lifestyle risk assessment - nhsgchdmcn.scot.nhs.uk · cvd risk assessment when? who? how? 40 – 74...
TRANSCRIPT

LIFESTYLE RISK ASSESSMENT
How and Why do we it?

What are we going to cover?
Basic epidemiologyRisk factorsStrategies for preventionHow do we calculate riskManagement of high risk individuals

CVD RISK - backgroundCardiovascular disease (CVD) is currently the main cause of preventable death in the UK and a major cause of disability and ill-healthCVD includes coronary heart disease (CHD), stroke and peripheral artery diseaseCHD is most commonly caused by atherosclerosis, which occurs when deposits of cholesterol accumulate to form a plaque accumulate leading to a cascade of inflammatory processes.Cost to nhs is £30 billion per year

What are the risk factors?MODIFIABLE/NON-MODIFIABLE
Ethnicity (ancestry from India, Pakistan, Bangladesh, or Sri Lanka) Increasing ageMale genderSocioeconomic deprivationLifetime smoking habitHigh ratio of total cholesterol to HDL cholesterolHigh systolic BPAdipositySedentary lifestyleAlcohol abusePsychosocial stress

Risk factors continued….
Co-Morbidities
People who already have CHD, CVD, PVDDiabetes (Type 1 and 2)Familial hypercholesterolaemia, familial mixed dyslipidaemia, or other inherited dyslipidaemiasFamily history of premature CVDImpaired glucose regulationHigh triglyceridesRenal dysfunction [CKD]Left ventricular hypertrophyAFAutoimmune disorders [RA/SLE]
Treatment of these should be optimizied

Most risk factors are not independent e.g. social deprivation, smoking, stress and alcohol abuse are associated. Also ethnicity, adiposity, blood lipids and diabetes.
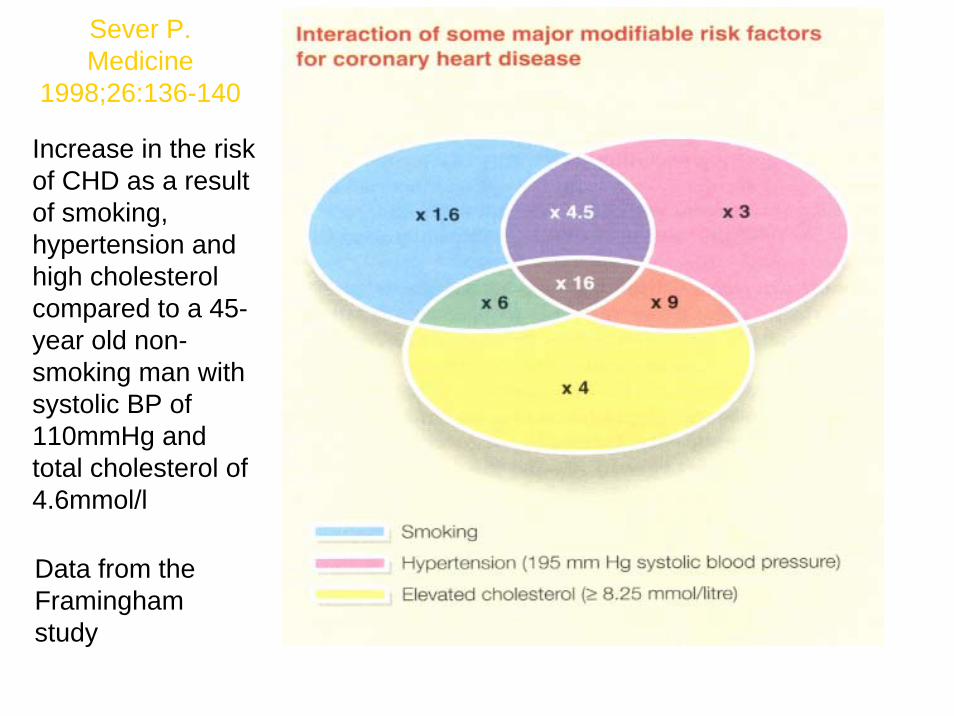
Sever P.Medicine
1998;26:136-140
Increase in the risk of CHD as a result of smoking, hypertension and high cholesterol compared to a 45-year old non-smoking man with systolic BP of 110mmHg and total cholesterol of 4.6mmol/l
Data from the Framingham study

ROLE OF CVD RISK ASSESSMENT IN STRATEGIES FOR PREVENTION
Can be targeted at individuals or populationsCVD risk assessment is central to prevention strategies and an important component of population based strategies to reduce the burden of CVD.High risk individuals have the most to gain from RF modifications and are given the highest priorityPopulation based strategies are supported by a method to screen patient records to identify ^ risk individuals. They are then formally assessed and offered advice and treatment. This is recommended by NICE in addition to opportunistic assessment e.g. Granite Study and the Keep Well ProgrammeThe QIS standards for HD April 2010 recommends a mechanism be in place to identify individuals (without confirmed CVD) in high priority groups :-
Socially deprived areasConfirmed hypertension
Regular smokers1st degree relatives with premature CVD
Serious and enduring mental health problemsLearning disabilities
BMI >40Ethnicity (south Asian)

