ria vergara-lluri - lasop.comlasop.com/pgs/hdouts/2012-05_ria vergara-lluri - diagnosis.pdf · ria...
TRANSCRIPT
Ria Vergara-Lluri Resident, PGY-4
David Geffen School of Medicine at UCLA
Submission to Los Angeles Society of Pathology (LASOP) Resident and Fellow Symposium 2012
A Unique Sarcoma with Dual Morphologic, Cytogenetic, and Molecular Signatures

Pertinent history and symptoms
43 year old woman presented in 2011 with recurrent soft tissue tumor in the left arm
In 2004, at age 35, she presented at another institution with a 5-year history of a left arm mass (7.5 x 5.5 x 4 cm), which was resected and diagnosed as a sarcoma**
Because she lost her medical insurance, she did not receive any further therapy after surgical resection
At re-presentation in 2011, she had a large, protuberant and firm soft tissue mass (9.6 x 7.6 x 6.5 cm ) located along the posterior arm/triceps muscle
Based on diagnosis of high-grade sarcoma,** patient received induction chemotherapy followed by surgical resection with intraoperative and subsequent external beam radiation
**Diagnoses will be revealed later

External and cut surfaces of recurrent
tumor (9.6 x 7.6 x 6.5 cm)









S-100
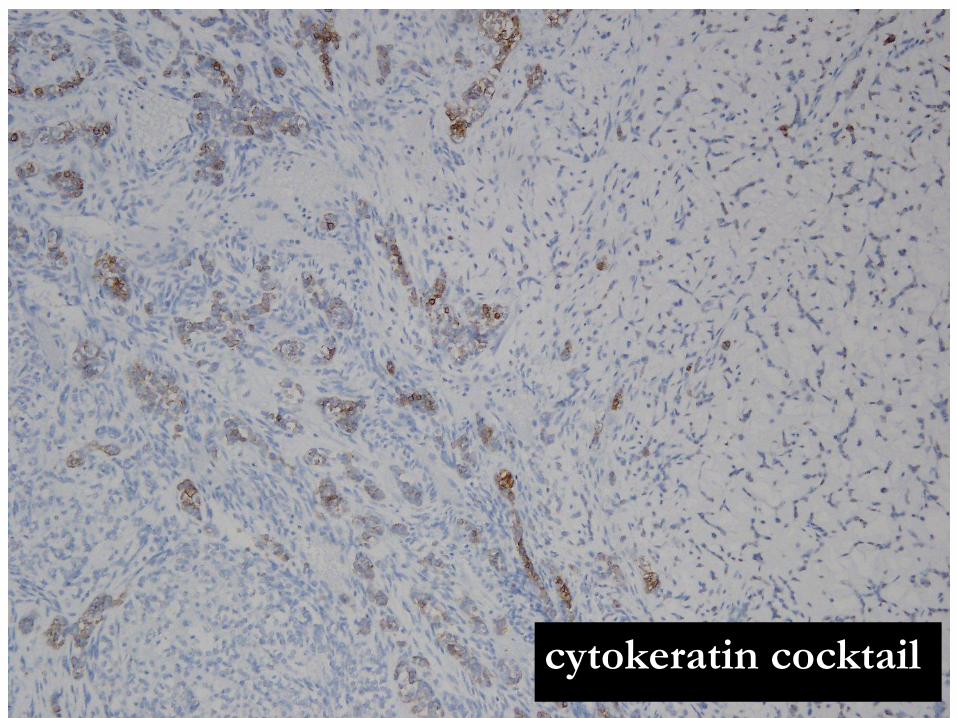
cytokeratin cocktail

bcl-2

Summary of Morphologic and
Immunohistochemical (IHC) Features
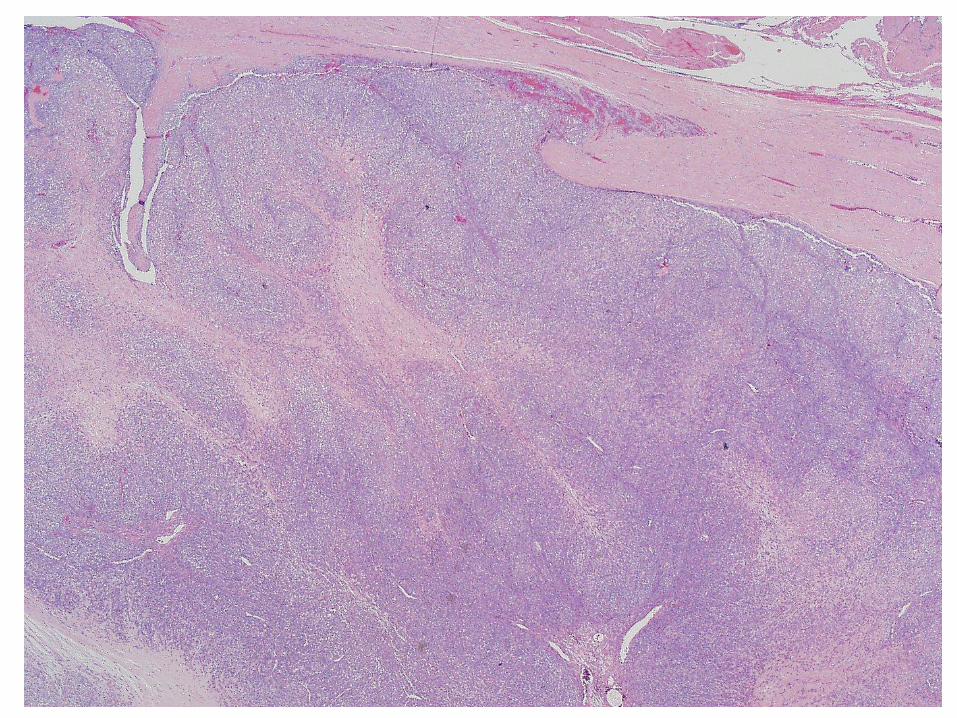
