l’arrêt cardiaque du domicile à la rééducation - · pdf...
TRANSCRIPT

L’arre ̂t cardiaque du domicile à la rééducation
Alain Cariou Intensive Care Unit -
Cochin HospitalParis Descartes University –
INSERM U970

ARRET CARDIAQUE : 1 VIE = 3 GESTES


Magnitude of SCA in the US
• US Census Bureau. Statistical Abstract of the United States: 2001• American Cancer Society, Inc., Surveillance Research, Cancer Facts and Figures 2001• 2002 Heart and Strokes Statistical Update, American Heart Association• Circulation 2001; 104: 2158-2163
Comparison of published VF OHCA survival percentages in various US cities before (white bars) and after (black bars) an EMS–based early defibrillation program was instituted

Scope of the problem
0 50 000 100 000 150 000 200 000
Cardiac Arrest Survivors
Traumatic Brain Injury
Minimally Conscious State
Persistent Vegetative State
New cases/yr in the US
Thurman D et al. JAMA 1999Engdahl et al. Resuscitation 2002

Hospital period
1.
Post cardiac arrest shock
2.
Brain injuries
50,000 sudden deaths / year
15,000 CPR attempts
5,000 ROSC…
… and hospitalized
3,000 survivors
1000-15OO without severe sequellae
Prognosis after cardiac arrest

Gueugniaud PY et al. NEJM 2008
0 20 40 60 80 100
1-year survival
Hospital discharge
Hospital admission
ROSC
Randomized
Epinephrine only Combination treatment
Short-term survivors
Long-term survivors

Immediate
Early
Intermediate
Recovery
Rehabilitation
PhaseROSC
20 min
6-12 hours
72 hours
Discharge
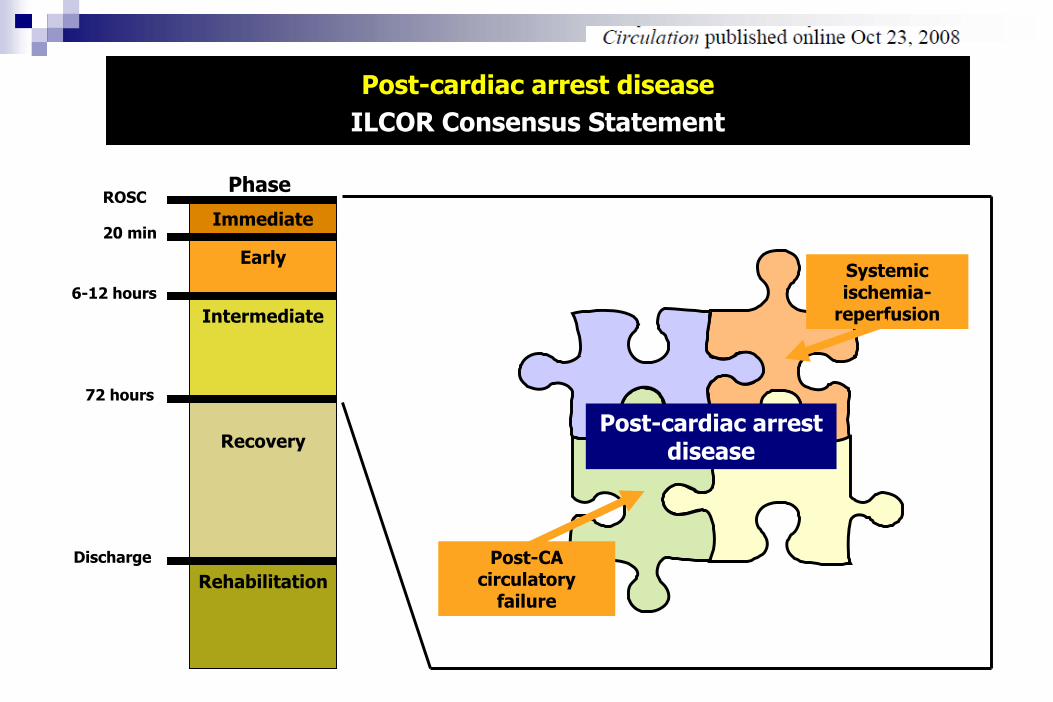
Post-cardiac arrest diseaseILCOR Consensus Statement
Post-cardiac arrest disease
Systemicischemia-
reperfusion

