luciano phddefense
DESCRIPTION
Joanne S. Luciano, PhD Defense @ Boston University, 1996. Neural Network Models of Unipolar Depression. Patterns of Recovery and Prediction of Outcome. Work lead to two US PatentsTRANSCRIPT
Neural Network Modeling of Unipolar Depression:Patterns of Recovery and Prediction of Outcome
Joanne Sylvia Luciano, Jr. B.S., M.S.
Data from: Depression Research Facility, McLean Hospital; Massachusetts Mental Health Center;
and Harvard Medical School
Dissertation Defense30 August 1995 5:15 PM
2 Cummington Street, Room 101Boston, MA 02215
Department of Cognitive and Neural Systems, Boston University
J. S. Luciano Ph.D. Defense
30 August 1995 Page 1

Depression is a BIG problemCharacterized by persistent and pathological
sadness, dejection, and melancholyPrevalence (US)
17% experience it in lifetime10% a year (25 million)
Cost (US)$44 billion a year (1990)
Impact (US)1% improvement means 250,000 people helped1% means $440 million savings
J. S. Luciano Ph.D. Defense
30 August 1995 Page 2

The Economic Burden of DepressionDepression Costs the U.S. $43.7 Billion Annually
Source: Paul Greenberg et alMIT Sloan School of Management/Analysis Group, Inc.
$23.8 Billion
$12.4 Billion
$7.5 Billion
Direct Costs:Treatment &
Rehabilitation
Loss of Earnings Due toDepression-Induced
Suicides
Workplace Costs:Absenteeism
& Lost Productivity
J. S. Luciano Ph.D. Defense
30 August 1995 Page 3

Research Goals
Correct Treatment
IlluminatePath to Recovery
Individualized Treatment
J. S. Luciano Ph.D. Defense
30 August 1995 Page 4
!"#$%&'("#)!*+)#!"#!"$%&"'%("
!"#$$$%&
)"*+,!-.
)"*+,!-/
,+,-./#(!,'0!#0!$%1#2%$,!
J. S. Luciano Ph.D. Defense
30 August 1995 Page 5

Depression Background
Clinical DepressionTreatmentMeasurementNot specific diagnosisNot specific treatment
J. S. Luciano Ph.D. Defense
30 August 1995 Page 6

