report chronic pain dutch council for the quality of health care prof.dr. frank huygen department...
TRANSCRIPT

Report Chronic Pain Dutch Council for the Quality of Health Care
Prof.dr. Frank Huygen
Department Anesthesiology Painmedicine Erasmusmc
Rotterdam The Netherlands
Disclosure
European Scientific and educational advisoryboard "Change Pain"
Global Scientific advisorboard Spinal Modulation (Spinal Modulation)
Editorial board "Painpractice" (Wiley Blackwell)
Editorial board "Praktische richtlijnen anesthesiologische pijnbestrijding"
(Tijdstroom)
Editorial board "Evidence based interventional painmedicine" (Wiley Blackwell)
Teacher "educational programs neuropathic pain" (Pfizer)
Chairman multidisciplinary guideline committee mechanical low back (orde van
medisch specialisten)
Chairman workgroup chronic pain Dutch council for the quality of health care
Member workgroup development indicators "failed back surgery syndrome"
(Zichtbare Zorg ziekenhuizen)
Member program committee NeuroSIPE (Stichting Technische
Wetenschappen)

Prevalence chronic pain in Europa
• Mean percentage chronic pain: 19% (n= 8815)
Breivik et al 2006
Chronic pain-> 6 months-piain in the previous months-≥ 2 x a week- ≥ 5 on a 10 point NRS

Prevalence chronic pain compared to other chronic diseases in the Netherlands
Bala et al 2011
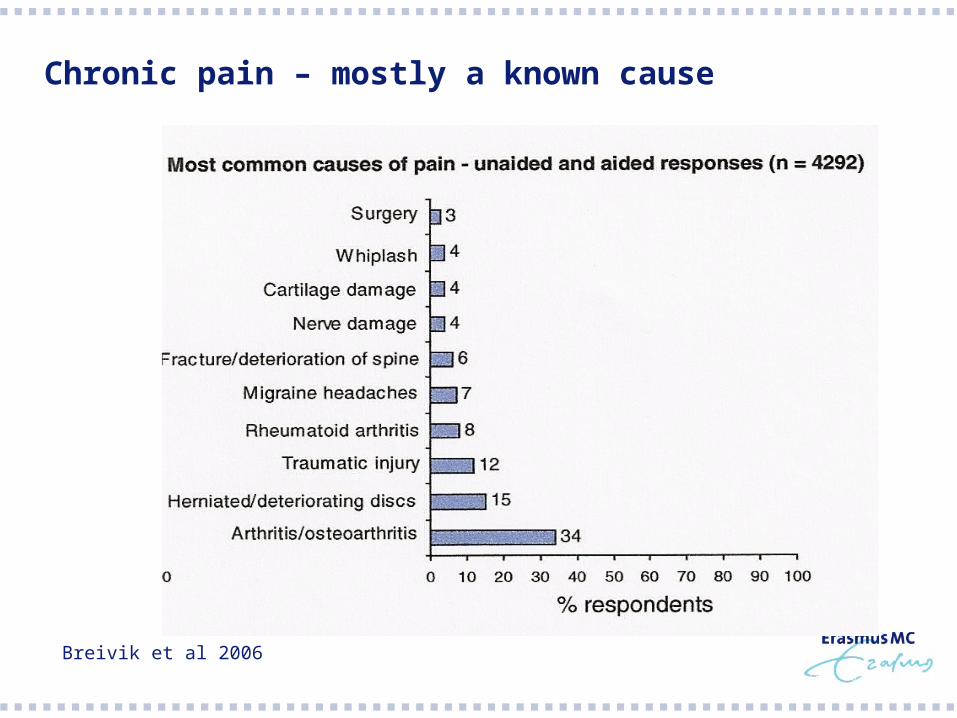
Chronic pain – mostly a known cause
Breivik et al 2006

