pvd, aaa and renal stones dörthe and jo. case study bob, 70 years old 1 month history intermittent...
TRANSCRIPT

PVD, AAA and renal stones
Dörthe and Jo
Case Study
• Bob, 70 years old• 1 month history intermittent back pain

HPCS lumbosacral
Q Dull achy sensationSometimes sharp
I 5-7 /10
T IntermittentVaries in duration
A Low back movement, standing, sitting, drivingPartially relieved by tramadol
R Radiates to posterior leg
S No morning stiffnessNo bowel/ bladder problemNo lower limb weakness or tingling sensationNo weight loss or feverNo interruption to walkingNo recent trauma/heavy lifting

PMH/ Risk factorsRisk factor Importance / Relevance
HypertensionHypercholesterolaemiaSmokingDiabetes
Atherosclerosis
Age 5% of population over 6015% of population over 80
FHx Genetic in 10-20% of First degree relatives-Marfan’s-Ehler’s Danlos
Gender Male to female ratio 6:1

Presenting complaint of AAA
Aneurysm •asymp
tomatic
Increasing size
• epigastric or back pain
Leak/ Rupture
•Testicular pain
•Collapse
•Abdominal pain

On Examination
• Feel above the umbilicus for aortic aneurysm• If leaking or rupture
HypotensionTachycardia
pallor
Pulsatile mass
Abdominal painBack pain
Definition
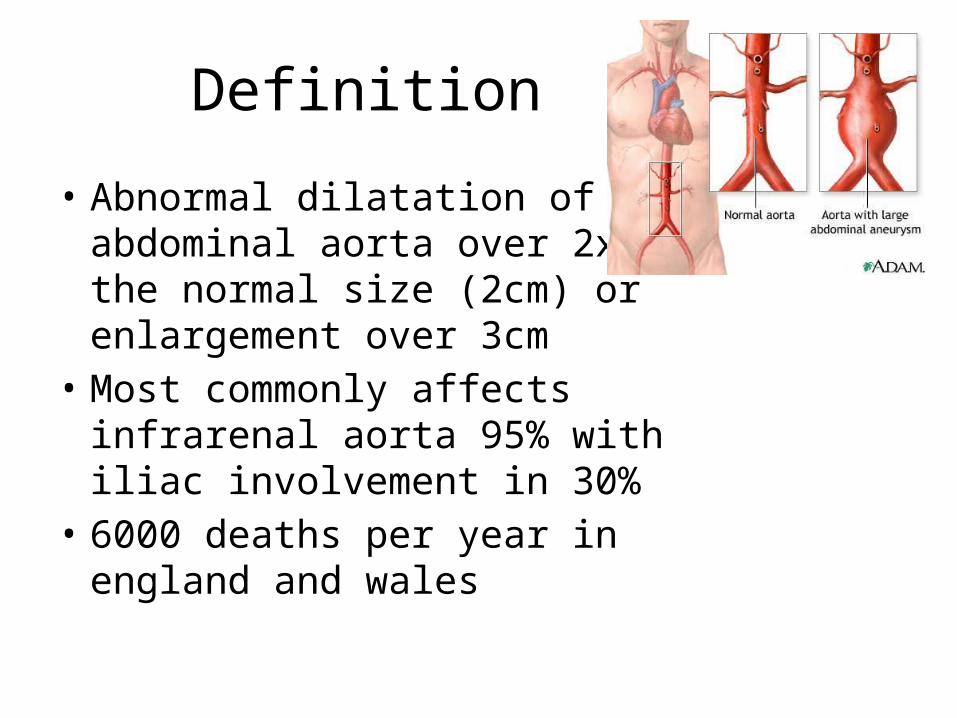
• Abnormal dilatation of abdominal aorta over 2x the normal size (2cm) or enlargement over 3cm
• Most commonly affects infrarenal aorta 95% with iliac involvement in 30%
• 6000 deaths per year in england and wales

True or false aneurysm?
• True aneurysm– Dilatation of all three layers of vessel
• False aneurysm– Dilatation of artery not involving all three layers

