emerging infectious diseases - commonwealth medicine€¦ · standard precautions necessary to...
TRANSCRIPT
Emerging Infectious DiseasesDonna Gallagher,
PhD, ANP-C,MS, FAAN
PI, NEAETC
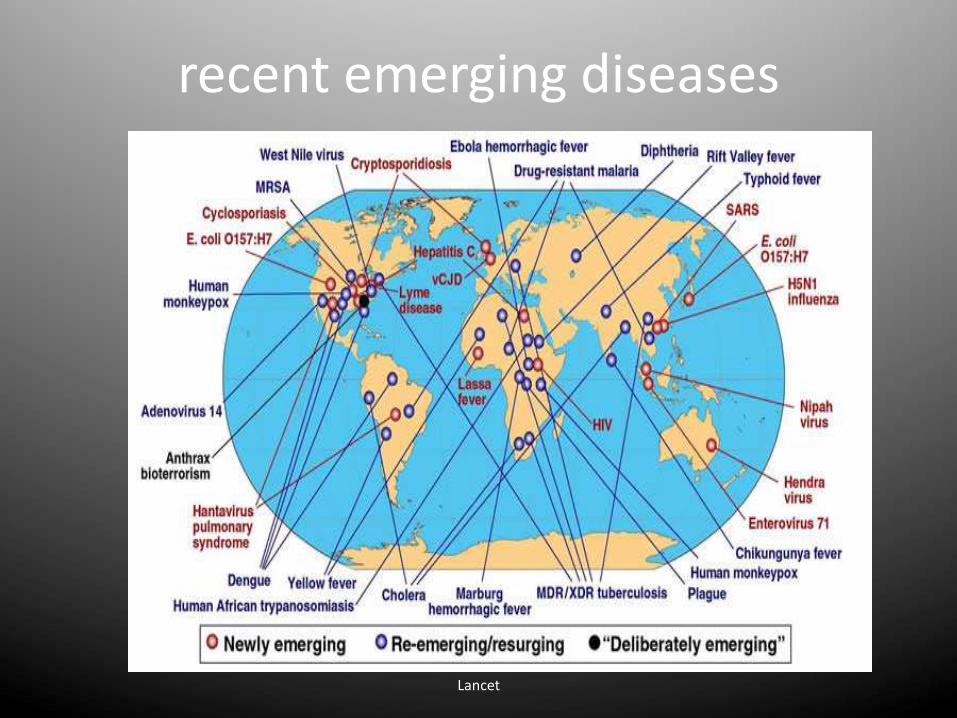
Lancet
recent emerging diseases
Emerging and re-emerging infectious diseases
• AIDS
• Avian Influenza
• Ebola
• Marburg
• Cholera
• Rift Valley Fever
• Typhoid
• Lassa Fever
• Tuberculosis
• Leptospirosis
• Malaria
• Japanese encephalitis
• Chikungunya
• Dengue
• Antimicrobial resistance
• MERS
Factors contributing to emergence
AGENT
• Evolution of pathogenic infectious agents (microbial adaptation & change)
• ex: influenza
• Development of resistance to drugs • ex: MRSA, KPC
• Resistance of vectors to pesticides• ex: malaria
Factors contributing to emergence
HOST
» Human demographic change (inhabiting new areas)
» Human behaviour (sexual & drug use)
» Human susceptibility to infection (Immunosuppression)
» Poverty & social inequality
Factors contributing to emergence
ENVIRONMENT
»Climate & changing ecosystems
»Economic development & Land use (urbanization, deforestation)
»Technology & industry (food processing & handling)
Transmission of Infectious Agent from Animals to Humans
• Emerging Influenza infections in Humans associated with Geese, Chickens & Pigs
• Animal displacement in search of food after deforestation/ climate change (Lassa fever)
• Humans themselves penetrate/ modify unpopulated regions- come closer to animal reservoirs/ vectors (Yellow fever, Malaria)
Dr. KANUPRIYA CHATURVEDI
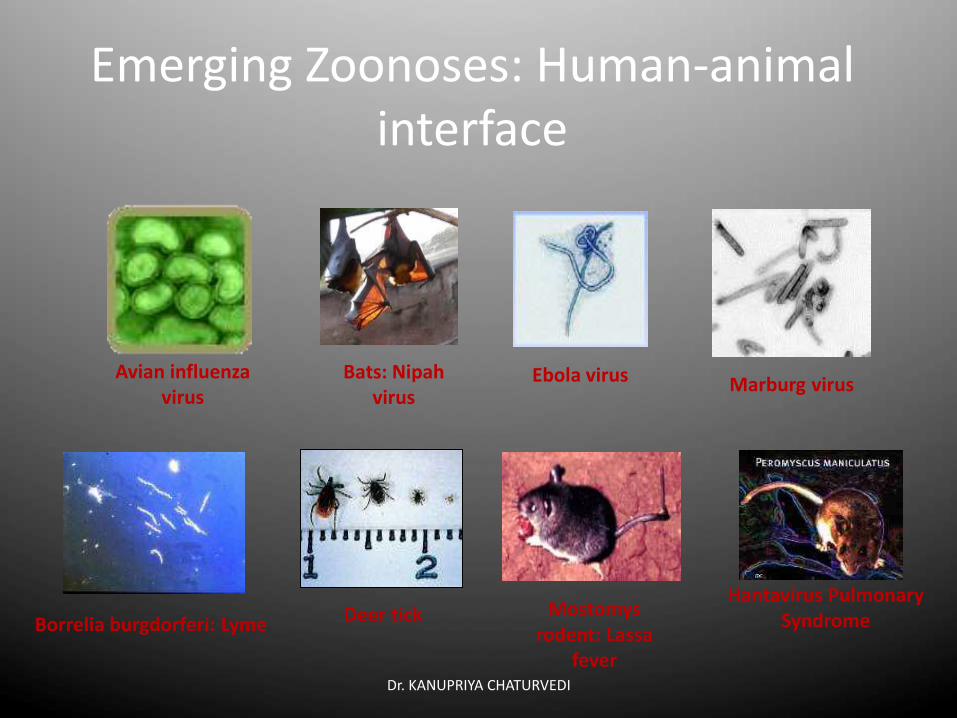
Emerging Zoonoses: Human-animal interface
Marburg virus
Hantavirus Pulmonary Syndrome
Ebola virus
Borrelia burgdorferi: Lyme Deer tick Mostomysrodent: Lassa
fever
Avian influenza virus
Bats: Nipahvirus
Pandemic and Epidemic Diseases department - 9
How Ebola Outbreaks Start
●First human cases start with infection by an animal ●Bats to chimpanzes, other animals and bush meat. How current
outbreak started in unknown, but killing and preparing bush meat can spread other viral illnesses
●Infection from person-to-person creates an outbreak• Direct or indirect physical contact with body fluids of a sick
infected person (blood, saliva, vomitus, urine, stool, semen)
●Well known locations where transmission occurs• Hospital:
• Health care workers, other patients, unsafe injections
• Houses and Communities:
• Family, friends, contacts caring for ill, through funeral practices---ie contact with dead bodies
Pandemic and Epidemic Diseases department - 10
Critical Issues
● First large Ebola outbreak in West Africa
● Underlying weakness in health systems
● Lack of preparedness and poor surveillance, health care, diagnostics, communications …
• Health worker infections & inadequate infection control & prevention The affected countries in West Africa have some of the worst physician–patient ratios in the world:
– Liberia: more than 86 000 patients per physician
– Sierra Leone: more than 45 000 patients per physician
Effect of fear
● Strong community resistance in places ……..

Training ………… screening
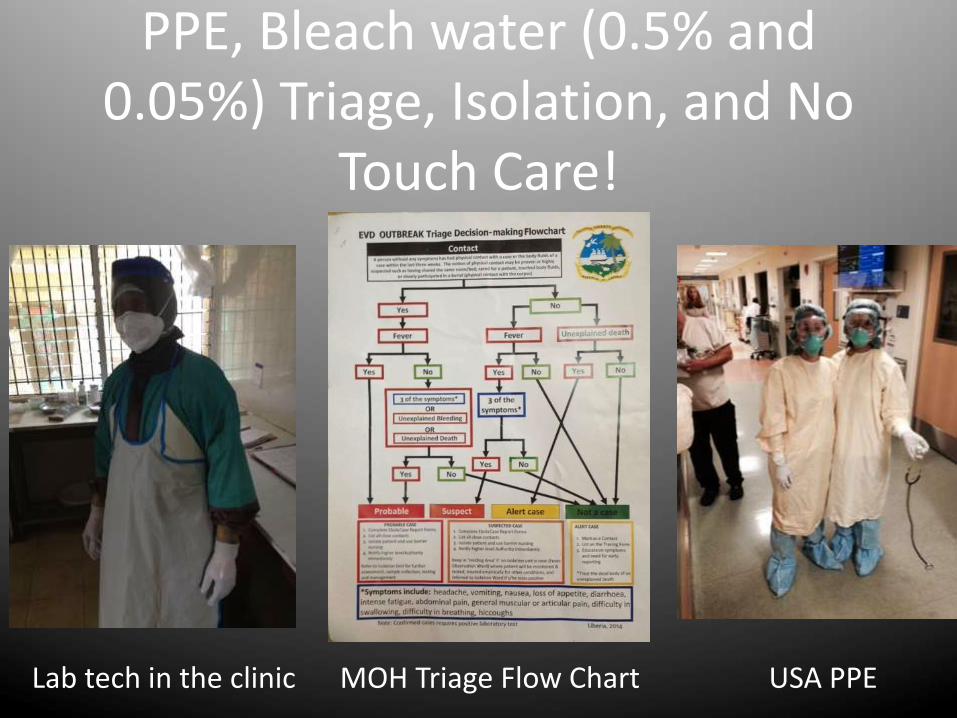
PPE, Bleach water (0.5% and 0.05%) Triage, Isolation, and No
Touch Care!