Variably cellular and multinodular neoplasm
Hypercellular areas with spindled cells in streaming to storiform growth pattern
Hypocellular areas with round cells embedded in fibromyxoid to hyalinized stroma
Hypercellular areas exhibit subtle transition to hypocellular areas
Round cells with eccentrically placed nuclei, irregular nuclear contours, hyperchromasia, multiple chromocenters, and moderate amount of dense eosinophilic cytoplasm
Mitotic activity up to 12 mf/10 high power fields
Post-treatment necrosis approximately 20%
Lymphovascular space invasion present
IHC positive for S-100 (patchy), cytokeratin cocktail AE1/AE3 + CAM5.2 (patchy), EMA (patchy), MUC4 (focal), and bcl-2 (diffuse)
IHC negative for CD99, synaptophysin, chromogranin, SMA, calponin, GFAP, desmin, myogenin

Differential Diagnosis
Soft tissue myoepithelioma (aka soft tissue
mixed tumor or parachordoma)
Extraskeletal Myxoid Chondrosarcoma
(EMC)
Synovial Sarcoma (SS)
Further cytogenetic and molecular testing
performed on original and recurrent
tumors
FISH
RT-PCR to elucidate the gene fusion partners
for EWSR1 and SYT rearrangements in
tumors
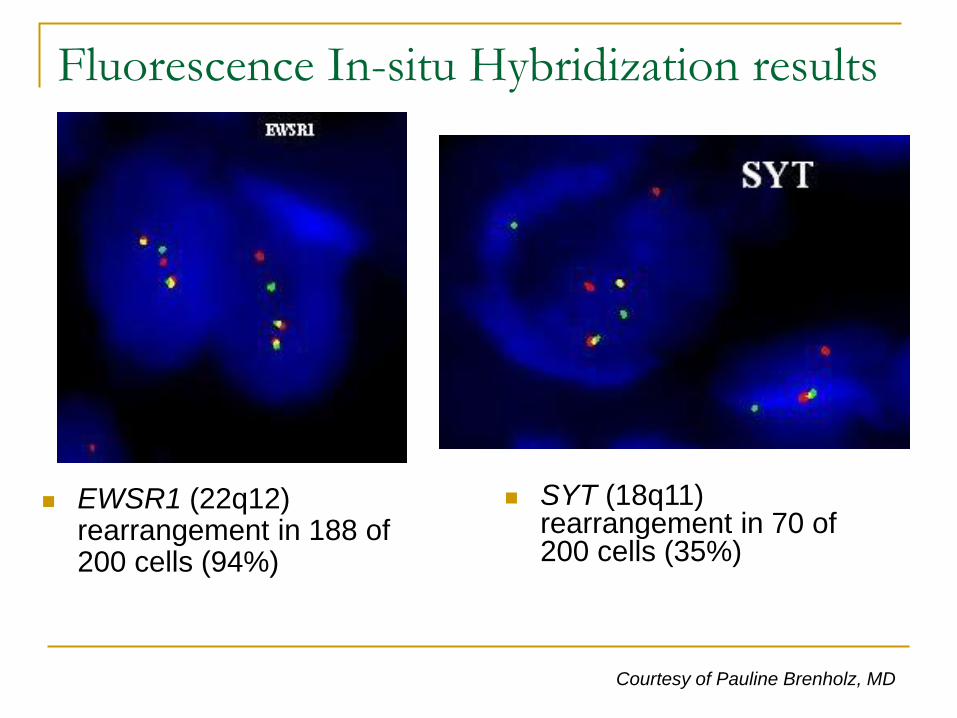
Fluorescence In-situ Hybridization results
EWSR1 (22q12) rearrangement in 188 of 200 cells (94%)
SYT (18q11) rearrangement in 70 of 200 cells (35%)
Courtesy of Pauline Brenholz, MD

