diagnÓstico no invasivo de cirrosis e...
TRANSCRIPT

DIAGNÓSTICO NO INVASIVO
DE CIRROSIS
E HIPERTENSIÓN PORTAL
Salvador Augustin Hepatología-Medicina Interna
Hospital Vall d’Hebron, Barcelona
5º Curso de Residentes AEEH 30-31 Octubre 2015
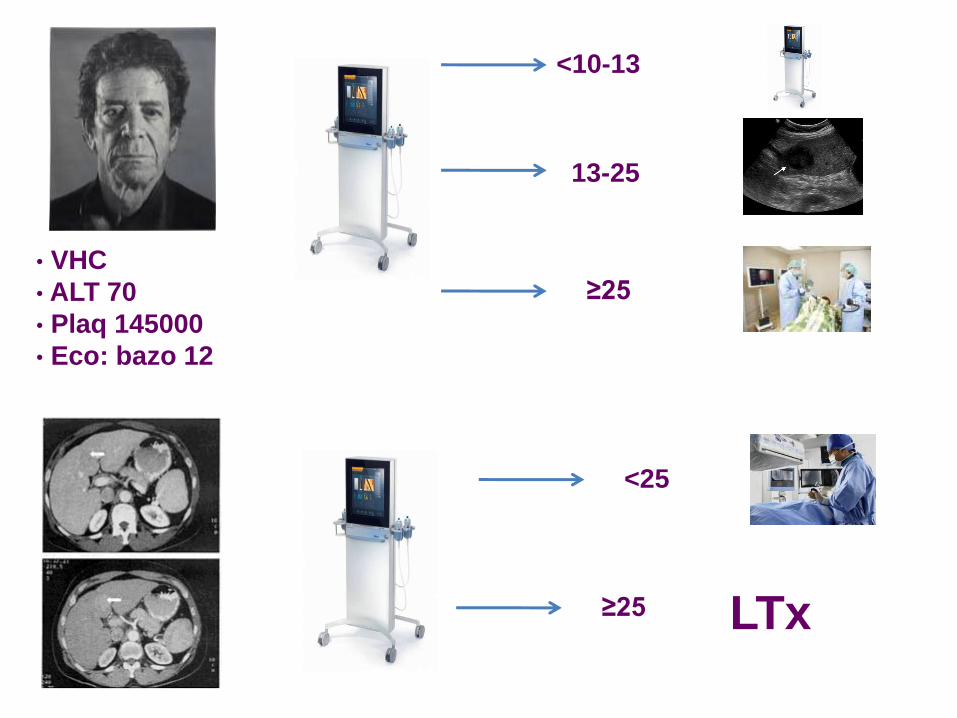
• VHC
• ALT 70
• Plaq 145000
• Eco: bazo 12
BIOPSIA
GPVH
ENDOSCOPIA
Elastografía-cACLD
• Diabetes
• ALT 35, GGT 60
• Eco: esteatosis
• Control, dieta
Diagnóstico No Invasivo
Cirrosis / Hipertensión portal
i. Para qué el diagnóstico de cirrosis/HTP
ii. Diagnóstico NO invasivo HOY
iii. Hacia dónde vamos
Diagnóstico No Invasivo
Cirrosis / Hipertensión portal
i. Para qué el diagnóstico de cirrosis/HTP
ii. Diagnóstico NO invasivo HOY
iii. Hacia dónde vamos
Para qué el diagnóstico de
cirrosis/HTP
1. Cribado de complicaciones
• Varices
• HCC
2. Pronóstico
• Decisiones prácticas
• Estudios
3. Interpretar los síntomas y signos del paciente
Diagnóstico No Invasivo
Cirrosis / Hipertensión portal
i. Para qué el diagnóstico de cirrosis/HTP
ii. Diagnóstico NO invasivo HOY
iii. Hacia dónde vamos
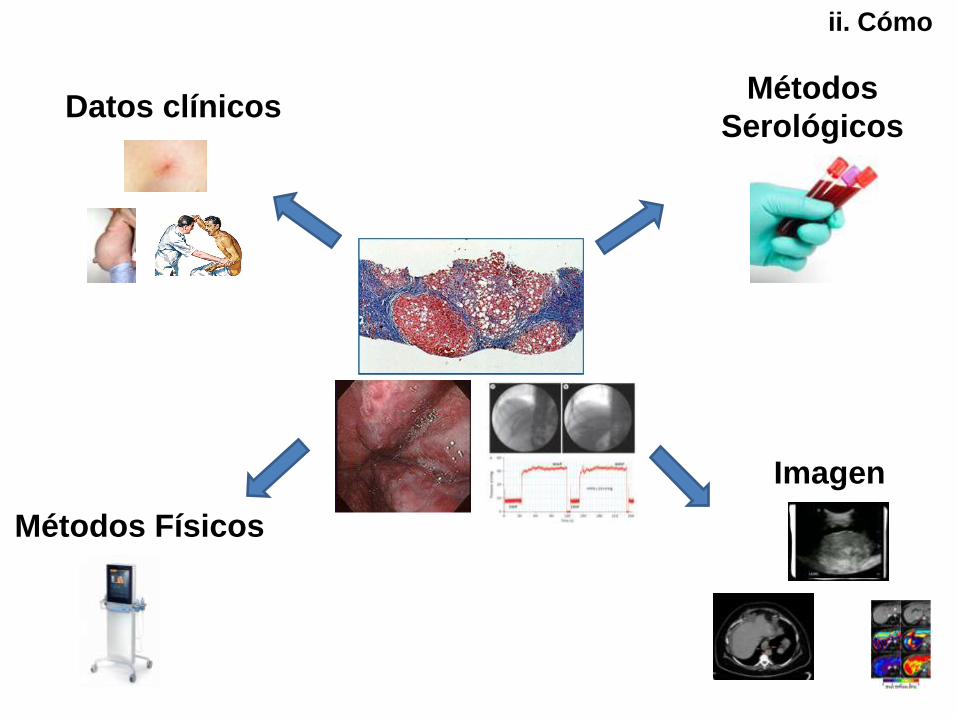
Métodos Físicos
Métodos
Serológicos
Imagen
Datos clínicos
SIGNOS ROJOS EN V. ESOFAGICAS
ii. Cómo

ii. Cómo

ii. Cómo
Qué nospermiten HOY los métodos
diagnósticos no invasivos
1. Evitar exploraciones invasivas
– FGS (DESCARTAR varices)
– HVPG (ASUMIR CSPH)
2. Identificar precozmente cirrosis “oculta”
3. Estadiar al paciente (estudios)
ii. Cómo

¿A TODOS LOS PACIENTES CON CIRROSIS?
NO
Elastografía-cACLD
SIGNOS ROJOS EN V. ESOFAGICAS
¿Cómo EVITAR endoscopia de cribado
VARICES?
- Métodos NO invasivos: DESCARTAR VNT
- Mejor COMBINACIONES de métodos: LSPS,
VRS, ANTICIPATE
- Riesgo aceptable : <5% VNT

N All
varices
VNT Classification rule All varices
NPV
VNT
NPV
Varices
missed
VNT
missed
Endoscopies
avoided
Augustin, et al 49 10% 0 LSM<25
LSM<25+Pla≥150
93%
100%
100%
100%
7%
0
0
0
61%
20%
Montes, et al 85 45%* 20% LSM<20
LSM<20 and/or Pla>120
90%
100%
-
100%
9.5%
0
-
0
25%
15%
Ding, et al 271 - 10% LSM<25+Pla≥100 - 100% - 0 39%
ANTICIPATE 379 42% 15% LSM<25+Pla≥100
LSM<25+Pla≥150
79%
86%
95%
96.5%
21%
14%
5%
3.5%
45%
23%
Elastografía-cACLD
¿Cómo EVITAR endoscopia de cribado
VARICES?
Fibroscan (LSM) + plaquetas

