evaluating induction-salvage treatment regimes in therapy of aml/mds wahed and thall, “evaluating...
TRANSCRIPT

Evaluating Induction-Salvage Treatment Regimes in Therapy of AML/MDS
Wahed and Thall, “Evaluating joint effects of induction-salvage treatment regimes on overall survival in acute leukemia.” J. Royal Statistical Society, Series C. In press.

Example 1: Treating Severe Infection
Each “stage” of therapy is approximately one week.
Stage 1 Based on the patient’s type of infection and characteristics, choose an antibiotic and a dose.
a) “Success” = Infection is resolved within 1 weekb) “Failure” = The patient diesc) If the patient is alive with infection Go to Stage 2
Stage 2 Based on the patient’s updated characteristics, choose a second, different antibiotic and dose.
a) “Success” = Infection is resolved within 1 weekb) “Failure” = The patient diesc) If the patient is alive with infection Go to Stage 3
And so on

BaselinePrognosticCovariates
Alive,Infection
Alive, No Infection
Antibiotic# 1
Death
Antibiotic# 2
The choice of Antibiotic # 2 may be informed by updated patient covariates, called “tailoring variables”
The Basic Algorithm :Try something. If it doesn’t work, try something else. Repeat as needed.
Repeat, until “Death” or “Alive, No Infection”

Example 2: A Trial of 12 Dynamic Treatment Regimes for Advanced Prostate Cancer
(Thall, Millikan, et al., Stat in Med, 2000; JNCI 2007, 2008; Wang, et al., J. American Statistical Assoc, In press.)
The Basic Idea: Try a chemo combination. If it works,
repeat it. If it fails, try something else.
Four chemo combinations (Chosen by R. Millikan, PI) TEE = Taxol / Estramustine / VP-16 (Etoposide) KAVE = Ketoconazole / Adriamycin / Vinblastin / VP-16 CVD = Cyclophosphamide / VCR / Dexamethasone TEC = Taxol / Estramustine / Carboplatin

First Success >40% drop in PSA from baselineRegression of any measurable diseaseImprovement in cancer-related symptomsNo new lesions or cancer-related symptoms
Second Success ( “Raise the bar” )>80% drop in PSA from baseline Resolution of all cancer-related symptomsTumor regression of > 50%No new lesions or cancer-related symptoms
Per-Course (8 week) Treatment Success(Also defined by R. Millikan)

Randy Millikan’s Dynamic Treatment Regime 1. Randomize each patient among the 4 treatments 2. Repeat a successful treatment, otherwise re-randomize the
patient among the other 3 treatments 3. Stop therapy if overall success or overall failure occurs
Overall Success = {2 consecutive successful courses}Overall Failure = {2 unsuccessful courses}
The first randomization was stratified by disease volume.Each patient received 2, 3, or 4 courses of chemotherapy. 4 Treatments 4x3 = 12 possible two-stage strategies
Goals: Estimate frontline agent effects, salvage agent effects,
and the effect of each two-stage regime

