mariane de montalembert, md service de pédiatrie hospital necker paris, france
DESCRIPTION
Mariane de Montalembert, MD Service de Pédiatrie Hospital Necker Paris, France. Adjusting Chelator Dose in Response to Adverse Events in a Patient with Sickle Cell Disease. Patient Presentation. 14-year-old boy Diagnosed through neonatal screening No siblings - PowerPoint PPT PresentationTRANSCRIPT
Adjusting Chelator Dose in Response to Adverse Events in a Patient with
Sickle Cell Disease
Mariane de Montalembert, MDService de Pédiatrie
Hospital NeckerParis, France
Patient Presentation
• 14-year-old boy
• Diagnosed through neonatal screening
• No siblings
• Acute chest syndrome (ACS) at age 2 and 6 years
• 2–3 hospitalizations per year for vaso-occlusive crises (VOC) from age 5–7 years
• Treatment with hydroxyurea initiated at age 7 years– Initial dosage 15 mg/kg/d
– Progressive increase to 25 mg/kg/d
– Initial success: no new VOC or ACS from age 7–12 years
• ACS and repeated VOC at age 12 years
• Progressive increase of dosage of hydroxyurea to 35 mg/kg/d with no subsequent reduction in frequency of pain crises
Decision Point 1What Is the Best Next Step?
a. Transfusion
CORRECT:CORRECT: Chronic transfusion can decrease the incidence of Chronic transfusion can decrease the incidence of VOC and ACSVOC and ACS
b. Bone marrow transplant
INCORRECT: The patient has no sibling to serve as a potential donor
c. Increase dosage of hydroxyurea
INCORRECT: Hydroxurea dosage >35 mg/kg/d is not recommended
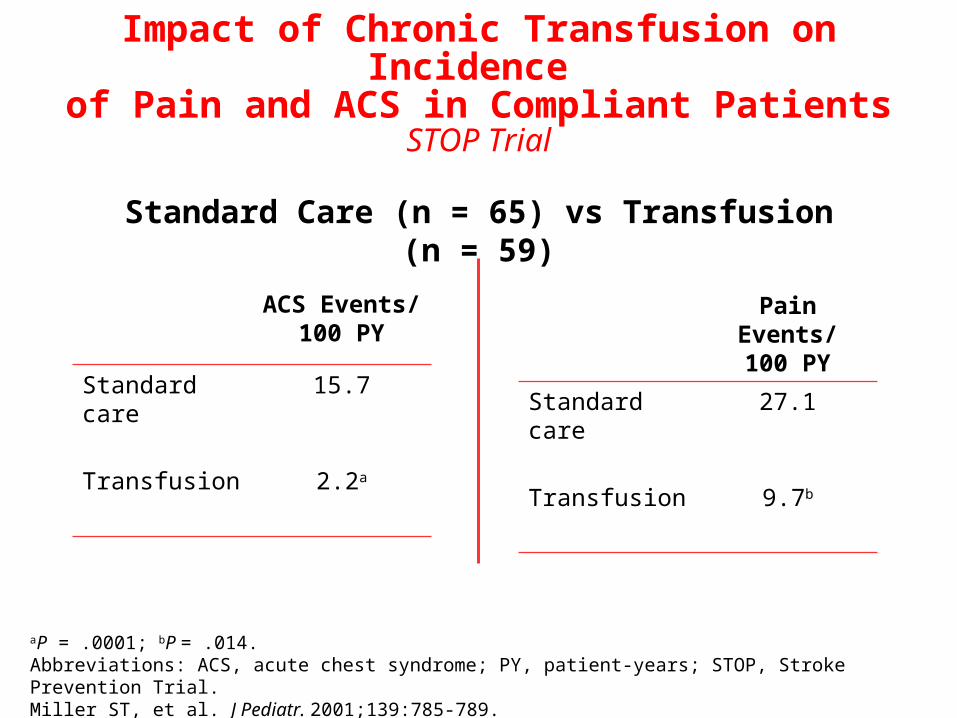
ACS Events/100 PY
Standard care 15.7
Transfusion 2.2a
Pain Events/100 PY
Standard care 27.1
Transfusion 9.7b
Impact of Chronic Transfusion on Incidence of Pain and ACS in Compliant Patients
STOP Trial
Standard Care (n = 65) vs Transfusion (n = 59)
aP = .0001; bP = .014.Abbreviations: ACS, acute chest syndrome; PY, patient-years; STOP, Stroke Prevention Trial.Miller ST, et al. J Pediatr. 2001;139:785-789.