Lab tech in the clinic MOH Triage Flow Chart USA PPE
US
• Contact Precautions
• Working knowledge of emerging diseases
• Know where your PPE is located
• Know who to call
• Don’t Panic
EMERGING INFECTIONS: STANDARD AND TRANSMISSION-BASED PRECAUTIONS FOR AMBULATORY HEALTHCARE SETTINGS
Kathy Eklund RDH, MHP
The Forsyth Institute
Disclosures
Disclosure: Neither I nor members of my immediate family have any financial relationships with commercial entities that may be relevant to
this presentation.Visuals of products and devices are examples and
are not an endorsement.
Objectives
• Differentiate standard and transmission-based precaution measures
• Identify measures and resources clinicians may use to promote respiratory hygiene and setting-specific illness recognition.
What is an Infection Prevention and Control Program?
A system of policies, procedures and practices that when successfully implemented, will minimize the risk of transmission of pathogenic microorganisms. The goal is to prevent:
– healthcare-associated infections in patients
– injuries and illnesses in healthcare personnel

Public Trust & Expectations
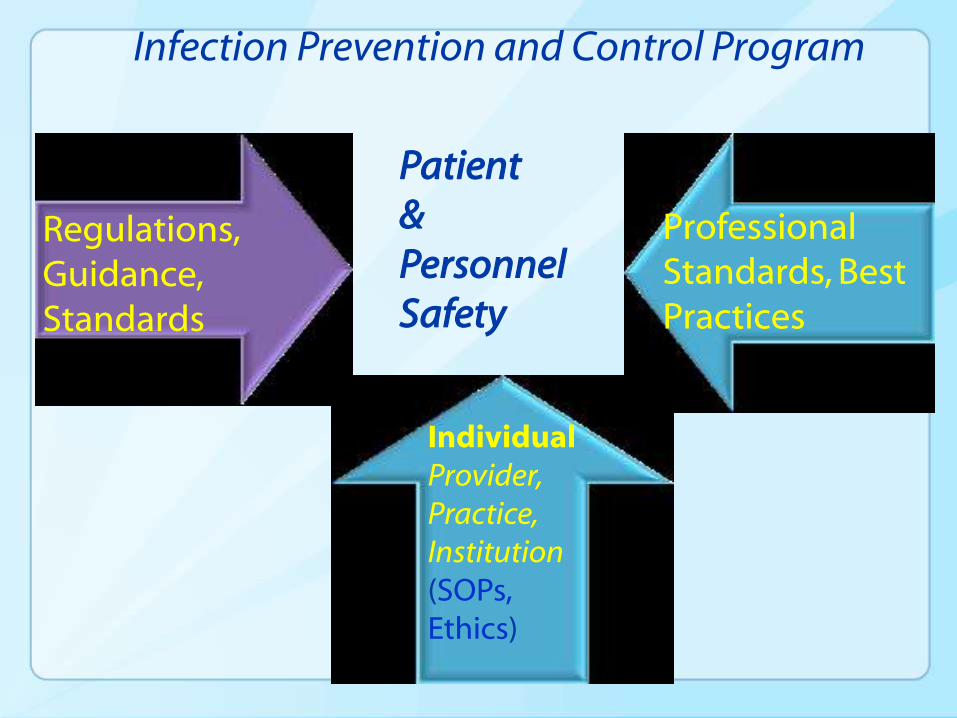
Infection Prevention and Control Program
Professional Standards, Best Practices
Regulations, Guidance, Standards
IndividualProvider,Practice,Institution(SOPs, Ethics)
Patient &Personnel Safety
Infection Control Policies and Procedures..
• Should be supported by an authoritative source
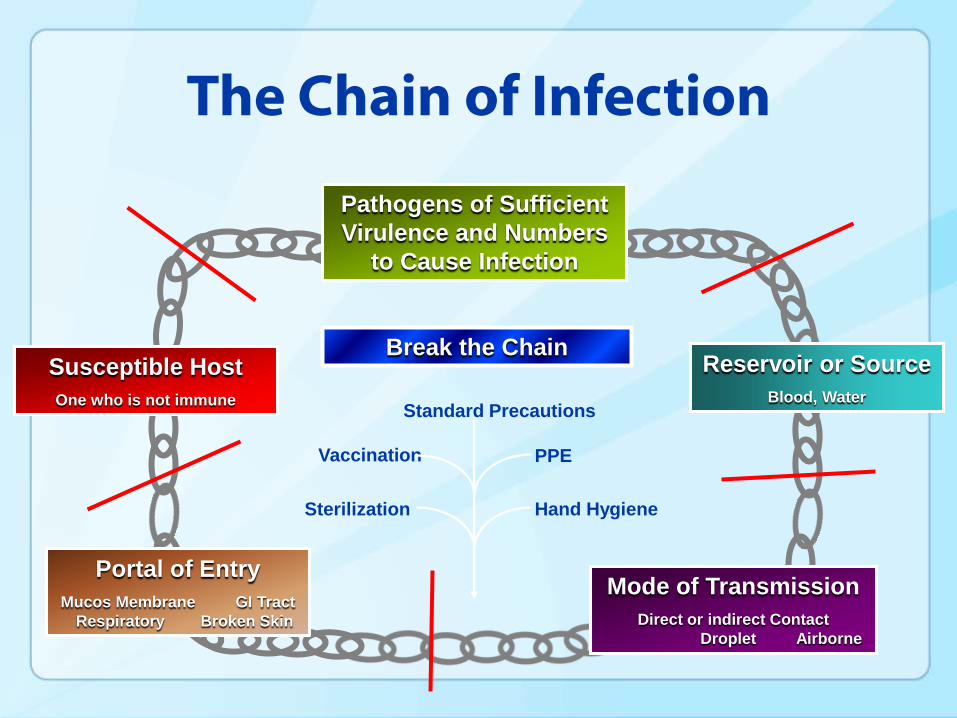
The Chain of Infection
Standard Precautions
Sterilization
Vaccination
Hand Hygiene
PPE
Portal of Entry
Mucos Membrane GI Tract
Respiratory Broken Skin
Pathogens of Sufficient
Virulence and Numbers
to Cause Infection
Susceptible Host
One who is not immune
Mode of Transmission
Direct or indirect Contact
Droplet Airborne
Reservoir or Source
Blood, Water
Break the Chain
Summary
A variety of infectious agents can be transmitted in ambulatory healthcare settings through contact, droplet and airborne modes
Standard precautions remain the major infection prevention strategy to prevent transmissions
Hepatitis B and C virus transmission in healthcare remain preventable risks
Standard Precautions
• Synthesize major features of Universal Precautions
– Applies to all patients regardless of diagnosis or infection status
– Includes blood and all body fluids except sweat (includes saliva in all settings)
• May be supplemented by special isolation precautions for diseases transmitted by contact, droplet or airborne routes
Guideline for Isolation Precautions in Hospitals
Epidemiol 1996;17:53-80, and Am J Infect Control 1996;24:24-52.
Standard Precautions
• MUST be used in the care of all patients regardless of their infection status.
• Some patients require additional measures = ‘transmission-based precautions’– Interrupt potential spread of diseases via
airborne, droplet, or contact transmission.
– e.g. TB, influenza, and chickenpox
– Spread via coughing, sneezing or contact with skin.
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf.
Transmission-Based Precautions
Pathogen and syndrome-based precautions, termed transmission-based precautions, for the care of patients who are infected or colonized with pathogens spread through airborne, droplet, or contact routes.
• Standard Precautions +…..
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf. Guidelines for infection control in dental health-care settings—2003. http://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
Standard Precautions +
TRANSMISSION-BASED PRECAUTIONS
• Transmission-based precautions are designed for patients documented or suspected to be infected or colonized with pathogens that require additional precautions beyond the standard precautions necessary to interrupt transmission.
• These precautions apply to airborne, droplet, and contact transmissions. The precautionsmay be combined for diseases that have multiple routes of transmission.
• Whether singly or in combination, they are always to be used in addition to standard precautions.
Transmission-Based Precautions• Might include:
• Patient placement (e.g., isolation)
• Adequate room ventilation
• Respiratory protection (e.g., N-95 masks) for dental health-care personnel (DHCP)
• Postponement of nonemergency dental procedures.