Clinical Data
Hamilton Depression Rating Scale21 Symptoms (scale of 0..4)Overall Severity of Depression
Treatments (3 clinical studies)Desipramine (DMI)Cognitive Behavioral Therapy (CBT)Fluoxetine (Prozac)
Outcome (responded to treatment)Categorical (YES/NO)Continuous (How much? % change)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 7
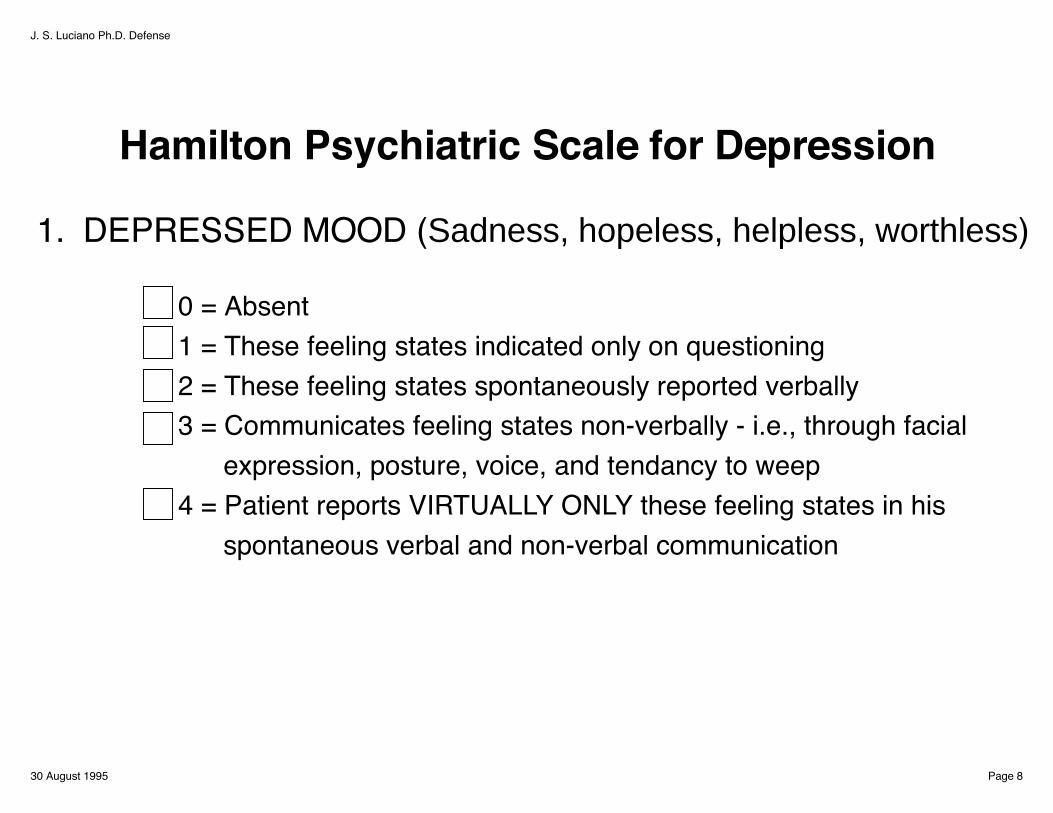
Hamilton Psychiatric Scale for Depression
1. DEPRESSED MOOD (Sadness, hopeless, helpless, worthless)
0 = Absent1 = These feeling states indicated only on questioning2 = These feeling states spontaneously reported verbally3 = Communicates feeling states non-verbally - i.e., through facial expression, posture, voice, and tendancy to weep4 = Patient reports VIRTUALLY ONLY these feeling states in his spontaneous verbal and non-verbal communication
J. S. Luciano Ph.D. Defense
30 August 1995 Page 8

Modeling Background
Recast problem into mathematical terms
Easier to understandEasier to manipulateEasier to analyze
J. S. Luciano Ph.D. Defense
30 August 1995 Page 9

TreatmentNot
DepressedDepressed
symptoms pattern outcome
ModelingRecovery
Predicting Response
Clinical Data
J. S. Luciano Ph.D. Defense
30 August 1995 Page 10

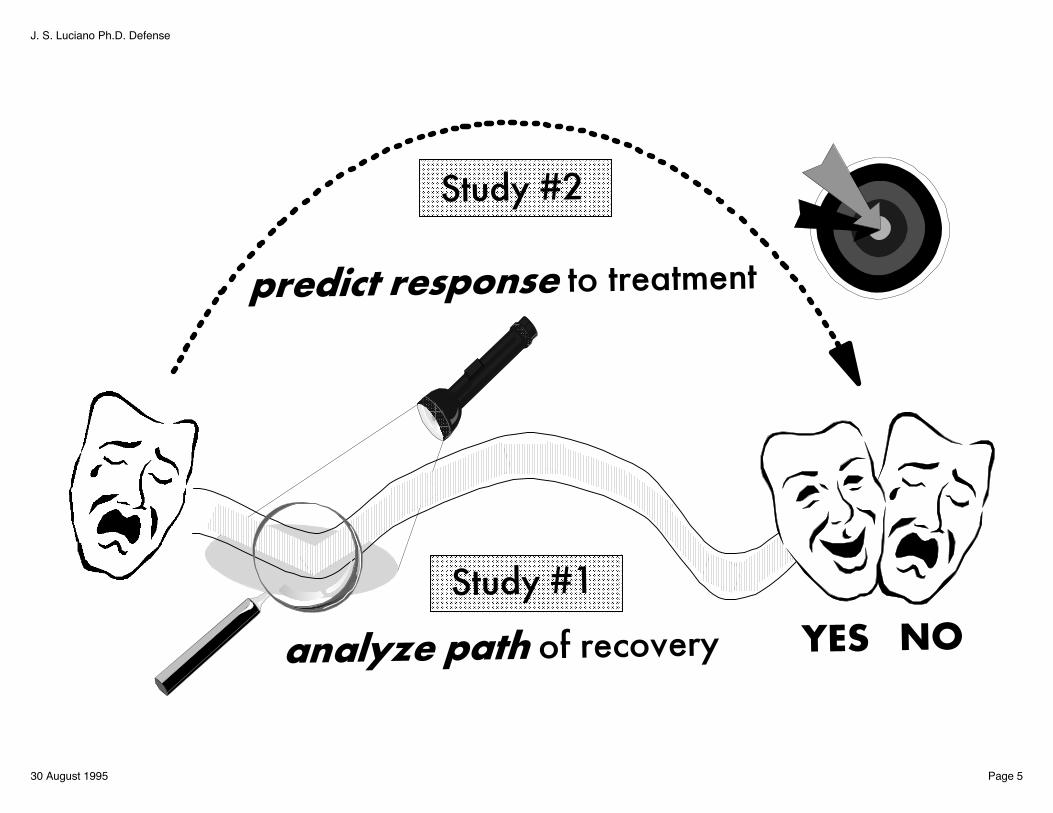
Study # 1
Analyze path of RECOVERY
J. S. Luciano Ph.D. Defense
30 August 1995 Page 11

