hemodynamic monitoring does one size fit all? - pulsion.com filefor example, applicable for heart...
TRANSCRIPT

Prof. JeanProf. Jean--Louis TEBOUL, Louis TEBOUL,
Medical ICUBicetre hospital
University Paris XIFrance
HemodynamicHemodynamic monitoring monitoring
Does one size fit all?Does one size fit all?
MemberMember ofof thethe MedicalMedical AdvisoryAdvisory BoardBoardofof Pulsion Pulsion MedicalMedical SystemsSystems
((GermanyGermany))
Conflicts of interestConflicts of interest
definition (s) of definition (s) of hemodynamichemodynamic monitoring? monitoring?
•• InitiallyInitially
monitoring monitoring warning systemwarning system ((““moneremonere””: : ““to warnto warn””))
For example, applicable for heart rateheart rate continuous monitoring
• Detection of sudden tachycardia, bradycardia or arrhythmias
•• Useful inUseful in stable patients stable patients butbut at risks of instability at risks of instability (operating room)(operating room)
•• The concept has evolved over timeThe concept has evolved over time considerable technologic development
availability of various invasiveinvasive and non invasivenon invasive hemodynamiccontinuouscontinuous or non continuousnon continuous monitoring systems
availability of numerous hemodynamic variables
• in relation to:
-- volume depletion or volume depletion or maldistributionmaldistribution
-- decreased vascular tonedecreased vascular tone
• often in association with acute lung injuryacute lung injury
• and that can result in peripheral peripheral hypoperfusionhypoperfusion and organ dysfunctionorgan dysfunction
22-- Because the patients areBecause the patients are hemodynamicallyhemodynamically unstableunstable
-- cardiac dysfunction or failurecardiac dysfunction or failure
Why to use Why to use hemodynamichemodynamic monitoring? monitoring?
11-- Because the patients areBecause the patients are at risks of at risks of hemodynamichemodynamic instabilityinstability
22-- Because the patients are Because the patients are hemodynamicallyhemodynamically unstableunstable
Why to use Why to use hemodynamichemodynamic monitoring? monitoring?
11-- Because the patients are at risks of Because the patients are at risks of hemodynamichemodynamic instabilityinstability
44-- Because weBecause we need:need:
-- toto identifyidentify cardiovascular disease patterns,cardiovascular disease patterns,
-- toto understandunderstand pathophysiogicalpathophysiogical processes,processes,
-- toto assessassess thethe degreedegree ofof eacheach hemodynamichemodynamic disorderdisorder
for for choosingchoosing thethe bestbest therapytherapy Fluids Fluids VasopressorsVasopressors InotropesInotropes
-- toto titrate titrate these therapiesthese therapies
33-- Because clinical assessment is insufficient Because clinical assessment is insufficient to adequately evaluate to adequately evaluate the the hemodynamichemodynamic statusstatus of ICU patientsof ICU patients

•• continuouscontinuous andand realreal--timetime display display ofof relevant relevant variablesvariables
•• or or repeatablerepeatable measurementsmeasurements atat frequentfrequent intervalsintervals
•• non invasivenon invasive
•• easyeasy to to learnlearn
•• easyeasy to useto use
•• non non operatoroperator--dependentdependent
•• nonnon expansiveexpansive
•• positive impact on positive impact on outcomeoutcome
thethe idealideal hemodynamichemodynamic monitoring monitoring tooltool…….. .. doesdoes notnot yetyet existexist
WhatWhatshould be?should be?
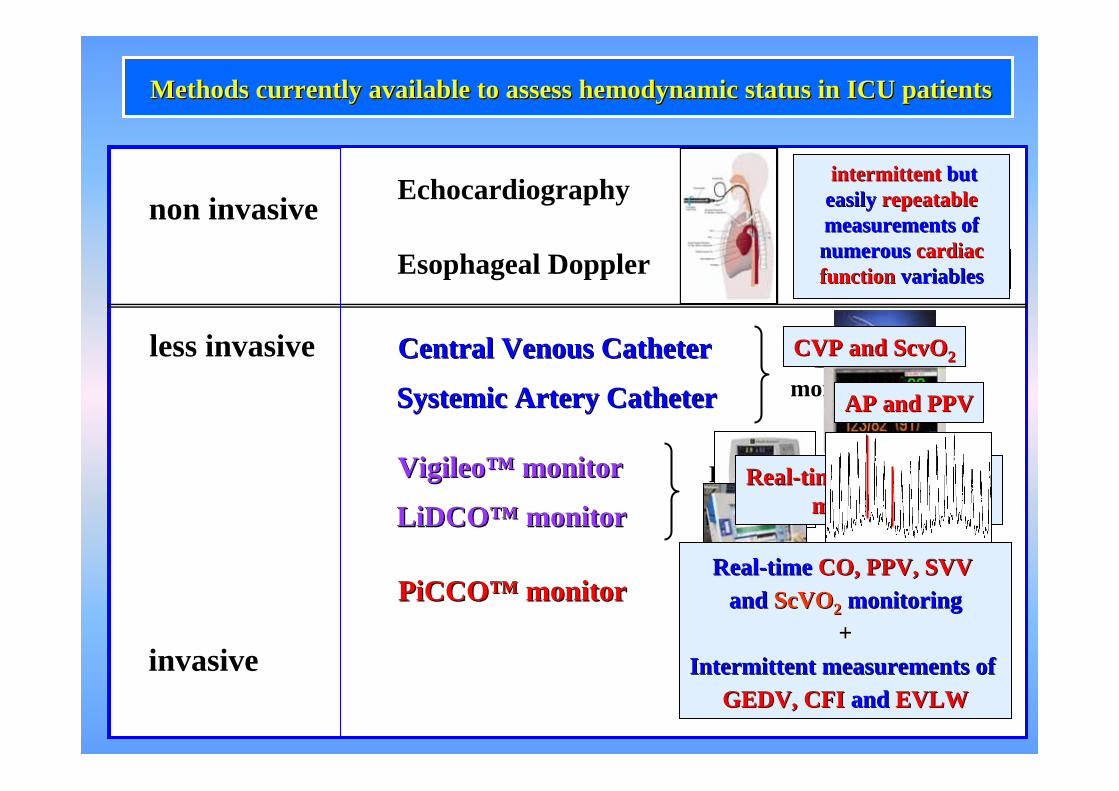
PiCCOPiCCO™™ monitormonitor
SystemicSystemic ArteryArtery CatheterCatheter
invasive
less invasive
Echocardiography
Esophageal Doppler
non invasive
MethodsMethods currentlycurrently availableavailable to to assessassess hemodynamichemodynamic statusstatus in ICU patients in ICU patients
VigileoVigileo™™ monitormonitor
Central Central VenousVenous CatheterCatheter
LiDCOLiDCO™™ monitormonitor
Basic Basic monitoringmonitoring
Intermediate Intermediate monitoringmonitoring
CVP and ScvOCVP and ScvO22
AP and PPVAP and PPV
RealReal--time CO and SVV time CO and SVV monitoringmonitoring
aortic blood flowaortic blood flow
intermittent intermittent but but easilyeasily repeatable repeatable measurements of measurements of numerousnumerous cardiac cardiac function function variablesvariables
RealReal--timetime CO, PPV, SVV CO, PPV, SVV and and ScVOScVO22 monitoringmonitoring
++IntermittentIntermittent measurements ofmeasurements of
GEDV, CFI GEDV, CFI and and EVLWEVLW