ANTICIPATE STUDY
N 23%
VNT 3.5%
N 34%
VNT 12%
N 57%
VNT 9%
N 43%
VNT 23%
N 12%
VNT 17%
N 31%
VNT 25%
379 patients with endoscopy
LSM ≥25 kPa LSM <25 kPa
Plat ≥ 150 000 Plat < 150 000 Plat ≥ 150 000 Plat < 150 000
393 patients with compensated cirrhosis
Abraldes et al., EASL 2015

ANTICIPATE STUDY
N 45%
VNT 5%
N 12%
VNT 24%
N 57%
VNT 9%
N 43%
VNT 23%
N 24%
VNT 17%
N 19%
VNT 29%
379 patients with endoscopy
LSM ≥25 kPa LSM <25 kPa
Plat ≥ 100 000 Plat < 100 000 Plat ≥ 100 000 Plat < 100 000
393 patients with compensated cirrhosis
Abraldes et al., EASL 2015
Baveno VI
SESSION 1 – Screening and surveillance ; invasive and non invasive methods
IDENTIFICATION OF PATIENTS WITH cACLD WHO CAN SAFELY AVOID SCREENING ENDOSCOPY
• Patients with a liver stiffness < 20 kPa and with
a platelet count > 150,000 have a very low risk of having varices requiring treatment, and can avoid screening endoscopy (3,B)
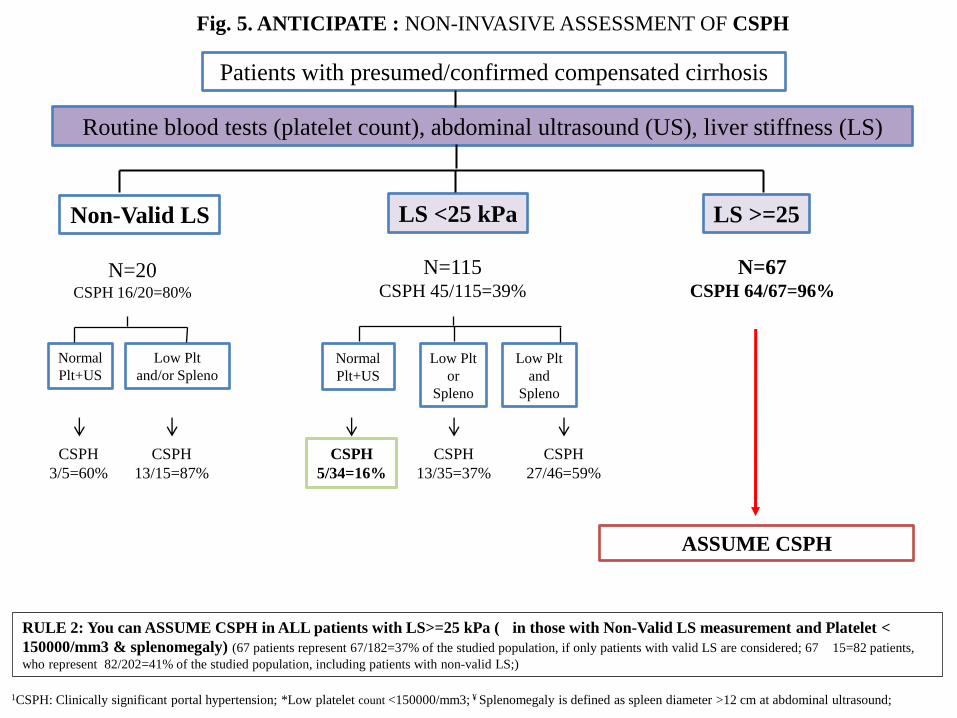
Patients with presumed/confirmed compensated cirrhosis
Routine blood tests (platelet count), abdominal ultrasound (US), liver stiffness (LS)
Non-Valid LS LS <25 kPa LS >=25
N=20 CSPH 16/20=80%
Normal
Plt+US
Low Plt
and/or Spleno
CSPH
3/5=60%
CSPH
13/15=87%
ASSUME CSPH
RULE 2: You can ASSUME CSPH in ALL patients with LS>=25 kPa (
in those with Non-Valid LS measurement and Platelet <
150000/mm3 & splenomegaly) (67 patients represent 67/182=37% of the studied population, if only patients with valid LS are considered; 67
15=82 patients,
who represent 82/202=41% of the studied population, including patients with non-valid LS;)
1CSPH: Clinically significant portal hypertension; *Low platelet count <150000/mm3; ¥ Splenomegaly is defined as spleen diameter >12 cm at abdominal ultrasound;
Fig. 5. ANTICIPATE : NON-INVASIVE ASSESSMENT OF CSPH
N=115 CSPH 45/115=39%
N=67 CSPH 64/67=96%
Normal
Plt+US
Low Plt
or
Spleno
Low Plt
and
Spleno
CSPH
5/34=16%
CSPH
13/35=37%
CSPH
27/46=59%