Case Continues
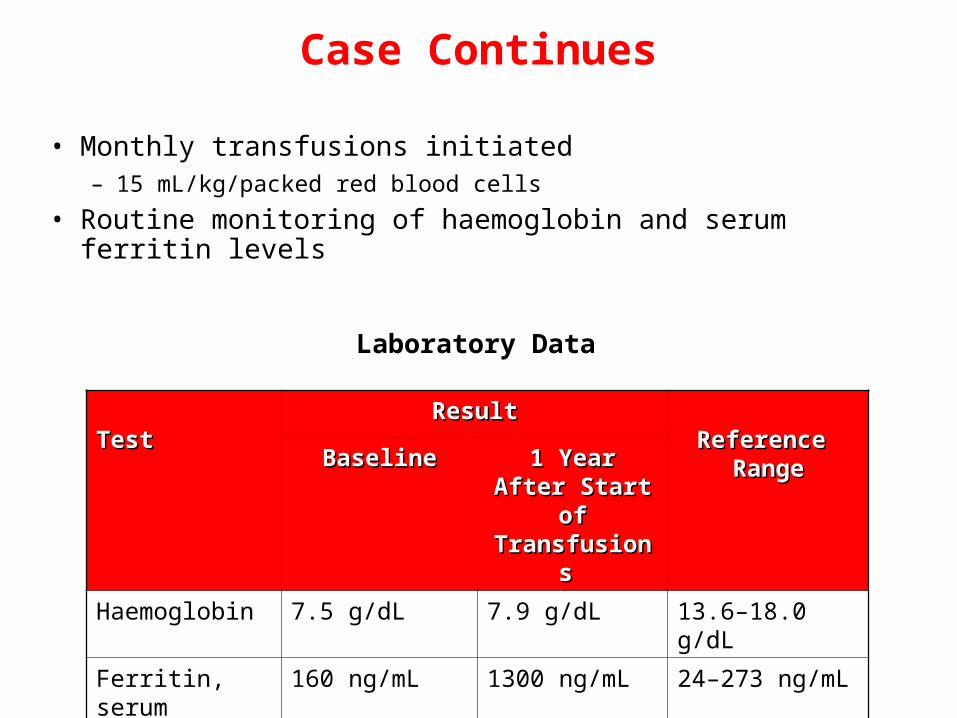
• Monthly transfusions initiated– 15 mL/kg/packed red blood cells
• Routine monitoring of haemoglobin and serum ferritin levels
TestTestResultResult
Reference Reference RangeRangeBaselineBaseline 1 Year After 1 Year After
Start of Start of Transfusions Transfusions
Haemoglobin 7.5 g/dL 7.9 g/dL 13.6–18.0 g/dL
Ferritin, serum 160 ng/mL 1300 ng/mL 24–273 ng/mL
Laboratory Data
Case Continues
• Chelation therapy started 1 year after the beginning of transfusions– Deferasirox 20 mg/kg/d
• Patient develops a rash after 2 weeks of treatment– moderate to severe rash
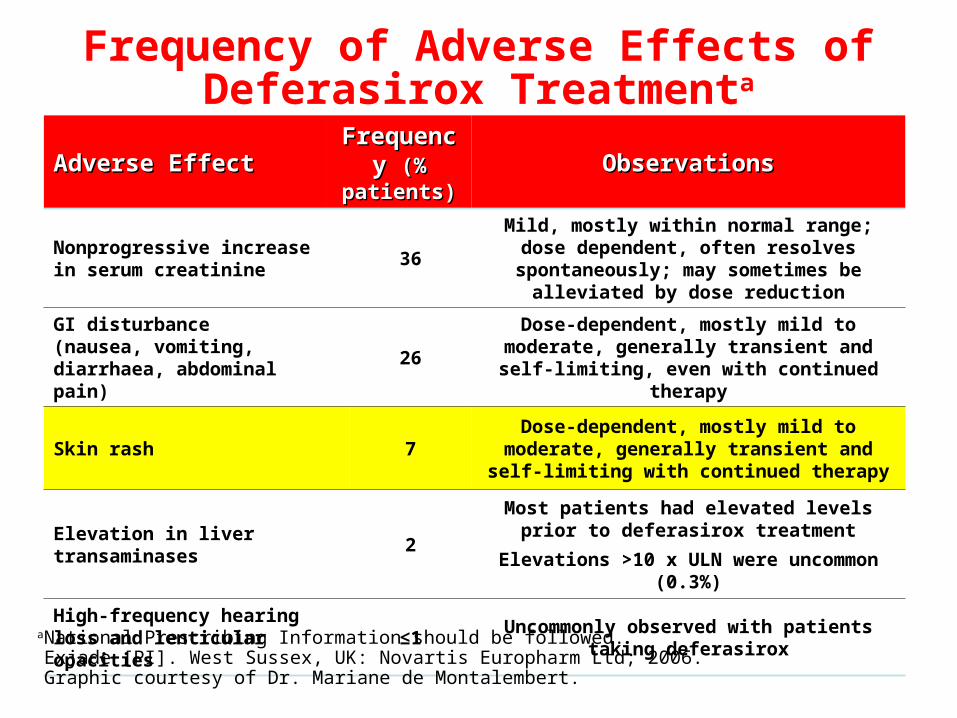
Frequency of Adverse Effects of Deferasirox Treatmenta
Adverse EffectAdverse Effect Frequency Frequency (% patients)(% patients)
ObservationsObservations
Nonprogressive increase in serum creatinine
36
Mild, mostly within normal range; dose dependent, often resolves spontaneously;
may sometimes be alleviated by dose reduction
GI disturbance(nausea, vomiting, diarrhaea, abdominal pain)
26Dose-dependent, mostly mild to moderate,
generally transient and self-limiting, even with continued therapy
Skin rash 7Dose-dependent, mostly mild to moderate, generally transient and self-limiting with
continued therapy
Elevation in liver transaminases 2Most patients had elevated levels prior to
deferasirox treatment
Elevations >10 x ULN were uncommon (0.3%)