GRANITEGrampian Risk Assessment aNd InTErvention
• Utilises “ predictive “ software to calculate probable risk• Uses ASSIGN calculator to estimate the risk• All the relevant risk factors taken into account including Social deprivation • Structured clinics with Questionnaires & Near Patient Testing• Helps increase Practice prevalence rates• Identifies & addresses co‐morbidities• Allows intervention if alcohol excess• Fulfils QIS standard criteria

Peterhead GRANITE: pop cohorts

CVD RISK ASSESSMENT WHEN? WHO? HOW?
40 – 74 yrs, andAny age individuals with 1st degree relative with premature CVD/ familial dyslipidaemia
Should be risk assessed every 5 years.Individuals on anti-hyp meds or lipid lowering therapy
Should be risk assessed annually.> 40yrs with DM or * familial hypercholestrolaeamia should be assumed as high risk with no risk calculator neededAn appropriate risk calculator should be used and adjusting risk for any factors not taken into account by calculator – ASSIGN currently used in Scotland. Clinical judgement should be adopted in indiviuals (who do not fall into categories above or are <20%) but display other risk factors.

Active autoimmune disorders such as Rheumatoid Arthritis , SLE, Gout CKD (eGFR less than 60)Learning disability, severe mental illnessOn antipsychotic medicationObesityEthnic minorities Erectile DysfunctionOn treatment for human immunodeficiency virus
Risk < 20% but other risk factors


• LDL cholesterol is raised (TChol>7.5 mmol/l, LDL>4.9 mmol/l)
• Personal history of premature coronary heart disease
• Tendon xanthomata• Family history of above (MI in 2nd degree relative
<50 years, MI in 1st degree relative <60years)
Don’t Forget !
Suspect familial hypercholesterolaemia where:
Genetics test, consent formwith patient informationleaflet
If treated early enough,patients live longer !

Pre-lipid assessment should include:-Smoking cessAlcohol consumptionBP BMI / waist circumLipids [pref fasting]BGLRenal functionLFT’sTSH [if dyslipidaemia present]

IDENTIFIED AS HIGH RISK NOW WHAT?
Advise risk is an estimate which is more likely to be accurate if >20% and emphasise 10yrs not a lifetimeCommunicate with patient to motivate/engage them in reducing their cvd risk.Offer advice on modifiable risk factorsOffer drug therapy

COMMUNICATIONFind out what they have been told about cvd risk assessment – how do they feel?Explore their beliefs about what determines future good healthAssess their readiness/willingness and confidence to make changes to their lifestyle, take tests and drug therapyInvolve them in a shared management planInform them of future management and benefits of changes based on current evidence and best practice.Take into account their needs and preferences –culture/physical/sensory/language/learning disabilitiesPsychosocial issues – depression and isolation, lack of social support.Most importantly check their understanding of what has been discussed and planned.

LIFESTYLE MODIFICATIONSCARDIOPROTECTIVE DIET
low in total and saturated fatsFive a day2 portions of fish per week – 1 of oilyReduced salt
PHYSICAL ACTIVITYAt least 30mins moderate intensity exercise per day at least 5 days per week.Encourage to exercise at maximum safe capacity10 min bouts to achieve 30minsRecommend exercise that can be incorporated into everyday life

LIFESTYLE contd…..OBESITY
Offer advice on weight loss to people with BMI >25Refer to weight loss programmes if availableAdvise risks associated with ^ BMIAdvise benefits of 5-10 % wgt loss
ALCOHOL CONSUMPTIONMen 21 units per week…women 14 units per weekAvoid binge drinking with one or two alcohol free days pwAlcohol calculator

LIFESTYLE contd…
SMOKINGStop smokingSupport and adviceReferral to smoking cessation servicesNicotine replacement therapy

DRUG THERAPY IN PRIMARY PREVENTION
Individuals identified as high risk either due to existing co-morbidities or risk calculator result >20% should be offered statin therapy as directed by the Grampian Joint statement on the use of lipid lowering agents – dec 2010.If simvastatin 40mg contraindicated / not tolerated offer a lesser dose or alternative lose dose statin [ atorva 20mg].Higher intensity statins not indicated in primary prevention and no target TCLNo need for repeat lipid measurements – LFT’s at 3/12 and 1yr.Fibrates not indicated in primary preventionCombination therapy not indicated [fibrate and statin]NICE recommend Ezetimibe can be considered in primary hypercholestrolaemia but not in grampian joint statement.

REFERENCES
NICE GUIDELINE 67 – lipid modification and quick ref guide N675SIGN GUIDELINE 69 and Heart Disease quick ref guideJOINT FORMULARY STATIN GUIDELINESeatwell.gov.uk5aday.nhs.ukCounterweight.org