nicotine replacement therapy in the intensive care unit a...
TRANSCRIPT

Nicotine Replacement Therapy in the Intensive Care Unit
A Randomized Controlled Pilot Study
Report Research Clerkship
Anne Schuppers
University of Groningen
S2016575
Faculty and daily supervisor: Second supervisor:
H. van den Oever, MD B. de Jong, MD
Deventer Hospital Gelderse Vallei Hospital Ede
Department of Intensive care Department of Intensive care
Presently Radboudumc Nijmegen
Co-investigators: Department of Intensive care
M. Arbouw, PhD
Deventer Hospital Co-investigator:
Department of Clinical Pharmacy A. R. H. van Zanten, MD, PhD
A. Kruisdijk-Gerritsen, ICU nurse Gelderse Vallei Hospital Ede
Deventer Hospital Department of Intensive care
Department of Intensive care

2
Table of contents
Table of contents......................................................................................................................2
Abstract (English)....................................................................................................................3
Abstract (Nederlands).............................................................................................................4
List of abbreviations................................................................................................................5
Introduction.............................................................................................................................6 Delirium and nicotine withdrawal
Nicotine replacement therapy (NRT)
Metabolism of nicotine
Previous studies in critically ill patients
Aim of the study.......................................................................................................................8
Materials and methods............................................................................................................9
Trial design
Participants
Randomisation
Blinding
Data collection
Data analysis
Statistical methods
Ethics approval
Results......................................................................................................................................13
Study progress
Baseline characteristics
Primary outcome parameter
Secondary outcome parameters
Safety evaluation
Outcome parameters defined post hoc
Discussion.................................................................................................................................20
Summary of main findings
Strengths and weaknesses
Conclusion................................................................................................................................22
Recommendations
Acknowledgements..................................................................................................................23
References................................................................................................................................24
Appendix..................................................................................................................................27
1 AUDIT test om alcoholafhankelijkheid te meten
2 Test van Fagerström om nicotineafhankelijkheid te meten
3 Charlson Comorbidity index
4 SOFA SCORE, The APACHE II score and The APACHE IV score
5 Sample size calculations
Supplementary figures............................................................................................................33

3
Abstract (English)
Nicotine Replacement Therapy in the Intensive Care Unit; a Randomized Controlled
Pilot Study
Introduction:
Delirium and agitation are common in mechanically ventilated patients admitted to the
intensive care unit (ICU). Retrospective data have shown that smoking, or the acute
abstinence of smoking, is an additional risk factor for agitation. A safe and effective method
to treat nicotine withdrawal symptoms in outpatient and hospitalized smoking adults is
transdermal nicotine replacement therapy (NRT). Previous studies on the use of transdermal
NRT in critically ill smokers admitted to the ICU have produced conflicting results.
The aim of this study was to assess the safety and efficacy of transdermal NRT in
mechanically ventilated smokers admitted to the ICU.
Methods:
In this two-centre, randomized, controlled pilot study, mechanically ventilated smokers
admitted to the ICU were included. Subjects received either a nicotine patch (14 or 21
mg/day) or a placebo patch daily until ICU discharge or for a maximum of 30 days. The
primary outcome was 30-day mortality. Secondary outcomes included 90-day mortality,
length of stay, duration of ventilation, delirium, RASS score, SOFA score, hours of physical
restraint, incidence of new nosocomial infections, number of self-removed devices and
number of (serious) adverse events. We performed a post hoc analysis and defined the
outcome parameter as time spent in a favourable condition (alive without sedation and
delirium in the ICU) during the first 30 days.
Results:
Due to recruitment failure the study was stopped after the inclusion of 47 patients. The two
groups were comparable with respect to baseline characteristics. No differences were found in
30-day mortality and 90-day mortality between NRT and the control group (2/21 vs. 2/26;
p=0.843 and 3/21 vs. 5/26; p=0.665). During the first 10 days the NRT group had spent more
time in a ‘favourable’ condition (160 hours (96-216) vs. 88 hours (20-210) (p=0.043)) and
during the first 20 days (400 hours (316-448) vs. 304 hours (110-432) (p=0.033)).There was
no difference in the number of adverse and serious adverse events between NRT and control
patients (102 vs. 177 (p=0.096) and 5 vs. 11 (p=0.251)).
Conclusion:
The results of this pilot study showed that with some modifications of the trial design, a
randomized controlled study to assess the safety and efficacy of transdermal NRT in
mechanically ventilated smokers admitted to the ICU is feasible. Transdermal NRT in
mechanically ventilated smokers had no effect on 30- and 90-day mortality, although our
study was underpowered to establish such differences. Furthermore, the number of (serious)
adverse events between the two groups were comparable. Finally, patients with NRT spent
more time in a ‘favourable’ condition during the first 20 days of admission to the ICU. We
suggest that future trials should focus on a possible effect of NRT on predefined delirium and
agitation endpoints, particularly in the second and third week of ICU stay.
4
Abstract (Nederlands)
Nicotine vervangende therapie op de intensive care; een gerandomiseerde,
gecontroleerde pilotstudie
Introductie:
Delirium en agitatie zijn veelvoorkomend bij beademende intensive care (IC) patiënten.
Retrospectieve studies hebben aangetoond dat roken, of het acuut abstineren van roken, een
extra risicofactor is voor agitatie. Nicotine vervangende therapie is een veilige en effectieve
manier om nicotine ontwenningsverschijnselen te behandelen bij volwassen rokers binnen en
buiten het ziekenhuis. Eerdere studies naar het gebruik van transdermale nicotinevervangende
therapie bij ernstig zieke rokers opgenomen op de IC hebben tegenstrijdige resultaten laten
zien.
Het doel van onze studie was om de veiligheid en werkzaamheid van transdermale nicotine
vervangende therapie bij beademende IC patiënten te beoordelen.
Methoden:
Beademende rokers die opgenomen lagen op de IC werden geïncludeerd in deze
gerandomiseerde, gecontroleerde pilotstudie uitgevoerd in twee centra. Proefpersonen kregen
dagelijks een nicotinepleister (14 of 21 mg/dag) of een placebo pleister gedurende hun IC
opname of voor een maximale duur van 30 dagen. De primaire uitkomstmaat was 30-dagen
mortaliteit. Secondaire uitkomstmaten waren 90-dagen mortaliteit, opnameduur,
beademingsduur, delirium, RASS score, SOFA score, aantal uren fixatie, incidentie van
nieuwe nosocomiale infecties, aantal zelfverwijderde tubes en lijnen en aantal (ernstig)
ongewenste medische voorvallen. Een gecombineerde post-hoc uitkomstmaat werd
gedefinieerd als tijd levend doorgebracht zonder sedatie of delirium op de IC gedurende de
eerste 30 dagen.
Resultaten:
Na 47 patiënten is de studie gestopt als gevolg van moeizame inclusie. De twee groepen
waren vergelijkbaar met betrekking tot basiskarakteristieken. Er werd geen verschil gevonden
in 30-dagen en 90-dagen mortaliteit tussen de behandelde groep en de controle groep (2/21
vs. 2/26; p=0.843 and 3/21 vs. 5/26; p=0.665). Gedurende de eerste 10 dagen had de
behandelde groep meer tijd levend doorgebracht zonder sedatie of delirium (160 uren (96-
216) vs. 88 uren (20-210) (p=0.043)) en in de eerste 20 dagen (400 uren (316-448) vs. 304
uren (110-432) (p=0.033)). Er was geen verschil met betrekking tot het aantal ongewenste en
ernstige, ongewenste medische voorvallen tussen de behandelde groep en de controle groep
(102 vs. 177 (p=0.096) and 5 vs. 11 (p=0.251)).
Conclusie:
Op basis van de resultaten van deze pilotstudie is een gerandomiseerde, gecontroleerde studie
om de veiligheid en werkzaamheid van transdermale nicotine vervangende therapie bij
beademende IC patiënten te beoordelen haalbaar. Transdermale nicotine vervangende therapie
had geen effect op 30-dagen en 90-dagen mortaliteit bij beademde rokers, hoewel onze studie
onvoldoende power had om dergelijke verschillen vast te stellen. Het aantal (ernstig)
ongewenste medische voorvallen was vergelijkbaar tussen de twee groepen. Gedurende de
eerste 20 dagen brachten patiënten in de behandelde groep meer tijd door zonder delirium of
sedatie. Het is aan te raden om in toekomstige studies de focus te leggen op een mogelijk
effect van nicotinevervangende therapie op vooraf gedefinieerde delirium en agitatie
uitkomstmaten en dan voornamelijk gedurende de tweede en derde week van een IC opname.

