injuria cerebral traumatica 2012-2 (1)
TRANSCRIPT

Severe TraumaticBrain Injury
Halinder S. Mangat, MD
ABSTRACTPurpose of Review: Although adherence to traumatic brain injury (TBI) guidelineshas been associated with improved patient outcomes, guideline adherence remainssuboptimal in practice. With neurologists becoming increasingly involved in specializedneurointensive care units and in the care of patients with severe TBI, familiarizationwith these guidelines is essential.Recent Findings: Intracranial monitoring of different physiologic variables has in-creased in the past few years. Intracranial pressure (ICP)Ydriven therapy has beenreplaced by ICPYcerebral perfusion pressure (CPP)Ydriven therapy. More recently, theimportance of brain oxygen optimization in addition to ICP-CPP has been recognized,and clinical trials are underway to study the effect of this approach. Surgicalmanagement of patients with TBI is also evolving rapidly with further studies on de-compressive craniectomy. These are significant advances to improve TBI outcomes.Summary: This article summarizes the routine monitoring of patients with severe TBIand offers insight into some novel physiologic monitoring devices available. Theguidelines for management of patients with severe TBI are summarized along withoutcome measures.
Continuum Lifelong Learning Neurol 2012;18(3):532–546.
INTRODUCTIONInjuries are the leading cause of deathbetween the ages of 1 and 44 years.1
Traumatic brain injury (TBI) accountsfor 30% of the mortality associated withinjury-related death.2 TBI is defined asan alteration in brain function or otherevidence of brain pathology caused byan external force.3 A severe TBI is onein which the patient presents with lossof consciousness and a Glasgow ComaScale (GCS) score of less than 9. Neuro-imaging usually shows diffuse or focallesion(s). Severe TBI results in highmortality whereas mild TBI is increas-ingly recognized as causing significantfunctional morbidity.
EPIDEMIOLOGYApproximately 1.7 million Americanshave a TBI every year.2 This leads to
1.3 million visits to the emergency de-partment, 275,000 hospitalizations, and52,000 deaths. Fortunately, 75% of allTBIs are mild. The common causes ofTBI are falls (35%), motor vehicle acci-dents (17%), struck-by events (17%),assaults (10%), and unknown causes(21%). The highest incidence of TBIoccurs among children younger than 4years and adults older than 65 years.In these ages, falls are themost commoncause. Between ages 14 and 34, thereis a high incidence of motor vehicleYrelated TBI. Patients older than 75 havethe highest TBI-related mortality. Menare four times more likely to have a TBIthan women in the same age group.Direct medical costs and indirect costsof TBI, such as loss of productivity, to-taled $60 billion in the United States inthe year 2000.4
Address correspondence toDr Halinder Mangat, WeillCornell Medical Center,Department of Neurologyand Neuroscience, 525 E.68th St., Ste F-610,New York, NY 10021,[email protected].
Relationship Disclosure:Dr Mangat reports nodisclosure.
Unlabeled Use ofProducts/Investigational
Use Disclosure:Dr Mangat reports nodisclosure.
* 2012, American Academyof Neurology.
532 www.aan.com/continuum June 2012
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

CEREBROVASCULARPHYSIOLOGYWe will first review the cerebrovascu-lar physiology that forms the basis oftherapeutic strategies in severe TBI.
Monro-Kellie DoctrineThe contents of the cranial cavity arebrain, CSF, and blood (arterial andvenous). In an adult, the brain makes up80% of the contents, and the CSF and theblood each make up 10%. Because thecranial vault cannot expand, the totalintracranial volume remains constant.Therefore, an increase in the volume ofone compartment or appearance of a newmass lesion must result in a decrease inthe volume of the other compartments.
To compensate for any increase involume due to a lesion, compartmentscontaining blood and CSF experiencedecreases in volume. Cerebral bloodvolume is distributed between venoussinuses (two-thirds) and arterioles (one-third). To compensate for the volume ofa new lesion (such as a hematoma,cerebral contusion, or cerebral edema),
the venous sinuses collapse readily andpush venous blood into the systemiccirculation. The arteriolar bed then re-mains the main blood volume regulatorand can compensate for up to 75 mLin volume. The most important bloodvolume regulator is arteriolar carbondioxide. Similarly, the CSF compart-ment compensates by decreasing CSFproduction and increasing absorption,and some CSF is also pushed into thesubarachnoid space from the ventricles.
Brain ComplianceOnce intracranial compensatory mecha-nisms are exhausted, small increases inintracranial volume can cause largeincreases in ICP, leading to herniation.It is therefore imperative for the neuro-intensivist to know the compliance sta-tus of the brain. Brain compliance isdivided into the following stages, asshown in Figure 2-1:5
1. High compliance + normal ICP2. Low compliance + normal ICP3. Low compliance + increased ICP
KEY POINTS
h In an adult, the brainmakes up 80% of thecontents of the cranialcavity, and the CSF andthe blood each makeup 10%.
h Once intracranialcompensatorymechanisms areexhausted, smallincreases in intracranialvolume can cause largeincreases in ICP, leadingto herniation. It istherefore imperative forthe neurointensivist toknow the compliancestatus of the brain.
FIGURE 2-1 Brain compliance curve demonstrating different stages of braincompliance.
Reprinted from Brunicardi FC, Andersen DK, Billiar TR, et al, editors. Schwartz’s principles of surgery. 9thed. New York, NY: McGraw-Hill Professional, 2009.5 B 2009, with permission from The McGraw-HillCompanies, Inc.
533Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Progression beyond the third stagecauses precipitous rise in ICP and brainherniation. Herniation, however, mayalso occur at an earlier stage if there arefocal lesions with compartmental highICP. This can occur with temporal lobecontusions and result in uncal herniation.
Cerebral Blood FlowAutoregulationBrain perfusion is maintained by a con-stant cerebral blood flow (CBF) over awide range of systemic blood pressure(mean arterial pressure [MAP] 60mmHgto 160 mm Hg or CPP 50 mm Hg to150mmHg) (Figure 2-2).6 This constantCBF is achieved by a mechanism calledpressure autoregulation. This occurs atthe arteriolar level by vasodilatation atlow perfusion pressures and vasocon-striction at higher perfusion pressures.Beyond these autoregulation thresholds,the arterioles are no longer able tocompensate, resulting in abnormal CBFand severe ischemia. The autoregu-lation curve shifts to the left in states
of high ICP and to the right in long-standing systemic arterial hypertension.
Flow-metabolism coupling is themechanism by which CBF is coupledto cerebral metabolism and is thereforeproportional to it. Lowering brain me-tabolism consequently decreases CBF.This serves as a basis for reducing ICPby sedation and hypothermia.