• More than 1 transmission category may apply
• Always used IN ADDITION to Standard Precautions
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf. Guidelines for infection control in dental health-care settings—2003. http://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
Contact PrecautionsContact transmission, the most important and frequent mode of transmission of heahcare-associated infections, is divided into two subgroups:
direct-contact transmission
indirect-contact transmission
Example: MRSA
Contact: Droplet Precautions• Droplet transmission,
theoretically, is a form of contact transmission. However, the mechanism of transfer of the pathogen to the host is quite distinct from either direct- or indirect-contact transmission. Therefore, droplet transmission is considered a separate route of transmission
• Examples:– Influenza– Chickenpox
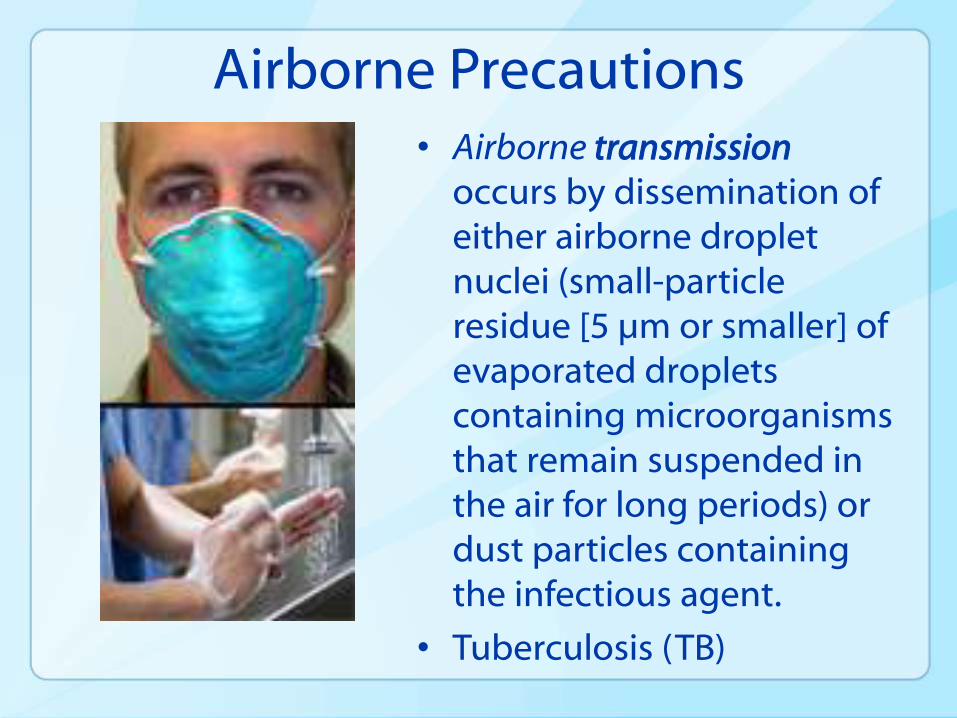
Airborne Precautions• Airborne transmission
occurs by dissemination of either airborne droplet nuclei (small-particle residue [5 µm or smaller] of evaporated droplets containing microorganisms that remain suspended in the air for long periods) or dust particles containing the infectious agent.
• Tuberculosis (TB)
2014 Ebola Outbreak Response
West Africa
• Centers for Disease Control and Prevention
• Ebola Response 2014
2014 Ebola Outbreak
Healthcare Providers in the United States CDC encourages all U.S. healthcare providers to:
Ask patients about their travel histories to determine if they have traveled to West Africa within the last three weeks
Know the signs and symptoms of Ebola – fever (greater than 100.4°F or 38°C), severe headache, muscle pain, vomiting, diarrhea, abdominal (stomach) pain, or unexplained hemorrhage (bleeding or bruising)
Know what to do if they have a patient with Ebola symptoms:
• First, properly isolate the patient
• Then, follow infection control precautions to prevent the spread of Ebola.
• Avoid contact with blood and body fluids of infected people
Infection Control Principles
Early recognition Early recognition is critical for infection control
Patient Placement Patients should be placed in a single patient room containing a
private bathroom with the door closed
Protecting healthcare providers IDENTIFY-ISOLATE-INFORM
Guidance for hospitals available at: http://www.cdc.gov/vhf/ebola/hcp/infection-prevention-and-control-recommendations.html
Guidance for emergency departments available at: http://www.cdc.gov/vhf/ebola/hcp/ed-management-patients-possible-ebola.html
Guidance for ambulatory care settings in development
Elements of Standard Precautions
• Handwashing
• Personal protective equipment
• Sterilization of instruments and devices
• Cleaning/disinfecting environmental surfaces
• Engineering/work practice controls
• Respiratory hygiene/cough etiquette
• Safe injection practices
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf.
Acknowledge:CAPT Raymond A. Strikas, MD, MPH, FACP, FIDSASarah Schillie, MD, MPH, MBA
www.cdc.gov/mmwr/preview/mmwrhtml/rr6007a1.htm?s_cid=rr6007a1_e
Immunization of Health-Care Personnel
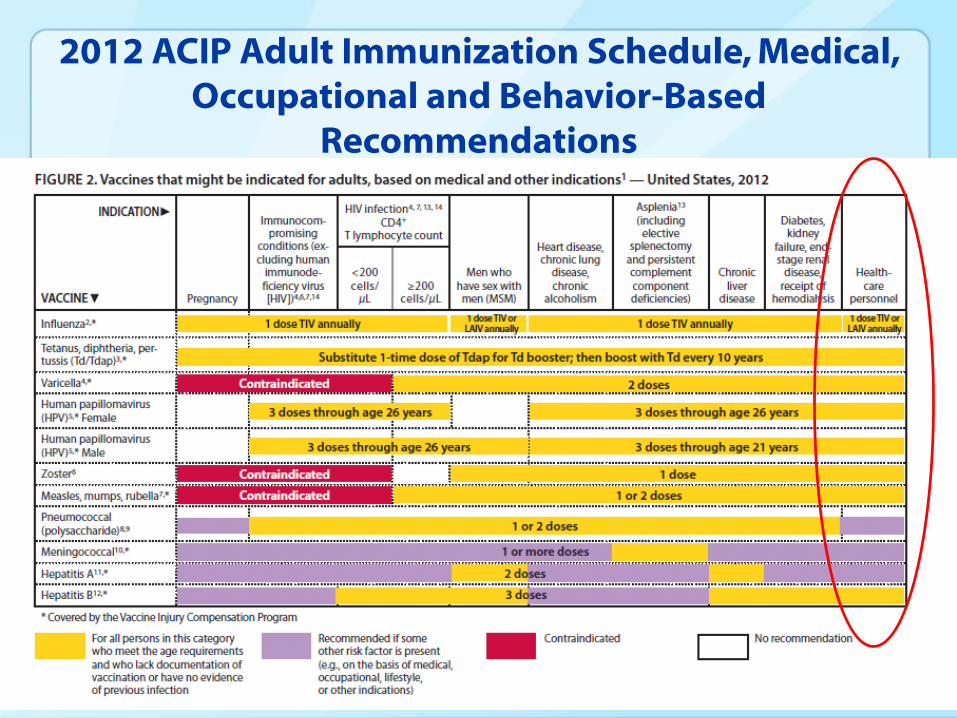
2012 ACIP Adult Immunization Schedule, Medical, Occupational and Behavior-Based
Recommendations
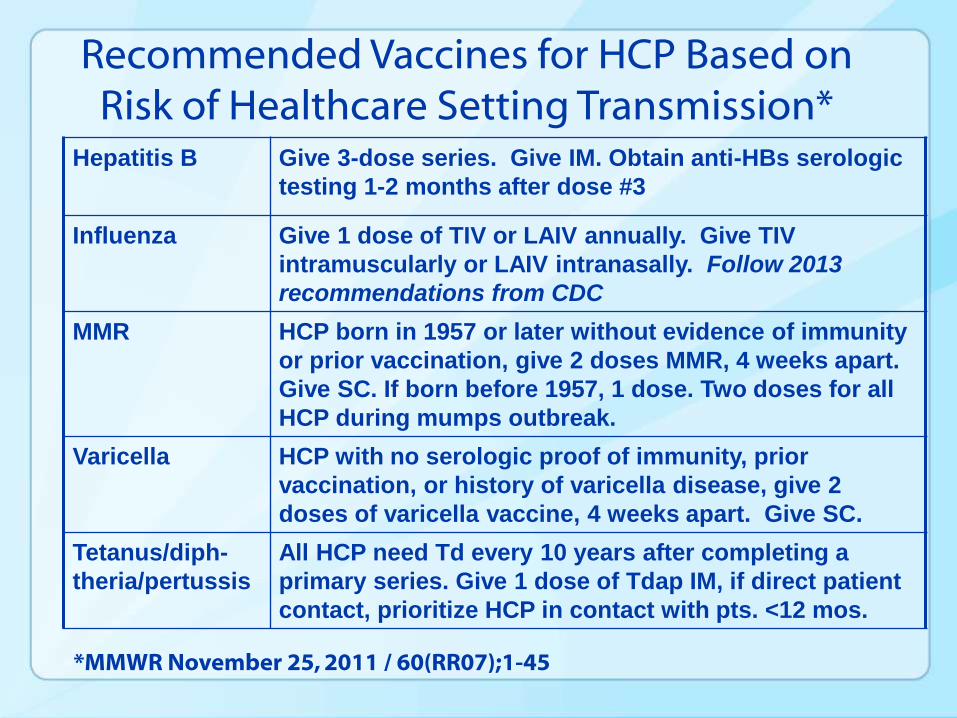
Recommended Vaccines for HCP Based on Risk of Healthcare Setting Transmission*
*MMWR November 25, 2011 / 60(RR07);1-45
Hepatitis B Give 3-dose series. Give IM. Obtain anti-HBs serologic
testing 1-2 months after dose #3
Influenza Give 1 dose of TIV or LAIV annually. Give TIV
intramuscularly or LAIV intranasally. Follow 2013
recommendations from CDC
MMR HCP born in 1957 or later without evidence of immunity
or prior vaccination, give 2 doses MMR, 4 weeks apart.