5
List of abbreviations
AE Adverse Event
APACHE Acute Physiology and Chronic Health Evaluation
AUDIT Alcohol Use Disorders Identification Test (1)
BMI Body Mass Index
CAM-ICU Confusion Assessment Method for the Intensive Care Unit
CI Confidence Interval
DOS Delirium Observation Screening
DH Deventer Hospital
FTND Fagerström Test for Nicotine Dependence
ICU Intensive Care Unit
IQR Interquartile range
ITT Intention-to-treat
NPPV Non-invasive Positive Pressure Ventilation
NRT Nicotine Replacement Therapy
OR Odds Ratio
RASS Richmond Agitation-Sedation Scale
SAE Serious Adverse Event
SD Standard Deviation
SOFA Sequential Organ Failure Assessment
GVH Gelderse Vallei Hospital

6
Introduction
Delirium and nicotine withdrawal
Delirium is a disturbance in attention, awareness and cognition which develops over a short
period and fluctuates over time (2). Two types of delirium are recognized, a hypoactive and
hyperactive form (3). Many factors can contribute to the emergence of delirium, including
alcohol abstinence, acute illness or changes in medication (4). An association between
enforced nicotine abstinence, agitation, and (hyperactive) delirium has been suggested by
several authors (5-7). However, it remains unclear whether this should be seen as
(hyperactive) delirium provoked by enforced nicotine abstinence, or nicotine withdrawal with
a similar symptomatology (confusion, restlessness and irritability) not sufficient to meet the
criteria of delirium (8). The incidence of delirium in the general ICU population is
approximately 32 percent (9) and may rise as high as 89 percent when mechanically
ventilated patients are considered (10,11). Delirium has been associated with increased
mortality (9,10,12), greater need for sedatives (13), physical restraints (13), extended duration
of mechanical ventilation and in-hospital/ICU stay (9,10,12) and therefore prevention is
considered important. Patients smoking ≥ 10 cigarettes per day have a significantly increased
risk of developing delirium (14). The prevalence of smoking in ICU patients is estimated at
20-57 percent (15-19). It is generally believed that nicotine abstinence can lead to withdrawal
symptoms, including difficulty concentrating, insomnia, agitation and physical complains (20-
22). These symptoms generally peak within the first week and continue for 2 to 4 weeks (23).
Although the symptoms of nicotine abstinence are non-life threatening in outpatient and
hospitalized adults, their role in the mental processes of mechanically ventilated patients is
not well understood (24).
Nicotine replacement therapy (NRT)
NRT is a safe and effective method to treat nicotine withdrawal symptoms in smoking healthy
and hospitalized adults (25-27). It might be plausible to assume that nicotine withdrawal
symptoms also play a role when actively smoking patients are mechanically ventilated, and
that these patients therefore would benefit from NRT. A reduction of symptoms of nicotine
withdrawal could prevent self-removal of tubes and catheters, need for supplemental
medication and physical restraints (6). On the other hand, nicotine is a potentially harmful
drug and if replacement does not prevent withdrawal symptoms and/or delirium, its side
effects might actually cause harm. In order to prevent or ease nicotine withdrawal symptoms
transdermal NRT is a potential option because it provides relatively constant withdrawal relief
over 24 hours (28). It has been used in hospitalized smokers in whom it immediately
alleviated or remedied withdrawal symptoms (29). Common side effects related to NRT
products reported in the general population include local irritation, headache, vertigo,
insomnia and gastrointestinal symptoms (21,22,30).
Metabolism of nicotine
Approximately 80 to 90 percent of nicotine is metabolized by lung, liver and kidney (31) and
17 percent of nicotine is excreted unchanged in the urine (32). Cotinine is a metabolite of
nicotine and is used as a biomarker of nicotine exposure. The plasma concentration of
cotinine is 10 times higher than nicotine. The half-life of cotinine is 15 to 20 hours (31).
7
Previous studies in critically ill patients
Some authors have reported beneficial effects of NRT in patients admitted to the ICU. One of
the success stories was a case series describing 5 smokers admitted to the neuro-ICU, who
developed an agitated delirium 2 to 10 days after smoking cessation and showed improvement
after placement of a 21 mg nicotine patch (7). It was recognized that the risk of selection bias
was considerable. Soon, several retrospective cohort studies, evaluating NRT in ICU patients,
appeared in the literature. In general, these were not supportive of NRT. In a cohort of
neurosurgical ICU patients, Panos et al. showed that smokers receiving NRT had longer ICU
stay and hospital stay than smokers who did not receive NRT or nonsmokers (33).
Prevalences of delirium or agitation were not reported in that study. The issue of agitation was
addressed in two other studies. The group of Kerr et al. (34) did a case-control study,
comparing smokers who received NRT to smokers who did not. They found that NRT treated
patients were intubated longer, and required more antipsychotic medication and physical
restraints. These results seemed to match well with the observations described by Seder et al.,
who found more delirium and more seizures in a neuro-ICU cohort of smokers who had
received NRT, compared to an untreated cohort (35). These latter two studies also looked at
mortality. There was no mortality difference in the Kerr study and, quite remarkably, in the
Seder study, despite the higher incidence of delirium, NRT was associated with a survival
benefit through multivariate analysis (34,35). In contrast with the Seder study, Lee and Afessa
showed data from a case-control study in their medical ICU, which quite convincingly
demonstrated increased mortality in active smokers treated with NRT (36). A trend towards
increased mortality was also found in the intervention group in actively smoking coronary
artery bypass graft surgery patients admitted to an ICU (37). A retrospective cohort study in a
mixed ICU, done by Gillies et al., showed that in terms of mortality, smokers receiving NRT
fared neither worse, nor better, than smokers without NRT (38). A prospective observational
study by Cartin-Ceba, looking at smokers admitted to a medical ICU with and without NRT,
also showed similar mortality rates (39).
These nonrandomized studies, whether focussing on delirium and agitation, or on mortality,
all suffer from the same potential bias: it is not known why some smokers were prescribed
NRT and others not. It might be that some received NRT because they were already agitated
or because it was recognized that they were more prone to delirium. Perhaps a higher risk of
mortality was appreciated early on, which may have influenced the decision to pre-emptively
treat against nicotine withdrawal symptoms. However, this respectable body of retrospective
research cleared the way for randomized studies.
One single-centre, randomized double-blind pilot study has been published today. The results
showed a trend towards decrease in ICU stay and duration of mechanical ventilation in the
NRT group, although this was not statistically significant. However, this was a pilot study
with a small sample size (40 subjects) (40).
Two systematic reviews in 2014 and 2016 concluded that there is no consensus on whether
NRT is a safe and effective method to prevent or treat nicotine withdrawal symptoms in
critically ill smokers. They suggested that powered randomized controlled trials are needed
with regards to the use of NRT to prevent, ease, or treat delirium and agitation in patients
admitted to the ICU (41,42).

8
Aim of the study
Previous studies on the use of transdermal NRT in critically ill smokers admitted to the ICU
have produced conflicting results and have been mainly retrospective which made them
vulnerable to selection bias and confounding. There is a need for randomized, controlled
research.
We set out to conduct a two-centre pilot study to investigate whether a randomized controlled
trial would be feasible.
The objective of this study was to assess the safety and efficacy of transdermal nicotine
replacement therapy in mechanically ventilated smokers admitted to the ICU.
The following hypothesis was tested:
H0: the effect of transdermal nicotine replacement therapy is equal to the effect of the control
product with respect to 30-day mortality in mechanically ventilated smokers admitted to the
ICU.

9
Materials and methods
Trial design
A two-centre, randomized, controlled, double-blind, parallel-group, pilot study was
conducted.
Participants
Mechanically ventilated smokers admitted to the ICU in two centres (Deventer Hospital (DH)
and Gelderse Vallei Hospital (GVH), the Netherlands) were included in this study. Table 1
shows the inclusion and exclusion criteria. Eligible patients or their legal representatives were
informed about the study and gave written consent. When surrogate consent was obtained, the
patient was requested to confirm the consent in writing when approachable and accountable.
The number of patients screened for inclusion was not recorded, although every mechanically
ventilated smoker admitted to the ICU had been screened.
Table 1. Inclusion and exclusion criteria. Inclusion criteria Exclusion criteria
- ≥ 18 years
- Understanding Dutch
- Critically ill smokers
- Being mechanically ventilated
- Start of study product application within 48
hours after ICU admission
- Mechanical ventilation was expected to be
continued for > 48 hours from the start of the
study onwards
- Written informed consent must be obtained
from each subject or legal representative
- Cardiovascular diseases*
- Chronic dementia or psychosis
- (Acute) neurologic disease
- Hearing deficiency
- Moribund
- Pregnant or breastfeeding woman
- Last cigarette smoked > 72 hours before
admission
- NRT within two weeks before admission
- Skin diseases interfering with NRT
absorption
- Hyper sensibility to nicotine or components
of the transdermal therapeutic system
- Participating in another study
* Acute myocardial infarction, severe cardiac arrhythmia, unstable/deteriorating angina pectoris.
Randomisation Participants were randomly allocated to receive either the test product or the control product
in a 1:1 ratio by block randomisation in groups of four, stratified to patient type (medical vs.
surgical), study site (GVH vs. DH) and nicotine dosage (14 vs. 21 mg/day). A randomisation
list, developed by using a computer random number generator, was kept at the hospital
pharmacy. Randomisation codes were unknown to the investigator and site staff. Details of
the product codes were contained in a set of opaque sealed code envelopes.
Blinding
Participants received either a transdermal nicotine patch (Nicotinell, Novartis Consumer
Health) or a nontransparent plaster similar in size, shape, and colour until ICU discharge or
with a maximum of 30 days. The dosage of the test product was aligned with the amount of
cigarettes smoked on a daily bases as indicated by the participant or next of kin. Participants
smoking ≤ 20 cigarettes per day were given 14 mg nicotine per 24 hours and participants
smoking ≥ 21 cigarettes per day were given 21 mg nicotine per 24 hours. Subsequently, a non
transparent plaster was used to cover the transdermal nicotine patch. The plasters were
exchanged by nurses not involved in the daily care of the participants. In GVH nurses from
the lung department exchanged the plasters. In DH, this was done by registered nurses from
the ICU, who were solely devoted to management tasks during the week and by nurses from
the coronary care unit (CCU) on weekends.