PATHOPHYSIOLOGY OF SEVERETRAUMATIC BRAIN INJURYPrimary InjuryThe forces of impact determine thenature of primary injury from TBI. Themechanisms implicated are acceleration-deceleration (motor vehicle accidents,falls), rotational (motor vehicle accidents,falls), crush (struck-by events, motorvehicle accidents), andmissile (gun shot,shrapnel). Focal lesions include subduralhematomas (SDHs), cerebral contusionswith intracerebral hemorrhage, epiduralhematoma (EDH), and traumatic subar-achnoid hemorrhage (tSAH). Diffuselesions include tSAH and diffuse axonalinjury due to shear forces. The mainstayof reducing primary injury is prevention.
Secondary InjuryNumerous factors cause secondary in-jury, and it is imperative to anticipatethese and minimize their detrimentaleffect. Frequently, the initial injury issevere but treatable, such as an acuteSDH or EDH. However, patients oftendeteriorate further and become severelyill due to secondary injuries, such asischemia, hypoxia, edema, and resultantintracranial hypertension.
Hypoxia-ischemia is one of the mostimportant secondary factors that influ-ences outcome after TBI. The most crit-ical time is during resuscitation andimmediately post-injury, when systemichypoxia and hypotension are likely to oc-cur due to either inability to establish anairway or volume loss fromhemorrhage.
KEY POINTS
h The Monro-Kelliedoctrine states thatintracranial volumeremains constant, andaddition or increase inthe volume of onecompartment mustcause a decrease inanother or result in anincrease in intracranialpressure. Cerebral bloodflow remains constantat mean arterialpressures between60 mm Hg and 160 mmHg by autoregulatorymechanisms.
h In addition to initialinjury, secondary injuryis caused by hypoxia,hypotension, ischemia,seizures, and metabolicimpairment such asmitochondrial injury.
FIGURE 2-2 Autoregulation curve with vessel caliber.
CBF = cerebral blood flow;CVR = cerebrovascular resistance.
Reprinted with permission from Rosenthal G, Sanchez-Mejia RO, Phan N,et al. Incorporating a parenchymal thermal diffusion cerebral blood flowprobe in bedside assessment of cerebral autoregulation and vasoreactivity inpatients with severe traumatic brain injury. J Neurosurg 2011;114(1):62Y70.6
thejns.org/doi/abs/10.3171/2010.6.JNS091360?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
534 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Subsequent hypoxia-ischemia alsoresults from vascular injury, systemiccauses, cerebral edema (which causesa diffusion gradient for oxygen), intra-cranial hypertension, and exaggeratedhyperventilation.
Disordered cerebral metabolismmaybe due to cellular as well as mitochon-drial injury. Mitochondrial membranesand oxidative metabolic processes aredisrupted, which results in toxic calciuminflux and cellular death. In SDH, PETimaging shows that metabolic impair-ment occurs well beyond the extent ofinjury visible on CT imaging.7
CBF dysautoregulation also occurs asa result of severe TBI and is associatedwith poor outcome.8 Dysautoregulationcan be focal or diffuse, and its presencepredisposes tissue to hyperperfusionand vasogenic edema. The state of auto-regulation can be determined by sim-ple observation of changes in ICP withspontaneous changes in MAP. With lossof autoregulation, ICP increases line-arly, with increases in MAP even withinthe postulated autoregulation range.The pressure reactivity index (PRx) is amoving index of correlation betweenICP and MAP and is used as an index ofautoregulation. It ranges fromj1 to+1.A negative value (including 0) indicatesgood autoregulation, and a positive valueindicates decreased autoregulation.
Inflammatory mechanisms are beingincreasingly recognized as mediators ofsecondary injury by inducing inflamma-tory cytokines as well as microglial ac-tivation in the brain.
Electrophysiologic phenomena suchas seizures and epileptiform dischargesoccur in the postinjury period and leadto detrimentalmetabolic derangements.Monitoring for these phenomena isimportant because they can be subclin-ical.9 Cortical spreading depression(CSD) is an electrophysiologic phe-nomenon that occurs after TBI and isassociated with poor prognosis. CSD
occurs over the injured cortex, involv-ing waves of depolarization that spreadat 2 mm/min to 5 mm/min and causeionic fluxes, metabolic derangements,and vascular flow abnormalities.10
Secondary injury results from a com-posite of the above processes and leadsto cell injury, death, and apoptosis. Re-sultant inflammation and edema, alongwith evolution of primary lesions suchas cerebral contusions, cause intracra-nial hypertension. This causes furthercellular hypoxia and injury and cascadesinto a positive feedback cycle. While itis essential to arrest all of these pro-cesses, the occurrence of each cannotyet be determined clinically or by bed-side monitoring. Therefore, the main-stay of therapy targets treatment ofintracranial hypertension, cerebralhypotension, and cerebral hypoxia.
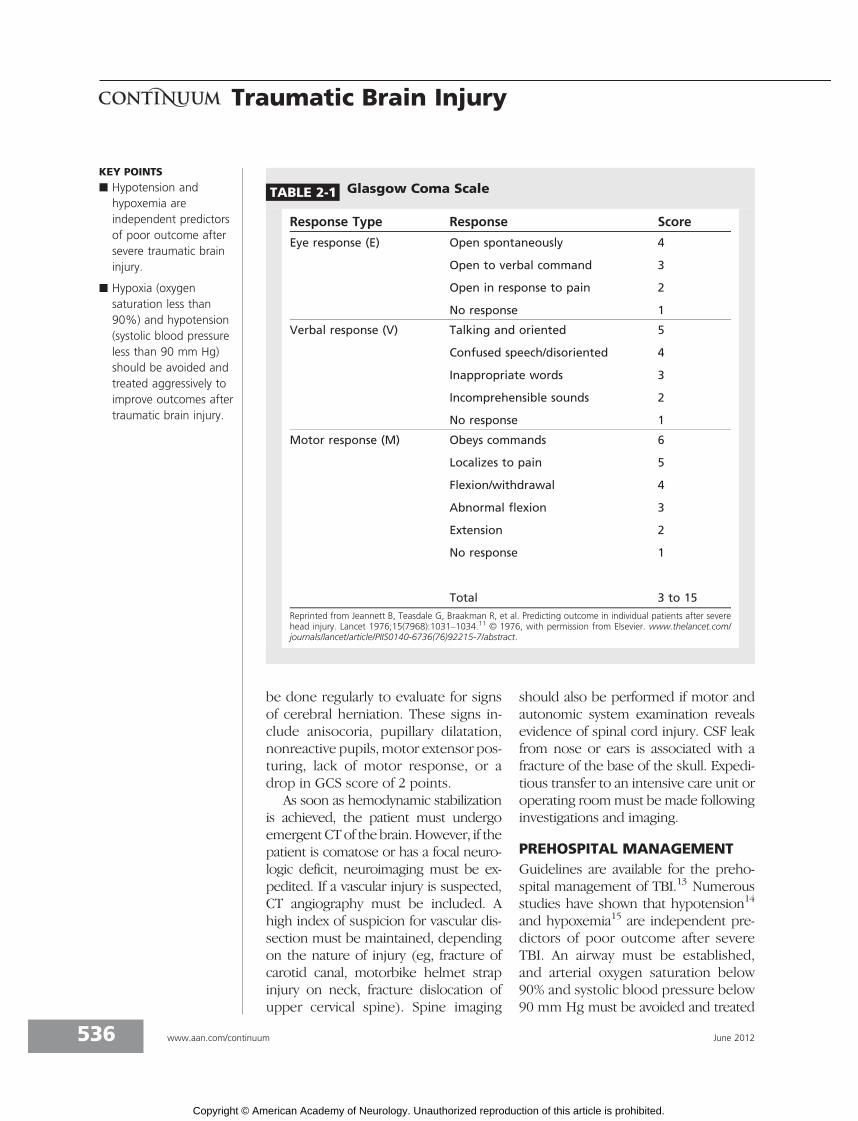
EVALUATION AND DIAGNOSISEarly evaluation is essential for earlyintervention and begins at the scene ofthe injury. Airway, breathing, and circu-lation must be assessed. Preliminaryneurologic examination at the sceneshould focus on the GCS (Table 2-1)11
and examination of the pupils. Pupillarysize, reactivity, and asymmetry shouldbe noted. Pupillary asymmetry isdefined as a size difference greater than1 mm. A fixed pupil is defined as onethat has a response to light of less than1 mm. Orbital trauma must be noted.The GCS and pupils must be assessedregularly and in the absence of medi-cations that may interfere with an ac-curate response.