GEDV :GEDV :
measuremeasure of of cardiaccardiac preloadpreload

-2
2
6
10
14
Changes in COChanges in GEDV
% **
fluidfluid loadingloading dobutaminedobutamine
**
**
GEDV behaves as a marker of preload
Chest 2003; 124:1900-1908

CFI:CFI:
Index ofIndex of
cardiaccardiac systolicsystolic functionfunction

44
CFICFI
prediction of LV FAC < 40 %prediction of LV FAC < 40 %

0
20
40
60
80
100
0 20 40 60 80 100100 - specificity
Sens
itivi
ty3.5 min-1
CFI for detectingLVEF ≤ 35%
Cardiac function index provided by transpulmonary thermodilutionbehaves as an indicator of left ventricular contractility.Jabot J, Monnet X, Lamia B, Chemla D, Richard C, Teboul JL
Crit Care Med 2009 (in press)

-40
-20
20
40
60
80
100
120
-40 -20 20 40 60 80 100 120
% c
hang
e in
LV
EF
% change in CFI
Changes induced by- fluid infusion- dobutamine
r = 0.79r = 0.79
Cardiac function index provided by transpulmonary thermodilutionbehaves as an indicator of left ventricular contractility.Jabot J, Monnet X, Lamia B, Chemla D, Richard C, Teboul JL
Crit Care Med 2009 (in press)

-15
-5
5
15
25
35
45
55
Volume expansionVolume expansion DobutamineDobutamine
*
% changes in CFI
CFI CFI behavesbehaves as a marker of as a marker of systolicsystolic functionfunction
Cardiac function index provided by transpulmonary thermodilutionbehaves as an indicator of left ventricular contractility.Jabot J, Monnet X, Lamia B, Chemla D, Richard C, Teboul JL
Crit Care Med 2009 (in press)
EVLW:EVLW:
Index ofIndex of
pulmonarypulmonary edemaedema
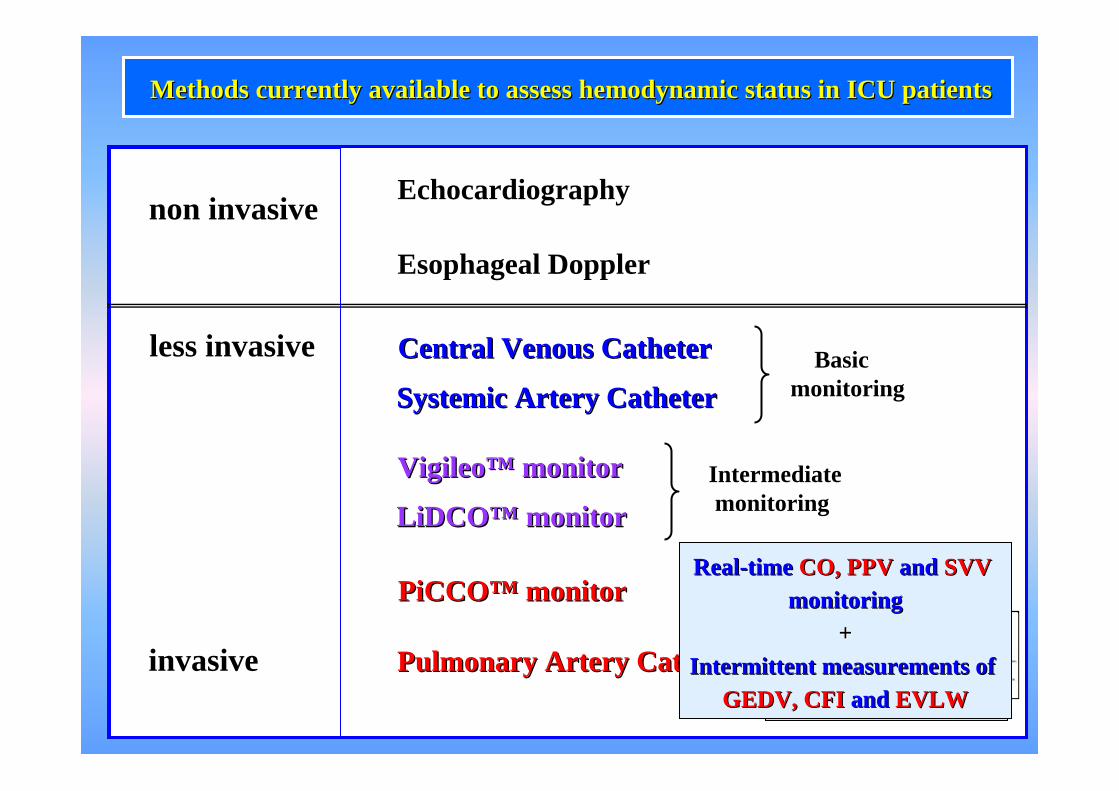
PulmonaryPulmonary ArteryArtery CatheterCatheter
PiCCOPiCCO™™ monitormonitor
SystemicSystemic ArteryArtery CatheterCatheter
invasive
less invasive
Echocardiography
Esophageal Doppler
non invasive
MethodsMethods currentlycurrently availableavailable to to assessassess hemodynamichemodynamic statusstatus in ICU patients in ICU patients
VigileoVigileo™™ monitormonitor
Central Central VenousVenous CatheterCatheter
LiDCOLiDCO™™ monitormonitor
Basic Basic monitoringmonitoring
Intermediate Intermediate monitoringmonitoring
Advanced Advanced monitoringmonitoring
Continuous Continuous CO and SvOCO and SvO22
monitoringmonitoring+
IntermittentIntermittent measurements measurements PAOP, RAP and PAPPAOP, RAP and PAP
RealReal--timetime CO, PPV CO, PPV andand SVV SVV monitoringmonitoring
++IntermittentIntermittent measurements ofmeasurements of
GEDV, CFI GEDV, CFI and and EVLWEVLW