10
Start of study product application occurred within 48 hours after ICU admission.
There were no restrictions in any other treatment modalities except the use of nicotine
replacement therapy for both the test group and control group.
Data collection
Baseline
Patients characteristics were collected at baseline, including age, sex, and body height and
weight (in order to calculate Body Mass Index (BMI)). Next of kin were interviewed using
the Alcohol Use Disorders Identification Test (AUDIT) to assess alcohol consumption,
drinking behaviour, and alcohol-related problems (Appendix 1), and the Fagerström Test for
Nicotine Dependence to evaluate the quantity of cigarette consumption, the compulsion to
use, and dependence (Appendix 2). Admission diagnosis, patient type (medical vs. surgical)
and comorbidities according to the Charlson Comorbidity index were also recorded (Appendix
3). A pregnancy test was conducted for women with childbearing potential. Sequential Organ
Failure Assessment (SOFA) score on admission, Acute Physiology and Chronic Health
Evaluation (APACHE) II and APACHE IV scores were determined over the first 24 hours
after ICU admission (Appendix 4). In order to determinate serum cotinine concentrations,
blood samples were gathered before the start of the study product application.
Intervention period (day 0 - day 30)
The following assessments were performed daily: SOFA score, hours of physical restraints,
self-removed devices, duration of mechanical ventilation, serious adverse events and adverse
events, new nosocomial infections according to the CDC definitions (43,44), and total dosage
of antipsychotics. RASS score (agitation/sedation score), CAM-ICU score and DOS score
(delirium scores) were expressed as hours. Because sedation and delirium were measured
three times per day (once per nursing shift) numbers of hours resulted in multiples of eight.
Follow up (day 90)
Patient location and survival status was confirmed by telephone interviews with the patient or
their legal representative to document mortality, length of stay (ICU, in-hospital) and patient
location (ICU, in-hospital, care facility, home or death).
Data analysis
Outcome parameters predefined in the study protocol
The primary outcome parameter was 30-day mortality.
Secondary outcome parameters included 90-day mortality, ICU and in-hospital mortality,
length of stay and patient location at day 30 and 90, total maximum SOFA score (summing
the worst scores for each of the organ systems) (45), delta SOFA score (total maximum SOFA
score minus total SOFA score) at admission (46), RASS score (median, highest, lowest, and
number of hours scored outside the optimal range, defined as <-3 and/or >1, ventilation-free
hours starting 48 hours after extubation or stop non-invasive positive pressure ventilation
(NPPV), the number of hours with delirium assessed by CAM-ICU score or DOS score, hours
of physical restraint, number of self-extubations (tube and tracheal cannula), self-removed
catheters (urinary catheter, venflon, arterial catheter, central line, nasogastric tube), new
nosocomial infections, total dosage of antipsychotics and number of serious adverse events
and adverse events.

11
Outcome parameter defined after data analysis
A post hoc outcome parameter was created and defined as time (hours) spent in a ‘favourable’
condition (discharged from the ICU or alive without sedation and without delirium in the
ICU) or ‘unfavourable’ condition (sedated, delirious or death). These parameters were
measured during the first 30 days for each individual subject after admission to the ICU or till
discharge to the general ward. Delirium was recorded by using the CAM-ICU score or DOS
score and sedation based on the RASS score. A subgroup analysis dosage-effect relationship
was performed on this composite endpoint parameter.
Statistical methods
Sample size
The combined mortality among smokers and non-smokers on the ICU was estimated to be
about 13% (data GVH). Assuming a higher mortality in smokers than in non-smokers and a
decrease in mortality due to NRT, we calculated that 485 patients per group would be needed
to detect a reduction in mortality from 20% to 15% (using a significance level (α) of 0.05, and
a power of 80%). This would not be feasible within two years. The number of hours of
admission or mechanical ventilation could have been an outcome parameter, but would
require more than 250 or 450 patients. Overseeing these large sample sizes we concluded that
a randomized controlled trial would not be possible within the two ICUs involved. For this
reason we chose to conduct a pilot study with 70 subjects, 35 patients per study arm.
Statistical analysis
Descriptive statistics were used to compare the groups at baseline.
Data were presented as mean (±SD) or median (IQR) depending on their distribution.
Each parameter was tested for normality. Student’s t-test was used to analyse differences
between continuous data which were normally distributed and the Mann-Whitney U test was
used when data were not normally distributed. To analyse categorical data we used the
Fisher’s exact or the Chi-Square test. Survival analysis was assessed by using Kaplan-Meier
curves using the log-rank test. The primary outcome parameter was subjected to logistic
multivariate analysis, in which the stratification variables (patient type, nicotine dosage and
study site) were included (47). A p-value < 0.05 was considered significant.
Data were collected in a database using Microsoft Office Access 2007 and were analysed
using IBM SPSS Statistics 22 on an intention-to-treat (ITT) basis.
Ethics approval
The study was approved by the Medical Research Ethics Committee of the University
Medical Centre Utrecht.

12
Schematic diagram of trial design.

13
Results
Study progress
After enrolment of 48 patients from July 2012 to June 2016 the study was stopped due to
recruitment failure. One patient was excluded from the study at her own request and the data
were removed from the analysis, resulting in 47 patients remaining for analysis: 21(45%) in
the NRT group and 26 (55%) in the control group. GVH included 26 patients and DH 21
patients. Median time from ICU admission until the start of the study was 38 hours (IQR 22-
48). 3.2% of the delirium and agitation/sedation scores were missing, however by screening
the electronic record files and by clinical reasoning complete records were available for all
cases with regards to the outcome parameters. Protocol violation was recorded in one patient
in the control group refusing the patch since day two after the start of the study and in one
patient in the NRT group receiving a placebo patch instead of a nicotine patch for one day.
The number of patients screened and the reasons for exclusion were not formally recorded.
However, the perception was that because of the contraindication of cardiovascular diseases
(indistinctness regarding unstable angina pectoris or increased cardiac enzymes secondary to
critical illness), as well as language barrier and mental deficit, many patients were excluded.
Presumably, the absence of the principal investigator in GVH during the last phase of the
study period caused a significant decrease in the number of inclusions. Data on the number of
ventilated patients and number of enrolled patients per ICU per year are listed in Table 1.
Table 1. Number of ventilated patients and number of enrolled patients per location. DH, 12 ICU beds GVH, 17 ICU beds
Year Ventilated patients Inclusions Ventilated patients Inclusions
2012-2013 317 0* 516 15
2013-2014 297 8 461 8
2014-2015 292 6 464 2
2015-2016 211 7 474 1
*Inclusion in DH was started ± 1 year after GVH.
Baseline characteristics
The two groups were comparable with respect to baseline characteristics.
Baseline characteristics are presented in Table 2. Data on alcohol units per day were missing
for 3 patients. There were 5 missing scores on the AUDIT test and 2 on the Fagerström test.
14
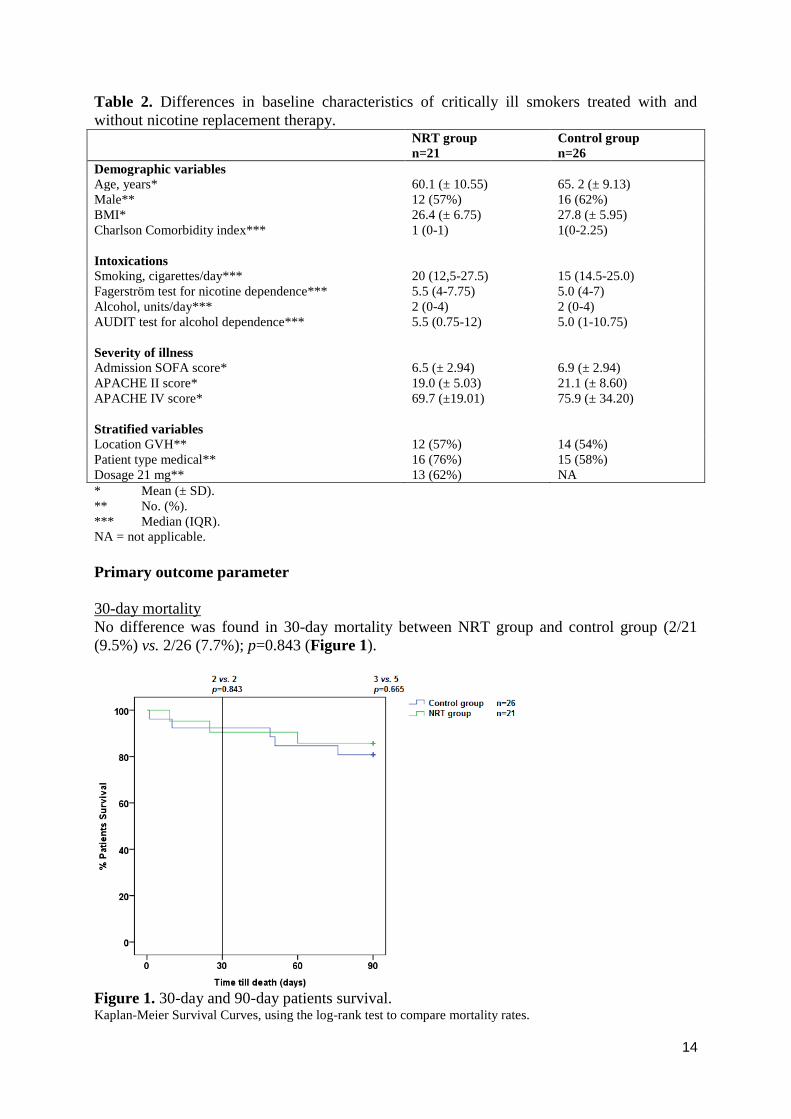
Table 2. Differences in baseline characteristics of critically ill smokers treated with and
without nicotine replacement therapy. NRT group
n=21
Control group
n=26
Demographic variables
Age, years* 60.1 (± 10.55) 65. 2 (± 9.13)
Male** 12 (57%) 16 (62%)
BMI* 26.4 (± 6.75) 27.8 (± 5.95)
Charlson Comorbidity index*** 1 (0-1) 1(0-2.25)
Intoxications
Smoking, cigarettes/day*** 20 (12,5-27.5) 15 (14.5-25.0)
Fagerström test for nicotine dependence*** 5.5 (4-7.75) 5.0 (4-7)
Alcohol, units/day*** 2 (0-4) 2 (0-4)
AUDIT test for alcohol dependence*** 5.5 (0.75-12) 5.0 (1-10.75)
Severity of illness
Admission SOFA score* 6.5 (± 2.94) 6.9 (± 2.94)
APACHE II score* 19.0 (± 5.03) 21.1 (± 8.60)
APACHE IV score* 69.7 (±19.01) 75.9 (± 34.20)
Stratified variables
Location GVH** 12 (57%) 14 (54%)
Patient type medical** 16 (76%) 15 (58%)
Dosage 21 mg** 13 (62%) NA
* Mean (± SD).
** No. (%).
*** Median (IQR).
NA = not applicable.
Primary outcome parameter
30-day mortality
No difference was found in 30-day mortality between NRT group and control group (2/21
(9.5%) vs. 2/26 (7.7%); p=0.843 (Figure 1).
Figure 1. 30-day and 90-day patients survival. Kaplan-Meier Survival Curves, using the log-rank test to compare mortality rates.