Fibroscan – CSPH en HCC
HCV All patients
Llop et al., J Hepatology 2012
Baveno VI
SESSION 1 – Screening and surveillance ; invasive and non invasive methods
DIAGNOSIS OF CSPH IN PATIENTS WITH cACLD
• In patients with virus-related cACLD non-invasive methods are sufficient to rule-in CSPH, defining the group of patients at risk of having endoscopic signs of PH. The following can be used (3, B): – Liver stiffness by TE (≥20-25 kPa) alone or combined to Plt and
spleen size – Imaging showing collateral circulation
• The diagnostic value of TE for CSPH in other etiologies remains to be ascertained (5, D)
Elastografía-cACLD
Cirrosis oculta
Elastografía-cACLD
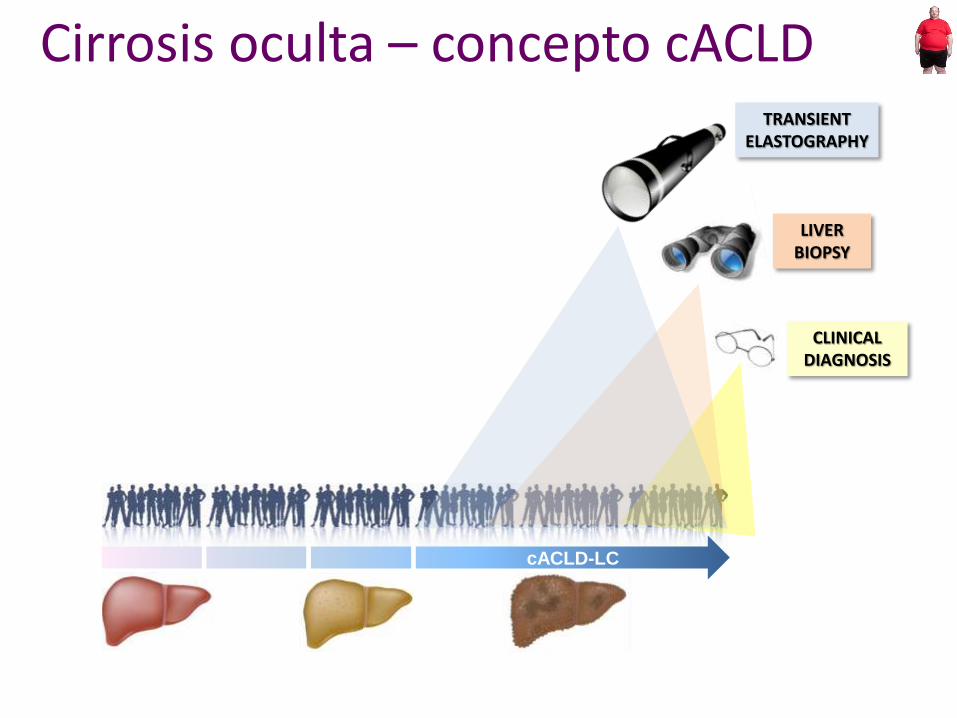
cACLD-LC
CLINICAL DIAGNOSIS
LIVER BIOPSY
TRANSIENT ELASTOGRAPHY
Cirrosis oculta – concepto cACLD
Elastografía-cACLD
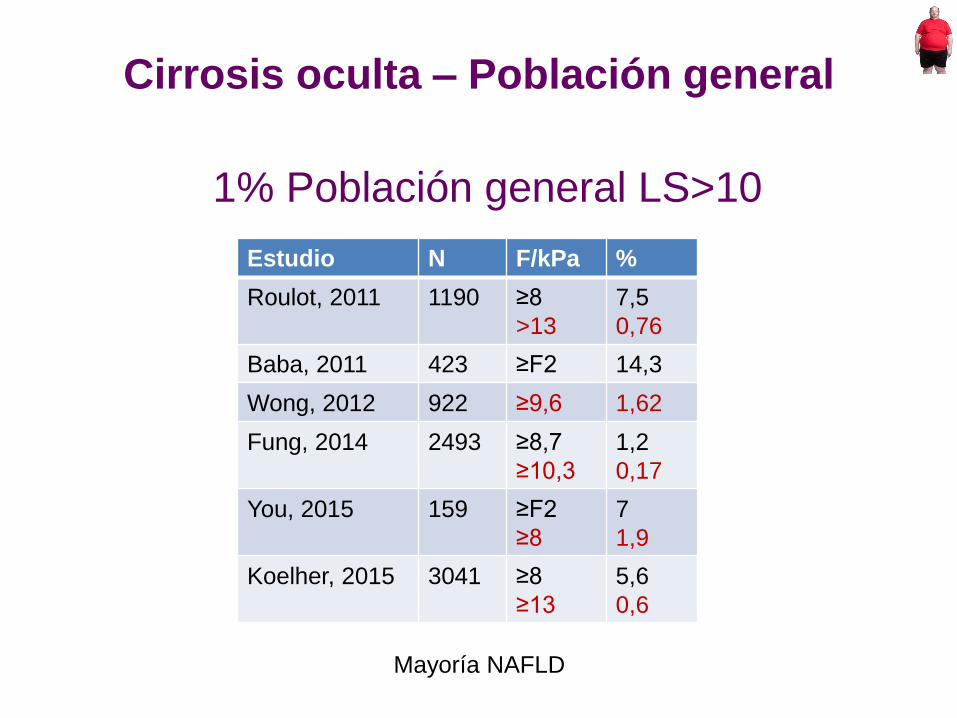
Estudio N F/kPa %
Roulot, 2011 1190 ≥8
>13
7,5
0,76
Baba, 2011 423 ≥F2 14,3
Wong, 2012 922 ≥9,6 1,62
Fung, 2014 2493 ≥8,7
≥10,3
1,2
0,17
You, 2015 159 ≥F2
≥8
7
1,9
Koelher, 2015 3041 ≥8
≥13
5,6
0,6
Mayoría NAFLD
Cirrosis oculta – Población general
1% Población general LS>10
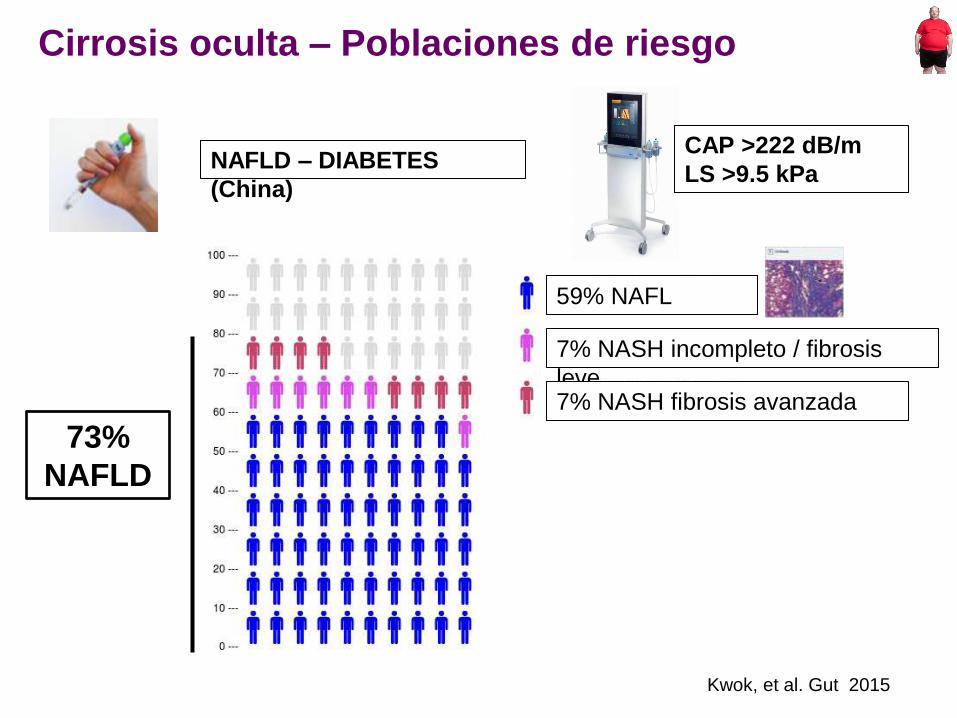
59% NAFL
7% NASH incompleto / fibrosis
leve 7% NASH fibrosis avanzada
73%
NAFLD
Kwok, et al. Gut 2015
NAFLD – DIABETES
(China)
CAP >222 dB/m
LS >9.5 kPa
Cirrosis oculta – Poblaciones de riesgo
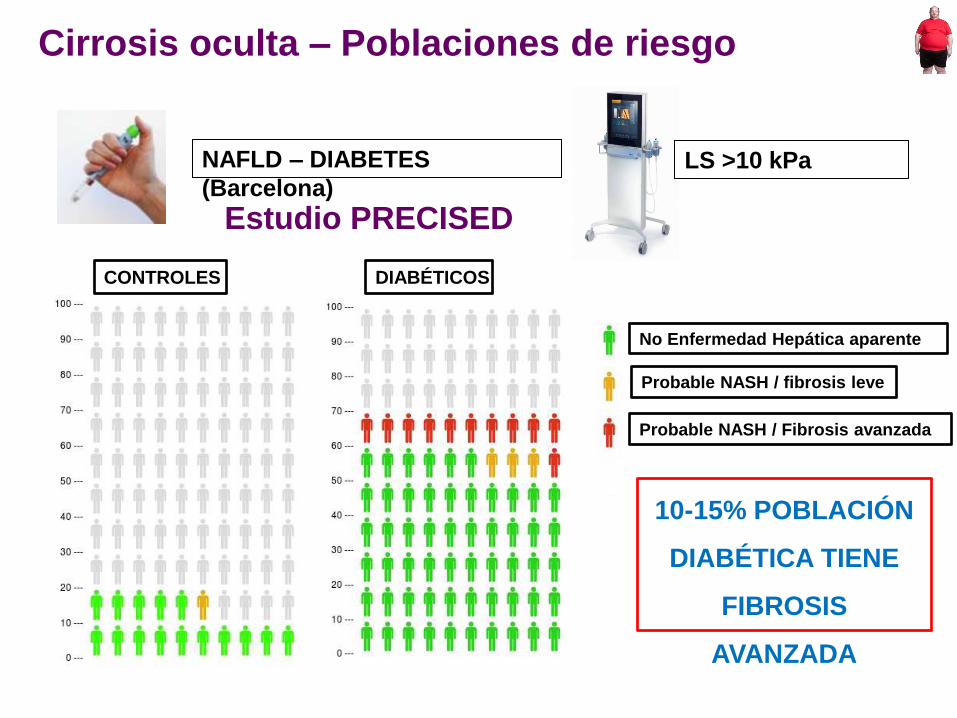
