mechanical support and mobility: ecmo, iabp, and...
TRANSCRIPT

Mechanical Support and Mobility:
ECMO, IABP, and TAH
Meghan Lahart PT, DPT, CCS
Cori Shank PT, CCS
Christina Fields PT, MPT, CCS

Disclosures
• No relevant financial relationship exists with any of the
presenters in this presentation and there are no conflicts of
interest in this presentation.

Course Objectives
• 1. Be able to describe the different types of and uses for
mechanical support devices noted above.
• 2. Be aware of important safety measures for PTs related to
each device.
• 3. Be able to state indications and contraindications to
mobility for each device.
• 4. Provide cases of patients that have been successfully
mobilized using this equipment.
• 5. Open up discussion for a round table to discuss what is
working at different hospital systems that are mobilizing with
these machines
Subclavian Intra-Aortic Balloon Pump
Meghan Lahart PT, DPT, CCS
University of Chicago Medical Center
Email: [email protected]

Subclavian Intra-Aortic Balloon Pump
What is an IABP?
• First described as used for patients with cardiogenic shock
• Typically placed in the femoral artery which requires bedrest
and significant risk for lower extremity ischemia.
• Indicated for patients with
– refractory angina pectoris
– post-cardiopulmonary bypass shock
– temporizing complications of percutaneous coronary intervention
– complications of myocardial infarction refractory to pharmacologic
therapy

Patient Selection for Ambulatory IABP
• Used in patients who benefit from IABP therapy but need
ambulatory and long-term support
• Requires ICU setting
• Used as
– Bridge to transplant: status 1a
– Bridge to MCS
– Bridge to determination
– Bridge to recovery
• Post-MI or Post ECMO
• After high-risk surgery

What does an IABP do?
• Increases myocardial oxygen perfusion while increasing
cardiac output
• Increasing cardiac output therefore increases coronary blood
flow which then increases myocardial oxygen delivery
• Balloon sits in aorta
– Actively deflates during systole: increases forward blood flow by
reducing afterload
– Actively inflates during diastole: increases blood flow to coronary
arteries via retrograde flow

IABP Console
• Computer-controlled mechanism that inflates the balloon with
helium linked to an electrocardiogram or pressure transducer at
the distal tip of catheter
• Helium has low viscosity and allows it to travel quickly
through long connecting tubes as well as lower risk of causing
embolism if balloon ruptures.
• IABP augmentation can be set at 1:1, 1:2, 1:3
• Typically when using as bridge to transplant or LVAD will use
a 1:1 augmentation

IABP Console Screen

Considerations and Safety Measures
• Limit shoulder flexion on side of IABP placement to 90
degrees
• Leveling the arterial line connected to IABP when ambulating
• Ensuring that the physical therapist has undergone training so
as to leave ICU unit with patient
• Never take patient into an area where there are no outlets to
plug console in if battery starts to die
• Checking battery life frequently
Subclavian IABP UCMC
• Russo et al. JTCVS 2012;144:951-5
• 52 patients in last 3 years (duration 2-100 days)
– 34/37 successful bridge to transplant
• 3 required MCS due to worsening CHF
– 9 optimize to MCS. All implanted
– 6 planned slow wean to recovery after high-risk cardiac surgery in low EF patients. 5
discharged
• Lessons learned
– 90% showed decrease in PCWP, increased CO, increased BP allowing up-titration of
medication, renal improvement
• Need stable rhythm
– 1CVA with long term deficit during pumping – poor management of driveline rupture

Subclavian IABP Vanderbilt
• Umakanthan et al. JTCVS 2012:143;1193-7
• 18 patients 2007-2010 (duration 5-63 days)
– >50% contraindications to traditional LVADs
• Subclavian Hemashield graft, daily/aggressive ambulation
• 13/18 successful bridge to transplant
– 3 too sick for LVADs
– 1 MI
– 1 arrhythmia

Axillary IABP Methodist, Houston
• Estep et al. JACC HF 2013:V1;No 5
• 50 patients 2007-2012 (duration 4-152 days; median 18)
• Subclavian percutaneous with sheath
– Minimal ambulation
– Increased vascular complications due to approach
• 44% required re-positioning, 20% exchange
• 42/50 successful bridge to transplant
– 4 died and had contraindications for LVADs
– 3 required increased support
– 1 needed repositioning to femoral location

Axillary IABP Case


What is ECMO?
• Extracorporeal Membrane
Oxygenation (ECMO) or
Extracorporeal Life Support
(ECLS)
• The use of mechanical
devices to temporarily
support heart and/or lung
function during
cardiopulmonary failure,
allowing organ recovery or
replacement
17