15
Secondary outcome parameters
90-day mortality
No difference was found in 90-day mortality between NRT group and control group (3/21
(14.3%) vs. 5/26 (19.2%) p=0.665) (Figure 1). Four patients died during their ICU stay, one
(5%) in the NRT group and three (12%) in the control group (p=0.617).
Length of stay
The median ICU stay at 30 days was 186 hours in the NRT group (IQR 127-278) vs. 246
hours in the control group (IQR 88-694), which was not significantly different. The median
length of stay at day 90 was similar, and was not significantly different between the groups
(Figure 2A).
2A p=0.410 p=0.392
The median hospital stay at 30 days was 313 hours (IQR 226-528) in the NRT group vs. 408
hours (IQR 220-720) in the control group. The median hospital stay at day 90 was similar,
except for the IRQ of the control group (220-885) (Figure 2B).
2B p=0.356 p=0.369
Figure 2. Length of stay in the Intensive Care Unit (Figure 2A) and in the hospital (Figure
2B) at day 30 and day 90. Median (IQR), lowest value and highest value, using the Mann-Whitney U test to compare the medians.
Mechanical ventilation There was no significant difference in mechanical ventilation-free hours between the two
groups at day 30 (Table 3). 17 patients (81%) in the NRT received respiratory support for
more than 48 hours and 20 patients (77%) in the control group. In the NRT group two patients
(9.5%) and in the control group one patient (3.8%) received only non-invasive ventilation.

16
Sequential Organ Failure Assessment (SOFA) score
There was no significant difference in the total maximum SOFA score and the delta SOFA
score between the NRT group and the control group as presented in Table 3.
Table 3. Secondary outcome parameters. NRT group
n=21
Control group
n=26
p-value
(2-tailed)
Mechanical ventilation
Mechanical ventilation-free hours at day 30* 559 (494-605) 515 (135-606) 0.152
SOFA score
Total maximum SOFA score** 7.6 (3,0) 8.2 (3,0) 0.462
Delta SOFA score* 1.0 (0.0-2) 0.5 (0-2.25) 0.982
Delirium
Hours with delirium* 8 (0-44) 16 (0-86) 0.274
RASS score
Mean RASS score* -1.0 (-2.1/-0.2) -1.3 (-2.3/-0.7) 0.266
Highest RASS score* 1 (0-1) 1 (0/1) 0.615
Lowest RASS score* -4 (-5/-2.5) -5 (-5/-4) 0.132
Hours RASS score outside optimal range* 40 (0-64) 48 (14-122) 0.202
Physical restraints
Hours of physical restraints* 12.0 (0-85.5) 44.5 (0-123) 0.417
Number of self-removed devices
Self-extubations*** 1 4 0.245
Self-removed catheters*** 24 36 0.886
Number of new nosocomial infections*** 7 22 0.285
Total dosage of haloperidol (mg)* 9 (0-24.5) 19.5 (3.25-31) 0.185
* Median (IQR), the Mann-Whitney U test was used to compare the two groups.
** Mean (±SD), using the Student’s t-test to compare means.
*** Group differences were tested with the Mann-Witney U test.
SOFA score = Sequential Organ Failure Assessment.
RASS score = Richmond Agitation-Sedation Scale.
Delirium, agitation and sedation
Hours with delirium assessed by the CAM-ICU score and DOS score were not significantly
different between the NRT group and the control group (Table 3).
When comparing the Richmond Agitation-Sedation Scale (RASS) score between the two
groups there were no significant differences in mean, highest and lowest RASS score and
hours RASS score outside optimal range (< -3 and/or > +1) (Table 3).
There was no significant difference in the hours of physical restraints (Table 3).
Self-removed devices and new nosocomial infections
No significant differences were found between the two groups when comparing number of
self-extubations (tube and tracheal cannula), self-removed catheters (urinary catheter,
intravenous cannula, arterial catheter, central line, nasogastric tube) and new nosocomial
infections (Table 3).

17
Total dosage of antipsychotics
The median dosage of haloperidol was not significantly different between the two groups,
9.0 mg (IQR 0.0-24.5) in the NRT group and 19.5 mg (IQR 3.25-31.0) in the control group
(p=0.185) within the first 30 days (Table 3). In addition, one patient in the NRT group
received 120 mg of olanzapine and one patient in the control group 17.5 mg, none of the
patients received quetiapine.
Patient location on day 30 and day 90
At day 30, there was a significant difference in patient location between the two groups. In
the NRT group, more patients were in a care facility or at home as compared to the control
group (more patients still in the hospital or the ICU). This difference disappeared after 90
days, as shown in (Figure 3).
p=0.028 p=0.338
Figure 3. Patient location on day 30 and day 90. The Chi-Square test was used to compare the two groups.
NRT = Nicotine replacement therapy.
ICU = Intensive Care Unit.
Safety evaluation
Serious adverse events (SAE)
In total, 15 SAE were reported, 4 in the NRT group and 11 in the control group (p=0.129).
The causes of death in the NRT group (n=2) were respiratory failure and hypercapnic coma
after extubation with treatment limitations. The 2 other SAE in the NRT group were
hemothorax and respiratory insufficiency after extubation. The causes of death in the control
group (n=3) were respiratory failure, refractory pneumosepsis and acute persistent severe
hypoxemia following no reintubation at patients request. In the control group, there were 8
other SAE including hemorrhagic shock, respiratory insufficiency (2 times), stoma necrosis,
duodenal perforation, sigmoid ischemia, asystole and ischemic colitis with abdominal
compartment syndrome and multi-organ failure. None of the SAEs were attributed to the
treatment with, or abstinence from nicotine.
Adverse events
There was no significant difference between treatment groups in the occurrence of 279
adverse events (p=0.096) (Table 4). However, it was remarkable that the frequency of
cardiovascular adverse events, tended to occur more often in the control group than in the
NRT group.
18
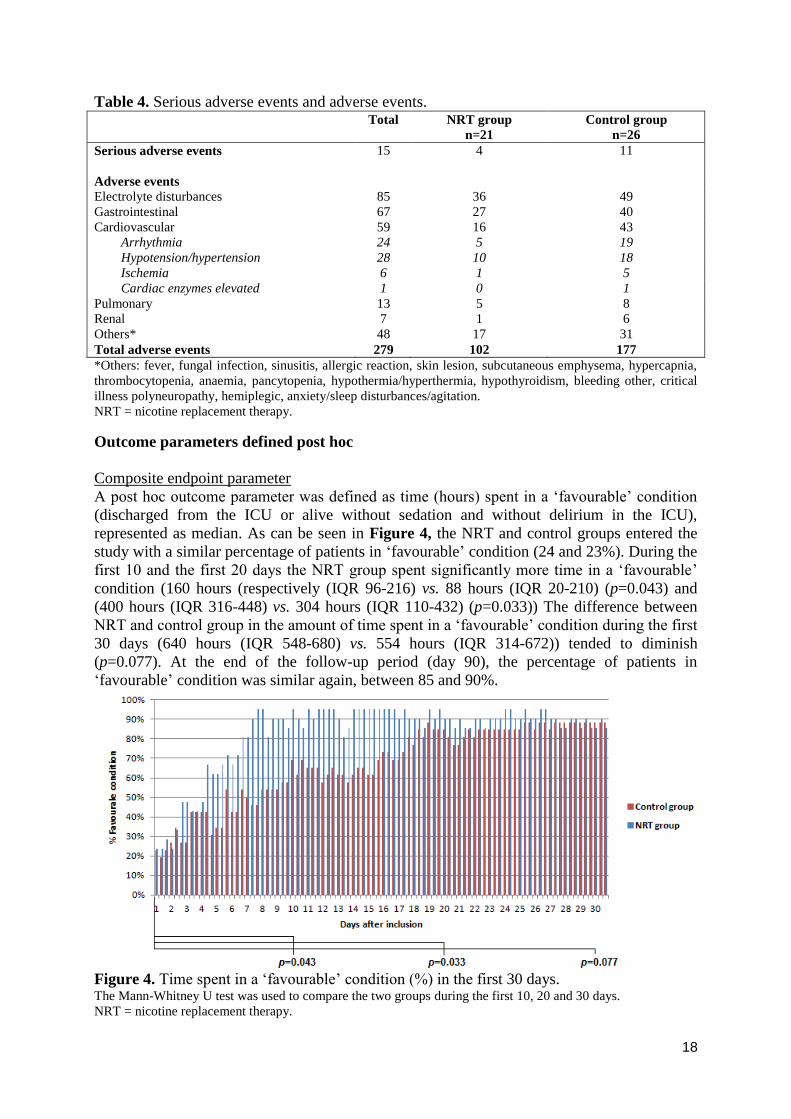
Table 4. Serious adverse events and adverse events. Total NRT group
n=21
Control group
n=26
Serious adverse events 15 4 11
Adverse events
Electrolyte disturbances 85 36 49
Gastrointestinal 67 27 40
Cardiovascular 59 16 43
Arrhythmia 24 5 19
Hypotension/hypertension 28 10 18
Ischemia 6 1 5
Cardiac enzymes elevated 1 0 1
Pulmonary 13 5 8
Renal 7 1 6
Others* 48 17 31
Total adverse events 279 102 177
*Others: fever, fungal infection, sinusitis, allergic reaction, skin lesion, subcutaneous emphysema, hypercapnia,
thrombocytopenia, anaemia, pancytopenia, hypothermia/hyperthermia, hypothyroidism, bleeding other, critical
illness polyneuropathy, hemiplegic, anxiety/sleep disturbances/agitation.
NRT = nicotine replacement therapy.
Outcome parameters defined post hoc
Composite endpoint parameter
A post hoc outcome parameter was defined as time (hours) spent in a ‘favourable’ condition
(discharged from the ICU or alive without sedation and without delirium in the ICU),
represented as median. As can be seen in Figure 4, the NRT and control groups entered the
study with a similar percentage of patients in ‘favourable’ condition (24 and 23%). During the
first 10 and the first 20 days the NRT group spent significantly more time in a ‘favourable’
condition (160 hours (respectively (IQR 96-216) vs. 88 hours (IQR 20-210) (p=0.043) and
(400 hours (IQR 316-448) vs. 304 hours (IQR 110-432) (p=0.033)) The difference between
NRT and control group in the amount of time spent in a ‘favourable’ condition during the first
30 days (640 hours (IQR 548-680) vs. 554 hours (IQR 314-672)) tended to diminish
(p=0.077). At the end of the follow-up period (day 90), the percentage of patients in
‘favourable’ condition was similar again, between 85 and 90%.
Figure 4. Time spent in a ‘favourable’ condition (%) in the first 30 days. The Mann-Whitney U test was used to compare the two groups during the first 10, 20 and 30 days.
NRT = nicotine replacement therapy.