Elastografía-cACLD
Estudio PRECISED
CONTROLES DIABÉTICOS
No Enfermedad Hepática aparente
Probable NASH / fibrosis leve
Probable NASH / Fibrosis avanzada
10-15% POBLACIÓN
DIABÉTICA TIENE
FIBROSIS
AVANZADA
NAFLD – DIABETES
(Barcelona) LS >10 kPa
Cirrosis oculta – Poblaciones de riesgo
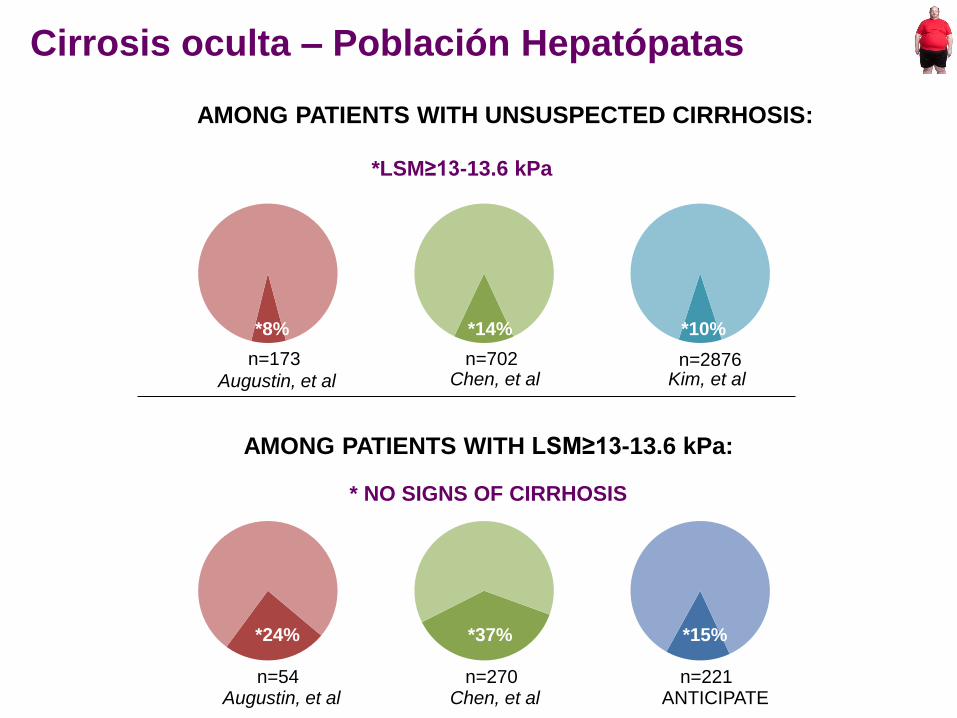
Elastografía-cACLD
AMONG PATIENTS WITH UNSUSPECTED CIRRHOSIS:
Augustin, et al
Augustin, et al
Chen, et al
Chen, et al ANTICIPATE
*LSM≥13-13.6 kPa
* NO SIGNS OF CIRRHOSIS
AMONG PATIENTS WITH LSM≥13-13.6 kPa:
n=173
*8%
n=702
*14%
n=54 n=270 n=221
*24% *37% *15%
*10%
n=2876 Kim, et al
Cirrosis oculta – Población Hepatópatas
Elastografía-cACLD
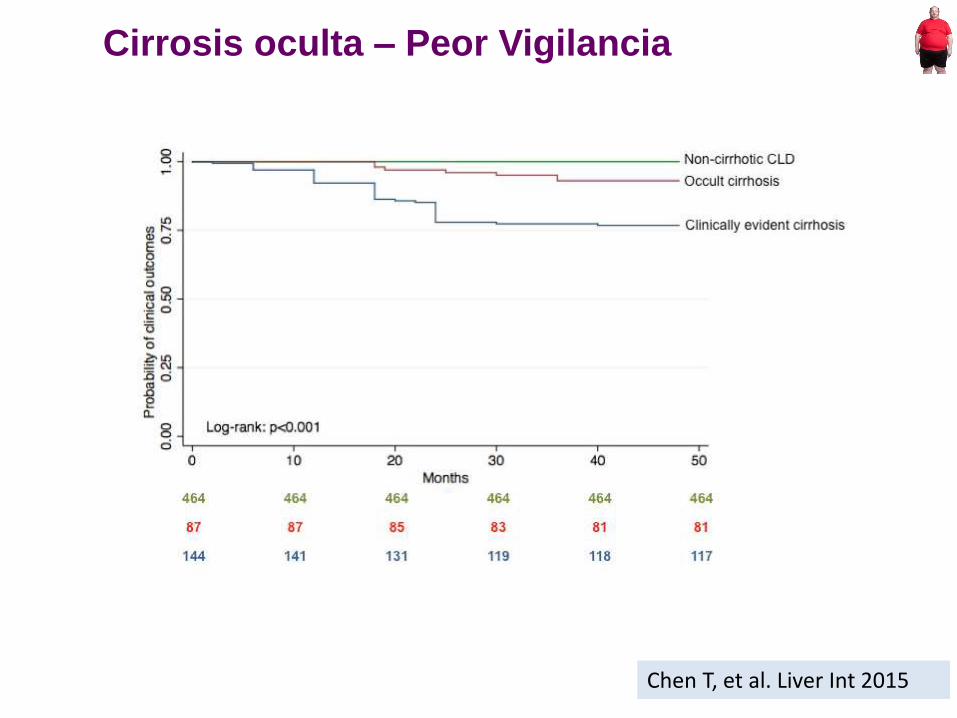
Chen T, et al. Liver Int 2015
Cirrosis oculta – Peor Vigilancia
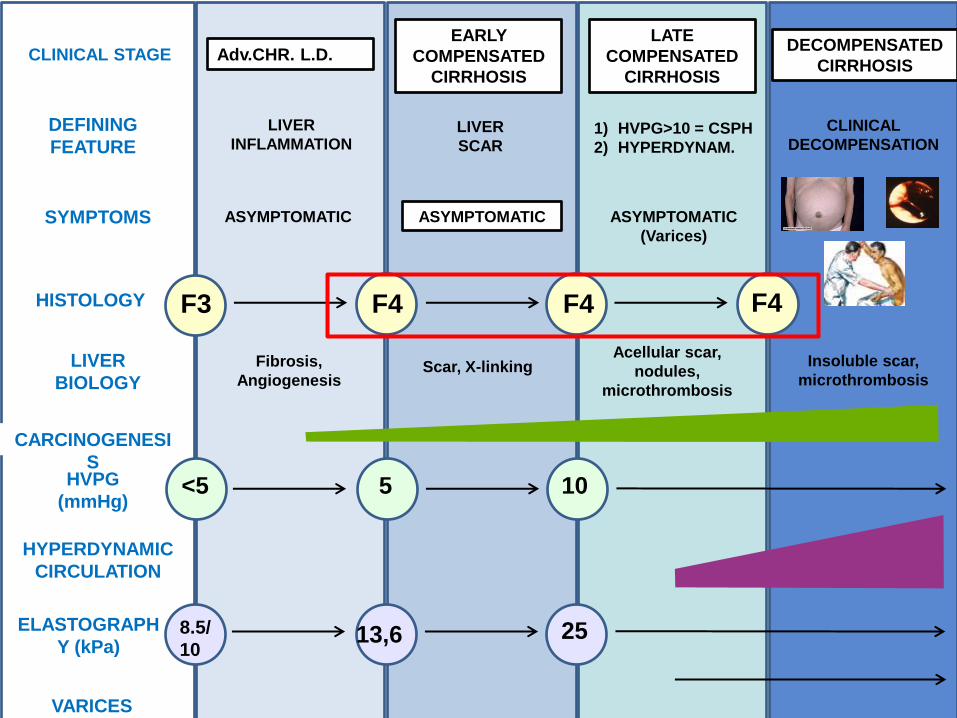
CLINICAL STAGE Adv.CHR. L.D. EARLY
COMPENSATED
CIRRHOSIS
LATE
COMPENSATED
CIRRHOSIS
DECOMPENSATED
CIRRHOSIS
LIVER
BIOLOGY
HISTOLOGY F3 F4 F4 F4
HVPG
(mmHg) <5 5 10
ELASTOGRAPH
Y (kPa) 8.5/
10 13,6 25
VARICES
SYMPTOMS ASYMPTOMATIC ASYMPTOMATIC ASYMPTOMATIC
(Varices)
HYPERDYNAMIC
CIRCULATION
DEFINING
FEATURE
Fibrosis,
Angiogenesis Scar, X-linking
Acellular scar,
nodules,
microthrombosis
Insoluble scar,
microthrombosis
LIVER
INFLAMMATION LIVER
SCAR 1) HVPG>10 = CSPH
2) HYPERDYNAM.
CLINICAL
DECOMPENSATION
CARCINOGENESI
S
• VHC
• ALT 70
• Plaq 145000
• Eco: bazo 12
<10-13
13-25
≥25
≥25 LTx
<25

