il monitoraggio emodinamico invasivo in anestesia · il monitoraggio emodinamico invasivo in...
TRANSCRIPT

IL MONITORAGGIO EMODINAMICO INVASIVO IN ANESTESIA
A.O.R.N. SAN SEBASTIANOCASERTA
Luigi Belloni
Corso in Anestesiologia:SCUOLA DI DOTTORATO
“SCIENZE BIOMEDICHE VETERINARIE,SANITA’ ANIMALE E SICUREZZA ALIMENTARE
“Federico II”

L. Belloni, NAPOLI 16/03/05
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
Who benefits from invasive hemodynamic monitoring?
M.R.Pinsky ANESTH ANALG 2003 ;96:1245-7
Hemodynamicallyunstable patients
Incorrect treatment or delay in appropriate treatment results in markedly increased
morbidity and mortality.
Evaluation of cardiopulmonary status
and the subsequentphysiologic response.
Whymonitoring
Appropiatetreatment

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
HIGH RISK SURGERYMortality: 30%
Who benefits from invasive hemodynamic monitoring?
CARDIAC SURGERY
CABG IN HIGH RISK PATIENTS
CABG IN OFF PUMP SURGERY

HIGH RISK SURGERY
L. Belloni, NAPOLI 16/03/05
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
STRATIFICAZIONE PRE-OPERATORIA DEL RISCHIO
OPERATORIO
Categorie di rischio Categorie di rischio cardiovascolare cardiovascolare
(ACC/AHA)(ACC/AHA)
Stratificazione delrischio in rapportoal tipo di procedura
chirurgica
Stratificazione delStratificazione delrischio in rapportorischio in rapportoal tipo di procedura al tipo di procedura
chirurgicachirurgica
Condizioni cliniche preoperatoria

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Categorie di rischio cardiovascolare
Categorie di rischio Categorie di rischio cardiovascolarecardiovascolare
Fattori di rischio maggioriFattori di rischio maggioriAngina instabile.IMA (<30 gg)Insuff.cardiaca scompensataBAV avanzato, aritmie ventricolari
sintomatiche, aritmie sopraventricolari ipercinetiche
Approfondimento cardiologico

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Stratificazione delrischio in rapporto
al tipo di procedura chirurgica
Stratificazione delStratificazione delrischio in rapportorischio in rapporto
al tipo di procedura chirurgicaal tipo di procedura chirurgica
Rischio maggioreRischio maggiore Rischio minore
Rischio intermedio

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Rischio maggiore
Urgenze, specie nell’anzianoChir. Aortica e vascolare arteriosa perifericaProcedure chirurgiche prolungate e/o associate a importanti variazioni volemiche
Urgenze, specie nell’anzianoChir. Aortica e vascolare arteriosa perifericaProcedure chirurgiche prolungate e/o associate a importanti variazioni volemiche

ESISTONO DEI LIVELLI DI RACCOMANDAZIONE PER
L’IMPIANTO DI UN MONITORAGGIO EMODINAMICO?
L. Belloni, NAPOLI 16/03/05
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L’American College of Cardiology in risposta alle numerose richieste di chiarimento in merito ha prodotto recentemente un documento validato da una ConsensusConference di esperti e pubblicato nel settembre 1998.
Limitatamente all’indicazione nella chirurgia non cardiaca l’uso del catetere di Swan-Ganz ha un ruolo
riconosciuto nella guida al trattamento di pazienti selezionati con insufficienza cardiaca scompensata che devono essere sottoposti a chirurgia non cardiaca con
rischio medio od alto, mentre le opinioni divergono notevolmente se l’insufficienza è compensata.
GRADO DI RACCOMANDAZIONE ?

