta-lactams
Vd approx. 15 - 20 L
Quinolones
Vd approx 80 - 200 L
. . . . . .
.
. . . .
. . .
.
. . .
. .
Dimopoulos G. Curr Drugs Metab 2009;10(1):13-21
Vd = dose [mg] / concentration [mg / L]

Sepsis pathophysiology and
antibiotic pharmacology
SEPSIS
Increased Cardiac Index
Leaky Capillaries &/or altered protein binding End Organ
Dysfunction
Increased Clearances
Increased Volume of Distribution
Decreased Clearances
Low Serum
Concentrations
High Serum
Concentrations
Roberts & Lipman Clin pharmacokinet 2006

Creatinine clearance
0
50
100
150
200
250
0 50 100 150 200 250 300
Creatinine Clearance (mL/min)
Dru
g C
lea
ran
ce
(m
L/m
in)
Cefepime
Cefpirome
Lipman et al Anesth Analg 2003

Is continuous infusion better ?
• 57 ICU patients
• Randomised to bolus/CI
• 50 met a priori analysis criteria
• ie >3 days Rx
Better
clinical + bacteriological response
Roberts et al JAC 2007;59:285-91

Continuous infusion
• Continuous infusion • beta-lactam antibiotics may
optimize PK / PD profile
• For pathogens with MICs
close to the breakpoint
• Empirical therapy
• For carbapenems, prolonged
infusions (3 h) t.i.d. seem the
most suitable way of
administration
Through Infection Section of ESICM

New agents
Agent Class/mode of action Spectrum/phase
Avibactam(nxl104)
Diazabicyclooctane
Class a & c b-lactamase inhibit or(paired
with ceftaroline / ceftazidime & aztreonam)
Ps aeruginosa
MDR enterobacteriae
Phase II, III
mk-7655 Class a & c b-lactamase inhibitor
(paired with imipenem)
Ps aeruginosa
MDR enterobacteriae
Phase III
rpx7009 Boronic acid
derivative-paired with biapenem
MDR enterobacteriae
ME-1071 Maleic acid inhibitor
MBL inhibitor
(paired with carbapenems)
MBL producing bacteria

New agents with new mode of action
• LpxC inhibitors (CHIR-090)
– LpxC: deacetylase involved in the biosynthesis of lipid A of LPS
Mansoor UF, et al. Bioorg. Med. Chem. Lett. 2011;21(4):1155-1161
Rapid resistance and regrowth in phase II study!!! It was withdrawn
Leucyl-tRNA synthetase (LeuRS)
Future options The revival of isepamicin?
• Antimicrobial susceptibility for the 1,040 K.
pneumoniae isolates was highest for isepamicin
(95.3%), followed by colistin (89.3%)
• Regarding resistant K. pneumoniae isolates,
susceptibility to isepamicin was observed for
91.1%, 87.7%, and 85.6% of the isolates that
were non-susceptible to the carbapenems, all
other aminoglycosides, and colistin, respectively
Maraki S, Antimicrob Agents Chemother 2012 Mar 5

Future options
• PK/PD applications of
- Meropenem
- Doripenem
- Tigecycline
- colistin

PK-PD target attainment for β-lactams
Bacteriostatic and bactericidal activity of β-lactams depends on duration of time free (unbound) drug levels exceed MIC (% T>MIC)
Antimicrobials
Free Drug % Time >MIC
Bacteriostatic (%) Bactericidal (%)
Cephalosporins 35-40 60-70
Penicillins 30 50
Carbapenems 20-30 30-40
* 3 log reduction in colony –forming units
Drusano 2004, Nat Rev Microbiol 2:289

Bulic CC et al Antimicrob Agents Chemother 2010; 54: 804
fT > MIC 100% fT > MIC 75%

In Vivo Killing Kinetics of VIM and Non-VIM-Producing K. pneumoniae in the Thighs of Neutropenic
Mice Treated with Imipenem
MIC=0.125 μg/ml MIC=2 μg/ml
VIM-negative VIM-positive
Daikos GL et al Clin Microbiol Infect 2007; 13: 202-205

Pharmacokinetics of three different dosing regimens of meropenem
Simulated Target Attainment Probabilities for 50%T>MIC of three Different Dosing
Regimens of Meropenem

How To Optimize De-Escalation:
Use of Clinical Parameters To Modify or Stop Therapy
Luna CM et al. Crit Care Med (2003)
• Evolution of the CPIS
correlated with mortality.
• PaO2/FIO2 ratio was the best
correlate of clinical
response and outcome
Survivors (n=31)
Non-Survivors (n=32)
All (n=63)
Therapy Serial CPIS
Measurements to Determine
the Outcome in VAP
4
5
6
7
CP
IS
VAP-3 VAP VAP+3 VAP+5 VAP+7
Days 1
2
3
0

Back to the copper era? ATTIKON Hospital ICU- 2011

The Prorata trial Bouadma L et al, The Lancet 2010
Patients receiving antibiotics for days 1–28
Significantly fewer patients assigned to the procalcitonin group received antibiotics than did those assigned to the control
group (p<0·0001, generalised linear model test for repeated measures).