Elastografía-cACLD
• Diabetes
• ALT 35, GGT 60
• Eco: esteatosis
• Control, dieta
Diagnóstico No Invasivo
Cirrosis / Hipertensión portal
i. Para qué el diagnóstico de cirrosis/HTP
ii. Diagnóstico NO invasivo HOY
iii. Hacia dónde vamos

Future research
CHALLENGES
STRATEGIES
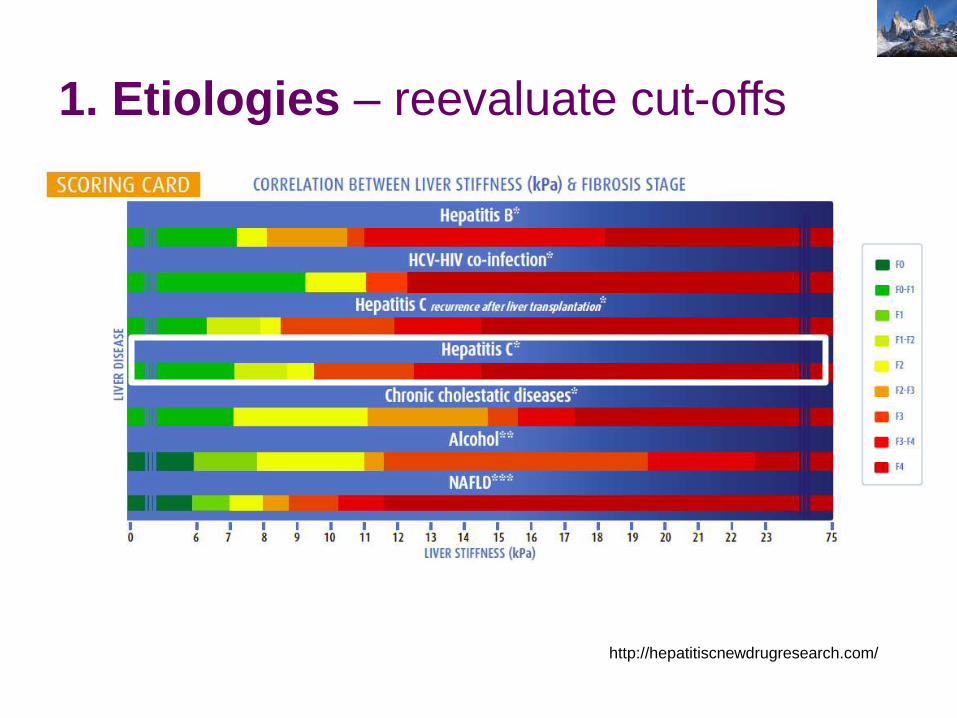
1. Etiologies – reevaluate cut-offs
http://hepatitiscnewdrugresearch.com/
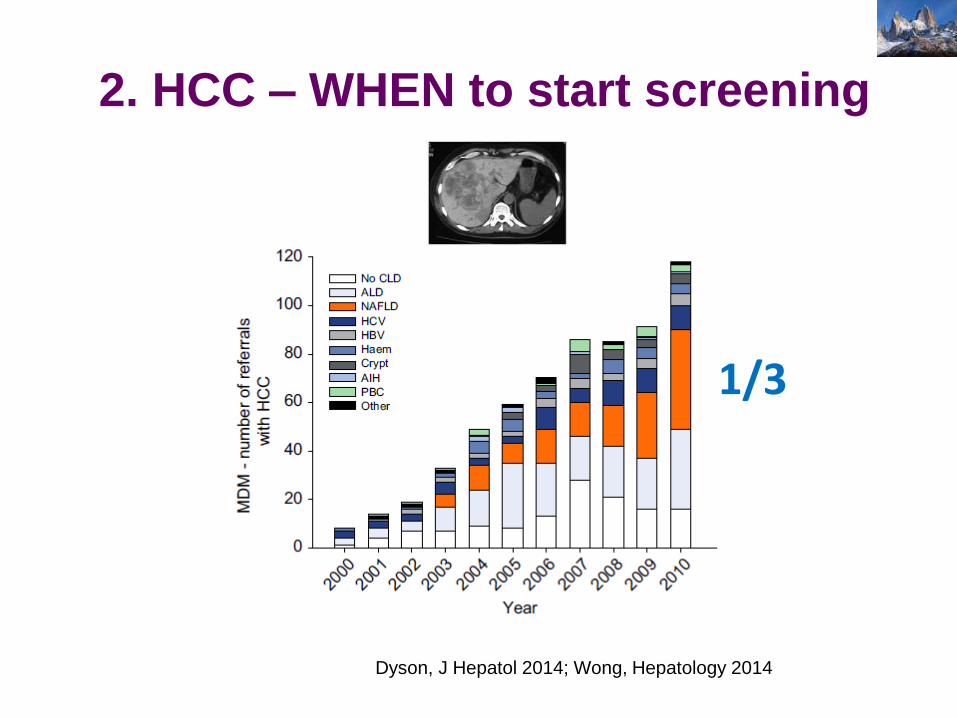
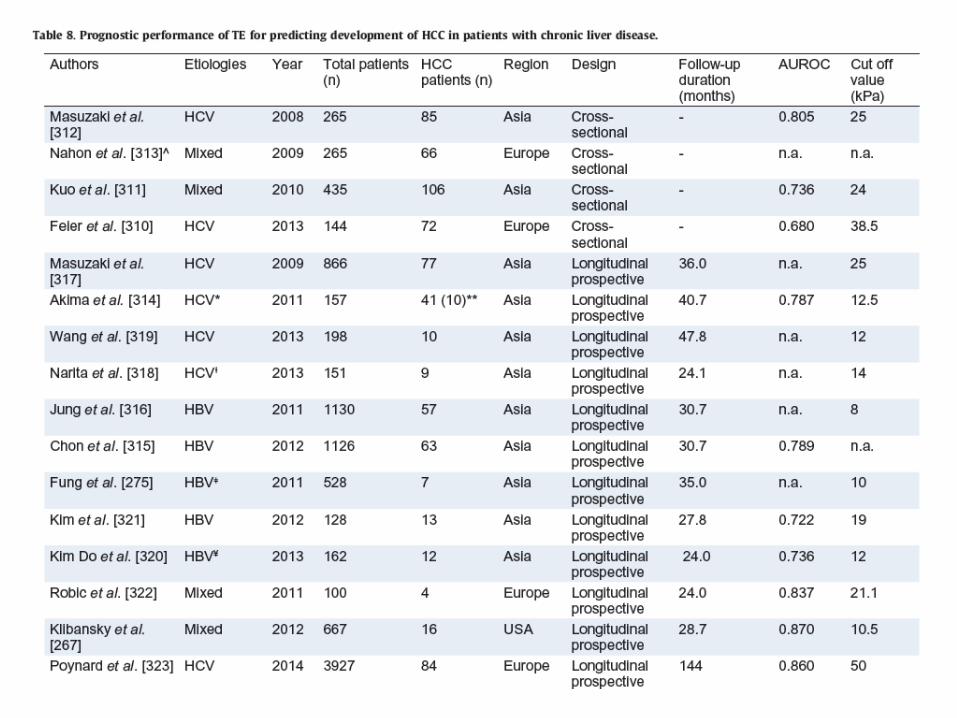
2. HCC – WHEN to start screening
Dyson, J Hepatol 2014; Wong, Hepatology 2014
1/3