Ischemia-reperfusion (simplified)
JNK/SAPK
MAPKs
Pro-death Activity
RTK
Ras
Raf
MAPK
ERK
Pro-SurvivalActivity
PLCgPI3-K
PKC
GrowthFactors Stress Signals
PKB
PCD Hour to Days
O2 = killer
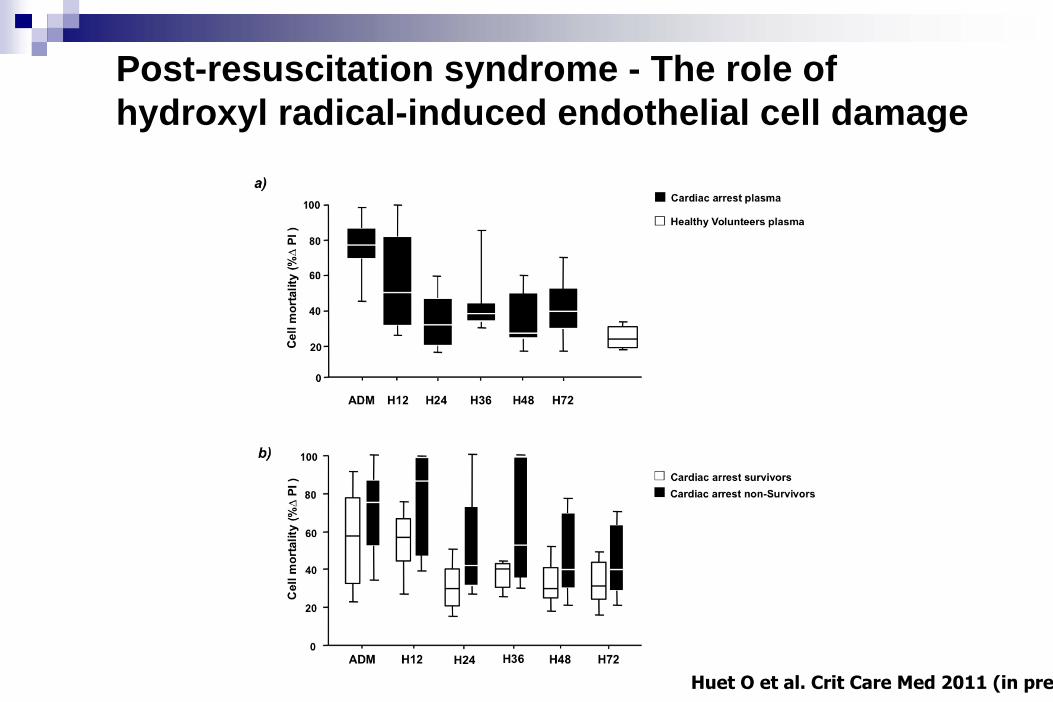
Post-resuscitation syndrome - The role of hydroxyl radical-induced endothelial cell damage
Huet O et al. Crit Care Med 2011 (in pre

Kilgannon JH et al. JAMA. 2010
Large US databasen=6326 post-CA pts
Exposed to Hypoxia<60 mmHgn=3999
Exposed to Normoxia
60-300 mmHgn=1171
Exposed to Hyperoxia>300 mmHgn=1156
Independant predictors of in-hospital mortality