RT-PCR fusion results
EWS:NR4A3 fusion
product from
t(9;22)(q22;q12)
characteristic of
EMC
AGAGGCCTTATGGATATGACCAG
EWS exon 12
ATCATGCCCAAG
NR4A3 exon 3
TGGTTTGATG
SS18 exon 10
ATATGCCCTGCGTCCAAG
SSX2 exon 6
SS18-SSX2 fusion
product from
t(X;18)(p11;q11)
characteristic of SS

Diagnosis
Sarcoma with dual morphologic, cytogenetic,
and molecular signatures of extraskeletal
myxoid chondrosarcoma and synovial
sarcoma
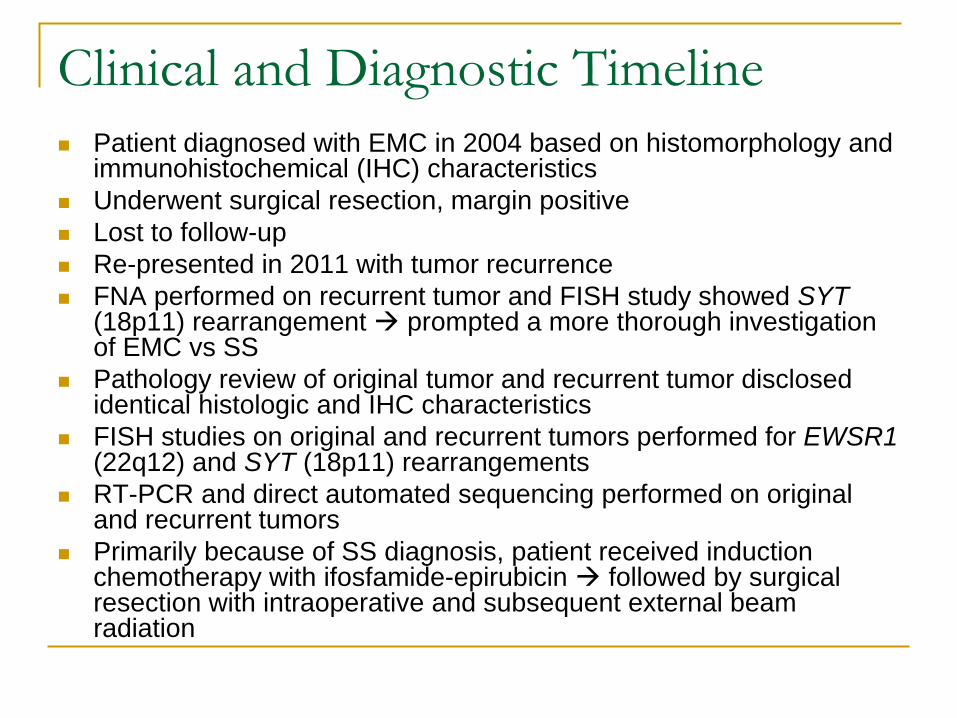
Clinical and Diagnostic Timeline
Patient diagnosed with EMC in 2004 based on histomorphology and immunohistochemical (IHC) characteristics
Underwent surgical resection, margin positive
Lost to follow-up
Re-presented in 2011 with tumor recurrence
FNA performed on recurrent tumor and FISH study showed SYT (18p11) rearrangement prompted a more thorough investigation of EMC vs SS
Pathology review of original tumor and recurrent tumor disclosed identical histologic and IHC characteristics
FISH studies on original and recurrent tumors performed for EWSR1 (22q12) and SYT (18p11) rearrangements
RT-PCR and direct automated sequencing performed on original and recurrent tumors
