health and economic mobility - urban.org
TRANSCRIPT
HEALTH and economic mobility
Jessica Kronstadt, The Urban Institute
KEY FINDINGS:
• While estimates vary, parents‘
health status accounts for a
relatively small share of
children‘s education attainment
and income mobility.
• Many studies find a link
between good health and positive
labor market outcomes
(potentially enhancing mobility),
but there is little consensus about
the magnitude of this connection.
• Studies that link catastrophic
health care costs to bankruptcy
and wealth dissipation, suggest a
negative link to intergenerational
mobility.
• Some studies show that poor
health conditions in childhood,
especially mental and emotional
problems, lead to less education
and potentially less economic
mobility.
• The causal link between health
insurance and health outcomes
(possibly leading to more or less
economic mobility) is difficult to
determine because there may be
systematic differences between
individuals who have health
insurance and those who do not.
There is ample evidence that health and wealth are
related, and it is possible that health helps drive—or hinder—
economic mobility. (The data suggesting this link are
summarized in Table 1.) If there is a causal link between health
and income, then negative health shocks could affect
intragenerational mobility if ill health precipitates income
drops. Also assuming that causal link, it is possible that health
could affect intergenerational mobility to the extent that health
status is passed on from one generation to another. Health also
might affect mobility if economic status helps to determine
childhood health and gives some children advantages or
disadvantages that may continue later in life. Some of the key
links established between socioeconomic status and health are
highlighted in the table below.
Link Between SES and Health
o Individuals who report excellent health hold 74 percent more wealth than those who report
fair or poor health (Smith 1999).
o Among children up to age three, fewer than 75 percent of those whose family incomes are
less than $10,000/year report excellent or very good health compared with 90 percent of
children in families with incomes that exceed $100,000 (Case and Paxson 2005). These
differences increase with age.
o Among poor children, 9.6 percent have a physical or mental disability that limits their
activities, compared with 5.7 percent of nonpoor children (Case and Paxson 2005, citing
Newacheck and Halfon 1992).
o For adults in most age groups, having at least a college degree is related to improvements in
mortality (Palloni 2006).
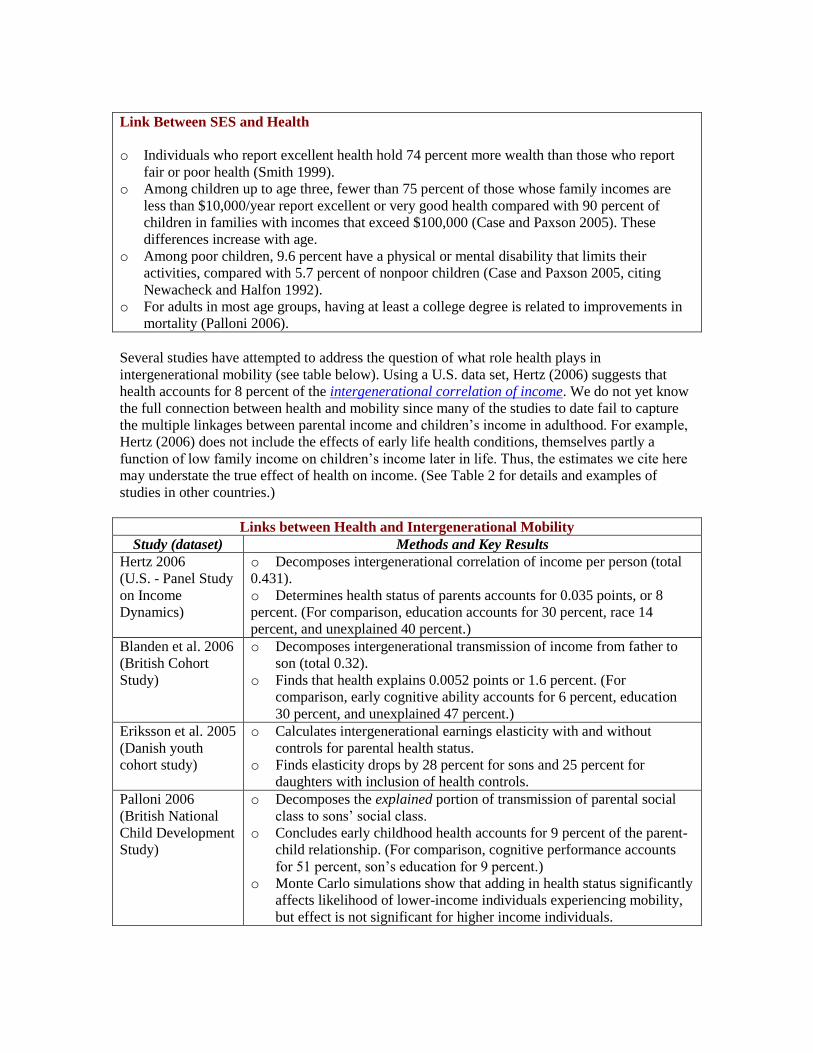
Several studies have attempted to address the question of what role health plays in
intergenerational mobility (see table below). Using a U.S. data set, Hertz (2006) suggests that
health accounts for 8 percent of the intergenerational correlation of income. We do not yet know
the full connection between health and mobility since many of the studies to date fail to capture
the multiple linkages between parental income and children‘s income in adulthood. For example,
Hertz (2006) does not include the effects of early life health conditions, themselves partly a
function of low family income on children‘s income later in life. Thus, the estimates we cite here
may understate the true effect of health on income. (See Table 2 for details and examples of
studies in other countries.)
Links between Health and Intergenerational Mobility
Study (dataset) Methods and Key Results
Hertz 2006
(U.S. - Panel Study
on Income
Dynamics)
o Decomposes intergenerational correlation of income per person (total
0.431).
o Determines health status of parents accounts for 0.035 points, or 8
percent. (For comparison, education accounts for 30 percent, race 14
percent, and unexplained 40 percent.)
Blanden et al. 2006
(British Cohort
Study)
o Decomposes intergenerational transmission of income from father to
son (total 0.32).
o Finds that health explains 0.0052 points or 1.6 percent. (For
comparison, early cognitive ability accounts for 6 percent, education
30 percent, and unexplained 47 percent.)
Eriksson et al. 2005
(Danish youth
cohort study)
o Calculates intergenerational earnings elasticity with and without
controls for parental health status.
o Finds elasticity drops by 28 percent for sons and 25 percent for
daughters with inclusion of health controls.
Palloni 2006
(British National
Child Development
Study)
o Decomposes the explained portion of transmission of parental social
class to sons‘ social class.
o Concludes early childhood health accounts for 9 percent of the parent-
child relationship. (For comparison, cognitive performance accounts
for 51 percent, son‘s education for 9 percent.)
o Monte Carlo simulations show that adding in health status significantly
affects likelihood of lower-income individuals experiencing mobility,
but effect is not significant for higher income individuals.

Health could affect intergenerational mobility if health plays a causal role in economic status and
if health transmits from one generation to another. Health may be passed on from parent to child
through genetics , parental behaviors and the home environment or a combination thereof.
There are several mechanisms through which health could affect earnings and wealth—either
directly if illness limits labor market attachment or restricts job choice, or indirectly if childhood
health affects cognition or educational attainment. These patterns can be seen among individuals
with disabilities. The hypothesis that health can impact future socioeconomic class is known as
―health selection‖ or ―social drift.‖
Health shocks could contribute to intragenerational mobility either because of their effects on
ability to work or because of large medical expenses. Hertz (2006) finds that health status was a
significant predictor of income change between 1997 and 1998, with self reports of fair or poor
health and having a disability associated with modest income declines. However, health did not
have significant effects on income mobility in the other two-year time periods Hertz studied—
1990–1991 and 2003–2004.
Health also could affect intergenerational mobility if the economic status into which a child is
born influences her health, which could, in turn, influence economic status in adulthood. There
are different hypotheses about how health at a very young age could affect health—and
potentially educational or employment—outcomes later in life. According to the fetal-origins
hypothesis, conditions in utero—often reflected in health at birth—can alter the ―programming‖
of vital organs, the effects of which may appear many years later. Life course models focus on the
role that childhood health plays in producing adult health status. In either of these models,
parents‘ socioeconomic status could affect either the likelihood that a child will experience health
problems or the consequences of those health conditions, or both. If, consistent with the
discussion above, health can help determine income in adulthood, it is possible that a portion of
the stickiness at the bottom of the income distribution may reflect a more complex version of one
of these patterns, as illustrated below::
Pathways between Health and Income in Adulthood
Low-income of parents
Worse health at birth or in childhood
Lower cognition and/or less schooling
Worse health in adulthood
Low-income in adulthood
This still leaves the question of why income might affect health. One theory holds that parents of
higher economic status may have the time, resources, and tastes to invest more heavily in
medical care and health insurance and good nutrition. Class may also dictate different living
environments, for example, as neighborhoods have different amounts of violence or different
levels of exposure to toxins. (See discussion of asthma as one example of how pollution could
adversely affect health.) Parental education may also play a substantial role in children‘s health, if
less well-educated parents do not know to take preventive measures or are less able to follow
medical advice.
It is possible also that the apparent relationship between socioeconomic status and health may be
influenced by parental behaviors. For example, Case and Paxson (2002, cited in Case et al. 2002)
find that children in lower-income households more often live with cigarette smokers, have
irregular bedtimes, and are less likely to wear seat belts. It seems unlikely that these parental
behaviors are the direct consequence of lower income. (Although it is possible that they reflect
responses to higher stress, less energy or resources for parenting, and lower levels of stability.)
Some of these characteristics, as well as factors like maternal weight, are also correlated with
children‘s health. In fact, Case et al. (2002) suggest that if it were possible to control for a full set
of parental decisions it may make the income gradient for child‘s health disappear.
Socioeconomic status continues to contribute to health in adulthood, potentially through
education or stress levels. Pathways models suggest that stress arising from low economic status
can lead to health problems later in life. In this hypothesis, health in childhood does not directly
affect health in adulthood, but affects economic status which then affects health. One provocative
variation of this theme is that inequality in income, rather than low income, leads to deteriorating
health. The complex interplay between health and socioeconomic status makes it difficult to make
a definitive determination on the role health plays in driving intergenerational mobility. If adult
health is in part determined by adult socioeconomic status, then health could be a symptom of
economic mobility rather than, or in addition to, being a driver of it.
These complicated relationships can be observed in the cases of obesity, substance abuse, and
mental illness. In each of these paradigms, there is evidence suggesting that
1) the condition is passed on from one generation to the next either genetically or
through the family environment;
2) lower economic status could exacerbate the condition; and
3) the condition could contribute to lower earnings.
Some public programs, like Medicaid, prenatal care, and nutrition programs, try to improve
health outcomes, but they are unable to overcome the link between socioeconomic status and
health. It is possible, however, that government transfer programs, like Social Security Disability
Insurance and Supplemental Security Income, that are designed to protect individuals from the
worst effects of health shocks may indirectly protect children‘s health. For example, if a parent
becomes disabled and is no longer able to work, the government program may prevent that person
from falling into deep poverty. Cushioning the parents‖ fall may not only mediate large drops in
intragenerational mobility, but may also help protect the child from some of the health (and
related educational and income consequences) that may stem from childhood poverty. An
interesting question for further research would be to consider how health-related governmental
social insurance programs affect intergenerational mobility.
As a general caveat, in addition to the difficulties of interpreting causality, any attempt to
determine the role health plays in economic mobility will likely be hindered by the data. Different
studies assess health in different ways. Many rely on self-reported health status. Others use easily

measurable variables as proxies for more complex underlying conditions—for example, birth
weight is often used as a stand in for in utero conditions. Finally, there are few U.S. data sets that
contain detailed health information and follow the same individuals over a long period of time.
For that reason, many of the studies discussed here either use data from other countries or they
study limited measures of health and socioeconomic status.