( TEE, TEC )
( TEE, CVD )
( TEE, KAVE )
TEE
KAVE
CVD
TEC
KAVE
CVD
TEE
KAVE
TEC
TEE
CVD
TEC
TEE
TEC
CVD
KAVE
( TEC, TEE )
( TEC, CVD )
( TEC, KAVE )
( CVD, TEE )
( CVD, TEC )
( CVD, KAVE )
( KAVE, TEE )
( KAVE, TEC )
( KAVE, CVD )
“The Scramble”
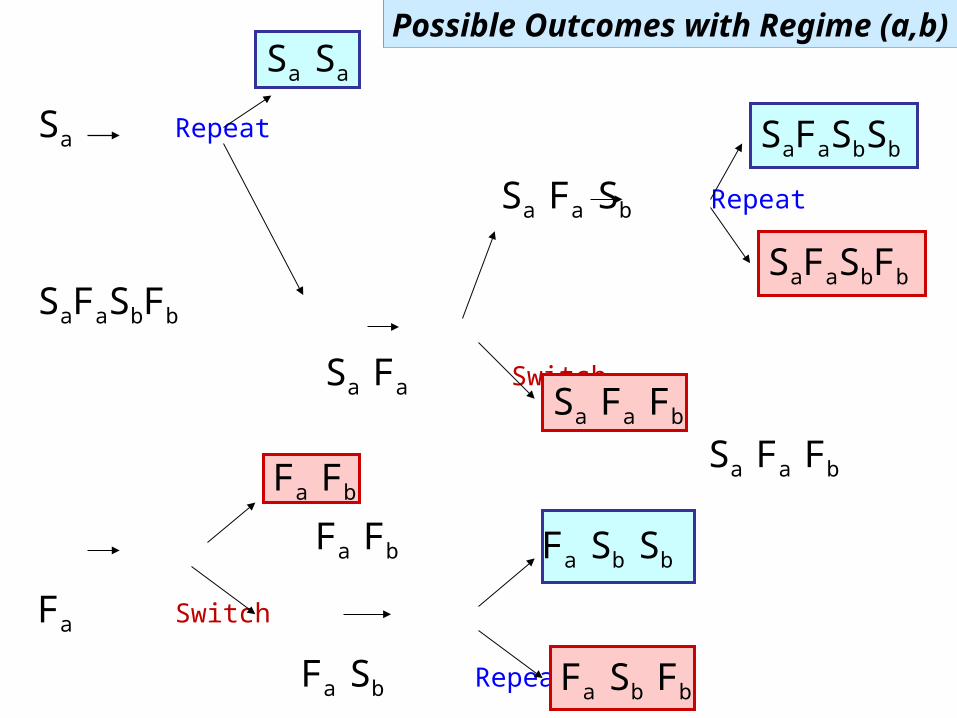
Sa Repeat
Sa Fa Sb Repeat
SaFaSbFb
Sa Fa Switch
Sa Fa Fb
Fa Fb
Fa Switch
Fa Sb Repeat
Fa Sb Fb
Sa Sa
Fa Sb Sb
Fa Sb Fb
Sa Fa Fb
SaFaSbSb
SaFaSbFb
Fa Fb
Possible Outcomes with Regime (a,b)

Armstrong et al. (letter to JNCI, 2008): “Because there was no docetaxel single-agent comparator arm in the study by Thall et al., it is difficult to judge the merits of this aggressive and toxic approach.”
Note: Their Docetaxel + Prednisone study was published in NEJM in 2004 . . . 6 years after “The Scramble” was started.
We used the fitted survival model of Armstrong et al., with our patients’ covariates, to estimate how long patients in “The Scramble” would have lived if they had been given Docetaxel + Prednisone. Then we wrote our own letter.
Love Letters

How long would the patients in “The Scramble” have lived if they had been treated with Docetaxel + Prednisone ?
Estimated Survival with Docetaxel + Prednisone
Kaplan-Meier Plot of Actual Survival Data
of the Patients in The Scramble
Possible Reasons Why Patients in The Scramble Survived Longer Compared to Their Estimated Survival with Docetaxel + Prednisone
1. The medical oncologists in the MDACC Genitourinary Oncology Dept are better physicians
2. The 12 two-stage regimes in The Scramble are better than Docetaxel + Prednisone
3. Using the “switch-away” rule is better than just giving the same treatment combination without switching.
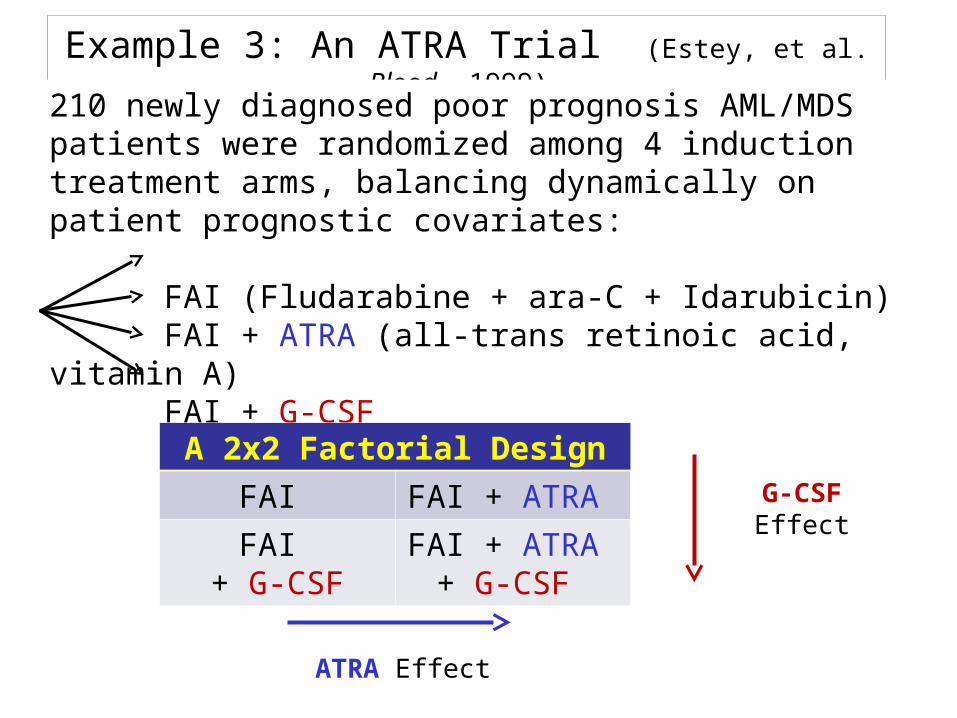
Example 3: An ATRA Trial (Estey, et al. Blood, 1999)
210 newly diagnosed poor prognosis AML/MDS patients were randomized among 4 induction treatment arms, balancing dynamically on patient prognostic covariates:
FAI (Fludarabine + ara-C + Idarubicin) FAI + ATRA (all-trans retinoic acid, vitamin A) FAI + G-CSF FAI + ATRA + G-CSF
A 2x2 Factorial Design
FAI FAI + ATRA
FAI + G-CSF
FAI + ATRA + G-CSF
G-CSF Effect
ATRA Effect
Goals and Results of the ATRA Trial in 1999
Goals: Assess the effects of adding ATRA, or G-CSF, or both, to FAI on Prob[Alive & in CR at 6 months] and on overall survival time
Results: Based on logistic and Cox model regressions . . . After accounting for prognostic covariates (age, platelets, treated in protected environment, performance status, cytogenetics), there was no difference among the 4 treatment arms in terms of CR, EFS, or EFS following CR (p-values = .18 to .99 for the various tests)