Take Home MessagesA neural network model is capable of predicting and describing recovery patterns in depression.
Recovery patterns differ by treatmentCognitive Behavioral Therapy
is sequentialDesipramine
is concurrent (after delay)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 12

Understanding Recovery
Patient Recovery pattern (Differential Equations) x
TreatmentNot
DepressedDepressed
Compare patterns of recovery
Recast as dynamical system
6 week When response begins (Latency) ! ! t7 symptoms Indirect (between symptoms) (Interaction Effects) w2 treatments Direct (on symptoms) (Treatment Effects) u,v
J. S. Luciano Ph.D. Defense
30 August 1995 Page 13

DepressionPhysical: E Sleep
M, L SleepEnergy
Performance: WorkPsychological: Mood
CognitionsAnxiety
7 Symptoms
2 Treatments Cognitive Behavioral Therapy (CBT)Desipramine (DMI)
Clinical Data Responders = improvement >= 50% N = 6 patients each study6 weeks = 252 data points each study
J. S. Luciano Ph.D. Defense
30 August 1995 Page 14

OverviewRecovery Model and Parameters
Latency
TreatmentEffects
InteractionEffects
Treatment
wij
! t! t
vu , ii
=
J. S. Luciano Ph.D. Defense
30 August 1995 Page 15