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Hemodynamic patterns of survivors and nonsurvivors during high risk elective surgical operations.Shoemaker WC, Wo CC, Thangathurai D, Velmahos G,Belzberg H, Asensio JA, Demetriades D.
World J Surg. 1999 Dec
Outcome was improved whenpotentially lethal circulatorypatterns were treated during the early (the first 8-12 hours)postoperative period but after the appearence of organfailure,reversal of non survivalpatterns ,did not improve the outcome.
But clinical evidence ……
Early postoperativemonitoring revealeddifferences in survivor and non survivors patterns and provided goals for improvingoutcomeIntraoperative evaluation of tissue perfusion in high-risk patients by invasive and noninvasive hemodynamicmonitoring Shoemaker WC, Thangathurai D, Wo CC, KuchtaK, Canas M, Sullivan MJ, Farlo J, Roffey P, Zellman V, Katz RL
Crit Care Med. 1999 Oct
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
The three most prognostic variables were:
Cardiac index > 4.5 l/min/m2,
Oxygen delivery > 600 ml/ min/m2
Oxygen consumption > 170 ml/min/m2 -’dysoxia’ First noted by Shoemaker et al - 30 years ago
• Through evaluation of 30 physiological variables in thousands of patients.
• Only those variables related to blood volume and flow had a significant
prognostic value in terms of morbidity and mortality.
• Most commonly measured variables of: blood pressure, heart rate,
temperature, CVP and urine output were poorly prognostic of outcome.
Clinical Experience in high risk surgery patients
Which prognostic variables??

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Clinical Experience
in high risk surgery patientsStudy n Timing Monitor Goals Intervention
Bender 1997 104 Pre PAC
PAC
PAC
PAC
ODM
PAC
PAC
ODM
PAC
PAC
PAC
PAC
CI Fluids + vasoactives
Berlauk 1991 89 Pre, Intra CI Fluids + vasoactives
Boyd 1993 107 Pre, Intra, Post DO2 Fluids + vasoactives
Lobo 2000 37 Pre DO2 Fluids + vasoactives
Mythen 1995 60 Intra SV Fluids
Polonen 2000 393 Post SvO2/Lactate Fluids + vasoactives
Shoemaker 1988 58 Pre CO/DO2/VO2 Fluids + vasoactives
Sinclair 1997 40 Intra SV Fluids + vasoactives
Ueno 1998 34 Post CI/DO2/VO2 Fluids
Valentine 1998 120 Pre CI Fluids + vasoactives
Wilson 1999 138 Pre DO2 Fluids + vasoactives
Ziegler 1997 72 Pre SvO2 Fluids + vasoactives

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
11 22 33 44 55 66
CCardiac ardiac IIndex (First 4 P.O. ndex (First 4 P.O. HrsHrs))
1.01.0
0.20.2
0.40.4
0.80.8
0.60.6Pr
obab
ility
Prob
abili
tyof
Car
diac
of
Car
diac
Dea
thD
eath
p = 0.0002p = 0.0002
11 22 33 44 55 66
CCardiac ardiac IIndex (First 4 P.O. I)ndex (First 4 P.O. I)
00
1.01.0
0.20.2
0.40.4
0.80.8
0.60.6
p = 0.0001p = 0.0001
JW Kirklin UAB, 1975JW Kirklin UAB, 1975--1979 1979

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
O2O2ERER%%
SvO2SvO2%%
RelationshipRelationship betweenbetween intra and intra and postoperativepostoperative
oxygenoxygen transporttransport and and prolongedprolongedintensive care after cardiac surgery: intensive care after cardiac surgery:
a a prospectiveprospective studystudy
Pölönen P. et al.A.A. Scandinavica 1997: 810-817
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
1971
Realizzato il primo microprocessore
Ottenuto il DNA ricombinante
“A new technique for measurement of
cardiac output by thermodilution in men”
HJC Swan - W Ganz
Am J. Cardiol 1971
Which parameters are detectable?
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
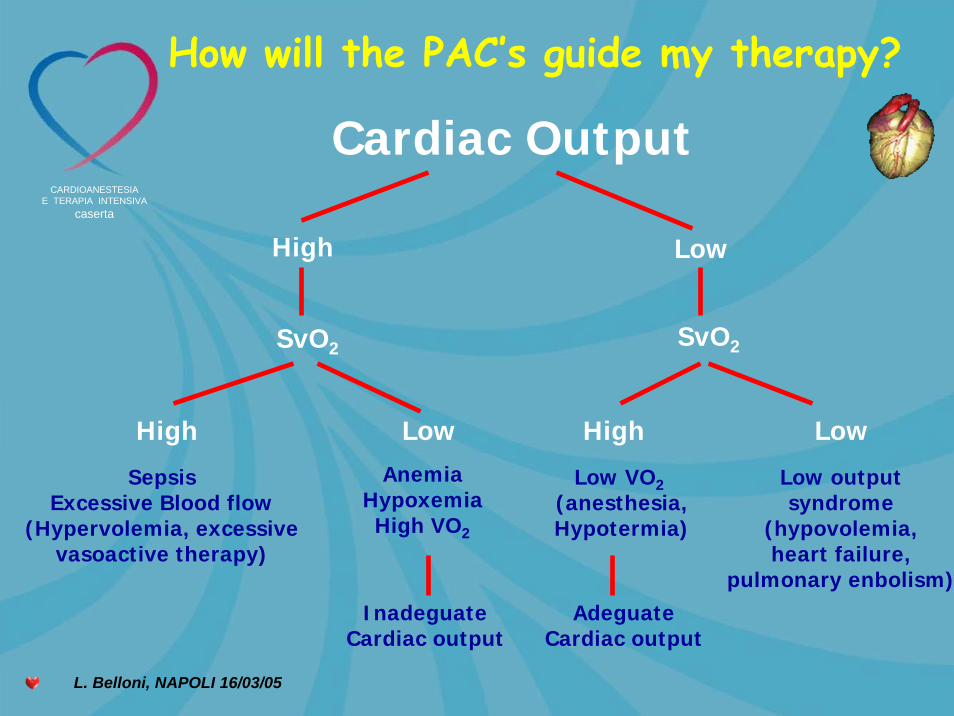
How will the PAC’s guide my therapy?
Low
SvO2
Low
Cardiac Output
High
SvO2
High LowHigh
SepsisExcessive Blood flow
(Hypervolemia, excessivevasoactive therapy)
AnemiaHypoxemiaHigh VO2
InadeguateCardiac output
Low VO2 (anesthesia,Hypotermia)
AdeguateCardiac output
Low outputsyndrome
(hypovolemia,heart failure,
pulmonary enbolism)