Continuous Continuous oror intermittent intermittent hemodynamichemodynamic assessment? assessment?
It depends on the clinical situationclinical situationand on the questionquestion you are asking
• for managing high risk patientshigh risk patients in the OROR, continuouscontinuous monitoring of CO CO is probably important.
In most OR patients, a sudden fall in CO witnesses a sudden volume depletion.
Coupling continuous monitoring of COmonitoring of CO and of pulse pressure variationpulse pressure variation (PPV) or of stroke volume variationstroke volume variation (SVV) is helpful since the meaning of such indicesis straightforward in this setting.
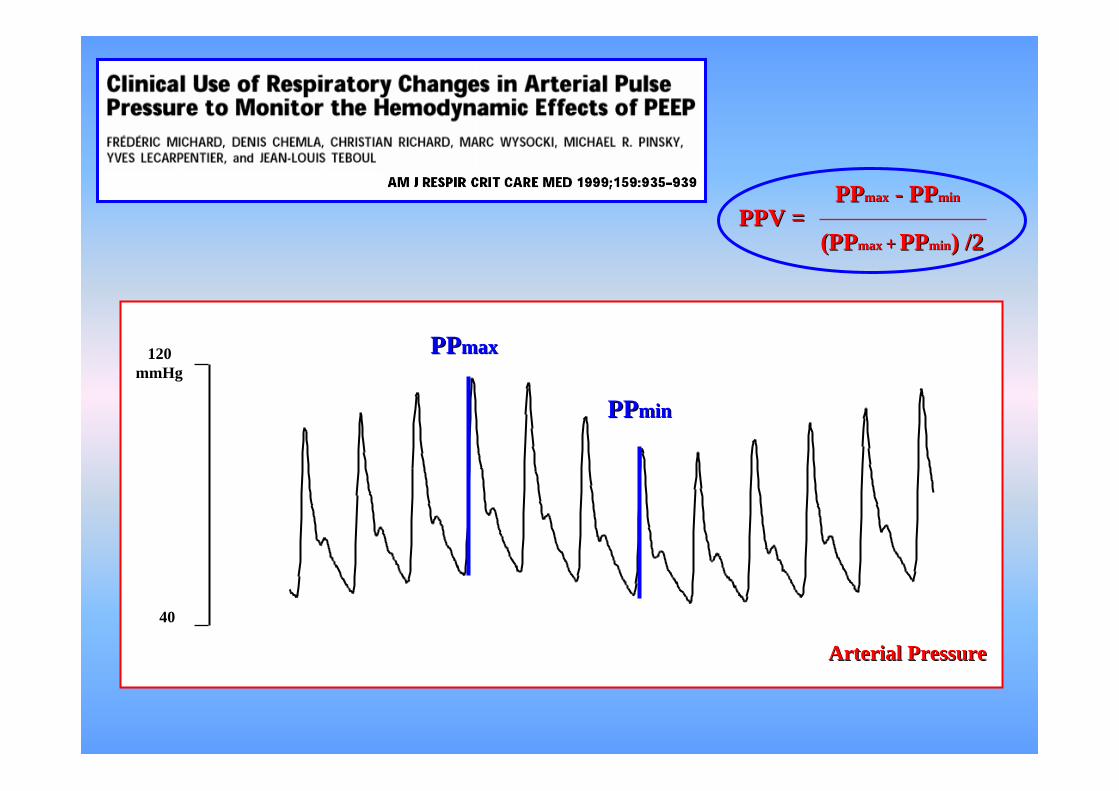
120 mmHg
40
ArterialArterial PressurePressure
PPPPmaxmax
PPPPminmin
PPPPmaxmax -- PPPPminmin
((PPPPmaxmax ++ PPPPminmin) /2) /2PPV =PPV =