PATHS THROUGH WHICH POOR HEALTH COULD AFFECT EARNINGS
AND WEALTH
1. Health and Labor Market Activity
Ill health can affect earnings by reducing wages or limiting participation in the labor force. Currie
and Madrian (1999) find that many studies have detected a link between health and the labor
market, but that little consensus has emerged about the magnitude of that connection. They
identify three ways in which wages could be damped by poor health: through reductions in
productivity; costs for the employer to accommodate the individual; or discrimination. However,
in an extensive literature review, they conclude that in general the negative relationship between
earnings and health is not primarily the result of differences in wages, but in amount of time
worked. As an example of the ability of health to restrict labor force participation and hours
worked, Smith (1999) analyzed data on individuals in the Health and Retirement Study. He finds
that people who experience a severe new health problem between two waves of the survey
reduced their weekly hours of work by four hours; further, their likelihood of staying in the
workforce declines by 15 percentage points. Additionally, if, over time, less healthy individuals
have more spells out of the workforce, their income may reflect this decline in cumulative
workforce experience. (See also, discussion of disability.)
2. Health Costs and Wealth
Health can affect economic well-being in ways outside of the labor market. For one, health crises
can be very expensive. In a study of families who filed for bankruptcy in 2001, 28 percent of
individuals surveyed cited illness or injury as the specific reason for their bankruptcy
(Himmelstein et al. 2005). Furthermore, among those who stated illness as the cause, the average
out-of-pocket costs since the start of the condition were $11,854, even though three-quarters of
those individuals had health insurance when their condition began. Savings behavior may also
change (Smith 1999, Adams et al. 2003). Savings could increase either because marginal utility
of consumption may be reduced when individuals are ill, or out of a desire to ensure adequate
resources for a potential surviving spouse. Alternatively, assets may be spent down to cover other
medical and nonmedical costs associated with illness. Health conditions may also increase
resources if they trigger new government transfers.
3. Childhood Health and Cognition
Poor health earlier in life may have an adverse effect on later earnings, indirectly, by limiting
cognition or educational attainment. Palloni (2006) finds that early cognitive ability is correlated
both with health status and adult cognition—a trait that the labor market rewards. Additionally, he
finds that in the British National Child Development Study cognition at age 11 is strongly
associated with low birth weight and health status at age seven. (See Currie and Madrian (1999)
for a discussion of some of the other literature on this topic.)
4. Childhood Health and Education
In their review of the literature, Currie and Madrian (1999) state that many researchers have
suggested that poor childhood health is correlated with less education (for example, Grossman
1975, Perri 1984, Wolfe 1985, Wadsworth 1986). An evaluation of British data finds that after
controlling for parental and household traits, each adverse health condition at age seven is related
with a 0.3 drop in the number of 0-level exams passed, and each condition at age 16 is associated
with an additional 0.2 decline (Case et al. 2005). The study also finds that different conditions
had different effects, with mental and emotional problems at either age related to educational
outcomes, as are ―systems‖ conditions (including lung, heart, blood, and neurological conditions)
at age seven. On the other hand, physical impairment had no significant effect. Grossman and
Kaestner (1997, cited in Currie and Stabile 2003) also review this literature and suggest that
health-related school absence explains a portion of this effect (See also the discussion of asthma
for an example of a condition that contributes to school absence.). Currie (2008, forthcoming)
reviews the links between parent socioeconomic status and child health and between child health
and future outcomes like educational attainment. She documents strong links between each pair
above, but she points out that the size of the effect of child health on subsequent outcomes is
difficult to measure in part due to the fact that health is multi-dimensional and not easily
quantified in single-index measures.
5. Childhood Health and Social Status
Case et al. (2005) present compelling evidence that childhood health can have lasting effects on
social status in adulthood. For each chronic condition at age 16, the probability of employment at
age 42 is reduced by 5 percentage points. This relationship exists even when taking into account
the individual‘s education, and his health and socioeconomic status at ages 23 and 33. Each
additional chronic condition at age seven is also associated with a reduction in social status,
measured on a six-point scale of employment type (ranging from professional to unskilled labor).
6. Interactions between Health and Labor Market, Education and Cognition
Several authors attempt to determine the extent to which the health effects on employment work
directly through health or through education or cognition. When decomposing the path model,
Palloni (2006) suggests that early health affects social class later in life only through cognitive
ability and a rating of maladjustment at age 11, not through direct health effects. Palloni‘s
inclusion of what he terms ―unconventional market traits‖ stems from his insight that some
factors that are associated with poor health may also help shape personality. He refers to a study
by Stormer and Harrison (2003), which suggests that food insecurity—a potential signal of stress,
anxiety, or family disorganization—influences social skills. When Blanden et al. (2006)
decompose their measure of intergenerational income persistence, they find that of the total health
effect, only a small portion (10.5 percent) comes through passage of 0-level exams.
Caveats
Because it is possible for decreased income to adversely affect health in adulthood, some of the
correlation between labor force participation and health noted above may result from reverse
causality. Additionally, individuals who chose not to participate in the labor force may have
reason to report poor health in order to be eligible for government transfer programs such as
disability insurance.
In addition to the link from child health to education explored elsewhere in this review, it is also
possible for education to affect long-term health (Mazumder, 2008 forthcoming). For cohorts
born in the early twentieth century, Census data suggest that increased education accounts for
much of the decline in mortality rates during the 1960s and 1970s (Lleras-Muney, 2005). While
these findings are not robust to the inclusion of state-specific time trends1 (to control for
simultaneous reforms in, for example, child nutrition), SIPP data on individuals affected by those
early reforms reveal significant reductions in mortality due to compulsory education (Mazumder
2008, forthcoming). The author cautions, however, that the mechanisms theorized to explain the
causal link between education and health do not appear to be relevant, suggesting either that our
theories are insufficient or that compulsory schooling laws are poor instruments.
1 Mazumder‘s IV model with state-specific time trends suggests a 25 percent reduction in mortality due to
compulsory schooling laws compared with the roughly 60 percent reduction suggested by Lleras-Muney.
Further decomposing the results, he finds that the gains are concentrated among the earliest birth cohorts,
actually finding an insignificant increase in mortality among later cohorts due to compulsory education.

DISABILITY
Individuals with disabilities fare worse financially than their nondisabled peers. For example, in
2003, 23 percent of individuals with at least one disability were living in poverty, compared with
9 percent of individuals without disabilities (Stapleton et al. 2006, citing data from the American
Community Survey). Part of this gap reflects lower earnings and higher unemployment rates
among Americans with disabilities. The economic status of people with disabilities may improve
when taking into account government transfer programs like Supplemental Security Insurance
(SSI) and Disability Insurance (DI)—particularly among those of lower socioeconomic status
who are more likely to receive the benefits and who have higher replacement rates (benefits
relative to pre-disability earnings). Yet even with these transfers and other forms of household
income, the gap remains (Bound and Burkhauser 1999). Also, public programs entail work
disincentives, which, some argue, may help trap people with disabilities in or near poverty.
Following the onset of disability, many individuals who continue to work see their income drop,
primarily due to a reduction in hours. Charles (2003) observed in the Panel Study of Income
Dynamics data set that working age men with severe disabilities (who reported disability all years
following onset) see a decline in annual earnings of 23 percent below expected levels in the year
of disability onset. Although these men go through an initial recovery over the next several years,
they continue to see lower earnings, so that 10 years after onset they are earning 15 percent less
than would have been expected. On the other extreme, men who report a disability in only one
year eventually regain their expected earnings. Intermediate results occur for individuals who
report disability only sporadically after the year of initial onset.
Age at Onset of Disability
Older workers in the Charles (2003) study experienced larger initial drops after onset and did not
see an annual upward trend in earnings following the initial two-year recovery period. Charles
argues that older workers may have accumulated more human capital stock and therefore may see
it drop more dramatically after a disability if some of that stock has diminished usefulness when
disabled. Furthermore, younger workers, because they will have more time to benefit from further
investment in capital stock, may be more likely to take actions that will help them to recover. As
support to this hypothesis, Charles notes that younger men are more likely to switch industries
after onset of disability and this behavior helps account for their better recovery. Not only are
younger adults more likely to switch occupations and recover compared to older adults, Charles
finds, but white men and men with at least some college education are more likely to change
occupations, relative to nonwhite men and less well educated ones.
The decline in earnings and, in some instances, recovery among working individuals following
onset of disability could explain some instances of intragenerational mobility. Additionally,
many individuals exit the workforce (or fail to enter it) because of disability. The disparity in
employment rates between disabled and non-disabled individuals of working ages has been
shown in many different national surveys. For example, the 2003 American Community Survey
finds that 38 percent of working-aged adults who reported at least one disability were employed,
compared to 78 percent of individuals without disabilities (Stapleton et al. 2006). Similar to the
impact of age at onset among disabled workers, Loprest and Maag (2003) find that people with
late onset of disability (after age 22) were significantly less likely to be employed than those
whose disability first created limitations prior to age 22, when controlling for demographics,
education, severity of disability, and receipt of benefits. The authors suggest that this could be
because people who first experience disability early in life have more time to adjust or to select
career paths that will be more accommodating.

Work and Disability
Throughout the 1990s, a greater share of people with disabilities report being unable or
unavailable to work. Burkhauser and Stapleton (2003) consider some of the potential reasons for
this pattern such as changes in job characteristics, the demographics of population with
disabilities, or the severity of disabilities. Other theories have more direct policy implications. For
example, individuals with disabilities who require costly care may seek public disability and
health benefits rather than working for an employer with limited or no health insurance.
Alternatively, employers may limit job opportunities for those with disabilities fearing the
expenses of accommodation associated with the Americans with Disabilities Act. (See Bound and
Burkhauser 1999 for a discussion of this literature.) Some research suggests that between 30 to 40
percent of people who apply for Social Security Disability Insurance would work if there were no
disincentives imposed by the program. (See Stapleton et al. 2006 for overview.)
Job Characteristics and Disability
Another potential contribution to the correlation between low-income and disability is that certain
jobs may both pay lower wages and contribute to the likeliness of disability. Occupation could
directly lead to disability if the disabling condition arose from a workplace injury; one study finds
that more than a third of disabled people ages 51 to 61 attribute their disability to injuries and
illnesses on the job (Reville and Schoeni 2003/4). Lower educational attainment is identified as a
determinant of nonfatal work injuries (Oh and Shin 2003). Additionally, some theorize that lower
income individuals may have fewer skills that allow them to change jobs, leading them to stay in
high risk jobs longer (Hayward et al. 1989).
Childhood Disability
Childhood disability may hinder educational outcomes. For example, Loprest and Maag (2003)
find that individuals with limitations by the age of 22 graduate from high school less often than
people without disabilities (33 percent compared to 13 percent). They estimate that 13 percent of
the difference in employment rates between disabled and nondisabled individuals can be
attributed to educational differences. However, they caution that it is not clear whether the
disability impairs educational attainment or if other environmental factors increase the probability
of both disability and poorer school outcomes. Charles (2003) finds that prior to reported onset of
limitations, individuals who eventually report a disability have less education than those who
remain non-disabled throughout the course of their study. This raises the possibility either that
poor health preceding manifestation of the limitation could account for lower educational
attainment or that other factors related to lower educational or economic status lead to higher
rates of disability. Loprest and Maag (2003) find that young people with disabilities have a
greater likelihood of coming from households living below the federal poverty level than their
non-disabled peers.