Give SC. If born before 1957, 1 dose. Two doses for all
HCP during mumps outbreak.
Varicella HCP with no serologic proof of immunity, prior
vaccination, or history of varicella disease, give 2
doses of varicella vaccine, 4 weeks apart. Give SC.
Tetanus/diph-
theria/pertussis
All HCP need Td every 10 years after completing a
primary series. Give 1 dose of Tdap IM, if direct patient
contact, prioritize HCP in contact with pts. <12 mos.
39
CDC Recommendations for Hepatitis B Protection among HCP
(2013)
www.cdc.gov/mmwr/preview/mmwrhtml/rr6210a1.htm?s_cid=rr6210a1_w
HCP with Hepatitis B Vaccination in the Remote Past
40
Increasing proportion of HCP entering training and workforce have received HepB vaccination as infants or in the remote past
Anti-HBs testing not recommended after routine infant HepB vaccination
Anti-HBs after vaccination wanes over time, although protection believed to persist
HCP with Hepatitis B Vaccination in the Remote Past
(with Documentation of Complete, ≥3-dose HepB vaccine series)
41
May undergo anti-HBs testing upon hire or matriculation
Anti-HBs ≥10 mIU/mL: Considered immune
Anti-HBs <10 mIU/mL: 1 additional dose of HepBvaccine, followed by anti-HBs testing 1-2 months later
• HCP whose anti-HBs remains <10 mIU/mL should receive 2 additional doses (usually 6 doses total), followed by repeat anti-HBs testing 1-2 months after last dose
Pre-exposure anti-HBs Testing HCP Vaccinated in the Remote Past
42
~72% of institutions measure anti-HBs upon hire/matriculation for remotely vaccinated HCP
Advantages
Results in fewer cases of occupational Hepatitis B
transmission
Provides greatest protection for HCP (including protection against unrecognized/unreported exposures)
More cost-effective over time • 2013 MMWR

INFLUENZA VACCINE
Tools for the Prevention of Influenza
Influenza vaccine
Antiviral medications Can be used for treatment or prevention (prophylaxis)
Hand hygiene
Masks
Respirators
Environmental controls E.g. ensuring appropriate ventilation, air exchange, physical
barriers, etc.
Influenza Vaccine
Primary means for preventing influenza
Recommended annually for all people 6 months of age and older Including pregnant women
Including healthcare personnel
“Insurance” against infection
Benefit to those vaccinated plus decreases risk of spreading influenza to others Not 100% effective
Need to use other tools in addition to vaccination
Influenza and Vaccination
Four types of influenza vaccines available:
Traditional inactivated (“killed”) influenza vaccine injected in muscle • anyone 6 months of age or older
Nasal spray vaccine (LAIV): healthy individual• ages 2-49 years
• HCP not working with patients in a protected environment
High-dose inactivated injectable vaccine • 65 years and older
Intradermal inactivated vaccine: uses very small needle• 18-64 years old
Influenza and Mask or Respirator Use
Relatively few clinical studies done to assess reduction in influenza illness in clinical setting for masks or respirators
Household transmission studies and one study of college students found
Limited reductions with mask +/- hand hygiene when
• High levels of compliance with mask use
• Early initiation of mask use
No reductions in influenza with increase in hand hygiene alone
Study of 2009 H1N1 in hospital workers
Masks likely helpful
Emergency Department workers more likely to become ill with influenza than other types of workers
• May have been related to lack of wearing mask with first encounter with patient
Apisarnthanarak CID 2012; Vanhems Archives Intern Med 2011; Aiello JID 2010; Cowling Epi Infect 2010; Aiello AJPH 2008
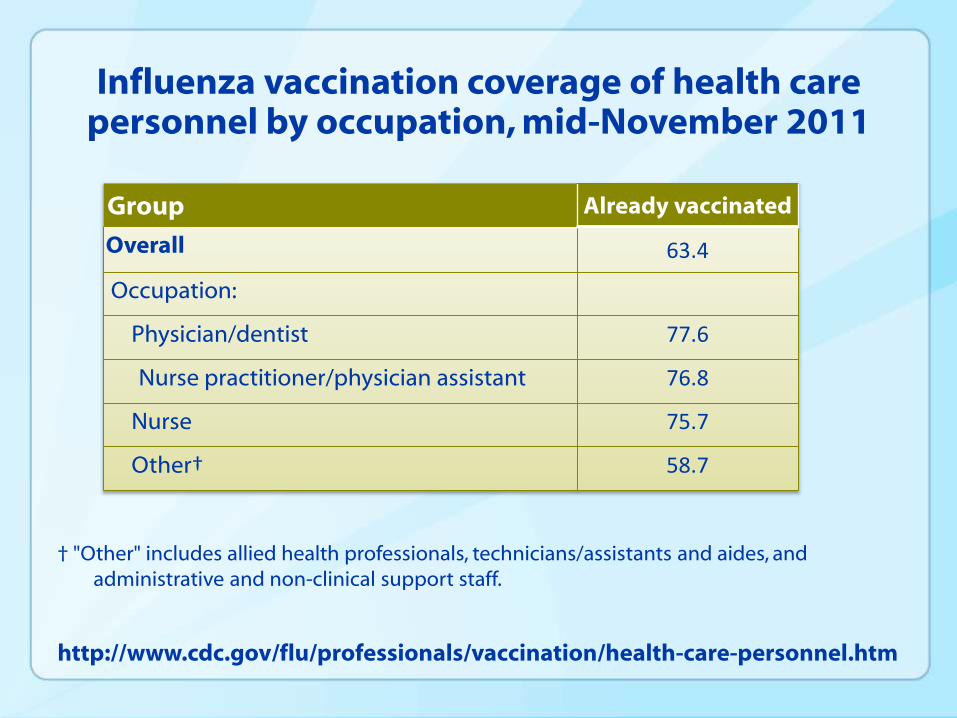
Influenza vaccination coverage of health care personnel by occupation, mid-November 2011
† "Other" includes allied health professionals, technicians/assistants and aides, and administrative and non-clinical support staff.
Group Already vaccinated
Overall 63.4
Occupation:
Physician/dentist 77.6
Nurse practitioner/physician assistant 76.8
Nurse 75.7
Other† 58.7
http://www.cdc.gov/flu/professionals/vaccination/health-care-personnel.htm
Conclusions for Influenza
Many tools for influenza prevention, but vaccination is the primary means to prevent influenza
Best insurance against influenza infection and transmission to HCP family, friends, coworkers and patients
Vaccination should be used in conjunction with other influenza prevention tools to most effectively decrease the spread of influenza
Common Reasons HCP and Adult Patients Might Give for Not Getting Vaccinated
10. Vaccine preventable diseases are a thing of the past.
9. Vaccines don’t work.
8. I am great at washing my hands.
7. I always put on a mask before I am near patients that may have [INSERT DISEASE HERE].
6. I never come to work sick.
5. Vaccines will make me sick.
4. It is easier to deal with the rare case than to vaccinate routinely.
3. My patients are already vaccinated so I don’t need to be.
2. The healthcare facility where I work doesn’t require vaccines.
1. My doctor didn’t recommend any vaccines for me.

Summary
Outbreaks of vaccine preventable diseases continue to occur
Result in health risks to patients and HCP and their families
Very disruptive and expensive to investigate and manage
Can be difficult to recognize early and before many people have been exposed
Exposures and illnesses can result in substantial lost work time as early awareness and implementation of control measures challenging
Conclusions
Vaccines have been highly successful in reducing the burden of many diseases
Vaccination are a critical component of infection control to protect HCP and their patients, coworkers and families
DHCP should be
Assessed for vaccination and immunity status at the time of hire and at least annually to ensure they are up to date with recommended vaccines.