1. Ischemia and reperfusion syndrome
2. Inflammatory response
3. Coagulopathy
4. Circulatory failure
5. Adrenal dysfunction
Current Opinion in Crit Care. 2004
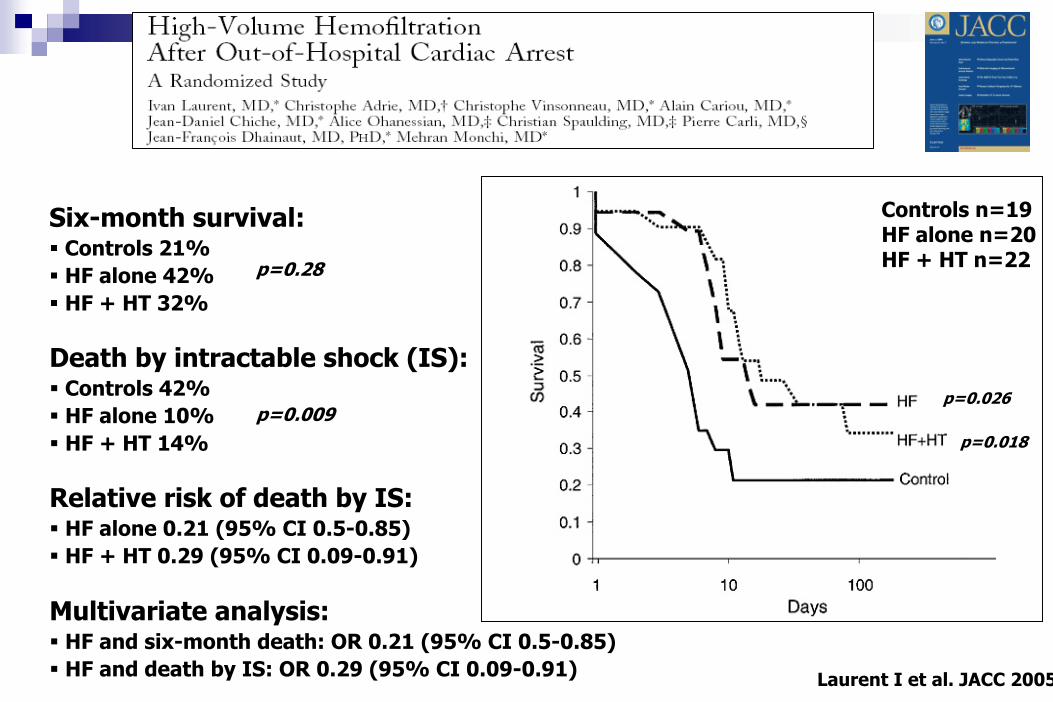
Six-month survival: Controls 21%HF alone 42%HF + HT 32%
Laurent I et al. JACC 2005
p=0.28
Death by intractable shock (IS): Controls 42%HF alone 10%HF + HT 14%
p=0.009p=0.026
p=0.018
Relative risk of death by IS: HF alone 0.21 (95% CI 0.5-0.85)HF + HT 0.29 (95% CI 0.09-0.91)
Controls n=19HF alone n=20HF + HT n=22
Multivariate analysis: HF and six-month death: OR 0.21 (95% CI 0.5-0.85)HF and death by IS: OR 0.29 (95% CI 0.09-0.91)
Recovery
RehabilitationDischarge
Post-cardiac arrest diseaseILCOR Consensus Statement
Post-cardiac arrest disease
Post-CA circulatory
failure
Immediate
Early
Intermediate
PhaseROSC
20 min
6-12 hours
72 hours
Systemicischemia-
reperfusion



Immediate
Early
Intermediate
Recovery
Rehabilitation
PhaseROSC
20 min
6-12 hours
72 hours
Discharge
Post-cardiac arrest diseaseILCOR Consensus Statement
Post-CA circulatory
failure
Post-cardiac arrest
Systemicischemia-
reperfusion
Persistent precipitating
pathology

Value of ECG abnormalities after cardiac arrest?
Should we restrict the use of immediate coronary angiogram …
to AMI with ST-segment elevation?

ICUN=714
ROSCN=1198
CPR attemptedN=3494
Out-of-hospital cardiac arrestN=6766
CPC 1/2N=160
Hospital discharge
N=174 (39%)
No obvious extra-cardiac cause of arrest
N=435
Admitted in ICUN=714
Jan. 2003 Nov. 2009Dumas F, Cariou A, Carli P, Spaulding A. Circ Cardiovasc Int 2
Should We Perform an Immediate Coronary Angiogram in All Survivors of OHCA With No Obvious Extra-Cardiac Cause? Insights from the PROCAT registry

Multivariate analysis of early predictors of survival in OHCA patients without obvious extra-cardiac etiology
0 1 2 3 4
BetterprognosisWorse prognosis
p‐value
ST segment elevation 0.778(0.60‐1.98)1.09
[95%
Conf.Interval]OR
BLS to ROSC > 15 minutes < 0.001(0.19‐0.55)0.28
Diabete mellitus 0.015(0.20‐0.84)0.42
Collapse to BLS >
5 minutes <0.001(0.17‐0.49)0.32
Age > 59 yrs 0.002(0.27‐0.75)0.45
Blood lactate <0.001(0.44‐0.70)0.55
Initial Arrest Rhythm: VT/VF 0.035(1.04‐3.19)1.82
Successfull PCI 0.013(1.16‐3.66)2.06
N=435
Should We Perform an Immediate Coronary Angiogram in All Survivors of OHCA With No Obvious Extra-Cardiac Cause? Insights from the PROCAT registry
Dumas F, Cariou A, Carli P, Spaulding A. Circ Cardiovasc Int 2