High-frequency hearing loss and lenticular opacities
≤1Uncommonly observed with patients taking
deferasirox
M8.19
aNational Prescribing Information should be followed.Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006. Graphic courtesy of Dr. Mariane de Montalembert.

Decision Point 2What Is the Best Next Step?
a. Continue deferasirox at same dose and apply over-the-counter steroid creme
INCORRECT: Inconsistent with guidelines for product use
b. Stop deferasirox until rash resolves, then restart
CORRECT: Consistent with guidelines for product useCORRECT: Consistent with guidelines for product use
c. Reduce deferasirox dose until rash resolves
INCORRECT: Inconsistent with guidelines for product use

Mild to moderate rashMild to moderate rash Continue treatment without interruption
1. Interrupt treatment
2. After resolution of rash, reintroduce deferasirox at lower dose maybe in combination with oral steroid
3. Gradually escalate dose
Moderate to severe Moderate to severe rashrash
M8.7
1. Interrupt treatment
2. Reintroduce deferasirox at lower dose after resolution of rash
3. Gradually escalate dose
1. Interrupt treatment
2. After resolution of rash, reintroduce deferasirox at lower dose
3. Gradually escalate dose
aNational Prescribing Information should be followed.Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006. Graphic courtesy of Dr. Mariane de Montalembert.