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Cateterismo di Swan-Ganz: Rilevamento pressorio
PVC: 0-8 mmHgPr.Sist.:15-25 mmHgPr.Diast.: 0-8 mmHg
Pr.Sist.: 15-25mmHgPr.Diast.: 6-12 mmHg 4-12 mmHg

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Implicazione clinica del valore di PAOP
(pressione wedge)PAOP< 8mmHg
Tra 8-12 mmHg
Tra 12-18 mmHg
18 mmHg
IPOVOLEMIA POTENZIALE
NORMALITA’
AREA GRIGIA (potenzialmente può significare un incremento di contrattilità se seguente a riempimento volemico).
SVILUPPO DI DISFUNZIONE ED INSUFFICIENZA VENTRICOLARE SX.

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Filling pressure are staticparameters and are not a gold standards for ………
CautionCaution!!!!!!!!!!!!
PRELOAD ASSESSMENT!!!
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
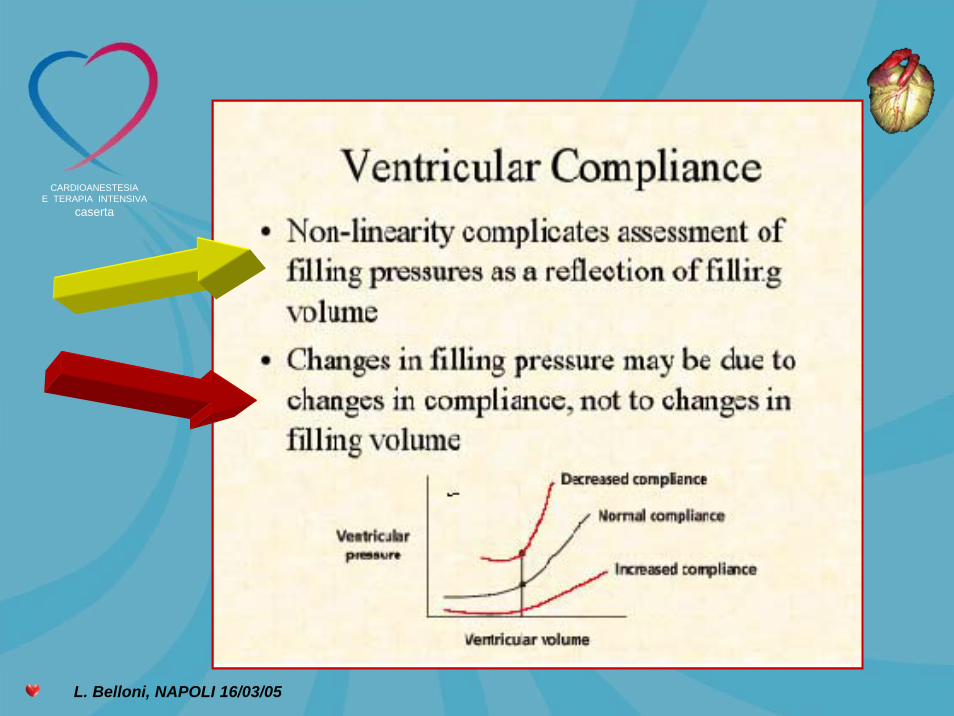
Changes in ventricularcompliance
Decreased compliance (Compliance curve to the left)
IschemiaRestrictive cardiomyopathiesIncreased intratoracic pressure (PPV and PEEP)Increased pericardial pressure (cardiac tamponade)Increased abdominal pressure
In a non compliant ventricle, a greater pressure isgenerated with very little increase in volume.