Involved healthcare professionals
Breivik et al 2006

Dutch Council for the Quality of Health Care
Established in 2009 by the Minister of Health to promote high-quality
care in the Netherlands. The working area of the Council covers
prevention, cure and long-term care. The Council sets tasks for
advisory and research activities and gives recommendations. The
activities are mainly aimed at increasing safety, enhancing the
patient/client perspective and stimulating the efficacy of care.
Examples of topics of the Council for the quality of health care
Guideline on Guidelines
Prioritised list of guideline topics
Expensive drugs in guidelines and off label use of drugs
Restructuring 2nd line obstetric care – an exploration on the effects of concentration
Deducting valid and trustworthy patient information from authorised guidelines
www.regieraad.nl

Council –Chronic pain
November 2010
Presentation data epidemiology of chronic pain in the Netherlands
January 2011
Initiation workgroup chronic pain council
April 2011
Pressure cooker session
September 2011
Presentation report workgroup to council

Presentation data epidemiology of chronic pain in the Netherlands
Prevalence chronic pain > other
chronic diseases, however it gets less
attention
Diagnosis and treatment have a great
variety and are often inadequate
Chronic pain has a big impact on
quality of life and functionality and has
high direct and indirect costs
Bala et al 2011

Workgroup chronic pain council
Name Discipline
Dr. Dolf Boerman Neurologist
Dr. Jannes J.E. van Everding Secretary council
Drs. Ruud Gardenbroek Medical adviser
Marion Giesberts Pain nurse
Prof.dr. Frank Huygen Anesthesiologist
Prof.dr. Bart Koes Epidemiologist, general practice
Dr. Ingeborg Meijer, Independent advisor
Dr. Roberto S.G.M Perez Physiotherapist/movement scientist
Prof.dr. Rob J.E.M. Smeets Rehabilitation doctor
Ilona Thomassen Patient
Dr. Gerbrig Verstegen, Psychologist
Prof.dr. Pieter A.M. Vierhout Chairman council
Prof.dr. Kris Vissers Anesthesiologist

Workgroup chronic pain council
Members of the workgroup are invited based on:
Individual title
Longterm approved involvement in chronic pain
Representative for different stakeholders

Pressure cooker session
Discussion based on “statements” brought in by participants
Statements
Chronic pain is a disease in its own right
A national guideline on chronic pain could improve diagnosis and
treatment
A mechanism based treatment is preferred
Besides attention for the cause and treatment of pain, there should be
more attention for perception and behaviour

Statements
(un)justified fear for opioid dependency results in undertreatment
There is not enough attention for pain medicine in the educational
programs for healthcare professionals
Insurance/social doctors are not well enough equipped to estimate
chronic pain
Statements
There are huge health care and socio-economic costs in chronic pain
Chronic pain is so prevalent that disease management/chain care is
necessary to come to a solution. The first line plays a key role in
prevention and treatment
A discipline oriented care system is an obstruction for a solution of the
pain problem. Pain medicine will benefit from a patient oriented
approach
Profits can be gained with prevention and early recognition and
treatment of chronic pain
Discussion
Broadening and deepening of pain medicine is necessary
But
On short term the biggest profit is gained by simple interventions in
non-pain specialists

Conclusion and recommendations
Put chronic pain on the agenda of the council in 2012
Use the workgroup chronic pain as a platform which together with
partners in the field searches for solutions to improve care of patients
with chronic pain

Conclusions and recommendations
Develop together with the scientific associations and other
stakeholders a national guideline on chronic pain
Starting questions for such a guideline would be:
- Definition and classification system
- Prescription of analgesics, therapy compliance, prevention of
addiction
- Algorithm for diagnosis and treatment
- Use of psychometric instruments in diagnosis
- Prevention
- Impairment in chronic @@@

Conclusions and recommendations
Stimulate education and training in pain medicine
Stimulate the development of research programs for chronic pain

Comment round
Asked for attention for specific groups, e.g. chronic pain in the eldery
Asked about the responsibilities of different scientific associations

1st step
Publication report chronic pain by council
Consultation General practitioners association about development
guideline chronic pain

1st Step
Handover report to chairman of permanent parliamentary commission
Thank you for your attention
Discussion?