Skin Rash–Deferasirox Dose Modification Algorithma
Severe rashSevere rash
• Deferasirox temporarily stopped
• When rash resolved, deferasirox reintroduced at 10 mg/kg/d
• After 1 month, dose reincreased up to 20 mg/kg/d, without recurrence of the rash
Case Continues
Case Continues
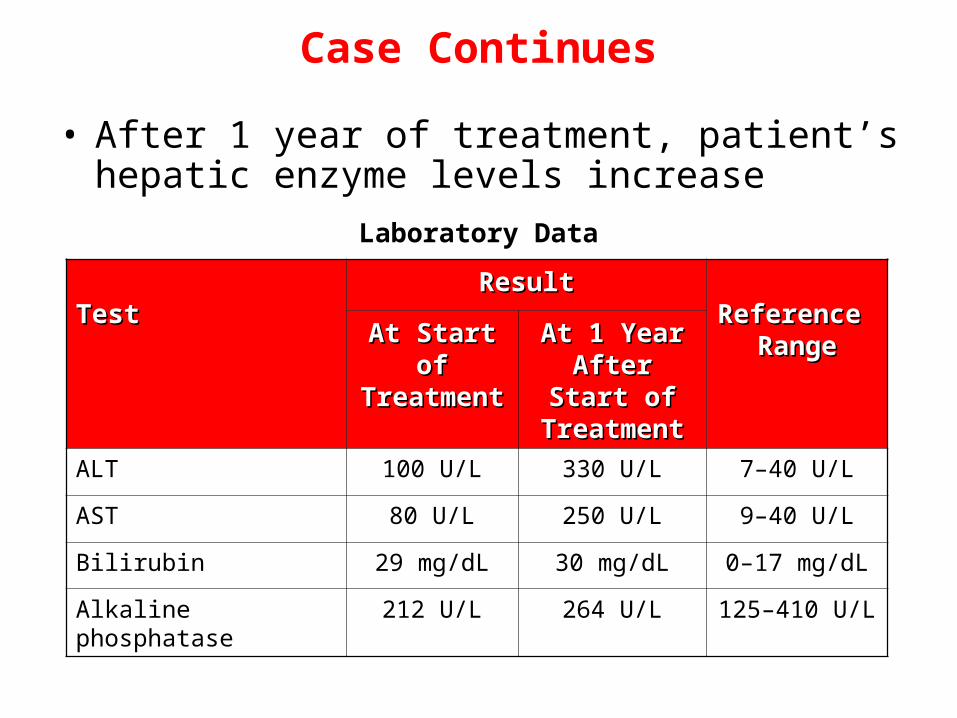
• After 1 year of treatment, patient’s hepatic enzyme levels increase
TestTestResultResult
Reference Reference RangeRangeAt Start of At Start of
TreatmentTreatmentAt 1 Year At 1 Year
After Start of After Start of TreatmentTreatment
ALT 100 U/L 330 U/L 7–40 U/L
AST 80 U/L 250 U/L 9–40 U/L
Bilirubin 29 mg/dL 30 mg/dL 0–17 mg/dL
Alkaline phosphatase 212 U/L 264 U/L 125–410 U/L
Laboratory Data
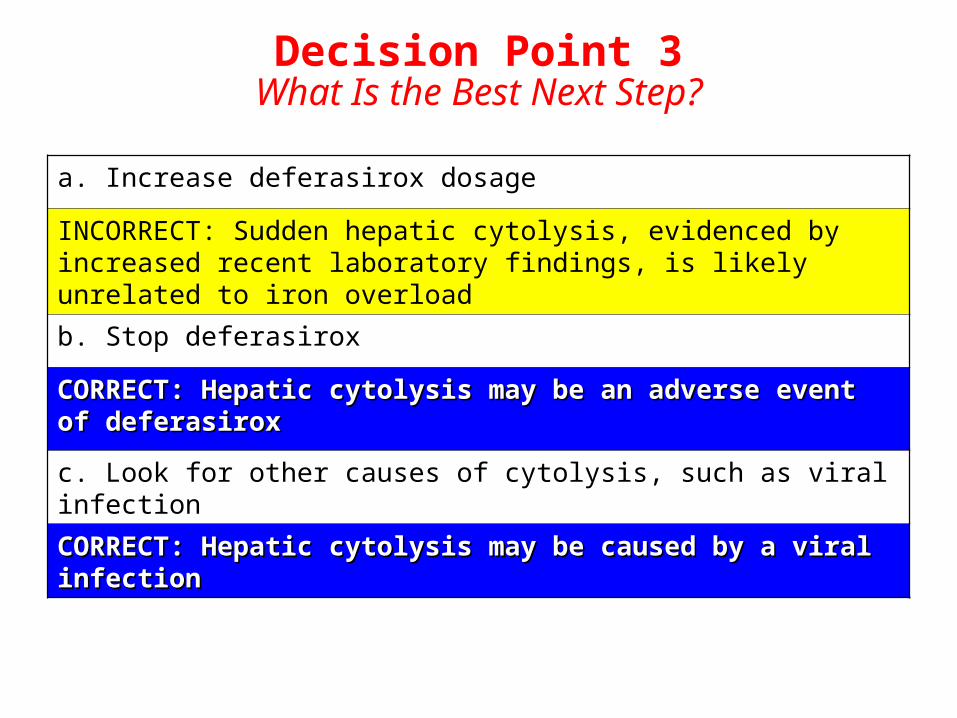
Decision Point 3What Is the Best Next Step?
a. Increase deferasirox dosage
INCORRECT: Sudden hepatic cytolysis, evidenced by increased recent laboratory findings, is likely unrelated to iron overload
b. Stop deferasirox
CORRECT: Hepatic cytolysis may be an adverse event of CORRECT: Hepatic cytolysis may be an adverse event of deferasirox deferasirox
c. Look for other causes of cytolysis, such as viral infection