Aetiology
• Atherosclerotic in 95%• 5% inflammatory
• Others– Traumatic– Infective (mycotic aneurysm)– CTD – Ehler’s Danlos,Marfans
Pathophysiology
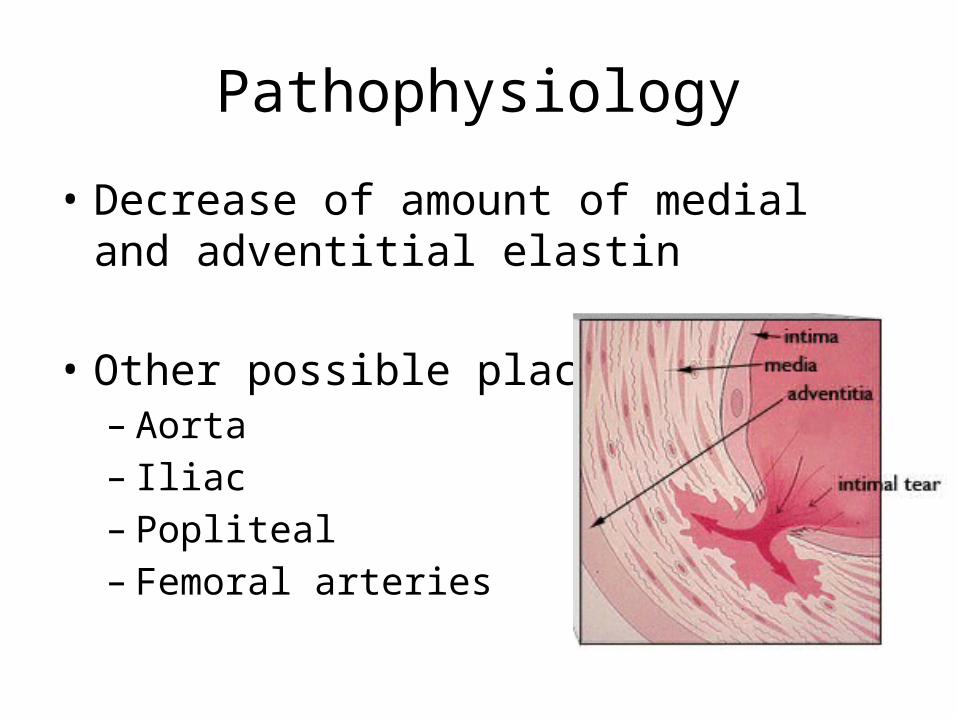
• Decrease of amount of medial and adventitial elastin
• Other possible places– Aorta– Iliac– Popliteal – Femoral arteries

Investigations
• Acute – CT scan, Bloods, ECG• US for screening purposes ( over
65 )• AAA on AXR – eggshell
appearance due to calcification aneurysm wall
Management
• Conservative– If asymptomatic– Under 5.5cm
– Regular follow ups with US
– Management of cardiovascular risk factors
• Surgical– Prosthetic graft
placement – rewrapping of native aneurysm around to reduce incidence of enterograft fistula formation
– Endovascular EVAR – placement stent through distant percutaneous access

Criteria for surgery
1. AAA over 5.5 cm2. Rupture3. Rapid growth4. Embolisation of plaque5. Symptomatic
Complications
General• Risk of rupture
– Under 5cm – 4%– 5-7cm diameter – 7%– More than 7cm – 20%
• Rupture• Distal embolus• Sudden complete
thrombosis• Fistulae formation• Infection
Of surgery• Elective mortality – under
4%• Emergency surgery
mortality 50%• Haemorrhage• Graft infection• Thrombosis/embolism• Colonic ischaemia• Renal failure
Peripheral vascular disease

Definition
• Also called peripheral arterial disease• Occlusive atherosclerotic disease in lower
extremities• Occlusion distal to aortic arch• Up to 12% of 55-70year old affected• Rare causes – vasculitis, Buerger’s disease

Atherosclerosis
• Atheromas containing cholesterol and lipid form within intima and inner media, often accompanied by ulceration and smooth muscle hyperplasia
• Risk factors – hypertension, smoking, diabetes, FHx, hypercholesterolaemia, high LDL, obesity