In patients with ROSC after cardiac arrest, does the routine use of PCI, compared with standard management (without PCI), improve outcomes (eg, survival, rearrest, etc)?
Treatment RecommendationIn OHCA patients with STEMI or new LBBB on ECG following ROSC, early angiography and PCI should be considered. It is reasonable to perform early angiography and PCI in selected patients despite the absence of ST-segment elevation on the ECG or prior clinical findings, such as chest pain, if coronary ischemia is considered the likely cause on clinical grounds. Out-of-hospital cardiac arrest patient are often initially comatose but this should not be a contraindication to consider immediate angiography and PCI. It may be reasonable to include cardiac catheterization in a standardized post– cardiac-arrest protocol as part of an overall strategy to improve neurologically intact survival in this patient group.

Immediate
Early
Intermediate
Recovery
Rehabilitation
PhaseROSC
20 min
6-12 hours
72 hours
Discharge
Post-cardiac arrest diseaseILCOR Consensus Statement
Post-cardiac arrest disease
Post-CA myocardial dysfunction
Systemicischemia-
reperfusion
Treatment targets
Post-anoxic brain injury
Persistent precipitating
pathology


« On the basis of the published evidence to date, the Advanced Life Support (ALS) Task Force of the
International Liaison Committee on Resuscitation (ILCOR) made the following recommendations in October
2002 :
• Unconscious adult patients with spontaneous circulation after out-of-hospital cardiac arrest should be cooled to 32°C to 34°C for 12 to 24 hours when the initial rhythm was ventricular fibrillation (VF)• Such cooling may also be beneficial for other rhythms or in-hospital cardiac arrest »
Therapeutic Hypothermia After Cardiac ArrestAn Advisory Statement by the Advanced Life Support Task Force of theInternational Liaison Committee on ResuscitationWriting GroupJ.P. Nolan, FRCA; P.T. Morley, MD; T.L. Vanden Hoek, MD; R.W. Hickey, MDMembers of the Advanced Life Support Task ForceW.G.J. Kloeck, MBBCh, DipPEC(SA), Chair; J. Billi, MD; B.W. Böttiger, MD; P.T. Morley, MD;J.P. Nolan, FRCA; K. Okada, MD; C. Reyes, MD; M. Shuster, MD, FRCPC; P.A. Steen, MD;M.H. Weil, MD, PhD; V. Wenzel, MDMember of the Pediatric Life Support Task ForceR.W. Hickey, MDAdditional ContributorsP. Carli, MD; T.L. Vanden Hoek, MD; D. Atkins, MD
Circulation. 2003;108:118-121

Quels patients ?
Hypothermie thérapeutique

VF studies

Effect of MTH in non shockable patients On 6 month mortality in randomized studies
On in-hospital mortality in non-randomized studies
Kim YM et al. Resuscitation 2011

Circulation 2011
Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Insights from a large registry.
F. Dumas, D. Grimaldi, B. Zuber, J. Fichet, J. Charpentier, F. Pene, O. Varenne, P. Carli, X. Jouven, JP. Empana, A. Cariou

VF/VT group
Circulation 2011
Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Insights from a large registry.
F. Dumas, D. Grimaldi, B. Zuber, J. Fichet, J. Charpentier, F. Pene, O. Varenne, P. Carli, X. Jouven, JP. Empana, A. Cariou

Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Insights from a large registry.
F. Dumas, D. Grimaldi, B. Zuber, J. Fichet, J. Charpentier, F. Pene, O. Varenne, P. Carli, X. Jouven, JP. Empana, A. Cariou
PEA/Asystole Group
X
Circulation 2011

Comment ?
Hypothermie thérapeutique


Méthodes de refroidissement
Méthodes Vitesse (°C/h)
Maintien de l’hypothermie
Utilisable pour réchauffement Surcoût
Couverture à
air froid Lent +/- +++ +
Packs de glace Lent ++ 0 0
Tunnel glacé 1.1 ++ 0 0
Casque réfrigérant 1.5 + 0 ++
Lit liquide froid circul. 1.5-3 +++ +++ ++
Bain froid 9.3 +++ 0 ?
Lit à
air refroidissant - ++ +++ ?
Perfusion sérum froid 0.6-2.5 0 0 +
KT endovasculaires 2 +++ +++ +++
CEC >4 +++ +++ +++

Circulation 2010
“Eighteen device-related adverse events (1 periorbital emphysema, 3 epistaxis, 1 perioral bleed, and 13 nasal discolorations) were reported.”