CORRECT: Hepatic cytolysis may be caused by a viral infectionCORRECT: Hepatic cytolysis may be caused by a viral infection
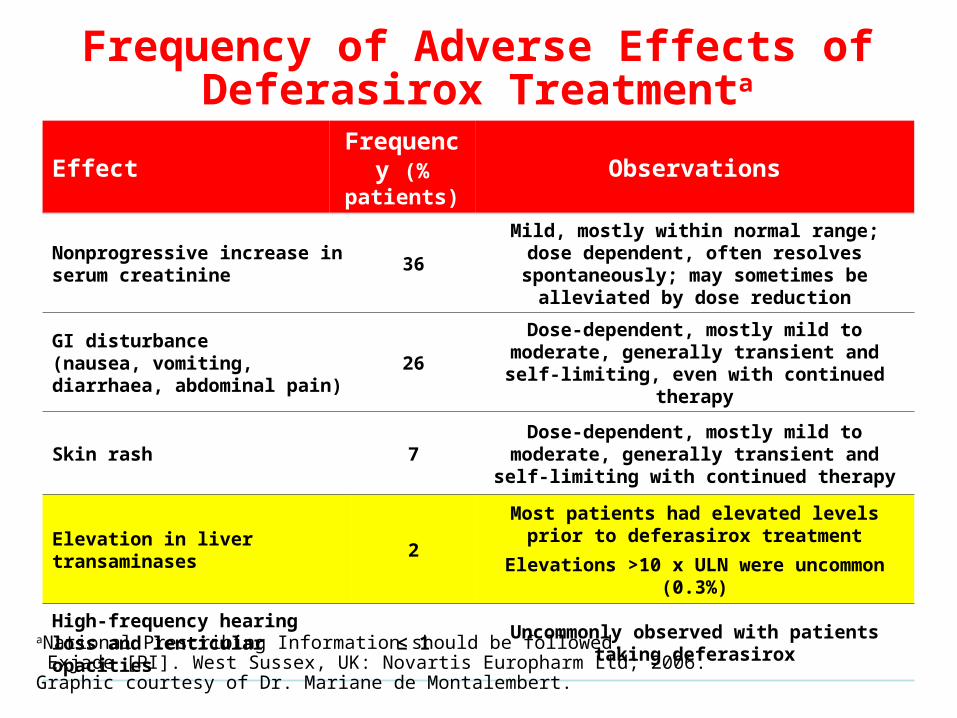
Frequency of Adverse Effects of Deferasirox Treatmenta
Effect Frequency (% patients)
Observations
Nonprogressive increase in serum creatinine
36Mild, mostly within normal range; dose
dependent, often resolves spontaneously; may sometimes be alleviated by dose reduction
GI disturbance(nausea, vomiting, diarrhaea, abdominal pain)
26Dose-dependent, mostly mild to moderate,
generally transient and self-limiting, even with continued therapy
Skin rash 7Dose-dependent, mostly mild to moderate, generally transient and self-limiting with
continued therapy
Elevation in liver transaminases 2Most patients had elevated levels prior to
deferasirox treatment
Elevations >10 x ULN were uncommon (0.3%)
High-frequency hearing loss and lenticular opacities
≤ 1Uncommonly observed with patients taking
deferasirox
M8.19
aNational Prescribing Information should be followed. Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006. Graphic courtesy of Dr. Mariane de Montalembert.