PRENATAL CONDITIONS AND HEALTH AT BIRTH
Studies show that low birth weight (LBW)2 negatively influences educational attainment, health,
and income in later life. Evidence also suggests that parents who were LBW themselves more
often have LBW children. Furthermore some researchers posit that both the risk of having a LBW
child and the adverse consequences of LBW status may be greater among poorer families,
implying that LBW may create a particular obstacle for some children to move up from poverty.
Link between Low Birth Weight (LBW) and Health
Many studies link LBW to higher mortality rates. For example, a study of 16,000 individuals born
in Hertfordshire between 1911 and 1930 finds that those with lower birth weights are twice as
likely to experience fatalities in adulthood due to coronary heart disease as are those at the top of
the birth weight distribution. The Nurses Study in the United States provides similar evidence
(Barker 1997). Other studies show that the rate of fetal growth, perhaps a better measure of
distress in utero than birth weight, affects death from heart disease in a large Swedish cohort. (See
Rasmussen 2001 for summary of this and other studies.)
Additionally, signs of poor fetal environments, such as maternal smoking or LBW, correlate with
poor health in adulthood, with the relationship strengthening as individuals age (Case et al. 2005).
A series of indicators of in utero conditions, including maternal smoking, remain a jointly
significant predictor of health at age 42, on top of the impact on reported health status at age 42 of
health at ages 23 and 33. In an analysis of data from the Panel Study on Income Dynamics,
Johnson and Shoeni (2007) find a gradient of increasingly worse health among LBW children.
For example, they find that the effect of being LBW on adult health is similar to the effect of
being 8.7 years older. They also find that, although the impact on child health declines when they
control for shared sibling characteristics, LBW still has a modest effect on childhood health.
According to the fetal-origins theory, shocks that occur in utero can have health effects that
appear years later. Barker (1997) explains that an inadequate supply of nutrients or oxygen can
slow the process of cell division. Depending on the timing of those deprivations, the number of
cells in particular organs may be reduced, or under-nutrition can change the amount of hormones
including insulin and growth hormone. According to Barker, this lack of nutrition can
permanently alter or ―program‖ the body. Barker has refined his theory to indicate different risks
related to different periods of gestation. For example, fetal growth slowed during the first
trimester may contribute to stroke through elevated blood pressure; coronary heart disease may
reflect complications with insulin arising in the second trimester. (See Rasmussen 2001 for a
summary.) Others propose that adult-onset diabetes is linked to ways that infants who have
retarded growth may adapt to ensure survival (Rasmussen 2001, citing Cianfarani et al. 1999).
The notion that ―programming‖ organs in the beginning of life can have lasting effects has also
been widely demonstrated in studies with other species (Rasmussen 2001). Almond (2006) uses
the dramatic variation in exposure to the influenza pandemic to estimate the long-term effects of
exposure to influenza in utero. The pandemic struck suddenly and subsided quickly, with
infections concentrated between October 1918 and January 1919, and there was great geographic
variation in exposure rates. Nearly one-third of pregnant women contracted the virus. Decennial
census data from 1960 to1980 reveal that educational attainment is a quarter year lower for the
2 LBW is typically defined as below 2,500 grams (5 lbs., 8 oz.). In developed countries most infants who
are LBW are delivered preterm (do not complete 37 weeks of gestation). LBW is commonly used as a
general proxy for adverse prenatal conditions because data on gestational age, as well as measures of size
relative to gestational age, are not as commonly available. (See Rasmussen 2001 for fuller discussion.)
cohort that was pre-natal during the pandemic and incomes are 6 percent lower. These results are
corroborated by SIPP data in Almond and Mazumder (2005).
There are other potential explanations as to why LBW may be associated with adverse health
effects. For example, the same genetic endowment that may result in LBW may cause other
health effects later in life (Behrman and Rosenzweig 2004). Alternatively, LBW may signal other
factors—maternal behaviors, medical care, and demographic characteristics—that may
themselves contribute to poor health later in life. Additionally, Conley and Bennett (2000) raise
the possibility that LBW children may suffer stigma or have fewer resources allocated to them
within the family with subsequent adverse health effects later in life.
The health consequences of LBW may vary according to economic status. For example, Case et
al. (2002, p. 1323) write that their estimates are ―consistent with the hypothesis that wealthier
children are less affected by poor health at birth, and recover more quickly.‖ Some research
suggests that having health insurance mitigates the effects of LBW, even after controlling for
childhood poverty (Johnson and Shoeni 2007).
Recent research calls into question the magnitude of the costs associated with LBW. Almond,
Chay, and Lee (2005) control for a number of confounding factors that may overstate earlier
LBW results. Using data that include all twins born in the United States between 1983 and 2000,
the authors control for maternal characteristics that are not influenced by policy—like race—as
well as for genetics by comparing identical twins and fraternal twins. Their results suggest an
impact of LBW on hospital costs, health outcomes (APGAR scores and use of ventilators), and
mortality that are smaller than earlier estimates by a factor between 4 and 20. Royer
(forthcoming) finds smaller effects of LBW on educational attainment than shown in most
previous studies (see below). Oreopoulos et al. (forthcoming) use data from Manitoba, Canada,
and find results for infant mortality that are similar to Almond, Chay, and Lee (2005). They also
find a lasting effect of poor infant health (low APGAR scores) on mortality through age 17.
Predictors of Low Birth Weight
The prevalence of LBW decreases as income increases. For example, National Health Interview
Survey data reveal that 9.3 percent of children whose family incomes are below $30,000 (in 2000
dollars) are born at LBW, compared with 6.9 percent for households with income between
$30,000 and $60,000, and 5.6 percent for families with more than $60,000 (Case and Paxson
2006). Johnson and Shoeni (2007) find that incremental increases in income decrease the
probability of low-weight birth only among low-income families, not among more well-off
families.3
Others show that race predicts LBW, with black babies having about twice the probability of
LBW relative to white babies, even after controlling for some measures of socioeconomic status
(Conley and Bennett 2000).4
3 Although others replicate the finding that LBW is associated with low socioeconomic status, even with
other demographic controls (Currie and Moretti 2007), Conley and Bennett (2001) conclude that the
income-to-needs ratio is associated with an increase in the child‘s birth weight only if the mother was
herself born LBW. 4 Johnson and Schoeni (2007) note that the difference in LBW rates helps account for some of the race
differential in adult health status as well.

Case and Paxson (2006) link mothers‘ education to behaviors that affect infant health, such as
smoking, which the Surgeon General has determined is causally related to LBW and shortened
gestation (CDC 2004). The authors also note that less well educated pregnant women less often
seek prenatal care in their first trimester than those with some college education (68 percent
compared to 91 percent, in the National Vital Statistics numbers they cite). Although some
studies identify significant differences in LBW rates among mothers receiving inadequate levels
of prenatal care compared with those who receive adequate care (Devaney et al. 1992), there is
some ambiguity about the impact of prenatal care. (See Box ―Can Prenatal Care Help Bridge the
Socioeconomic Divide in Childhood Health Outcomes‖ below.
Low-income women may also have inadequate nutrition during pregnancy. Although Rasmussen
(2001) concludes that few studies identify a significant causal link between maternal nutritional
status and LBW among women in developed countries, poor nutrition could contribute to other
complications. Lack of knowledge of or access to nutritional supplements could cause spina
bifida and other neural tube defects (Case and Paxson 2006).
Of particular relevance for a discussion of economic mobility is the fact that parental birth weight
status is a strong predictor of LBW in the next generation. For example, Conley and Bennett
(2000) find that infants are four times more likely to be LBW if their mothers were LBW and six
times more likely if their fathers were. Currie and Moretti (2007) say their ―findings suggest that
some of the intergenerational transmission of economic status could be due to intergenerational
transmission of low birth weight.‖
Effects on Education and Income
LBW and prenatal shocks may have consequences for cognition and educational attainment.
Conley and Bennett (2001) provide an overview of some studies that have detected effects of
LBW on psychological and intellectual development. Some of these deficiencies may translate
into different levels of success in schooling. Maternal smoking during pregnancy and LBW are
tied to poorer performance on O-level exams in Britain (Case et al. 2005). Johnson and Shoeni
(2007) find that reading comprehension and math scores are lower among LBW children. When
they control for sibling fixed effects, the impact of birth weight becomes marginally significant.
Conley and Bennett (2000) find that the probability of graduating from high school by age 19 is
reduced by 74 percent for LBW children compared with their siblings. Behrman and Rosenzweig
(2004) note that studies that simply use cross-sectional data without controls for genetics or
family background may underestimate the adverse effect of birth weight on schooling by as much
as 50 percent.
Royer (forthcoming) uses a sample of mothers who are twins born in California between 1960
and 1982 to test for the impact of LBW on educational attainment. She finds that ―[f]or a 200
gram increase in birthweight, likely an achievable policy manipulation, education would rise by
roughly 0.04 of one year.‖ This is roughly one-third to one-fourth the size of the Behrman and
Rosenzweig (2004) estimate of one-third of a year of education for a one-pound increase in
birthweight.
There is some evidence for relationship between LBW and earnings or socioeconomic status in
adulthood. Currie and Moretti (2007) find that if two sisters are born in the same neighborhood,
the one who weighed less at birth has a greater probability of living in a neighborhood that is
lower income when she herself gives birth. Johnson and Shoeni (2007) find that LBW has an
effect on earnings that increases with age. Case and Paxson (2006) estimate that being born LBW
may be associated with lowering earnings by 4 percent at age 33.

There are also some interactions between socioeconomic status at birth and socioeconomic
outcomes. One study finds that interacting LBW with income increases the effects of LBW on
education and the effect of the income-to-needs ratio, while the interaction term itself has
borderline significance (Conley and Bennett 2001). This suggests that families with higher
socioeconomic status can compensate for LBW. Yet, Currie and Hyson (1999) do not find that
LBW has an additional negative effect for people of lower economic status. In fact, it is LBW
boys who are high socioeconomic status who do less well in the British O-Level exams than their
peers of the same social status—being LBW removes most of the advantage that high
socioeconomic status boys usually have over their low socioeconomic class peers.
Can Prenatal Care Help Bridge the Socioeconomic Divide in Childhood Health Outcomes?
Although access to prenatal care has increased substantially in this country, there is mixed
evidence about its effectiveness (Fiscella 1995). For example, while infant mortality has declined,
the rates of LBW have remained steady or, in some cases, increased slightly (McCormick 2001).
Modest increases in LBW tend to be found only among infants who have around normal gestation
periods; prenatal care does not appear to greatly reduce the risk of premature birth or the slower
growth among those who are born prematurely (Currie and Groger 2002). Currie and Groger find
that increases in Medicaid caseloads increases prenatal care some. Yet birth weights do not
increase. Fetal death among black women and disadvantaged white women, on the other hand, do
decline, possibly because of better technology available at delivery. Currie and Groger speculate
that part of the reason that prenatal care does not always have much success is that it often fails to
come with smoking cessation, stress reduction or proper foods and vitamins—factors expected to
improve birth outcomes.

HEALTH IN CHILDHOOD
Health in childhood may have lasting impacts on health later in life. For example, if a child
develops a chronic condition at age 7 that continues through age 16, she is more likely to report
poorer health at age 42, even after accounting for negative health events earlier in adulthood
(Case et al. 2005). A 50-year study finds that early childhood events can predict cardiovascular,
respiratory, and neurological health in adulthood (Smith 1999 citing Wadsworth and Kuh 1997).
Child health is also strongly related to household income (both before the child is born and
throughout childhood) and parental education (Case et al. 2002). Further, evidence from the
United States and Canada (Case et al. 2002, Currie and Stabile 2003) indicate the existence of a
health gradient showing that health status becomes more highly correlated to their economic
status as children age. For example, after accounting for parental education, a doubling of
household income is associated with a 4.0 percent increase in the likelihood of excellent or very
good health at ages 0-3. The percentage increases to 4.9 for children ages 4 to 8, and up to 7.2
percent for children ages 13 to 17 (Case et al. 2002).
The higher prevalence of chronic conditions among children in households with lower income
provides one explanation for this gradient. With the exception of hay fever and sinusitis, one
analysis of U.S. data finds that all the chronic conditions measured have a negative relationship
with income in at least some age groups (Case et al. 2002). Similarly, in a Canadian study (Currie
and Stabile 2003) low social status children have higher rates of new health conditions, relative to
high social status children at all ages.
The severity of the condition, as well as the ability to manage it, could also account for part of the
gradient. For example, Case et al. (2002) find statistically significant interactions between all
health conditions except for kidney disease with income, suggesting that additional income can
have a protective effect for children. The strongest evidence for this interaction comes from
chronic conditions with the largest average effect on health status—asthma, diabetes, and
epilepsy. The differential occurs for severity of disease and not prevalence, supporting the health
gradient hypothesis. In contrast, Currie and Stabile‘s (2003) analysis of Canadian data does not
find that income buffers the impact of specific health shocks over the long run. Instead, their
study suggests that the gradient results from children of lower socioeconomic status suffering
more health shocks, without the double jeopardy of suffering more from a given shock. It is not
clear whether Canada‘s universal health care contributes to the different results in the two studies.
Little evidence is found of the gradient or of the link between parents‘ income and child health in
England, at least not when using health measured from nurse examinations and blood tests
(Currie et al. 2007, Doyle et al. 2005).
It is important to note that this income gradient does not appear to simply result from passing on
health status from parent to child. Case et al. (2002) find evidence of the gradient remained
statistically significant even when they include controls for parental health. To determine the role
of genetics the gradient, they compare gradients of adopted children with those living with their
biological parents (available in the National Health Interview Survey on Child Health). They do
not find significant differences, implying that more than simply genetics is at play. The income
gradient for childhood health also does not appear to be the sole result of differences in birth
weight. Although health at birth predicts later health and economic outcomes, it does not, in Case
et al. (2002), eliminate the gradient.
One caveat is that it is possible that children in ill health may reduce household income, reversing
the causality implied above. Case and Paxson (2006) discuss potential ways in which sick

children could depress income: parents of sick children may work less, or a child‘s health crisis
may disturb family relationships and potentially contribute to divorce.