A B Ventricular preload
Stroke volume
Sens
itivi
tySe
nsiti
vity
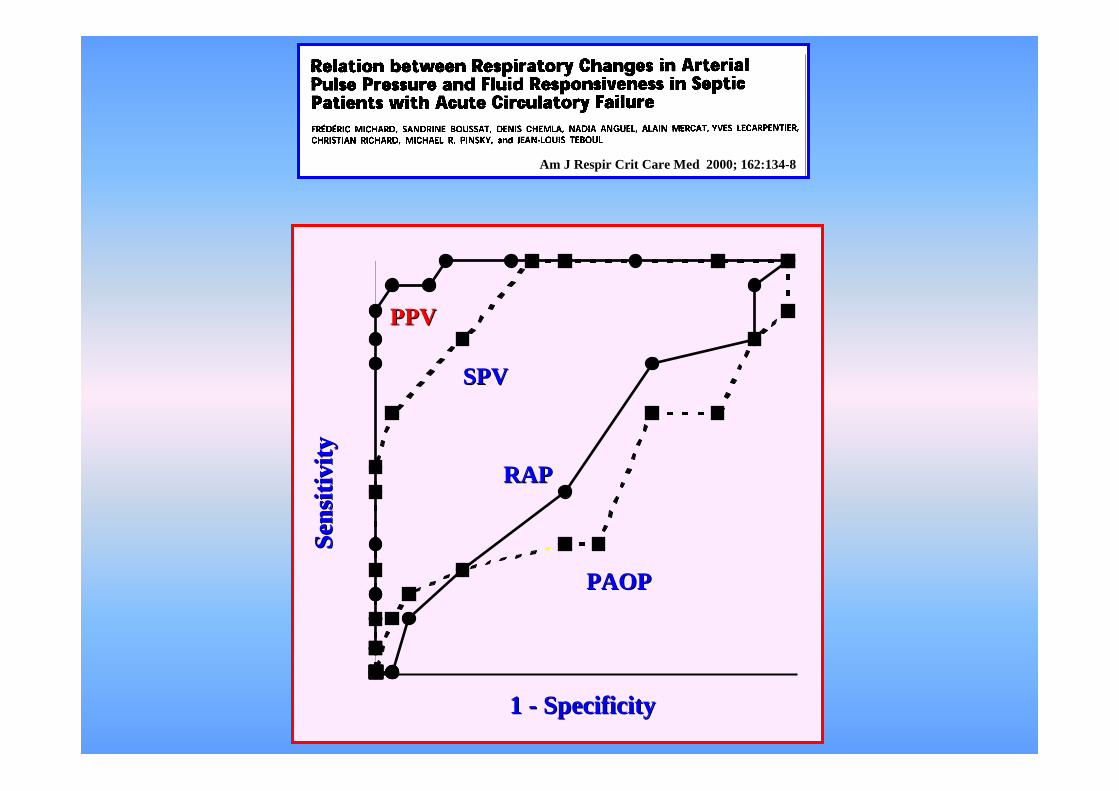
PPVPPV
SPVSPV
RAPRAP
PAOPPAOP
1 1 -- SpecificitySpecificity
Am J Am J RespirRespir CritCrit Care Med 2000; 162:134Care Med 2000; 162:134--88

Chest 2004, 126:1563-1568
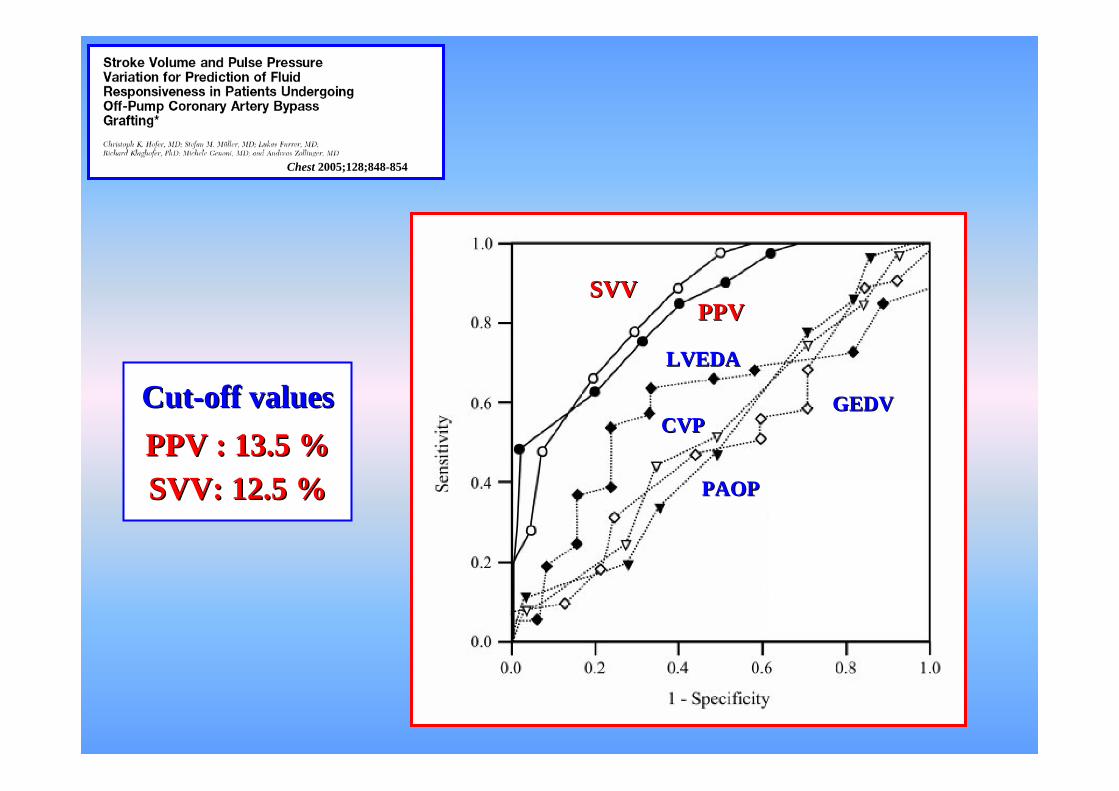
Chest 2005;128;848-854
Crit Care Med 2005;33:2534-9
PPVPPV
M. Cannesson, J. Slieker, O. Desebbe, F. Fahdi,O. Bastien, JJ. Lehot

StrokeStroke Volume Variation Volume Variation
SV maxSV max
SV minSV min
SV SV meanmean
SV max + SV minSV max + SV min
22SVV =SVV =