What Do These Examples Have in Common?
A “Dynamic Treatment Regime” (DTR) is a mathematical model for what physicians do in everyday practice.
A DTR is a set of rules for choosing a patient’s treatment at each stage of therapy, with each choice based on the patient’s entire history up to that stage - - including all previous treatments and outcomes.
Get baseline patient information Make 1st treatment decision Observe the outcome Make 2nd treatment decision Repeat, until some “final” event is observed
A “decision” may be complex - - because it is medical practice.
Choose a treatment or combination of treatments Modify a treatment dose or schedule Suspend or stop therapy due to severe toxicity

DTR as a Multi-Stage Process
A DTR has three components:Patient baseline prognostic covariatesTreatments given over timeOutcomes observed over time
Basic Form of a Dynamic Treatment Regime ObserveTreatObserveTreatObserve … Final Event
Some Mathematical Notation: For Outcomes (Y0, Y1, Y2, Y3, . .) and Treatments/Decisions, DTR = (T1, T2, T3, . .) The sequence is Y0 T1 Y1 T2 Y2 T3 Y3 . . .
The Essential Complication: Each treatment decision depends on all previous outcomes and decisionsFor example, T3 depends on (Y0 , T1 , Y1 , T2 , Y2 )

Evaluating Dynamic Treatment Regimes
Data Analysis Based on available data, estimate the effect of each DTR, i.e. each sequence of decision rules (T1, T2, T3, . . .), on some final outcome, such as overall survival time.
Trial Design Randomize wherever possible and ethical Evaluate and compare two or more competing DTRs, in
terms of their effects on the final outcome
Goal : Figure out which DTR (T1, T2, T3, . . .) is best.

Even A Two-Stage DTR May Be Non-Intuitive
Example 1: Obtaining a response in 1 or 2 stages
Response Probabilities
Treatment Frontline Salvage with C if Frontline
Fails
Overall(In 1 or 2 stages)
A 60% 10% 64%
B 50% 40% 70%
1) If salvage is ignored, then A > B as frontline therapy.
2) If the goal is to get a response in either 1 or 2 stages of therapy, then (B,C) > (A,C) as a two-stage strategy.
E.g. if A is highly immunosuppressive