Modeling Time to Response
" Rapidness of response! t Latency
Latency
Treatment onset
!tLatency
h t te t t( , ) ( )""
# =+ # #
!!
11 !t
! t
iu ivsymptom
J. S. Luciano Ph.D. Defense
30 August 1995 Page 16
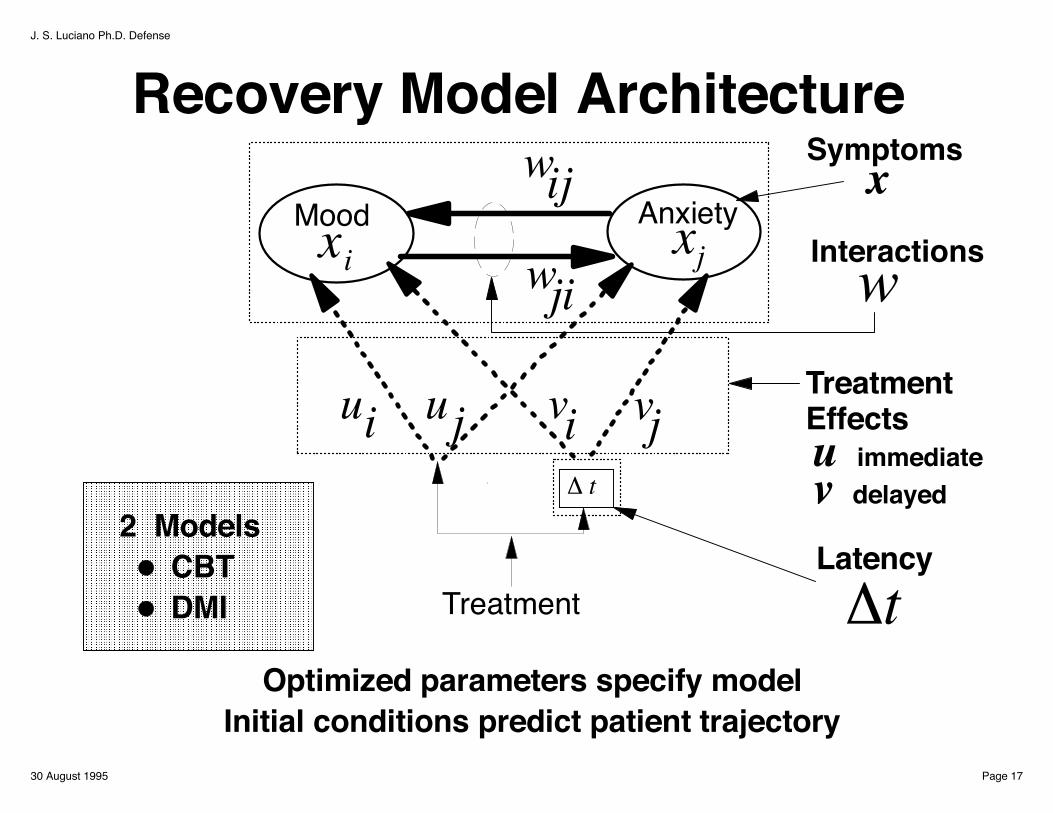
Recovery Model Architecture
InteractionsAnxiety
Symptoms
w
Latency!tTreatment
! t
xi xj
vjviiu uj
wij
wji
Mood
Treatment Effectsu immediatev delayed
2 Models CBT DMI
x
Optimized parameters specify modelInitial conditions predict patient trajectory
J. S. Luciano Ph.D. Defense
30 August 1995 Page 17

Recovery Model
x x
Treatment Effectson each symptom(strength)
Stabilizing factor
!! !
!, # t
Symptom
( )wx B ijj j#
Baseline
Interactions between symptoms
7 symptoms
Rate of symptom changeAi i i= #
+$j=1
7Acceleration of symptom
s(t) ui+
Latency
+ ( ) vih t
Immediate effectstep function
Delayed effect sigmoid function "
Steepness
J. S. Luciano Ph.D. Defense
30 August 1995 Page 18

Training the Model
actual
estimated
Obtain optimized parameters-fit patient data -train on time course-minimize error term L-gradient descent on parameters
L = Error termX = datai = symptomsj = parameterk = patients
( ) ( )L X X X f X dt K Pik ik ik ik ikik
T
jj= # + #$% + $&'(
)*+
&'(
)*+" "! "
2
0
2µ
J. S. Luciano Ph.D. Defense
30 August 1995 Page 19

Recovery Pattern and ErrorExample Patient (CBT)
0 10 20 30 400.20.40.60.8
Pat 1840201 ANXITEY [DAYS]0 10 20 30 40
0
0.2
Pat 1840201 COGNITIVE [DAYS]
0 10 20 30 400.20.4
Pat 1840201 MOOD [DAYS]0 10 20 30 40
0.40.60.8
Pat 1840201 WORK [DAYS]
0 10 20 30 400
0.5
Pat 1840201 ENERGY [DAYS]0 10 20 30 40
0
0.05
0.1
Pat 1840201 E SLEEP [DAYS]
0 10 20 30 400
0.05
0.1
Pat 1840201 M,L SLEEP [DAYS]0 200 400 600
0
100
200
(L=25.8) ERROR TREND [CYCLES]
J. S. Luciano Ph.D. Defense
30 August 1995 Page 20