A direct transfer must be made to aLevel I or Level II trauma center. Mortal-ity increases by 50% when patients arenot transferred directly to the appropri-ate hospital, even if it is not the nearesthospital.12 A complete primary survey bya certified traumatologist is essential torule out other potentially life-threateninginjuries. A neurologic examination must
KEY POINT
h Direct transfer to a LevelI or Level II traumacenter improvesoutcomes, even if sucha hospital is not thenearest one.
535Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
be done regularly to evaluate for signsof cerebral herniation. These signs in-clude anisocoria, pupillary dilatation,nonreactive pupils, motor extensor pos-turing, lack of motor response, or adrop in GCS score of 2 points.
As soon as hemodynamic stabilizationis achieved, the patient must undergoemergent CTof the brain. However, if thepatient is comatose or has a focal neuro-logic deficit, neuroimaging must be ex-pedited. If a vascular injury is suspected,CT angiography must be included. Ahigh index of suspicion for vascular dis-section must be maintained, dependingon the nature of injury (eg, fracture ofcarotid canal, motorbike helmet strapinjury on neck, fracture dislocation ofupper cervical spine). Spine imaging
should also be performed if motor andautonomic system examination revealsevidence of spinal cord injury. CSF leakfrom nose or ears is associated with afracture of the base of the skull. Expedi-tious transfer to an intensive care unit oroperating roommust be made followinginvestigations and imaging.
PREHOSPITAL MANAGEMENTGuidelines are available for the preho-spital management of TBI.13 Numerousstudies have shown that hypotension14
and hypoxemia15 are independent pre-dictors of poor outcome after severeTBI. An airway must be established,and arterial oxygen saturation below90% and systolic blood pressure below90 mm Hg must be avoided and treated
KEY POINTS
h Hypotension andhypoxemia areindependent predictorsof poor outcome aftersevere traumatic braininjury.
h Hypoxia (oxygensaturation less than90%) and hypotension(systolic blood pressureless than 90 mm Hg)should be avoided andtreated aggressively toimprove outcomes aftertraumatic brain injury.
TABLE 2-1 Glasgow Coma Scale
Response Type Response Score
Eye response (E) Open spontaneously 4
Open to verbal command 3
Open in response to pain 2
No response 1
Verbal response (V) Talking and oriented 5
Confused speech/disoriented 4
Inappropriate words 3
Incomprehensible sounds 2
No response 1
Motor response (M) Obeys commands 6
Localizes to pain 5
Flexion/withdrawal 4
Abnormal flexion 3
Extension 2
No response 1
Total 3 to 15
Reprinted from Jeannett B, Teasdale G, Braakman R, et al. Predicting outcome in individual patients after severehead injury. Lancet 1976;15(7968):1031Y1034.11 B 1976, with permission from Elsevier. www.thelancet.com/journals/lancet/article/PIIS0140-6736(76)92215-7/abstract.
536 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

immediately, as illustrated in Case 2-1.End-tidal carbon dioxide must be main-tained between 35 mm Hg and 40 mmHg. Volume status should be assessedand resuscitation begun. In pediatricpatients, critical low threshold for sys-tolic blood pressure is less than 60 mmHg for 0 to 28 days of age; less than70 mm Hg for 1 to 12 months of age;less than 70 mm Hg plus 2 times agein years for 1 to 10 years; and less than90 mm Hg for older than 10 years.
Cerebral herniation can be treatedwith mild hyperventilation to targetend-tidal carbon dioxide 30 mm Hg to35 mm Hg. This is a temporizing mea-sure and should be discontinued oncesigns resolve and other therapies havebeen delivered. Hyperventilation shouldbe delivered by administering 20 breaths/min in an adult, 25 breaths/min in achild, and 30 breaths/min in an infant.
INTENSIVE CARE UNITMONITORING OF A PATIENTWITH SEVERE TRAUMATICBRAIN INJURYOn arrival at the trauma bay, a completeprimary surveymust be done, followedbymanagement of the most life-threateninginjuries. Once diagnostic and immediate
surgical interventions are completed,the patient must be transported to anintensive care unit (ICU). Patients caredfor in a specialized neurocritical care unithave improved outcomes.16 Precautionsshould be taken to assess spinal injuryand to document any suspicion thereof.
The Brain Trauma Foundation en-dorses very elaborate yet clear guide-lines for the critical care management ofa patient with severe TBI.17 The mainprinciples of therapy are to ensure ade-quate cerebral perfusion and oxygen-ation while brain swelling and injuryimprove. The next sections discuss theparameters that can be monitored assurrogate indices of brain ischemia andhypoxia. (A below/above critical thresh-old value is defined as one that remainsabnormal for 5 consecutive minutesand is considered normalized when ithas remained within normal range for5 consecutive minutes.)
Blood Pressure and SystemicOxygenationAs reviewed earlier, blood oxygen satu-ration should remain at greater than90% throughout the critical care of apatient with severe TBI. In addition,arterial blood sampling must be donefrequently to maintain a PaO2 greater
KEY POINT
h Very elaborate yet clearguidelines for the criticalcare management ofa patient with severeTBI are endorsedby the Brain TraumaFoundation. The mainprinciples of therapy areto ensure adequatecerebral perfusion andoxygenation while brainswelling and injuryimprove.
Case 2-1A 24-year-old man was found after his car struck a tree. He wasunconscious with no visible external injury. Emergency medical serviceswas called and arrived in 3 minutes. On arrival, paramedics extricated himfrom the car and stabilized his neck and spine. His airway was assessedas inadequate, his blood pressure was 80/40 mm Hg, his pulse rate was110 beats/min, and pulse oximetry was 80%. His pupils were asymmetric;the left was 5 mm and unreactive and the right was 3 mm and reactive.He was intubated at the scene and given IV fluids and 100% oxygen. Hewas mildly hyperventilated en route to the nearest trauma center.