Managing Liver Function Test
Abnormalitiesa
2. Check for other causes of the liver function test abnormalities
3. When liver function tests return to baseline level, cautiously reintroduce deferasirox at 10 mg/kg/d
5. If no further increase, gradually increase dose to 20 mg/kg/d
4. Check ALT and AST every week for 1 month
6. Check ALT, AST, bilirubin, and alkaline phosphatase monthly
1. Discontinue deferasirox
aNational Prescribing Information should be followed. Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006.

Case Continues
• No other cause of abnormal liver function tests found (hepatitis B and C serologies negative, hepatic echo normal)
• Deferasirox discontinued
• Liver function tests returned to baseline level after 2 weeks– Then, deferasirox cautiously reintroduced at 10 mg/kg/d
• ALT and AST checked every week for 1 month with no further increase
• Deferasirox gradually increased to 20 mg/kg/d
• ALT, AST, bilirubin, and alkaline phosphatase checked monthly

Case Continues
Evolution of Urinary Markers of Renal Function
TestTestResultsResults
Reference Reference RangeRangeBaselineBaseline 1 Year After 1 Year After
Start of Start of DeferasiroxDeferasirox
2 Years After 2 Years After Start of Start of
DeferasiroxDeferasirox
Creatinine urine (mmol/L)
7.3 4.2 10.3 2.5–19
Creatinine clearance (mL/min)
110 120 120 >90
Total protein (g/L) .082 .047 .117 <.15 g/L
Total protein/creatinineratio
.10 .10 .10 <.50