An ESICM systematic review and meta-analysis
of procalcitonin-guided antibiotic therapy algorithms
in adult critically-ill patients
• 7 RCTs
• in the duration of first episode of antibiotic treatment
pooled WMD of -3.15 days FEM, 95% CI – 4.36 to 1.95, P<0.001
• No difference in 28-day mortality
FEM, OR=0.96, 95% CI 0.79 to 1.15, P=0.63
• in antibiotic free days within the first 28 days of hospitalization
pooled WMD of 3.08 days FEM, 95% CI 2.06 to 4.10, P<0.001)
• No difference between regarding the remaining outcomes
• Sensitivity analyses yielded similar results
Matthaiou D, Ntani G, Kontogeorgi M, Poulakou G, Armaganidis A, Dimopoulos G. Intensive Care Med. 2012 Jun;38(6):940-9
WMD = weighted mean differences, FEM= fixed effects model

NOTE: Weights are from random effects analysis
Overall (I-squared = 88.7%, p = 0.000)
Schroeder et al
Nobre et al
Study
Hochreiter et al
Stolz et al
Bouadma et al
2009
2008
Year
2009
2009
2010
-3.15 (-4.35, -1.95)
-1.70 (-2.39, -1.01)
-4.00 (-6.64, -1.36)
WMD (95% CI)
-2.00 (-2.46, -1.54)
-5.00 (-6.13, -3.87)
-3.80 (-4.83, -2.77)
100.00
23.06
11.36
Weight
24.07
20.44
21.08
%
-3.15 (-4.35, -1.95)
-1.70 (-2.39, -1.01)
-4.00 (-6.64, -1.36)
WMD (95% CI)
-2.00 (-2.46, -1.54)
-5.00 (-6.13, -3.87)
-3.80 (-4.83, -2.77)
100.00
23.06
11.36
Weight
24.07
20.44
21.08
%
0-4 -2 0 2 4
Favors PCT arm Favors control arm
Weighted mean difference of
duration of first episode
of antibiotic treatment.
Overall (I-squared = 0.0%, p = 0.906)
Schroeder et al
Study
Hochreiter et al
Bouadma et al
Nobre et al
Stolz et al
Jensen et al
Svoboda et al
2009
Year
2009
2010
2008
2009
2011
2007
0.96 (0.79, 1.15)
0.91 (0.15, 5.58)
OR (95% CI)
0.99 (0.43, 2.32)
1.05 (0.71, 1.55)
0.99 (0.27, 3.63)
0.59 (0.22, 1.59)
0.97 (0.76, 1.24)
0.58 (0.21, 1.57)
100.00
1.11
Weight
4.87
22.70
2.09
4.65
%
59.98
4.60
0.96 (0.79, 1.15)
0.91 (0.15, 5.58)
OR (95% CI)
0.99 (0.43, 2.32)
1.05 (0.71, 1.55)
0.99 (0.27, 3.63)
0.59 (0.22, 1.59)
0.97 (0.76, 1.24)
0.58 (0.21, 1.57)
100.00
1.11
Weight
4.87
22.70
2.09
4.65
%
59.98
4.60
1.148 1 6.76Favors PCT arm Favors control arm
An ESICM systematic review and meta-analysis
of procalcitonin-guided antibiotic therapy algorithms
in adult critically-ill patients
Odds ratios of
28-day mortality
Matthaiou D, Ntani G, Kontogeorgi M, Poulakou G, Armaganidis A, Dimopoulos G. Intensive Care Med. 2012 Jun;38(6):940-9

Resistance emergence and spread
SELECTION
of resistant strains
Eradication of the susceptible strains
Growth of the resistant strains
Function of antimicrobial activity and
the pharmacokinetics of the antibiotic
Environmental factors
and fitness of the resistant strain
TRANSMISSION
amplification and
spread of resistance
GENETIC EVENT
emergence of the
resistant strain
Spontaneously
Independent of antibiotic presence
A function of the bacterial
and of the antibiotic
Hawkey, BMJ 1998; 317:657–60; Freney, Précis de bactériologie Clinique Ed. ESKA 2000; Andremont,Med Mal Inf.2005;35 sup3:S207-11; Rice, Clin
Infect Dis 2000; 31:762–9; Livermore, Clin Infect Dis 2003;36Sup1:S11-23
• The emergence of bacterial resistance is
through two mechanisms
Mutation Acquisition of foreign DNA +

Control of Resistance by Antibiotic Restriction
• Rise in the rate of multiresistant (including gentamicin) Enterobacteriaceae in neuro-units.
• Unable to control with hygiene methods:
– education
– hand washing
– barrier precautions.
• Added temporary restrictive antibiotic policy (TRAP) in Period III
0
5
10
15
20
25
30
35
40
I II III IV
% with GRE
SEL/SUP Ratio
TRAP
*Period I (week 23 to week 45, 1995), Period II (week 46, 1995, to week 22, 1996), period III (week 23 to week 45, 1996), Period IV (week 46, 1996, to week 22, 1997)
Leverstein-van Hall et al. Eur J Clin Microbiol Infect Dis 2001;20:785–791
Nu
mb
er
of p
atie
nts
Period*
Conclusions
Antimicrobial treatment of VAP - early adequate and appropriate empiric therapy
- local epidemiology
- short duration of antibiotics
Treatment of MDR pathogens
- carbapenems, colistin, gentamicin, tigecycline
- synergistic actions (TIGE- + MERO-) ?
- the role of fosfomycin ?
Use of antibiotics
- Pk/PD properties in septic patients
- Surveillance
- Avoiding development of resistance