0 0.5 10 0.5 1
11-- specificityspecificity
sens
itivi
tyse
nsiti
vity
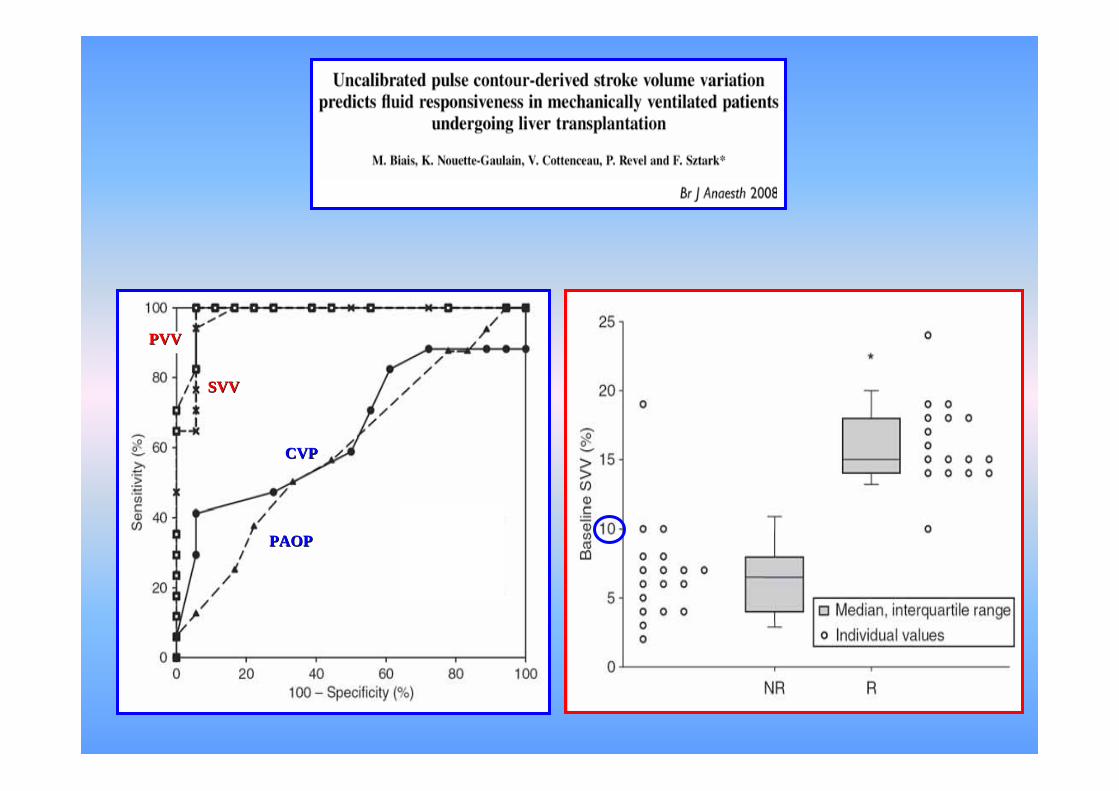
SVVSVV
CVPCVP
00
0.60.6
0.40.4
11
0.80.8
0.20.2
10 %10 % sensitivitysensitivity = 79 %= 79 %
specificityspecificity = 93 %= 93 %

SVV
SV
V b
asel
ine
base
line (
%)
(%)
CardiacCardiac Output changes Output changes afterafter fluidfluid infusion infusion (%)(%)
r = 0.74r = 0.74
Chest 2005;128;848-854
CutCut--offoff valuesvaluesPPVPPV : 13.5 %: 13.5 %SVV: 12.5 %SVV: 12.5 %
SVVSVVPPVPPV
CVPCVP
PAOPPAOP
GEDVGEDV
LVEDALVEDA
SVVSVV
PVVPVV
PAOPPAOP
CVPCVP
Continuous Continuous oror intermittent intermittent hemodynamichemodynamic assessment? assessment?
It depends on the clinical situationclinical situationand on the questionquestion you are asking
• for managing severe septic ptssevere septic pts in the ERER, SvOSvO22 monitoringmonitoring is probably important(in addition to conventional hemodynamic parameters) (see Rivers’ study)
SvOSvO22 > 70%> 70% considered as a targettarget for hemodynamic therapy
At this early stage, a more sophisticated monitoring device is rarely mandatory
• for managing high risk patients in the OR, continuous monitoring of CO/PPV is probably important.

Continuous Continuous oror intermittent intermittent hemodynamichemodynamic assessment? assessment?
It depends on the clinical situationclinical situationand on the questionquestion you are asking
• for managing severe septic pts in the ER, SvO2 monitoring is probably important
• for managing complex septic shock patients in the ICU, SvOSvO22 monitoringmonitoring alone is probably insufficient (see Gatinnoni’s study)but repeatablerepeatable (even intermittent) measurements of pertinentpertinent hemodynamicvariables are important
- to diagnosediagnose the cardiovascular disorders - to perform testsperform tests aimed at unmasking CV characteristics-- to choose and titratechoose and titrate therapies
ex: passive leg raisingpassive leg raising for detecting preload responsiveness
• for managing high risk patients in the OR, continuous monitoring of CO/PPV is probably important.