Case Continues
Evolution of Urinary Markers of Renal Function
TestTestResultsResults
Reference Reference RangeRangeBaselineBaseline 1 Year After 1 Year After
Start of Start of DeferasiroxDeferasirox
2 Years After 2 Years After Start of Start of
DeferasiroxDeferasirox
Creatinine urine (mmol/L)
7.3 4.2 10.3 2.5–19
Creatinine clearance (mL/min)
110 120 120 >90
Total protein (g/L) .082 .047 .117 <.15 g/L
Total protein/creatinineratio
.10 .10 .10 <.50
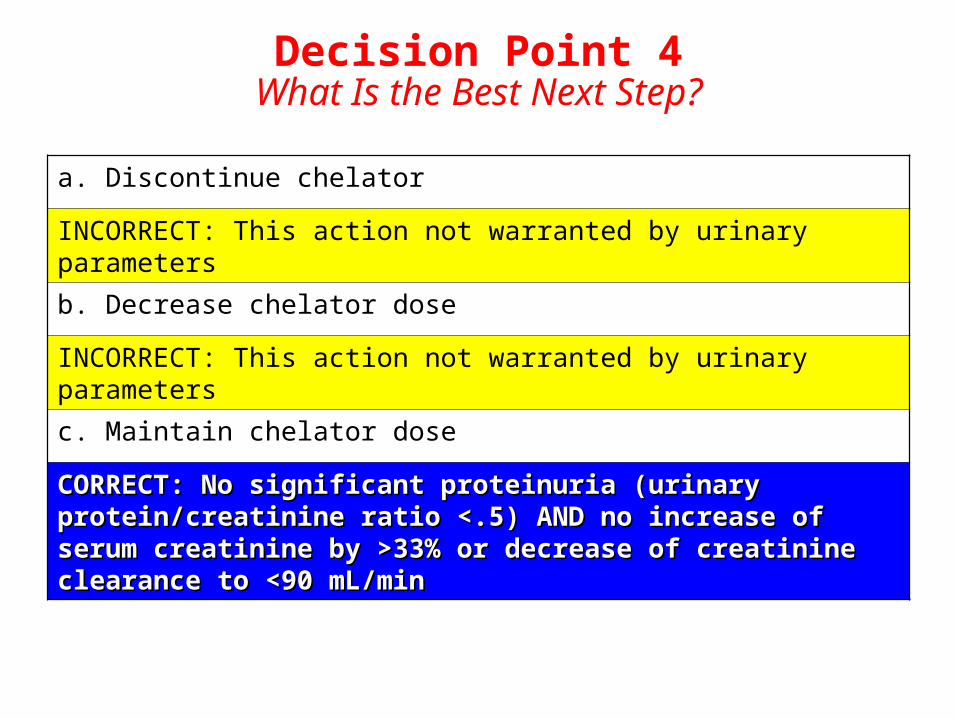
Decision Point 4What Is the Best Next Step?
a. Discontinue chelator
INCORRECT: This action not warranted by urinary parameters
b. Decrease chelator dose
INCORRECT: This action not warranted by urinary parameters
c. Maintain chelator dose
CORRECT: CORRECT: No significant proteinuria (urinary protein/creatinine No significant proteinuria (urinary protein/creatinine ratio <.5) AND no increase of serum creatinine by >33% or ratio <.5) AND no increase of serum creatinine by >33% or decrease of creatinine clearance to <90 mL/mindecrease of creatinine clearance to <90 mL/min
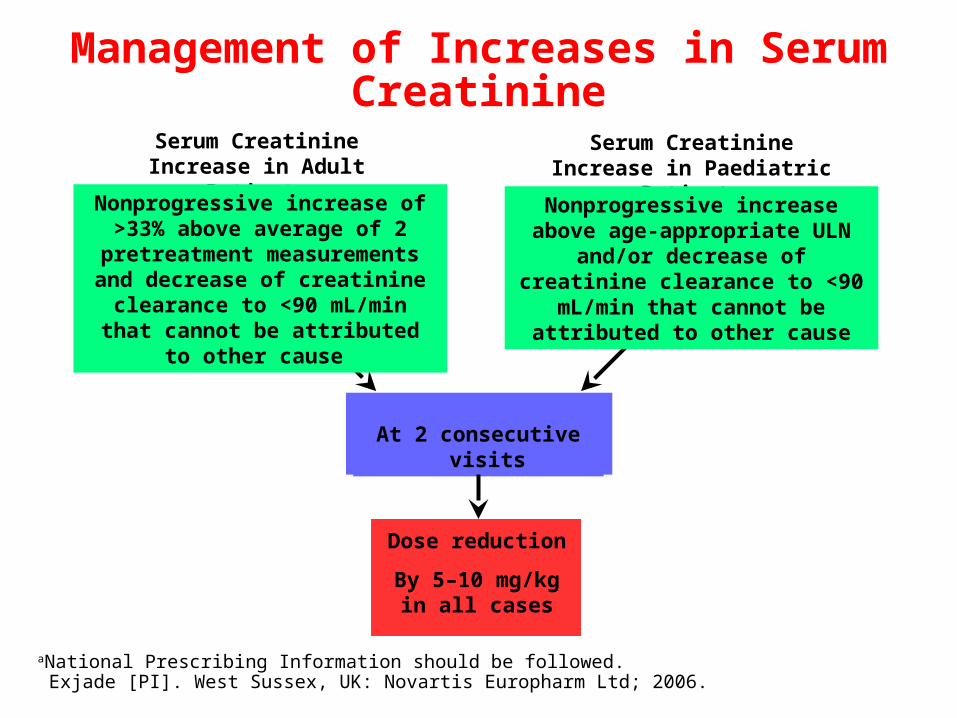
Management of Increases in Serum Creatinine
Dose reduction
By 5–10 mg/kg in all cases
Serum Creatinine Increase in Adult Patients
At 2 consecutive visits
M8.15
Serum Creatinine Increase in Paediatric Patients
aNational Prescribing Information should be followed. Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006.