Mittal, Clin Gastro Hepatol 2015
86%
72%
58%
0
10
20
30
40
50
60
70
80
90
100
Virus OH NAFLD
Cirrosis AP
N=1419 HCC
(VA – USA)
2. HCC – WHEN to start screening
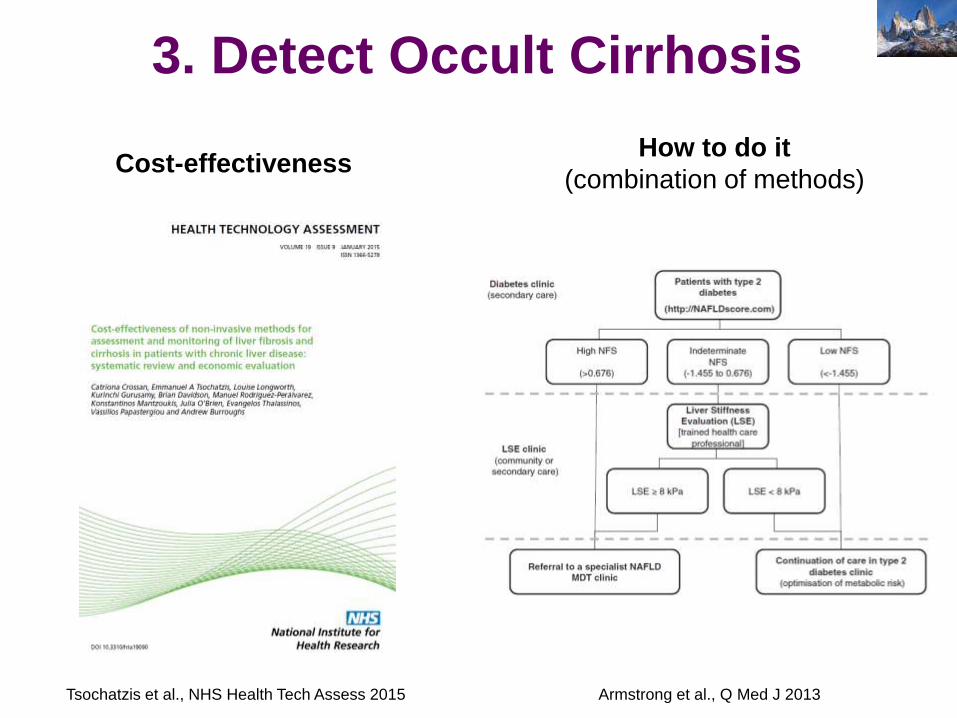
Cost-effectiveness
Tsochatzis et al., NHS Health Tech Assess 2015 Armstrong et al., Q Med J 2013
How to do it
(combination of methods)
3. Detect Occult Cirrhosis