Smooth muscle hyperplasia and plaque deposition
Growth factor release
Platelets adhere
Endothelial injury
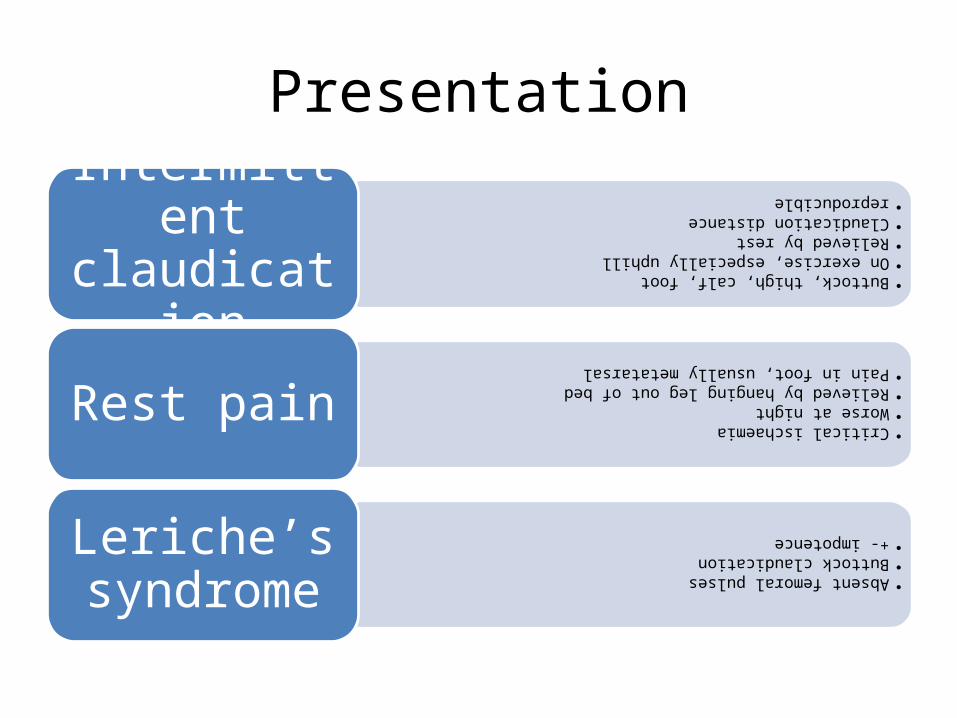
Presentation
•Buttock, thigh, calf, foot
•On exercise, especially uphill
•Relieved by rest
•Claudication distance
•reproducible
Intermittent claudication
•Critical ischaemia
•Worse at night•Relieved by
hanging leg out of bed
•Pain in foot, usually metatarsal
Rest pain
•Absent femoral pulses
•Buttock claudication
•+- impotence
Leriche’s syndrome

On examination
• Legs– Weak/ absent pulses– Reduced CRT– Cold, pale legs– Hair loss– Atrophic skin changes– Painful, punched out ulcers – pressure areas– venous ulceration – medial malleolus
• Also examine CVS

Investigations
• Handheld Doppler• ABPI – Normal= 1, claudication <0.6, rest pain <0.4
• Bloods –anaemia, ESR, thrombophilia screen, lipids
• ECG - ?CAD• Arterial Duplex• CT angiogram• Angiogram

Cx of PVD
• Amputation• Gangrene– Dry – dry necrosis of tissue without signs of infection– Wet – moist necrotic tissue with signs of infection
• Ulcers
• Risk of limb loss with claudication 5% per year• Risk of limb loss with rest pain over 50% per year

Management – Conservative and Medical
RF
• Smoking• Exercise• Weight• Statins• Anti HTN• DM Mx
Antiplatelets
• Aspirin• Clopidogrel
Vasodilators
• Naftidrofuryl oxalate

Surgical Management
• Indications– Disabling claudication– Critical ischaemia– Weak/absent femoral pulses
• Angioplasty +- stenting• Surgical bypass graft

Prognosis
• High risk for all-risk mortality, especially cardiovascular
• 15% progress to critical ischaemia• 50% improve• 25% stabilise• 20% worsen– 20% need intervention– 8% need amputation