Nonprogressive increase above age-appropriate ULN and/or
decrease of creatinine clearance to <90 mL/min that cannot be attributed to other cause
Nonprogressive increase of >33% above average of 2 pretreatment measurements and decrease of
creatinine clearance to <90 mL/min that cannot be attributed to other
cause
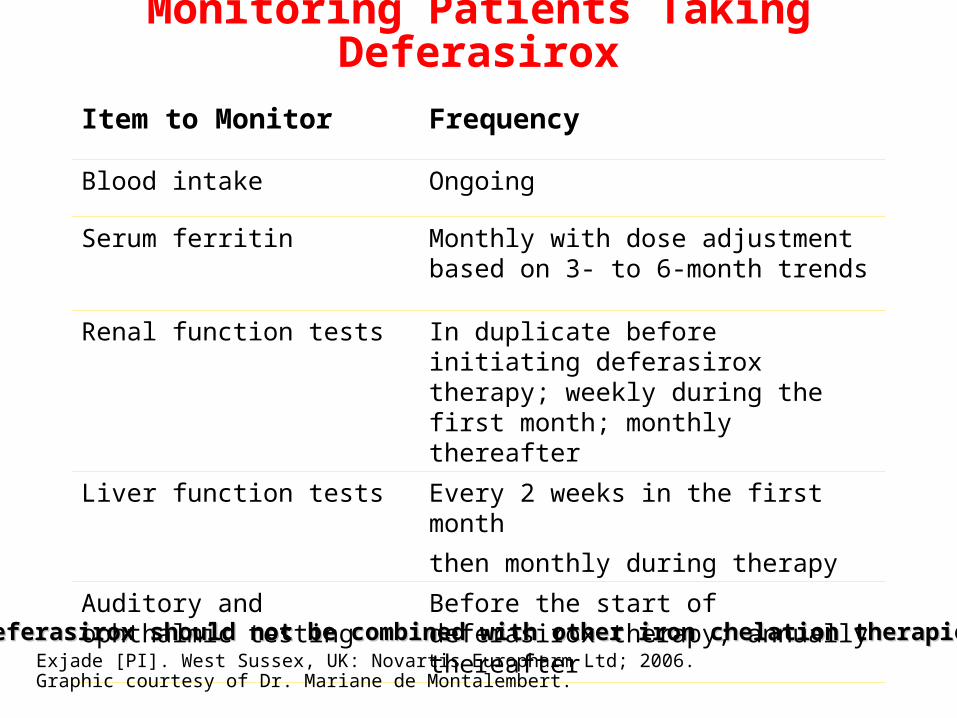
Deferasirox should not be combined with other iron chelation therapiesDeferasirox should not be combined with other iron chelation therapies
Monitoring Patients Taking Deferasirox
Item to Monitor Frequency
Blood intake Ongoing
Serum ferritin Monthly with dose adjustment based on 3- to 6-month trends
Renal function tests In duplicate before initiating deferasirox therapy; weekly during the first month; monthly thereafter
Liver function tests Every 2 weeks in the first month
then monthly during therapy
Auditory and ophthalmic testing
Before the start of deferasirox therapy; annually thereafter
Exjade [PI]. West Sussex, UK: Novartis Europharm Ltd; 2006. Graphic courtesy of Dr. Mariane de Montalembert.
Conclusion
• Prevention of iron overload allows continuation of transfusion and its clinical benefit
• Competency in chelation therapy – Knowing when to begin chelation therapy
– Knowing when and how to adjust dosage in response to adverse events (eg, GI, rash, alterations in renal function) in order to maintain patients on therapy
• Transfusional strategies may vary throughout the world but key principles are consistent