MEDICAL CARE AND HEALTH INSURANCE
Socioeconomic status is highly correlated with the likelihood of having health insurance. There is
evidence suggesting that people with insurance receive more medical care. However, some
controversy remains about whether having insurance actually leads to better health outcomes and
therefore health insurance may not have much to do with economic mobility. This causal link is
difficult to determine for several reasons, including the fact that there may be systematic
differences between individuals who have health insurance and those who do not. In theory,
uninsured people might be healthier than the insured—if less healthy people are more motivated
to purchase health insurance—or vice versa—if people who are less healthy are also less likely to
have jobs that offer health insurance. Research attempting to determine the direct effects of health
insurance must disentangle factors related to the decision to obtain insurance. Additionally, all
health insurance is not alike. For example, some studies fail to find a large positive effect from
Medicaid. This may result from a lower quality of care or may reflect the characteristics of the
program‘s enrollees.
Health insurance status varies dramatically with socioeconomic class with over one-third of
nonelderly people living below the federal poverty level in 2005 being uninsured compared with
9 percent of people above three-times poverty (Kaiser Commission 2006). Many other studies
have documented the relatively low levels of health insurance coverage among low-income
individuals. (See Institute of Medicine (IOM) 2001). Striking differences in insurance coverage
also exist by race. (See Box ―Racial Disparities and Health Care‖ below.) To assess the effect of
health insurance coverage on economic mobility, it is important to determine if insurance makes a
difference in the amount of health care consumed and, ultimately, health outcomes. Substantial
evidence suggests that individuals who do not have insurance less often have a usual source of
care, have fewer doctor visits in a year, and have a smaller probability of any physician visit
within the last year. (See IOM 2001 for an overview.) Surveys reveal that uninsured individuals
are more likely to forgo preventive care,5 and treatment for serious chronic conditions (Ayanian
et al. 2000, Baker et al. 2000).
Some studies further document that the lack of care leads to poorer health outcomes. A 2002 IOM
report finds that cancer patients who lack insurance die sooner on average than insured patients,
and they attribute this in large part to delay in diagnosis.6 Additionally, quality of care may differ
by insurance status. In reviewing studies of trauma care for appendicitis and automobile
accidents—both of which are typically considered exogenous shocks with little correlation with
the individual‘s decision to purchase insurance—Hadley (2003) presents some evidence that
uninsured patients are more likely to die in the hospital.
Other studies examine the links between the costs of medical care and health outcomes. Goldman
et al. (2007) report that studies examining patients with chronic conditions like congestive heart
failure, lipid disorders, diabetes, and schizophrenia, find an association between individuals
facing higher costs for prescription drugs and higher use of inpatient and emergency care. This
finding suggests that individuals may not have been taking needed medication and faced health
5 Lack of dental care also can potentially affect economic mobility by interfering with education and
employment outcomes. (See Currie and Lin 2007 for brief discussion.) 6 Some researchers are not convinced of the link between insurance, screenings, and good health outcomes.
Ross and Mirowsky (2000) point out that other factors may be important. For example, education may
dictate whether an individual receives necessary screenings and appropriate follow up. They also suggest
that the data are not conclusive that general screenings, such as routine check-ups, have a significant
positive effect on health.

consequences. On the other hand, studies broader in scope find ambiguous results on the effect of
health insurance on health. Ross and Mirowsky (2000) use longitudinal data and find that
individuals with health insurance did not have better health outcomes three years later than did
uninsured individuals, after controlling for initial health conditions. In general, researchers are
divided about the effectiveness of medical care, and, in particular, of health insurance. Several
studies find that accounting for health insurance does not eliminate the entire difference in health
across socioeconomic status. (See Case et al. 2002, Newacheck et al. 2003, Ross and Mirowsky
2000).
Public health insurance programs do not appear to eliminate health disparities. On a cross-country
basis, Ross and Mirowsky (2000) note that there are socioeconomic class differentials in
mortality rates in countries with national health care. Findings on how effectively Medicaid
improves health are also mixed. For example, Kaestner et al. (1999) find ―at best weak support‖
for the theory that Medicaid has positive effects on children‘s health. Hadley (2003) offers
potential explanations for why studies often do not find positive impacts of Medicaid on health,
and indeed many find a negative correlation. In addition to citing some data problems,7 he
discusses the fact that people who enroll in Medicaid may be in worse health, particularly because
individuals are often enrolled in the program upon arrival at a hospital. Medicare, on the other
hand, may eliminate the link between socioeconomic status and death from acute, sudden-onset
diseases among people ages 70 and older (Adams et al. 2003). However, a correlation still exists
between socioeconomic status and mortality for conditions that may have a more gradual
development. Adams et al. note that even with Medicare, affordability of care for less acute
conditions may still be a limiting factor.
Some of the difference in rates of insurance across socioeconomic status may reflect the fact that
the majority of nonelderly Americans receive health insurance through employers, which is not
equally available to all workers. Workers who are below the poverty level are much less likely to
work in firms that sponsored health plans than workers with incomes above 400 percent of the
poverty level (Clemans-Cope and Garrett 2006).
Racial Disparities and Health Care
An extensive literature details disparities in self-reported health and disease-specific mortality
rates across racial and ethnic categories. Although the gap in self-reported health between whites
and blacks is reduced when comparing individuals in the same income categories, it does not
disappear (Kaiser Family Foundation 2007).
Insurance status differs by race and ethnicity, with approximately one third of Hispanics being
uninsured, 20 percent of blacks, and 13 percent of whites (Kaiser Commission 2006). Public
programs may help bridge some gaps in access to care. One small sample in New York reveals
that racial and ethnic disparities affecting a usual source of care and unmet health needs among
children disappear after enrollment in the State Children‘s Health Insurance Program (Shone et al.
2005).
Racial disparities in care—perhaps because of differences in quality of care or in different
funding levels for hospitals—may have spillover effects (Deaton 2003). One study finds that
mortality rates of older white people are positively associated with the proportion of blacks in the
community (Fuchs et al. 2001).
7 For example, many studies that consider effects of Medicaid expansions and contractions do not identify
specific individuals who gain or lose eligibility but look more broadly at potentially affected populations.

NUTRITION AND OBESITY
Although few children in the United States are malnourished, a larger share may not follow a
nutritional diet, which could have health consequences and potentially hinder educational
development. Social class may influence diets either if parents are not aware of or do not have the
resources necessary to provide healthy meals for their children. Poor nutritional choices may lead
to obesity, which has been linked to many health problems throughout the life span and, in some
instances, to lower wages in adulthood.
Emerging research suggests that diet may contribute to a host of conditions including anemia,
dental disease, hypertension, non-insulin dependent diabetes, coronary artery disease,
cerebrovascular disease, some cancers, and bone density problems. (See James et al. 1997 for an
overview.) One estimate attributes 365,000 deaths in 2000 to poor diet or lack of physical activity
(Mokdad et al. 2004). Additionally, pregnant women who do not consume adequate amounts of
some nutrients may risk having shorter pregnancies and delivering babies with lower
birthweights. (Read about the consequences of low birthweight.) Currie et al. (2007) find that
one nutritional choice—eating vegetables regularly—is significantly associated with better
childhood health, even when controlling for family income.
A child‘s nutrition can also affect academic achievement, which in turn may be critical for future
earnings. The Centers for Disease Control and Prevention (CDC) notes that when children are
chronically undernourished they perform less well on standardized achievement tests, perhaps in
part because they may be more prone to infections and miss more school (CDC 1996). Iron
deficiency, which can result from inadequate amounts of iron and vitamin C and lead to anemia,
is linked to fatigue, shorter attentions spans, and poorer intellectual performance (CDC 1996).
Not eating breakfast may also hamper academic performance. One study finds that participants in
the School Breakfast Program attend school more often and do better on standardized tests than
students who qualify for the program but do not participate (CDC 1996, citing Meyers et al.
1989). Some evidence suggests ties between food insecurity and behavioral problems. However,
it is not clear whether the behavioral problems result directly from poorer nutrition or the
psychosocial effect of uncertainty about food availability (Olson 1999).
Children at lower ends of the socioeconomic spectrum more often experience food insecurity.
One study finds that households living below the federal poverty line are more than 3.5 times as
likely to have insufficient food supplies compared with those above the poverty threshold (Rose
1999). Poorer families are also more likely to alter their food purchasing in response to changing
financial conditions. For example, during particularly cold months, poor families spend less on
food, while richer families do not decrease their grocery expenditures (Bhattacharya et al. 2002).
Although Bhattacharya et al. (2002) conclude that Food Stamps and other related social programs
are not sufficient to buffer poor families from some budget shortfalls, Rose (1999) argues that
Food Stamps do make a significant difference.
Although the research is not entirely consistent, several studies find that lower income households
are also less likely to make food consumption choices that are in line with nutritional
recommendations (James et al. 1997, Turrell et al. 2002). Palloni (2006) notes a socioeconomic
status gradient for macronutrient intake among adults in the United States and Canada (citing
Dubois and Girard 2001). Some evidence suggests that children are often spared the worse of
food shortages. For example, although food insufficient adults tend to have low nutrient intakes
(less than 50 percent of the recommended daily allowance) relative to non-insufficient
individuals, their children did not exhibit such patterns (Rose 1999).

Several factors could compound budgetary constraints in accounting for differences in nutritional
intakes by socioeconomic class. Low-income households tend to face slightly higher (about 1
percent) prices for the same food products as more well-off families, primarily because they are
less likely to live near and shop at large grocery stores (Kaufman et al. 1997). Yet, lower-income
families also spend less per unit of food in almost all categories than higher income individuals
(Kaufman et al. 1997). It is not clear whether those savings come at a cost of selecting foods with
lower nutritional content. Perhaps because of these types of barriers, coupled with financial
instability, some researchers suggest that efforts to educate families about better nutrition and
more healthful habits may have more of an effect on higher income individuals than lower-
income ones (Turrell et al. 2002). Kawachi and Marmot (1998) comment on a similar
phenomenon related to efforts to promote more exercise. They explain that people of higher
socioeconomic status may face fewer barriers—fear of crime, constraints on time particularly if
child care must be arranged, inability to afford membership to or living farther away from
recreational facilities—than poorer families.
Poor nutritional choices can also lead to overweight or obesity. Some evidence suggests that food
insecurity is associated with overweight. Olson (1999) finds a borderline statistically significant
relationship between food insecurity and body mass index (BMI), even after controlling for
income, education, single parent status, and employment status. In a review of literature, Burns
(2004) finds a consistent link between the risk of obesity for women and food insecurity
throughout Australia, Europe, and the United States. Burns provides an overview of theories
about how food insecurity and obesity could coexist, although there is little definitive evidence
for these pathways. For example, some suggest that the stress of food insecurity and lower
economic status contribute to obesity through either enodcrinological pathways or disordered
eating patterns. Townsend et al. (2001, cited in Burns 2004) theorize that people who receive
Food Stamps have greater supplies of food in the first three weeks of the month and run low at
the end of the month. This cycle of eating too much and then too little could lead to greater
weight gains—a theory that has not been tested in humans, but has been found in animals.
Different nutritional patterns by socioeconomic class may be related to the greater risk of
overweight for lower income children. For example, Strauss and Knight (1999) use the National
Longitudinal Survey of Youth to follow over a six year period children who start out at normal
weight. They find that when controlling for initial height and weight and maternal BMI, being in
the bottom 15th percentile of family income significantly increases the risk of the child being
obese. Strauss and Knight also find that the maternal obesity is greatest predictor of childhood.
Research on twins and adopted families suggests that heredity may count for between 5 and 40
percent of the risk of obesity, and genetics may play an even greater influence on BMI (U.S.
Department of Health and Human Services, ―Childhood Obesity‖).
In addition to health consequences, some studies link obesity to poorer academic outcomes. Datar
et al. (2004) find that overweight children fall behind their peers in math and reading test scores
starting as early as kindergarten. Several studies tie weight to poorer employment and income
outcomes in adulthood. There are several potential explanations: high body weight could lead to
lower income because of discrimination or lower productivity or academic achievement; lower
income status could lead to obesity, perhaps through some of the nutritional pathways discussed
above; or there could be a third factor responsible for both body weight and educational or
occupational outcomes. Cawley (2004) finds that overweight white females earn on average 4.5
percent less than those of normal weight, and obese white women earn 11.9 percent less than
normal weight women. He argues that the magnitude of the second effect is comparable to the
impact of 1.8 years of education or 3.8 years of work experience. Obese black and Hispanic
females also earn less than their peers with healthy weight, but the effect size is smaller. Conley

and Glauber (2005) find that although a women‘s body mass does not seem to have a direct effect
on her labor market earnings, her weight is highly correlated with her family income. Body
weight 13 to 15 years earlier is a good predictor of a women‘s probability of being married, both
her and her husband‘s occupational prestige, and her spouse‘s earnings.
This discussion points to several ways that nutrition and overweight may be mechanisms through
which economic status is passed on through the generations. Just as in the discussion of children‘s
health in general, if poorer children consume worse nutrition it could make it harder for them to
succeed in school and cause health problems that eventually lead to declines in earnings. In
addition, the strong genetic component of overweight may be transmitted from one generation to
the next.