82-83% Prog. LENTOS (> 7 años)
Prog. RÁPIDOS (<6 años)
17%
18%
Singh et al., Clin Gastro Hepatol 2015; McPherson et al. J Hepatol 2015
4. Identify rapid progressors
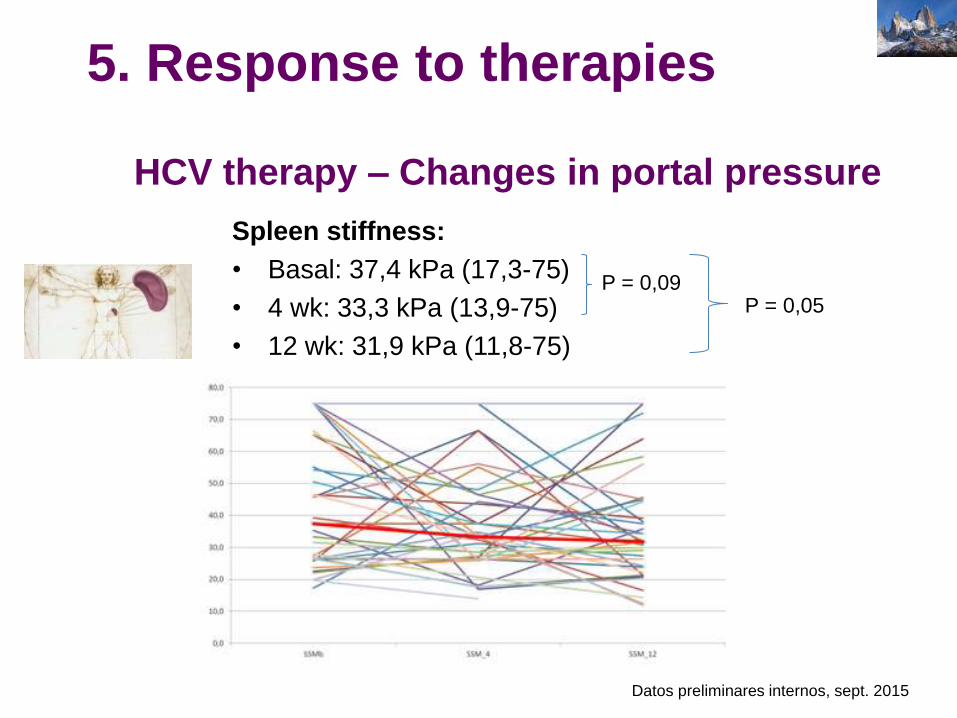
Spleen stiffness:
• Basal: 37,4 kPa (17,3-75)
• 4 wk: 33,3 kPa (13,9-75)
• 12 wk: 31,9 kPa (11,8-75)
P = 0,09 P = 0,05
Elastografía-cACLD
Datos preliminares internos, sept. 2015
5. Response to therapies
HCV therapy – Changes in portal pressure
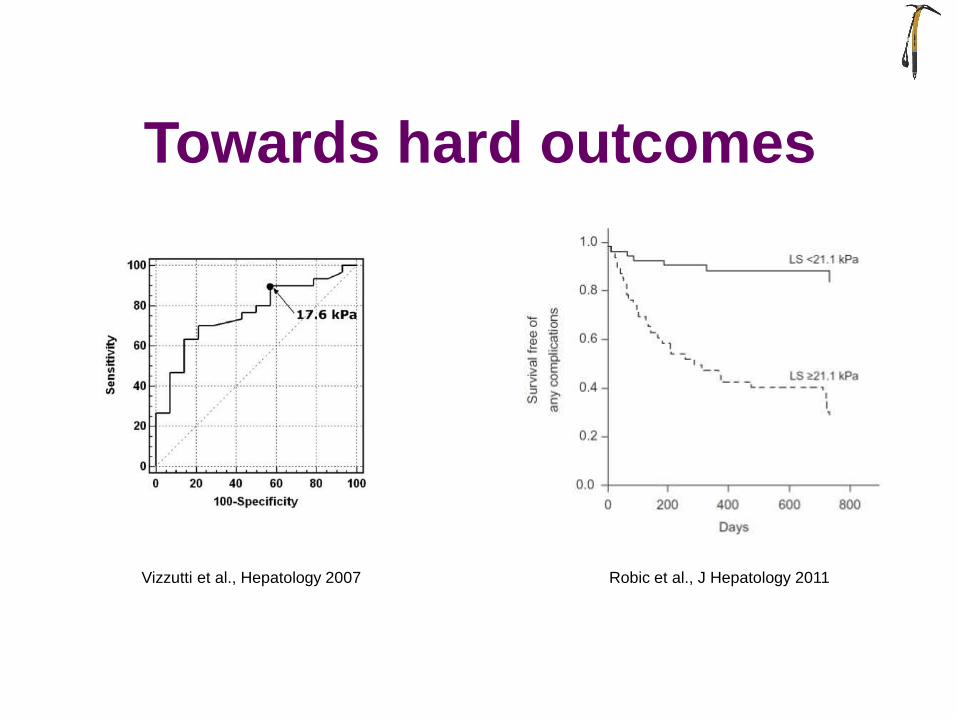
Towards hard outcomes
Vizzutti et al., Hepatology 2007 Robic et al., J Hepatology 2011
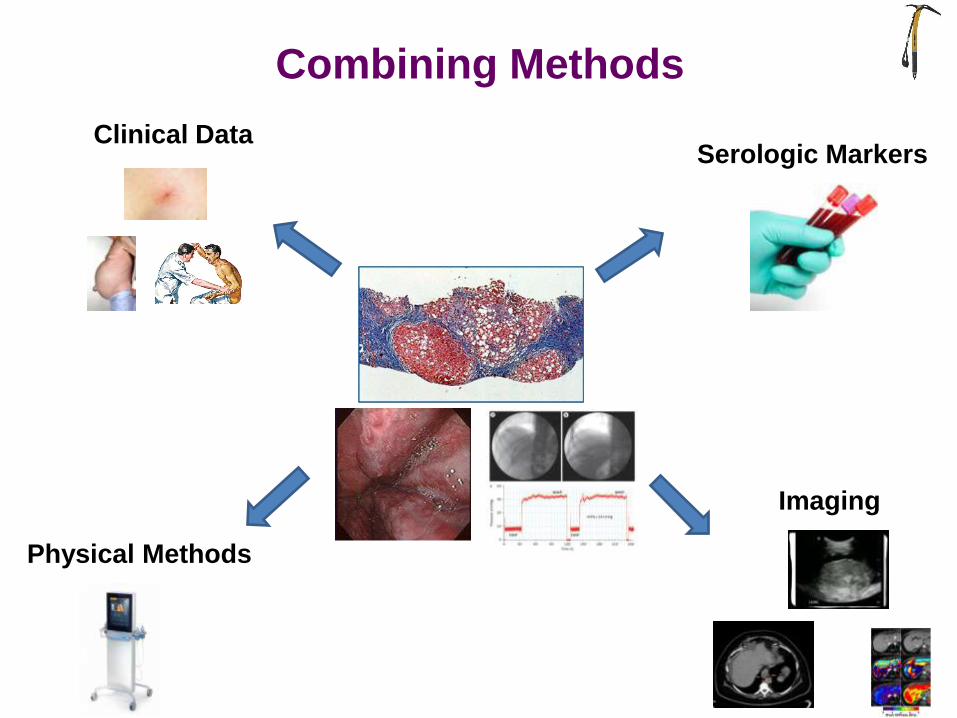
Physical Methods
Serologic Markers
Imaging
Clinical Data
SIGNOS ROJOS EN V. ESOFAGICAS
Combining Methods
Take-Home Messages
• Evitar exploraciones invasivas
– FGS (DESCARTAR varices)
– HVPG (ASUMIR CSPH)
• Detección precoz cirrosis “oculta”
• Redefinición del concepto clínico de cirrosis
Impacto Métodos No Invasivos

CAPACIDAD PREDICTIVA
+ ¿ ?

Muchas Gracias
Q&A slides
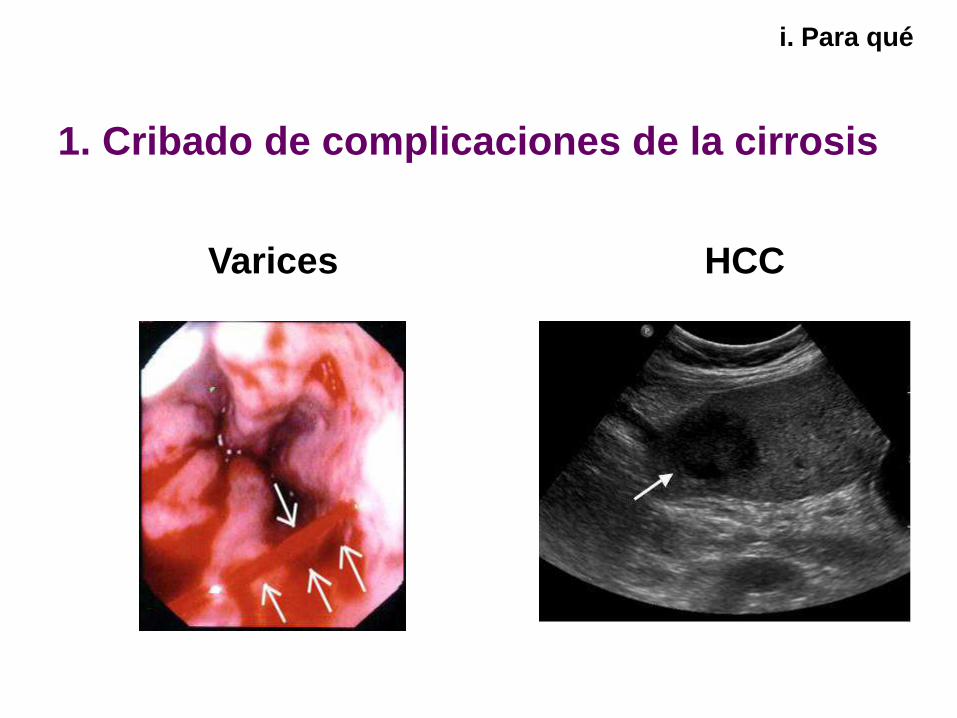
i. Para qué
1. Cribado de complicaciones de la cirrosis
Varices HCC
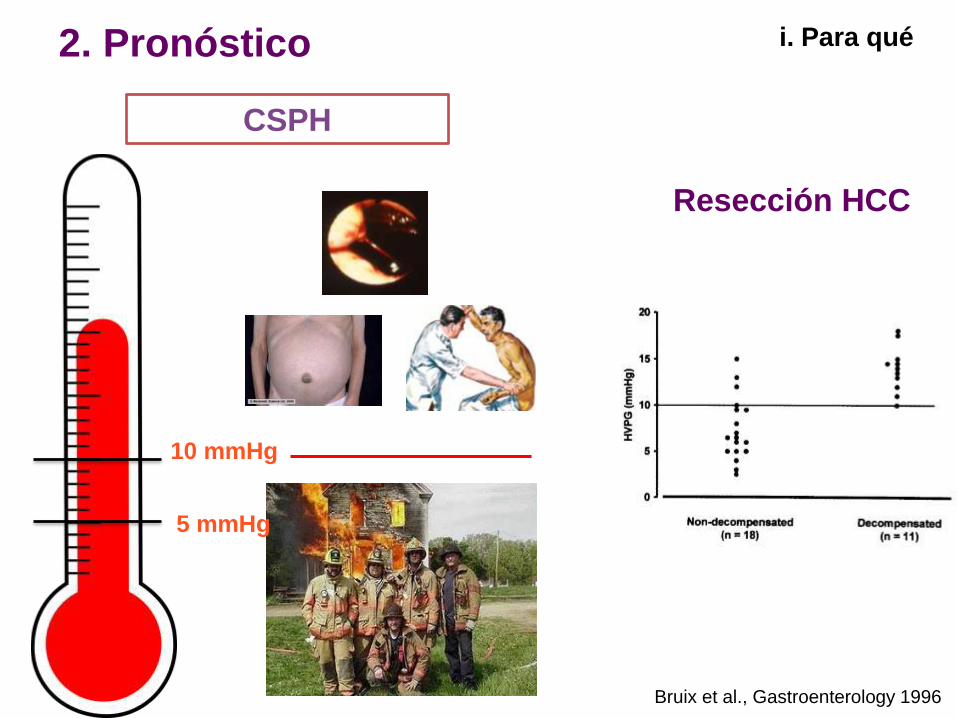
i. Para qué 2. Pronóstico
Resección HCC
Bruix et al., Gastroenterology 1996
CSPH
5 mmHg
10 mmHg