19
Subgroup analysis dosage-effect relationship of nicotine replacement therapy
After dividing the study population into dosage groups 14 mg/day (n=23) and 21 mg/day
(n=24), the difference in time spent in ‘favourable’ condition between NRT and control
groups remained consistent (no statistics performed) (Supplementary figure 1). A presumed
stronger effect in the higher treatment group was not observed (Table 5). A correlation
between the serum cotinine and the number of cigarettes per day has not been found
(Supplementary figure 2A). Between the serum cotinine and the Fägerstrom test for nicotine
dependence no correlation had been found either (Supplementary figure 2B).
Table 5. Dosage-effect relationship of nicotine replacement therapy.
Time (hours) spent in a ‘favourable’ condition. During the first 10 days During the first 20 days During the first 30 days
Control group total 88 304 554
14 mg 56 304 528
21 mg 96 320 560
NRT group total 160 400 640
14 mg 200 440 680
21 mg 144 376 616
NRT = nicotine replacement therapy.
Multivariate analyses on the primary outcome parameter using randomisation strata
The odds ratio (OR; 95% CI) for 30-day mortality in a logistic univariate analysis for the
NRT group was 1.263 (0.163-9.815) suggesting that the risk for 30-day mortality was similar
between the NRT group and the control group (Table 6). After introducing the three
randomisation strata (patient type, dosage nicotine, study site) into a multivariate model, the
OR was 0.956 (0.111-8.228) (Table 6). As the CIs overlapped, patient type, dosage nicotine
and study site were not considered confounders for the lack of association between NRT or
control group and 30 day mortality.
Table 6. Univariate and multivariate analysis for 30-day mortality for the nicotine
replacement therapy group. Odds ratio Confidence interval
Univariate analysis 1.263 0.163-9.815
Multivariate analysis* 0.956 0.111-8.228
*After introducing the three randomisation strata (patient type, dosage nicotine, study site).
20
Discussion
The aim of this project as a pilot study was to evaluate on the feasibility of a randomized
controlled trial, to predict sample sizes and to explore alternatives for improvement of the
study design. Our results showed that, with some modifications of the trial design (discussed
below under ‘Recommendations’), a randomized controlled study to assess the safety and
efficacy of transdermal NRT in mechanically ventilated smokers admitted to the ICU is
feasible.
The objective of this pilot study was to assess the safety and efficacy of transdermal NRT in
mechanically ventilated smokers admitted to the ICU. Based on our study results, the
hypothesis that ‘the effect of transdermal NRT was equal to the effect of the control product
with respect to 30-day mortality in mechanically ventilated smokers admitted to the ICU’
could not be rejected.
Summary of main findings
The NRT and control groups were comparable with respect to baseline characteristics.
The results indicated that transdermal NRT in mechanically ventilated smokers had no
significant effect on 30-day and 90-day mortality. Relevant for the interpretation of these data
is that our study had limited power to identify such an effect, even if it existed. Therefore, the
null hypothesis could also not be confirmed. Based on our results, a large effect of NRT on
mortality would be unlikely. In previous studies there were varying results with respect to
mortality, ranging from increased to reduced risk or no difference, but all of these studies
were retrospective and of limited sample size, and therefore prone to unrecognized
confounding (34-37). In order to detect a 20% mortality difference (from 8% to 10%, as in
our study), applying commonly used cut-off values for type I and II errors (α = 0.05 and
power 80 %), a total number of 6452 patients would need to be randomized (see Appendix 5
for calculations). We are inclined to regard that as not feasible.
The patient location on day 30 was significantly different between the two groups with a
higher number of patients at home or in a care facility in the NRT group and more patients
located in the ICU or the hospital in the control group. This difference was no longer visible
on day 90. At this point, it is not clear what this means, as the observed difference was not
supported by other outcomes such as a longer stay in the ICU or in the hospital. There was
also no significant difference in other outcome parameters such as mechanical ventilation free
hours, hours with delirium, sedation/agitation scores, antipsychotic use, or any of the other
predefined secondary outcome parameters, although most of these parameters were trending
towards benefit for the NRT group.
The reason for stopping this study before 70 patients had been included was a low inclusion
rate. Although we did not exactly monitor the reasons for exclusion, it was felt that
recruitment proceeded much slower than anticipated due to the protocolized exclusion of
comorbidities such as acute myocardial infarction, severe cardiac arrhythmia or unstable
angina pectoris. These comorbidities are prevalent among smokers. On the other hand, in
critically ill and mechanically ventilated ICU patients, transient increases in cardiac enzymes
are common and it is often difficult to establish whether these are due to cardiac ischemia or
for example secondary to sepsis or other critical illnesses. We suspect that an unknown
number of patients have been excluded for this reason, in the absence of true coronary artery
disease. Because the numbers of adverse events, serious adverse events, and specifically
cardiac events were comparable between the two groups and actually trended toward benefit

21
in the NRT group, we would advocate that the exclusion of patients with cardiovascular
diseases in future NRT trials would be applied less strictly.
To summarize these findings, our study showed no relevant differences in predefined outcome
parameters. However, in order to get a better understanding of the prevalence of delirium and
agitation, and the interaction with the need for sedation in our study patients over time, a
composite outcome parameter was created post hoc. It was recognized that sedation and
delirium can be competing events, because delirium can not be measured in sedated patients
and patients may be sedated longer when signs of (hyperactive) delirium are present.
Therefore, this parameter was defined as time (hours) spent in a ‘favourable’ condition
(discharged from the ICU or alive without sedation and without delirium on in the ICU). Both
groups had a similar percentage of patients in a ‘favourable’ condition at the start of the study.
During the first 10 and 20 days the NRT group had spent significantly more time alive and
free of delirium and sedation or discharged from the ICU than the control group. When
comparing the two groups in the last 10 days (day 20 till day 30), this difference seemed to
gradually stagnate. At the end of the 30 days of study period, the majority of patients were
unsedated and free of delirium in both groups. A small percentage of patients (8% in the NRT
group and 10% in controls) was no longer alive at day 30. The observed differences remained
unaltered after correction for the stratification parameters in multivariate logistic analysis.
Strengths and weaknesses
The strength of this study lies in the fact that this was a randomized controlled study, which
can prevent selection bias and the influence of the results by confounders. The randomisation
was stratified to nicotine dosage (14 vs. 21 mg/day), study site (GVH vs. DH) and patient type
(medical vs. surgical) to prevent possible unequal distribution of these prognostic factors. This
stratification was used in combination with block randomisation in order to distribute the
intervention evenly on both study arms. As a result, groups were balanced well on baseline
characteristics. The internal validity was ensured by random treatment allocation that was
done by an independent party and by blinding of the patient, the investigator, and the
attending staff. The number of protocol violations was low. Moreover, follow-up was
complete for all subjects and analysis was done on an intention-to-treat (ITT) basis. The ITT-
analysis avoids bias associated with non-random loss of participants, which increases the
credibility of this research. In addition, there were few missing values which ensured high
quality of data including a representative overview of our group and thereby reducing the
probability of selection bias.
The study findings are limited by low event rates and a small sample size. This study was
underpowered to establish significant differences in primary and secondary outcome
parameters between the NRT group and the control group. It is of concern that due to small
numbers, relatively small baseline differences might become relevant confounders. Despite
adequate randomization, unrecognized confounders, which may not have been accounted for
in multivariate analysis, may have influenced the outcomes. Analyses that were not
predefined in the study protocol are particularly vulnerable to that. Furthermore, it can be seen
as an omission that the number of screened patients has not been recorded, as this figure in
combination with power analysis could have helped to determine the size of a future trial.
Only two ICUs were involved in this trial, which limits the generalizability and therefore
external validity to broader ICU settings. We selected ICU patients who were mechanically
ventilated, thereby being at risk of emergence of delirium and agitation (and possible death).
However, because of the strict exclusion criteria, especially the patients with cardiovascular
diseases (which may be related to their smoking behaviour) were excluded because of the