ASTHMA
Asthma plays a particularly important role in explaining the income gradient in health.8
According to Case et al. (2002), the greater frequency of occurrence of the respiratory condition
and its greater severity among poorer children accounts for 20 percent, or the largest share, of that
gradient. Although there is no association between asthma and socioeconomic class for older
children or teenagers, asthma is more prevalent among lower-income children (Case et al. 2002,
Neidell 2004 quoting American Academy of Pediatrics 2000). Asthma has deleterious effects on
health both among children and adults. It is the most common reason for children‘s emergency
hospital visits and hospital admissions (Neidell 2004 citing National Institute of Environmental
Health Sciences 2000). It also is associated with conditions later in life such as lung cancer
(Neidell 2004 citing Ernster 1996).
Several studies suggest that differences in rates of asthma diagnoses and severity of the condition
may be linked to exposure to toxins. Prevalence of indoor allergens may contribute to these
patterns (Milton et al. 2004 citing Kitch et al. 2000; Rauh et al. 2002). Neidell (2004) shows that
lower socioeconomic communities (defined by zip codes with a high share of adults over age 25
without a high school diploma) have higher average levels of all pollutants. He finds that
exposure to carbon monoxide significantly affects asthma-related hospitalizations for children.9
Neidell (2004) further finds an interaction between SES and pollution exposure for some age
groups, supporting the theory that the same amount of pollution may have a greater negative
impact on poor children than on non-poor children.
In addition to affecting health, childhood asthma may impede children‘s education. Asthma is one
of the leading causes of children missing school (Neidell 2004 citing National Institute of
Environmental Health Sciences 2000). Yet, despite consistent findings that children with asthma
have higher absence rates, a review of the literature finds no studies revealing a difference in
academic performance between asthmatic children and asymptomatic ones (Milton et al. 2004).
On the other hand, some evidence suggests that asthma has a more negative impact on children in
lower-income families. For example, Fowler et al. (1992) conclude that for children living in
families with less than $20,000 in income, asthmatic children had twice the odds of grade failure
than their non-asthmatic peers. A limiting factor among earlier studies of asthma and school
readiness /or behavior is that asthma is more prevalent among poor and minority children Currie
(2008, forthcoming). Furthermore, these children are less likely than other asthmatic children to
receive regular treatment. The small number of studies that examine whether the impacts of
childhood asthma extend to the working world, find a small decrease in labor market participation
associated with childhood asthma (Milton et al. 2004).10
8Environmental toxins also influence health through mechanisms other than asthma. For example, higher
amounts of air pollution correlate with community-level mortality rates (Fuchs et al. 2001 and Mokdad et
al. 2004). Currie (2008) provides a more complete review of this literature. 9 Opponents of this view point out that asthma hospitalizations have increased, even as pollution has
decreased. Neidell, however, finds a significant relationship between asthma and pollution when he takes
into account the fact that individuals may avoid exposure to pollution—for example by reducing outdoor
time on days that have smog warnings. 10
One study only finds an effect for women; the other focuses on severe cases of asthma.

HEALTH IN ADULTHOOD
As with childhood health, a gradient can be observed by which mortality declines and self-
reported health status improves with greater income.11
The correlation between the logarithm of
family income and self-reported health peaks between ages 50 and 60 with a value of about -0.4
(Deaton and Paxson 1998).12
Some evidence suggests that this gradient has increased over time.
Several factors could contribute to this relationship. For one, health could influence labor force
participation or earnings. Although some economists doubt that causality could flow from
economic status to health (see Ericksson et al. 2005, for example), others find support for the
notion that lower income in adulthood could contribute to worse health—either as a direct effect
on the ability to purchase medical care and other healthful resources, or because lower income is
correlated with stresses and occupational attributes that are deleterious to health. Another
possibility is that inequities in income may contribute to poor health. If both lower socioeconomic
status in adulthood leads to poor health and poor health leads to lower socioeconomic status, the
health-socioeconomic status cycle in adulthood could affect intragenerational mobility.
Individuals may experience more stickiness in their relative socioeconomic position if their health
status helps reinforce that position. Additionally, intergenerational mobility could be hampered if
parents‘ socioeconomic status and genetics help determine a child‘s health. Childhood health,
directly or through education, might help determine adult health, which could influence income.
Case et al. (2005) provide some evidence suggesting that health in childhood can have a direct
effect on health in adulthood. For example, both parental health and chronic conditions at age 16
help predict health in middle age, even after controlling for education, health, and economic
status as a young adult. Alternatively, pathways models hold that the resemblance between health
in childhood and health in adulthood occurs because poor childhood health lowers socioeconomic
status in early adulthood, which in turn contributes to deteriorating health. Childhood health may,
for example, impact educational achievement. Researchers hypothesize that education influences
adult health if greater education allows individuals to better chose health resources, follow
medical advice, or become more ―future oriented.‖ Currie and Madrian (1999) note that the
means by which education might contribute to health are uncertain. Grossman and Kaestner
(1997) conclude that such a causal relationship likely does exist. It is also possible that
individuals with better education or more financial resources may be better able to take measures
to promote health—such as getting more regular exercise (Kawachi and Marmot 1998).
Others hypothesize that stress from lower economic status reduces health. Smith (1999) describes
a physiological process by which stress releases adrenalin, which may over time affect blood
pressure, heart rate, and the immune system. Animal models supply some support for this notion
(see discussion in Marmot et al. 1997).
Evidence from the Whitehall studies of British social servants falls in line with the hypothesis
that occupational status and related stress might contribute to a health gradient. Men with the
lowest grade (clerical and office-support) have an age-adjusted odds ratio of developing coronary
heart disease of 1.5 relative to men at the highest grade (Marmot et al. 1997). This study finds
11
Health status is an ordinal variable with better health conditions taking on lower values than worse health
conditions, leading to the negative correlation coefficient in the Deaton and Paxson 1998 study mentioned
below. 12
Deaton and Paxson (1998) note that after age 60, income is less able to predict self-reported health status.
The authors hypothesize this could reflect both participation in Medicare and a shift of income from labor
earnings to pension.

that the largest contributing factor to explaining this gradient was the amount of control
individuals had over their work.
Additionally, Wilkinson (1994) discusses research suggesting that friendships and social support
may benefit health and in particular may be protective in economic hardship; yet poorer
individuals and those in occupations with lower status often have less social contact. In another
study, individuals who eventually lost their jobs because of a factory closure began to experience
deteriorating health after the announcement was made, but before they were actually unemployed
(Wilkinson 1994, citing Beale and Nethercott 1985). In their longitudinal study, Ross and
Mirowsky (2000) also find that change in employment is more likely to have a significant impact
on health than baseline employment.
A controversial extension to the notion that status-related stress may lead to health problems is
that greater income inequality may account for differences in health in cross-country
comparisons. Wilkinson (1994) argues that relative deprivation has a larger impact on mortality
rates among developed countries than absolute living standard; countries with the most narrow
income distributions and the fewest people living in relative poverty have the highest life
expectancies. Deaton (2003) reviews this literature and concludes that although stress may play a
role in deteriorating health, it is not necessarily because of differences in income per se. Other
studies find that controlling for other factors can explain away much of the apparent income-
inequity health disparity.
The correlation between health in adulthood and economic status may also be partially attributed
to the physical demands of some jobs. For example, Case et al. (2005) find that having a manual
labor position helps explain the health deficit among people of lower economic status. (See also
discussion of disability.)

SUBSTANCE USE
Smoking and alcohol abuse lead to adverse health effects, and some evidence suggests that the
behaviors are transmitted from one generation to the next. In addition, some evidence suggests
that these behaviors can lead to declines in socioeconomic status. Also, exposure to the stresses
of lower social class may increase the behavior in future generations.
The health effects of smoking and excessive drinking are well established. Numerous Surgeon
General‘s reports identify tobacco use as the largest cause of avoidable disease, disability, and
death in this country (CDC 2007). The most recent says the ―evidence is sufficient to infer a
causal relationship between smoking‖ and 10 forms of cancer, coronary heart disease, chronic
obstructive pulmonary disease, and a host of other conditions (CDC 2004). Tobacco use can also
have severe consequences for nonsmokers, as demonstrated by increased morbidity and mortality
for individuals exposed to secondhand smoke (CDC 2006). Of particular interest in the question
of economic mobility is the long-term effects on the health of children who were exposed to
maternal second hand smoke during gestation. (See discussion on health at birth.) Alcohol use
also has the potential to reduce health: not only can excessive use in the short term contribute to
traffic accidents, other unintentional injuries, and potentially fatal alcohol poisoning, but over
time it is linked to depression, cancers, and liver disease (CDC ―General Information on Alcohol
and Health‖).
Alcoholism and smoking behavior can be transmitted from one generation to the next through a
combination of genetic pathways and cultural and environmental ones. A review of studies finds
that alcoholics have a four-fold increased risk of having a first-degree relative who is alcoholic,
compared with the general population (Agarwal 2001). A meta-analysis of twin studies finds that
genetics accounts for about 37 percent of the determination of smoking initiation in male adults
and 55 percent in female adults (Li et al. 2003). Genetics may play an even more prominent role
in the progression of smoking behavior and the strength of nicotine dependence (Vink et al. 2005,
Fowler et al. 2007). Additionally, specific gene mutations may increase not only susceptibility to
smoking behavior, but also the likelihood of suffering adverse health risks such as cancer
(Munafò et al. 2004). (See Kronstadt literature review on genetics and economic mobility.) For
a nongenetic explanation, Duncan et al. (2005) suggest that role modeling may play a role—if
children observe their parents drinking heavily or using drugs, they may determine that it is
acceptable for them as well.
There is also evidence of a greater prevalence of substance dependence and smoking among
people of lower socioeconomic class. For example, college graduates have lower rates of
substance dependence or abuse than non-high-school-graduates13
and data show that 17.6 percent
of unemployed adults show substance dependence or use compared with only 10.2 percent of
adults with full-time work (SAMHSA). For smoking, being below 200 percent of the poverty
line, having less than a college degree, and being a blue collar worker are all associated with
significantly higher odds of being a current smoker (Barbeau et al. 2004). One hypothesis that
seeks to explain why lower economic status might lead to more risk behaviors, is that children
growing up in low-income households may be more likely to use substance abuse as a mechanism
for coping with stress. For example, one study finds that among children whose parents had
divorced by age 15 (a non-economic stress), girls have higher rates of smoking and boys have
higher rates of alcohol consumption (Smith 1999 citing Wadsworth and Kuh 1997).
13
Current college students have higher rates.