Quels problèmes ?
Hypothermie thérapeutique
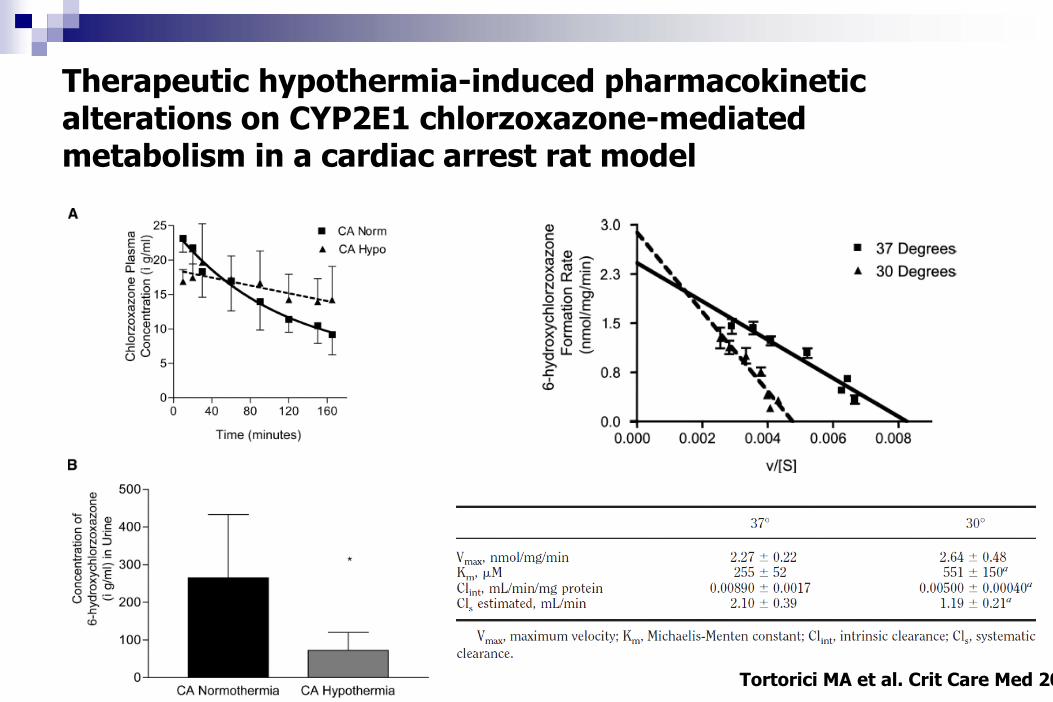
Therapeutic hypothermia-induced pharmacokinetic alterations on CYP2E1 chlorzoxazone-mediated metabolism in a cardiac arrest rat model
Tortorici MA
et al. Crit Care Med
20

85%
9%
3% 1% 1% 1%
Pneumonie n=318
Bactériémie n=35
Infection liée au cathéter n=11
Infection intra-abdominale n=5
Infection urinaire n=4
Sinusite n=3
281/421 patients (67%) ont développé un total de 373 épisodes infectieux:

Early onset pneumonia after cardiac arrest: characteristics, risk factors and influence on prognosis
Sébastien Perbet, Nicolas Mongardon, Florence Dumas, Cédric Bruel, Virginie Lemiale, Bruno Mourvillier, Pierre Carli, Olivier Varenne, Jean-Paul Mira, Michel Wolff, Alain Cariou.
Cohorte bicentrique de 641 patients500 (78%) patients traités par hypothermie419 (65%) pneumonies précoces
Am J Resp Crit Care Med 2011 (in press)
En analyse multivariée, un seul facteur de risque hypothermie thérapeutique
OR= 1,90 [IC95% 1,28-2,80]; p=0,001

Evaluation du pronostic : quels « outils » ?