Primarily because of SS diagnosis, patient received induction chemotherapy with ifosfamide-epirubicin followed by surgical resection with intraoperative and subsequent external beam radiation
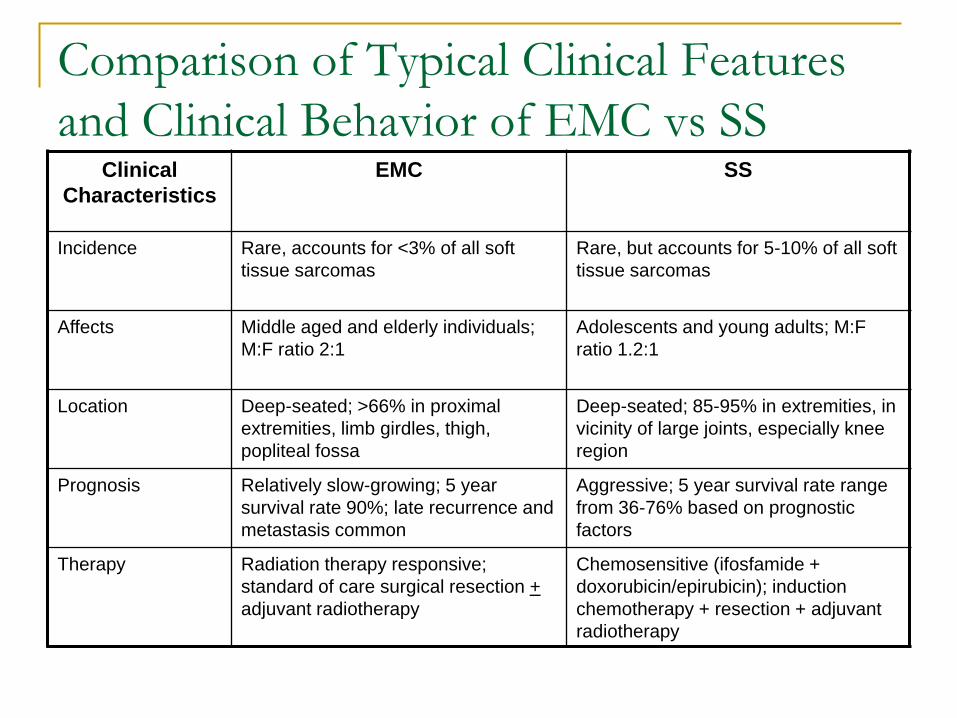
Comparison of Typical Clinical Features
and Clinical Behavior of EMC vs SS Clinical
Characteristics
EMC SS
Incidence Rare, accounts for <3% of all soft
tissue sarcomas
Rare, but accounts for 5-10% of all soft
tissue sarcomas
Affects Middle aged and elderly individuals;
M:F ratio 2:1
Adolescents and young adults; M:F
ratio 1.2:1
Location Deep-seated; >66% in proximal
extremities, limb girdles, thigh,
popliteal fossa
Deep-seated; 85-95% in extremities, in
vicinity of large joints, especially knee
region
Prognosis Relatively slow-growing; 5 year
survival rate 90%; late recurrence and
metastasis common
Aggressive; 5 year survival rate range
from 36-76% based on prognostic
factors
Therapy Radiation therapy responsive;
standard of care surgical resection +
adjuvant radiotherapy
Chemosensitive (ifosfamide +
doxorubicin/epirubicin); induction
chemotherapy + resection + adjuvant
radiotherapy