Provided with information about risks and benefits of the vaccines
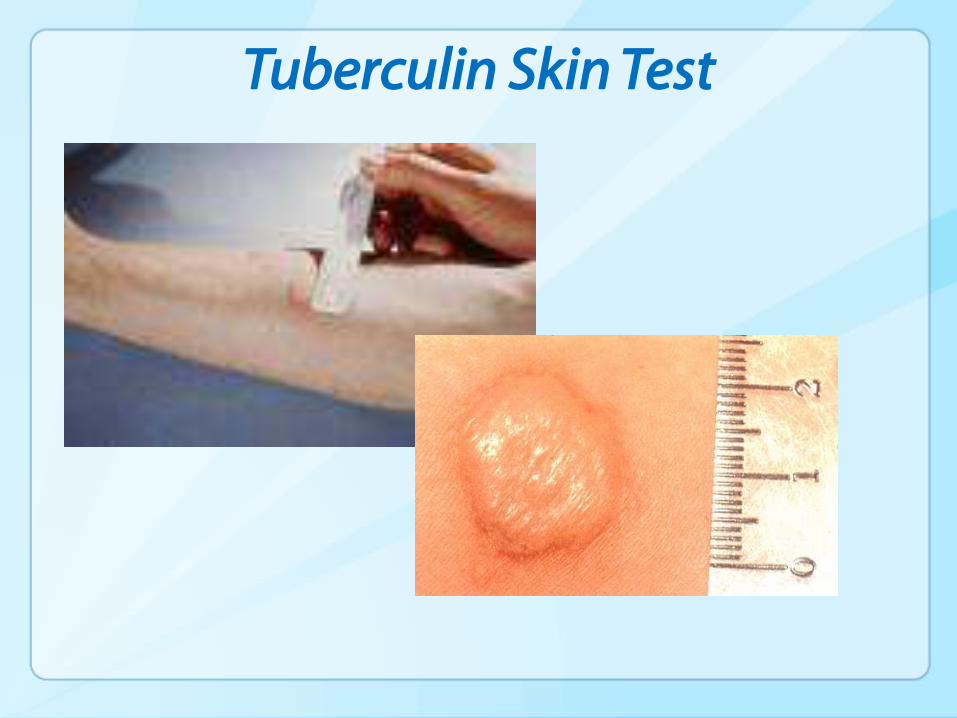
Tuberculin Skin Test
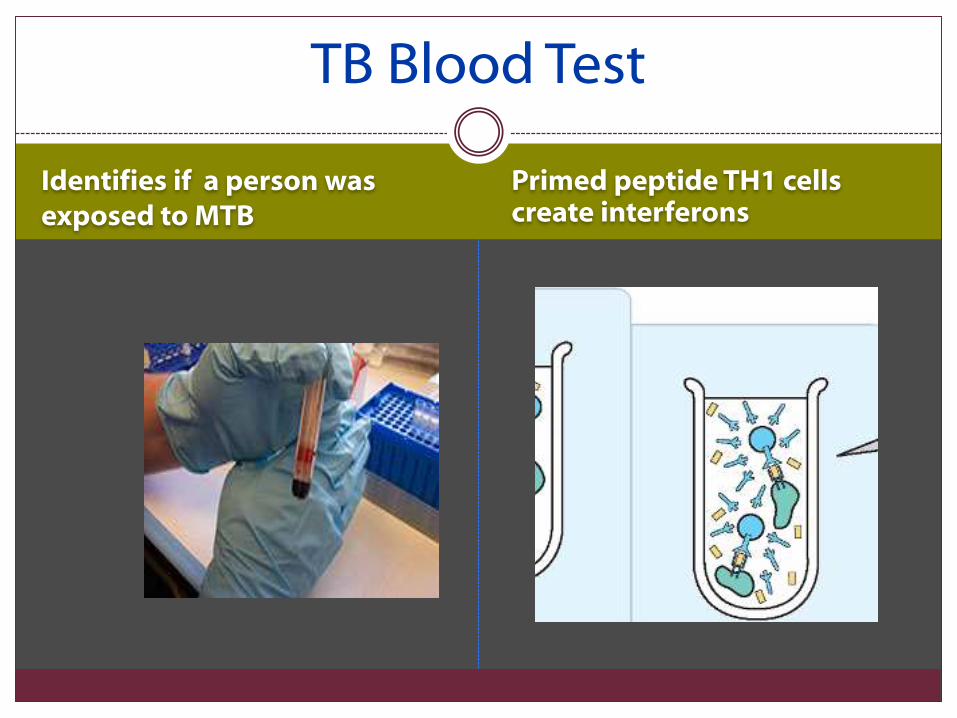
TB Blood Test
Identifies if a person was exposed to MTB
Primed peptide TH1 cells create interferons
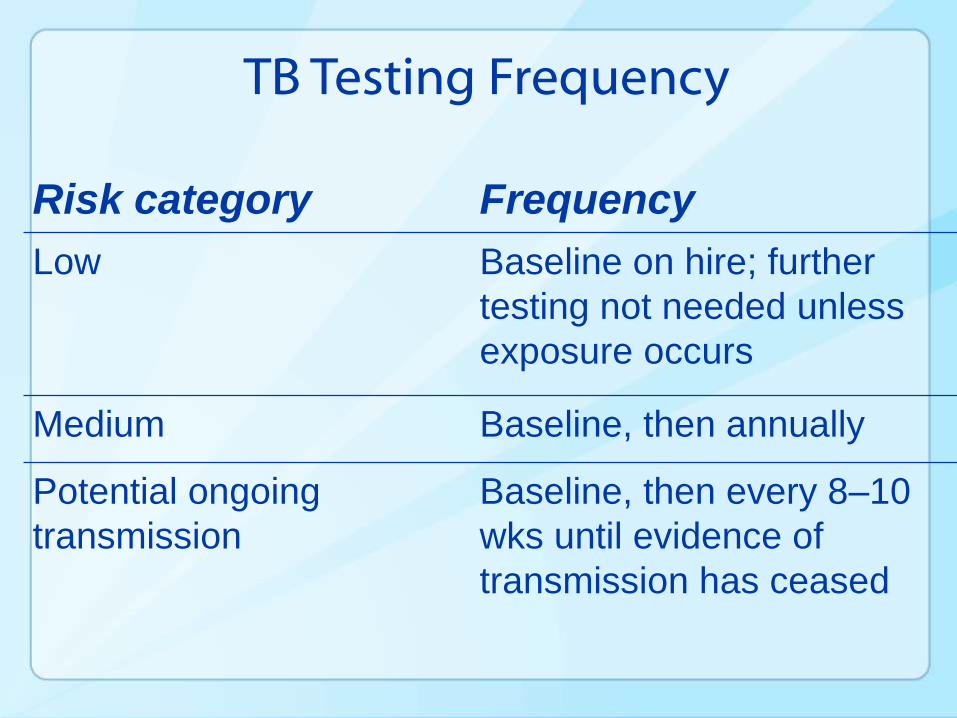
TB Testing Frequency
Risk category Frequency
Low Baseline on hire; further
testing not needed unless
exposure occurs
Medium Baseline, then annually
Potential ongoing
transmission
Baseline, then every 8–10
wks until evidence of
transmission has ceased
Program Evaluation: Immunization of HCP
• Program Element
– Appropriate immunization of health-care personnel (HCP).
• Develop and implement a program that promotes immunity of health-care personnel according to current CDC ACIP recommendations for health-care personnel.
– HBV Vaccine: OSHA Bloodborne Pathogens Standard Regulate Employer provide Education and Training, access to HBV vaccine during normal working hours, and pay for the vaccine. If employee refuses, the OSHA Declination form must be signed, but employee can change his/her mind.
– Other CDC recommended vaccines………
• Evaluation Activity
– Conduct an annual review of personnel records to ensure up-to-date immunizations.
• Keep updated immunization records of personnel.
• Refer non-immune personnel to a qualified health-care provider for evaluation and indicated vaccinations/immunizations.
Work Restrictions of HCP
Medical Conditions, Work-Related Illness,
and Work Restrictions
• HCP are responsible for monitoring their own health status. HCP who have acute or chronic medical conditions that render them susceptible to opportunistic infection should discuss with their personal physicians or other qualified authority whether the condition might affect their ability to safely perform their duties.
• Under certain circumstances, health-care facility managers might need to exclude HCP from work or patient contact to prevent further transmission of infection (e.g., conjunctivitis, influenza, etc.)
Medical Conditions, Work-Related Illness, and Work Restrictions
• Under certain circumstances, health-care facility managers might need to exclude HCP from work or patient contact to prevent further transmission of infection (e.g., conjunctivitis, influenza, etc.)
• Managers may exclude HCP from patient contact to prevent transmission
– Work restrictions based on mode of transmission and period of infectivity
– Written policies should define who can exclude HCP (e.g., personal physicians) and be clearly communicated
Medical Conditions, Work-Related Illness, and Work Restrictions
Decisions concerning work restrictions are based on the mode of transmission and the period of infectivity of the disease.
Medical Conditions, Work-Related Illness and Work Restrictions
• Exclusion policies should
– 1) be written,
– 2) include a statement of authority that defines who can exclude DHCP (e.g., personal physicians), and
– 3) be clearly communicated through education and training. Policies should also encourage DHCP to report illnesses or exposures without jeopardizing wages, benefits, or job status.
Medical Conditions, Work-Related Illness and Work Restrictions
Policies should encourage DHCP to report illnesses or exposures without jeopardizing wages, benefits, or job status.
Work Restrictions: Influenza• Self-assess daily for symptoms
of febrile respiratory illness (fever plus one or more of the following:
– nasal congestion/runny nose,
– sore throat
– cough.
• Personnel who develop fever and respiratory symptoms should promptly notify their supervisor and should not report to work.
Work Restrictions - Influenza
Personnel should remain at home until at least 24 hours after they are free of fever (100°F/37.8°C), or signs of a fever, without the use of fever-reducing medications.