PATIENT SELECTION
• Must be a reversible process.
• Patient should be placed on ECMO within first 5 days.
• Have an “exit strategy”.
• Bridge to recovery
• Bridge to transplant
• Bridge to implantable device – LVAD
• Goal of ECMO?
18
Types of ECMO Support
• Veno-arterial (VA) ECMO
–Blood is removed from a vein, circulated through a
blood pump and artificial lung, and returned to an artery
–Supports heart and lungs
• Veno-venous (VV) ECMO
–Blood is removed from a vein, circulated through a
blood pump and artificial lung, and returned to a vein
–Supports lungs only
1/12/2015 19

Indications for VA-ECMO
• Cardiogenic shock with inability to oxygenate due to
• Acute MI
• Cardiac arrest
• Decompensated heart failure
• Post-partum cardiomyopathy
• Post-cardiotomy shock
• Bridge to durable VAD/TAH support or transplant
• Absence of non-reversible organ failure
• Neurologic
• Underlying end-stage malignancies
1/12/2015 20

V-A ECMO Cannulation
• Surgeon
• At bedside or in OR
• Central cannulation
• Femoral cannulation
1/12/2015 21

Indications for VV-ECMO
• Potential reversible lung insult
• Condition consistent with ARDS
• Mechanical ventilation < 7 days
• Profound hypoxemia or hypercapnea
• Bridge to lung transplantation
• Absence of non-reversible organ failure
• Neurologic
• Underlying end-stage malignancies
1/12/2015 22
V-V ECMO Cannulation
• Surgeon
• At bedside or in OR
• Avalon Catheter – Bi-caval catheter inserted into the right
internal jugular vein.
• Blood is removed from superior and inferior vena cava and returned to the
right atrium directly at the tricuspid valve
• Femoral vein-Internal Jugular cannulation
1/12/2015 23

ECMO CIRCUIT
Main components:
• Tubing
• Gas exchange
• Blood pump
• Heat exchange

ECMO CIRCUIT

ECMO CIRCUIT

Patient Management on ECMO
• Lots of info! How long do I have?
• Support gas exchange and allow lungs to rest
• Anticoagulation…risk for bleeding!
• Prophalactic Antibiotics
• Diuretics
• Appropriate sedation and anxiety control
• Neuro checks
• Limb perfusion

Target Guidelines
The Red Book
• Temp
• pH
• pCO2
• pO2
• Hgb saturation (SpO2)
• Hgb
• INR
• Platelets
• ACT

What does that mean for me as a PT?
• Aren’t these patients too sick?
• Ambulatory ECMO??
• PT implications
What does Research say?

Lung Transplant and Ambulatory ECMO
• Pre Transplant
• IPF
• Cystic Fibrosis
• Post Transplant
• Primary Graft Dysfunction

Physical Therapy and ECMO
• Appropriateness for PT
• Plan of care
• Considerations and Safety Measures
• Center specific protocols

Appropriateness for PT
• Is the patient stable?
• Vent settings.
• Bleeding
• Vital signs
• Communication with team is crucial

Plan of Care

Considerations and safety measures
• Cannulation sites
• Ambulatory team
• Equipment
• Unexpected outcomes

Cannulation Sites
• How do you secure those big cannulas so they don’t
kink or dislodge?
• Any ideas?

Ambulatory team; the key players.
• Time for PT! Who needs to be there?
– PT
– ECMO clinician (perfusionist/RN/RT)
– RT
– RN
– Extra hands! Rehab tech, CNA, RN
– OOPS!...Let’s not leave out the docs!
• Cardiothoracic surgeon
• Intensivist/pulmonologist
• Cardiologist

Equipment
• Treadmill
– Safety precautions:
• Stationary Bike
– Safety precautions:
• Walking with a walker/standing frame/walking frame
– Safety precautions:
• Weights

Show me some action!
• video

SynCardia temporary Total Artificial
Heart
Tina Fields, PT, MPT, CCS
University of Michigan Hospital
Email: [email protected]

What is the SynCardia Total Artificial Heart
(TAH)
• A mechanical assist device for persons with biventricular heart
failure.
• Switched from animal models to human implants early 1980s
• First BTT in 1985
• To date >1,350 implants worldwide.
• Replaces both native ventricles and all four heart valves.
• Pneumatic Device -- Pulsatile
• Successful bridge to transplant in 70-80% of cases depending
on source of information.