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
La PVC la PAOP sono buon indicatori di Stato
Volemico,Pre-load nel paziente in anestesia
CVP-PAOP
VOLEMIA
TONO VENOSO
PRESSIONE
ADDOMINALE
PRESSIONE INTRATORACICA
COMPLIANCE VENTRICOLARE……….NO !!!!

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Dynamic CVP changes rather thanstatic or mean CVP values might be
most accurate.
The rise in Cardiac Output after volume challenge is muchbetter in critically ill patients who experience a greater than1 mm Hg change in CVP during a single breath than in those
with a less than 1 mmHg fluctuation.Magder S,J Crit Care,7:76-85,1992
Pressure DerivedData (PAC)
Volume DerivedData (Volumetric
Technology: PiCCO andLiDCO)
Vs
EchoCVP PAOP
PAD

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Echocardiography provides a measurementof true cardiac preload : LVEDA and LVEDV
Echo is a tool forhemodynamic monitoring
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
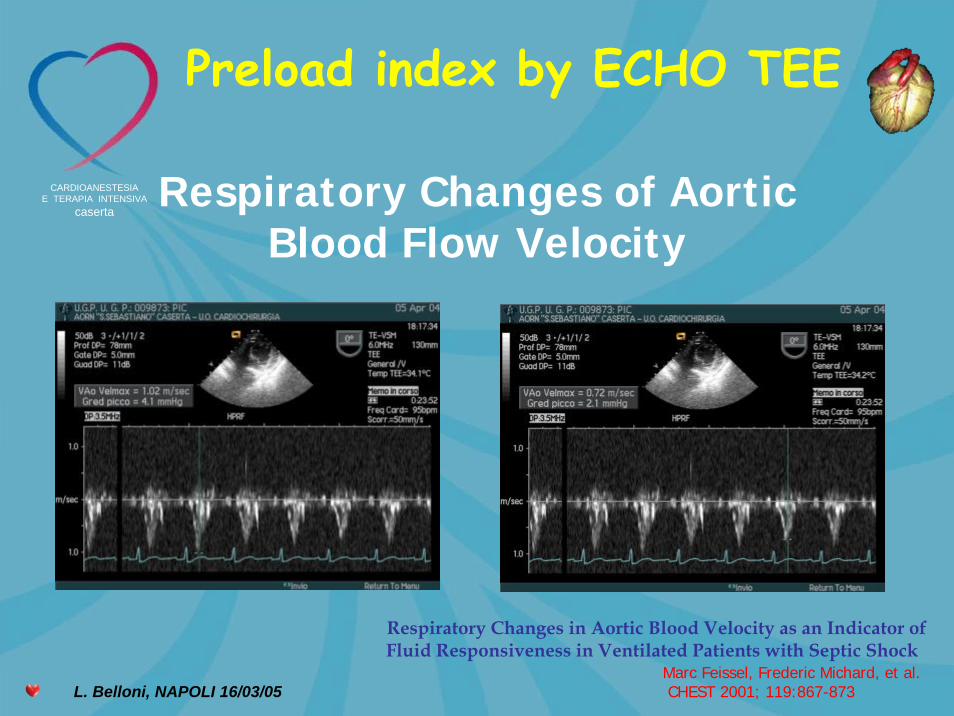
Respiratory Changes of AorticBlood Flow Velocity
Respiratory Changes in Aortic Blood Velocity as an Indicator ofFluid Responsiveness in Ventilated Patients with Septic Shock
Preload index by ECHO TEE
Marc Feissel, Frederic Michard, et al.CHEST 2001; 119:867-873
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
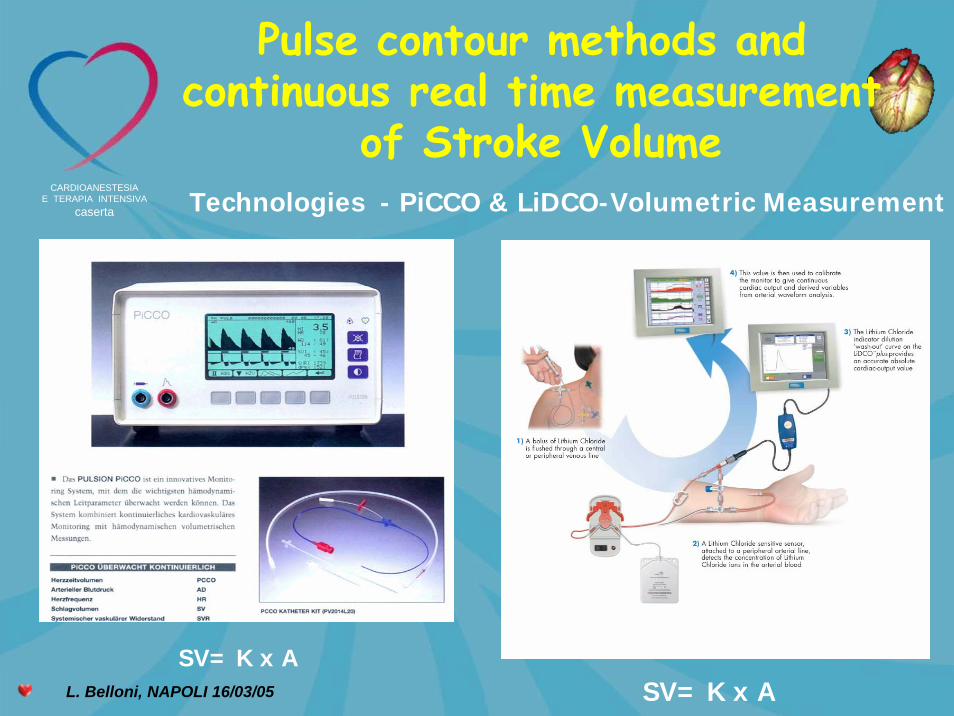
Technologies - PiCCO & LiDCO-Volumetric Measurement
Pulse contour methods and continuous real time measurement
of Stroke Volume
SV= K x ASV= K x A