22
precaution of using NRT in these patients, while one might expect that these patients in
particular could benefit from NRT. In addition, delirium and sedation were only recorded
during ICU admission and when patients were discharged from the ICU it was assumed that
they were not delirious or sedated, which may not always be true. It would have been more
accurate to continue recording delirium scores on the general wards. Finally, the delirium and
agitation outcome parameter was defined post hoc. This puts these conclusions at risk of
being data driven. However, as this was a pilot study, these results can be useful to improve
future study designs.
Conclusion Our results demonstrated that, with proper modifications of the trial design, a randomized
controlled study to assess the safety and efficacy of transdermal NRT in mechanically
ventilated smokers admitted to the ICU would be feasible. In our pilot of 47 randomized
patients transdermal NRT in mechanically ventilated smokers had no effect on 30-day and 90-
day mortality, although our study was underpowered to establish such differences.
Furthermore, the number of (serious) adverse events between the two groups was comparable.
Finally, patients with NRT spent more time being discharged from the ICU or alive and free
from delirium and sedation during the first 20 days after ICU admission.
Recommendations
Despite the fact that this was a two-centre pilot study with a small sample size, some positive-
trending results indicated the need for further randomized studies. Enrolling more subjects to
increase the power of the study would help to better define the effects of NRT in the ICU
setting. In a future study, we would suggest that limiting the cardiovascular exclusion criteria
could augment patient recruitment. This might be justified, because the potential of benefit of
NRT is the largest in heavy smokers, who by necessity bring along related comorbidities. Our
pilot showed no trend towards cardiovascular harm in the NRT group. Excluding too many
active smokers might limit not only the practical feasibility, but also the generalizability of a
future NRT trial. We would also suggest that future trials should not focus on mortality, but
rather on predefined delirium and agitation endpoints. The difficulty with quantifying
delirium is that patients may be sedated longer to attenuate the related restlessness, and also
that delirium itself might increase mortality. In this way, the prevalences of sedation and
death may actually compete with the prevalence of delirium. One way to manage competing
events would be, as we did in our post hoc analysis, to create a composite end-point of
delirium and agitation free days. This has been done in other delirium studies in the ICU
population (48). The separation on the composite delirium endpoint between the NRT and the
control groups was most pronounced between day 4 and day 21 of the study period. In order
to avoid unnecessary data collection we would recommend a study period of 2 to 3 weeks
after admission to the ICU. This is supported by the theory that nicotine withdrawal
symptoms also peak in the first 2 to 3 weeks (23). Furthermore, we advise that data should be
collected on delirium in the period after ICU discharge as well, to obtain reliable data for the
entire follow up period. In Appendix 5 an example of a power analysis is presented that would
provide 80% power and an α of 0.05 if one were to use the composite delirium and agitation
endpoint that we proposed in our post hoc analysis to design a future RCT. This power
analysis shows that to reveal a difference of 2 days on this composite endpoint (time
discharged from the ICU or spent alive on the ICU without sedation or delirium during the
first 20 days) 218 patients would be needed. A multicentre trial in this order of magnitude
would be feasible. Being a multifactorial disorder, an intervention study to diminish delirium
is particularly prone to confounding by imbalances at study entry. Therefore, a balanced
allocation design might deserve consideration, stratifying at baseline for factors that are
23
known to influence the delirium risk, such as alcohol or nicotine use, disease severity or age
(4). From the literature it is known that, infection, changes in medication, acute illness and
pre-existing delirium
might be relevant confounders to consider (4,11). Although the findings of our study are
valuable and warrant further investigation, based on the data published thus far, considerable
reserve is warranted with regards to the use of NRT in patients admitted to the ICU. Earlier
studies have pointed to potential harm and this study does not change that. Future studies
must reveal whether or not the transdermal NRT is safe and efficacy in smokers admitted to
the ICU.
Acknowledgments
Special thanks to my daily supervisor Huub van den Oever for his support and feedback
during the research clerckship and to my second supervisor Ben de Jong. I would like to thank
them for the opportunity to conduct this reseach clerkship with their supervision.
Gratitude is also expressed to Arriette Kruisdijk-Gerritsen, Maurits Arbouw, Arthur van
Zanten en Esther van ’t Riet for their help during the research clerkship.

24
References
(1) Moss M, Burnham EL. Alcohol abuse in the critically ill patient. Lancet 2006 Dec
23;368(9554):2231-2242.
(2) American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders,
fifth edition (DSM-5) 2013 May.
(3) Steiner LA. Postoperative delirium. Part 1: pathophysiology and risk factors. Eur J
Anaesthesiol 2011 Sep;28(9):628-636.
(4) Zaal IJ, Devlin JW, Peelen LM, Slooter AJ. A systematic review of risk factors for
delirium in the ICU. Crit Care Med 2015 Jan;43(1):40-47.
(5) Dubois MJ, Bergeron N, Dumont M, Dial S, Skrobik Y. Delirium in an intensive care
unit: a study of risk factors. Intensive Care Med 2001 Aug;27(8):1297-1304.
(6) Lucidarme O, Seguin A, Daubin C, Ramakers M, Terzi N, Beck P, et al. Nicotine
withdrawal and agitation in ventilated critically ill patients. Crit Care 2010;14(2):R58.
(7) Mayer SA, Chong JY, Ridgway E, Min KC, Commichau C, Bernardini GL. Delirium
from nicotine withdrawal in neuro-ICU patients. Neurology 2001 Aug 14;57(3):551-553.
(8) Hsieh SJ, Shum M, Lee AN, Hasselmark F, Gong MN. Cigarette smoking as a risk factor
for delirium in hospitalized and intensive care unit patients. A systematic review. Ann Am
Thorac Soc 2013 Oct;10(5):496-503.
(9) Salluh JI, Wang H, Schneider EB, Nagaraja N, Yenokyan G, Damluji A, et al. Outcome of
delirium in critically ill patients: systematic review and meta-analysis. BMJ 2015 Jun
3;350:h2538.
(10) Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE,Jr, et al. Delirium as
a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA
2004 Apr 14;291(14):1753-1762.
(11) Zaal IJ, Slooter AJ. Delirium in critically ill patients: epidemiology, pathophysiology,
diagnosis and management. Drugs 2012 Jul 30;72(11):1457-1471.
(12) Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and
consequences of ICU delirium. Intensive Care Med 2007 Jan;33(1):66-73.
(13) Micek ST, Anand NJ, Laible BR, Shannon WD, Kollef MH. Delirium as detected by the
CAM-ICU predicts restraint use among mechanically ventilated medical patients. Crit Care
Med 2005 Jun;33(6):1260-1265.
(14) Van Rompaey B, Elseviers MM, Schuurmans MJ, Shortridge-Baggett LM, Truijen S,
Bossaert L. Risk factors for delirium in intensive care patients: a prospective cohort study.
Crit Care 2009;13(3):R77.
(15) Clark BJ, Moss M. Secondary prevention in the intensive care unit: does intensive care
unit admission represent a "teachable moment?". Crit Care Med 2011 Jun;39(6):1500-1506.
(16) Centers for Disease Control and Prevention (CDC). Current cigarette smoking
prevalence among working adults--United States, 2004-2010. MMWR Morb Mortal Wkly
Rep 2011 Sep 30;60(38):1305-1309.
(17) Benowitz NL, Schultz KE, Haller CA, Wu AH, Dains KM, Jacob P,3rd. Prevalence of
smoking assessed biochemically in an urban public hospital: a rationale for routine cotinine
screening. Am J Epidemiol 2009 Oct 1;170(7):885-891.
(18) Calfee CS, Matthay MA, Eisner MD, Benowitz N, Call M, Pittet JF, et al. Active and
passive cigarette smoking and acute lung injury after severe blunt trauma. Am J Respir Crit
Care Med 2011 Jun 15;183(12):1660-1665.