Resource: Preventing Transmission of Influenza in Healthcare Settings
• http://www.cdc.gov/flu/pdf/infectioncontrol_seasonalflu_ICU2010.pdf
• On July 29, 2010, CDC issued Recommendations for the Prevention and Control of Influenza
• http://www.cdc.gov/flu/professionals/infectioncontrol/healthcaresettings.htm
• http://www.cdc.gov/flu/professionals/infectioncontrol/
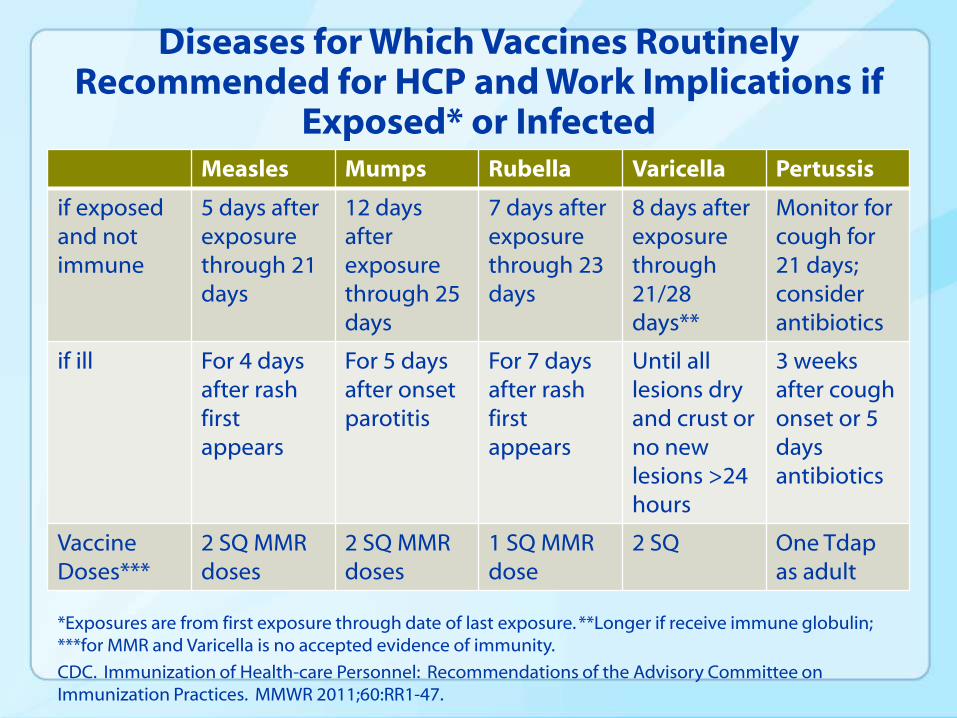
Diseases for Which Vaccines Routinely Recommended for HCP and Work Implications if
Exposed* or InfectedMeasles Mumps Rubella Varicella Pertussis
if exposed and not immune
5 days after exposure through 21 days
12 days afterexposure through 25 days
7 days after exposurethrough 23 days
8 days after exposurethrough 21/28 days**
Monitor for cough for 21 days; consider antibiotics
if ill For 4 days after rashfirst appears
For 5 days after onset parotitis
For 7 days after rash first appears
Until all lesions dryand crust or no new lesions >24 hours
3 weeks after cough onset or 5 days antibiotics
Vaccine Doses***
2 SQ MMR doses
2 SQ MMR doses
1 SQ MMR dose
2 SQ One Tdapas adult
*Exposures are from first exposure through date of last exposure. **Longer if receive immune globulin; ***for MMR and Varicella is no accepted evidence of immunity.
CDC. Immunization of Health-care Personnel: Recommendations of the Advisory Committee on Immunization Practices. MMWR 2011;60:RR1-47.
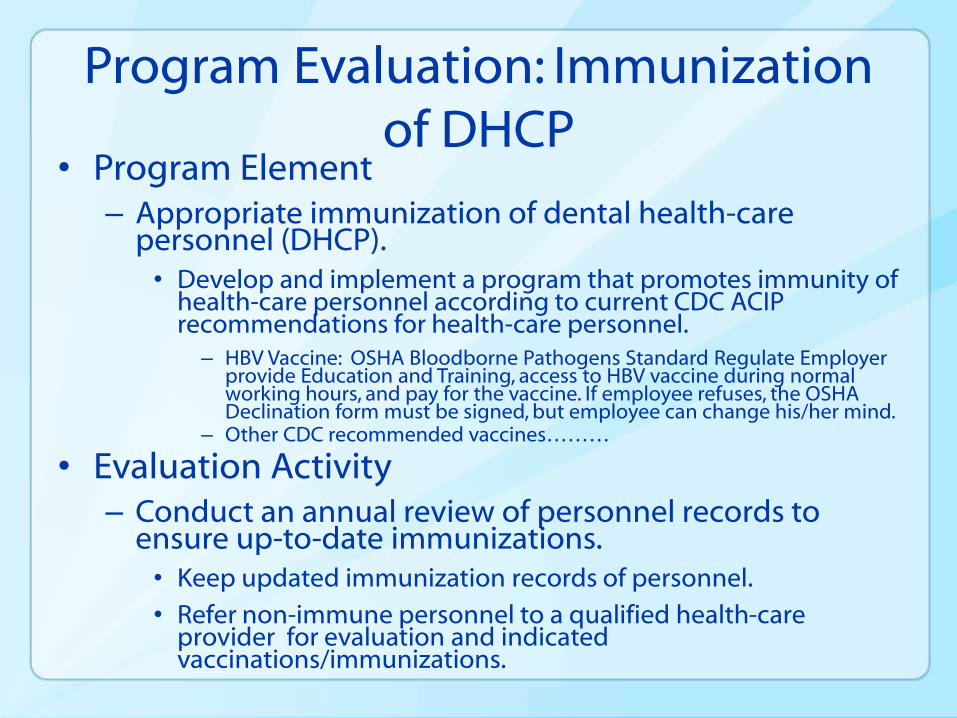
Program Evaluation: Immunization of DHCP
• Program Element– Appropriate immunization of dental health-care
personnel (DHCP). • Develop and implement a program that promotes immunity of
health-care personnel according to current CDC ACIP recommendations for health-care personnel.
– HBV Vaccine: OSHA Bloodborne Pathogens Standard Regulate Employer provide Education and Training, access to HBV vaccine during normal working hours, and pay for the vaccine. If employee refuses, the OSHA Declination form must be signed, but employee can change his/her mind.
– Other CDC recommended vaccines………
• Evaluation Activity– Conduct an annual review of personnel records to
ensure up-to-date immunizations.• Keep updated immunization records of personnel.
• Refer non-immune personnel to a qualified health-care provider for evaluation and indicated vaccinations/immunizations.
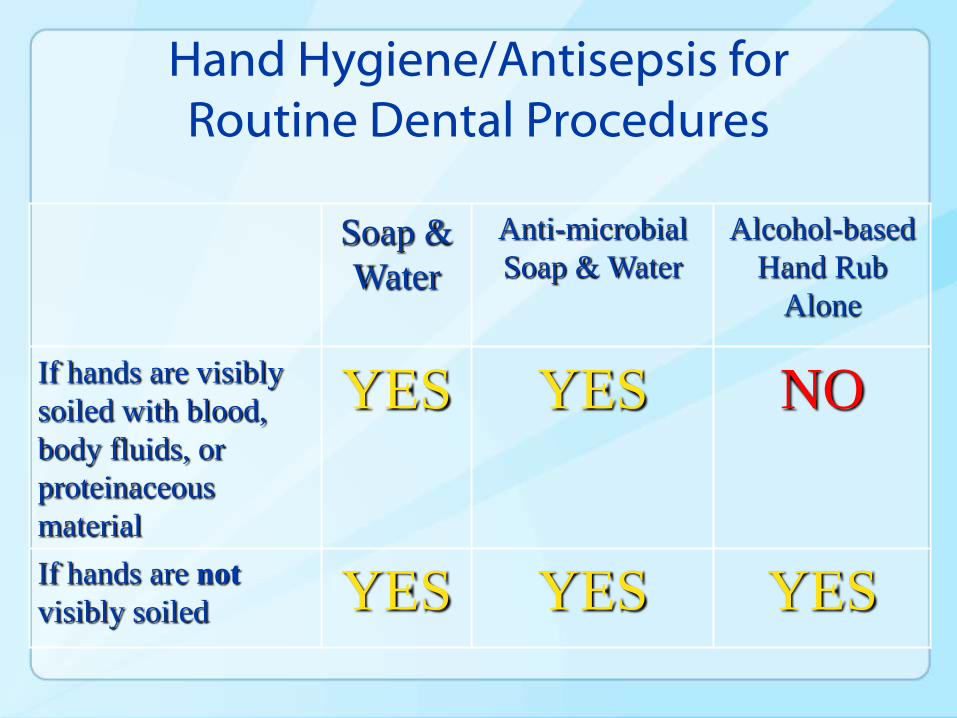
Hand Hygiene/Antisepsis for Routine Dental Procedures
Soap &
Water
Anti-microbial
Soap & Water
Alcohol-based
Hand Rub
Alone
If hands are visibly
soiled with blood,
body fluids, or
proteinaceous
material
YES YES NO
If hands are not
visibly soiled YES YES YES
In the News…
December 13, 2013
70
• FDA issues proposed rule to determine safety and effectiveness of over the counter antibacterial soaps
– http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm378542.htm
– proposed rule to require manufacturers of antibacterial hand soaps and body washes to demonstrate that their products are safe for long-term daily use and more effective than plain soap and water in preventing illness and the spread of certain infections.
– Under the proposal, if companies do not demonstrate such safety and effectiveness, these products would need to be reformulated or relabeled to remain on the market.