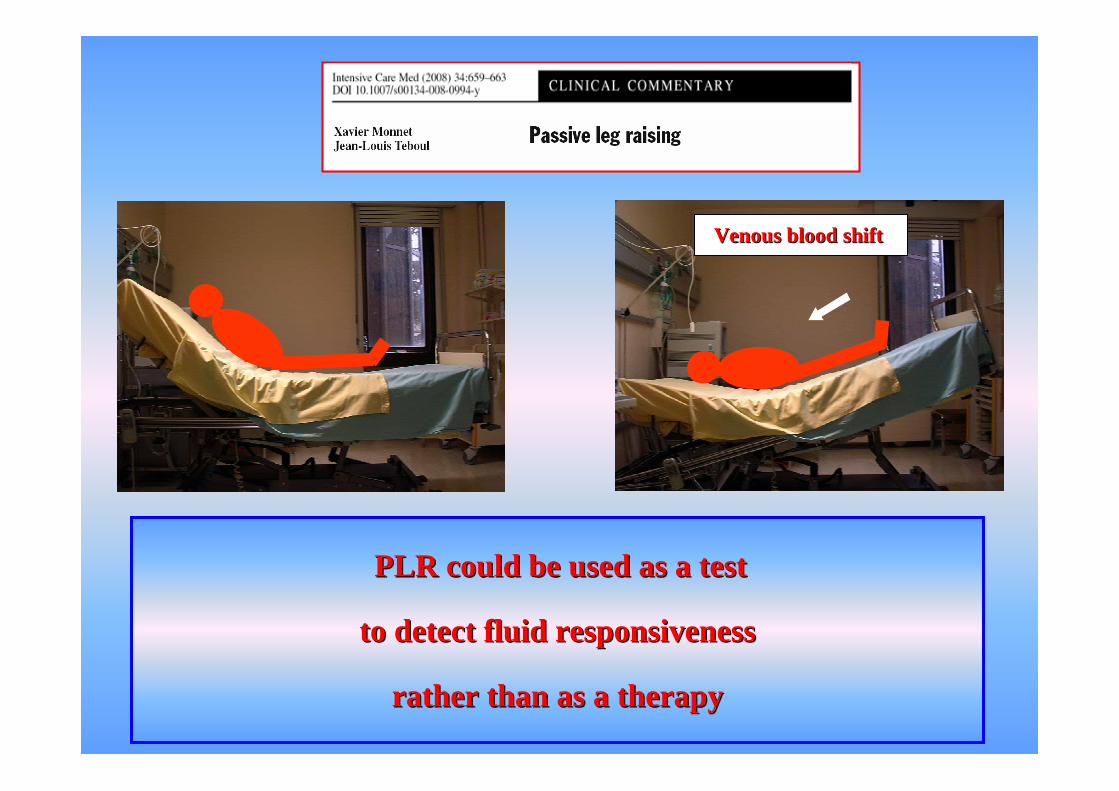
VenousVenous bloodblood shiftshift
IncreaseIncrease in in leftleft ventricularventricular preloadpreload (Rocha 1987, De Hert 1999)
IncreaseIncrease in right in right ventricularventricular preloadpreload (Thomas 1965) ReversibleReversible andandtransienttransient effectseffects
PLR PLR couldcould bebe usedused as a test as a test
to to detectdetect fluidfluid responsivenessresponsiveness
ratherrather thanthan as a as a therapytherapy

«« ContinuousContinuous »» thermodilutionthermodilution COCO monitoringmonitoring cannotcannot bebe usedused
for a PLR test because for a PLR test because thethe timetime--responseresponse isis tootoo longlong
The hemodynamic response to PLR can predict the hemodynamic response to volume infusion
RealReal--timetime CO monitoringCO monitoring isis mandatorymandatory

RealReal--timetime responseresponse ofofaorticaortic bloodblood flowflow
RealReal--timetime responseresponse ofofPulse contour COPulse contour CO RealReal--timetime responseresponse ofof
VTIVTI
The hemodynamic response to PLR can predict the hemodynamic response to volume infusion
RealReal--timetime CO monitoringCO monitoring isis mandatorymandatory

0
20
40
60
80
100
0 20 40 60 80 100
100 - specific ity
sens
itivity
Effects of passive leg rais ing on pulse pressure
A UC 0.675 [0.497-0.829]
0
20
40
60
80
100
0 20 40 60 80 100
100 - specific ity
sens
itivity
Effects of passive leg rais ing on pulse pressure
0
20
40
60
80
100
0 20 40 60 80 100
100 - specific ity
sens
itivity
Effects of passive leg rais ing on pulse pressure
A UC 0.675 [0.497-0.829]AUC: 0.675AUC: 0.675 [0.497-0.829]
PredictionPrediction of volume of volume responsivenessresponsivenessby the by the responseresponse of of Pulse PressurePulse Pressure
to PLRto PLR
100 - specificity
Effects of passive leg raising Effects of passive leg raising on Pulse contour COon Pulse contour CO
RR-10
0
10
20
30
40
50
60
70
80
90
NR
%
-10
0
10
20
30
40
50
60
70
80
90
-10
0
10
20
30
40
50
60
70
80
90
NR
%
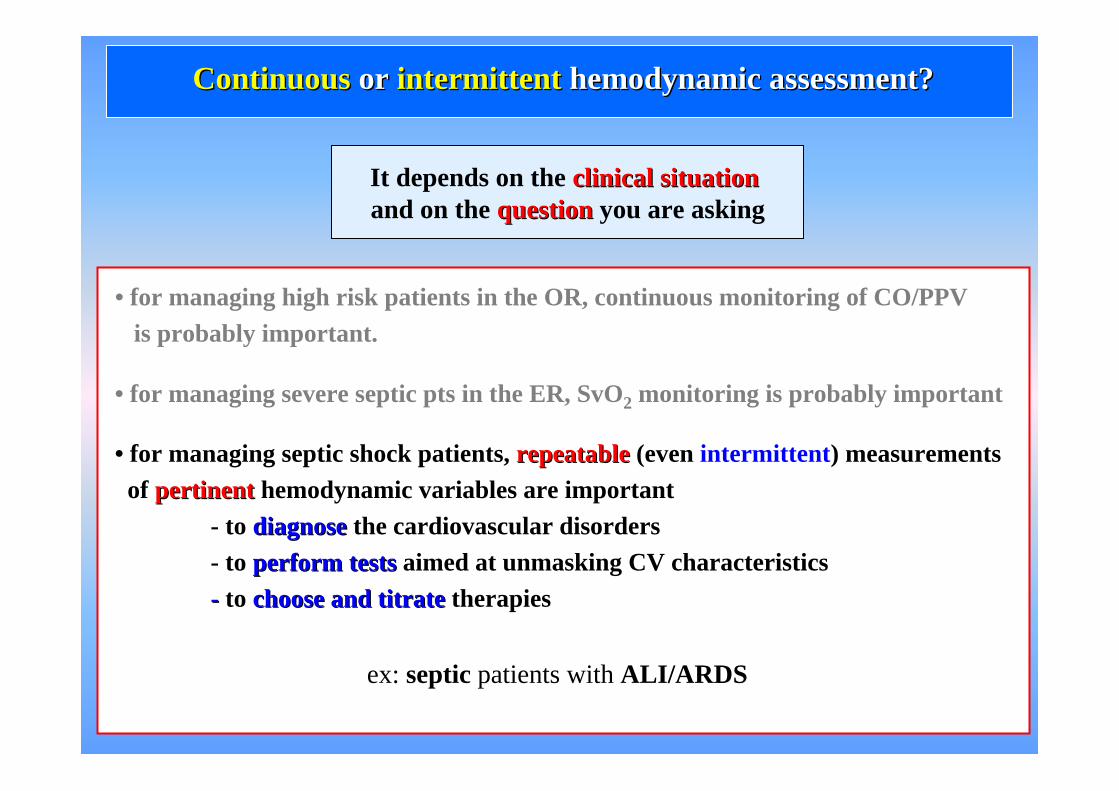
Continuous Continuous oror intermittent intermittent hemodynamichemodynamic assessment? assessment?
It depends on the clinical situationclinical situationand on the questionquestion you are asking
• for managing severe septic pts in the ER, SvO2 monitoring is probably important
• for managing septic shock patients, repeatablerepeatable (even intermittent) measurements of pertinentpertinent hemodynamic variables are important
- to diagnosediagnose the cardiovascular disorders - to perform testsperform tests aimed at unmasking CV characteristics-- to choose and titratechoose and titrate therapies
• for managing high risk patients in the OR, continuous monitoring of CO/PPV is probably important.
ex: septic patients with ALI/ARDS
Therapeutic conflictTherapeutic conflict
On the one hand, septic patients are likely to be hypovolemic….. and thus should need fluid.
On the other hand, in ALI/ARDS patients, who suffer from high permeability pulmonary edema, a “dry” therapeutic attitude is recommended.
septic patients with ALI/ARDS