Comparison of Histopathologic and
Immunohistochemical Features of EMC vs SS
Features EMC Monophasic SS
Spindle cell population Sometimes Characteristic
Abundant myxoid
matrix
Characteristic Sometimes
Multinodularity Characteristic Sometimes
Epithelioid cells Characteristic Focally
S-100 + (18-50%) + (30%)
Cytokeratin cocktail - + (69%)
EMA + (30%) + (97%)
MUC4 - + (30%)
bcl-2 + (>95%) + (>95%)

Comparison of Molecular Signatures
Associated with EMC vs SS
Translocations Genes Incidence
Extraskeletal
myxoid
chondrosarcoma
t(9;22)(q22;q12)
t(9;17)(q22;q11)
t(9;15)(q22;q21)
NR4A3*;EWS
NR4A3;RBP56**
NR4A3;TCF12
70%
20%
Synovial
Sarcoma
t(X;18)(p11;q11) SS18-SSX1
SS18-SSX2
SS18-SSX4
>95%
*NR4A3, also known as CHN, NOR1, TEC
**RBP56, also known as TAF15

Significance of this finding
First sarcoma reported in the literature with two translocation-defining abnormalities
(EWS-NR4A3 & SS18-SSX2)
Tumor displays morphologic and immunophenotypic overlap between EMC & SS
Reinforces idea that specific genetic alterations can drive tumor morphology
The discovery of SS18-SSX2 fusion (in addition to EWS-NR4A3 fusion) allowed clinical team to institute a more effective chemoradiation regimen directed toward synovial sarcoma
As molecular testing for tumors becomes more widespread, perhaps more tumors with dual differentiation will be discovered lead to greater understanding of the link between specific gene rearrangements and morphology and clinical behavior

Acknowledgements
This work was accepted for publication to American
Journal of Surgical Pathology** on January 2012
UCSF
- Andrew Horvai, MD, PhD (principal investigator)
- Bradley Stohr, MD, PhD
Integrated Genetics (formerly Genzyme)
- Pauline Brenholz, MD
Kaiser Oakland
- Balaram Puligandla, MD
**All figures used in this presentation are original and were not used for publication.

References
Fletcher CDM, Unni KK, Mertens F. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon: IARC Press, International Agency for Research on Cancer; 2002.
Weiss SW, J.R. G. Enzinger and Weiss's Soft Tissue Tumors. Philadelphia: Elsevier; 2008.
Meis-Kindblom JM, Bergh P, Gunterberg B, et al. Extraskeletal myxoid chondrosarcoma: a reappraisal of its morphologic spectrum and prognostic factors based on 117 cases. Am J Surg Pathol. 1999;23:636-650.
Iliszko M, Rys J, Wozniak A, et al. Complex tumor-specific t(X;18) in seven synovial sarcoma tumors. Cancer Genet Cytogenet. 2009;189:118-121.
Krane JF, Bertoni F, Fletcher CD. Myxoid synovial sarcoma: an underappreciated morphologic subset. Mod Pathol. 1999;12:456-462.
Cooney TP, Hwang WS, Robertson DI, et al. Monophasic synovial sarcoma, epithelioid sarcoma and chordoid sarcoma: ultrastructural evidence for a common histogenesis, despite light microscopic diversity. Histopathology. 1982;6:163-190.
Fisher C, Schofield JB. S-100 protein positive synovial sarcoma. Histopathology. 1991;19:375-377.
Sun B, Sun Y, Wang J, et al. The diagnostic value of SYT-SSX detected by reverse transcriptase-polymerase chain reaction (RT-PCR) and fluorescence in situ hybridization (FISH) for synovial sarcoma: a review and prospective study of 255 cases. Cancer Sci. 2008;99:1355-1361.
Daugaard S, Christensen LH, Hogdall E. Markers aiding the diagnosis of chondroid tumors: an immunohistochemical study including osteonectin, bcl-2, cox-2, actin, calponin, D2-40 (podoplanin), mdm-2, CD117 (c-kit), and YKL-40. APMIS 2009 Jul;117(7):518-25.
Suster S, Fisher C, Moran CA. Expression of bcl-2 oncoprotein in benign and malignant spindle cell tumors of soft tissue, skin, serosal surfaces, and gastrointestinal tract. Am J Surg Pathol 1998;22:863-72.
Doyle LA, Moller E, et al. MUC4 is a highly sensitive and specific marker for low-grade fibromyxoid sarcoma. Am J Surg Pathol 2011;35:733-41.