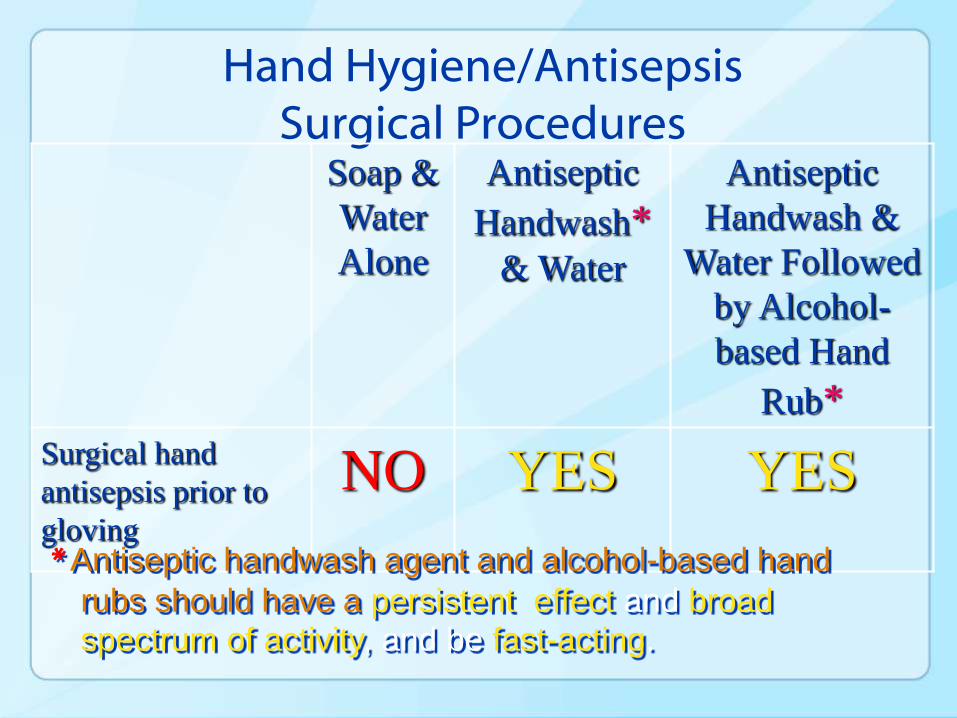
Hand Hygiene/AntisepsisSurgical Procedures
Soap &
Water
Alone
Antiseptic
Handwash*& Water
Antiseptic
Handwash &
Water Followed
by Alcohol-
based Hand
Rub*
Surgical hand
antisepsis prior to
gloving
NO YES YES
* Antiseptic handwash agent and alcohol-based hand
rubs should have a persistent effect and broad spectrum of activity, and be fast-acting.
PPE
• Wear long-sleeved disposable or reusable gowns, lab coats, or uniforms that cover skin and personal clothing likely to be soiled with blood, saliva or infectious material
• Change if visible soiled, or as soon as possible
• Remove all barriers before leaving patient care or laboratory areas
72
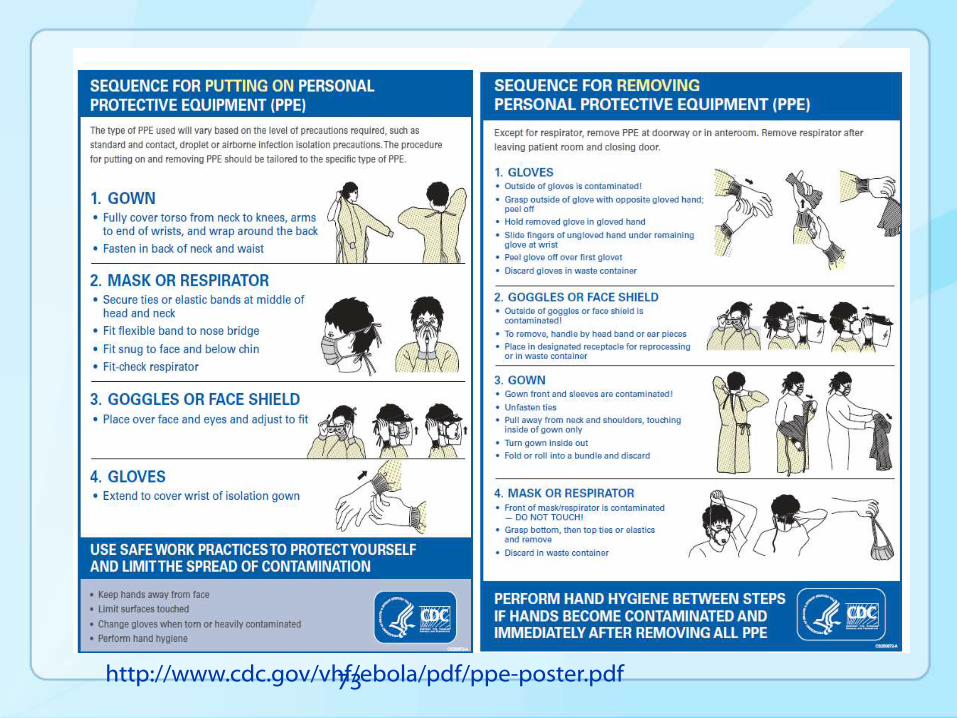
73http://www.cdc.gov/vhf/ebola/pdf/ppe-poster.pdf
New Elements to Standard Precautions (2007)
• ‘Infection control problems that are identified in the course of outbreak investigations often indicate the need for new recommendations or reinforcement of existing infection control recommendations to protect patients.’
• Two areas of practice relevant to dentistry added:
– Respiratory Hygiene/Cough Etiquette
– Safe Injection Practices
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf.
Respiratory Hygiene/Cough Etiquette
• Grew out of observations during severe acute respiratory syndrome (SARS) outbreaks where failures to implement simple source control measures with patients, visitors, and health-care personnel with respiratory symptoms may have contributed to SARS-coronavirus (SARS-CoV) transmission.
• Conclusions of the investigations of transmissions that could have been prevented by adherence to basic principals of aseptic technique for the preparation and administration of parenteral medications
Safe Injection Practices
Respiratory Hygiene/Cough Etiquette
• Cover your mouth and nose with a tissue when coughing or sneezing;
• Use in the nearest waste receptacle to dispose of the tissue after use;
• Perform hand hygiene after having contact with respiratory secretions and contaminated objects/materials.
http:///www.cdc.gov/flu/professionals/infectioncontrol/resphygiene.htm
Supplies for Patient Areas
Kleenex
Hand sanitizer
Masks – specifications
and proper use
• Identify patients with signs and symptoms of fever and cough.
• Place symptomatic patients in separate room.
• Give patient surgical face mask
• Contact providers should wear at least surgical face mask.
http://www.health.state.mn.us/divs/idepc/dtopics/infectioncontrol/cover/hcp/notice.pdf
Safe Injection Practices
• Safe Injection Practices are a set of recommendations within Standard Precautions, which are the foundation for preventing transmission of infections during patient care in all healthcare settings
Note: In dentistry, generally applies to administration of parenteral medications not related to local anesthesia.
http://www.cdc.gov/injectionsafety/IP07_standardPrecaution.html
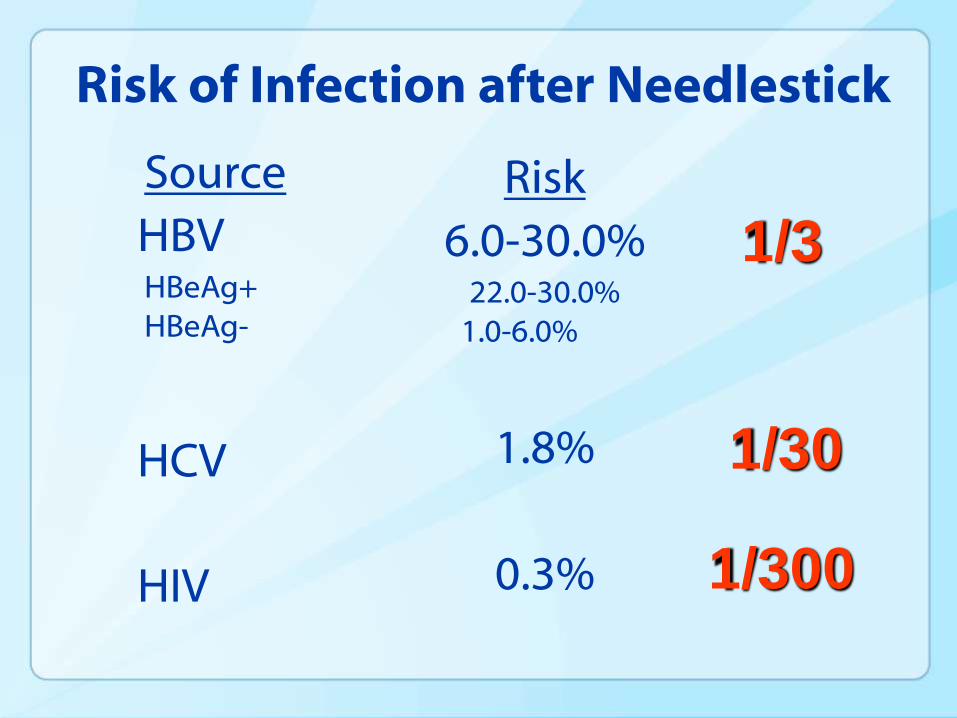
Risk of Infection after Needlestick
Source
HBVHBeAg+HBeAg-
HCV
HIV
Risk
6.0-30.0%22.0-30.0%
1.0-6.0%
1.8%
0.3%
1/3
1/300
1/30
Safe Injection Practices = Aseptic Technique for Parenteral Medications
• Do not administer medications from a syringe to multiple patients, even if the needle on the syringe is changed (IA) (378).
• Use single-dose vials for parenteral medications when possible (II) (376,377).
• Do not combine the leftover contents of single-use vials for later use (IA) (376,377).
• Use fluid infusion and administration sets (i.e., IV bags, tubing and connections) for one patient only and dispose of appropriately (IB) (378).