25
(19) Hsieh SJ, Ware LB, Eisner MD, Yu L, Jacob P,3rd, Havel C, et al. Biomarkers increase
detection of active smoking and secondhand smoke exposure in critically ill patients. Crit
Care Med 2011 Jan;39(1):40-45.
(20) EPA Guidance on tobacco dependence and strategies for smoking cessation in people
with mental illness - Scientific Figure on ResearchGate. Available at:
https://www.researchgate.net/260022901_tbl1_Table-3-American-Psychiatric-Association-
DSM-IV-TR-and-World-Health-Organization. Cited 2017 Jan 24.
(21) Farmacotherapeutisch Kompas. Middelen bij de behandeling van verslavingsziekten
Nicotine. Available at: https://www.farmacotherapeutischkompas.nl/bladeren-volgens-
boek/preparaatteksten/n/nicotine. Cited 2017 Jan 24.
(22) Bijsluiter van Nicotinell. Nicotinell TTS 30, 21 mg/24 uur, pleister voor transdermaal
gebruik Nicotine. Available at: http://db.cbg-meb.nl/Bijsluiters/h14831.pdf. Cited 2017 Jan
24.
(23) Hughes JR. Effects of abstinence from tobacco: valid symptoms and time course.
Nicotine Tob Res 2007 Mar;9(3):315-327.
(24) Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with
nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-
analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis
2010 Jul 13;8:8-9625-8-8.
(25) West R, Zhou X. Is nicotine replacement therapy for smoking cessation effective in the
"real world"? Findings from a prospective multinational cohort study. Thorax 2007
Nov;62(11):998-1002.
(26) Hatsukami DK, Stead LF, Gupta PC. Tobacco addiction. Lancet 2008 Jun
14;371(9629):2027-2038.
(27) Stead LF, Perera R, Bullen C, Mant D, Hartmann-Boyce J, Cahill K, et al. Nicotine
replacement therapy for smoking cessation. Cochrane Database Syst Rev 2012 Nov
14;11:CD000146.
(28) Hartmann-Boyce J, Aveyard P. Drugs for smoking cessation. BMJ 2016 Feb
23;352:i571.
(29) Rigotti NA. Clinical practice. Treatment of tobacco use and dependence. N Engl J Med
2002 Feb 14;346(7):506-512.
(30) Drug and Therapeutics Bulletin. Republished: Nicotine and health. BMJ 2014 Nov
26;349:2014.7.0264rep.
(31) Hukkanen J, Jacob P,3rd, Benowitz NL. Metabolism and disposition kinetics of nicotine.
Pharmacol Rev 2005 Mar;57(1):79-115.
(32) Giardina EG. Cardiovascular effects of nicotine. Nov 05, 2015; Available at:
https://www.uptodate.com/contents/cardiovascular-effects-of-nicotine. Cited 2017 Mar 16.
(33) Panos NG, Tesoro EP, Kim KS, Mucksavage JJ. Outcomes associated with transdermal
nicotine replacement therapy in a neurosurgery intensive care unit. Am J Health Syst Pharm
2010 Aug 15;67(16):1357-1361.
(34) Kerr A, McVey JT, Wood AM, Van Haren F. Safety of nicotine replacement therapy in
critically ill smokers: a retrospective cohort study. Anaesth Intensive Care 2016
Nov;44(6):758-761.
(35) Seder DB, Schmidt JM, Badjatia N, Fernandez L, Rincon F, Claassen J, et al.
Transdermal nicotine replacement therapy in cigarette smokers with acute subarachnoid
hemorrhage. Neurocrit Care 2011 Feb;14(1):77-83.
(36) Lee AH, Afessa B. The association of nicotine replacement therapy with mortality in a
medical intensive care unit. Crit Care Med 2007 Jun;35(6):1517-1521.

26
(37) Paciullo CA, Short MR, Steinke DT, Jennings HR. Impact of nicotine replacement
therapy on postoperative mortality following coronary artery bypass graft surgery. Ann
Pharmacother 2009 Jul;43(7):1197-1202.
(38) Gillies MA, McKenzie CA, Whiteley C, Beale RJ, Tibby SM. Safety of nicotine
replacement therapy in critically ill smokers: a retrospective cohort study. Intensive Care Med
2012 Oct;38(10):1683-1688.
(39) Cartin-Ceba R, Warner DO, Hays JT, Afessa B. Nicotine replacement therapy in
critically ill patients: a prospective observational cohort study. Crit Care Med 2011
Jul;39(7):1635-1640.
(40) Pathak V, Rendon IS, Lupu R, Tactuk N, Olutade T, Durham C, et al. Outcome of
nicotine replacement therapy in patients admitted to ICU: a randomized controlled double-
blind prospective pilot study. Respir Care 2013 Oct;58(10):1625-1629.
(41) Wilby KJ, Harder CK. Nicotine replacement therapy in the intensive care unit: a
systematic review. J Intensive Care Med 2014 Jan-Feb;29(1):22-30.
(42) Kowalski M, Udy AA, McRobbie HJ, Dooley MJ. Nicotine replacement therapy for
agitation and delirium management in the intensive care unit: a systematic review of the
literature. J Intensive Care 2016 Nov 15;4:69.
(43) Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-
associated infection and criteria for specific types of infections in the acute care setting. Am J
Infect Control 2008 Jun;36(5):309-332.
(44) Srinivasan A. Vital signs: central line-associated blood stream infections – United States,
2001, 2008, and 2009. MMWR Morb Mortal Wkly Rep 2011;60:243-248. .
(45) Moreno R, Vincent JL, Matos R, Mendonca A, Cantraine F, Thijs L, et al. The use of
maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a
prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM.
Intensive Care Med 1999 Jul;25(7):686-696.
(46) Centers for Disease Control and Prevention (CDC). Vital signs: central line-associated
blood stream infections--United States, 2001, 2008, and 2009. MMWR Morb Mortal Wkly
Rep 2011 Mar 4;60(8):243-248.
(47) Kahan BC, Morris TP. Reporting and analysis of trials using stratified randomisation in
leading medical journals: review and reanalysis. BMJ 2012 Sep 14;345:e5840.
(48) Pandharipande PP, Pun BT, Herr DL, Maze M, Girard TD, Miller RR, et al. Effect of
sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically
ventilated patients: the MENDS randomized controlled trial. JAMA 2007 Dec
12;298(22):2644-2653.
27
Appendix 1
AUDIT test om alcoholafhankelijkheid te meten 1. Hoe vaak drinkt u alcohol? □ 4 of meer keer per week 4 punten
□ 2 tot 3 keer per week 3 punten □ 2 tot 4 keer per maand 2 punten □ 1 keer per maand of minder 1 punt □ Nooit 0 punten 2. Op een dag waarop u alcohol drinkt, hoeveel glazen drinkt u dan gewoonlijk? □ 10 of meer 4 punten
□ 7 tot 9 3 punten □ 5 of 6 2 punten □ 3 of 4 1 punt □ 1 of 2 0 punten 3. Hoe vaak zijn er gelegenheden waarop u 6 of meer glazen alcohol drinkt? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten 4. Hoe vaak heeft u het afgelopen jaar gemerkt dat u niet kon stoppen met drinken als u
eenmaal begonnen was? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten 5. Hoe vaak was u in het afgelopen jaar vanwege drankgebruik niet in staat om de dingen te
doen die normaal van u verwacht worden? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten 6. Hoe vaak heeft u het afgelopen jaar ’s ochtends alcohol nodig gehad om weer op gang te
komen nadat u veel had gedronken? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten 7. Hoe vaak heeft u zich het afgelopen jaar schuldig gevoeld of spijt gehad nadat u
gedronken had? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten

28
8. Hoe vaak kon u zich het afgelopen jaar niet herinneren wat de vorige avond gebeurd was
doordat u gedronken had? □ Dagelijks of bijna dagelijks 4 punten
□ Wekelijks 3 punten □ Maandelijks 2 punten □ Minder dan 1 keer per week 1 punt □ Nooit 0 punten 9. Bent uzelf, of is iemand anders ooit gewond geraakt doordat u gedronken had? □ Ja, in het afgelopen jaar 4 punten □ Ja, maar niet in het afgelopen jaar 2 punten □ Nee 0 punten 10. Heeft een familielid, vriend, dokter of andere hulpverlener zich ooit zorgen gemaakt over
uw drankgebruik of u aangeraden om minder te drinken? □ Ja, in het afgelopen jaar 4 punten □ Ja, maar niet in het afgelopen jaar 2 punten □ Nee 0 punten Totaal aantal punten:

29
Appendix 2
Test van Fagerström om nicotineafhankelijkheid te meten 1. Wanneer steekt u na het ontwaken uw eerste sigaret op? □ Binnen 5 minuten 3 punten □ Binnen 30 minuten 2 punten □ Binnen 60 minuten 1 punt □ Na meer dan 60 minuten 0 punten 2. Vindt u het moeilijk om niet te roken op plaatsen waar dit is verboden, bijvoorbeeld de
kerk, bibliotheek of bioscoop? □ Ja 1 punt □ Nee 0 punten 3. Welke sigaret kunt u het moeilijkste missen? □ De eerste sigaret ’s morgens 1 punt □ Alle andere sigaretten 0 punten 4. Hoeveel sigaretten rookt u per dag? □ 31 of meer 3 punten □ 21 – 30 2 punten □ 11 – 20 1 punt □ 10 of minder 0 punten 5. Rookt u meer tijdens de eerste uren na het ontwaken dan de rest van de dag? □ Ja 1 punt □ Nee 0 punten 6. Rookt u als u zo ziek bent dat u gedurende het grootste gedeelte van de dag in bed moet
blijven? □ Ja 1 punt □ Nee 0 punten Totaal aantal punten:

30
Appendix 3

31
Appendix 4
The SOFA score
The SOFA score describes the degree of organ dysfunction over time and evaluates morbidity
in ICU patients. The SOFA scoring scheme daily assigns 1 to 4 points to each of the
following six organ systems depending on the level of dysfunction: respiratory, circulatory,
renal, haematology, hepatic and central nervous system. The point score is calculated by
summing the worst scores for each organ system from admission until randomisation or until
maximally 24 hours after admission (for screening) or over the scheduled calendar days.
The APACHE II score
APACHE II score is an adult ICU severity of disease classification system. The point score is
calculated by summing the worst scores from 12 routine physiological measurements during
the first 24 hours after admission (temperature, mean arterial pressure, heart rate,
respiratory rate, oxygenation, arterial pH, serum sodium, potassium and creatinine,
hematocrit, white blood cell count, and Glascow Coma Scale), a history of chronic organ
insufficiency or immunosuppresion, age and the absence/presence of acute renal failure.
The APACHE IV score
APACHE IV score is an adult ICU severity of disease classification system. The point score
is calculated by summing the highest and/or lowest values from 19 physiological
measurements during the first 24 hours after admission (temperature, systolic and diastolic
blood pressure, heart rate, respiratory rate, FiO2, arterial pH, arterial PO2 and PCO2, serum
sodium, glucose, creatinine, albumin, bilirubin, blood urea nitrogen, urine output, white
blood cell count, hematocrit, Glascow Coma Scale), age, chronic health condition and ICU
admission information.