Example 2: Maximizing time to failure in 2 stages
Mean Time to Failure, in Months
Treatment Frontline Salvage with C if Frontline
Fails
Overall, if Pr(salvage is
possible) = .80
A 16 6 20.8
B 14 12 23.6
If 80% of frontline failures allow subsequent salvage therapy
(frontline failure is PD, not death, dropout, or severe toxicity) A > B as frontline (B,C) > (A,C) as a 2-stage strategy
This may occur, e.g., if C acts synergistically if given after B
Even A Two-Stage DTR May Be Non-Intuitive

“Treatment” at each stage may be complex.
The # stages of therapy varies from patient to patient, depending on the patient’s outcomes.
Physicians typically use patient covariates, at each stage, as “tailoring variables” to choose a treatment. But this introduces “selection bias” if it is ignored in the statistical analysis!
Adverse outcomes (progressive disease, severe toxicity) often cause physicians to stop therapy. Such decisions are part of the regime.
Some Complications with DTRs

A Closer Look at the 1999 AML/MDS Trial Data:
Accounting for Both Induction and Salvage Therapies

Survival Time =TD if death during inductionTR + TRD if death after salvage for resistant diseaseTC + TCP + TPD if death after salvage for progression after CR TC + TCD if death in CR
Keeping Track of Survival Time

Re-Analysis of the ATRA Trial Data
Because there were many salvage treatments We classified each salvage as either containing high dose ara-C (HDAC) or not.
We distinguished between − Salvage for resistant disease during induction chemo − Salvage at disease progression following CR
There were 16 regimes, of the form(frontline, salvage after resistance, salvage after progression)
FAIFAI + ATRAFAI + G-CSF
FAI + ATRA + G-CSF
HDAC or Other HDAC or Other

The 16 Actual Dynamic Treatment Regimes in the AML/MDS Trial
Induction Salvage for Resistant Disease
Salvage after Progression
FAI HDAC HDAC
FAI HDAC Other
FAI Other HDAC
FAI Other Other
FAI + ATRA HDAC HDAC
FAI + ATRA HDAC Other
FAI + ATRA Other HDAC
FAI + ATRA Other Other
FAI + G-CSF HDAC HDAC
FAI + G-CSF HDAC Other
FAI + G-CSF Other HDAC
FAI + G-CSF Other Other
FAI + G-CSF + ATRA HDAC HDAC
FAI + G-CSF + ATRA HDAC Other
FAI + G-CSF + ATRA Other HDAC
FAI + G-CSF + ATRA Other Other

The 16 Actual Dynamic Treatment Regimes in the AML/MDS Trial
Induction Salvage for Resistant Disease
Salvage after Progression
FAI HDAC HDAC
FAI HDAC Other
FAI Other HDAC
FAI Other Other
FAI + ATRA HDAC HDAC
FAI + ATRA HDAC Other
FAI + ATRA Other HDAC
FAI + ATRA Other Other
FAI + G-CSF HDAC HDAC
FAI + G-CSF HDAC Other
FAI + G-CSF Other HDAC
FAI + G-CSF Other Other
FAI + G-CSF + ATRA HDAC HDAC
FAI + G-CSF + ATRA HDAC Other
FAI + G-CSF + ATRA Other HDAC
FAI + G-CSF + ATRA Other Other

The 16 Actual Dynamic Treatment Regimes in the AML/MDS Trial
Induction Salvage for Resistant Disease
Salvage after Progression
FAI HDAC HDAC
FAI HDAC Other
FAI Other HDAC
FAI Other Other
FAI + ATRA HDAC HDAC
FAI + ATRA HDAC Other
FAI + ATRA Other HDAC
FAI + ATRA Other Other
FAI + G-CSF HDAC HDAC
FAI + G-CSF HDAC Other
FAI + G-CSF Other HDAC
FAI + G-CSF Other Other
FAI + G-CSF + ATRA HDAC HDAC
FAI + G-CSF + ATRA HDAC Other
FAI + G-CSF + ATRA Other HDAC
FAI + G-CSF + ATRA Other Other

The 16 Actual Dynamic Treatment Regimes in the AML/MDS Trial
Induction Salvage for Resistant Disease
Salvage after Progression
FAI HDAC HDAC
FAI HDAC Other
FAI Other HDAC
FAI Other Other
FAI + ATRA HDAC HDAC
FAI + ATRA HDAC Other
FAI + ATRA Other HDAC
FAI + ATRA Other Other
FAI + G-CSF HDAC HDAC
FAI + G-CSF HDAC Other
FAI + G-CSF Other HDAC
FAI + G-CSF Other Other
FAI + G-CSF + ATRA HDAC HDAC
FAI + G-CSF + ATRA HDAC Other
FAI + G-CSF + ATRA Other HDAC
FAI + G-CSF + ATRA Other Other