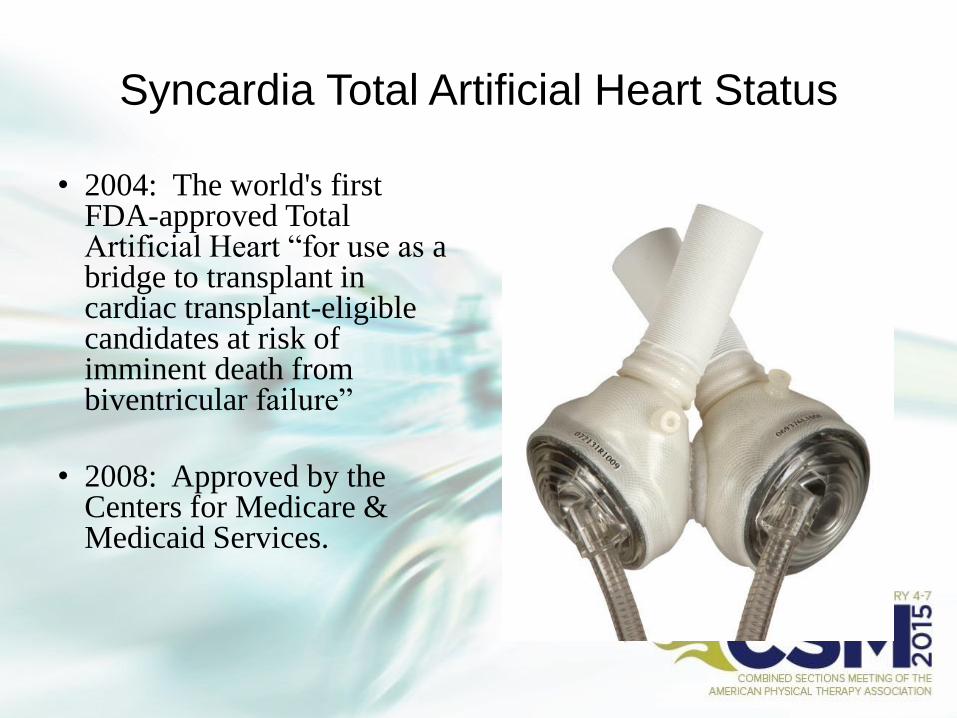
Syncardia Total Artificial Heart Status
• 2004: The world's first FDA-approved Total Artificial Heart “for use as a bridge to transplant in cardiac transplant-eligible candidates at risk of imminent death from biventricular failure”
• 2008: Approved by the Centers for Medicare & Medicaid Services.

How it works
• Replaces all 4 valves & both ventricles:
– 70cc ventricles (non compliant)
– No inotropes, ECG, CPR, Defibrillation
• Pneumatic Device:
– Airflow empties ventricles with each beat
– External Console or Driver provides air supply and power to device
when mobilizing the patient.
• Preload Dependent (goal CVP 5-10)

Candidates for TAH
• Candidates Include:
– Patients with biventricular heart failure
– Heart Transplant Candidate
– BSA >1.7m2 (3D imaging to check size)
– Must tolerate anti-coagulation
• Exclusions:
– Ineligible for heart transplant
– BSA<1.7m2
– Unable to be anti-coagulated
– Medically Unstable.

Risks of TAH
• Stroke (<2.5%)
• Infection
• Anemia (avoid transfusion)
• Bleeding (10-20% in first 24-48 hours)
• Cardiac Tamponade (can occur into recovery period)

TAH vs LVAD
• TAH:
– Is not dependent on right heart function
– No hemodynamic consequence from arrhythmias
– Minimal device to blood contact – less risk of clotting
– No issues with VSD
– Cannot be explanted
– Less oxygen demand (ventricles ~10%)
– No surgical pocket required

TAH “Vital” Signs
• Heart Rate: fixed (120 to135bpm)
• BP: (goal SBP <140)
• Oxygen Saturations: (92-100%)
• % Systole: fixed (50 to 60%)
• Vacuum: fixed (0 to -10)
• Stroke Volume: (50s-low 60s mL)
• Cardiac Output: Can be as high as 9.5L/min

Safety measures with TAH
• Ventricles should always partially fill
• Ventricles should always fully empty
• Battery Power check for transport
• Portable air tanks (~15 minutes per 1000psi)
• Avoid kinking or splitting of tubing
• No CPR or defibrillation


Thoughts for PT
• Immediate post-operative increase in Cardiac Output
• Sternotomy Precautions:
– no lift/push/pull >10
– full shoulder ROM
• Start PT POD#1 assuming hemodynamic stability.
• Monitor for partial fill & complete emptying
• Noise of device – sleep, constant reminder
• Stuck in hospital if don’t qualify for Freedom Driver