ResultsOptimized parameters specify model
Initial conditions predict pattern trajectory
Latency
TreatmentEffects
InteractionEffects
Treatment
wij
! t! t
viui 2 Models
CBT DMI
J. S. Luciano Ph.D. Defense
30 August 1995 Page 21

Latency!!t = response delay
CBT: 1.2 weeks DMI: 3.4 weeks
0 1 2 3 4 5 6
Weeks!!t Latency parameter
CBT
DMI
J. S. Luciano Ph.D. Defense
30 August 1995 Page 22

Mean 1/2 Reduction Time
CBT
DMI
0 1 2 3 4 5 6
2.57
3.74
1.51
3.54
1.37
2.09
2.21
2.67
2.76
2.1
4.63
2.96
5.04
3.89
AnxietyCognitionsMoodWorkEnergyE SleepM,L Sleep
Weeks
CBT varies 3.7DMI varies 1.8
J. S. Luciano Ph.D. Defense
30 August 1995 Page 23

Direct Effect of TreatmentDesipramine
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6
Immediate 3.4 Weeks
Cognitive Behavioral Therapy
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6
Immediate 1.2 Weeks
AnxietyCognitionsMoodWorkEnergyE SleepM, L Sleep
(u )iImmediate vs. Delayed (v )icoefficients (strength)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 24

Direct Treatment Intervention Effect
CBT
! t
CM
MS
ES
W E
ui
TreatmentEffects
(u )i DMI
! t
A
CM
MS
ES
W E
v )i(u ,i (v )i
A AnxietyC CognitionsM MoodW Work
Weak
Strong
E EnergyES E SleepMS M, L Sleep
Immediate Delayed
A
iv,J. S. Luciano Ph.D. Defense
30 August 1995 Page 25

Treatment Effects and Interactions DMI (delayed)
CONCURRENTCBT
SEQUENTIAL
J. S. Luciano Ph.D. Defense
30 August 1995 Page 26

ConclusionsAn neural network model is capable of predicting and describing recovery patterns in depression.
Recovery patterns differ by treatmentCognitive Behavioral Therapy
is sequentialDesipramine
is concurrent (after delay)
Combined treatment for suicidal patents? Reduce suicidal tendency quickly?
J. S. Luciano Ph.D. Defense
30 August 1995 Page 27
LimitationsModel:
Assumes symptoms interactAssumes treatment acts directlyPermanent vs. transientCausal vs. sequentialStatistical fluctuations not handled
Study:CBT measurement intervals varySmall sample sizeInitial 6 weeks of CBT (entire=16)Finer resolution of measurements (daily)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 28

Consistent with earlier studies
Bowden 1993 Mood at 3 weeks predicts response for fluoxetine (Prozac)
*some discrepancies with our patient data
Persistent improvement after delayQuitkin, 1984, 1987
Katz, 1987Mood and cognitive impairment at 1 week predicts response Retardation improves much later*
Nagayama 1991 Severity at 1 week predicts response
J. S. Luciano Ph.D. Defense
30 August 1995 Page 29

Future Studies
Larger databaseNon-respondersOther illnessesOther measuresOther treatmentsLink to brain regions
J. S. Luciano Ph.D. Defense
30 August 1995 Page 30

Study # 2
Predict Response to Treatment
J. S. Luciano Ph.D. Defense
30 August 1995 Page 31

Will an individual respond?Methods
BackpropagationMultiple Regression
Output
7 SmptomsTreatmentSeverity99 patients
InputNone (Raw)NormalExponentialGamma
Transformations
Tells what to prescribeBetter match (diagnosis & treatment)1% = 250,000 people helped
$440 million saved
Categorical Yes/No
ContinuousHow much
Potential Benefits:
J. S. Luciano Ph.D. Defense
30 August 1995 Page 32
16 Studies attempted to predict response
Prior Results
These comprise 224 individual findings:
Severity: 10 significant 9 not significant
Used linear methodsYielded inconsistent results
Symptoms 10 significant 95 not significant
J. S. Luciano Ph.D. Defense
30 August 1995 Page 33