Comment. This patient has a severe traumatic brain injury. He has aninadequately secured airway and is hypotensive and hypoxic, all of whichneed to be treated emergently on the scene. He also has signs of cerebralherniation as evidenced by a dilated and fixed pupil. He should havemild hyperventilation to reverse herniation until arrival at the hospital.
537Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

than 60 mm Hg. Systolic blood pressuremust be maintained above 90 mm Hg.Hypotonic and dextrose-containing IVfluids should not be used.
Intracranial PressureICP can be measured either by an intra-ventricular device (external ventriculardrain connected to an external straingauge transducer) or by an intraparen-chymal probe (strain gauge or fiber-optic). The latter can be either tunneledor placed via a cranial bolt.
A sustained ICP greater than 20 mmHg is considered harmful and is associ-ated with poor outcome.18 Higher ICPcauses secondary ischemia to the brain.ICP-directed therapy should be used tomaintain ICP less than 20 mm Hg.
TBI guidelines recommend that ICPbe monitored in all patients with a se-vere TBI (GCS score less than 9) and an
abnormal CT scan of the brain (Level IIrecommendation). An abnormal scan isdefined as one with hematoma, contu-sion, swelling, herniation, or effacedbasal cisterns. ICP monitoring is also in-dicated in patients with a normal CTscan of the brain and GCS score lessthan 9 if they have two of the followingthree characteristics: age older than 40years, motor posturing, or systolic bloodpressure less than 90 mm Hg.
Cerebral Perfusion PressureCPP is derived from MAP and ICP. CPPequals MAP minus ICP. It can only bedetermined when ICP measurementis also being performed. The currentguideline recommendation is to use ICP-and CPP-guided therapy, as illustratedin Case 2-2A.
A CPP less than 50 mm Hg is as-sociated with poor outcome even if it
KEY POINT
h A sustained ICP greaterthan 20 mm Hg isconsidered harmful andis associated with pooroutcome. Higher ICPcauses secondaryischemia to the brain.ICP-directed therapyshould be used tomaintain ICP less than20 mm Hg.
Case 2-2AA 50-year-old man was admitted to the neurointensive care unit following amotor vehicle accident. His admission Glasgow Coma Scale (GCS) score was 5.His CT scan showed a skull fracture and a large epidural hematoma withcontralateral traumatic subarachnoidhemorrhage (Figure 2-3). He had noextracranial injuries. He had beenadequately resuscitated and wasnormotensive and normoxic. Theepidural hematoma was operatedon and removed. The patientremained comatose with a GCSscore of 5. An intracranial pressure(ICP) monitor was placed, and theICP was 24 mm Hg and the cerebralperfusion pressure (CPP) was48 mm Hg.
Comment. This is an example ofa patient with a severe traumaticbrain injury who presented withan intracranial lesion, intracranialhypertension, and a poor GCSscore. Such a patient requires ICPand CPP monitoring. If possible,brain oxygenation should alsobe monitored.
FIGURE 2-3 Patient with right-sideskull fracture, epiduralhematoma, and
contralateral traumatic subarachnoidhemorrhage.
538 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

occurs only periodically.19 The ischemicthreshold seems to lie below a CPP of50 mm Hg. However, in patents withpoor cerebral autoregulatory function,a lower CPP of 50 mm Hg to 60 mm Hgis advised and tolerated because of ahigher blood flow at the same CPP. Inpatients with intact or minimally dis-turbed autoregulation, a slightly higherCPP of 60 mm Hg to 70 mm Hg is rec-ommended. Overall goal for CPP shouldbe 50 mm Hg to 70 mm Hg.
Brain OxygenationTwo different methods are commonlyused to measure brain oxygenation.Jugular oximetry is a global measure ofcerebral oxygen consumption and ex-traction. It is measured by samplingblood from a catheter in the internaljugular vein, positioned cranially to thedrainage of the facial vein. It serves as agood monitoring marker for hyperventi-lation. Maintaining the catheter in anappropriate position is technically diffi-cult, which has led to its falling out offavor in clinical practice. When donevigorously, hyperventilation leads to se-vere vasoconstriction and ischemia andis manifested by low jugular venoussaturation (less than 50%). Brain tissueoximetry is a focal measurement (13mm2) of oxygen tension and is used asa marker for cerebral hypoxia. This ismeasured via a microprobe in the brainparenchyma and can be tunneled orinserted via a bolt. The measurementis in a small focal brain volume andmay not detect events in regions re-moved from the probe. A drift mayoccur over longer periods of monitor-ing (more than 7 days) and at highertemperatures.
Per TBI guidelines, there is only aLevel III recommendation regardingmonitoring and thresholds for jugularvenous saturation and brain tissue oxy-genation, with critical low thresholds of50% and 15 mm Hg, respectively. More
recent studies, however, suggest thattherapy that includes a brain oximetrytarget greater than 20 mm Hg, in ad-dition to recommended ICP and CPPtargets, improves outcomes.20 A ran-domized controlled clinical trial (theBOOST 2 trial) is underway to examinethe benefit of ICP-, CPP- and oximetry-directed therapy (http://clinicaltrials.gov/ct2/show/NCT00974259).
Cerebral MicrodialysisMicrodialysis is a technique ofmeasuringbrain metabolism. It is done by placing acatheter with a filtration membrane atthe tip into the brain parenchyma. Usingdialysis technology, artificial CSF is per-fused through the catheter and intersti-tial solutes are dialyzed out in microlitervolumes. These solutes are then ana-lyzed using an online high-performanceliquid chromatography technique. Inter-stitial concentrations of lactate, pyruvate,glucose, glutamate, and glycerol are ob-tained. The most common values ana-lyzed are the ratio between lactate andpyruvate (L/P ratio) and the ratio be-tween lactate and glucose (L/G ratio).These ratios provide insight into cere-bral energy metabolism, albeit focal, andprovide an understanding of the patho-physiology of ongoing secondary injuryto the brain. The L/P ratio indicates thebalance between aerobic and anaerobicmetabolism. Glucose levels signifyadequate substrate delivery, and thetrends of these values are frequentlymore important than the values them-selves. Abnormal levels of lactate andpyruvate and abnormal L/P and L/Gratios are indicative of both ischemicand nonischemicmetabolic stress. Whilethese values are directly proportional,pyruvate is inversely related to the extentof metabolic disorder. Further, patho-logic values that are refractory to ther-apeutic maneuvers are likely due tomitochondrial injury or substrate diffu-sion gradient due to edema.
KEY POINT
h A cerebral perfusionpressure less than50 mm Hg is associatedwith poor outcomeeven if it occurs onlyperiodically. Overall goalfor cerebral perfusionpressure should be50 mm Hg to 70 mmHg.
539Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

The threshold for critical metabolicdisorder is thought to be an L/P ratio of25 to 40. A recent study shows that anL/P ratio greater than 25 is correlatedwith unfavorable outcome or death.21
The probe is most commonly placedin the frontal lobe on the nondominantside and is assessed on CT by visualizingits gold tip, which is radio-opaque. It isconsidered to be perilesional if the tip iswithin 0.5 cm to 1.5 cmof a radiographiclesion, or in normal brain if it is greaterthan 1.5 cm away. Perilesional valuestend to be higher than those in normalbrain.22 Just like brain oximetry, themicrodialysis measurement is also focaland may miss ischemia distant from theprobe location. No prospective ran-domized trials have evaluated the roleof microdialysis in affecting patientoutcomes, likely because few patientsundergo this monitoring and the patientgroups are heterogeneous. However, anInternational Consensus statement doesrecommend the use of microdialysis inthe management of patients with severeTBI.23
Continuous EEGThe risk of early posttraumatic seizuresranges between 10% and 20%. In pa-tients with depressed skull fractures orpenetrating injury, continuous EEGmaybe useful to screen for subclinical sei-zures. Many different epileptiform dis-charges are seen in patients with TBI,and they precede actual seizures.9
TREATMENT OF SEVERETRAUMATIC BRAIN INJURYAs discussed above, the aims of ICUtherapy of severe TBI are to maintainadequate cerebral perfusion by target-ing ICP and CPP. In addition, therapiesshould be instituted to avoid cerebralhypoxia. In one study, patients whoresponded to ICP-lowering therapy hada 64% lower risk of death at 2 weeks.24
The target value for ICP is less than 20
mm Hg, for CPP is 50 mm Hg to 70mm Hg, and for brain oxygenation isgreater than 15 mm Hg.
Therapies to Lower IntracranialPressureHead end elevation. The head of thebed should be elevated 30 to 45 degrees.This maximizes cerebral venous drain-age via jugular veins. However, the pa-tient should be inclined only if the spinehas been deemed stable. Inclination alsohelps reduce the incidence of ventilator-associated pneumonia.
Ventriculostomy. Insertion of a ven-triculostomy drain can be done in thetrauma bay of the emergency depart-ment, in the operating room, or at thebedside in the ICU. CSF drainage re-duces intracranial volume and thus pres-sure. An external ventricular drain mayalso be used for ICP measurement byconnecting it to an external transducersetup. This transducer must be zeroedat the level of the pinna, which corre-sponds to the level of the foramen ofMonro. The drainage circuit must re-main closed at all times, as it is in directcommunication with the intracranialcavity. Routine CSF sampling is notnecessary because it increases risk ofinfection. CSF sampling should be doneonly in the presence of fevers orelevated white blood cell count or ifinfection is suspected. Ventriculitis istreated by drain replacement, systemicantibiotics, and, on occasion, intrathecalantibiotics. If intrathecal antibiotics areadministered, they must be speciallyprepared for intrathecal use and con-tain no preservatives, as these can causechemical meningitis.
Hyperosmolar therapy. A dose of1 g/kg to 1.5 g/kg of 20% mannitol maybe administered for cerebral herniationor raised ICP, and doses may be re-peated if required. Mannitol should begiven only in the setting of raised ICP orherniation, as prophylactic therapy with
KEY POINT
h Patients with severetraumatic brain injuryhave improved outcomeswhen cared forin a specializedneurointensive care unit.Per guidelines,intracranial pressure andcerebral perfusionpressure should bemonitored and treated ifthey are abnormal.Brain oxygenation,microdialysis, and EEGare other modalities usedto monitor brain injuryand can help directtherapies that improveoutcomes.
540 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

mannitol is of little benefit because ofthe risk of hypovolemia and hypoten-sion. Hypertonic saline (HTS) may alsobe used and is available in concentra-tions ranging from 2% to 23.4%. Both ofthese osmotic agents work by increasingcapillary perfusion by improving redblood cell rheology, augmenting cardiacoutput, causing water shifts from braintissue, and improving laminar capillaryflow by dehydrating endothelial cells.The effects of mannitol are typicallyshorter than those of HTS. A single 30mL dose of 23.4% HTS has been shownto rapidly reverse transtentorial hernia-tion.25 HTS also improves elevated ICPthat is refractory to mannitol by im-proving cerebral oxygenation and hemo-dynamics.26 Whereas mannitol carriesthe risk of renal failure, HTS mayprecipitate pulmonary edema. Serumosmolality and sodium must be checkedfrequently, and hyperosmotics can beused with ICP spikes to maximal serumosmolality of 330 mOsm/kg (mannitol)or serum sodium 160 mEq/L (HTS).27
Sedation and analgesia. Analgesiais essential to prevent a rise in ICP dur-ing stimulation, movement, and nursingprocedures such as endotracheal suc-tioning. In patients with severe intra-cranial hypertension, these procedurescan provoke a sustained ICP crisis.Concomitant use of analgesia and seda-tion also reduces the total dose of seda-tive required. The preferred analgesicsare opiates.
Sedation provides anxiolysis, agita-tion control, and hypnosis and improvescerebral physiology. It lowers cerebralmetabolic rate and thereby CBF becauseof flow-metabolism coupling. The re-duction in CBF reduces ICP. Propofoland benzodiazepines such as midazo-lam preserve flow-metabolism couplingand are therefore desirable. Inhaled an-esthetic agents do not maintain flow-metabolism coupling and are thereforeless favored. Most sedative agents cause
hypotension. In addition, the risk ofpropofol infusion syndrome and hyper-triglyceridemia must be kept in mind.Sedation must be ‘‘titrated to effect’’for ICP control, and prophylactic burstsuppression with any agent is notadvisable.
Hyperventilation. Hyperventilationcauses hypocarbia and vasoconstriction,which reduce CBF and therefore cere-bral blood volume. There is a positivelinear relationship between arterial car-bon dioxide and CBF between a PaCO2of 20 mm Hg to 80 mm Hg. However,below the threshold of a PCO2 of 28 mmHg, severe vasoconstriction results in adecrease in CBF to ischemic levels inthe brain. The target for mild hyper-ventilation is a PaCO2 of 32 mm Hg to 36mm Hg and for moderate hyperventila-tion is 28 mm Hg to 32 mm Hg. Con-tinuous monitoring of end-tidal carbondioxide is essential to ensure regulatedhypocarbia. Alternately, jugular venoussaturations or brain tissue oxygenationmust be monitored to avoid cerebralhypoxia and ischemia. Hyperventilationmust be avoided in the first 24 hoursafter a severe TBI as the brain is hy-permetabolic and CBF is depressed inrelation to metabolic rate. Vasocon-striction in this time period causesischemia.28 However, transient hyper-ventilation is an excellent tool to re-duce ICP in emergent situations, suchas a herniation syndrome, while othertherapies to lower ICP are being imple-mented. Hyperventilation should notbe used prophylactically as it increasesthe ischemic burden of the brain.7
Muscle relaxation. It is important tomaintain a constant PaCO2 because of itseffect on ICP. Muscle relaxants may beneeded for this purpose. This is espe-cially the case if hyperventilation needsto be maintained. Muscle relaxantsmay also be indicated if hypothermiaor controlled normothermia is imple-mented and causes shivering. When
KEY POINT
h Hyperventilation mustbe avoided in the first24 hours after a severeTBI as the brain ishypermetabolic and CBFis depressed in relationto metabolic rate.Vasoconstriction in thistime period causesischemia.
541Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

muscle relaxants are used, all feedingtubes must be postpyloric.
Hypothermia. Numerous trials havebeen conducted to evaluate the benefitof prophylactic hypothermia as a neuro-protective therapy in severe TBI. Thereappears to be a clear lack of benefit evenwhen hypothermia is administered veryearly in severe TBI.29 Hypothermia isbeneficial, however, in controlling highICP refractory to other therapies. Mildhypothermia to 35-C for more than 48hours effectively reduces high ICP andimproves outcome in such patients.30
Hypothermia can be induced and main-tained using surface cooling devices orIV cooling catheters. Hypothermiacauses shivering, immunosuppression,arrhythmias, cold diuresis, myocardialsuppression, hypokalemia, and increasedvasopressor requirement. Paralysis maybe required to control shivering. Re-warming must be done slowly at a rateof 1-C every 8 to 12 hours, and patientsshould be monitored for hyperkalemiaand vasodilatation.
Barbiturate coma. High-dose barbi-turates used to achieve EEG burst sup-pression are recommended to controlelevated ICP refractory to maximal med-ical and surgical therapy.27 Barbituratesmaintain flow-metabolism coupling (al-beit not very closely) and lower CBFand cerebral blood volume. They alsoacutely lower ICP and long-term ICPtrends. Patients with refractory increasedICP who do not respond to barbiturateshave a significantly higher mortality thanthose who respond. Hemodynamic sta-bility is essential before and during ther-apy because of the hypotension causedby barbiturates. Every effort must bemade to avoid systemic hypotension,which will further lower CPP. Pentobarbi-tal is the most common agent used. Aftera bolus of 10 mg/kg given over 60 min-utes, the dose is maintained at 1 mg/kg/hto 5 mg/kg/h to achieve burst suppres-sion (3 to 6 bursts per minute). Con-
tinuous EEG monitoring is essential tomonitor burst suppression. The mor-bidity of high-dose barbiturates is highbecause of the immunosuppression,myocardial suppression, and hypoten-sive effects.
Decompressive craniectomy. Stud-ies illustrate improvement in ICP aftercraniectomy,31 and retrospective studiessuggest favorable outcomes after de-compressive craniectomy.32 However,the recently published DecompressiveCraniectomy in Diffuse TBI (DECRA)trial concluded that early bifrontotem-poroparietal decompressive craniectomylowered ICP and length of stay in theICU but increased mortality.33 In thisstudy, however, all patients who had sur-gical removal of a mass lesion wereexcluded, and patients underwent de-compressive craniectomy without max-imal medical therapy. Another clinicaltrial, called Randomised Evaluation ofSurgery with Craniectomy for Uncontrol-lable Elevation of Intra-Cranial Pressure(RESCUEicp), is underway and random-izes patients to receive either barbituratetherapy or decompressive craniectomyas the last step in management of in-tracranial hypertension (www.rescueicp.com). The results of this trial are eagerlyawaited. Therefore, while no random-ized controlled trials supporting theuse of craniectomy in TBI in adults havebeen reported, nonrandomized trialsusing historic controls suggest it is bene-ficial when maximal medical therapy hasfailed. This is illustrated in Case 2-2B.
Therapies to Increase CerebralPerfusion PressureLowering intracranial pressure. Themost common cause of low CPP is a highICP, and lowering ICP often increasesCPP. However, sometimes the cause ofsuboptimal CPP is systemic hypotensionor hypovolemia.
Fluids. Hypotonic and dextrose-containing fluids must not be used.
KEY POINT
h Intracranial pressureshould be maintained atless than 20 mm Hg.This can be done usingsedation, analgesia,CSF drainage, mildhyperventilation,hypothermia, barbituratecoma, anddecompressivecraniectomy. Each ofthese therapeuticmodalities has adverseeffects of which thephysician should beaware.
542 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Isotonic or hypertonic fluids are effectivefor resuscitating patients with severe TBIand shock. Colloids may also be used,although theymust be given in judiciousquantities to avoid a coagulopathy.
Vasopressors. After volume resusci-tation, a patient may still have a low CPP,necessitating use of a vasopressor. Nor-adrenaline has some beneficial effectsover dopamine. The former has a morepredictable and efficient augmentationof CPP and CBF as estimated by trans-cranial Doppler.34 Johnston and col-leagues35 demonstrated a reduction inoxygen extraction and a significant in-crease in brain tissue oxygenation whenCPP was augmented with noradrenaline.Caution must be exercised if vasopres-sin is used as it may cause cerebral va-sodilatation and increase in ICP.
Drugs. Sedatives, analgesics, and bar-biturates all cause hypotension, andtheir doses must be optimized to mini-mize systemic hypotension.
Optimal cerebral perfusion pressure.Optimal CPP is defined as the CPP atwhich autoregulation status is most in-tact in a patient. This is measured by plot-tingCPP against PRx. Patients treatedwithoptimal CPP have improved outcomes.36
Therapies to Increase BrainOxygenationLowering intracranial pressure. HighICP causes tissue hypoxia and is-
chemia. Lowering ICP increases tissueoxygenation.
Increasing cerebral perfusionpressure. Low CPP also causes tissueischemia and hypoxia. A trial of increasein CPP must be done to examinewhether cerebral hypoxia is responsiveto perfusion pressures. This may requirethe use of a vasopressor.
Increasing fraction of inspiredoxygen. Increase in inspired oxygen in-creases blood oxygen content and deliv-ery to tissue at risk.
Hematocrit. Blood transfusion in-creases the oxygen-carrying capacity anddelivery to brain tissue.37 No definedhemoglobin target exists.
Hypertonic saline. In patients withICP refractory tomannitol, HTS increasesbrain oxygenation by improving capillaryperfusion and CBF.26 Boluses of 250 mLof 7.5% HTS may be given.
Management of Other CriticalCare IssuesSeizure prophylaxis. Early seizurescause metabolic stress and acute in-creases in ICP. Left untreated, seizurescan cause hippocampal atrophy.38 Whileguidelines do not recommend routineseizure prophylaxis to prevent late-onsetposttraumatic epilepsy, if a patient is athigh risk for early seizures (eg, has apenetrating TBI, depressed skull frac-ture, cortical contusion, SDH, or EDH),
KEY POINTS
h Cerebral perfusionpressure should bemaintained at 50 mmHg to 70 mm Hg.Normovolemia isessential andoccasionally inducedhypertension may berequired.
h Brain oxygenation ofless than 20 mm Hgshould be avoided andmay be treated withhyperoxia, increasedcerebral perfusionpressure, or bloodtransfusion.