Some evidence supports the hypothesis that these risky behaviors might lead to lower income by
reducing the amount of time individuals spend at work. The Surgeon General‘s report points out a
consistent pattern of higher rates of absenteeism among cigarette smokers compared with
nonsmokers (2004). Another study tracks individuals over time to determine the sequel to a
hospitalization for an alcohol-related condition (Romelsjo et al. 2004). This study concludes that
following the hospitalization, individuals of all socioeconomic classes have a significantly higher
probability of leaving the workforce compared with individuals in the general population.
Research by Mullahy and Sindelar (1993) indicates that alcoholism may adversely affect income,
largely by reducing the likelihood of working. However, the authors caution that the correlation
between alcoholism and earnings may stem from another problem that influences both working
and drinking behavior. Alternatively, lower earnings may contribute to alcoholic behavior.
However, risky behaviors are unlikely to explain the entire gap in health status across the income
spectrum. Smith (1999, p. 148) notes that ―research consensus is that health disparities by
economic status are only partially mitigated when extensive controls are included for health risk
behaviors.‖

MENTAL HEALTH
A number of epidemiological studies identify an association between mental illness and
socioeconomic status, measured using education, income, or occupation. Hudson and
Dohrenwend (1992) provide a brief overview of this literature. There is no consensus yet on the
causal direction behind this relationship—whether low socioeconomic status contributes to
mental illness (causation) or whether mental illness may limit the ability of individuals to get
ahead by limiting educational attainment and employment (selection).
The causation theory suggests that factors more common in low socioeconomic status
environments may help precipitate mental illnesses. According to Miech et al. (1999) some of the
factors examined include stress, weaker coping resources, and less control (occupational or
otherwise). For example, Hudson (2005) finds that signs of economic stresses, including
unemployment, affordability of housing, and poverty rates, help explain the mental illness.
In contrast, selection theories suggest that mental illness leads to lower socioeconomic status.
Selection process may help explain downward intragenerational mobility if adults have difficulty
maintaining their employment because of mental illness. About 27 percent of recipients of Social
Security Disability Insurance have mental conditions other than retardation (Social Security
Administration 2006). Bartel and Taubman (1986) find that mental illness has a strong negative
effect on earnings of working age men. Another study finds that psychiatric disorders reduce the
likelihood of employment by approximately 11 percentage points (Ettner et al. 1997). Although
researchers try to account for reverse causality, it is difficult to rule out the possibility that poorer
labor force outcomes contribute to mental illness. Bartel and Taubman (1986) examine the effect
of mental illness on marriage and find signs of causality running in both directions. They
conclude that some diagnoses make it more likely that individuals never marry, whereas divorce
and death of a spouse are also associated with new diagnoses of mental illness.
As Miech et al. (1999) explain, selection may also work across generations because there is
evidence that genetic and environmental factors help transmit disorders. For example, Ritscher et
al. (2001) explain that individuals with a family history of major depressive disorder are at
increased risk of the condition. It is also quite possible that selection and causation work together.
For example, if socioeconomic class-related stresses cause individuals to slip into a lower class,
the stresses from being in that class might further exacerbate the mental condition (Miech et al.
1999). Extending this to two generations, it is possible that living with a parent who is unable to
provide a stable environment may ―cause‖ a child to develop a mental disorder. (See
Childrearing in Families by Kronstadt and Favreault.) This effect could be exacerbated if the
parent passes along a genetic predisposition for the condition.
Several studies examine whether intergenerational mobility differs for seriously mentally ill
individuals compared with the general population. This evidence is mixed and seems to depend
on methodological differences. For example, Fox (1990, cited in Rodgers and Mann 1993) finds
little evidence of statistically significant differences between the two populations. However,
Rodgers and Mann (1993) find significantly greater downward mobility among patients with
psychiatric disorders when analyzing the same data sets with a different approach.
Socioeconomic pathways associated with mental illness appear to vary by condition. For
example, schizophrenia often supports theories of selection, suggesting that genetics may play a
more important role than stresses in transmitting this condition from one generation to the next
(Dohrenwend et al. 1992). Research consistently finds that schizophrenics have a lower level of
occupational attainment than would be predicted by their level of education, implying that the

disorder prevents them from reaching their income potential (Link et al. 1986). However, the
relationship may be more complicated. When Link et al. (1986) examine the first jobs of
schizophrenics, they find no deficit in prestige given their educational level. Yet a higher
proportion of schizophrenics are exposed to what they term ―noisome‖ conditions—such as
extreme temperatures, loud noises, or dangers—in that first job relative to individuals who do not
have schizophrenic episodes. These authors interpret their study as suggesting that at least among
individuals who might be susceptible to schizophrenia, some individuals from lower
socioeconomic status families may end up in jobs that expose them to stresses that may help
trigger the disorder. It is also possible that the precursors of the mental illness select them into
lower education outcomes, which then increase their likelihood of landing a first job that further
exacerbates the condition.
In contrast, more evidence appears to support causation theories for depression. One study finds
that children of parents with low parental socioeconomic status have more than triple the risk of
having a major depressive disorder even after controlling for a history of depression among the
parents (Ritscher et al. 2001). Yet these researchers find no evidence that either having a parent
with depression or the respondents‘ own depression links to failure to succeed in terms of income,
occupational status, or education. Other research finds that holding a job involving control and
direction helps protect against depression (Hudson 2005, citing Link et al. 1993). Furthermore,
wealth seems to be negatively associated with depression even when controlling for job prestige.
Marmot (2002) suggests that this could be causal—if having more wealth, for example, makes
people feel more optimistic. Alternatively, wealth may reflect past advantages, or may be a signal
for another trait altogether.
Some evidence suggests that adolescents with depression do not succeed as well in school, which
might be consistent with selection models. Twenge and Nolen-Hoeksema (2002) review literature
suggesting that children with chronic, moderate depression do not perform as well in school and
may have some interpersonal impairments. Other research shows that conduct disorder leads to
lower education attainment. Miech et al. (1999) find that New Zealander adolescents who meet a
clinical criteria for conduct disorder are 4.5 times less likely to earn a school certificate, when
controlling for family socioeconomic status. In their longitudinal study, they find failing to
achieve academic success further exacerbates their condition several years later—indicating that
both selection and causation might be at play.
Attention Deficit and Hyperactivity Disorder (ADHD) is also associated with poorer academic
achievement (Miech et al. 1999, also Barkley et al. 1990, cited in Currie and Lin 2007). Currie
and Lin (2007) find ADD more prevalent among poor children, and they are more likely to be
limited by the condition. The authors suggest the importance of helping poor families better
manage these types of mental conditions. They also mention research showing that premature
birth may increase the risk of ADHD (Currie and Lin 2007, citing Linnet et al. 2006).

GLOSSARY
Intrageneraional Mobility measures the change in one‘s economic situation over a period of years
within a single generation, or one lifetime. By measuring the evolution of an individual‘s
or family‘s income over time, one can determine intragenerational mobility in absolute or
relative terms.
Intergenerational Mobility refers to mobility from one generation to the next and captures the
extent to which a child‘s economic success is independent from that of his or her parents.
A society will have greater intergenerational mobility when there is a weaker correlation
between a child‘s income and his or her parents‘ income.
Intergenerational Correlation of Income is one way of measuring intergenerational economic
mobility and describes the strength of the relationship between parents‘ and children‘s
income. The correlation can range from 0 to 1; the higher the correlation the stronger the
association between parents‘ and child‘s incomes.

REFERENCES
Adams, Peter, Michael Hurd, Daniel McFadden, Agnela Merrill, and Tiago Ribeiro. 2003.
―Healthy, Wealthy and Wise? Tests for direct causal paths between health and socioeconomic
status.‖ Journal of Econometrics, 112 (1): 3–56.
Agarwal, Dharam P. 2001. ―The Genetics of Alcohol Metabolism and Alcoholism.‖ International
Journal of Human Genetics, 1 (1): 25–32.
Almond, Douglas. 2006 ―Is the 1918 Influenza Pandemic Over? Long-term Effects of In Utero
Influenza Exposure in the Post-1940 U.S. Population.‖ Journal of Political Economy,
114 (4): 672–712.
Almond, Douglas, Kenneth Chay, and David Lee. 2005. ―The Costs of Low Birth Weight.‖
Quarterly Journal of Economics, 120 (3): 1031–1084.
Almond, Douglas and Bhashkar Mazumder. 2005. ―The 1918 Influenza Pandemic and
Subsequent Health Outcomes: An Analysis of SIPP Data.‖ American Economic Review,
95 (2): 258–262.
American Academy of Pediatrics. 2000. Guide to Your Child’s Allergies and Asthma. New York:
Villard Books.
Ayanian, J. Z., J. S. Weissman, E. C. Schneider, J. A. Ginsburg, and A. M. Zaslavsky. 2000.
―Unmet Health Needs of Uninsured Adults in the United States.‖ Journal of the American
Medical Association, 284 (16): 2061–2069.
Baker DW, MF Shapiro, and CL Schur. 2000. ―Health Insurance and Access to Care for
Symptomatic Conditions.‖ Archives of Internal Medicine, 160 (9): 1269–1274.
Barbeau, Elizabeth M, Nancy Krieger, and Mah-Jabeen Soobader. 2004. ―Working Class Matters:
Socioeconomic Disadvantage, Race/Ethnicity, Gender, and Smoking in NHIS 2000.‖
American Journal of Public Health, 94 (2): 269–278.
Barker, David JP. 1997. ―Maternal Nutrition, Fetal Nutrition and Diseases in Later Life.‖
Nutrition, 13 (9): 807–813.
Barkley, RA, M Fischer, CS Edelbrock, and LMA Smallish. 1990. ―The Adolescent Outcome of
Hyperactive Children Diagnosed by Research Criteria: I. An Eight-Year Prospective Follow-
up Study.‖ Journal of the American Academy of Child and Adolescent Psychiatry, 29 (4):
546–557.
Bartel, A and P Taubman. 1986. ―Some Economic and Demographic Consequences of Mental
Illness.‖ Journal of Labor Economics, 4 (2): 243–256.
Beale, Norman and Susan Nethercott. 1985. ―Job-Loss and Family Morbidity: A Study of a
Factory Closure.‖ Journal of the Royal College of General Practitioners, 35 (280): 510–514.
Behrman, JR, and MR Rosenzweig. 2004. ―Returns to Birth Weight.‖ Review of Economics and
Statistics, 86(2): 586–601.
Bhattacharya, J, T DeLeire, S Haider, and J Currie. 2002. ―Heat or Eat? Cold Weather Shocks
and Nutrition in Poor American Families.‖ NBER Working Paper no. 9004. Cambridge, MA:
National Bureau of Economic Research.

Blanden, J, P Gregg, and L Macmillan. 2006. ―Explaining Intergenerational Income Persistence:
Non-cognitive Skills, Ability and Education.‖ Centre for Market and Public Organisation
Working Paper no. 06/146. Bristol, United Kingdom: Centre for Market and Public
Organisation.
Bound, John, and Richard V Burkhauser. 1999. ―Economic Analysis of Transfer Programs
Targeted on People with Disabilities.‖ In Handbook of Labor Economics, vol. 3A, edited by
Orley Ashenfelter and David Card (3417–3528). Amsterdam: Elsevier Science/North
Holland.
Burkhauser, Richard V, and David C Stapleton. 2003. ―Introduction.‖ In The Decline in
Employment of People with Disabilities: A Policy Puzzle, edited by Stapleton and Burkhauser
(1–21). Kalamazoo, MI: WE Upjohn Institute for Employment Research.
Burns, Cate. 2004. ―A Review of the Literature Describing the Link between Poverty, Food
Insecurity and Obesity with Specific Reference to Australia.‖ Melbourne: Victorian Health
Promotion Foundation.
Case, Anne, Angela Fertig, and Christina Paxson. 2005. ―The Lasting Impact of Childhood
Health and Circumstance.‖ Journal of Health Economics, 24 (2): 365–389.
Case, Anne, Darren Lubotsky, and Christina Paxson. 2002. ―Economic Status and Health in
Childhood: The Origins of the Gradient.‖ American Economic Review, 92 (5): 1308–1334.
Case, Anne and Christina Paxson. 2002. ―Parental Behavior and Child Health.‖ Health Affairs, 21
(2): 164–178.
–––2006. ―Children‘s Health and Social Mobility.‖ The Future of Children, 16 (2): 151–173.
Cawley, John. 2004. ―The Impact of Obesity on Wages.‖ Journal of Human Resources, 39 (2):
451–74.
Centers for Disease Control and Prevention. 1996. ―Guidelines for School Programs to Promote
Lifelong Healthy Eating.‖ Morbidity and Mortality Weekly, 45 (RR-9): 1–33.
––– 2004. ―2004 Surgeon General‘s Report—The Health Consequences of Smoking.‖
http://www.cdc.gov/tobacco/data_statistics/sgr/sgr_2004.
––– 2006. ―General Information on Alcohol and Health.‖
http://www.cdc.gov/alcohol/quickstats/general_info.htm.
––– 2007. ―Targeting Tobacco Use: The Nation‘s Leading Cause of Preventable Death: At a
Glance 2007.‖ http://www.cdc.gov/nccdphp/publications/aag/osh.htm.
––– 2006. ―The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of
the Surgeon General—Executive Summary.‖ Washington, D.C.: Department of Health and
Human Services.
Charles, Kerwin Kofi. 2003. ―The Longitudinal Structure of Earnings Losses among Work-
Limited Disabled Workers.‖ The Journal of Human Resources, 38 (3): 618–646.
Cianfarani, S, D Germani, and F Branca. 1999. ―Low Birthweight and Adult Insulin Resistance:
The ‗Catch-up Growth‘ Hypothesis.‖ Archives of Disease in Childhood-Fetal and Neonatal
Edition, 81: F71–F73.