Patient Mobilization s/p TAH
• Multiple Team Players:
– Console (skilled)
– Portable Air Supply (prn)
– Lines/oxygen
– Wheelchair Follow (prn)
– Physical Assistance for mobility
– Assistive Device
• Progresssion = Aggressive
• Limitations

What is the Freedom Portable Driver?
• A wearable power supply and air compressor for the TAH
• It allows patients who are medically stable to leave the hospital
s/p TAH implant.
• To qualify patients must tolerate the Freedom Driver settings.
• 2014: The Freedom® portable driver received FDA approval
on June 26, 2014

Patient s/p TAH implantation


Freedom Portable Driver
• Weighs 13.5 lbs
• Driveline = 5 feet
• Driveline Pressures Fixed
• % Systole Set (50%)
• Vacuum Set (-10)
• HR is only adjustable
variable from 120-135.

Wearable: Backpack
Upcoming Trials
• Destination Therapy Trial:
– Device avg implant time is 6 mo to 2 years
• 50cc Ventricle Trial:
– Allow use for patients with BSA >1.1m2 (female and pediatric
patients)
– Capable of producing 4.5-6 lpm

References
Annich GM, MacLaren ed. ECMO: Extracorporeal cardiopulmonary support in
critical care 4th edition. Ann Arbor, MI: Extracorporeal Life Support Organization;
2012.
Turner DA, Cheifetz IM, Rehder KJ et al. Active rehabilitation and physical therapy
during extracorporeal membrane oxygenation while awaiting lung transplantation: a
practical approach. Crit Care Med. 2001; 39(12):2593-8.
Garcia JP, Kon ZN, Evans C et al. Ambulatory veno-venous extracorporeal membrane
oxygenation: innovation and pitfalls. J Thorac Cardiovasc Surg. 2011; 142(4):755-61.
Javidfar J, Brodie D, Iribarne A et al. Extracorporeal membrane oxygenation as a
bridge to lung transplantation and recovery. J Thorac Cardiovasc Surg. 2012; 144(3):
716-21.
Hayes D, Kukreja J, Tobias J et al. Ambulatory venovenous extracorporeal respiratory
support as a bridge for cystic fibrosis patients to emergent lung transplantation. J
Cystic Fibrosis. 2012; 11(1): 40-45.
References
• Maccioli GA, Lucas WJ, Norfleet EA. The intra-aortic balloon pump: a review. J Cardiothorac Aneth.
1988;2:365-73.
• Mayer JH. Subclavian artery approach for insertion of intraaortic balloon. J Thorac Cardiovasc Surg. 1978;
76-61-3.
• Cochran RP, Starkey TD, Panos AL, Kunzelman KS. Ambulatory intra-aortic balloon pump use as bridge to
heart transplant. Ann Thorac Surg. 2002;74:746-52.
• Raman J, Loor G, London M, Jolly N. Subclavian artery access for ambulatory balloon pump insertion. Ann
Thorac Surg. 2010;90:1032-4.
• Russo MJ, Jeevanandam V, Stepney J, et al. Intra-aortic balloon pump inserted through the subclavian
artery: a minimally invasive approach to mechanical support in the ambulatory end-stage heart failure
patient. J thorac Cardiovasc Surg 2012;144:951-5.
• Estep JD, Cordero-Reyes AM, Bhimaraj A, Trachtenberg, B et al. Percutaneous placement of an intra-aortic
balloon pump in the left axillary/subclavian position provides safe, ambulatory long-term support as bridge
to heart transplantation. JACC 2013; 5:382-8.

References
• Copeland, Jack G, MD. SynCardia Total Artificial Heart: Update and Future. Tex
Heart Inst J. 2013; 40(5): 587–588.
• Fernandez, N, Ford K. Early Progressive Mobilization and Physical Therapy
Management in a patient with a Total Artificial Heart Device. Cardiopulmonary
Physical Therapy Journal. March 2014.
• Miessau J, Yang Q, Unai S, Entwistle J, Cavarocchi N, Hirose H. Veno-venous
extracorporeal membrane oxygenation using a double-lumen bi-caval cannula for
severe respiratory failure post total artificial heart implantation.” Perfusion. Sept
2014.
• Spiliopoulos S, Dogan G, Guersoy D, Serrano MR, Koerfer R, Tenderich G. Veno-
venous extracorporeal membrane oxygenation with a bicaval dual-lumen catheter in
a SynCardia total artificial heart patient. Journal of Cardiothoracic Surgery
2013;8:179. doi:10.1186/1749-8090-8-179.
• Torregrossa G, Anyanwu A, Zucchetta F and Gerosa G. Syncardia: The Total
Artificial Heart. Ann Cardiothorac Surg. Nov 2014; 3(6): 612–620.
• www.syncardia.com