Case 2-2BThe patient presented in Case 2-2A was treated with sedation and 80 g ofmannitol. His ICP decreased to 12 mm Hg and his CPP rose to 60 mm Hg.Over the next few days, however, he required frequent hypertonic salineboluses and mild hyperventilation to a Paco2 of 32 mm Hg. His serumsodium was 155 mEq/L. Because his ICP remained above 20 mm Hg,hypothermia (to 35-C) was initiated, and thereafter he underwent aright-sided hemicraniectomy. Following the hemicraniectomy, his ICP wascontrolled and his neurologic examination started to improve after 10 days.
Comment. This patient experienced significant secondary injury andedema, which produced refractory intracranial hypertension requiringmaximal medical and surgical therapy.
543Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

antiepileptics should be used for 7 days.Levetiracetam or phenytoin may beused in usual doses with cost-utilityanalysis favoring phenytoin.
Thromboprophylaxis. TBI is anindependent risk factor for deep veinthrombosis. The risk of developing adeep vein thrombosis in the absence ofthromboprophylaxis is estimated to be20%, with an incidence of 0.38% forpulmonary embolism. Mechanical meth-ods such as compression stockings orpneumatic compression stockingsshould be initiated early unless injury tolower extremities precludes their use.No reliable recommendation existsregarding when to begin pharmacologicprophylaxis. Generally, this may bestarted once sequential CT of the brainshows no further evolution of hemor-rhage and at least 24 hours have elapsedsince the last neurosurgical intervention.
Nutrition. Patients often experiencea systemic and cerebral hypermetabolicstate after severe TBI, which may berelated to a stress response. Patients notfed in the first 7 days have a fourfoldincrease in mortality at the end of 2weeks. Patients given early nutritionhave lower mortality and 55% lowerinfection rates. Current guidelines rec-ommend nutrition at 140% of restingrequirement in nonparalyzed patientsand at 100% in paralyzed patients. Asstated earlier, feeding tubes must bepostpyloric in all patients receiving par-alytic agents.
Glycemic control. While strict gly-cemic control is recommended, its as-sociation with hypoglycemic episodeshas been increasingly recognized. Theneurologic outcomes among patientswith strict control (less than 110 mg/dL)and conventional control (less than 180mg/dL) are no different.39 Moreover, ce-rebral microdialysis reveals increasedepisodes of cerebral hypoglycemia withstrict control.40 This deserves furtherstudy.
Steroids. Steroids have no role in thetreatment of acute TBI.
Tracheostomy. Early tracheostomyreduces days on ventilator but does notreduce ventilator-associated pneumo-nias or mortality.
Endocrine abnormalities. A com-mon neuroendocrine abnormality ishypopituitarism, most commonly mani-festing as increased vasopressor require-ment or cerebral salt wasting. Thiscan be treated in the acute phase withreplacement-dose hydrocortisone or flu-drocortisone. Diabetes insipidus mustbe managed aggressively to avoid highserum sodium. Once hypernatremia ispresent, serum sodium should be low-ered gradually so as not to worsen orcause malignant rebound cerebraledema.
OUTCOMESThe major predictors of outcome aftersevere TBI are GCS score after full re-suscitation, age, pupillary reactivity, CTfindings, and presence of major extrac-ranial injury.41 The GCS has a 70% pre-dictive value. Patients with lower GCSscores have a higher probability of pooroutcomes. Only up to 20% of patientswith a GCS score of 3 will survive.Mortality and outcome worsen withincreasing age. Above 60 years, pooroutcome increases dramatically. Bilateralunreactive pupils predict poor outcomeand, when present, are the strongestpredictor. Dilated pupils (greater than 4mm) are also a poor prognostic in-dicator. The following CT findings areassociated with poor outcome: com-pressed or absent basal cisterns, tSAH,midline shift, and intracranial lesions.
A web-based outcome predictionmodel is available at the CRASH2website(crash2.lshtm.ac.uk/Risk%20calculator/index.html).41 Adherence to formulatedguidelines improves outcomes and de-creases hospital expenses.42 Having aguideline-driven institutional ICP-CPP
KEY POINTS
h Bilateral unreactivepupils predict pooroutcome and, whenpresent, are thestrongest predictor.
h Age, Glasgow ComaScale score, pupillaryreaction, and CTfindings are predictorsof outcome after severetraumatic brain injury.
544 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

protocol helps around-the-clock care ofthe patient and decreases subjective var-iations in care.
REFERENCES1. Centers for Disease Control and Prevention.
Web-based injury statistics query andreporting system (WISQARS). www.cdc.gov/injury/wisqars. Accessed December 2, 2011.
2. Faul M, Xu L, Wald MM, Coronado VG.Traumatic brain injury in the United States:emergency department visits, hospitalizations,and deaths. Atlanta: Centers for DiseaseControl and Prevention, National Center forInjury Prevention and Control, 2010.
3. Menon DK, Schwab K, Wright DW, et al;Demographics and Clinical AssessmentWorking Group of the International andInteragency Initiative toward Common DataElements for Research on Traumatic BrainInjury and Psychological Health. Positionstatement: definition of traumatic braininjury. Arch Phys Med Rehabil 2010;91(11):1637Y1640.
4. Finkelstein EA, Corso PS, Miller TR. Theincidence and economic burden of injuriesin the United States. New York: OxfordUniversity Press, 2006.
5. Brunicardi FC, Andersen DK, Billiar TR, et al,editors. Schwartz’s principles of surgery.9th ed. New York, NY: McGraw-HillProfessional, 2009.
6. Rosenthal G, Sanchez-Mejia RO, Phan N,et al. Incorporating a parenchymal thermaldiffusion cerebral blood flow probe inbedside assessment of cerebralautoregulation and vasoreactivity inpatients with severe traumatic brain injury.J Neurosurg 2011;114(1):62Y70.
7. Coles JP, Fryer TD, Smielewski P, et al.Defining ischemic burden after traumaticbrain injury using 15O PET imaging ofcerebral physiology. J Cereb Blood FlowMetab 2004;24(2):191Y201.
8. Hiler M, Czosnyka M, Hutchinson P, et al.Predictive value of initial computerizedtomography scan, intracranial pressure, andstate of autoregulation in patients withtraumatic brain injury. J Neurosurg 2006;104(5):731Y737.
9. Ronne-Engstrom E, Winkler T. ContinuousEEG monitoring in patients with traumaticbrain injury reveals a high incidence ofepileptiform activity. Acta Neurol Scand2006;114(1):47Y53.
10. Hartings JA, Watanabe T, Bullock MR, et al.
Spreading depolarizations have prolongeddirect current shifts and are associated withpoor outcome in brain trauma. Brain 2011;134(pt 5):1529Y1540.
11. Jeannett B, Teasdale G, Braakman R, et al.Predicting outcome in individual patientsafter severe head injury. Lancet 1976;15(7968):1031Y1034.
12. Hartl R, Gerber LM, Iacono L, et al. Directtransport within an organized state traumasystem reduces mortality in patients withsevere traumatic brain injury. J Trauma2006;60(6):1250Y1256; discussion 1256.