CDC 2007 Guideline for Isolation Precautionshttp://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf. Guidelines for infection control in dental health-care settings—2003. http://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
Environmental Surfaces
Clinical Contact Housekeeping
Environmental Stability
• HBV can survive in dried blood on environmental surfaces for at least one week.
• In vitro studies have shown the HCV can remain infective on dry surfaces for up to 6 weeks.
• HBV and HCV transmission via contact with environmental surfaces has been demonstrated in investigations of outbreaks among patients and staff of hemodialysis units.
Bond WW et al, Lancet 1981Kamili S et al, Infect Control Hosp Epidemiol 2007Paintsil E, J Infect Dis 2014.
• Remove
• Replace• Spray
• Clean/wipe
• Spray
Barriers VS. Cleaning and Disinfection
84
Clean and disinfect using an EPA registered low- ( HIV/HBV claim) to intermediate- (tuberculocidal claim) level hospital disinfectant
Premoistened Disinfectant Wipes
• Wipe (clean)
• Wipe (disinfect)
• Wait (manufacturer’s claim)
• Follow specific Product Manufacturer’s Instructions for use.
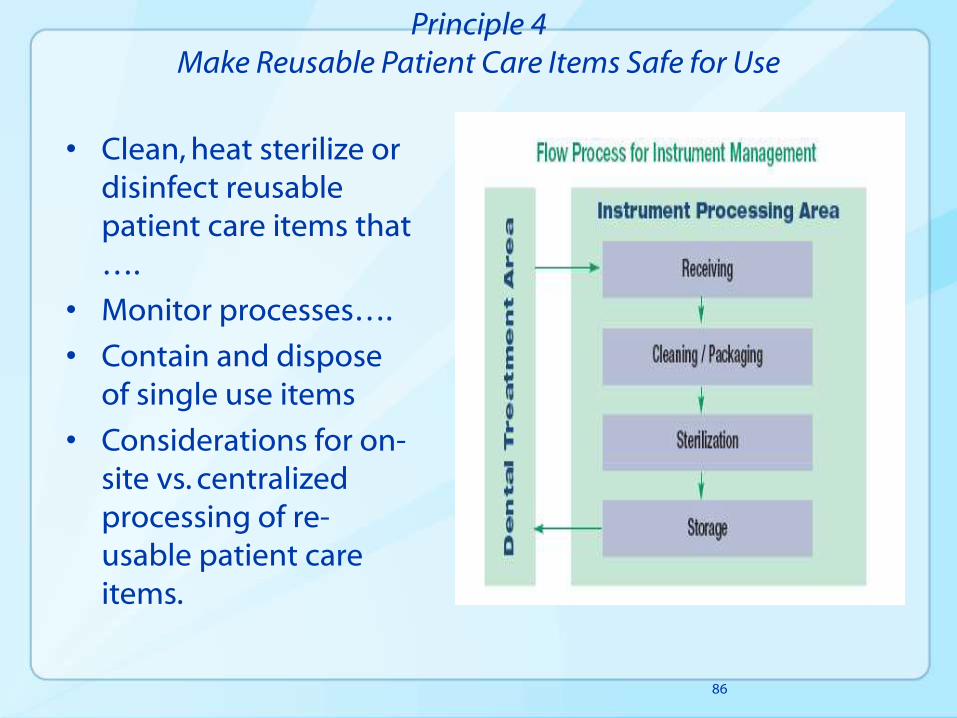
Principle 4Make Reusable Patient Care Items Safe for Use
• Clean, heat sterilize or disinfect reusable patient care items that ….
• Monitor processes….
• Contain and dispose of single use items
• Considerations for on-site vs. centralized processing of re-usable patient care items.
86
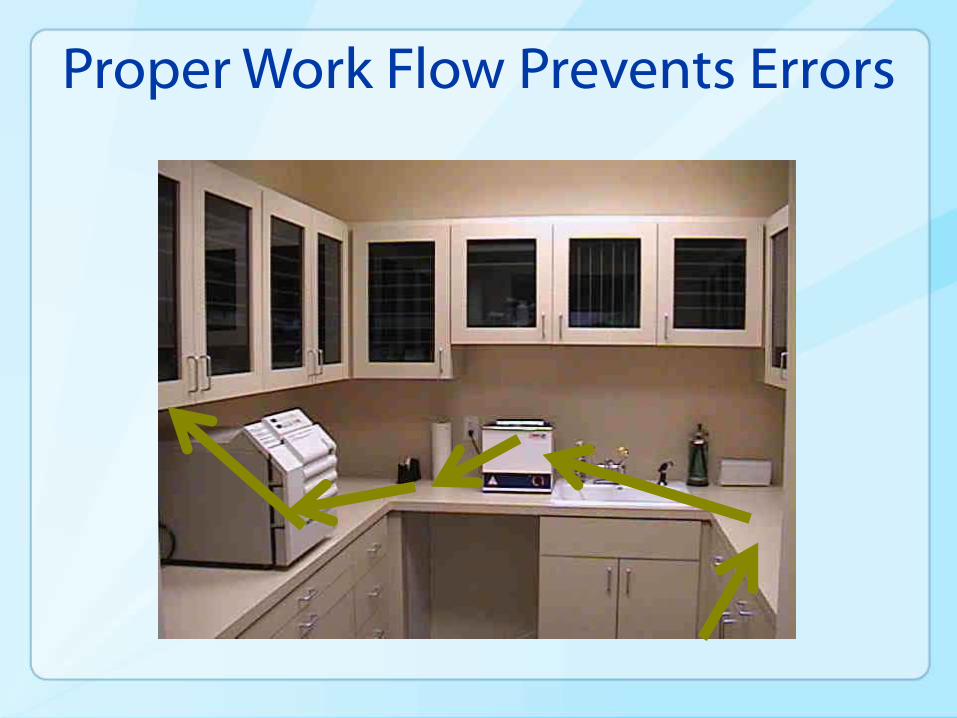
Proper Work Flow Prevents Errors
“Program evaluation provides an
opportunity to identify and change
inappropriate practices, thereby
improving the effectiveness of your
infection control program.”
• Centers for Disease Control (CDC) “Guidelines for Infection Control in Dental Health-Care Settings – 2003”
Implementing Change
Proactive
Reactive
Program Evaluation
• Strategies and Tools
–Periodic observational assessments
–Checklists to document procedures
–Routine review of occupational exposures to bloodborne pathogens
Checklists for Repeatable Processes
• Remind individuals of critical steps to complete each time
• Provide verification that the steps have been completed
• Create a history that can be reconstructed if there is an adverse event
2011
Guide and Checklist for Outpatient Settings
http://www.cdc.gov/HAI/settings/outpatient/outpatient-settings.html
2011 Guide Summary
Basic infection prevention recommendations for outpatient settings Administrative measures
• Education and training of all HCP
• Report process and outcome measures
Standard Precautions Hand hygiene PPE
Injection safety Environmental cleaning
Medical equipment Resp hygiene/cough etiquette
Resources Disinfection and sterilization
FDA device information
Transmission based precautions
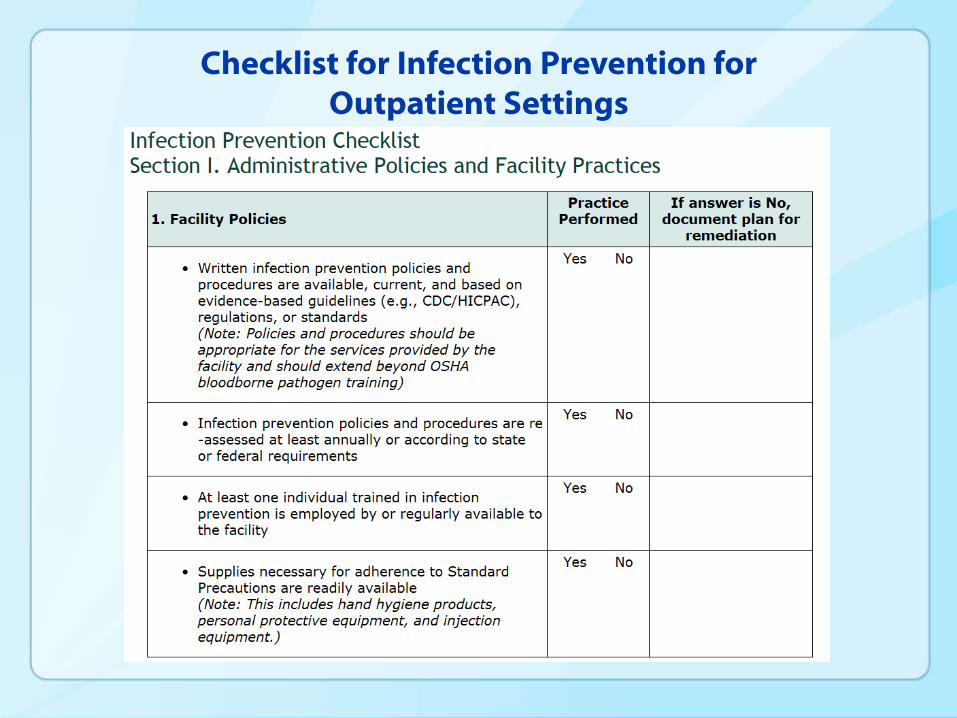
Checklist for Infection Prevention for Outpatient Settings
Thank You