Pronostic factor: SSEP
Zandbergen EGJ, et al., Lancet 1998:352:1808‐1812

NSE P S‐100
Zandbergen et al. Neurology 2006


PET-scan: resting brain metabolism
Healthy control Brain death Vegetative state
Laureys S, Nature Rev 2005;6:899-909


Immediate
Early
Intermediate
Recovery
Rehabilitation
PhaseROSC
20 min
6-12 hours
72 hours
Discharge
Post-cardiac arrest diseaseILCOR Consensus Statement
Que deviennent les «
survivants
»
?
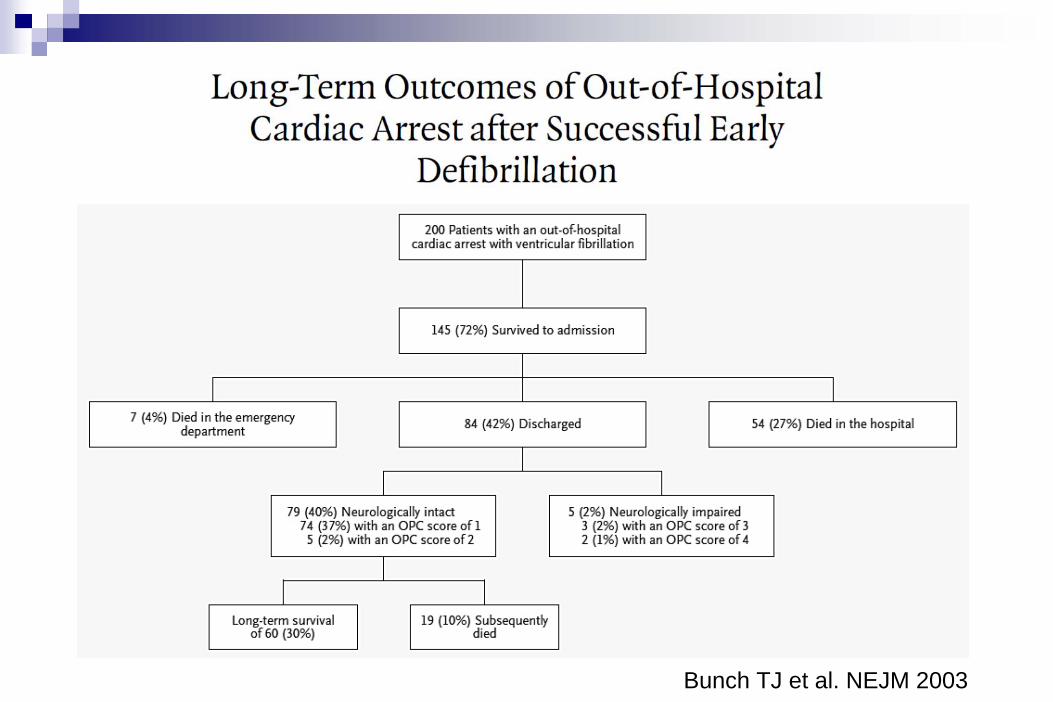
Bunch TJ et al. NEJM 2003

Bunch TJ et al. NEJM 2003
Mean length of follow-up was 4.8±3.0 years

Bunch TJ et al. NEJM 2003
« In summary, the rate of survival to hospital discharge was relatively high in a city that had a program of rapid defibrillation. The majority of survivorsreturned to work, and their quality of life was in most respects indistinguishable from that of the general population. The long-term survival rate was similar to that of age-, sex-, and disease- matched controls who did not have an OHCA. »



« The majority of studies concluded that the provision of resuscitation after cardiac arrest does provide patients
with a good quality of life after discharge from hospital »


NEJM 1997
The cumulative percentage of patients with any activation of the defibrillator, either antitachycardia pacing or shock, was as follows: • for the patients with VF, 36% at 3 months, 68% at 1 year, 81% at 2 years, and 85% at 3 years;• for the patients with VT, 15%, 39%, 53 percent, and 69%, respectively.

CMAJ 2007

Bunch TJ et al. Mayo Clin Proc 2005
Long-term management of CA survivors
Neurological injury• Rehabilitation• Care to minimize disabilities
Psychiatric disease• Depression• Anxiety
Secondary prevention of arrhythmias• ICD placement
Secondary prevention of CAD• Treatment of hypertension, hyperlipidemia, diabetes, obesity, nicotine dependence• Use of life-saving medications
Lifestyle modifications• Weight loss• Tobacco cessation• Exercise
Cardiac rehabilitation
Kliegel et al. Resuscitation 2002; 52:301-4