32
Appendix 5
Sample size calculations
In order to detect a 20% mortality difference (from 8 to 10%, as in our study), applying
commonly used cut-off values for type I and II errors (α = 0.05 and power 80 %), a total
number of 6452 patients would need to be randomized.
(z1-α/2 + z1-β)2 (σ1
2+σ2
2)
n1 = n2 = ----------------------------
(m1-m2)2
σ1 = standard deviation for the NRT group = 0.301
σ2 = standard deviation for the control group = 0.272
m1 = mean value of the NRT group = 0.10
m2 = mean value of the control group = 0.08
n1 = n2 = 3225,866 (rounded to 3226) per treatment arm
n x 2 = 6452
A power analysis that provides 80% power and an α of 0.05 if one were to use the composite
delirium and sedation endpoint that we proposed in our post hoc analysis to design a future
RCT. It shows that to reveal a difference of 2 days on this composite endpoint (time
discharged from the ICU, or spent alive on the ICU without sedation or delirium during the
first 20 days), 218 patients would be needed.
n2= 2 x ((s 12+ s 2
2)/2) (z1-α/2 + z1-β)
2
-----------------------------------
ν2
ν = difference = 2 days (2 days = 6 shifts of 8 hours)
s 1 = standard deviation for the NRT group = 10.505
s 2 =standard deviation for the control group = 19.717
n2 = 109
n x 2 = 218
33
Supplementary figures
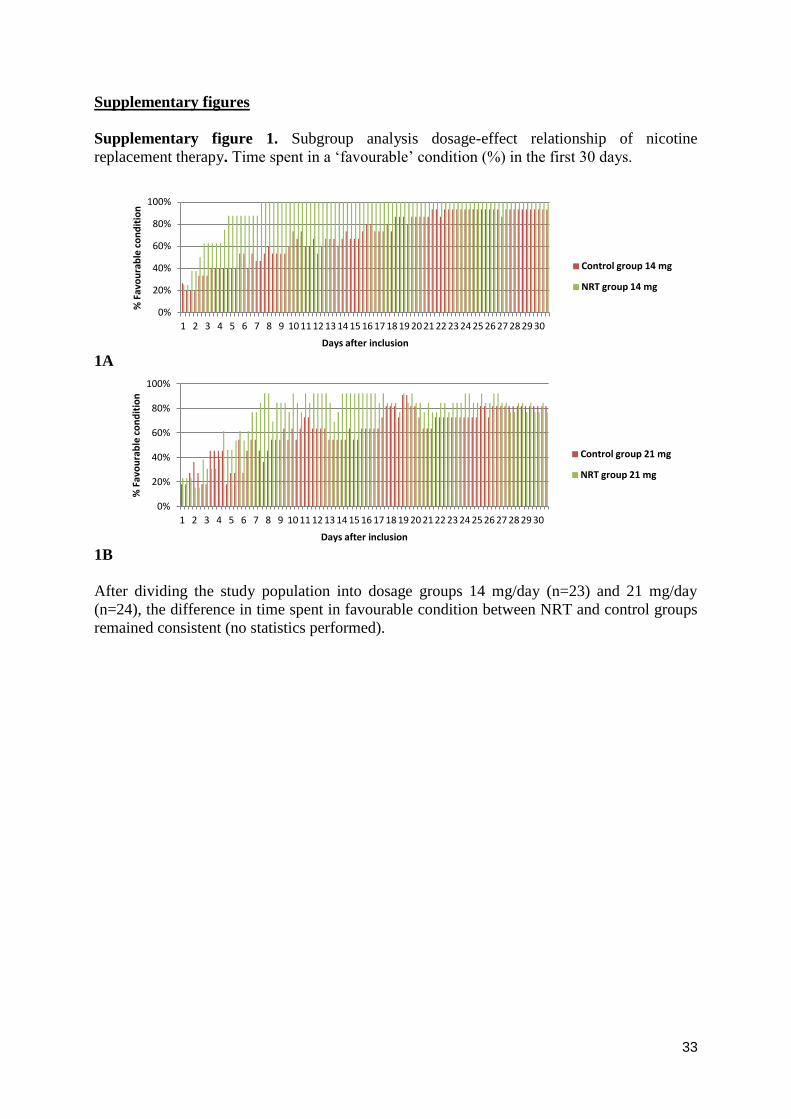
Supplementary figure 1. Subgroup analysis dosage-effect relationship of nicotine
replacement therapy. Time spent in a ‘favourable’ condition (%) in the first 30 days.
1A
1B
After dividing the study population into dosage groups 14 mg/day (n=23) and 21 mg/day
(n=24), the difference in time spent in favourable condition between NRT and control groups
remained consistent (no statistics performed).
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
% F
avo
ura
ble
co
nd
itio
n
Days after inclusion
Control group 14 mg
NRT group 14 mg
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
% F
avo
ura
ble
co
nd
itio
n
Days after inclusion
Control group 21 mg
NRT group 21 mg
34
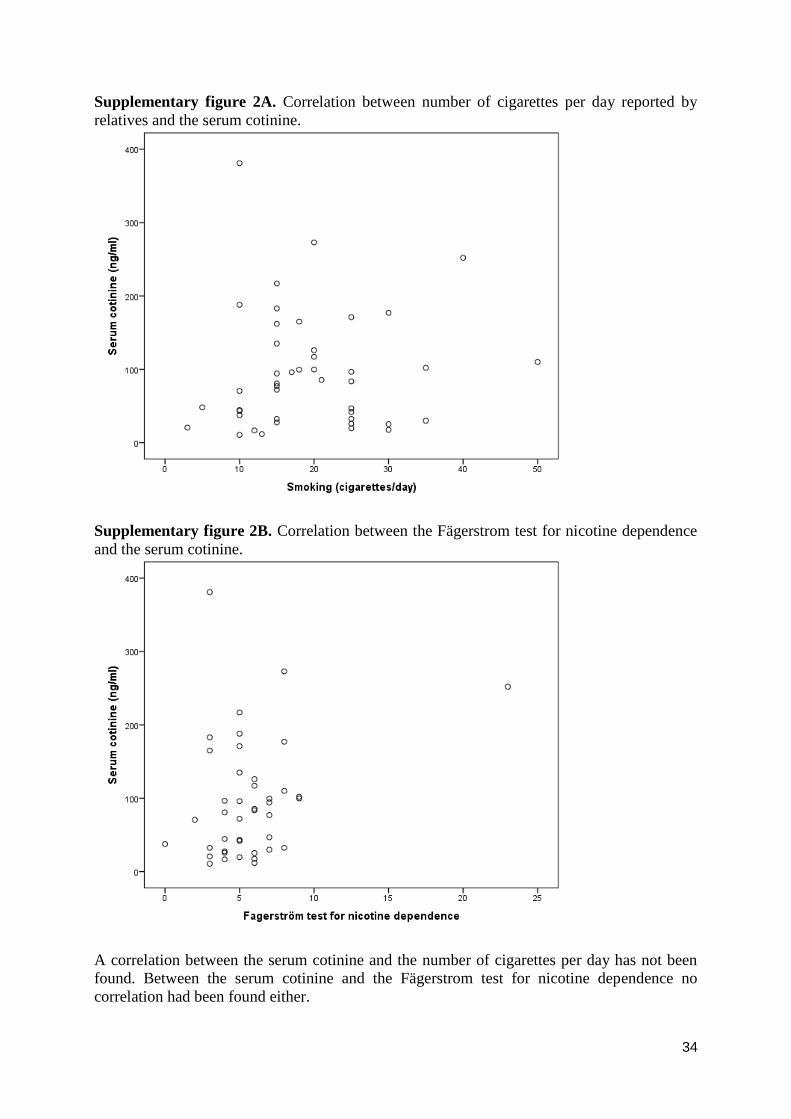
Supplementary figure 2A. Correlation between number of cigarettes per day reported by
relatives and the serum cotinine.
Supplementary figure 2B. Correlation between the Fägerstrom test for nicotine dependence
and the serum cotinine.
A correlation between the serum cotinine and the number of cigarettes per day has not been
found. Between the serum cotinine and the Fägerstrom test for nicotine dependence no
correlation had been found either.