The Nonlinear Approach
Previous failures used linear methods, so....
We tried nonlinear methods
More powerfulCapture nonlinear interactions
J. S. Luciano Ph.D. Defense
30 August 1995 Page 34

Data sets & PreprocessingInitial Input-Output Pairs
Categorical Continuous (normalize [0..1])
Raw
Exponential
Gamma
Normal
3 different models BP (2) BP (8) Linear Regression (MR)
z-score
J. S. Luciano Ph.D. Defense
30 August 1995 Page 35

HOW?
Start simpleBackpropagation
Independent variables21 Symptoms, Severity, Treatment
Dependent variablesCategorical (Responder / Nonresponder)Continuous (percent improved)
Train on 99 Patients' data (symptoms, severity, treatment, response)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 36

MethodsData comprises 99 input/output pairs
Inputs21 Symptoms1 Overall Severity3 Treatments
OutputResponsea. Categorical (Yes/No)b. Continuous (% change)
PreprocessingRemove Irregularities (transformations: exp, gamma, norm)
Normalize (z-score [0..1])
Linear Regression, BP (2), BP (8) yields 24 datasets
J. S. Luciano Ph.D. Defense
30 August 1995 Page 37

Results
Categorical (yes/no)
Best performance CorrectBackpropagation (2) Hidden Units 54.5 %Backpropagation (8) Hidden Units 54.5 %Linear Regression 51.5%Chance 50.0 %
J. S. Luciano Ph.D. Defense
30 August 1995 Page 38

ResultsBest performance: Lowest RMS Error (%)
Raw Norm Exp GamMR 27.7 27.4 24.6 24.7BP (2 Hidden) 23.5 23.1 20.3 20.6Difference 3.2 6.1 4.3 5.1
Exponential transformation bestBP better than MR in every caseworst BP better than best MR
J. S. Luciano Ph.D. Defense
30 August 1995 Page 39

Backpropagation (Nonlinear) Performed Slightly Better
BUT...
Still not statistically significant:
WHY?
J. S. Luciano Ph.D. Defense
30 August 1995 Page 40