13. Badjatia N, Carney N, Crocco TJ, et al; BrainTrauma Foundation; BTF Center forGuidelines Management. Guidelines forprehospital management of traumatic braininjury 2nd edition. Prehosp Emerg Care2008;12(suppl 1):S1YS52.
14. Chesnut RM, Marshall LF, Klauber MR, et al.The role of secondary brain injury indetermining outcome from severe headinjury. J Trauma 1993;34(2):216Y222.
15. Stocchetti N, Furlan A, Volta F. Hypoxemiaand arterial hypotension at the accidentscene in head injury. J Trauma 1996;40(5):764Y767.
16. Patel HC, Menon DK, Tebbs S, et al.Specialist neurocritical care and outcomefrom head injury. Intensive Care Med 2002;28(5):547Y553.
17. Brain Trauma Foundation, AmericanAssociation of Neurological Surgeons,Congress of Neurological Surgeons.Guidelines for the management of severetraumatic brain injury [erratum publishedin J Neurotrauma 2008;25(3):276Y278].J Neurotrauma 2007;24(suppl 1):S1YS106.
18. Marmarou A, Anderson RL, Ward JD. Impactof ICP instability and hypotension onoutcome in patients with severe headtrauma. J Neurosurg 1991;75:S59YS66.
19. Stein DM, Hu PF, Brenner M, et al. Briefepisodes of intracranial hypertension andcerebral hypoperfusion are associated withpoor functional outcome after severetraumatic brain injury. J Trauma 2011;71(12):364Y373; discussion 373Y374.
20. Spiotta A, Stiefel MF, Gracias VH, et al.Brain tissue oxygen-directed managementand outcome in patients with severetraumatic brain injury. J Neurosurg 2010;113(3):571Y580.
21. Timofeev I, Carpenter KLH, Nortje J, et al.Cerebral extracellular chemistry andoutcome following traumatic brain injury: amicrodialysis study of 223 patients. Brain2011;134(pt 2):484Y494.
545Continuum Lifelong Learning Neurol 2012;18(3):532–546 www.aan.com/continuum
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

22. Timofeev I, Czosnyka M, Carpenter KLH,et al. Interaction between brain chemistryand physiology after traumatic brain injury:impact of autoregulation and microdialysiscatheter location. J Neurotrauma 2011;28(6):849Y860.
23. Bellander BM, Cantais E, Enblad P, et al.Consensus meeting on microdialysis inneurointensive care. Intensive Care Med2004;30(12):2166Y2169.
24. Farahvar A, Gerber LM, Chiu Y-L, et al.Response to intracranial hypertensiontreatment as a predictor of death in patientswith severe traumatic brain injury.J Neurosurg 2011;114(5):1471Y1478.
25. KoenigMA, BryanM, Lewin JL, et al. Reversalof transtentorial herniation with hypertonicsaline. Neurology 2008;70(13):1023Y1029.
26. Oddo M, Levine JM, Frangos S, et al. Effectof mannitol and hypertonic saline oncerebral oxygenation in patients with severetraumatic brain injury and refractoryintracranial hypertension. J NeurolNeurosurg Psychiatry 2009;80(8):916Y920.
27. Marshall GT, James RF, Landman MP, et al.Pentobarbital coma for refractory intra-cranialhypertension after severe traumatic braininjury: mortality predictions and one-yearoutcomes in 55 patients. J Trauma 2010;69(2):275Y283.
28. Coles JP, Minhas PS, Fryer TD, et al. Effect ofhyperventilation on cerebral blood flow intraumatic head injury: clinical relevance andmonitoring correlates. Crit Care Med 2002;30(9):1950Y1959.
29. Clifton GL, Valadka A, Zygun D, et al. Veryearly hypothermia induction in patients withsevere brain injury (the National Acute BrainInjury Study: Hypothermia II): a randomisedtrial. Lancet Neurol 2011;10(2):131Y139.
30. Jiang JY, Xu W, Li WP, et al. Effect oflong-term mild hypothermia or short-termmild hypothermia on outcome of patientswith severe traumatic brain injury. J CerebBlood Flow Metab 2006;26(6):771Y776.
31. Weiner GM, Lacey MR, Mackenzie L, et al.Decompressive craniectomy for elevatedintracranial pressure and its effect on thecumulative ischemic burden and therapeuticintensity levels after severe traumatic braininjury. Neurosurgery 2010;66(6):1111Y1118;discussion 1118Y1119.
32. Williams RF, Magnotti LJ, Croce MA, et al.Impact of decompressive craniectomy on
functional outcome after severe traumaticbrain injury. J Trauma 2009;66(6):1570Y1574;discussion 1574Y1576.
33. Cooper DJ, Rosenfeld JV, Murray L, et al.Decompressive craniectomy in diffusetraumatic brain injury. N Engl J Med 2011;364(16):1493Y1502.
34. Steiner LA, Johnston AJ, Czosnyka M, et al.Direct comparison of cerebrovascular effectsof norepinephrine and dopamine inhead-injured patients. Crit Care Med 2004;32(4):1049Y1054.
35. Johnston AJ, Steiner LA, Chatfield DA, et al.Effect of cerebral perfusion pressureaugmentation with dopamine andnorepinephrine on global and focal brainoxygenation after traumatic brain injury.Intensive Care Med 2004;30(5):791Y797.
36. Steiner LA, Czosnyka M, Piechnik SK, et al.Continuous monitoring of cerebrovascularpressure reactivity allows determination ofoptimal cerebral perfusion pressure inpatients with traumatic brain injury. CritCare Med 2002;30(4):733Y738.
37. Zygun DA, Nortje J, Hutchinson PJ, et al.The effect of red blood cell transfusion oncerebral oxygenation and metabolism aftersevere traumatic brain injury. Crit CareMed 2009;37(3):1074Y1078.
38. Vespa PM, McArthur DL, Xu Y, et al.Nonconvulsive seizures after traumatic braininjury are associated with hippocampalatrophy. Neurology 2010;75(9):792Y798.
39. Coester A, Neumann CR, Schmidt MI.Intensive insulin therapy in severe traumaticbrain injury: a randomized trial. J Trauma2010;68(4):904Y911.
40. Oddo M, Schmidt JM, Carrera E, et al.Impact of tight glycemic control on cerebralglucose metabolism after severe braininjury: a microdialysis study. Crit Care Med2008;36(12):3233Y3238.
41. MRC CRASH Trial Collaborators; Perel P,Arango M, Clayton T, et al. Predictingoutcome after traumatic brain injury:practical prognostic models based on largecohort of international patients. BMJ2008;336(7641):425Y429.
42. Fakhry SM, Trask AL, Waller MA, et al.Management of brain-injured patients by anevidence-based medicine protocol improvesoutcomes and decreases hospital charges.J Trauma 2004;56(3):492Y499; discussion499Y500.
546 www.aan.com/continuum June 2012
Traumatic Brain Injury
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.