Benefit/risk ratio ?Benefit/risk ratio ?
Predictors of fluid responsiveness (PPV, SVV, passive leg raising)are needed.
Quantitative indicators of pulmonary edema and of increased lung permeability are needed.

Central venous catheter
Thermodilution
femoral artery
catheter
EVLW a quantitative marker of lung edema
PVPI (EVLW/ PBV) a quantitative marker of pulmonary vascular permeability
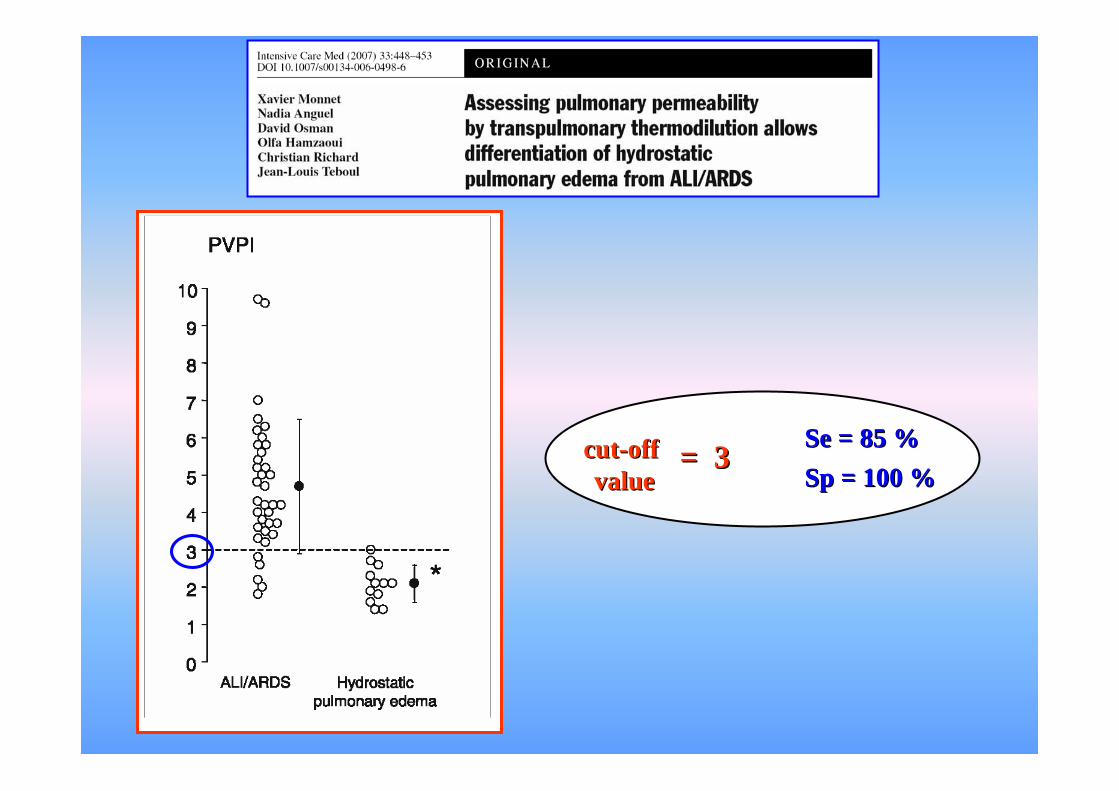
Se = 85 %Se = 85 %SpSp = 100 %= 100 %
cutcut--offoffvaluevalue
= 3= 3

SVV/SVV/PPVPPVPVPIPVPICOCOEVLWEVLW
To give fluidTo give fluid
decisiondecision To continue fluidTo continue fluid
To stop fluidTo stop fluid
SVV and PPVSVV and PPV for predicting volume responsiveness
PVPI PVPI for anticipating the degree of lung fluid filtration
EVLWEVLW for judging lung tolerance to fluid infusion
CO CO for evaluating the actual response to fluid once infused
Usefulness of the Usefulness of the PiCCOPiCCO devicedevice
for guiding fluid resuscitation/restriction for guiding fluid resuscitation/restriction especially in patients with ALI/ARDS and circulatory shockALI/ARDS and circulatory shock

HRHR: 125125 beats/min
BPBP: 80 / 3580 / 35 mmHg
PPVPPV: 2323 %
A 30 yrs old patient admitted for self-poisoning who developed severe ARDS at D2and presented an acute episode of septic shock (nosocomial infection) at D7.The patient received rapidly 2 L of saline2 L of saline, norepinephrinenorepinephrine (NE) at increasing doses and hemisuccinatehemisuccinate of hydrocortisoneof hydrocortisone.
Urine flow remained low. P/FP/F was 1191193 µg/kg/min NE
An arterial line was set up