Clemans-Cope, L and B Garrett. 2006. ―Changes in Employer-Sponsored Health Insurance
Sponsorship, Eligibility, and Participation: 2001–2005.‖ Washington, D.C.: Kaiser
Commission on Medicaid and the Uninsured.
Conley, D and NG Bennett. 2000. ―Is Biology Destiny? BirthWeight and Life Chances.‖
American Sociological Review, 65 (3): 458–467.
––– 2001. ―Birth Weight and Income: Interactions across Generations.‖ Journal of Health and
Social Behavior, 42 (4): 450–465.
Conley, D and R Glauber. 2005. ―Gender, Body Mass and Economic Status.‖ NBER Working
Paper no. 11343. Cambridge, MA: National Bureau of Economic Research.
Currie, J. Forthcoming. ―Healthy, Wealthy, and Wise: Is There a Causal Relationship Between
Child Health and Human Capital Development?‖ Journal of Economic Literature.
Currie, Alison, Michael A Shields, Stephen Wheatley Price. 2007. ―The Child Health/Family
Income Gradient: Evidence from England.‖ Journal of Health Economics, 26 (2): 213–232.
Currie, J and R Hyson. 1999. ―Is the Impact of Health Shocks Cushioned by Socio-Economic
Status? The Case of Low Birthweight.‖ American Economic Review, Papers and Proceedings,
89 (2): 245–250.
Currie, J and W Lin. 2007. ―Chipping away at Health: More on the Relationship between Income
and Child Health.‖ Health Affairs, 26 (2): 331–344.
Currie, J and B Madrian. 1999. ―Health, Health Insurance and the Labor Market.‖ In Handbook of
Labor Economics, vol. 3A, edited by Orley Ashenfelter and David Card (3309–3416).
Amsterdam: Elsevier Science/ North Holland.
Currie, J and E Moretti. 2007. ―Biology as Destiny: Short and Long-Run Determinants of
Intergenerational Transmission of Birth Weight.‖ Journal of Labor Economics, 25 (2): 231–
264.
Currie, J and M Stabile. 2003. ―Socioeconomic Status and Child Health: Why Is the Relationship
Stronger for Older Children?‖ American Economic Review, 93 (5): 1813–1823.
Datar, A, R Sturm, and JL Magnabosco. 2004. ―Childhood Overweight and Academic
Performance: National Study of Kindergartners and First-Graders.‖ Obesity Research, 12 (1):
58–68.
Davidoff, A, G Kenney, L Dubay. 2005. ―Effects of State Children‘s Health Insurance Program
Expansions on Children with Chronic Health Conditions.‖ Pediatrics, 116 (1): e34–e42.
Deaton, Angus. 2003. ―Health, Inequality, and Economic Development.‖ Journal of Economic
Literature, 41 (1): 113–158.
Deaton, A and C Paxson. 1998. ―Aging and Inequality in Income and Health.‖ American
Economic Review, Paper and Proceedings, 88 (2): 248–253.
Devaney, Barbara, Linda Bilheimer, and Jennifer Schore. 1992. ―Medicaid Costs and Birth
Outcomes: The Effects of Prenatal WIC Participation and the Use of Prenatal Care.‖ Journal
of Policy Analysis and Management, 11 (4): 573–592.
Dohrenwend, BP, I Levav, PE Shrout, S Schwartz, G Naveh, BG Link, AE Skodol, and A Stueve.
1992. ―Socioeconomic Status and Psychiatric Disorders: The Causation-Selection Issue.‖
Science, 255 (5047): 946–952.
Doyle, O, C Harmon, and I Walker. 2005. ―The Impact of Parental Income and Education on the
Health of their Children.‖ IZA Working Paper no. 1832. Bonn, Germany: IZA.
Dubois, L and M Girard. 2001. ―Social Position and Nutrition: A Gradient Relationship in
Canada and the USA.‖ European Journal of Clinical Nutrition, 55 (5): 366–373.
Duncan, G, A Kalil, SE Mayer, R Tepper, and MR Payne. 2005. ―The Apple Does Not Fall Far
from the Tree.‖ In Unequal Chances: Family Background and Economic Success, edited by
Samuel Bowles, Herbert Gintis, and Melissa Osborne Groves (23–79). New York: Russell
Sage Foundation and Princeton University Press.
Eriksson, T, B Bratsberg, and O Raaum. 2005. ―Earnings Persistence across Generations:
Transmission through Health?‖ University of Oslo, Department of Economics, Memorandum
no. 35/2005. Oslo, Norway: University of Oslo.
Ernster, V. 1996. ―Female Lung Cancer.‖ Annual Review of Public Health, 17: 97–114.
Ettner, SL, RG Frank, and RC Kessler. 1997. ―The Impact of Psychiatric Disorders on Labor
Market Outcomes.‖ NBER Working Paper no. 5989. Cambridge, MA: National Bureau of
Economic Research.
Fiscella, K. 1995. ―Does Prenatal Care Improve Birth Outcomes? A Critical Review.‖ Obstetrics
& Gynecology, 85 (3): 468–479.
Fowler, MG, MG Davenport, and R Garg. 1992. ―School Functioning of U.S. Children with
Asthma.‖ Pediatrics, 90 (6): 939–944.
Fowler, T, K Lifford, K Shelton, F Rice, A Thapar, MC Neale, A McBride, MBM van den Bree,
and BM Marianne. 2007. ―Exploring the Relationship between Genetic and Environmental
Influences on Initiation and Progression of Substance Use.‖ Addiction, 102 (3): 413–422.
Fox, John W. 1990. ―Social Class, Mental Illness, and Social Mobility: The Social Selection-Drift
Hypothesis for Serious Mental Illness.‖ Journal of Health and Social Behavior, 31 (4): 344–
353.
Fuchs, Victor, Mark McClellan, and Jonathan Skinner. 2001. ―Area Differences in Utilization of
Medical Care and Mortality among U.S. Elderly.‖ NBER Working Paper no. 8628.
Cambridge, MA: National Bureau of Economic Research.
Garrett, B and A Yemane. 2006. ―Racial and Ethnic Differences in Insurance Coverage and
Health Care Access and Use: A Synthesis of Findings from the Assessing the New
Federalism Project.‖ Assessing the New Federalism Discussion Paper 06-01. Washington,
D.C.: The Urban Institute.
Goldman, DP, Geoffrey F Joyce, and Yuhui Zheng. 2007. ―Prescription Drug Cost Sharing:
Associations with Medication and Medical Utilization and Spending and Health.‖ Journal of
the American Medical Association, 298 (1): 61–69.

Grossman, M. 1975. ―The Correlation between Health and Schooling.‖ In Household Production
and Consumption, edited by Nestor E. Terleckyj (147-211). New York: National Bureau of
Economic Research.
Grossman, Michael and Robert Kaestner. 1997. ―Effects of Education on Health.‖ In The Social
Benefit of Education, JR Behrman and N. Stacey (69–123). Ann Arbor, MI: University of
Michigan Press.
Hadley, Jack. 2003. ―Sicker and Poorer: The Consequences of Being Uninsured.‖ Medical Care
Research and Review, 60 (2) supplement: 3S–75S.
Hayward, Mark D, William R Grady, Melissa A Hardy, and David Sommers. 1989.
―Occupational Influences on Retirement, Disability, and Death.‖ Demography, 26 (3): 393–
409.
Hertz, Tom. 2006. ―Understanding Mobility in America.‖ Washington, D.C.: Center for
American Progress.
Himmelstein, David U, Elizabeth Warren, Deborah Thorne, and Steffie Woolhandler. 2005.
―MarketWatch: Illness and Injury as Contributors to Bankruptcy.‖ Health Affairs, Web
Exclusive. http://content.healthaffairs.org/cgi/content/abstract/hlthaff.w5.63v1.
Hudson, CG. 2005. ―Socioeconomic Status and Mental Illness: Tests of the Social Causation and
Selection Hypotheses.‖ American Journal of Orthopsychiatry, 75 (1): 3–18.
Institute of Medicine. 2001. Coverage Matters: Insurance and Health Care. Washington, D.C.:
Institute of Medicine, National Academy Press.
–––2002. Care without Coverage: Too Little, Too Late. Washington, D.C.: Institute of medicine,
National Academy Press.
James, W Philip T, Michael Nelson, Ann Ralph, and Suzi Leather. 1997. ―Socioeconomic
Determinants of Health: The Contribution of Nutrition to Inequalities in Health.‖ BMJ, 314:
1545–1549.
Johnson, RC, and RF Schoeni. 2007. ―Early Life Events and Health and Labor Market Outcomes
in Adulthood.‖ Revised draft of paper presented at the annual meeting of the Society of Labor
Economists, Cambridge, May 5, 2006.
Kaestner, R, T Joyce, and A Racine. 1999. ―Does Publicly Provided Health Insurance Improve
the Health of Low-Income Children in the United States?‖ NBER Working Paper no. 6887.
Cambridge, MA: National Bureau of Economic Research.
Kaiser Commission on the Medicaid and the Uninsured. 2006. ―The Uninsured: A Primer.‖
Washington, D.C.: Kaiser Commission on Medicaid and the Uninsured.
Kaiser Family Foundation, Henry J. 2007. ―Key Facts: Race, Ethnicity & Health Care.‖
http://www.kff.org/minorityhealth/upload/6069-02.pdf.
Kaufman, Philip R, James M MacDonald, Steve M Lutz, and David M Smallwood. 1997. ―Do the
Poor Pay More for Food? Item Selection and Price Differences Affect Low-Income
Household Food Costs.‖ Agricultural Economic Report No. 759. Washington, D.C.: U.S.
Department of Agriculture.