The 16 Actual Dynamic Treatment Regimes in the AML/MDS Trial
Induction Salvage for Resistant Disease
Salvage after Progression
FAI HDAC HDAC
FAI HDAC Other
FAI Other HDAC
FAI Other Other
FAI + ATRA HDAC HDAC
FAI + ATRA HDAC Other
FAI + ATRA Other HDAC
FAI + ATRA Other Other
FAI + G-CSF HDAC HDAC
FAI + G-CSF HDAC Other
FAI + G-CSF Other HDAC
FAI + G-CSF Other Other
FAI + G-CSF + ATRA HDAC HDAC
FAI + G-CSF + ATRA HDAC Other
FAI + G-CSF + ATRA Other HDAC
FAI + G-CSF + ATRA Other Other

Ignoring salvage treatment may lead to biased estimation of induction treatment effects on survival The goal of the analysis to estimate overall survival for the induction-salvage treatment regimes, not just the 4 frontline combinations. Main Question: Which induction-salvage treatment regimes (if any) led to longer overall survival time?
This requires modern statistical methods for analyzing Dynamic Treatment Regimes
Why We Evaluated DTRs

patients in one induction arm had a higher rate of resistant disease than the other arms?
patients in the 4 induction arms received salvage treatments at disproportionate rates?
one particular salvage treatment led to longer (or shorter) overall survival than the others?
one particular salvage treatment led to longer overall survival than the others, but only among patients who were resistant to induction?
What if . . .

1. For each transition time, in each possible pathway to death, we accounted for :− Four possible distributional forms (“Goodness of Fit”)− Effects of Age and Cytogenetic Category− Effects of previous transition times− Effects of frontline and salvage treatments (the DTR)
2. Mean survival time was − modeled as a weighted average of all 4 possible mean survival times, and − estimated for each of the 16 possible regimes
3. We analyzed the data two different ways : − Likelihood Based− Inverse-Probability-of-Treatment-Weighted (IPTW)The two methods gave the same conclusions.
Re-Analysis of the ATRA Trial Data

Likelihood Based Estimation of Overall Mean Survival
=

Inverse Probability of Treatment Weighted (IPTW) Estimation of Overall Mean Survival
IPTW is used to correct for selection bias

Final Estimates of Overall Mean Survival
?


Some Conclusions from the ATRA Trial Data
1) FAI + ATRA followed by HDAC at progression after CR seems promising, versus the other regimes
2) FAI + ATRA followed by either HDAC or not for resistant disease also seems promising, versus the other regimes
3) If we had done this analysis in 1999, ATRA might have been studied further :
− ATRA dose and schedule were never optimized
− Many combinations and sequences are possible
4) Tailoring variables probably were used to choose salvage regimens Can we do a more refined analysis?
5) There are many possible molecular mechanisms of interactions between ATRA and the cytotoxic agents, and possible sequential effects

Current Events
Schlenk et al. (Blood 118, 2011; ASH 2011 Abstract 80) reported a large randomized study of 1112 AML patients, age < 60 years (conducted 2004 – 2009) :
Induction: 2 cycles of ICE(Idarubicin + Cytarabine + Etoposide) +/- ATRA
Consolidation or Salvage : High risk patients, or induction failures, received allosct, if a matched donor was available, others received HDAC (“tailoring variables” were used)
1) Survival benefit in the ATRA arm (p= .02)
2) Patients with the NPM1 mutation had significantly higher CR rate and better EFS
Remark: This data set might reveal more, with a DTR analysis accounting for consolidation and salvage.

Some General Conclusions
1) Actual oncology practice is a DTR. Most cancer patients receive two or more treatments in sequence, chosen adaptively at each stage.
2) Conventional clinical trials are of limited use to practicing physicians – because they focus on only one stage of therapy, and so do not reflect actual medical practice.
3) Studying actual treatment regimes provides more clinically useful data, and more informative conclusions.
4) With many regimes, # pats/regime is small, but one may borrow strength between regimes for estimation.
5) Conducting trials of DTRs actually is not difficult.
6) Designing trials of DTRs is very difficult: It is a complex process, involving physicians, nurses, administrators, statisticians, and programmers.