PerformanceTraining good, test poorNetwork can't generalize
# parameters 54 # samples 66
PoV should be 84%, but actually only 4.5%
Reduce 21 HDRS to 7 Symptom Factors
= = 84%Expected PoV =
J. S. Luciano Ph.D. Defense
30 August 1995 Page 41
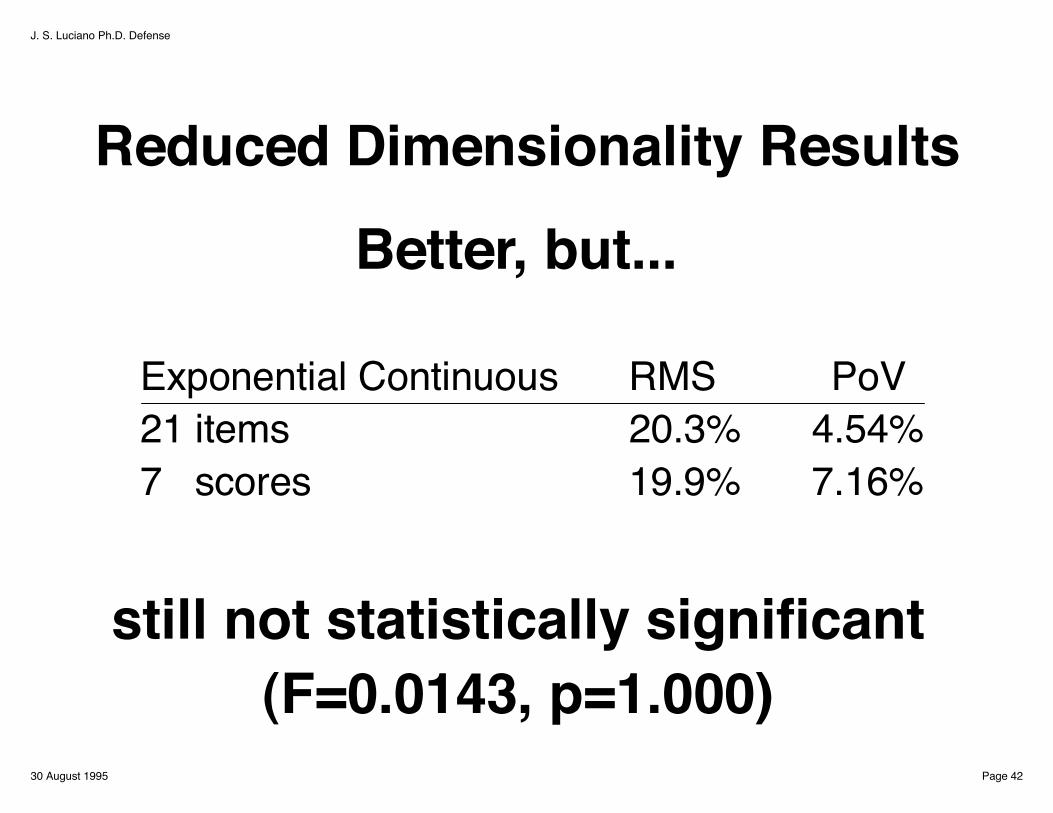
Reduced Dimensionality Results
Better, but...
still not statistically significant(F=0.0143, p=1.000)
Exponential Continuous RMS PoV21 items 20.3% 4.54%7 scores 19.9% 7.16%
J. S. Luciano Ph.D. Defense
30 August 1995 Page 42

Is Data Random?
#params 27 #samples 99
Trial PoV Chance (expected) 27.27 % Chance (random sample) 24.85 % Raw Categorical 46.46 % Exp Categorical 45.87 % Raw Continuous 45.33 % Exp Continuous 66.61%
Expected PoV = 27%==
J. S. Luciano Ph.D. Defense
30 August 1995 Page 43

Weight Analysis
Responder predicted when:
Fluoxetine (Prozac) (+)Cognitions (-)Early Sleep Disturbance (+)Anxiety (+)Severity (-)
(+) present (-) absent
J. S. Luciano Ph.D. Defense
30 August 1995 Page 44

ConclusionsBP (nonlinear method) consistently outperformed MR (linear method)
Still, the prediction was not statistically significant (F=0.0143, p=1.000)
But, the theory implies proportion of variancefor the network is df/N = 27/99=27.3% for ramdom data Actual was 66.7% >> 27.3%
Suggestspredictive relationships are presentlarger study with more data needed
J. S. Luciano Ph.D. Defense
30 August 1995 Page 45

SummaryNeural network methods applied to clinical research in depression
Useful to understanding recovery dynamics
More powerful than current methodsused for clinical depression research
J. S. Luciano Ph.D. Defense
30 August 1995 Page 46

Future....Integrated Model
LinkSymptomsBrain Region ActivityNeurotransmitters
Combine data fromClinical StudiesAnimal ModelsImaging DataMetabolite Studies
J. S. Luciano Ph.D. Defense
30 August 1995 Page 47

Link to the FutureIntegrate knowledge about:symptoms, brain regions, transmitter systems,pharmacological agents, and dynamicsto build integrated models
Two norepinephrine pathways locus coeruleus to the hypothalamusaffect feeding behavior.
One excites, the other inhibits.DMI (presynaptic drug) induces eating prevents norepinephrine inactivation by blocking reuptake
symptom: appetite & weight
Pontine (ACh)
++ - -
--
"-receptors
,-receptors
PeriventricularNucleus
PerifornicalNucleus
Pons
Hypothalamus
Locus Coeruleus
Stops Eating
Starts Eating
J. S. Luciano Ph.D. Defense
30 August 1995 Page 48