Kawachi, I and MG Marmot. 1998. ―What Can We Learn from Studies of Occupational Class and
Cardiovascular Disease?‖ American Journal of Epidemiology, 148 (2): 160–163.
Kitch, BT, G Chew, HA Burge, ML Muilenberg, ST Weiss, TAE Platts-Mills, G O‘Connor, and
DR Gold. 2000. ―Socioeconomic Predictors of High Allergen Levels in Homes in the
Greater Boston Area.‖ Environmental Health Perspectives, 108 (4): 301–307.
Li, MD, R Cheng, JZ Ma, GE Swan. 2003. ―A Meta-analysis of Estimated Genetic and
Environmental Effects on Smoking Behavior in Male and Female Adult Twins.‖ Addiction,
98 (1): 23–31.
Link, BG, BP Dohrenwend, and AE Skodol. 1986. ―Socio-economic Status and Schizophrenia:
Noisome Occupational Characteristics as a Risk Factor.‖ American Sociological Review, 51
(2): 242–258.
Link, BG, MC Lennon, and BP Dohrenwend. 1993. ―Socioeconomic Status and Depression: The
Role of Occupations involving Direction, Control, and Planning.‖ American Journal of
Sociology, 98 (6): 1351–1387.
Linnet, KM, K Wisborg, E Agerbo, NJ Secher, PH Thomsen, and TB Henriksen. 2006.
―Gestational Age, Birth Weight, and the Risk of Hyperkinetic Disorder.‖ Archives of Disease
in Childhood, 91 (8): 655–660.
Lleras-Muney, A. 2005. ―The Relationship between education and adult mortality in the United
States.‖ Review of Economic Studies, 72 (1): 189–221.
Loprest, PJ and E Maag. 2003. ―The Relationship between Early Disability Onset and Education
and Employment.‖ Washington, D.C.: The Urban Institute.
Marmot, Michael. 1999. ―Multi-Level Approaches to Understanding Social Determinants.‖ In
Social Epidemiology, edited by Lisa Berkman and Ichiro Kawachi. Oxford: Oxford
University Press.
––– 2002. ―The Influence of Income on Health: Views of an Epidemiologist. Does Money Really
Matter? Or Is It a Marker for Something Else?‖ Health Affairs, 21 (2): 31–46.
Marmot, MG, H Bosma, H Hemingway, E Brunner, and S Stansfeld. 1997. ―Contribution of Job
Control and Other Risk Factors to Social Variations in Coronary Heart Disease Incidence,‖
Lancet, 350 (9073): 235–239.
Mazumder, Bhashkar. Forthcoming. ―Does Education Improve Health? A Re-examination of the
Evidence from Compulsory Schooling Laws.‖ Economic Perspectives.
McCormick, Marie C. 2001. ―Prenatal Care - Necessary but Not Sufficient.‖ Health Services
Research, 36 (2): 399–403.
Meyers AF, AE Sampson, M Weitzman, BL Rogers, and H Kayne. 1989. ―School Breakfast
Program and School Performance.‖ American Journal of Diseases of Children, 143 (10):
1234–1239.
Miech, RA, A Caspi, TE Moffitt, BR Entner Wright, and PA Silva. 1999. ―Low Socioeconomic
Status and Mental Disorders: A Longitudinal Study of Selection and Causation during Young
Adulthood.‖ American Journal of Sociology, 104 (4): 1096–1131.

Milton, B, M Whitehead, P Holland, and V Hamilton. 2004. ―The Social and Economic
Consequences of Childhood Asthma across the Lifecourse: A Systematic Review.‖ Child
Care, Health and Development, 30 (6): 711–728.
Mokdad, Ali H, James S Marks, Donna F Stroup, Julie L Gerberding. 2004. ―Actual Causes of
Death in the United States, 2000.‖ Journal of the American Medical Association, 291 (10):
1238–1245.
Mullahy, J and JL Sindelar. 1993. ―Alcoholism, Work, and Income.‖ Journal of Labor
Economics, 11(3): 494–520.
Munafò, MR, TG Clark, EC Johnstone, MFG Murphy, and RT Walton. 2004. ―The Genetic Basis
for Smoking Behavior: A Systematic Review and Meta-analysis.‖ Nicotine & Tobacco
Research, 6 (4): 583–597.
National Institute of Environmental Health Sciences. 2000. ―Asthma and Allergy Prevention.‖
http://www.niehs.nih.gov/airborne/research/background.html.
Neidell, MJ. 2004. ―Air Pollution, Health, and Socio-Economic Status: The Effect of Outdoor Air
Quality on Childhood Asthma.‖ Journal of Health Economics, 23 (6): 1209–1236.
Newacheck, PW, and N. Halfon. 1992. ―Prevalence and Impact of Disabling Chronic Conditions
in Childhood.‖ American Journal of Public Health, 88 (4): 610–617.
Newacheck, PW, YY Hung, MJ Park, CD Brindis, and CE Irwin, Jr. 2003. ―Disparities in
Adolescent Health and Health Care: Does Socioeconomic Status Matter?‖ Health Services
Research, 38 (5): 1235–1252.
Oh, JH and EH Shin. 2003. ―Inequalities in Nonfatal Work Injury: The Significance of Race,
Human Capital, and Occupations.‖ Social Science and Medicine, 57 (11): 2173–2182.
Olson, Christine M. 1999. ―Nutrition and Health Outcomes Associated with Food Insecurity and
Hunger.‖ Journal of Nutrition, 129 (2): 521S–524S.
Oreopoulos, Philip, Mark Stabile, Leslie Roos, and Randy Walld. Forthcoming. ―The Short,
Medium, and Long Term Effects of Poor Infant Health.‖ Journal of Human Resources.
Palloni, Alberto. 2006. ―Reproducing Inequalities: Luck, Wallets, and the Enduring Effects of
Childhood Health.‖ Demography, 43 (4): 587–615.
Perri, TJ. 1984. ―Health Status and Schooling Decisions of Young Men.‖ Economics of
Education Review, 3 (3): 207–213.
Rasmussen, Kathleen Maher. 2001. ―The ‗Fetal Origins‘ Hypothesis: Challenges and
Opportunities for Maternal and Child Nutrition.‖ Annual Review of Nutrition, 21: 73–95.
Rauh, V, G Chew, and R Garfinkel. 2002. ―Deteriorated Housing Contributes to High Cockroach
Allergen Levels in Inner-city Households.‖ Environmental Health Perspectives, 110 (Suppl
2): 323–327.
Reville, Robert T and Robert F Schoeni. 2003/2004. ―The Fraction of Disability Caused at
Work.‖ Social Security Bulletin, 65 (4): 31–37.
Ritsher, J, EB Warner, JG Johnson, and BP Dohrenwend. 2001. ―Inter-generational Longitudinal
Study of Social Class and Depression: A Test of Social Causation and Social Selection
Models.‖ British Journal of Psychiatry, 178 (Suppl 40): s84–s90.
Rodgers, B and SL Mann. 1993. ―Re-thinking the Analysis of Intergenerational Social Mobility:
A Comment on John W. Fox‘s ‗Social Class, Mental Illness, and Social Mobility.‘‖ Journal
of Health and Social Behavior, 34 (2): 165–172.
Romelsjö, Anders, Marlene Stenbacka, Michael Lundberg, and Marianne Upmark. 2004. ―A
Population Study of the Association between Hospitalization for Alcoholism among
Employees in Different Socio-economic Classes and the Risk of Mobility out of, or within,
the Workforce.‖ The European Journal of Public Health, 14 (1): 53–57.
Rose, Donald. 1999. ―Economic Determinants and Dietary Consequences of Food Insecurity in
the United States.‖ Journal of Nutrition, 129 (2): 517S–520S.
Ross, CE, and J Mirowsky. 2000. ―Does Medical Insurance Contribute to Socioeconomic
Differentials in Health?‖ The Milbank Quarterly, 78 (2): 291–321.
Royer, Heather. Forthcoming. ―Separated at Girth: U.S. Twin Estimate of the Effects of
Birthweight.‖ American Economic Journal: Applied Economics.
Shone LP, AW Dick, JD Klein, J Zwanziger, and PG Szilagyi. 2005. ―Reduction in Racial and
Ethnic Disparities after Enrollment in the State Children‘s Health Insurance Program.‖
Pediatrics, 115 (6): e697–e705.
Smith, James. 1999. ―Healthy Bodies and Thick Wallets: The Dual Relation between Health and
Economic Status.‖ Journal of Economic Perspectives, 13 (2): 145–166.
Social Security Administration. 2006. ―Annual Statistical Report on the Social Security Disability
Insurance Program, 2005.‖ Washington, D.C.: Social Security Administration.
Stapleton, David C, Bonnie L. O‘Day, Gina A. Livermore, and Andrew J. Imparato. 2006.
―Dismantling the Poverty Trap: Disability Policy for the Twenty-First Century.‖ The Milbank
Quarterly, 84 (4): 701–732.
Stormer, A and GG Harrison. 2003. ―Does Household Food Security Affect Cognitive and Social
Development in Kindergartners?‖ Institute for Research on Poverty Discussion Paper no.
1276-03. Madison, WI: University of Wisconsin-Madison.
Strauss, Richard S. and Judith Knight. 1999. ―Influence of the Home Environment on the
Development of Obesity in Children.‖ Pediatrics, 103 (6): e85.
Substance Abuse and Mental Health Services Administration (SAMHSA). 2006. ―2005 National
Survey on Drug Use & Health.‖
http://www.oas.samhsa.gov/nsduh/2k5nsduh/2k5Results.htm.
Townsend, MS, J Peerson, B Love, C Achterberg, and SP Murphy. 2001. ―Food Insecurity is
Positively Related to Overweight in Women.‖ Journal of Nutrition, 131 (6): 1738–1745.
Turrell, G, B Hewitt, C Patterson, B Oldenburg, and T Gould. 2002. ―Socioeconomic Differences
in Food Purchasing Behavior and Suggested Implications for Diet-related Health Promotion.‖
Journal of Human Nutrition and Dietetics, 15 (5): 355–364.

Twenge, JM and S Nolen-Hoeksema. 2002. ―Age, Gender, Race, Socioeconomic Status, and
Birth Cohort Differences on the Children‘s Depression Inventory: A Meta-Analysis,‖ Journal
of Abnormal Psychology, 111 (4): 578–588.
U.S. Department of Health and Human Services. 2008. ―Childhood Obesity.‖
http://aspe.hhs.gov/health/reports/child_obesity.
Vink, JM, G Willemsen, and DI Boomsma. 2005. ―Heritability of Smoking Initiation and
Nicotine Dependence.‖ Behavior Genetics, 35 (4): 397–406.
Wadsworth, ME. 1986. ―Serious Illness in Childhood and Its Association with Later-Life
Achievement,‖ in R. Wilkinson, ed., Class and Health: Research and Longitudinal Data.
London: Tavistock Publications. pp. 50–74.
Wadsworth, MEJ and DJL Kuh. 1997. ―Childhood Influences on Adult Health: A Review of
Recent Work from the British 1846 National Birth Cohort Study, the RMC National Survey
of Health and Development.‖ Pediatric and Perinatal Epidemiology, 11 (1): 2–20.
Wilkinson, Richard G. 1994. ―The Epidemiological Transition: From Material Scarcity to Social
Disadvantage?‖ Deadalus, 123 (4): 61–77.
Wolfe, B. 1985. ―The Influence of Health on School Outcomes: A Multivariate Approach.‖
Medical Care, 23 (10): 1127–1138.

HEALTH and economic mobility
acknowledgements
The author thanks Bhashkar Mazumder, PhD., The Federal Reserve Bank of Chicago, for comments on
an earlier draft. Also Brendan Cushing-Daniels, PhD., Gettysburg College and the Urban Institute,
helped with revisions to this literature review. This literature review represents the views of the author
and not affiliated individuals or institutions.
All Economic Mobility Project materials are guided by input from the Principals’ Group
and the project’s Advisory Board. However, the views expressed in this report represent those
of the author and not necessarily of any affiliated individuals or institutions.
project principals
Marvin Kosters, Ph.D., American Enterprise Institute
Isabel Sawhill, Ph.D., Center on Children and Families, The Brookings Institution
Ron Haskins, Ph.D., Center on Children and Families, The Brookings Institution
Stuart Butler, Ph.D., Domestic and Economic Policy Studies, The Heritage Foundation
William Beach, Center for Data Analysis, The Heritage Foundation
Eugene Steuerle, Ph.D., Urban-Brookings Tax Policy Center, The Urban Institute
Sheila Zedlewski, Income and Benefits Policy Center, The Urban Institute
project advisors
David Ellwood, Ph.D., John F. Kennedy School of Government, Harvard University
Christopher Jencks, M. Ed., John F. Kennedy School of Government, Harvard University
Sara McLanahan, Ph.D., Princeton University
Bhashkar Mazumder, Ph.D., The Federal Reserve Bank of Chicago
Ronald Mincy, Ph.D., Columbia University School of Social Work
Timothy M. Smeeding, Ph.D., Maxwell School, Syracuse University
Gary Solon, Ph.D., Michigan State University
Eric Wanner, Ph.D., The Russell Sage Foundation
The Pew Charitable Trusts (www.pewtrusts.org) is driven by the power of knowledge to solve today‘s most
challenging problems. Pew applies a rigorous, analytical approach to improve public policy, inform the public and
stimulate civic life. We partner with a diverse range of donors, public and private organizations and concerned
citizens who share our commitment to fact-based solutions and goal-driven investments to improve society.