HRHR: 125125 beats/min
BPBP: 80 / 3580 / 35 mmHg
PPVPPV: 2323 %
A 30 yrs old patient admitted for self-poisoning who developed severe ARDS at D2and presented an acute episode of septic shock (nosocomial infection) at D7.The patient received rapidly 2 L of saline2 L of saline, norepinephrinenorepinephrine (NE) at increasing doses and hemisuccinatehemisuccinate of hydrocortisoneof hydrocortisone.
Urine flow remained low. P/FP/F was 1191193 µg/kg/min NE
An arterial line was set up Which Which hemodynamichemodynamic therapy therapy do you propose?do you propose?
A- Nothing else
B- Infuse again fluid first and then reevaluate
C- Increase vascular tone first and then reevaluate
D- Give dobutamine first and then reevaluate
E- More information is needed before taking a decision
Because of hypoxemic increased permeability lung edema,
infusing more fluid can killkill the patient
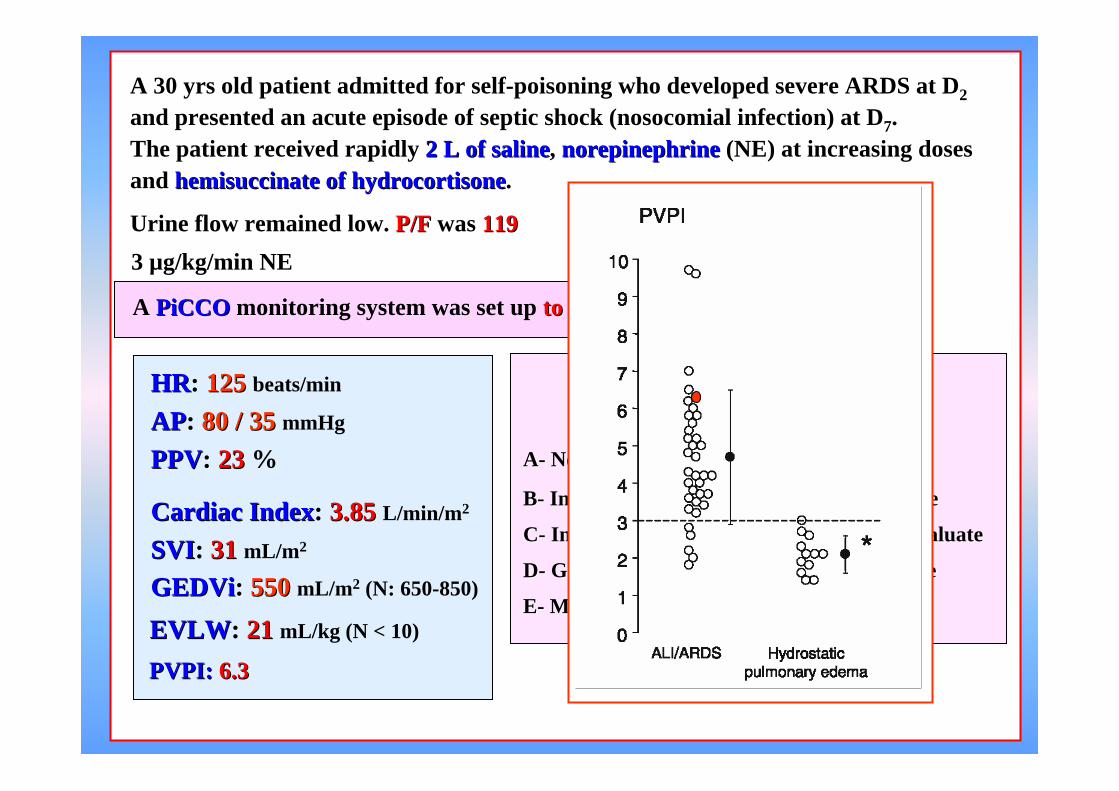
A 30 yrs old patient admitted for self-poisoning who developed severe ARDS at D2and presented an acute episode of septic shock (nosocomial infection) at D7.The patient received rapidly 2 L of saline2 L of saline, norepinephrinenorepinephrine (NE) at increasing doses and hemisuccinatehemisuccinate of hydrocortisoneof hydrocortisone.
Urine flow remained low. P/FP/F was 1191193 µg/kg/min NE
A PiCCOPiCCO monitoring system was set up to to knowknow EVLW EVLW andand PVPIPVPI
HRHR: 125125 beats/min
APAP: 80 / 3580 / 35 mmHg
PPVPPV:: 2323 %
CardiacCardiac IndexIndex: 3.853.85 L/min/m2
SVISVI: 3131 mL/m2
GEDViGEDVi:: 550550 mL/m2 (N: 650-850)
EVLWEVLW: 2121 mL/kg (N < 10)
PVPI:PVPI: 6.36.3
Which Which hemodynamichemodynamic therapy therapy do you propose?do you propose?
AA-- NothingNothing elseelse
BB-- Infuse Infuse againagain fluidfluid first first andand thenthen reevaluatereevaluate
CC-- IncreaseIncrease vascularvascular tonetone first and first and thenthen reevaluatereevaluate
DD-- GiveGive dobutaminedobutamine first and first and thenthen reevaluatereevaluate
EE-- More information More information isis neededneeded

Conclusion Conclusion
• for managing severe septicsevere septic pts in the ERER, SvOSvO22 monitoringmonitoring is probably important
• for managing septic shockseptic shock patients in the ICU, repeatablerepeatable measurements of pertinentpertinent hemodynamic variables are more important.
In the frequent case of combination of shockshock and lung injurylung injury, advanced monitoring device (like PICCO) can be helpful (PPV/SVV, CO, PVPI, EVLW)(PPV/SVV, CO, PVPI, EVLW).
--
• for managing high riskhigh risk patients in the OROR, continuouscontinuous monitoring of CO CO and PPVPPV (SVV) is probably important.
Hemodynamic monitoring: one size does not fit all
ThankThank youyou for for youryour attentionattention