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
The patient is the more preload responsive the greater the
arterial pressure/stroke volume variation is.

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
Before fluid loading After fluid loading
RESPONDER
Percent change in stroke volume over a floating period of 7.5 secs
StrokeStroke Volume Volume VariationVariation

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05
pts
resp
onde
rs
T0 T1
HR 84.6±15 85±15
mAP 72±10.4 75±8
CVP 5.3±2.5 6.1±2.7
PAOP 12±3 13±2
CI 3.0±0.5 3.2±0.6
SVV 13.7±3.1 7.8±2.1*
SVI 34.4±7 39.6±6.9*p<0.05
Anesthesiology 2001; 95:A243
Della Rocca G, Pompei L, Costa MG, Coccia C, Pierconti F and Pietropaoli P.
STROKE VOLUME VARIATION DURING ANESTHESIA

L. Belloni, NAPOLI 16/03/05
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
The anesthesiologist’s job is toassess the patient, surgeon, and anesthetic thecnique with
minimal hemodynamic disturbance plus activeischemia monitoring, and
aggressive treatment of bothhemodynamic abnormalities and
myocardial ischemia.
L. Belloni, NAPOLI 16/03/05
CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
If is done poorly, the Anesthesiologistbecomes a major
risk factor. Kaplan JA, 1993

CARDIOANESTESIAE TERAPIA INTENSIVA
caserta
L. Belloni, NAPOLI 16/03/05A.O.R.N. “San Sebastiano” Caserta
Cardioanestesia e Terapia Intensiva
Monitoraggio emodinamicostandard (ECG, PA,
saturimetria transcutanea, EtCO2)parametri ventilatori
Echo TEE
PAC/PAC modified
Volumetric monitoring
- PERSONAL EXPERIENCE -
THANK YOU