i. Para qué
3. Estudios
HVPG ≥10
HVPG<10
Pacientes Outcomes
Ripoll et al., Gastroenterology 2007
Groszmann et al., NEJM 2005

i. Para qué
4. Interpretación de eventos clínicos del
paciente

“Complexity is
the enemy of
execution”
Development
of new
IDEAS
Development
of new
TOOLS

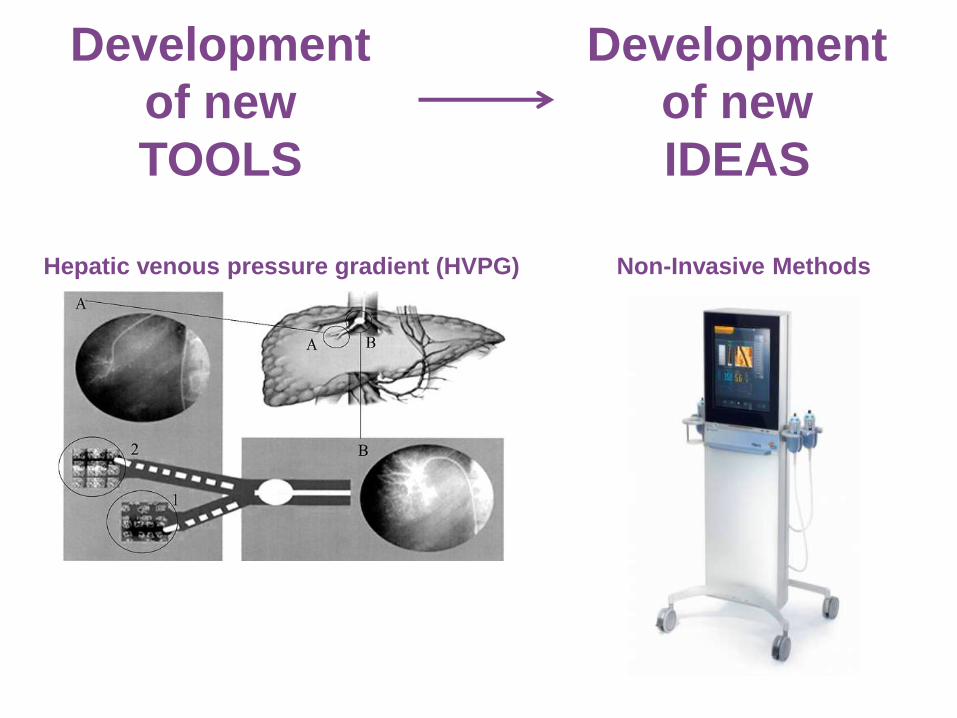
Development
of new
TOOLS
Development
of new
IDEAS
Development
of new
TOOLS
Non-Invasive Methods Hepatic venous pressure gradient (HVPG)
Development
of new
IDEAS
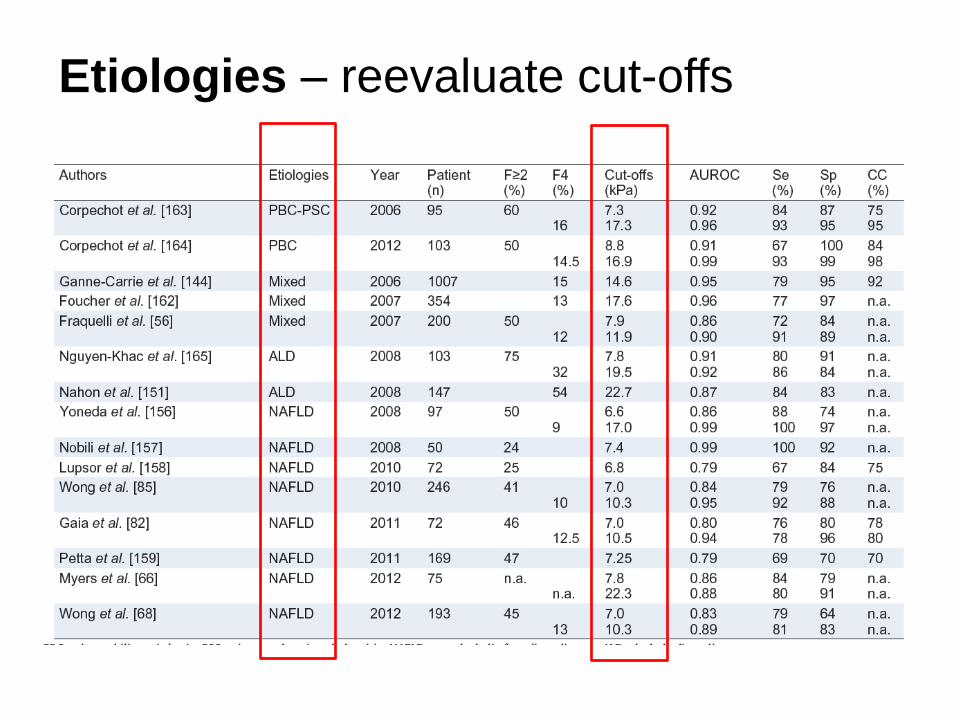
Etiologies – reevaluate cut-offs

What we talk about when we talk about cirrhosis
PROGNOSIS - RISKS
“Now there are many where before there was one…”

Robic et al. J Hepatol 2011
-100 Px -16 meses -65% CH -HVPG ≥10: 51% -Varices: 72% de CH -No tratamiento -41% alguna complicación
Elastografía-cACLD
Impacto elastografía-Pronóstico

G. García-Tsao, Hepatology 2010